Embed Size (px)
Citation preview

R E S EARCH ART I C L E
EP I L EPSY
Spreading depolarization in the brainstemmediates sudden cardiorespiratory arrest inmouse SUDEP modelsIsamu Aiba1 and Jeffrey L. Noebels1,2,3*
http://stmD
ownloaded from
Cardiorespiratory collapse after a seizure is the leading cause of sudden unexpected death in epilepsy (SUDEP)in young persons, but why only certain individuals are at risk is unknown. To identify a mechanism for thislethal cardiorespiratory failure, we examined whether genes linked to increased SUDEP risk lower the thresholdfor spreading depolarization (SD), a self-propagating depolarizing wave that silences neuronal networks. Micecarrying mutations in Kv1.1 potassium channels (−/−) and Scn1a sodium ion channels (+/R1407X) phenocopymany aspects of human SUDEP. In mutant, but not wild-type mice, seizures initiated by topical application of 4-aminopyridine to the cortex led to a slow, negative DC potential shift recorded in the dorsal medulla, a brain-stem region that controls cardiorespiratory pacemaking. This irreversible event slowly depolarized cells andinactivated synaptic activity, producing cardiorespiratory arrest. Local initiation of SD in this region by potas-sium chloride microinjection also elicited electroencephalographic suppression, apnea, bradycardia, andasystole, similar to the events seen in monitored human SUDEP. In vitro study of brainstem slices confirmedthat mutant mice had a lower threshold for SD elicited by metabolic substrate depletion and that immaturemice were at greater risk than adults. Deletion of the gene encoding tau, which prolongs life in these mutants,also restored the normal SD threshold in Kv1.1-mutant mouse brainstem. Thus, brainstem SD may be a criticalthreshold event linking seizures and SUDEP.
.sc
by guest on November 29, 2020
iencemag.org/
INTRODUCTION
Sudden unexpected death in epilepsy (SUDEP) is the leading cause ofmortality in individuals with seizure disorders (1). Among neurolog-ical disorders, SUDEP is second only to stroke in the number of po-tential life years lost (2). One major class of causative genes expressedin the heart and brain (3–5) and two epidemiological SUDEP riskfactors (younger age and high incidence of pharmacoresistant sei-zures) have been identified, but the mechanisms leading to suddenautonomic collapse at the moment of death remain to be elucidated.Effective prediction or intervention is currently unavailable.
Most individuals with epilepsy experience tachycardia and onlytransient hypoxia during a seizure as a result of central respiratorydepression or tonic spasm of the diaphragm. Rarely, paradoxical slow-ing of heart rate or even prolonged cardiac asystoles are recorded, butboth are reversible during or within moments after the seizure (6).One-third of unwitnessed SUDEP instances lack evidence of a recentseizure (7). However, more than 10% of patients with chronic refrac-tory temporal lobe epilepsy eventually fail to self-resuscitate after a sei-zure, with variable patterns of electroencephalographic (EEG) andcardiorespiratory shutdown at the moment of death (8–10). Studiesin humans (11, 12) and in mouse models (2, 5) suggest the presenceof a rare genetic dysregulation of a centrally mediated autonomicfunction in individuals at risk for SUDEP, arising from intrinsic mem-brane hyperexcitability or reduced synaptic inhibition in pathwaysthat slow the heart rate or alter gasp reflexes. However, the basis of
1Developmental Neurogenetics Laboratory, Department of Neurology, and NIH/NINDSCenter for SUDEP Research, Baylor College of Medicine, Houston, TX 77030, USA.2Department of Neuroscience, Baylor College of Medicine, Houston, TX 77030, USA.3Department of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX77030, USA.*Corresponding author. E-mail: [email protected]
www.Sc
the irreversibility is unclear, and why, especially in a person at highgenetic risk, the first seizure is not also the last is unknown.
Spreading depolarization (SD) is a pathological, self-regeneratingwave of depolarization in neurons and glia that is associated with ex-cess glutamate release and extracellular potassium elevation. A varietyof factors regulate the onset and propagation of the slow (2 to 6 mm/min)wave, which contributes to transient human neurological deficits dur-ing cerebral ischemia, trauma, and migraine (13). SD has been studied inthe neocortex, hippocampus, and brainstem, where it produces pro-found reversible or irreversible loss of neural activity (14, 15). AlthoughSD can be evoked experimentally by high potassium or tetanic neu-ronal stimulation, it can also arise spontaneously during limited en-ergy substrate availability (hypoxia and ischemia) or hyperthermia.Each of these conditions may also provoke seizures. Despite this sharedvulnerability, seizure and SD have nonoverlapping age- and region-dependent thresholds (16–18). We reasoned that a high thresholdfor SD normally acts as a protective barrier against dysregulation ofthe central autonomic output initiated by the seizure itself, preventinga fatal outcome. Therefore, we investigated whether the threshold forbrainstem SD is lower in genetic SUDEP mouse models and exploredthe possibility that such a decreased threshold could mediate centralautonomic death.
RESULTS
Brainstem SD coincides with terminal cardiorespiratorydysregulation during seizuresKv1.1 channels conduct a critical potassium current in neurons thatprevents hyperexcitability, and mice lacking the gene recapitulate crit-ical SUDEP phenotypes, including frequent generalized seizures, auto-nomic instability, and premature death at a young age (4, 19). We
ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 1

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
investigated the excitability in the dorsalmedulla during seizures triggered in thecortex of these anesthetized juvenile mice[postnatal day 18 (P18) to P25], an agewhen roughly 50% of Kv1.1 mice diesuddenly. We generated recurrent corti-cal seizures by topical focal applicationof 4-aminopyridine (4AP) within a smallcranial window over the somatosensorycortex (Fig. 1, A and B) of wild-type andKv1.1−/− [knockout (KO)] animals. Appli-cation of 4AP onto Kv1.1 KO cortex trig-gered seizures with postictal suppressionof cortical EEG, ictal and peri-ictal apnea,transient bradycardia, and asystoles (Fig.1 and figs. S1 and S2). At least one epi-sode of reversible apneic bradycardia/asystole was observed in 84% (21 of 24)of Kv1.1 KO mice tested. We performedDC recordings in the dorsal medulla of 18of these mice, and 50% (9 of 18) showedsudden brainstem SD coincident with au-tonomic failure, which was uniformlyand rapidly fatal (Fig. 1C). In all ninemice, fatal autonomic failure and corticalEEG suppression coincided with a slowDC potential shift (mean amplitude,−17.8 ± 7.4 mV) in the dorsal medulla(Fig. 1, D and E), linking this brainstemevent to fatal autonomic collapse. In con-trast, cortical seizures had minimal cardio-respiratory effects in wild-type mice (Fig. 2,A to D), with 100% postictal survival (n = 15;Fig. 1C). Brainstem SD was not detectedin these mice (Fig. 2A).
There was a variable latency (1 to 3min)between the onset of arrhythmias andapneas, which occurred during the sei-zure, and detection of SD after the end ofthe seizure (Fig. 3A), which may havebeen in part due to microscopic differencesin the placement of the brainstem record-ing electrode and in the patterns of SDpropagation. The time to complete cardi-ac arrest after the onset of irrecoverablesinus bradycardia was ~3 min and wasusually preceded by loss of cortical EEGactivity and apneas, although variationsin this sequence were observed, as inmonitored human cases (8).
We noted a variable amount of time(up to ~13 min) between the end of a cor-tical seizure and the onset of the lethal car-
diorespiratory depression, whereas the brainstem SD was followed closelyby cardiorespiratory arrest and death in KO mice (Fig. 3A). Figure 3 (Band C) shows a detailed analysis of the two recordings from the Kv1.1KO mice shown in Fig. 1. In Fig. 3B, brainstem SD occurred 17 s afterthe termination of a brief seizure and coincided with postictal corticalwww.Sc
EEG suppression and cardiorespiratory depression. Full cardiac arrestoccurred 230 s later. The power spectra of the recurrent cortical sei-zures before death were similar and did not clearly predict the onset ofbrainstem SD. In another case (Fig. 3C), brainstem SD appeared over11 min after the seizure. In every case, however, the normal respiration
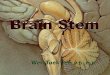
Fig. 1. Premorbid cardiorespiratory dysregulation and brainstem SD in Kv1.1 mutant associatedwith cortical seizures in vivo. (A) Diagram of experimental setup for application of 4AP and recording of
EEG and brainstem DC potentials in spontaneously breathing urethane-anesthetized juvenile mice (P18 toP25). (B) Illustration of brainstem recording area (red circle). (C) Time until death in Kv1.1 wild-type (WT)and KO mice after focal 4AP application. (D and E) Representative traces of premorbid sequence of thecortical EEG, brainstem DC current, ECG, and respiration in two Kv1.1 KO mice. Expanded traces shown inthe lower half of the panels illustrate the temporal association between loss of cortical EEG activity, brain-stem SD, and development of cardiorespiratory arrhythmias. Asterisk, gasping. (D) Immediate postictalEEG flattening tightly coupled to onset of cardiorespiratory dysregulation and brainstem SD. Vertical scale:cortical EEG, 0.35 mV; brainstem DC, 5 mV; ECG, 0.22 mV; respiration, arbitrary units. (E) Delayed corticalsuppression and cardiorespiratory shutdown >10 min after final intense seizure activity. The respiratorytrace in the box is further expanded and shown in the inset. Vertical scale: cortical EEG, 0.31 mV; brainstemDC, 18 mV; ECG, 0.43 mV; respiration, arbitrary units.ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 2

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
patterns seen before the seizure (Fig. 3D) were severely disrupted dur-ing (Fig. 3E) and after (Fig. 3F) the seizure, and audible agonal breath-ing (that is, inspiratory stridor) was frequently detected. Ventilatory
www.ScienceTranslationalMedi
compromise produced a severe drop in blood oxy-gen saturation in two mice, falling from >90% to38 and 36%.
Similar experiments were conducted in Scn1aR1407X mice, a second SUDEP mouse model(20), containing a knock-in (Ki) truncation mu-tation that causes Dravet Syndrome in humans,an epileptic encephalopathy with a highly ele-vated risk for postictal EEG suppression, cardiacinstability, and SUDEP (21). In six juvenile mu-tant mice (P20 to P30), the evoked seizures re-sulted in bradycardia and apneas, and four micedied of sudden cardiorespiratory arrest coincid-ing with the onset of brainstem DC shifts (Fig. 4,A and B).
These in vivo results implicate hypoxia, a crit-ical determinant of SD threshold, in the demiseof Kv1.1 KO animals, as reported for humans (1, 22).By inactivating the nucleus tractus solitarius (NTS)and dorsal vagal motor nuclei, which are criticalcentral pathways supporting tissue oxygenation,SD in this region may produce further hypoxia,leading to a vicious spiral progressing to terminalcardiorespiratory arrest.
Locally evoked brainstem SDtriggers cardiorespiratory arrest andcortical EEG suppressionTo separate the contribution of brainstem SD–associated cortical and cardiorespiratory collapsefrom other potential causes of cortical seizure–driven bradycardia and hypoxia, we initiated localbrainstem SDs in the absence of cortical 4AP-induced seizures in juvenile mice (P20 to P30).In 50% of the trials in wild-type animals, a pulseof potassium chloride (KCl) delivered by micro-pipette generated a slow DC brainstem potentialshift (Fig. 5A). Unexpectedly, the brainstem SD in-duced brief suppression of cortical EEG amplitudein both wild-type and Kv1.1 KO animals, similar tothat seen after cortical seizures in mice and inmonitored SUDEP cases (8). The brainstem-drivenEEG suppression in the absence of cortical seizurewas nevertheless accompanied by transient brady-cardia and apnea in all Kv1.1 KO mice (Fig. 5A)and, less reliably, in wild-type mice. A corticalnegative DC potential shift was absent during thisperiod, suggesting that the depressed EEG am-plitude was not a result of intrinsic SD propaga-tion in the cortex. Sinus bradycardia was moresevere (P = 0.03; Fig.5B) and lasted longer (P =0.011; Fig. 5C) in Kv1.1 KO mice than in controlanimals (Fig. 5C) and always outlasted the brain-stem DC potential shift. On the other hand,there was no genotype difference in the dura-
tions of EEG suppression (Fig. 5D) or apnea (Fig. 5E). A short du-ration of brainstem SD was critical for recovery; prolonged SD (>10 min),triggered by KCl microinjection total in wild-type mice, produced
Fig. 2. Cardiorespiratory dysregulation and brainstem SD inWT mice associated with cortical seizures in vivo. (A to D) Rep-
resentative traces of premorbid sequence of the cortical EEG,brainstem DC current, ECG, and respiration in one WT mouse (Kv1.1+/+) with expanded tracesfrom time points a, b, and c shown in (B) to (D). In the EEG power spectrum, vertical axis showsEEG frequency band, and the color map indicates power. (B) Interictal cardiorespiratory tone. Nodeleterious cardiorespiratory rhythms were observed during the interictal period. (C) Ictal apneaand recovery. Cortical seizure triggered a very brief respiratory arrest (red arrow). (D) Breathingduring seizure. During sustained seizure, breathing rate slowed but remained regular.
cine.org 8 April 2015 Vol 7 Issue 282 282ra46 3

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
persistent bradycardia, apnea, and death,as in the cortical seizure model (Fig. 5F).Therefore, isolated brainstem SD cancause the neurophysiological and car-diorespiratory hallmarks of imminentdeath, even in the absence of a corticalseizure.
SUDEP mutations lower brainstemSD threshold in vitroWe used an in vitro brainstem slice prep-aration to test whether Kv1.1 channel de-ficiency lowered the threshold for intrinsicbrainstem SD under conditions of con-stant metabolic substrate depletion. Cor-onal brainstem slices from juvenile miceat the age of peak incidence of prematuredeath in Kv1.1 KO mice (P18 to P25) (4)were deprived of oxygen and glucose (OGD),and SD was visualized by changes in in-trinsic optical signal (IOS). Exposure toOGD solution reliably generated an IOSwave of cellular depolarization in dor-somedial nuclei (Fig. 6A and movie S1),the same area in which we had detectedSD in vivo. In this slice orientation, SDarose spontaneously and reproducibly inthe lateral NTS and spread medially toinvade vagal and hypoglossal nuclei, themicrocircuits involved in vital cardiores-piratory reflexes. Voltage-clamp recordingsrevealed a slow inward current (Fig. 6B)and suppression of excitatory transmis-sion from the visceral afferent axons (thatis, tractus solitarius) onto NTS neuronsupon arrival of the IOS peak (Fig. 6C).The propagation pattern and speed ofSD were indistinguishable between juve-nile wild-type and Kv1.1 KO slices (wild-type: 0.60 ± 0.21 mm/min, KO: 0.55 ±0.13 mm/min, n = 9 each, P > 0.5). Howev-er, SD onset was significantly earlier in
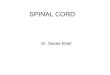
Fig. 3. Characterization of premorbid sei-zures and autonomic deregulation in Kv1.1
KO mice. (A) Time delay to the onset of le-thal cardiorespiratory failure from the end ofintense seizure (left) or the beginning ofbrainstem SD (right). (B to F) Representativetraces showing development of cortical sei-zures and terminal cardiorespiratory deregu-lation. Expanded traces are shown in (D) to(F). (B) Recurring high-amplitude seizures untilbrainstem SD and death. Regular cardiorespi-ratory tone during baseline (D) and failureduring seizure (E). (C) An intense cortical sei-zure triggering cardiorespiratory deregulation(F), leading to brainstem SD and death.www.ScienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 4

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
mutant slices (Fig. 6D), indicating a lower intrinsic SD threshold dur-ing substrate deprivation in Kv1.1 KO than in wild-type brainstem.The difference became even more obvious when the glucose concen-tration was elevated to 5 mM [50% of normal artificial cerebrospinalfluid (ACSF)]. Under this condition, SD was delayed or prevented inwild-type slices, whereas SD was still reliably generated in KO slices(Fig. 6D). A further increase in glucose concentration to 10 mM com-pletely prevented hypoxic SD in all Kv1.1 wild-type and KO tissues(Kv1.1 wild type and KO, n = 9 each).
We next examined the SD threshold for adult Kv1.1 mutants (age >90 days) that had survived the early SUDEP susceptibility period.Consistent with previous studies (23, 24), brainstem slices of olderanimals were highly resistant to hypoxia-induced SD. In adult Kv1.1KO mice, SD was detected in only 33% (3 of 9) of slices and never(0 of 9) in wild-type slices (Fig. 6D; P = 0.2, Fisher’s exact probabilitytest). Because genetic Kv1.1 deletion may alter brain development, weexamined the direct role of Kv1.1 channels on the OGD-SD thresholdin adult wild-type mice by acute pharmacologic inhibition of Kv1.1currents, which are typically generated through heteromeric Kv1.1/Kv1.2 channels. Exposure of slices to the Kv1.1/Kv1.2 specific inhib-
www.Sc
itor dendrotoxin-K (DTX-K; 50 nM) significantly decreased the laten-cy to SD onset in wild-type slices compared to that observed in Kv1.1KO slices, whereas the toxin was without additional effect in KO slices(Fig. 6E). These results indicate that loss of the Kv1.1 channel is suf-ficient to lower the brainstem SD threshold, consistent with its effectin the cerebellar cortex (25). We also found that bath application ofthe N-methyl-D-aspartate receptor antagonist MK801 (30 mM), whichinhibits SD in other models (13), also inhibited SD in Kv1.1 KO brain-stem (SD onset: control, 5.7 ± 2.8 min; MK801, 16.3 ± 2.6 min; P <0.001, n = 6 each). Together, these in vitro findings confirm that theSUDEP risk factors identified in vivo (Kv1.1 deficiency and youngerage) are intrinsic to Kv1.1 KO neuronal networks and increase thevulnerability of brainstem dorsal nuclei to hypoxic SD generation.
To determine whether Kv1.1 KO mice are unique among SUDEPmodels in exhibiting a decreased SD threshold, we examined brain-stem slices from juvenile Scn1a R1407X mice, a mouse model of DravetSyndrome (20). Pathogenic mutations in this syndrome elevate networkexcitability by impairing sodium conductance and by network dis-inhibition (16, 26, 27). We found that the threshold for brainstemSD was also significantly lowered in this mouse loss-of-function model(Fig. 6F), whereas SD propagation rate was unchanged (wild-type:0.46 ± 0.17 mm/min, heterozygote: 0.62 ± 0.21 mm/min, P > 0.1,n = 9 and 10, respectively). We also tested whether a known genetic mod-ifier of life span in SUDEP mice influenced SD threshold. Prematuredeath in both Kv1.1 KO and Scn1a Ki mutant mice is largely rescuedby ablation of the gene MapT that encodes the axonal microtubule-associated protein tau (28, 29). Consistent with its striking prolongationof survival, tau deletion normalized the latency to onset of brainstem SDin Kv1.1 KO slices (Fig. 6G). Thus, Kv1.1/tau double KO (Kv1.1−/−,tau−/−) mice showed a raised brainstem SD threshold, and onset laten-cy was delayed to that seen in control slices (Kv1.1+/+, tau−/−).
DISCUSSION
Our data point to an active intermediary role of SD in the postictalcardiorespiratory collapse that leads to sudden mortality in epilepsy.This conclusion rests on several lines of evidence in two geneticallyvalidated mouse models of human SUDEP and suggests an approachfor therapeutic intervention in this life-threatening condition.
First, we demonstrated that a deleterious positive feedback rela-tionship occurs when SD silences brainstem dorsal nuclei whosefunction is to ensure oxygenation of the nervous system; depolarizingblockade of these cells prevents normal autoresuscitation. This centralshutdown of the cardiorespiratory centers may explain the failure of ef-forts to revive epilepsy patients by cardioresuscitation after cardiacarrest. Second, we found a lowered brainstem threshold to SD in twovalidated SUDEP models generated by decreased function in the genesKcna1 and Scn1a. These genes alter excitability through distinct mem-brane and synaptic mechanisms, reinforcing the generality of our find-ings. Loss of Kv1.1 current has a powerful effect on both excitatoryand inhibitory neurons (19, 30), whereas Scna1a channel deficiencypreferentially decreases the excitability of interneurons in the forebrain(20, 26). Nevertheless, both mouse models exhibited a heightened sen-sitivity to SD. Human SCN1A mutations are also linked to familialhemiplegic migraine type 3 (FHM3) (31), and two other genes for FHMphenotypes also lower thresholds for SD, seizures, and premature deathin mouse models. A gain-of-function mutation, S218L, in CACNA1A
Fig. 4. Characterization of premorbidseizures and autonomic deregulationin the Scn1a (+/R1407X) mouse. (A) Sta-ble baseline cardiorespiratory tone. (B) De-
generative cardiorespiratory response during the onset of brainstem SD.Sudden onsets of agonal breathing, cardiac arrhythmias, and cortical EEGsuppression preceded the onset of negative DC potential shift in brainstemDC trace. Asterisk, gasping. Vertical scale: cortical EEG, 1.1 mV; brainstemDC, 7.5 mV; ECG, 0.22 mV; respiration, arbitrary units.
ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 5

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
(FHM1) encoding P/Q-type cal-cium channels lowers SD thresh-old, and 20% of FHM patientscarrying this mutation developseizures during attacks (13). Micebearing the S218L Cacna1amu-tation show low SD threshold,seizures, and premature death(32), whereas a loss-of-functionCacna1a mutation raises SDthreshold (33) and prolongs sur-vival in Kv1.1 KO mutants (34).Humans andmicewithmutationsin the Na+, K+-ATPase genesATP1A2 and ATP1A3 causehemiplegic migraine. Atp1a2 mu-tations (FHM2) lower SD thresh-old (35), and Atp1A3 mutationscause seizures and prematuredeath in mice (36) and seizuresin 33% of patients with variableautonomic and respiratory dis-turbances (37). Finally, we andothers have recently shown thatthe loss-of-function modifier geneMapT (tau) prevents seizures andprolongs longevity in Kv1.1 andScn1a mutants (28, 29).
Here, light anesthesia was re-quired for stable and noninjur-ious DC recordings in the smallmouse brainstem during sei-zures. Urethane anesthesia con-serves cardiovascular reflexes(38) and creates a physiologicalstatus similar to sleep (39), whichmay be relevant given the fre-quent occurrence of SUDEP dur-ing sleep (8). Because SD canbe readily triggered by a me-chanical pinprick, motor move-ments prevented us from recordingunprovoked brainstem DC re-sponses during spontaneous con-vulsive seizures in freely movinganimals. This technical challengemust be overcome to directlymonitor spontaneous brainstemdeath in unanesthetized animalmodels.
Our study identifies func-tional mutations in genes regulat-ing SD threshold as a significantcontributor to the risk of SU-
DEP. Like those for cardiac long QT syndrome (LQTS), the list of path-ogenic SD mutations will continue to grow and serve as candidate targetsfor individualized therapeutic strategies. Computer simulations indicatethat SD threshold, latency, and duration are under the coordinate controlwww.Sc
of membrane conductances regulated by multiple voltage- and ligand-gated channels, supporting an oligogenic model underlying cardio-respiratory instability and SUDEP (40, 41). Given the complexity ofion channel gene variation contributing to epilepsy itself (12), an
Fig. 5. Locally evoked brainstem SD triggers corticalsuppression and cardiorespiratory collapse. Localbrainstem SD initiated by KCl microinjection into the dor-sal medulla of anesthetized spontaneously breathingmouse. (A) Representative cortical and cardiorespiratoryresponses in juvenile WT mouse. Brainstem SD transientlysuppressed cortical EEG, ECG, and spontaneous respira-tion. The expanded trace shown below illustrates periodiccortical EEG suppression, bradycardia, and apnea. Gaspingwas observed during the recovery from apnea. Verticalscale: cortical EEG, 0.15 mV; brainstem DC, 4.5 mV; ECG,0.2 mV; respiration, arbitrary unit. (B to E) Quantificationof central and peripheral consequences of brainstemSD. Duration of bradycardia was longer and the peakheart rate decrease (analyzed every 1-s bin) was lowerin Kv1.1 KO mice. There was no difference in the durationof cortical EEG suppression and the duration of apnea.WT, n = 10; Kv1.1 KO, n = 4. *P < 0.05, **P < 0.01; n.s., notsignificant. We note that 63% (7 of 11) of Kv1.1 KO micedied after SD and were excluded from the analyses. (F)Microinjection of KCl triggered prolonged DC potentialshift, followed by death. Vertical scale: cortical EEG,0.25 mV; brainstem DC, 10 mV; ECG, 0.18 mV; respiration,arbitrary unit.
ienceTranslationa
lMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 6
R E S EARCH ART I C L E
www.Sc
integrated biological and in silico analysis of variant function willbe essential to refine the prognostic value of epistatic variant pro-files in evaluating personal risk for SUDEP.
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
MATERIALS AND METHODS
Study designIn vivo studies were first conducted in a set of Kv1.1 KO animals toexamine cardiorespiratory abnormalities as well as brainstem SDevents. Later experiments alternated between littermate wild-type con-trol mice to characterize contribution of the genotype. The in vivoexperiments could not be blinded to the genotype of the animal be-cause the genotype was apparent by the behavior of the mutant animalduring the surgical preparation. We did not perform an a priori poweranalysis for in vivo analyses of physiological variables. All post hocquantitative analysis of digitized data was performed identically usingobjective measurement algorithms and maintained in chronologicalorder on the laboratory computer.
Prospective quantitative comparison was conducted for the in vitroanalyses of SD onset (Fig. 3). Experiments were designed to test (i) atleast two brainstem slices from each mouse to evaluate experimentalerror and (ii) at least four mice to evaluate between-animal differencesby using nonparametric analysis (see below). Variability within or be-tween animals was similar and small in Kv1.1 KO preparations, andthus SD onset of each slice was used as individual data sample.
AnimalsAll experimental protocols were approved by Institutional AnimalCare and Use Committee of Baylor College of Medicine (BCM).Kv1.1 wild-type (+/+) and KO (−/−) were obtained from heterozygous(Kv1.1+/−/C57BL6×C3HeB/FeJ hybrid) breeding colonies establishedat BCM. Scn1a R1407X Ki mice (19) were obtained by crossingwild-type and heterozygous mice, maintained in C57BL6/SV129hybrid (75 to 88% C57BL6) background. Kv1.1/tau double KO micewere generated as described previously (27). Retrospectively, ~55 and~15% of Kv1.1 KO and Scn1a (R1407X) heterozygotes, respectively, werefound dead before P30. Our study therefore used juvenile (P16 to 25) andadult mice (P >90). Both male and female mice were used and were notrandomized. Genotypes of Kcna1 and Scn1a mutant alleles weredetermined by polymerase chain reaction methods (4, 19). Genotypecould be readily identified on the basis of their behavior and pheno-type, and thus experiments were not blinded to the experimenter. Allmice were bred at BCM and housed at 22°C with a 12-hour light cyclewith ad libitum access to food and water.
In vivo electrophysiologyMice were anesthetized with urethane (1.0 to 1.5 g/kg, intraperiton-eally) and mounted on a stereotaxic frame. Body temperature wasmaintained at 37°C with a thermistor feedback-controlled thermalblanket. Electrocardiogram (ECG) was recorded with subcutaneouselectrodes over the thorax. Respiration was measured by temperaturefluctuations detected with a thermocouple placed at the mouth afterocclusion of the nares. Cortical EEG was recorded with a silver/silverchloride ball electrode placed on the thinned skull and held with super-glue. Seizures were evoked by application of a pledget soaked with 4AP(100 mM, ~10 ml) on the cortical surface accessed through a smallcranial window. Glass electrodes (1 to 2 megohms) were inserted in
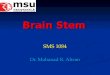
Fig. 6. SD threshold is influencedby age, ion channel deficiency, and taudeletion in brainstem slices. SD was triggered in coronal medulla slices by
OGD and monitored by IOS. (A) Raw image (a) and montage of video frames(b to e, see movie S1). TS, tractus solitarius; AP, area postrema; X, dorsal motornucleus of vagus; XII, hypoglossal nucleus. Scale bar, 500 mm(B) IOS andwhole-cell recording of NTS neurons showing compromised afferent input after SDonset. Vertical lines in the whole-cell current trace are test responses of mem-brane resistance to a train of excitatory postsynaptic currents (EPSCs) triggeredevery 20 s. Im, whole-cell current; DT/T0, relative transparency change. (C)Expanded traces of (a) and (b) from (B). (a) stimulation artifacts (red arrows)followed by EPSCs at baseline; (b) EPSC absent during SD. (D) SD onset wassignificantly faster in slices obtained from juvenile Kv1.1 KO (red). Adult slicesshowedamarked increase in SD threshold andnogenotypedifference. (E) TheKv1.1 channel inhibitor DTX-K (50 nM) reduced latency to SD onset in WT(black) but not in Kv1.1 KO slices (red). (F) Scn1a-deficient mice also showedlowered SD threshold (red). (G) Compound Kv1.1/tau deletion (red) abolishedlow SD threshold in Kv1.1 KO slices. The numbers indicate numbers of sliceswith SD out of total slices tested. *P < 0.05, **P < 0.01. n.s., not significant.ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 7

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
the dorsal brainstem (~500-mm caudal from obex, ~500-mm depth)through an opening in the occipital bone using a micromanipulator vi-sually guided by a surgical microscope. Themeninges overlying the brain-stem are thin and easily penetrated by the glass electrode. After 1 hour ofpostsurgical recovery, oxygen saturation (SpO2) and blood glucose levelswere tested using MouseOX (Starr Life Sciences) and FreeStyle glucoseoxidase strips (Abbott), respectively. Recordings were made for 2 hoursafter 4AP application. Brainstem SD was evoked by KCl microinjectionwith Picosplitzer II (Parker) in the superficial layer (~500 mm from thesurface, pipette tip diameter ~10 mm, 1 M KCl, 10 to 100 ms, 30 psi,~10 nl volume) in the caudal region of the fourth ventricular floorcontaining the NTS (<0.5 mm from the obex) while monitoring withthe glass micropipette electrode placed superficially (<1 mm below thesurface and >1 mm distant from the injection site). Prolonged SD wastriggered by a repetitive train of pressure pulses (0.1 to 0.2 Hz, total ~1 sduration). Microinjection >1.5 mm rostral to the NTS or ventral to thehypoglossal nucleus (>2 mm below the surface) did not evoke SD (n = 3each). Deathwas not associated with the presence (9 of 18) or absence(5 of 7) of the brainstem recording electrode (P = 0.7, Fisher’s exacttest). The anesthetizedmouse typically had a heart rate of ~ 600 beatsper minute and a respiration rate of ~80 breaths per minute before therecordings. Mice with abnormal heart rate and respiratory rate, SpO2
less than 95%, or blood glucose <100 mg/dl were euthanized. Corticaland brainstem electrical activities were amplified with Axoclamp-2A (Molecular Devices), and ECG and respiration signals were ampli-fied with a Model 410 amplifier (Brownlee Precision). All electricaldata were digitized with Digidata 1334 and analyzed with pClamp9.2software. Here, SD was defined as a negative electrical potential shift>−4 mV/min in the DC recording.
After recording, brains were extracted and kept in 4% para-formaldehyde at 4°C for >48 hours and were transferred in 30% su-crose. Brains were frozen and cut into 100-mm sections in a cryostat.Sections were directly mounted on glass slides, and the electrode po-sition was confirmed on the basis of a slit created by electrode insertion.
Slice electrophysiologyCoronal slices (300-mm thickness) were prepared from forebrainscontaining dorsal hippocampus and brainstem covering the NTS. Slicesobtained from±500mmfrom the obex showed similar SDonsets, and thusthe slices within this anatomical range were used for the analyses. Briefly,mice were deeply anesthetized with Avertin (250 mg/kg, intra-peritoneally) and decapitated. Brains were extracted in cold dissectionsolution (220mM sucrose, 10mM glucose, 6 mMmagnesium sulfate, 3mM KCl, 25 mM sodium bicarbonate, 1.25 mM sodium monopho-sphate, 2 mM calcium chloride, and 0.4 mM ascorbic acid equilibratedwith 95%O2/5% CO2), trimmed, and glued on the cutting stage. Brainslices were prepared on a vibratome and incubated inACSF (126mMsodium chloride, 10mMglucose, 1mMmagnesium sulfate, 3mMKCl,25 mM sodium bicarbonate, 1.25 mM sodiummonophosphate, 2 mMcalcium chloride, and 0.4 mM ascorbic acid equilibrated with 95% O2/5% CO2) at 35°C for 1 hour. After recovery, the slices were kept inACSF at room temperature until used for experiments.
For electrophysiological recording, the slices were transferred to asubmerged chamber (RC27, Warner Instruments) and were super-fused with oxygenated ACSF at 2 ml/min. Slices were visualized withan upright microscope (Axioskop, Zeiss; BX51, Olympus) with a charge-coupled device (CCD) camera (C2400, Hamamatsu). Whole-cell re-cordings were obtained from visually identified NTS neurons in the
www.Sc
translucent region of the dorsalmedulla. Patch pipetteswere filledwithintracellular solution [130 mM cesium gluconate, 1 mM magnesiumchloride, 5 mM sodium chloride, 10 mM 1,2-bis(2-aminophenoxy)ethane-N,N,N′,N′-tetraacetic acid (BAPTA), 10mMHepes, 5mM lid-ocaineN-ethyl chloride (QX314), 2mMadenosine triphosphate (ATP),0.3 mM guanosine triphosphate, and pH adjusted to 7.2 with cesiumhydroxide]. Signals were amplified (Multiclamp 200B), digitized byDigidata 1322A, and analyzed with pClamp9.2 software (MolecularDevices). Pairs of EPSCs were evoked by a bipolar electrode placedon the adjacent tractus solitarius controlled by an IsoFlex andMaster8 (100 ms, ~0.2 mA, 100-ms interval). Recorded Kv1.1 wild-type andKONTS neurons had similar input resistances (Kv1.1 wild type: 1.84 ±1.2 gigohms, n = 8, and KO: 1.99 ± 0.65 gigohms, n = 7) and capac-itances (Kv1.1 wild type: 10.5 ± 3.1 pF, n = 8, and KO: 10.6 ± 4.1 pF,n = 7). Series resistances were between 15 and 20 megohms, with com-pensation of 50 to 70%. SD was generated by OGD.We used the 5mMglucose level for comparative analyses, except where stated. Recordingswere made for 20 min after OGD exposure. SD was detected by a bandof increased light transmission (that is, IOS) traveling across the braintissue using the CCD camera. A sequence of images was acquired at1 Hz and was analyzed by ImageJ software.
At least four mice were used for each comparison to evaluate var-iances from animals. All experiments were interleaved between slicesobtained from the test genotype or treated with drugs.
ReagentsThe Kv1.1/Kv1.2 inhibitor DTX-K was purchased from AlomoneLabs. All other chemicals were obtained from Sigma-Aldrich.
StatisticsAll data are presented as means ± SD in text and/or box-and-whiskergraph with minimum to maximum data range bars. Data were com-pared by nonparametric Mann-Whitney U test, unless otherwise men-tioned. P < 0.05 was considered significant. In experiments of SDonsets, experiments with latency to SD onset >20 min were consideredas “SD blocked” and were treated as the highest rank value in the ranktest. Sample size was determined on the basis of pilot experiments.Statistical power was not calculated.
SUPPLEMENTARY MATERIALS
www.sciencetranslationalmedicine.org/cgi/content/full/7/282/282ra46/DC1Fig. S1. Peri-ictal autonomic abnormality in Kv1.1 KO mouse #1.Fig. S2. Peri-ictal autonomic abnormality in Kv1.1 KO mouse #2.Table S1. Raw dataMovie S1. OGD-SD in brainstem slice
REFERENCES AND NOTES
1. C. A. Massey, L. P. Sowers, B. J. Dlouhy, G. B. Richerson, Mechanisms of sudden unexpecteddeath in epilepsy: The pathway to prevention. Nat. Rev. Neurol. 10, 271–282 (2014).
2. D. J. Thurman, D. C. Hesdorffer, J. A. French, Sudden unexpected death in epilepsy: Assessingthe public health burden. Epilepsia 55, 1479–1485 2014).
3. A. M. Goldman, E. Glasscock, J. Yoo, T. T. Chen, T. L. Klassen, J. L. Noebels, Arrhythmia inheart and brain: KCNQ1 mutations link epilepsy and sudden unexplained death. Sci. Transl.Med. 1, 2ra6 (2009).
4. E. Glasscock, J. W. Yoo, T. T. Chen, T. L. Klassen, J. L. Noebels, Kv1.1 potassium channeldeficiency reveals brain-driven cardiac dysfunction as a candidate mechanism for suddenunexplained death in epilepsy. J. Neurosci. 30, 5167–5175 (2010).
ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 8

R E S EARCH ART I C L E
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from
5. F. Kalume R. E. Westenbroek, C. S. Cheah, F. H. Yu, J. C. Oakley, T. Scheuer, W. A. Catterall, Suddenunexpected death in amousemodel of Dravet syndrome. J. Clin. Invest. 123, 1798–1808 (2013).
6. A. J. Cole, E. Eskandar, T. Mela, J. L. Noebels, R. G. Gonzales, D. McGuone, Case records ofthe Massachusetts General Hospital. Case 18-2013―A 32-year-old woman with recurrentepisodes of altered consciousness. N. Engl. J. Med. 368, 2304–2312 (2013).
7. E. C. Stecker, K. Reinier, A. Uy-Evanado, C. Teodorescu, H. Chugh, K. Gunson, J. Jui, S. S. Chugh,Relationship between seizure episode and sudden cardiac arrest in patients with epilepsy: Acommunity-based study. Circ. Arrhythm. Electrophysiol. 6, 912–916 (2013).
8. P. Ryvlin, L. Nashef, S. D. Lhatoo, L. M. Bateman, J. Bird, A. Bleasel, P. Boon, A. Crespel, B. A. Dworetzky,H. Høgenhaven, H. Lerche, L. Maillard, M. P. Malter, C. Marchal, J. M. Murthy, M. Nitsche, E. Pataraia,T. Rabben, S. Rheims, B. Sadzot, A. Schulze-Bonhage, M. Seyal, E. L. So, M. Spitz, A. Szucs, M. Tan,J. X. Tao, T. Tomson, Incidence and mechanisms of cardiorespiratory arrests in epilepsymonitoring units (MORTEMUS): A retrospective study. Lancet Neurol. 12, 966–977 (2013).
9. S. Shorvon, T. Tomson, Sudden unexpected death in epilepsy. Lancet 378, 2028–2038 (2011).10. J. Jeppesen, A. Fuglsang-Frederiksen, R. Brugada, B. Pedersen, G. Rubboli, P. Johansen, S. Beniczky,
Heart rate variability analysis indicates preictal parasympathetic overdrive preceding seizure-induced cardiac dysrhythmias leading to sudden unexpected death in a patient with epilepsy.Epilepsia 55, e67–e71 (2014).
11. L. P. Sowers, C. A. Massey, B. K. Gehlbach, M. A. Granner, G. B. Richerson, Sudden unexpecteddeath in epilepsy: Fatal post-ictal respiratory and arousal mechanisms. Respir. Physiol. Neurobiol.189, 315–323 (2013).
12. T. Klassen, C. Davis, A. Goldman, D. Burgess, T. Chen, D. Wheeler, J. McPherson, T. Bourguin,L. Lewis, D. Villasana, M. Morgan, D. Muzny, R. Gibbs, J. Noebels, Exome sequencing of ionchannel genes reveals complex profiles confounding personal risk assessment in epilepsy.Cell 145, 1036–1048 (2011).
13. D. Pietrobon, M. A. Moskowitz, Chaos and commotion in the wake of cortical spreadingdepression and spreading depolarizations. Nat. Rev. Neurosci. 15, 379–393 (2014).
14. M. Lauritzen, J. P. Dreier, M. Fabricius, J. A. Hartings, R. Graf, A. J. Strong, Clinical relevanceof cortical spreading depression in neurological disorders: Migraine, malignant stroke, sub-arachnoid and intracranial hemorrhage, and traumatic brain injury. J. Cereb. Blood FlowMetab. 31, 17–35 (2011).
15. F. Richter, R. Bauer, A. Lehmenkühler, H. G. Schaible, The relationship between suddensevere hypoxia and ischemia-associated spreading depolarization in adult rat brainstemin vivo. Exp. Neurol. 224, 146–154 (2010).
16. M. A. Rogawski, in Jasper’s Basic Mechanisms of the Epilepsies, J. L. Noebels, M. Avoli,M. A. Rogawski, R. W. Olsen, A. V. Delgado-Escueta, Eds. (U.S. National Center for Bio-technology Information, Bethesda, MD, 2012).
17. I. Mody, J. D. Lambert, U. Heinemann, Low extracellular magnesium induces epileptiform ac-tivity and spreading depression in rat hippocampal slices. J. Neurophysiol. 57, 869–888 (1987).
18. J. J. Hablitz, U. Heinemann, Alterations in the microenvironment during spreading depressionassociated with epileptiform activity in the immature neocortex. Brain Res. Dev. Brain Res. 46,243–252 (1989).
19. S. L. Smart, V. Lopantsev, C. L. Zhang, C. A. Robbins, H. Wang, S. Y. Chiu, P. A. Schwartzkroin,A. Messing, B. L. Tempel, Deletion of the KV1.1 potassium channel causes epilepsy in mice.Neuron 20, 809–819 (1998).
20. I. Ogiwara, H. Miyamoto, N. Morita, N. Atapour, E. Mazaki, I. Inoue, T. Takeuchi, S. Itohara, Y. Yanagawa,K. Obata, T. Furuichi, T. K. Hensch, K. Yamakawa, Nav1.1 localizes to axons of parvalbumin-positiveinhibitory interneurons: A circuit basis for epileptic seizures in mice carrying an Scn1a genemutation. J. Neurosci. 27, 5903–5914 (2007).
21. S. H. Kim, D. R. Nordli Jr., A. T. Berg, S. Koh, L. Laux, Ictal ontogeny in Dravet syndrome. Clin.Neurophysiol. 126, 446–455 (2014).
22. L. M. Bateman, C. S. Li, T. C. Lin, M. Seyal, Serotonin reuptake inhibitors are associated withreduced severity of ictal hypoxemia in medically refractory partial epilepsy. Epilepsia 51,2211–2214 (2010).
23. F. Funke, M. Kron, M. Dutschmann, M. Müller, Infant brain stem is prone to the generationof spreading depression during severe hypoxia. J. Neurophysiol. 101, 2395–2410 (2009).
24. F. Richter, S. Rupprecht, A. Lehmenkühler, H. G. Schaible, Spreading depression can beelicited in brain stem of immature but not adult rats. J. Neurophysiol. 90, 2163–2170 (2003).
25. G. Chen, W. Gao, K. C. Reinert, L. S. Popa, C. M. Hendrix, M. E. Ross, T. J. Ebner, Involvementof kv1 potassium channels in spreading acidification and depression in the cerebellar cortex. J.Neurophysiol. 94, 1287–1298 (2005).
26. F. H. Yu, M. Mantegazza, R. E. Westenbroek, C. A. Robbins, F. Kalume, K. A. Burton, W. J. Spain,G. S. McKnight, T. Scheuer, W. A. Catterall, Reduced sodium current in GABAergic interneuronsin a mouse model of severe myoclonic epilepsy in infancy. Nat. Neurosci. 9, 1142–1149 (2006).
www.Sc
27. I. Ogiwara, T. Iwasato, H. Miyamoto, R. Iwata, T. Yamagata, E. Mazaki, Y. Yanagawa, N. Tamamaki,T. K. Hensch, S. Itohara, K. Yamakawa, Nav1.1 haploinsufficiency in excitatory neurons amelio-rates seizure-associated sudden death in a mouse model of Dravet syndrome. Hum. Mol. Genet.22, 4784–4804 (2013).
28. J. K. Holth, V. C. Bomben, J. G. Reed, T. Inoue, L. Younkin, S. G. Younkin, R. G. Pautler, J. Botas,J. L. Noebels, Tau loss attenuates neuronal network hyperexcitability in mouse and Drosophilagenetic models of epilepsy. J. Neurosci. 33, 1651–1659 (2013).
29. A. L. Gheyara, R. Ponnusamy, B. Djukic, R. J. Craft, K. Ho, W. Guo, M. M. Finucane, P. E. Sanchez,L. Mucke, Tau reduction prevents disease in a mouse model of Dravet syndrome. Ann. Neurol.76, 443–456 (2014).
30. E. M. Goldberg, B. D. Clark, E. Zagha, M. Nahmani, A. Erisir, B. Rudy, K+ channels at the axoninitial segment dampen near-threshold excitability of neocortical fast-spiking GABAergicinterneurons. Neuron 58, 387–400 (2008).
31. S. Cestèle, A. Labate, R. Rusconi, P. Tarantino, L. Mumoli, S. Franceschetti, G. Annesi, M. Mantegazza,A. Gambardella, Divergent effects of the T1174S SCN1Amutation associated with seizures andhemiplegic migraine. Epilepsia 54, 927–935 (2013).
32. A. M. van den Maagdenberg, T. Pizzorusso, S. Kaja, N. Terpolilli, M. Shapovalova, F. E. Hoebeek,C. F. Barrett, L. Gherardini, R. C. van de Ven, B. Todorov, L. A. Broos, A. Tottene, Z. Gao,M. Fodor, C. I. De Zeeuw, R. R. Frants, N. Plesnila, J. J. Plomp, D. Pietrobon, M. D. Ferrari,High cortical spreading depression susceptibility and migraine-associated symptomsin Cav2.1 S218L mice. Ann. Neurol. 67, 85–98 (2010).
33. C. Ayata, M. Shimizu-Sasamata, E. H. Lo, J. L. Noebels, M. A. Moskowitz, Impaired neuro-transmitter release and elevated threshold for cortical spreading depression in mice withmutations in the a1A subunit of P/Q type calcium channels. Neuroscience 95, 639–645(2000).
34. E. Glasscock, J. Qian, J. W. Yoo, J. L. Noebels, Masking epilepsy by combining two epilepsygenes. Nat. Neurosci. 10, 1554–1558 (2007).
35. L. Leo, L. Gherardini, V. Barone, M. De Fusco, D. Pietrobon, T. Pizzorusso, G. Casari,Increased susceptibility to cortical spreading depression in the mouse model of familialhemiplegic migraine type 2. PLOS Genet. 7, e1002129 (2011).
36. S. J. Clapcote, S. Duffy, G. Xie, G. Kirshenbaum, A. R. Bechard, V. R. Schack, J. Petersen, L. Sinai,B. J. Saab, J. P. Lerch, B. A. Minassian, C. A. Ackerley, J. G. Sled, M. A. Cortez, J. T. Henderson,B. Vilsen, J. C. Roder, Mutation I810N in the a3 isoform of Na+,K+-ATPase causes impair-ments in the sodium pump and hyperexcitability in the CNS. Proc. Natl. Acad. Sci. U.S.A.106, 14085–14090 (2009).
37. H. Rosewich, H. Thiele, A. Ohlenbusch, U. Maschke, J. Altmüller, P. Frommolt, B. Zirn, F. Ebinger,H. Siemes, P. Nürnberg, K. Brockmann, J. Gärtner, Heterozygous de-novo mutations in ATP1A3in patients with alternating hemiplegia of childhood: A whole-exome sequencing gene-identification study. Lancet Neurol. 11, 764–773 (2012).
38. S. Kasparov, J. F. Paton, Changes in baroreceptor vagal reflex performance in the devel-oping rat. Pflugers Arch. 434, 438–444 (1997).
39. S. Pagliardini, S. Gosgnach, C. T. Dickson, Spontaneous sleep-like brain state alternationsand breathing characteristics in urethane anesthetized mice. PLOS One 8, e70411 (2013).
40. H. Kager, W. J. Wadman, G. G. Somjen, Conditions for the triggering of spreading depres-sion studied with computer simulations. J. Neurophysiol. 88, 2700–2712 (2002).
41. Y. Wei, G. Ullah, S. J. Schiff, Unification of neuronal spikes, seizures, and spreading depres-sion. J. Neurosci. 34, 11733–11743 (2014).
Acknowledgments: We thank K. Yamakawa and J. Ziburkas for sharing SCN1A R1407X Kimice, and E. Roberson for the gift of tau KO mice. Funding: This work was supported by aPostdoctoral Fellowship award (14POST20130031) from the American Heart Association (I.A.),NINDS NS029709 and NS090340 (J.L.N.), and the Blue Bird Circle Foundation. Author contri-butions: I.A. and J.L.N. conceived and designed the experiments and wrote the manuscript. I.A.conducted the experiments and analyzed the data. Competing interests: The authors declarethat they have no competing interests. Data and materials availability: All raw data areavailable online in table S1.
Submitted 2 December 2014Accepted 16 February 2015Published 8 April 201510.1126/scitranslmed.aaa4050
Citation: I. Aiba, J. L. Noebels, Spreading depolarization in the brainstem mediates suddencardiorespiratory arrest in mouse SUDEP models. Sci. Transl. Med. 7, 282ra46 (2015).
ienceTranslationalMedicine.org 8 April 2015 Vol 7 Issue 282 282ra46 9

mouse SUDEP modelsSpreading depolarization in the brainstem mediates sudden cardiorespiratory arrest in
Isamu Aiba and Jeffrey L. Noebels
DOI: 10.1126/scitranslmed.aaa4050, 282ra46282ra46.7Sci Transl Med
seizure-induced death. Ultimately, genetic analysis could predict which patients are at the highest risk of SUDEP.the mutated ion channels and suggest that similar channel variations in humans may increase the risk ofmodifier gene prevented the mortality. The authors attribute the susceptibility to so-called spreading depression to in the brainstem, which shuts down the cardiorespiratory control centers, causing sudden death. Mutation in aSUDEP. After a seizure, epileptic mice with mutations in certain ion channels can show a massive depolarization
underliegenetically controlled sensitivity to inactivation of the heart and respiratory control centers of the brain may thatincreased risk of sudden death: SUDEP (sudden unexplained death in epilepsy). Aiba and Noebels now report
also face an−−even worse−−Patients with uncontrolled epilepsy can have a seizure at any time andSubduing SUDEP (sudden unexplained death in epilepsy)
ARTICLE TOOLS http://stm.sciencemag.org/content/7/282/282ra46
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2015/04/06/7.282.282ra46.DC1
CONTENTRELATED
http://stm.sciencemag.org/content/scitransmed/12/558/eaaz6100.fullhttp://stm.sciencemag.org/content/scitransmed/12/538/eaay4682.fullhttp://science.sciencemag.org/content/sci/353/6300/664.fullhttp://science.sciencemag.org/content/sci/359/6377/787.fullhttp://science.sciencemag.org/content/sci/359/6377/740.fullhttp://science.sciencemag.org/content/sci/359/6374/377.fullhttp://science.sciencemag.org/content/sci/353/6300/646.full
REFERENCES
http://stm.sciencemag.org/content/7/282/282ra46#BIBLThis article cites 40 articles, 7 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
Copyright © 2015, American Association for the Advancement of Science
by guest on Novem
ber 29, 2020http://stm
.sciencemag.org/
Dow
nloaded from