Embed Size (px)
Citation preview

Epidemiology of Mechanical Ventilation
Antonio Anzueto MDProfessor of Medicine
University of Texas Health Science Center, San Antonio, Texas

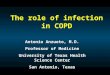
1952: Copenhagen polio epidemic
First month31 patients with respiratory paralysis
27 patients died (87%)

Bjørn Ibsen• The tank respirator
(negative-pressure) did not provide adequate ventilation
• An elevated CO2-content was indicative of CO2 retention, and not, as the epidemiologists considered, of metabolic alkalosis.
• Early application of positive-pressure ventilation

Hand ventilator used in the Copenhagen polio epidemic of 1952 by hundreds of “ventilators”

0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8
Mortality July 1952 March 1953
Months

“Anesthesiologic period”
Before 1970
1970 – mid ’90s
•New modes ofVentilation•PEEP
•Respiratory mechanics
late’90s - NowadaysProtectiveventilatory
strategy

How many patients admitted to an ICU receive mechanical ventilation?
What are the characterisitics of these patients?
How is mechanical ventilation applied?
What are the factors associated with outcome ?

How many patients admitted to an ICU receive mechanical ventilation?
What are the characterisitics of these patients?
How is mechanical ventilation applied?
What are the factors associated with outcome ?

USA/CAN SPA ARG BRA CHI POR URUUSA/CAN SPA ARG BRA CHI POR URU
COPDCOPD 16 16 1111 1010 9 9 1010 2323 55
ComaComa 77 2020 3232 2121 1515 1010 4343
Neuromus.Neuromus. 33 44 88 44 1313 1919 22
ARFARF 7474 6464 5050 6666 6262 4747 5050
ARDSARDS 77 99 99 77 2020 33 77
PneumoniaPneumonia 9’69’6 1111 8’58’5 1919 1212 99 1111
TOTALTOTAL
1313
1515
55
6666
88
1010
REASON FOR MV (%)REASON FOR MV (%)
A. Esteban, A. Anzueto, I. Alía et alAm J Respir Crit Care Med 2000;161:1450

LATIN LATIN AMERICAAMERICA
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
85 %85 %3 %3 %6 %6 %2 %2 %2 %2 %
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
74 %74 %5 %5 %9 %9 %2 %2 %7 %7 %
ACAC----------SIMV-PSVSIMV-PSV----------PCVPCV
71 %71 %
14 %14 %
7%7%
DAY 1DAY 1 DAY 4DAY 4 DAY 7DAY 7
USAUSA
CANADACANADA
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
46 %46 %6 %6 %
15 %15 %2 %2 %
20 %20 %
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
52%52%4 %4 %
10 %10 %4 %4 %
22 %22 %
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
39 %39 %3 %3 %
21 %21 %6 %6 %
24 %24 %
EUROPEEUROPE ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
62 %62 %3 %3 %9 %9 %1 %1 %
15 %15 %
ACACSIMVSIMVSIMV-PSVSIMV-PSVPSVPSVPCVPCV
57 %57 %2 %2 %6 %6 %2 %2 %
23 %23 %
ACAC--------SIMV-PSVSIMV-PSVPSVPSVPCVPCV
57 %57 %
5 %5 %4 %4 %
23 %23 %
MODES OF VENTILATIONMODES OF VENTILATION

J.F. Num, et al. BMJ 1972 1 ICU 426 100
23.5%Mech. Vent.
D.L. Gillespie, et al.
Chest 1986
1 ICU --- 327 Resp. failure
A. Esteban, et alChest 1994
42 ICU 630290 46%
Mech. Vent.
A.F. Connors, et al. AJRCCM 1996 5 ICU --- 1.016 COPD
A. Esteban, et al. AJRCCM 2000 412 ICU 4.1531.638
39%Mech. Vent.
M.L. Nevins, et al.Chest 2001
--- --- 166 COPD
A. Esteban, et al. JAMA 2002 361 ICU 15.7575.18333%
Mech. Vent.
S. Karason, et alActa Anaes. Scand. 2002
27 ICU --- 108Mech. Vent.
Place Patients admitted
Patients with MV
Type of patients

How many patients admitted to an ICU receive mechanical ventilation?
What are the characterisitics of these patients?
How is mechanical ventilation applied?
What are the factors associated with outcome ?

Are we changing the way we use mechanical
ventilation ?
1998 vrs 2004

17575 PATIENTS WERE ADMITTED 17575 PATIENTS WERE ADMITTED
FROM 1 TO 31 MARCH 1998FROM 1 TO 31 MARCH 1998
5183 RECEIVED M.V. > 12 h. (33 %)5183 RECEIVED M.V. > 12 h. (33 %)
361 ICUs361 ICUs
20 COUNTRIES20 COUNTRIES
MONITORING WAS PERFORMED MONITORING WAS PERFORMED DAILY DURING THE COURSE DAILY DURING THE COURSE OF MV UNTIL DAY 28OF MV UNTIL DAY 28
FOLLOW-UP WAS PERFORMED FOLLOW-UP WAS PERFORMED UNTIL HOSPITAL DISCHARGEUNTIL HOSPITAL DISCHARGE
A.Esteban, A. Anzueto, F. Frutos, I. Alía et al.JAMA 2002;287:345-355

1998 2004
Age 61 (46, 72) 61 (46, 72)
% Women 37% 40%
SAPS II 44 (34,54) 41 (30, 55)
Demographic Characteristics
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

1
6
21
72
2
10
17
69
Neuro.Msc.Dis
COPD
Coma
ARF
20041998
Reason for Mechanical Ventilation
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

2.5
4.5
10
8
9
14
21
3
4
7
5
10
11
16
Aspiration
ARDS
CHF
Trauma
Sepsis
Pneumonia
Post-OP
20041998
Etiology of Acute Respiratory Failure
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

How many patients admitted to an ICU receive mechanical ventilation?
What are the characterisitics of these patients?
How is mechanical ventilation applied?
What are the factors associated with outcome ?

0
10
20
30
40
50
60
70 CMV
SIMV-PSV
PCV
PSVSIMV
1998
1 3 5 7 9 11 13 15 17 19 21 23 25 27

0
10
20
30
40
50
60
70 CMV
SIMV-PSV
PCV
PSVSIMV
1998
1 3 5 7 9 11 13 15 17 19 21 23 25 270
60
10
20
30
40
50
CMVPSV
SIMV-PSVSIMV
PCVCVRP
2004

Ventilator Parameters
1998 2004
Tidal Volume (ml/kg)
9 (8, 10) 7 (6, 8)
RR 16 (14, 19) 17 (14, 20)
PEEP 4 (2,5) 5 (5, 7)
Plateau Pressure
23 (21, 26) 20 (16, 25)
>35 3% 2%
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

Ventilator Settings Ventilator Settings & &
ARDSARDS
• What are the usual What are the usual ventilator settings?ventilator settings?
• What are the outcomes What are the outcomes associated with small vs. associated with small vs. moderate or large tidal moderate or large tidal volumes?volumes?

MNVTKG1W
20191817161514131211109876543
MNVTKG1W
Freq
uenc
y
60
50
40
30
20
10
0
10 ml/kg Measured Body 10 ml/kg Measured Body Weight (= 12 ml/kg Predicted) is Weight (= 12 ml/kg Predicted) is the 75the 75thth percentile and is within percentile and is within one standard deviation of the one standard deviation of the mean of the average tidal mean of the average tidal volume used in the 1st week of volume used in the 1st week of ARDSARDS
Tidal Volume DistributionTidal Volume Distribution
Mean = 8.81Mean = 8.81
Std Deviation = 2.05Std Deviation = 2.05
Median = 8.66Median = 8.66
PP2525-P-P7575 = 7.50-10.00 = 7.50-10.00
Mean Tidal Volume (ml/kg)Mean Tidal Volume (ml/kg)
(1st week of ARDS)(1st week of ARDS)
PP7575
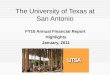
Fergusson et al CCM 2005; 33:21-30

36
54
82
111
84
64
33 32
0
10
20
30
40
50
60
70
80
90
100
<6 6 7 8 9 10 11 >12
Tidal Volume Category (ml/kg ABW)
% M
orta
lity
0
50
100
150
200
250
Num
ber o
f Pat
ient
s
Number of Patients Observed Mortality Corrected Mortality
Observed and Corrected ICU Mortality by Tidal Volume Category Observed and Corrected ICU Mortality by Tidal Volume Category
496 ARDS Patients496 ARDS Patients
Fergusson et al CCM 2005; 33:21-30

– These data suggest that the using tidal volumes of 6-7 ml/kg may These data suggest that the using tidal volumes of 6-7 ml/kg may be beneficial compared with 8-10 ml/kgbe beneficial compared with 8-10 ml/kg
PLPCORMT
PLP
4239363330272421181512
80
70
60
50
40
Corrected Mortality – PCorrected Mortality – PPLATPLAT
% M
orta
lity
% M
orta
lity
Plateau Pressure Category (cm HPlateau Pressure Category (cm H22O)O)
*
*p=0.37 for slope=0
VTOVCOR6
VTNOTLT6
1312111098765
80
70
60
50
40
Tidal Volume Category (ml/kg ABW)Tidal Volume Category (ml/kg ABW)
Corrected Mortality - VCorrected Mortality - VTT
% M
orta
lity
% M
orta
lity
*p=0.03 for slope=0
*
< 6 ml/kg group excluded
Fergusson et al CCM 2005; 33:21-30

ARDS: Ventilator Parameters
1998 2004
Tidal Volume (ml/kg) 8 (7, 10) 7 (6 , 9)
RR 18 (16, 21) 18 (16, 24)
PEEP 7 (5, 9) 9 (7, 11)
Plateau Pressure 27 (24, 30) 26 (22, 29)
>35 6% 3%

15
8
21
8
45
28
2
11
48
0
10
20
30
40
50
60
PSV SIMV SIMV+PSV MultipleSBT
Daily SBT
1998 2004
Weaning Modes
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

Outcome: Duration1998 2004
Mechanical Ventilation (days) 3 (2, 7) 4 (2, 9)
Weaning (days) 2 (1, 4) 2 (1,3)
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

Reintubation/Tracheostomy
1998 2004
Reintubation 14% 14%
Tracheostomy 11% 13%
Time 12 (7, 17) 11 (8, 16)
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

How many patients admitted to an ICU receive mechanical ventilation?
What are the characterisitics of these patients?
How is mechanical ventilation applied?
What are the factors associated with outcome ?

0
0.2
0.4
0.6
0.8
1
1 6 11 16 21 26 31 36 41 46 51 56
Days after initiation of mechanical ventilation
Su
rviv
al
(%
)COPD ARDS ARF no-ARDS
SURVIVAL CURVES ACCORDING TO REASON FOR M.V.SURVIVAL CURVES ACCORDING TO REASON FOR M.V.

PaOPaO2 2 / FiO/ FiO22
n=77n=7736.8%36.8%DEADDEAD
n=209n=209 50
SAPS IISAPS II
n=449n=449100%100%TOTALTOTAL
n=259n=25957.6%57.6%DEADDEAD
ICU MORTALITYICU MORTALITY
n=135n=13544.7%44.7%DEADDEAD
n=302n=302 NO
ACUTE RENALACUTE RENALFAILUREFAILURE
n=51n=5147.2%47.2%DEADDEAD
n=108n=108 < 100
OR = 2.58OR = 2.58
n=26n=2625.7%25.7%DEADDEAD
n=101n=101100 - 200
OR = 1OR = 1

AGEAGE
n=449n=449100%100%TOTALTOTAL
n=259n=25957.6%57.6%DEADDEAD
ICU MORTALITYICU MORTALITY
n=135n=13544.7%44.7%DEADDEAD
n=302n=302 NO
ACUTE RENALACUTE RENALFAILUREFAILURE
n=58n=5862.3%62.3%DEADDEAD
n=93n=93> 50
SAPS IISAPS II
n=11n=1136.6%36.6%DEADDEAD
n=30n=30 48
OR = 1.67OR = 1.67 OR = 8.47OR = 8.47
n=47n=4774.6%74.6%DEADDEAD
n=63n=63> 48

n=449n=449100%100%TOTALTOTAL
n=259n=25957.6%57.6%DEADDEAD
ICU MORTALITYICU MORTALITY
n=124n=12484.3%84.3%DEADDEAD
n=147n=147YES
ACUTE RENALACUTE RENALFAILUREFAILURE
PaOPaO2 2 / FiO/ FiO22
n=97n=9790.6%90.6%DEADDEAD
n=107n=107 < 100
OR = 25.98OR = 25.98
n=27n=2767.5%67.5%DEADDEAD
n=40n=40100 - 200
OR = 5.99OR = 5.99

1010No shock, SAPS II between 51 and 35, No shock, SAPS II between 51 and 35, PPaaOO22/F/FiiOO2 2 >150, coma, age 45>150, coma, age 45 103103 16 %16 % 1.73 (1.00 - 3.01)1.73 (1.00 - 3.01)
1111No shock, SAPS II between 51 and 35, No shock, SAPS II between 51 and 35, PPaaOO22/F/FiiOO2 2 >150, no coma, no sepsis>150, no coma, no sepsis 10841084 16 %16 % 1.64 (1.28 - 2.08)1.64 (1.28 - 2.08)
1212 No shock, PNo shock, PaaOO22/F/FiiOO2 2 >150, SAPS II <35>150, SAPS II <35 13321332 10%10% 11
NºNº Failure (%)Failure (%) ODDS RATIO (CI 95%)ODDS RATIO (CI 95%)
11Shock, non acute renal failure, PShock, non acute renal failure, PaaOO22/F/FiiOO2 2
<150<150 104104 81 %81 % 36.93 (21.98 - 62.05)36.93 (21.98 - 62.05)
22 Shock, acute renal failureShock, acute renal failure 533533 77 %77 % 30.26 (23.11 - 39.64)30.26 (23.11 - 39.64)
33Shock, non acute renal failure, Shock, non acute renal failure, PPaaOO22/F/FiiOO2 2 >150, SAPS II >52>150, SAPS II >52 176176 58 %58 % 12.04 (8.76 - 17.5712.04 (8.76 - 17.57
44 No shock, SAPS II >51, comaNo shock, SAPS II >51, coma 247247 52 %52 % 9.61 (7.08 - 13.06)9.61 (7.08 - 13.06)
55 No shock,SAPS II 51, PNo shock,SAPS II 51, PaaOO22/F/FiiOO22 <150 <150 273273 39 %39 % 5.67 (4.19 - 7.66)5.67 (4.19 - 7.66)
66No shock, SAPS II between 51 and 35, No shock, SAPS II between 51 and 35, PPaaOO22/F/FiiOO2 2 >150, coma, age >45>150, coma, age >45 160160 36 %36 % 4.87 (3.36 - 7.04)4.87 (3.36 - 7.04)
77No shock, SAPS II between 51 and 35, No shock, SAPS II between 51 and 35, PPaaOO22/F/FiiOO2 2 >150, no coma, sepsis>150, no coma, sepsis 7676 34 %34 % 4.57 (2.76 - 7.58)4.57 (2.76 - 7.58)
88 No shock, SAPS II >51, no comaNo shock, SAPS II >51, no coma 763763 33 %33 % 4.28 (3.39 - 5.41)4.28 (3.39 - 5.41)
99Shock, non acute renal failure, Shock, non acute renal failure, PPaaOO22/F/FiiOO2 2 >150, SAPS II 52>150, SAPS II 52 332332 29 %29 % 3.68 (2.74 - 4.95)3.68 (2.74 - 4.95)

Outcome: Length of Stay - Mortality1998 2004
ICU – LOS (days) 7 (4, 14) 7 (4, 14)
ICU – Mortality (%) 31% 35%
Hospital – LOS (days) 16 (9, 29) 16 (8, 30)
Hospital – Mortality (%) 40% 40%
A.Esteban, A. Anzueto, et al. JAMA 2002;287:345-355A. Esteban et al AJRCCM 2008; 177:170-177

Mechanical Ventilation:Conclusions
• Mechanical ventilation is use in a significant number of patients in the ICU.
• Outcome is related to both factors at baseline and complications of critical illness during the course of mechanical ventilation.
• There have being significant changes in the implementation of mechanical ventilation over the last 5 years.

Obrigado