Embed Size (px)
Citation preview

8/24/2011
1
Epidural Steroid Injections:A Review of the Recent Literature
Janette (Jan) Elliott, RN-BC, MS, AOCN
September 9, 2011
What is an Epidural Steroid Injection?
An injection of a steroid medication into the epidural space with the intent to alleviate pain
Epidural anatomy
Spinal meninges
Pia mater
Arachnoid
Dura
Epidural
“outside the dura”
8/24/2011
2
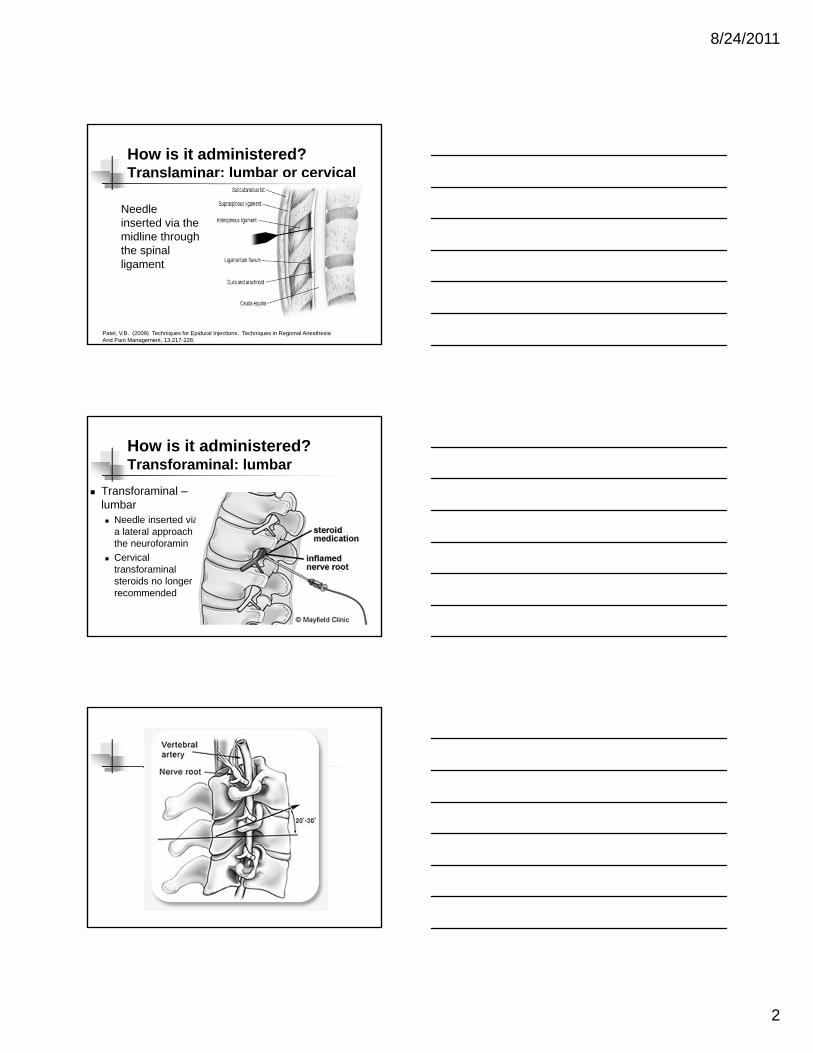
How is it administered?Translaminar: lumbar or cervical
Needle inserted via the midline through the spinal ligament
Patel, V.B. (2009) Techniques for Epidural Injections. Techniques in Regional AnesthesiaAnd Pain Management, 13:217-228.
How is it administered?Transforaminal: lumbar
Transforaminal –lumbar Needle inserted via
a lateral approach to the neuroforamin
Cervical transforaminal steroids no longer recommended
8/24/2011
3
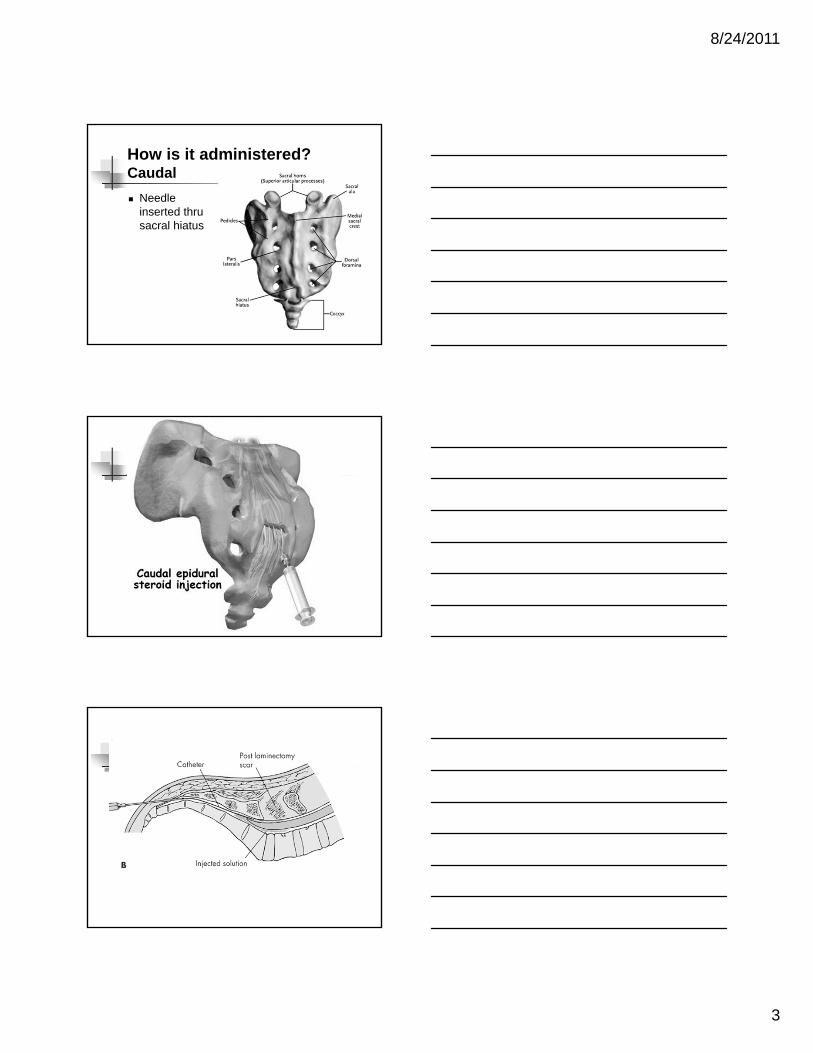
How is it administered?Caudal
Needle inserted thru sacral hiatus
8/24/2011
4
How do steroids work?
Reduce inflammation by blocking transmission of C fiber input.
Steroids decrease inflammation by inhibiting phospholipase A2 action.
Epidural steroid injection places the medication at the site of inflammation
Indications for Epidural Steroid Injection
Herniated nucleus pulposus with nerve root irritation
Herniated nucleus pulposus with nerve root compression
Annulus tear—hasten recovery
Spinal stenosis—transient relief
Post laminectomy syndrome
Contraindications of ESI
Uncontrolled diabetes +/- epidural lipomatosis Bleeding concerns
Anticoagulation Bleeding disorders
Bleeding factor deficiencies Von Willebrand’s disease Idiopathic thrombocytopenic purpura (ITP) Low platelet count Severe liver dysfunction Hemophilia
Infection
8/24/2011
5
Anticoagulants and ESIs
Warfarin (Coumadin) Stop 5 days in advance of procedure
Clopidogrel (Plavix)• Stop 7 days in advance of procedure
Low Molecular weight heparin (Enoxaparin)• Last dose 24 hours prior
Ticlopidine (Ticlid)• Stop 14 days prior
Anticoagulants and ESIs (cont)
Platelet GP IIb/IIIa receptor antagonists abciximab (Reopro) iptifibatide (Integrilin) tirofiban (Aggrastat)
Stop 5 days in advance of procedure Resume on postop day Enoxiparin bridge
Horlocker, T. et al, (2010) Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Regional Anesthesia and Pain Medicine. Volume 35(1), January/February 2010, pp 64-101, DOI: 10.1097/AAP.0b013e3181c15c70
Newer Anticoagulants
Dabigatran (Pradaxa)
Rivaroxaban (Xarelto)
Apixaban (Eliquis)--investigational
Dabigatran and Rivaroxaban approved in post-op total hip and knee patients
Research in other settings
Liau, J.V. and Ferrandis, R. (2009) New Anticoagulatns and Regional Anesthesia. Current Opinion in Anaesthesiology, 22:661-666.
8/24/2011
6
How is the procedure performed? Lumbar
Prone—Preferred Sitting—if person too heavy for procedure table, blind stick Side lying—more likely used with inpatients, blind stick Caudal – through sacral hiatus Loss of resistance technique +/- contrast
Cervical Prone—Preferred, may use fluoro Sitting Loss of resistance or hanging drop technique +/- contrast
Fluoroscopic guidance—current standard of care Ultrasound guidance—help determine depth
Potential complications
Dural puncture—”wet tap”
Hematoma Spinal injury
Direct nerve injury
Infection
Direct nerve injury from needle or pressure of injectate
Vertebral artery dissection
Stroke
Death
Potential side effects of the steroid medication
Localized increase in pain Non-positional headaches resolving within 24 hours Facial flushing Anxiety Sleeplessness Fever the night of injection High blood sugar A transient decrease in immunity because of the
suppressive effect of the steroid Stomach ulcers Severe arthritis of the hips (avascular necrosis) Cataracts
Staehler, R. (2007) Epidural Steroid Injections: Risks and Side Effects. Downloaded 8/10/11 from http://www.spine-health.com/treatment/injections/epidural-steroid-injections-risks-and-side-effects

8/24/2011
7
Epidural Space Identification
?? Liquid or air as medium for loss of resistance
5 publications included in a meta analysis
Hypothesis: LOR technique with liquid medium associated with fewer epidural-related complications
Results Not statistically different in obstetric population
Small statistically difference (1.5%) in chronic pain population for post dural puncture headache with fluid
Schier, R. et al, (2009) Epidural Space Identification: A Meta-Analysis of Complications After Air Versus Liquid as the Medium for Loss of Resistance. Anesthesia & Analgesia, 109:2012-2021.
Identification of Cervical Spinous Level
Control group—palpate for C7 with patient in anatomical position, N=48
Flex/Ex group—palpate for C& for flexing and extending patients neck, N=48
Used fluoro to confirm accuracy
Control—37.5% accurate
Flex/Ex—77.1% accurate
Shin, S., Yoon, D, and Yoon, K.B. (2011) Identification of the Correct Cervical Level by Palpation of Spinous Processes. Anesthesia-Analgesia, 112(5): 1232-1235
Ultrasound Guidance
Advantages Portability, cost, ability to see soft tissues, lack of
radiation
Help identify needle depth 100% lumbar L4/5, less at higher levels
Helpful in pediatric/infant populations

8/24/2011
8
Ultrasound Guidance (cont)
Limitations Lack of contrast medium for visualization of
vascular structures
Small window for visualization of needle, injectate and dura mater.
Requires 2 people
Shankar, H and Zainer, C. (2009) Ultrasound guidance for Epidural Steroid Injections. Techniques is Regional Anesthesia and Pain Management, 13:229-235.
Quality of Evidence Developed by U.S. Preventive Services Task Force
I: Evidence obtained from at least one properly randomized controlled trial
II-1: Evidence obtained from well-designed controlled trials without randomization
11-2: Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than one center or research group
II-3: Evidence obtained from multiple time series with or without the intervention. Dramatic results in uncontrolled experiments (such as the results of the introduction of penicillin treatment in the 1940s) could also be regarded as this type of evidence
III: Opinions of respected authorities, based on clinical experience descriptive studies and case reports or reports of expert committees
Adapted from Berg, A.O. and Allan, J.D. (2001) Introducing the Third U.S. Preventive Services Task Force. American Journal of Preventive Medicine, 20:21-35.
Outcome measures
Short term relief--< 6 months
Long term relief--> 6 months
Improvement in function or psychological status This wasn’t always commented on in the reviews
Return to work Not commented on in the reviews
Reduction in opioid intake Not commented on in the reviews
All of these reviews done by the same clinical group

8/24/2011
9
Buenaventura--Lumbar Transforaminal
Systematic Review—4 randomized studied included
Results Short term– level II-1
Long term—level II-2
Pain reduction—64-81%
Disability reduction—60-63%
Reduce depression—56%
Buenaventura, R.M., Datta, S., Abdi, S. and Smith, H.W. (2009) Systematic Review of Therapeutic Lumbar Transforaminal Epidural Steroid Injections. Pain Physician, 12:233-251.
Benyamin-Cervical Interlaminar
Systematic Review—1,994 reviewed--3 systematic reviews, 3 randomized studies and 5 observational studies included
Studies included multiple injections
Some used local anesthetic alone instead of steroid
Results—Level II-1 Pain reduction—68-79% at 6 months
Disability reduction—not reported
Reduce depression—not reported
Limitation—paucity of available research
Benyamin, R. et al (2009) Systematic Review of The Effectiveness of Cervical Epidurals in the Management of Chronic Neck Pain. Pain Physician, 12:137-157.
Parr—Lumbar InterLaminar
Systematic Review—1,647 reviewed—8 systematic reviews, 20 randomized studies and 30 observational studies included
Studies included multiple injections
Some used local anesthetic alone instead of steroid
Results— Level II-2 for short term and level III for long term--disc
herniation or radiculitis
Level III for short and long term—spinal stenosis and discogenic pain without radiculitis or hernation

8/24/2011
10
Parr—Lumbar InterLaminar (cont)
Pain reduction—at 3, 6 and 12 months no significant difference for disc herniation or
radiculitis Significant difference in 1 study at 3 months,
no significant difference at 6 or 12 months Disability reduction—not reported Reduce depression—not reported
Parr, A.T., Diwan, S., and Abdi, S. (2009) Lumbar Interlaminar Epidural Injections in Managing Chronic Low back and Lower Extremity Piana; A Systematic Review . Pain Physician, 12:163-188.
Conn—Caudal
Systematic Review—3,387 reviewed—18 randomized studies and 20 observational studies included
Studies included multiple injections
Some used local anesthetic alone instead of steroid
Conn—Caudal (cont)
Results— Level I for short and long term for disc herniation and/ and/or
radiculitis and discogenic pain
Level II1 or II-2 for Post-laminectomy syndrome and spinal stenosis
Pain reduction
56-81% for disc herniation or radiculitis
65-77% post-laminectomy syndrome
Disability reduction—not consistently stated in the review
One study showed > 40% decrease in 55-70% of patients
Conn, A., Buenaventura, R.M., Datta, S., Abdi, S and Diwan, S. (2009) Systematic Review of Caudal Epdiural Injections in the Management of Chronic Low Back Pain. Pain Physician, 12:109-135.

8/24/2011
11
Abdi--Epidural Steroids
Combines all types of ESIs < 6 weeks short term and > 6 weeks long term Concludes:
Moderate evidence for interlaminar cervical and lumbar for long term relief
Moderate for cervical and lumbar transforaminals for long term relief in nerve root pain
Moderate evidence for caudal for long term relief in nerve root pain and chronic LBP
Adbi, et al. (2007) Epidural Steroids in the Management of Chronic Spinals Pain: A Systematic Review. Pain Physician, 10:185-212
Boswell-Practice Guidelines-2007
Includes all spinal procedures but puts into separate procedures
Caudal--states the reviews come to different conclusions from the same studies
Concludes Chronic LBP and radicular pain
Short term benefit--strong Long term--moderate
Post laminectomy syndrome and spinal stenosis Limited evidence
Boswell-Practice Guidelines
Concludes Interlaminar in lumbar radiculopathy
Short term--strong Long term--limited
Interlaminar in postlaminectomy syndrome Limited
Interlaminar in cervical radiculopathy Short term & long term--moderate
Transforaminal lumbar Short-term--strong Long term--moderate
8/24/2011
12
Boswell-Practice Guidelines (cont)
Transforaminal cervical Short and long term--moderate
Evidence is indeterminate in managing axial LBP, axial neck pain, and lumbar disc extrusions
Boswell et al, (2007) Interventional Techniques: Evidence-based Practice Guidelines in the Management of Chronic Spinal Pain. Pain Physician: 10:7-111.
ASIPP IPM Guidelines-2009
Chronic Spinal Pain Interventional Techniques
Comprehensive review
Manchikanti, L. et al (2009) Comprehensive Evidence-Based Guidelines for interventional Techniques in the Management of Chronic Spinal Pain. Pain Physician: 12:699-802.
ASIPP--Caudal
Level 1—caudal for disc herniation or radiculitis and discogenic pain
Level II-1 or II-2 for post-laminectomy and spinal stenosis
8/24/2011
13
ASIPP—Cervical, Lumbar & Thoracic Interlaminar
Level II-1 or II-2
ASIPP Common Indications for ESIs
Chronic pain poorly responsive to non-interventional or non-surgical therapy Disc herniation or radiculitis
Spinal Stenosis
Post spinal surgery syndrome
Epidural fibrosis
DDD/discogenic pain
Absence of facet pain
Pain causing functional disability
Average pain level > 6
“Other causes”
Transforaminal Cervical ESIs Fallen into disfavor Catastrophes
Cerebellar and cerebral infarcts Spinal cord injury and infarction Massive cerebral edema Visual defects r/t vascular occlusion Persistent neurological deficits Transient quadriplegia Subdural hematoma
Unknown incidence, but “rare”
Adbi, et al. (2007) Epidural Steroids in the Management of Chronic Spinals Pain: A Systematic Review. Pain Physician, 10:185-212

8/24/2011
14
Frequency of ESIs
One week apart if in diagnostic phase, 2 weeks preferred in cancer pain
2 months or longer in therapeutic phase provided > 50% pain relief ofr 6-8 weeks
Repeated only as necessary according to medical necessity criteria
Limit to a max of 4-6 per year Manchikanti, L. et al (2009) Comprehensive Evidence-Based Guidelines for interventional
Techniques in the Management of Chronic Spinal Pain. Pain Physician: 12:699-802.
What steroid does one use?
Depends on the type of ESI to be performed
Cerebral/cerebellar complications occur mainly through intravascular embolization of the particulate steroid in transforaminal ESIs
No CNS events reported with interlaminar ESIs
No CNS events reported with non-particulate steroid
Medications
Methylprednisolone (Depo-medrol)
Triamcinolone (Kenalog)
Dexamethasone (Decadron)
Betamethasone (Celestone) Betamethadone sodium phosphate/betamethasone acetate
Betamethasone repository (compounded drug) Betamethadone sodium phosphate/betamethasone acetate
Betamethasone sodium phosphate
No study has directly compared efficacy

8/24/2011
15
Comparison of Drugs
Measured using laser scanning confocal microscope
Compared diluted vs non-diluted drug
Compared to size of blood vessels
Derby measured size of blood vessels
Steroid Medications Methylprednisone 80mg/ml with more particles than
40mg/ml
Compounded betamethasone with more particles than commercial betamethasone
No statistical difference between methylprednisolone and triamcinolone and compounded betamethasone
INCREASED proportion of particles in MORE HIGHLY DILUTED methylpredsinolone 80mg/ml
Otherwise dilution decreased % larger particles
Dexamethasone and betamethasone phospate were pure liquid
Steroid Medications Recommended
Benzon recommends non-particulate steroid betamethasone phospate for transforaminal ESIs
Benzon states dexamethasone should be used with caution until further studies clarify safety and efficacy
Derby states “interventionalists might consider using a nonparticulate steroid when performing cervical transforaminal injections”
Derby states “Dexamethasone is less likely to cause arterial or capillary obstruction…”
Benzon, H.T. et al. (2007) Comparison of the Particle Sizes of Different Steroids and the Effect of Dilution. Anesthesiology, 106:331-8
Derby, R. et al (2008) Size and Aggregation of Corticosteroids Used for Epidural Injections. Pain Medicine, 9(2): 227-234.
8/24/2011
16
Summary ESIs most used interventional technique
Many patients achieve significant benefit
Conflicting results from systematic reviews
None reach Level I evidence
No specific medication recommendations for interlaminar ESIs
Non-particulate medications recommended for transforaminal ESIs
Debate as to whether to do cervical transforaminal injections
ASRA recommendations for anticoagulation
Use of fluoroscopy is standard of care
References: Adbi, et al. (2007) Epidural Steroids in the Management of Chronic Spinals Pain: A
Systematic Review. Pain Physician, 10:185-212
Benyamin, R. et al (2009) Systematic Review of The Effectiveness of Cervical Epidurals in the Management of Chronic Neck Pain. Pain Physician, 12:137-157.
Benzon, H.T. et al. (2007) Comparison of the Particle Sizes of Different Steroids and the Effect of Dilution. Anesthesiology, 106:331-8
Berg, A.O. and Allan, J.D. (2001) Introducing the Third U.S. Preventive Services Task Force. American Journal of Preventive Medicine, 20:21-35.
Boswell et al, (2007) Interventional Techniques: Evidence-based Practice Guidelines in the Management of Chronic Spinal Pain. Pain Physician: 10:7-111.
Buenaventura, R.M., Datta, S., Abdi, S. and Smith, H.W. (2009) Systematic Review of Therapeutic Lumbar Transforaminal Epidural Steroid Injections. Pain Physician, 12:233-251.
Conn, A., Buenaventura, R.M., Datta, S., Abdi, S and Diwan, S. (2009) Systematic Review of Caudal Epdiural Injections in the Management of Chronic Low Back Pain. Pain Physician, 12:109-135.
Derby, R. et al (2008) Size and Aggregation of Corticosteroids Used for Epidural Injections. Pain Medicine, 9(2): 227-234.
Horlocker, T. et al, (2010) Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Regional Anesthesia and Pain Medicine. Volume 35(1), January/February 2010, pp 64-101, DOI: 10.1097/AAP.0b013e3181c15c70
References (cont) Liau, J.V. and Ferrandis, R. (2009) New Anticoagulatns and Regional Anesthesia.
Current Opinion in Anaesthesiology, 22:661-666.
Manchikanti, L. et al (2009) Comprehensive Evidence-Based Guidelines for interventional Techniques in the Management of Chronic Spinal Pain. Pain Physician: 12:699-802.
Parr, A.T., Diwan, S., and Abdi, S. (2009) Lumbar Interlaminar Epidural Injections in Managing Chronic Low back and Lower Extremity Piana; A Systematic Review . Pain Physician, 12:163-188.
Patel, V.B. (2009) Techniques for Epidural Injections. Techniques in Regional Anesthesia And Pain Management, 13:217-228.
Schier, R. et al, (2009) Epidural Space Identification: A Meta-Analysis of Complications After Air Versus Liquid as the Medium for Loss of Resistance. Anesthesia & Analgesia, 109:2012-2021 Shankar, H and Zainer, C. (2009) Ultrasound guidance for Epidural Steroid Injections. Techniques is Regional Anesthesia and Pain Management, 13:229-235.
Shin, S., Yoon, D, and Yoon, K.B. (2011) Identification of the Correct Cervical Level by Palpation of Spinous Processes. Anesthesia-Analgesia, 112(5): 1232-1235
Staehler, R. (2007) Epidural Steroid Injections: Risks and Side Effects. Downloaded 8/10/11 from http://www.spine-health.com/treatment/injections/epidural-steroid-injections-risks-and-side-effects





























