Embed Size (px)
Citation preview

InterventIon
Epilepsy in people with learning disabilitiesJodie Wilcox
Mike Kerr
Abstractthe diagnosis and management of epilepsy in the population of people
with learning disabilities can be complex and challenging. epilepsy is
the most common medical condition seen in people with learning dis-
abilities, and both the disorder and its treatment can have significant
impact upon an individual’s physical health and psychological wellbeing.
Assessment may be complicated by other common comorbidities, such
as communication difficulties, mental illness and challenging behaviour,
as well as issues raised by the individual’s capacity to consent to treat-
ment. the disorder itself may also be potentially more complex to treat,
with many individuals experiencing more than one seizure type and a
greater chance of treatment resistance compared with the general popu-
lation. these complicating factors and far-reaching consequences make
an accurate diagnosis and individualized management plan all the more
important in this population. this contribution addresses these issues,
focusing on individualized assessment and treatment and highlighting
the assessment of behaviour disturbance in conjunction with epilepsy
and its treatment.
Keywords antiepileptic drugs; assessment; behaviour; epilepsy;
learning disability; treatment
The diagnosis and management of epilepsy in the population of people with learning disabilities can be complex and challenging. Epilepsy is the most common medical condition seen in people with learning disabilities, and both the disorder and its treatment can have significant impact upon an individual’s physical health and psychological wellbeing. Assessment may be complicated by other common comorbidities, such as communication difficul-ties, mental illness and challenging behaviour, as well as issues raised by the individual’s capacity to consent to treatment. The disorder itself may also be potentially more complex to treat, with many individuals experiencing more than one seizure type and a greater chance of treatment resistance compared with the general population. These complicating factors and far-reaching
Jodie Wilcox MBBch MRCPsych is a Specialist Registrar in Learning
Disability Psychiatry. She is currently working for Bro Morgannwg
NHS Trust, South Wales, UK.
Mike Kerr MRCGP MRCPsych is Professor of Learning Disability Psychiatry
at the Welsh Centre for Learning Disabilities, Cardiff University, UK.
He qualified from Bristol University and trained as both a general
practitioner and a psychiatrist. His research interests are in epilepsy
and healthcare delivery to people with learning disabilities.
PSYCHIAtrY 5:10 372
consequences make an accurate diagnosis and individualized management plan all the more important in this population.
Epidemiology
The prevalence of epilepsy in the general population is estimated to be somewhere between 0.5% and 1%. Studies looking at rates of epilepsy in people with learning disabilities vary according to the population from which they are drawn. The prevalence amongst those with mild intellectual disability may be 6% whilst the prevalence may be as high as 40% for those resident in insti-tutional care. There is a strong association between severity of learning disability and presence of epilepsy, but community sur-veys estimate the overall figure to include approximately one-fifth of the learning disabled population, with a relatively higher prevalence in the younger age groups.
Aetiology
The aetiology of epilepsy in the general population is often multi-factorial, and in a large percentage the cause remains unknown. In people with learning disabilities it is likely that the underlying pathological cause for the learning disability may also have given rise to the seizure disorder.
In certain disorders the seizure characteristics and prognosis have been well defined. Identification of the cause of the learning disability may therefore have important implications for man-agement of the epilepsy. For example, a bimodal distribution of seizure onset is described in Down syndrome, with a peak occur-ring in childhood and again in middle age. The latter is associ-ated with the onset of Alzheimer’s disease.
In tuberous sclerosis, where approximately 80% of children experience seizures and 60% have learning disabilities, the most common presentation is of infantile spasms. Some may go on to develop Lennox–Gestaut syndrome, and in general the prognosis in terms of seizure control is poor (Table 1).
Other features of a person’s genetic disorder may complicate the picture of epilepsy; for example, in Rett syndrome both sei-zures and autonomic hyperventilation episodes are common and difficult to distinguish.
Seizure type
Studies attempting to determine the relative frequency of the different seizure types in both the general and learning-disabled population have encountered methodological problems. It is esti-mated that approximately two-thirds of epilepsies in the general population are partial and the remaining one-third generalized. However, it is acknowledged that these surveys are conducted on populations of patients with comparatively severe epilepsy, and focal seizures may be inherently more difficult to control. In addition, less frequent seizures are more likely to be classified inaccurately as there is less opportunity for a clinical description or characteristic recordings from EEG.
Estimates of frequency of seizure type in the learning disabled may be flawed for different reasons. In a study of epilepsy in learning-disabled children,1 only 10% of those with severe hand-icap underwent electrophysiological testing, hence the findings of a greater proportion of generalized seizures than those with
© 2006 elsevier Ltd. All rights reserved.
InterventIon
partial onset may have to be interpreted with caution. However, these results have been repeated elsewhere, and in one study of an institutionalized population, one-third of patients with assumed generalized epilepsy had EEG changes characteristic of idiopathic epilepsy.2
Seizure syndrome
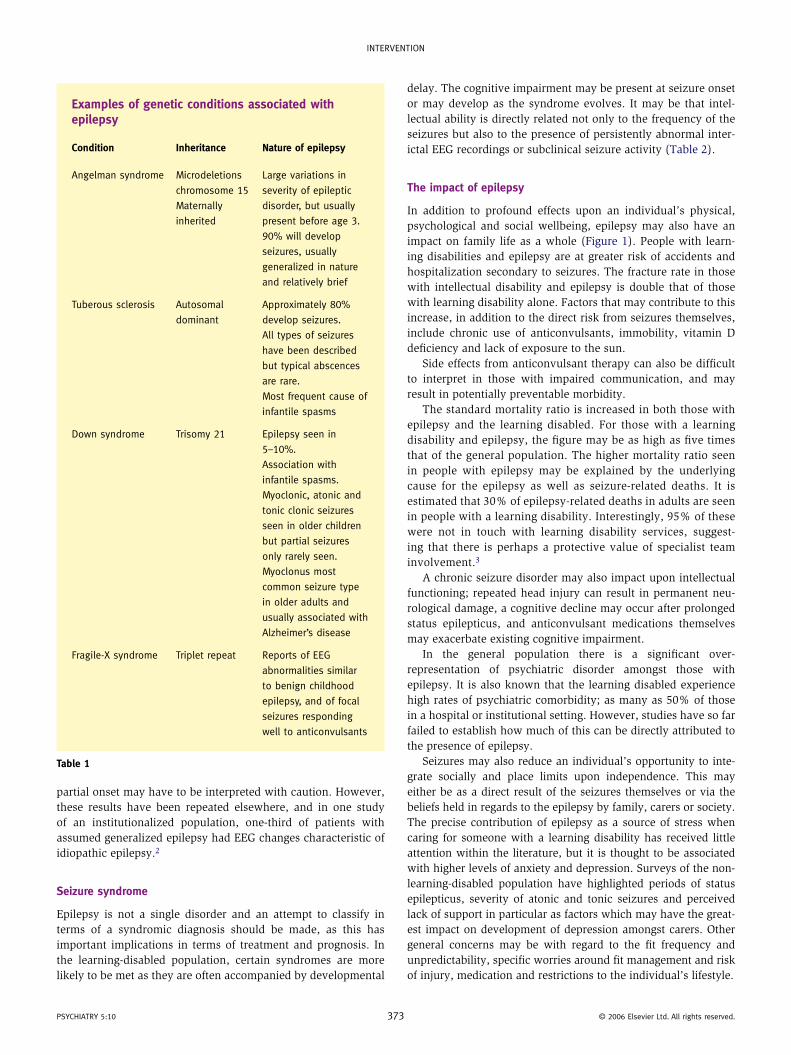
Epilepsy is not a single disorder and an attempt to classify in terms of a syndromic diagnosis should be made, as this has important implications in terms of treatment and prognosis. In the learning-disabled population, certain syndromes are more likely to be met as they are often accompanied by developmental
Examples of genetic conditions associated with epilepsy
Condition Inheritance Nature of epilepsy
Angelman syndrome Microdeletions
chromosome 15
Maternally
inherited
Large variations in
severity of epileptic
disorder, but usually
present before age 3.
90% will develop
seizures, usually
generalized in nature
and relatively brief
tuberous sclerosis Autosomal
dominant
Approximately 80%
develop seizures.
All types of seizures
have been described
but typical abscences
are rare.
Most frequent cause of
infantile spasms
Down syndrome trisomy 21 epilepsy seen in
5–10%.
Association with
infantile spasms.
Myoclonic, atonic and
tonic clonic seizures
seen in older children
but partial seizures
only rarely seen.
Myoclonus most
common seizure type
in older adults and
usually associated with
Alzheimer’s disease
Fragile-X syndrome triplet repeat reports of eeG
abnormalities similar
to benign childhood
epilepsy, and of focal
seizures responding
well to anticonvulsants
Table 1
PSYCHIAtrY 5:10 37
delay. The cognitive impairment may be present at seizure onset or may develop as the syndrome evolves. It may be that intel-lectual ability is directly related not only to the frequency of the seizures but also to the presence of persistently abnormal inter-ictal EEG recordings or subclinical seizure activity (Table 2).
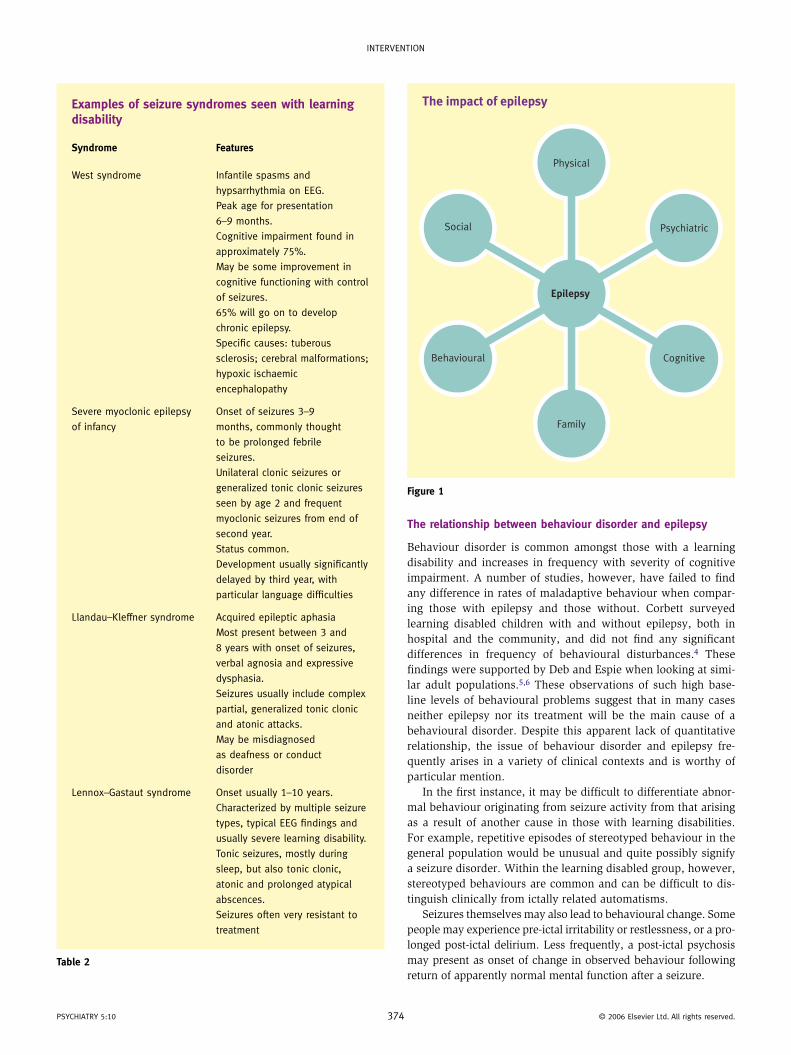
The impact of epilepsy
In addition to profound effects upon an individual’s physical, psychological and social wellbeing, epilepsy may also have an impact on family life as a whole (Figure 1). People with learn-ing disabilities and epilepsy are at greater risk of accidents and hospitalization secondary to seizures. The fracture rate in those with intellectual disability and epilepsy is double that of those with learning disability alone. Factors that may contribute to this increase, in addition to the direct risk from seizures themselves, include chronic use of anticonvulsants, immobility, vitamin D deficiency and lack of exposure to the sun.
Side effects from anticonvulsant therapy can also be difficult to interpret in those with impaired communication, and may result in potentially preventable morbidity.
The standard mortality ratio is increased in both those with epilepsy and the learning disabled. For those with a learning disability and epilepsy, the figure may be as high as five times that of the general population. The higher mortality ratio seen in people with epilepsy may be explained by the underlying cause for the epilepsy as well as seizure-related deaths. It is estimated that 30% of epilepsy-related deaths in adults are seen in people with a learning disability. Interestingly, 95% of these were not in touch with learning disability services, suggest-ing that there is perhaps a protective value of specialist team involvement.3
A chronic seizure disorder may also impact upon intellectual functioning; repeated head injury can result in permanent neu-rological damage, a cognitive decline may occur after prolonged status epilepticus, and anticonvulsant medications themselves may exacerbate existing cognitive impairment.
In the general population there is a significant over- representation of psychiatric disorder amongst those with epilepsy. It is also known that the learning disabled experience high rates of psychiatric comorbidity; as many as 50% of those in a hospital or institutional setting. However, studies have so far failed to establish how much of this can be directly attributed to the presence of epilepsy.
Seizures may also reduce an individual’s opportunity to inte-grate socially and place limits upon independence. This may either be as a direct result of the seizures themselves or via the beliefs held in regards to the epilepsy by family, carers or society. The precise contribution of epilepsy as a source of stress when caring for someone with a learning disability has received little attention within the literature, but it is thought to be associated with higher levels of anxiety and depression. Surveys of the non-learning-disabled population have highlighted periods of status epilepticus, severity of atonic and tonic seizures and perceived lack of support in particular as factors which may have the great-est impact on development of depression amongst carers. Other general concerns may be with regard to the fit frequency and unpredictability, specific worries around fit management and risk of injury, medication and restrictions to the individual’s lifestyle.
3 © 2006 elsevier Ltd. All rights reserved.
InterventIon
Examples of seizure syndromes seen with learning disability
Syndrome Features
West syndrome Infantile spasms and
hypsarrhythmia on eeG.
Peak age for presentation
6–9 months.
Cognitive impairment found in
approximately 75%.
May be some improvement in
cognitive functioning with control
of seizures.
65% will go on to develop
chronic epilepsy.
Specific causes: tuberous
sclerosis; cerebral malformations;
hypoxic ischaemic
encephalopathy
Severe myoclonic epilepsy
of infancy
onset of seizures 3–9
months, commonly thought
to be prolonged febrile
seizures.
Unilateral clonic seizures or
generalized tonic clonic seizures
seen by age 2 and frequent
myoclonic seizures from end of
second year.
Status common.
Development usually significantly
delayed by third year, with
particular language difficulties
Llandau–Kleffner syndrome Acquired epileptic aphasia
Most present between 3 and
8 years with onset of seizures,
verbal agnosia and expressive
dysphasia.
Seizures usually include complex
partial, generalized tonic clonic
and atonic attacks.
May be misdiagnosed
as deafness or conduct
disorder
Lennox–Gastaut syndrome onset usually 1–10 years.
Characterized by multiple seizure
types, typical eeG findings and
usually severe learning disability.
tonic seizures, mostly during
sleep, but also tonic clonic,
atonic and prolonged atypical
abscences.
Seizures often very resistant to
treatment
Table 2
PSYCHIAtrY 5:10 374
The relationship between behaviour disorder and epilepsy
Behaviour disorder is common amongst those with a learning disability and increases in frequency with severity of cognitive impairment. A number of studies, however, have failed to find any difference in rates of maladaptive behaviour when compar-ing those with epilepsy and those without. Corbett surveyed learning disabled children with and without epilepsy, both in hospital and the community, and did not find any significant differences in frequency of behavioural disturbances.4 These findings were supported by Deb and Espie when looking at simi-lar adult populations.5,6 These observations of such high base-line levels of behavioural problems suggest that in many cases neither epilepsy nor its treatment will be the main cause of a behavioural disorder. Despite this apparent lack of quantitative relationship, the issue of behaviour disorder and epilepsy fre-quently arises in a variety of clinical contexts and is worthy of particular mention.
In the first instance, it may be difficult to differentiate abnor-mal behaviour originating from seizure activity from that arising as a result of another cause in those with learning disabilities. For example, repetitive episodes of stereotyped behaviour in the general population would be unusual and quite possibly signify a seizure disorder. Within the learning disabled group, however, stereotyped behaviours are common and can be difficult to dis-tinguish clinically from ictally related automatisms.
Seizures themselves may also lead to behavioural change. Some people may experience pre-ictal irritability or restlessness, or a pro-longed post-ictal delirium. Less frequently, a post-ictal psychosis may present as onset of change in observed behaviour following return of apparently normal mental function after a seizure.
The impact of epilepsy
Epilepsy
Family
Physical
Psychiatric
CognitiveBehavioural
Social
Figure 1
© 2006 elsevier Ltd. All rights reserved.
InterventIon
The concept of forced normalization was first described by Landolt in 1958.7 He observed that when seizures were sup-pressed by anticonvulsants, certain individuals were noted to become psychotic and during this period their EEG normalized. With the return of seizures the EEG became abnormal and the psychosis resolved. The occurrence of this phenomenon may have to be considered a possibility given the presentation of inter-ictal behavioural change.
Another possible explanation for behavioural change is the ‘waking up’ of a patient following treatment, having previously experienced very frequent seizures or even non-convulsive status.
Finally, an issue that is frequently raised in clinical practice is the possibility of anticonvulsant medication causing or worsen-ing a pre-existing behaviour disorder. Here, as for all the other possible contributing factors, a structured approach is necessary to attempt to establish the exact relationship between behaviour, medication and seizures. Documentation of baseline behaviours prior to initiating a new drug may prove valuable at a later date.
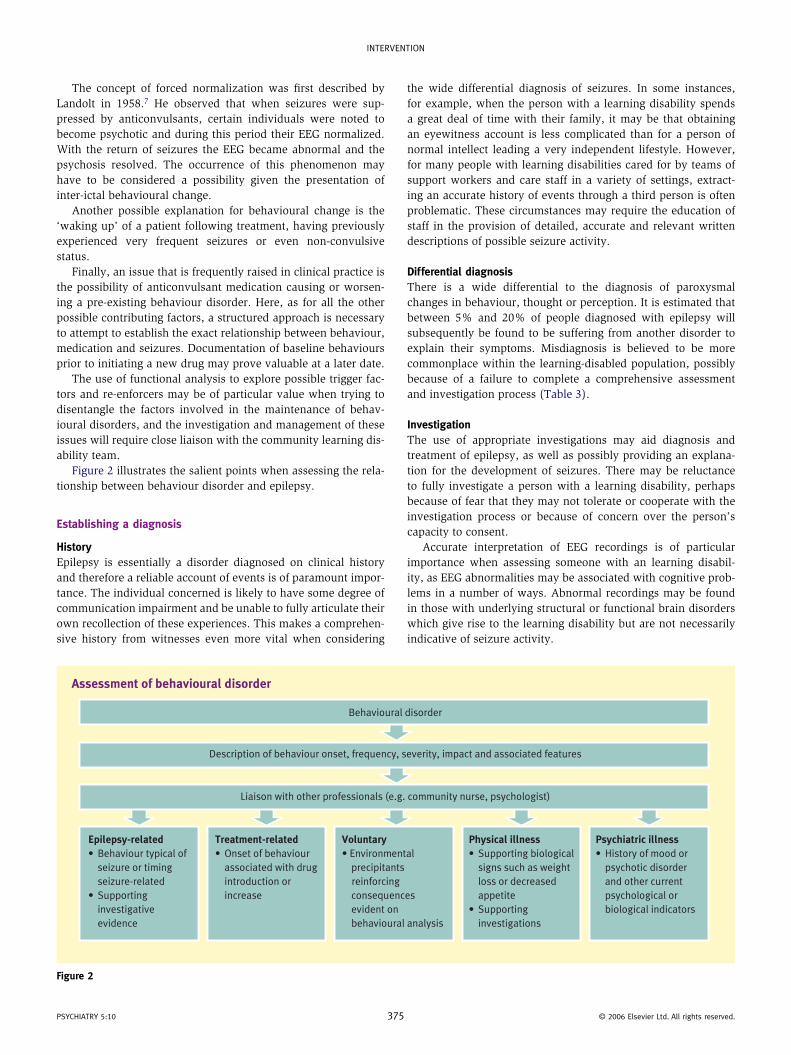
The use of functional analysis to explore possible trigger fac-tors and re-enforcers may be of particular value when trying to disentangle the factors involved in the maintenance of behav-ioural disorders, and the investigation and management of these issues will require close liaison with the community learning dis-ability team.
Figure 2 illustrates the salient points when assessing the rela-tionship between behaviour disorder and epilepsy.
Establishing a diagnosis
HistoryEpilepsy is essentially a disorder diagnosed on clinical history and therefore a reliable account of events is of paramount impor-tance. The individual concerned is likely to have some degree of communication impairment and be unable to fully articulate their own recollection of these experiences. This makes a comprehen-sive history from witnesses even more vital when considering
PSYCHIAtrY 5:10 37
the wide differential diagnosis of seizures. In some instances, for example, when the person with a learning disability spends a great deal of time with their family, it may be that obtaining an eyewitness account is less complicated than for a person of normal intellect leading a very independent lifestyle. However, for many people with learning disabilities cared for by teams of support workers and care staff in a variety of settings, extract-ing an accurate history of events through a third person is often problematic. These circumstances may require the education of staff in the provision of detailed, accurate and relevant written descriptions of possible seizure activity.
Differential diagnosisThere is a wide differential to the diagnosis of paroxysmal changes in behaviour, thought or perception. It is estimated that between 5% and 20% of people diagnosed with epilepsy will subsequently be found to be suffering from another disorder to explain their symptoms. Misdiagnosis is believed to be more commonplace within the learning-disabled population, possibly because of a failure to complete a comprehensive assessment and investigation process (Table 3).
InvestigationThe use of appropriate investigations may aid diagnosis and treatment of epilepsy, as well as possibly providing an explana-tion for the development of seizures. There may be reluctance to fully investigate a person with a learning disability, perhaps because of fear that they may not tolerate or cooperate with the investigation process or because of concern over the person’s capacity to consent.
Accurate interpretation of EEG recordings is of particular importance when assessing someone with an learning disabil-ity, as EEG abnormalities may be associated with cognitive prob-lems in a number of ways. Abnormal recordings may be found in those with underlying structural or functional brain disorders which give rise to the learning disability but are not necessarily indicative of seizure activity.
Assessment of behavioural disorder
Behavioural disorder
Description of behaviour onset, frequency, severity, impact and associated features
Liaison with other professionals (e.g. community nurse, psychologist)
Epilepsy-related
• Behaviour typical of
seizure or timing
seizure-related
• Supporting
investigative
evidence
Treatment-related
• Onset of behaviour
associated with drug
introduction or
increase
Voluntary
• Environmental
precipitants
reinforcing
consequences
evident on
behavioural analysis
Physical illness
• Supporting biological
signs such as weight
loss or decreased
appetite
• Supporting
investigations
Psychiatric illness
• History of mood or
psychotic disorder
and other current
psychological or
biological indicators
Figure 2
5 © 2006 elsevier Ltd. All rights reserved.
InterventIon
As in the general population, a single 30-minute EEG record-ing may not provide sufficient information, and use of prolonged recordings, either overnight or over a 24-hour period, may be required. Use of video telemetry may prove particularly helpful when trying to distinguish events of behavioural origin from those that are seizure-related.
Neuroimaging is most commonly used where there is suspicion from the history or EEG findings of focal epilepsy. In most cases a CT or MRI scan will be requested to visualize the structure of the brain, but in some cases functional imaging with single photon emission tomography (SPET) or photon emission tomography (PET) will be required. Neuroimaging has particular relevance in potential candidates for neurosurgery. Some patients may have difficulty cooperating with the procedures necessary for imaging techniques and therefore facilities for sedation or general anaes-thesia under these circumstances should be available.
Treatment
The decision to initiate treatment is usually made after an indi-vidual has had two or more seizures. For a minority of people who experience very infrequent partial seizures with little impact upon quality of life, it may be decided that the potential ben-efits to treatment are slight and outweighed by its side effects. In most cases, however, the aim will be to achieve optimum seizure control with minimum adverse effects. Seizure freedom with monotherapy is the ideal, but only 60–70% will achieve an adequate response to a single anticonvulsant. For those patients whom continue to experience seizures despite appropriate prescription of first-line therapy, prior to commencing alterna-tive treatment it may be prudent to first review the diagnosis, ensure compliance and increase to the maximum tolerated dose. If monotherapy is unsuccessful, one or more additional medi-cations may be required to achieve optimal seizure control. A proportion of patients will exhaust all medication options and
Differential diagnosis of epilepsy
System Examples
neurological transient ischaemic attack
Migraine
Cataplexy
tourette syndrome
Cardiovascular Syncope
Cardiac arrhythmia
Aortic stenosis
Mitral valve prolapse
other physical Hypoglycaemia
emotional Hyperventilation
Panic attack
Conversion disorder
Factitious disorder
Malingering
Table 3
PSYCHIAtrY 5:10 37
continue to experience dangerous or disabling seizures; for these patients the possibility of surgery or vagal nerve stimulation must be considered.
Choosing an anticonvulsantFew randomized trials have been conducted specifically in the learning disabled population. Therefore, in the majority of cases when making a choice of anticonvulsant, data will need to be extrapolated from evidence based on either the non-learning dis-abled population or a mixed population. Explanations for the lack of trial data in this group may include consent issues, difficulty in determining seizure type and presence of the comorbidities which are so frequently seen in the cognitively impaired. Of the few trials that have focused on the learning disabled, treatment of Lennox–Gestaut syndrome has been the focus of two; the first in 1997 demonstrated the efficacy of lamotrigine with relatively few side effects and the second in 1999 atonic seizure reduc-tion with topiramate but an apparent increase in behavioural problems.8,9
An accurate diagnosis of seizure type and syndrome is of par-ticular importance when prescribing medication, as some anti-convulsants may worsen certain types of seizures (e.g. the use of carbamazepine or phenytoin with absence or myoclonic sei-zures). The presence of common physical comorbid conditions such as obesity, dysphagia or reflux oesophagitis may also influ-ence the choice of drug or preparation. Other factors such as psy-chiatric illness or behavioural disorder will also need to be taken into consideration, as well as potential interactions between the proposed anticonvulsant and already established medication. The potential pro-convulsant effects of other medications may be of significance. One percent of patients maintained on antipsy-chotics develop seizures, although the risk is thought to be lower with rispiridone and olanzapine. Caution, however, may be required with the use of clozapine, which is believed to decrease the seizure threshold to a greater degree.
Knowledge of the side-effect profiles of the various anti-epileptic drugs is of particular importance as people with learning disabili-ties may be both more likely to develop these adverse effects and less likely to express their discomfort effectively to those around. Adverse effects can be minimized by a relatively low starting dose and slow titration. The risk of side effects increases in those taking more than one anti-epileptic, due to their potential interaction. In the non-learning-disabled population, delirium, psychotic symp-toms and cognitive changes have been linked with use of anticon-vulsants in particular. Phenobarbitone and primidone, and to a lesser extent carbamazepine and valproate, have been associated with the development of depressive symptoms. It has been sug-gested that gabapentin and lamotrigine have a low risk of precipi-tating psychiatric symptoms or worsening cognitive dysfunction. Where a psychiatric disorder has been induced by anticonvulsant medication it may respond to a reduction in dose or change of drug.
Withdrawal of medication can in some instances also result in changes to mental state. Barbiturate and benzodiazepine discontinuation has been associated with incidence of psychi-atric symptoms. In other cases, where an anticonvulsant with mood-stabilizing properties such as carbamazepine, valproate or lamotrigine is withdrawn, an underlying bipolar disorder may be unmasked.
6 © 2006 elsevier Ltd. All rights reserved.
InterventIon
Measuring outcomeThe assessment of treatment outcome is a continual process and will often involve multidisciplinary working. In order to make an accurate assessment of seizure frequency and severity, written recordings by either parents or carers should be made. Guidance in this matter will often be required to ensure accurate documentation. Ongoing evaluation of the impact of epilepsy upon the individual and their quality of life should be made, in order to identify possible areas for change aside from those related solely to medication, and the communication of this information should be coordinated so that it reaches the relevant professionals (e.g. the physician dealing with the epilepsy, the community nurse). ◆
REFERENCES
1 Shepherd C, Hosking G. epilepsy in school children with intellectual
impairments in Sheffield: the size and nature of the problem and
the implications for service provision. J Ment Defic Res 1989; 33:
511–4.
2 Mariani e, Ferini-Strambi L, Sala M et al. epilepsy in institutionalised
patients with encephalopathy: clinical aspects and nosological
considerations. Am J Ment Retard 1993; 98: 27–33.
3 epilepsy Bereaved. National sentinel clinical audit of epilepsy-
related death. Wantage: epilepsy Bereaved, 2002.
4 Corbett J A. epilepsy and mental retardation. In: trimble M r,
reynolds e H, eds. Epilepsy and psychiatry. edinburgh: Churchill
Livingstone, 1981.
5 Deb S, Courie v A, richens A. Folate metabolism and problem
behaviour in mentally handicapped epileptics. J Ment Defic Res
1987; 31: 163–8.
PSYCHIAtrY 5:10 37
6 espie C A, Pashley e S, Bonham K G, Sourindham I, o’Donovan M.
the mentally handicapped person with epilepsy: a comparative
study investigating psychosocial functioning. J Ment Defic Res
1989; 33: 123–35.
7 Landolt H. Serial electroencephalographic investigations during
psychotic episodes in epileptic patients and during schizophrenic
attacks. In: De Haas L A M, ed. Lectures on epilepsy. Amsterdam:
elsevier, 1958.
8 Motte J, travathen e, Barrerra M et al. Lamotrigine for generalised
seizures associated with Lennox–Gestaut syndrome. N Engl J Med
1997; 337: 1807–12.
9 Sachdeo r, Kugler S, Wenger e, Mandelbaum D. topiramate in
Lennox Gastaut syndrome. Epilepsia 1996; 37: 118.
Practice points
• epilepsy is a common and often difficult-to-treat comorbidity
in people with learning disabilities
• A comprehensive assessment including accurate diagnosis,
investigation and evaluation of impact of both the epilepsy
and the treatment is necessary to produce a management
plan
• An awareness of the significance of psychiatric disorder and
behavioural disorder in epilepsy are important, as people
with learning disabilities have a high baseline prevalence of
all three
• Multidisciplinary working will often be necessary to ensure
the appropriate information is available in order for an
informed decision regarding epilepsy management to be
made
7 © 2006 elsevier Ltd. All rights reserved.






![PERSONAL SHORT STORIES - The IBE · PWE People with Epilepsy . 3 Preface This booklet was compiled to inspire people with epilepsy [PWE] and general public that anyone with epilepsy](https://img.pdfslide.us/doc/110x75/5fe0ef284c0a727e886c2827/personal-short-stories-the-ibe-pwe-people-with-epilepsy-3-preface-this-booklet.jpg)






















