Embed Size (px)
Citation preview

EPIDEMIOLOGY UNIT, ASL 5 PIEDMONT REGION
RISK FACTORS FOR UPPER EXTREMITY MUSCOLOSKELETAL SYMPTOMS IN CALL CENTER EMPLOYEES
d’Errico A 1, Caputo P 2, Falcone U 3, Fubini L 3, Gilardi L 3, Mamo C 1, Migliardi A 1, Quarta D 1.
1 Epidemiologic Unit, ASL 5 - Piedmont Region,; 2 University of Turin; 3 Documentation Center for Health Promotion of Piedmont Region
Background
The call center sector has grown fast in the last decades in industrialized and in some less developed countries. In Italy a great expansion of this sector also occurred, with an increase from 1,500 workers employed in 1994 to more than 200 thousands in 2005-2006. In general terms, call centers are structures through which organizations of any kind (institutions, companies, banks, no-profit, etc.) manage telephone contacts with their clients, in order to provide information or assistance on the products/services offered.
Call centers have been defined as modern industries producing services using the information and communication technologies (Bagnara e Marti, 2001), owing to the nature and the organization of work performed, which expose workers to a variety of psychosocial, ergonomic and microclimatic hazards. (Australian CC guidelines)
Several studies have reported increased risks for different health outcomes among call centers operators, such as insomnia, anxiety, depression, visual fatigue and musculoskeletal disorders (MSDs). In particular, prevalences of musculoskeletal disorders of the back and upper limb appear very high in some studies, even greater than those observed in other occupational groups also considered at risk (Sprigg, 2003; Norman, 2004; Rocha et al., 2005).
Methods
Workers from seven call centers operating in the Turin area were invited to participate in the survey. During 2005-2006, 775 people working in telecommunications (70%), telemarketing (16%) and banking (14%) completed a standardized questionnaire on socio-demographics and lifestyle, working conditions, symptoms and diseases. The outcome was defined as the presence of musculoskeletal symptoms in the upper limb at any time during the last 28 days, for which a physician was consulted and/or drugs were taken. We explored the relationship between UEMSD and socio-demographic variables, and the following work-related features: sector and job seniority, weekly hours worked, shift work, workstation design, lighting, noise, microclimatic conditions, frequency and duration of breaks, number of and time between calls, supervisor and co-worker support, job insecurity, psychological demand, job control and job strain. The relative risks of UEMSD were estimated by prevalence rate ratios obtained from Poisson regression models with the Huber-White sandwich estimator of variance (Barros and Hirakata, 2003).
Results Overall, 336 (45%) workers reported upper extremity symptoms for which they consulted a physician and/or took drugs. Symptoms in the neck were the most prevalent (39%), followed by shoulder (22%), hand-wrist (10%) and elbow (4%); 169 (50%) workers reported symptoms in more than one region. Among workplace risk factors, the presence of any upper extremity symptom was significantly associated with lack of supervisor recognition, lack of wrist support during keyboarding, high job strain, continuously elevated noise and workplace humidity, along with previous injuries, chronic disease potentially related to UEMSD and leisure sport activities. Restricting the analysis to 200 workers with only neck/shoulder symptoms did not substantially change these results. As only 22 workers reported symptoms in the elbow/hand-wrist and not in the neck/shoulder, we examined all 89 workers with elbow/hand-wrist symptoms, although 67 (75%) had reported both. Supervisor recognition, aspects of workstation design and previous injuries were risk factors common to both upper extremity regions; elbow/hand-wrist symptoms were also associated with higher seniority in the call center sector, short interval between calls, frequent mouse use, job insecurity and low educational level. These same risk factors were found for workers who reported symptoms in both regions.
Discussion: The results of the present study confirm the etiologic role of wood and leather dusts on the genesis of SNC adenocarcinomas, suggesting also welding fumes and paint mists as probable causal agents. SNC with other histologies seem to recognize a different pattern of risk factors, probably including nickel compounds and possibly welding fumes and oil mists. The observed association with welding fumes, classified by IARC as a certain carcinogen (class 1), appears consistent with the excess risks found by Hernberg et al. (1983) among welders, and by Olsen (1988) in workers employed in the production of metal containers, where exposure to welding fumes is supposed to be widely spread. Paint mists have been reported to be associated with SNC by Olsen & Jensen (1987), who found a significant 6-folds increased risk in subjects working in the production of paints and enamels in Denmark, though based on few cases. Concerning oils mists, a significant association with SNC (OR=2.8) has been found by a case-control study conducted in Connecticut (Roush et al., 1980), while a significant excess mortality has been observed by the British Occupational Mortality Surveillance System among machine tool operators (Winter et al., 1995), whose main exposure is represented by cutting fluids.
Aims
1. To assess the prevalence of upper extremity musculoskeletal disorders (UEMSD) in a cross-sectional sample of Italian workers employed in the call center industry, and
2. to identify ergonomic, organizational and psychosocial factors at work associated with UEMSD.
References: • Hernberg S, Westerholm P, Schultz-Larsen K, et al. (1983). Nasal and sinonasal cancer: connection with occupational exposure in Denmark., Finland and
Sweden. Scand. J. Work Environ. Health, Vol. 9, No. 4, pp. 315-326. • Olsen JH (1988) Occupational risks of sinonasal cancer in Denmark. Br. J. Ind. Med., Vol. 45 No. 5, pp. 329-335.• Winter P, Inskip H, Coggon D, Pannett B (1995). Significant PMRs for each job group. In: Occupational Health. Decennial Supplement. Drever F. Editor. Office
of Population, Censuses and Surveys, Health and Safety Executive, London, HMSO, pp. 374. • Roush CG, Meigs JW, Kelly J, et al. (1980). Sinonasal cancer and occupation: a case-control study. Am. J. Epidemiol., Vol. 111, pp. 183-193. • Olsen JH & Jensen OM (1987) Occupation and risk of cancer in Denmark. An analysis of 93,810 cancer cases, 1970-1979. Scand. J. Work Environ. Health,
Vol. 13, Suppl 1, pp. 1-91
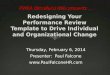
SELECTED WORKSTATION DESIGN CHARACTERISTICS BY ECONOMIC SECTOR (755 subject)
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
desk area insuff icient w orkstation spaceinsuff icient
incorrect keyboardheight
no w rist supportduring keyboarding
no forearm supportduring keyboarding
no forearm supportduring mouse use
chair not adjustable
workstation features
per
cen
tag
e
f inance
services
telecommunication
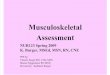
LIGHTING, NOISE AND MICROCLIMATE BY ECONOMIC SECTOR (755 subject)
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
insuff icient desklighting
insuff icient roomlighting
too high noise too hot in summer too cold in w inter insuff icient ventilation too high humidity
workplace features
pe
rce
nta
ge f inance
services
telecommunication
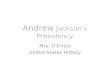
OVERLAP BETWEEN MUSCULOSKELETAL SYMPTOMS IN FOUR UPPER LIMB REGIONS (NECK, SHOULDER, ELBOW, WRIST/HAND)
39%
5%1%
6%
30%
1%
4%
0%1%
0%2%
7%0% 2% 2%
neck only
shoulder only
elbow only
hand/wrist only
neck+shoulder
neck+elbow
neck+wrist/hand
shoulder+elbow
shoulder+wrist/hand
elbow+wrist/hand
neck+shoulder+elbow
neck+shoulder+wrist/hand
shoulder+elbow+wrist/hand
neck+elbow+wrist/hand
neck+shoulder+elbow+wrist/hand
WORK ORGANIZATION CHARACTERISTICS BY ECONOMIC SECTOR (755 subjects)
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
90.00
100.00
variable w orkshifts
presence ofproductionstandard to
reach
presence ofperformance
monitoringsystems
not possible todecide w hen to
take a break
too shortduration of
breaks
<=2 secondsbetw een calls
at peakintensity
>=30 calls perhour at peak
intensity
high tertile ofdemand
high tertile ofcontrol
high tertile ofjob strain
workplace features
per
cen
tag
ef inance
services
telecommunication
Table 1: frequency distribution of the study population by socio-demographic characteristics
Socio-demographic characteristics n. subjects %SEXmales 195 25.8females 560 74.2AGE CLASS19-29 257 3430-39 289 38.340-49 125 16.6>50 84 11.1EDUCATIONless than high school degree 115 15.2high school degree 520 68.9university degree 120 15.9ECONOMIC SECTORbanking 118 15.6services 106 14telecommunication 531 70.3
n. cases IRR95% LCI 95% UCI
Any upper limb symptom 336banking 38 1 - -services 53 1.33 0.99 1.79telecommunication 245 1.26 0.97 1.64Neck-shoulder symptoms 200banking 29 1 - -services 29 1.22 0.82 1.83telecommunication 142 1.16 0.83 1.62Elbow-hand/wrist symptoms 89banking 5 1 - -services 19 3.28 1.27 8.42
Table 2 – Relative risks of upper limb musculoskeletal symptoms by economic sector
(adjusted for age class and sex)