Embed Size (px)
Citation preview

Epidemiology of food hyper-sensitivity in school children
Validation with double-blind placebo-controlled food challenges and biomarkers
The Obstructive Lung Disease in Northern Sweden (OLIN) Studies, Thesis XV
Anna Winberg
Department of Clinical Sciences, Pediatrics
Umeå University 2016

Responsible publisher under Swedish law: the Dean of the Medical Faculty
This work is protected by the Swedish Copyright Legislation (Act 1960:729)
ISBN: 978-91-7601-367-0
ISSN: 0346-6612-1763
Elektronisk version tillgänglig på http://umu.diva-portal.org/
Tryck/Printed by: Print och Media
Umeå, Sweden 2016

PROLOGUE
Bright eyed insight…
During our research travels in Northern Sweden, Åsa - my dear friend and fellow musketeer - and I - were still in denial regarding our uprising presbyopia. Due to our visual impairment we spent an absurd amount of time trying to decipher our study protocols, which, for some reason, were written in ridiculously small letters. During a food challenge series, one of our study participants sat watching us for a very long time and then he bursted out:
Ah! Now I understand what you mean by double-blind!
To all the amazing children who made this thesis possible…

i
Table of Contents
Table of Contents i Abstract iii Sammanfattning på svenska v Abbrevations viii Original Papers ix Introduction 1
Personal point of departure 1 Background 3
Definition of food hypersensitivity (FHS) 3 Prevalence of food hypersensitivity 3 Prevalence of food allergy 3 Prevalence of lactose intolerance 4 Factors associated with food hypersensitivity 5 Risk factors of food allergy 6 Risk factors of lactose intolerance 7 Immunological aspects of food allergy and tolerance development 8 IgE-mediated food allergy 9 Non-IgE-mediated and mixed-immune food allergies 11 Cytokine patterns in tolerance development and IgE-mediated food allergy 11 Allergic inflammation in the intestinal mucosa 12 Symptoms of food allergy 13 Symptoms of IgE-mediated food allergy 13 Symptoms of non-IgE mediated and mixed-immune food allergies 14 Establishing a food allergy diagnosis 15 Clinical history 15 IgE-tests 16 Oral food challenges 17
Open challenges 18 Blinded challenges 18
Complementary diagnostic tests and future prognostic biomarkers 19 Endoscopy 20 Inflammatory and regulatory makers in faeces 20 Atopy patch tests 20 Serological tests 21 Basophil activation tests 22 Cytokines 23
Objectives 25 Materials and methods 27

ii
1. Method: Paper I 27 Method: The OLIN studies 29 Study population 29 Questionnaires 30 Skin Prick Tests 30 Child interview 31 Serological tests 31 Statistical analyses 32 Definitions 33 2. Method: Paper II 37 3. Method: Paper III 39 4. Method: Paper IV 43 5. Method: Paper V 45
Results 49 Validation of new DBPCFC recipes (Paper I) 49 Incidence and remission of food hypersensitivity (Paper II) 50 Assessment of allergy to milk, egg cod and wheat (Paper III) 53 Milk hypersensitivity phenotypes (Paper IV) 54 Biomarkers in blood and stool samples (Paper V) 59
Discussion 63 Discussion of methodology 63 Sensory testing 63 Epidemiologic study design 63 Reported data 65 Analyses of associated risk factors 66 IgE-tests 67 Validation of reported data 68 The DBPCFC methodology 69 Cytokine mRNA expression in PBMC 69 Analyses of fecal biomarkers 70 Discussion of main results 71 Epidemiology of food hypersensitivity 71 Diagnosing food allergy 73 Ethical considerations 75 Personal point of closure 77
Acknowledgements 79 Funding 83 References 84 Supplement 101
Questions from structured interviews 101

iii
Abstract
Background
This thesis focuses on the incidence and remission of reported food
hypersensitivity in schoolchildren followed from 8 to 12 -years of age and the
prevalence of hypersensitivity to milk, egg, cod and wheat among 12-year
olds investigated by reported data, clinical investigation and double-blind
placebo-controlled food challenges and biomarkers.
Methods
The studies are mainly based on a population based cohort recruited in 2006
from three municipalities in Northern Sweden. All children in first and
second grade, aged 7-8 years, were invited to a parental questionnaire study
and 2585 (96% of invited) participated. The children in two of the
municipalities were also invited to a skin prick test with airborne allergens.
At age 11-12 years, there was a follow-up of the cohort using the same
methods, with the addition of a child interview and assessment of body mass
index (BMI).
At the follow-up, children who reported milk hypersensitivity were invited to
structured interviews and children reporting complete elimination of milk,
egg, cod or wheat due to perceived hypersensitivity were invited to a clinical
examination and blood sampling. According to test results, the children were
categorized into different food hypersensitivity phenotypes according to
preset criteria. Children categorized as current food allergy were then invited
to further evaluation with a double-blind placebo-controlled food-challenge
using newly developed recipes. Before their use, the recipes were successfully
validated regarding detectable sensorial differences between the active and
placebo substances in a separate cohort of healthy schoolchildren (n=275).
Before and after the challenge series blood samples were collected for
analyses of cytokine mRNA expression in peripheral blood mononuclear
cells including hallmark cytokines for the humoral allergy-promoting T
helper (Th) 2 response, cellular cytotoxicity-promoting Th1 response,
inflammatory-, and T regulatory responses. Fecal inflammatory biomarkers
were also analyzed before and after the challenge series.

iv
Results
Reported food hypersensitivity increased from 21% at age 7-8 years to 26%
at 11-12 years. There was a high incidence (15%) as well as a high remission
(33%) of reported food hypersensitivity. Risk factors associated with
incidence and remission were different for milk hypersensitivity and
hypersensitivity to foods other than milk. The agreement between reported
symptoms to milk, egg, cod, wheat, soy and peanut and sensitization to the
culprit food was poor. At 11 to 12-years of age the prevalence of reported
allergy to milk, egg, cod or wheat was 4.8% while the allergy prevalence
according to clinical evaluation was 1.4%. This figure was further halved
when evaluated with double-blind placebo-controlled food challenges.
The majority of children with reported allergy to milk, egg, cod and wheat
were categorized as other food hypersensitivity phenotypes, the most
common being probable lactose intolerance (40%) and outgrown food
allergy (19%). Even though reported milk hypersensitivity among the 11-12
year olds was 14.5%, only 3% were categorized as current milk allergy.
Current and outgrown milk allergy was associated with other atopic
disorders and a lower BMI (OR 0.8, 95% CI 0.80-0.98). Before the challenge
series, the mRNA expression of the cytokines IL-13 and IL-10 were higher
among children with a positive compared to a negative challenge outcome.
Conclusion
Reported food hypersensitivity was common among school children in
Northern Sweden and increased from 7-8 years to 11-12 years of age, and
both the incidence and remission of reported hypersensitivity was high.
There was an 8-fold difference in the prevalence of allergy to milk, egg, cod
or wheat when reported data was assessed by clinical examinations and
double-blind placebo-controlled food challenges. Allergy to milk, egg, cod
and wheat was an uncommon cause of complete avoidance of these foods
due to perceived hypersensitivity. Some of the analyzed biomarkers might
serve as prognostic markers for symptomatic, IgE-mediated food allergy but
need further validation.

v
Sammanfattning på svenska
Bakgrund
Födoämnesöverkänslighet håller på att bli ett stort och kostsamt
hälsoproblem i västvärlden. Prevalensen av rapporterad födoämnes-
överkänslighet bland barn ökar, men det är fortfarande oklart om detta
avspeglar en sann ökning i populationen. Det finns en stor spridning mellan
uppmätta prevalenstal i olika studier och i de få studier där man följt upp
rapporterade data med objektiva metoder ses en hög överrapportering.
Data saknas om reell prevalens av födoämnesöverkänslighet bland skolbarn i
Sverige. Befintliga prevalensdata baseras på rapporterad födoämnes-
överkänslighet och studier saknas där angiven födoämnesöverkänslighet i en
barnpopulationskohort validerats med objektiva metoder. Även om
dubbelblinda provokationer räknas som ”gold standard” används i praktiken
endast sjukhistoria, pricktest och analys av specifikt Immunoglubulin E
(IgE) samt öppna provokationer för diagnostik. Metoderna har flera felkällor
och mer tillförlitlig diagnostisk behövs, särskilt vid sena och svårtolkade
symtom. Korrekt diagnos är särskilt viktig när baslivsmedel har eliminerats
eftersom kostrestriktionerna riskerar att leda till negativa konsekvenser för
livskvalitet och intag av viktiga näringsämnen.
Syfte
Studierna i denna avhandling fokuserade på incidens och remission av
födoämnesöverkänslighet bland skolbarn i Norrbotten, som följdes från 7-8
år till 11-12 års ålder, och på prevalens av överkänslighet mot mjölk, ägg, fisk
och vete bland 12-åringar, undersökt med rapporterade data, klinisk
undersökning samt dubbelblinda placebokontrollerade födoämnes-
provokationer och biomarkörer.
Metod
Den huvudsakliga delen av det här projektet är baserat på en populations-
baserad kohort som rekryterades 2006 från 3 kommuner i norra Sverige.
Föräldrar till alla barn i klass 1 och 2 (7-8 år) bjöds in till ett frågeformulär,
som besvarades av 96% (n=2585) av de inbjudna. Barnen från två av
kommunerna, Luleå och Kiruna, bjöds också in till ett pricktest med 10
vanliga luftburna allergen och 90% (n=1700) av de inbjudna deltog. År 2010,
när barnen var 11-12 år, gjordes en studieuppföljning med samma metoder
och med ytterligare tillägg av en intervju med barnet och bestämning av
body mass index (BMI). Studiedeltagandet i enkäter och pricktest var lika
högt vid uppföljningen som vid studiestart.

vi
Vid studieuppföljningen bjöds barn med rapporterad mjölköverkänslighet in
till en strukturerad intervju och barn som helt undvek mjölk, ägg, fisk eller
vete på grund av upplevd överkänslighet, bjöds in till klinisk undersökning
och provtagning. Baserat på testresultaten kategoriserades barnen i olika
fenotyper av födoämnesöverkänslighet utifrån förutbestämda kriterier. Barn
som bedömdes ha en aktuell födoämnesallergi bjöds därefter in till vidare
utredning med dubbelblind placebokontrollerad födoämnes-provokation. De
recept som användes vid de dubbelblinda provokationerna hade
dessförinnan validerats avseende detekterbara smak- och konsistens-
skillnader mellan aktiv- och placebosubstans i en separat kohort av friska
skolbarn (n=275).
Före och efter den dubbelblinda provokationen samlades blodprover in för
analys av cytokin mRNA-uttryck i mononukleära celler. Analyserna
inkluderade cytokiner kännetecknande för humoralt allergidrivande T-
hjälpar 2 (Th2) svar, cellulärt cytotoxiskt drivande Th1 svar samt
inflammatoriskt- och T-reglerande svar. Vidare insamlades avföringsprover
för analys av inflammatoriska biomarkörer före och efter genomgången
provokationsserie.
Resultat
Prevalensen av föräldrarapporterad födoämnesöverkänslighet ökade från
21% vid 7-8 år till nästan 26% vid 11-12 års ålder. Incidensen av rapporterad
födoämnesöverkänslighet var hög (15%), liksom remissionen (33%).
Riskfaktorer associerade med incidens och remission var olika för mjölk-
överkänslighet och överkänslighet mot andra födoämnen. Vi såg också en
bristande samstämmighet mellan föräldrarapporterad överkänslighet mot
mjölk, ägg, fisk, vete, soja och jordnöt och IgE-sensibilisering mot det
aktuella födoämnet.
Vid 11-12 års ålder var prevalensen av rapporterad allergi mot mjölk, ägg,
fisk eller vete 4.8%, medan prevalensen baserad på klinisk undersökning och
provtagning var 1.4%. Prevalenssiffran halverades ytterligare när kliniskt
bedömd födoämnesallergi validerades med dubbelblinda placebo-
kontrollerade födoämnesprovokationer. Majoriteten av barnen med
rapporterad allergi mot mjölk, ägg, fisk eller vete klassificerades som andra
fenotyper av födoämnesöverkänslighet, varav de vanligast förekommande
var möjlig laktosintolerans (40%) och utläkt födoämnesallergi (19%).
Även om förekomsten av rapporterad mjölköverkänslighet bland 11-12
åringarna var så hög som 14.5%, kategoriserades bara 3% av dessa som en
aktuell mjölkallergi. Mjölkallergi, aktuell eller utläkt, var associerat med

vii
andra atopirelaterade tillstånd och ett lägre BMI (OR 0.82, 95% CI 0.80-
0.98) jämfört med barn som inte undvek mjölkprodukter.
Före den dubbelblinda provokationsserien var mRNA-uttrycket av den Th2-
relaterade cytokinen IL-13 och den regulatoriska cytokinen IL-10 högre
bland barn med provokationspåvisad födoämnesallergi jämfört med barn
med en negativ födoämnesprovokation. Såväl före som efter
provokationsserien kunde högre nivåer av inflammationsmarkörerna
eosinofil-deriverat neurotoxin (EDN) och kalprotektin uppmätas i
avföringsprover från barn med positivt provokationsutfall jämfört med barn
med negativ födoämnesprovokation. Skillnaderna i uppmätta nivåer av
biomarkörer i faeces uppnådde dock inte statistisk signifikans.
Slutsats
Rapporterad födoämnesöverkänslighet var vanligt förekommande bland
skolbarn i Norrbotten och ökade från 7-8 år till 11-12 års ålder. Incidensen av
rapporterad födoämnesöverkänslighet var hög, liksom remissionen.
Prevalensen av rapporterad allergi mot mjölk, ägg, fisk eller vete var 8
gånger högre än den prevalens som kunde påvisas med dubbelblind
placebokontrollerad födoämnesprovokation. Allergi mot mjölk, ägg, fisk och
vete var en ovanlig orsak till att barn helt undvek dessa födoämnen på grund
av upplevd överkänslighet. Några av de biomarkörer som analyserades innan
provokationsserierna visade lovande resultat som möjliga, framtida
prognostiska markörer för symptomatisk, IgE-medierad födoämnesallergi.
Dessa resultat behöver dock valideras med ytterligare studier.
viii
Abbrevations
BAT Basophil Activation Test
BMI Body Mass Index
CI Confidence Interval
DBPCFC Double-Blind Placebo-Controlled Food Challenge
EAACI European Academy of Allergology and Clinical Immunology
EDN Eosinophil-derived neurotoxin
ELISA Enzyme-Linked Immunosorbent Assay
EPX Eosinophilic cation protein X
FHS Food Hypersensitivity
FPIES Food Protein Induced Enterocolitis Syndrome
HBD2 Human Beta-Defensin 2
IgA Immunoglobulin A
IgE Immunoglobulin E
IgG Immunoglobulin G
IL- Interleukin
IFN-γ Interferon gamma
ISAAC International Study of Asthma and Allergy in Childhood
kU/L Kilo Units per Liter
MHC Major Histocompatibility Complex molecules
mRNA Messenger Ribonucleic Acid
OAS Oral Allergy Syndrome
OLIN Obstructive Lung Disease In Northern Sweden studies
OR Odds Ratio
PBMC Peripheral mononuclear blood cells
PUFA Polyunsaturated Fatty Acid
qRT-PCR Quantitative Real Time Polymerase Chain Reaction
SPT Skin Prick Test
Tc T-cytotoxic cell
Th T-helper cell
TGF-ß Transforming Growth Factor beta
tTGA Tissue Transglutaminase A
Treg T-regulatory cell
USA United States of America

ix
Original Papers
I Winberg A, Nordström L, Strinnholm Å, Nylander A, Jonsäll
A, Rönmark E, West CE. New validated recipes for double-
blind placebo-controlled low-dose food challenges. Pediatr
Allergy Immunol 2013;24:282-7.
II Winberg A, Strinnholm Å, Hedman L, West C.E,
Perzanowski M.S, Rönmark E. High incidence and remission
of reported food hypersensitivity in Swedish children followed
from 8 to 12 years of age – a population based cohort study.
Clin Transl Allergy 2014;4:32.
III Winberg A, West CE, Strinnholm Å, Nordström L, Hedman
L, Rönmark E. Assessment of Allergy to Milk, Egg, Cod, and
Wheat in Swedish Schoolchildren: A Population Based Cohort
Study. PLoS One. 2015;10(7):e0131804.
IV Winberg A, West CE, Strinnholm Å, Nordström L, Hedman
L, Rönmark E. Milk allergy is a minor cause of milk avoidance
due to perceived hypersensitivity among schoolchildren in
Northern Sweden. Acta Paediatr. 2015 Epub ahead of print
2015/11/01.
V Winberg A, Nagaeva O, Nagaev I, Lundell C, Arencibia I,
Mincheva-Nilsson L, Rönmark E, West CE. Dynamics of
cytokine mRNA expression and fecal biomarkers in school-
children undergoing a double-blind placebo-controlled food
challenge series. (In manuscript)
All published papers were reproduced with permission from the original
publishers. Paper II and paper IV are freely available (open acess).

x

1
Introduction
Personal point of departure
When I started working in pediatric Allergy around the millennium shift, one
of the greatest challenges in our clinic was the increasing number of children
reporting perceived food hypersensitivity. There was a lack of knowledge
about different types of food hypersensitivity, their underlying mechanisms
and the diagnostic tools available were insufficient. Much has happened
since then. Emerging interest and research in the area of food
hypersensitivity has broadened our understanding about the different
presentations of food hypersensitivity and how to manage this in the clinical
setting. Nevertheless, there is still a lack of knowledge about the prevalence
of hypersensitivity to different foods at different ages as well as the
prevalence of different phenotypes underlying reported food hypersensitivity
in children and adolescents. There is also a shortage of easily available
prognostic markers determining presence of tolerance.
Also, despite improved diagnostic methods, the number of children with
perceived food hypersensitivity seems to be continuously increasing. There
are data suggesting that this, at least partially, could be explained by a true
increase and changing patterns of food allergy, though there is still a lack of
available data on the prevalence, incidence and remission of food
hypersensitivity in Sweden as well as globally (1). This awoke the idea in our
pediatric allergy team to investigate the epidemiology of food
hypersensitivity among school children in Northern Sweden and for this we
joined the Obstructive Lung disease in Northern Sweden (OLIN) studies.
The extensive experience of population based epidemiological research
within the OLIN group made the project in this thesis possible.

2
Figure 1. Definition of food hypersensitivity (FHS).
(Modified from Johansson et al. Allergy 2001 (2) and printed with permission from
Wiley, Copyright © Munksgaard 2001)

3
Background
Definition of food hypersensitivity (FHS)
There is inconsistency in the terminology of food hypersensitivity (FHS). In
this work we have chosen to use the terminology stated in the World Allergy
Organization (WAO) position paper published in 2001 (2), where FHS is
defined as an umbrella term for adverse reactions to food including reactions
of both immunological origin i.e. allergies and reactions driven by non-
immunological mechanisms i.e. intolerances (Fig 1).
Allergies – can be either Immunoglobulin E (IgE) mediated or non-IgE
mediated. While the immunological mechanisms in IgE-mediated allergies
are well described (3) less is known about the causative mechanisms in non-
IgE mediated allergies, though T-cells seem to play important roles (4-6).
Intolerances – can be either enzymatic, pharmacological or driven by other,
still unknown mechanisms. The most common intolerances are caused by a
shortage of or a decreased function of an enzyme necessary for the digestion
of a component in food (4,7).
Prevalence of food hypersensitivity
Reported FHS has emerged as a costly health problem in Western countries
(8) affecting 3-35% of the population (9-11). The prevalence in different
studies is difficult to compare due to heterogeneity in methodology, study
populations and definitions of FHS. Most studies focus on the prevalence of
IgE-mediated food allergies.
Prevalence of food allergy
Food allergy is thought to affect nearly 8 % of young children and 5 % of
adults in Western countries (12) and there are data suggesting that the
prevalence is increasing (13). In a recent European study the pooled life-time
prevalence and point prevalence of reported food allergy was 17.9% and 5.6%
respectively (14). The prevalence of self-reported food allergy is usually
higher compared to challenge-proven allergy (9,15). In another recent
European meta-analysis, the prevalence of self-reported allergy to the 8
common foods: milk, egg, wheat, soy, fish, shellfish, peanuts and tree nuts
was 6.0% while the prevalence of challenge-proven allergy to these foods was

4
0.6%. In this meta-analysis, allergies to most foods except peanut and soy
were more common in Northern Europe (16).
Independent of geographic setting, 90% of IgE-mediated allergies in
children are elicited by eight foods; cow’s milk, soy, hen’s egg, peanut, tree
nuts, wheat, fish and shellfish (17). Milk, egg and peanut are the main
triggers in infants and young children (16,18,19), while peanut, tree nuts, fish
and shellfish are the main food allergy triggers in adults (16). The majority of
cow’s milk and hen’s egg allergic children develops tolerance during infancy
and early school age (20-22).
Allergies to peanuts and tree nuts are more likely to become permanent and
less than 20% become tolerant (23,24). Allergy to fish and shellfish can
emerge in early childhood, but more commonly at school age (5,16). In
addition, raw fruits and vegetables are common triggers of the oral allergy
syndrome (OAS) affecting more than 50% of individuals with birch pollen
allergy, which is common in the Swedish population (25). Population based
studies from the north of Sweden show a prevalence of IgE-sensitization to
birch among young adults of 23% (26) and 13% in children aged 7-8 years
(27).
While allergies to hen’s egg and cod are predominantly IgE-mediated, IgE
and non-IgE mediated allergy to cow’s milk is equally common as is
tolerance development in both of these conditions (15,28,29). In a recent
European study, 69% of children diagnosed with cow’s milk allergy at one
year of age had become tolerant by the age of 2 years (15). In this study,
children IgE-sensitized to cow’s milk were less prone to develop tolerance
compared to children with no detectable milk-specific IgE. Less is known
about the prevalence and natural development of non-IgE-mediated allergy
to other foods, like soy and cereals, but studies indicate that most of the
affected children develop symptoms during the first years of life and the
majority develop tolerance during childhood (4,6,22).
Prevalence of lactose intolerance
The most common variant of food intolerance is the adult-type lactose
intolerance, which is caused by down regulation of the intestinal enzyme
lactase resulting in a decreased capacity to digest lactose (30). The onset of
lactose intolerance symptoms most commonly begins during adolescence
and rarely before school age (7). The down regulation of lactase is caused by
a specific genotype that is common in most parts of the world, except in
Northern Europe, where the prevalence of lactase persistence is high (31).
The prevalence of lactose intolerance has not been well studied, neither

5
globally nor in Sweden (7). One Swedish study showed a higher-than-
expected prevalence of lactase down-regulation among Swedish school
children, the prevalence increasing from 8% to 14 % during a 10-year period
(32). Others have shown that over-reporting of lactose intolerance is
frequent even in populations in which lactase down-regulation is common
(33), suggesting that symptoms of lactose intolerance often are caused by
underlying mechanisms other than lactase down-regulation (34).
Factors associated with food hypersensitivity
A number of intrinsic and environmental factors have been associated with
reported food hypersensitivity. These include female sex, number of siblings,
allergic heredity, allergic sensitization and presence of atopy related
conditions like asthma, rhinitis and eczema (35-37). The prevalence of
reported food hypersensitivity also seems associated with age and native
country of the study population (10,14,38). Since the risk factors associated
with food hypersensitivity are related to the background mechanisms of the
different types of food hypersensitivity, risk factors will be discussed
separately for food allergy and lactose intolerance.
In conclusion:
Food hypersensitivity (FHS) is common in children as well as in
adults, though the prevalence varies. This is likely due to the use
of different study methods, age and origin of the study
population and the definition of FHS. Most studies focus on IgE-
mediated allergies, which affect around 8% of young children
and 5% of adults in Western countries and the prevalence of
food allergy seems to be increasing. The prevalence of reported
food allergy exceeds the prevalence of allergy established by an
oral challenge.

6
Risk factors of food allergy
Food allergy is a polygenic, complex disease in which the risk of developing
symptoms seems to depend on a number of genetic and environmental
factors (39). The strong relationship between allergic heredity and
development of food allergy is a compelling evidence of the contribution of
genetic factors in this disease (39,40). Nevertheless, the specific genetic loci,
which modulates food allergy remains to be identified (41) as does the roles
of gene-environment interaction, gene-gene interaction and epigenetics (39).
Most studies investigating risk factors of food allergy are focusing on IgE-
mediated allergies and early life environmental exposures, given their
possibility to modulate developing immune responses and tolerance (42)
and being plausibly modifiable. Since the introduction and extension of the
hygiene hypothesis (43), these possible early modulating factors include
exposures affecting gut microbial composition and diversity: such as family
size and place of upbringing (44,45), early infections (46,47), delivery mode
(48), use of antibiotics, breast feeding and pre- and probiotics (49,50). In
addition, many studies have investigated dietary components as vitamin D
(51,52) and polyunsaturated fatty acids (PUFA) (53) as modifiers of allergy
development.
Still, there are many questions in the search of the origin of food allergies.
Recent data suggest that early introduction of allergenic foods in a child’s
diet can steer the immune system towards tolerance development (54,55)
while a route of IgE-sensitization through a disrupted skin barrier might do
the opposite (56). Childhood eczema is a risk factor associated with
development as well as persistence of food allergy (36,57,58). In addition,
food allergies often co-exist with other atopy related conditions like asthma,
rhinitis and allergic sensitization, which suggests that these conditions may
have common risk factors (12,59,60).
Low-level IgE-sensitization and IgE-sensitization to one or a few food
allergens may predict remission of a food allergy, while multi-sensitization
and high levels of specific IgE is associated with development and
persistence of food allergy symptoms (20,23,61). As discussed above, food
allergy in children is strongly associated with allergies and atopic diseases in
their parents (59). Except for genetic factors, other variables that could affect
this association are exposure patterns including allergen avoidance in
families at risk of having a food allergic child and report bias (39,63,64).

7
Some of the differences in the prevalence of food allergy between
populations have been related to race. Studies from the USA have shown a
higher risk of IgE-sensitization to common food allergens and higher levels
of IgE-sensitization in children with self-reported black race and/or African
ancestry compared to Hispanic or Caucasian children (65). Further, the
prevalence of food allergy may be affected by sex (58,63). Even though food
allergies and allergic sensitization are more common among boys than girls
(59) there is a shift during adolescence making food allergies more common
among women (37,66). The reason for this shift is still unknown, though
contribution of hormonal factors has been suggested (67).
Similar to IgE-mediated allergies, non-IgE mediated food allergies are
thought to emerge from a failed immunological tolerance development (68).
However, the risk factors specifically related to non-IgE mediated food
allergies are currently un-explored (64).
Risk factors of lactose intolerance
As in non-IgE mediated food allergies, there is a lack of studies investigating
the risk factors of lactose intolerance (7). Since lactose intolerance is caused
by a genotype coding for down-regulation of the intestinal enzyme lactase
and different mutations of the lactase down-regulating gene are more or less
prone to cause symptoms (69), the occurrence of this condition is strongly
associated with heredity. Notably, large differences in the prevalence of
lactose intolerance have been found between populations (30,70).
In most cases, symptoms of lactose malabsorbtion develop successively
during adolescence making lactose intolerance uncommon in younger
children (71). Even though the distribution of the lactase down-regulating
genotypes is similar among men and women, symptoms of lactose
intolerance are more frequently reported by women than men (70,72).

8
Immunological aspects of food allergy and tolerance development
Food allergy is a general term for adverse immunological reactions to food
and includes a number of different disease phenotypes (4,5). A food allergy
can be IgE-mediated, non-IgE mediated or a combination of the two. Even
though the underlying immunological mechanisms are diverse, and in the
case of non-IgE mediated food allergies largely unknown, they are all
thought to emanate from failed or abrogated tolerance, which involve an
aberrant regulatory T-lymphocyte response (73).
The development of tolerance normally occurs in the immune system of the
gut (74). Even though most of our knowledge about tolerance emanates from
animal studies, the reigning current paradigm is that the interaction between
the gut microbiota, the immune cells of the gut and exposure of food
allergens through an oral route are essential for a successful tolerance
development also in humans (49).
In conclusion:
Factors including sex, race, allergic heredity and atopy related
diseases e.g. eczema, asthma and rhinitis have been associated with
reported food hypersensitivity. Most studies on risk factors of food
hypersensitivity focus on IgE-mediated allergy, which is a polygenic,
complex disease dependent on a number of genetic and environmental
factors. Many uncertainties remain regarding risk factors of food
allergy, though early introduction of “allergenic” foods seem to steer
the immune system towards tolerance development, while
sensitization through a disrupted skin barrier might do the opposite.
Risk factors of non-IgE mediated allergies and lactose intolerance are
yet to be explored.

9
T-lymphocytes have been given their designation letter because they mature
in the thymus (75). There are three subpopulations of T-cells: T-helper cells
(Th), T-cytotoxic cells (Tc) and T-regulatory cells (Treg). Following
recognition of cell membrane bound antigens called major
histocompatibility complex molecules (MHC), Th-cells differentiate into
effector cells that enhance the activation of various other cells that
participates in the immune response e.g. B-cells, Tc-cells and macrophages.
Alternatively, some Th-cells differentiate into memory cells (76). The
immune environment of cytokine and chemokine signaling steers the
differentiation of Th-cells into different subsets (77). The first two subsets
discovered were Th1 and Th2. A predominate Th1-activation is associated
with autoimmunity while a dominant Th2-response relates to IgE-mediated
allergy (78).
In recent years a number of additional Th-subsets have been discovered,
including Th3 and Th17, contributing to the complexness of immune
response patterns (73,79). Th17 cells are involved in autoimmunity and has
also been suggested a role in neutrophilic asthma (80), whereas Th3 cells are
part of T-regulatory cells. T-regulatory cells can suppress the immune
response, either by cell to cell contact and/or by the production of down-
regulatory cytokines (81,82). T-regulatory cells include CD4+CD25+ T-
regulatory (Treg) cells, inducing suppressive effects via cell contact and type
1 regulatory (Tr1) cells and Th3 cells mediating their effects via cytokines e.g.
interleukin 10 (IL-10) and transforming growth factor beta (TGF-β) (83).
Treg cells are thymus-derived and express CD25 (the IL-2 receptor) and the
transcription factor FoxP3. The suppressor function of Treg cells appear to
depend in part on TGF-β, but less on IL-10 (84). Th3 cells are gut derived
and characterized by production of TGF-β (+ IL-10), exerting their effects by
mediating mucosal tolerance and antigen-specific IgA production (85). Tr1
cells are derived from the periphery and have the capacity to produce IL-10.
However, their origin is unclear and as of yet it is not known whether they
represent a distinctive developmental pathway or are derived from Th or
Treg cells (86).
IgE-mediated food allergy
The allergic process starts with exposure of an allergen to the immune
system, in food allergy usually via the intestinal mucosa (87,88). In the
surface of the mucosa, dendritic cells can sample luminal allergens and
present them to naïve T-cells in nearby lymph nodes (88). An environment
of Th2-related cytokines and chemokines facilitates clonal expansion and
differentiation of the naïve T-cells into Th2 subsets and memory cells.

10
Further, some of the encountered food allergens are transferred and
presented to B-cells, triggering them to mature into plasma cells, that
subsequently produce and secrete allergen specific IgE. This process is called
allergic sensitization (87,89) (Figure 2).
Re-exposure to the food allergen leads to allergen binding to circulating and
cell surface bound specific IgE-antibodies. Cross-linking of IgE on the
surfaces of mast cells and basophils can, under the right circumstances, lead
to release of inflammatory mediators e.g. histamine and tryptase, capable of
triggering an allergic response. Partly due to cross-binding IgG4-antibodies
and cross-reactivity between allergens, IgE-sensitization to food allergens is
far more common than food allergy (90, 91).
Figure 2. Schematic illustration of allergic sensitization resulting in
circulating and receptor-bound food antigen specific IgE-antibodies.
11
Non-IgE-mediated and mixed-immune food allergies
Less is known about the background mechanisms resulting in a non-IgE
mediated food allergy (6). The non-IgE mediated food allergies are a
heterogeneous group of diseases thought to be driven by cell–mediated
immunity that can be separated into different phenotypes following
improved methods of clinical investigation including increased use of
endoscopy. These phenotypes include: food protein induced reflux,
eosinophilic esophagitis, eosinophilic gastroenteritis and colitis and food
protein induced proctitis (6,89). Non-IgE mediated food allergies often
comprise symptoms from the gastrointestinal tract (92) and in some of these
conditions signs of inflammation and disrupted cytokine responses have
been detected in the local intestinal mucosa (93).
In recent years, it has been shown that in some food allergic diseases, IgE
and non-IgE mechanisms can co-occur. In these conditions, T-cell mediated
mechanisms are thought to cause a disrupted barrier in the skin or gastro-
intestinal mucosa and thereby facilitate allergic sensitization (94). Examples
of these mixed immune food allergies are eosinophilic gastrointestinal
diseases e.g. eosinophilic esophagitis and atopic dermatitis. Much is yet to be
discovered about these complex diseases (64).
Cytokine patterns in tolerance development and IgE-mediated
food allergy
Cytokines are mediators and communicators of the immune system, steering
the immunological responses to antigens in predisposed directions (95,96).
Food allergens are mainly presented to the immune system in the gut where
interactions between the gut microbiota and T-regulatory cells induce a
tolerogenic IL-10/TGF-ß response that appears essential for tolerance
development (49,97,98). IL-10 is a major regulatory cytokine of
inflammatory responses (99) that inhibits the production of IgE and
upregulates the secretion of IgG4 (100) and seems to play a critical role in
tolerance development and outgrowth of food allergy (101-103). In addition,
the cytokine TGF-ß has been shown to enhance tolerance development by
down-regulation of the immune system e.g. by inhibiting proliferation of T-
cells and activation of macrophages (104). IL-10 and TGF-ß gene
polymorphisms are associated with persistent milk allergy in children (105).
Similarly to children with IgE-associated asthma and eczema, children with
IgE-mediated food allergy have a cytokine response pattern with increased
expression of Th2-related cytokines e.g. IL-4, IL-5 and IL-13 and reduced

12
production of the Th1-related cytokine interferon gamma (IFN-γ) (106). This
dysregulated cytokine response is usually present already at a very young age
(107, 108). Th2-associated cytokine patterns have even been detected in cord
blood from children who eventually developed food allergy (109). Following
stimulation with relevant food allergens, elevated levels of pro-inflammatory
cytokines e.g. IL-6 have been detected in challenge-proven milk and egg
allergic children compared to children who had developed tolerance to these
foods, indicating an inflammatory response triggered by the food allergen in
children with persistent allergy (110).
Allergic inflammation in the intestinal mucosa
The majority of children with food allergy have at least one symptom from
the gastrointestinal tract, which comports with the common route of food
allergen exposure (92). In gastrointestinal allergies signs of allergic
inflammation can often be detected where the vulnerable intestinal mucosa
has been exposed to the culprit food allergen. By examining mucosal
biopsies, a skilled pathologist can distinguish eosinophilic inflammation
caused by food allergy from other inflammatory diseases of the gut e.g.
gastroesophageal reflux and celiac disease (6,92). The increased use of
endoscopy in food allergy diagnosis opens up the possibility of measuring
cytokines and other biomarkers at the site of the allergic inflammation
(6,111). In addition, decomposing products emanating from an allergic
inflammation in the intestinal mucosa may be detected in stool samples from
food allergic children (112).
In conclusion:
Food allergy is a general term for a heterogeneous group of disease
phenotypes resulting from immunological reactions to food with failed
or abrogated tolerance and aberrant regulatory T-cell response as
common nominators. Cytokines are mediators and communicators of
immunological responses. From very early life, dysregulated cytokine
patterns can be detected in children eventually developing IgE-
mediated food allergies.

13
Symptoms of food allergy
Food allergy can cause a broad palette of symptoms and many food allergic
children develop symptoms from more than one organ system (5). The most
common locations for food allergy symptoms are the skin and the
gastrointestinal tract including the oral mucosa (36). Symptoms of food
allergy can occur within minutes of allergen exposure or require repeated
exposures over time to be elicited. In addition, food allergy mostly causes
benign symptoms but it can also be a life-threatening disease (3,113).
To further complicate the management and diagnostics of food allergies, the
liability to develop symptoms may differ in the same individual due to co-
factors like infections, drugs, simultaneous exposure to other allergens and
physical activity (114,115). Even though symptoms caused by different types
of food allergies may be confusingly similar, there are some reaction patterns
and combination of symptoms that may help in the differential diagnostics
(116).
Symptoms of IgE-mediated food allergy
The first symptoms of an IgE-mediated allergy classically occur within 2
hours of exposure and often within minutes (5). As a result, IgE-mediated
allergies are also called immediate-type allergies. In some cases, the IgE-
mediated food reaction may be biphasic with a symptom relapse within 1-6
hours and in rare cases within days of allergen exposure (91).
Symptoms associated with IgE-mediated food allergies are rapidly emerging
itching of the mouth, vomiting, urticaria, angioedema and symptoms from
the airways (5,94). IgE-mediated food allergies are also strongly associated
with acute life-threatening anaphylaxis, which comprises airway and/or
cardiovascular symptoms (117). However, even though food allergies are
common triggers of anaphylactic reactions in childhood, these reactions can
also be triggered by mechanisms other than IgE-sensitization (118).
Following IgE-sensitization to tree or grass pollens, birch pollen in
particular, the pollen-specific IgE-antibodies may bind to other proteins
similar to the original allergen occurring in numerous plants and vegetables
(119). The majority of these pollen cross-reactive IgE-sensitizations do not
cause clinical symptoms (120). Risk factors for symptom development are
clinically relevant pollen IgE-sensitizations and IgE-sensitization to multiple
pollens. This secondary type of IgE-mediated food allergy is called oral
allergy syndrome (OAS) or pollen-associated food allergy syndrome (94).

14
The clinical symptoms of this condition are usually limited to itching and
sometimes erythema of the oral mucosa shortly following allergen exposure.
Except for some rare conditions, symptoms of OAS are usually local and
benign. The oral symptoms may however be confused with oral symptoms as
a first sign of a primary IgE-mediated food allergy (5).
Symptoms of non-IgE mediated and mixed-immune food
allergies
The most common symptoms of a non-IgE mediated food allergy are skin
and/or gastrointestinal symptoms occurring hours and sometimes days after
allergen exposure (6,92). These symptoms are also common in mixed-
immune food allergies, though symptom onset may be quicker due to the IgE
component (94). The symptoms of non-IgE mediated and mixed immune
food allergies e.g. eczema, diarrhea, malabsorption, feeding difficulties and
failure to thrive are usually not as typically associated to food allergy as the
symptoms of an IgE-mediated allergy (5,94). Together with the late onset
symptoms, these non-specific symptom patterns often lead to a delayed
diagnosis (6,64).
During recent years, we have learned that food allergies affecting the gut can
be sorted into different phenotypes according to their location and/or
distinct symptom patterns (6). Examples of such gastrointestinal food allergy
phenotypes are: food-induced reflux, eosinophilic esophagitis, eosinophilic
enterocolitis or food induced proctitis, the latter strictly limited to the most
distal part of the colon resulting in blood-tinged stools in an otherwise
unaffected infant (6, 94).
As in IgE-mediated food allergies, the non-IgE and mixed immune food
allergies contain a broad variety of disease severity, ranging from mild
eczema to a potentially life-threatening disease (92). The food protein
induced enterocolitis syndrome (FPIES) is a non-IgE mediated food allergy
resulting in dramatic symptoms including profuse repeated vomiting, pallor
and apathy and in some cases hypovolemic shock. The symptoms of FPIES,
that usually occur 1-4 hours following allergen exposure, are often
misinterpreted as caused by other acute onset diseases like septicemia,
meningitis, severe gastroenteritis or an acute gastrointestinal event (121).

15
Establishing a food allergy diagnosis
Diagnosing food allergy is a challenge, in every meaning of the word
(64,116). There is a broad variety in symptoms, severity and background
mechanisms of food allergy. This, together with insufficient diagnostic tools,
means that investigation of a suspected food allergy requires knowledge of
the different disease phenotypes, potential differential diagnoses as well as
the possibilities and limitations of the tests available (122,123). To date, the
most reliable method to diagnose or rule out a suspected food allergy is to
perform an oral food challenge and the double-blind placebo-controlled food
challenge is considered gold standard (5,116,123).
Clinical history
Even though it cannot be used as a solitary tool for food allergy diagnostics, a
thorough clinical history can often narrow down the area of search to a few
differential diagnoses and be helpful in the choice of proper diagnostic
methods (5,116,123). A clinical history for food allergy diagnostics should
include: possible food triggers, type and severity of symptoms, time to onset
and duration of symptoms after allergen exposure, extrinsic co-factors, age
of onset, allergic heredity, other atopy related diseases, growth deviation and
eating habits of the child (5,116).
In conclusion:
There is a broad variety in symptoms and severity of food allergy,
ranging from local benign symptoms to life-threatening anaphylaxis.
Most food allergic children have symptoms from more than one organ
system, of which the skin and gastrointestinal tract are the most
common. IgE-mediated food allergies are usually characterized by
immediate onset reactions while non-IgE mediated food allergies
usually occur hours and sometimes days following allergen exposure.

16
Recently, a standardized diet history tool has been developed and published
in order to support the diagnosis of food allergy (124).
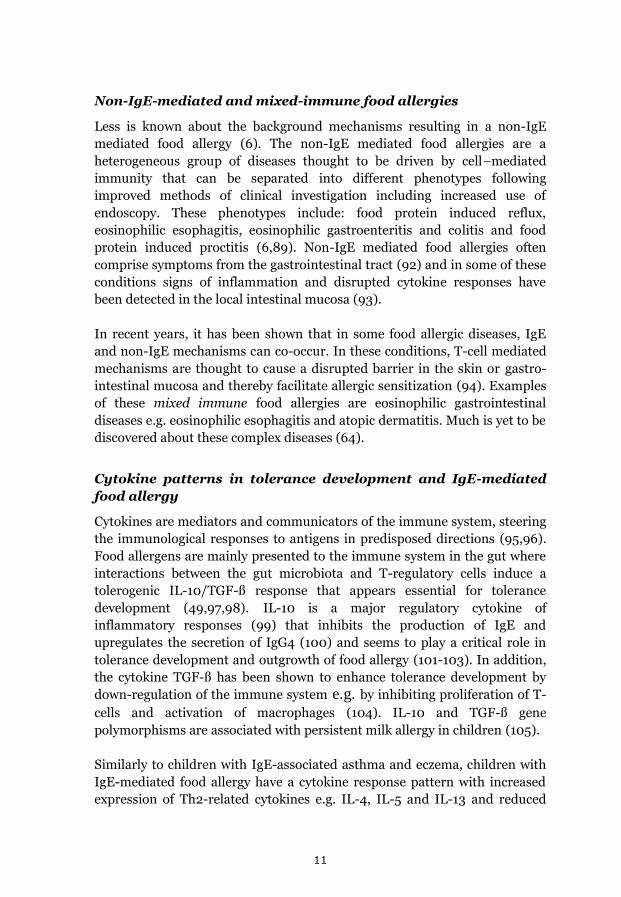
IgE-tests
The most common laboratory tests in allergy diagnostics are measurement of
allergen specific IgE in patient sera and skin prick tests (SPT), measuring the
reaction of allergen specific IgE clad mast cells in the subcutaneous tissue
when exposed to allergen through a disrupted skin barrier (90,125) (Figure
3). Both of these tests demonstrate IgE-sensitization and not allergy, which
also requires the presence of symptoms upon allergen exposure (5,126).
In population-based studies a relationship can be seen between the level of
IgE-sensitization and the presence of allergic symptoms following allergen
exposure (127). Due to the lack of reliable tests of individual tolerance and
diverse allergenic properties in commercially available allergens, there are
no valid cut-off levels of specific IgE that guarantee or exclude food allergy
(128,129). Nor can the level of specific IgE be used for determining the
disease severity (113). Since these tests measure IgE-sensitization, the results
must always be interpreted in light of the clinical history (5) and the tests are
consequently of no use in diagnosing a non-IgE mediated food allergy (6).
The first generation of IgE-assays was based on crude allergen extracts
derived from natural sources, including both allergenic and non-allergenic
compounds (90). Today, many allergenic molecules have been identified and
by the use of recombinant DNA technology allowing cloning and large-scale
production of recombinant allergens, component-resolved analyses of
molecular allergens are now available for a number of food allergens
(126,130). This new technique has improved the sensitivity and specificity of
the IgE-assay, among other things it helps in differentiating cross-reactions
from true IgE-sensitization (126). However, even though component
resolved diagnosis allows a more individualized IgE-testing, a thorough
clinical history is still essential for its interpretation (131).
17
Oral food challenges
In some cases of food allergy, such as severe immediate onset allergy to a
single food trigger, the allergy diagnosis can be based on the clinical history
in combination with a concordant IgE-test (132). In most cases of food
allergy, however, the clinical history and the results of skin prick tests or
serological analyses are not as clear-cut. In these cases further evaluation of
the suspected food allergy is needed and the recommended method is the use
of a diagnostic elimination diet followed by an oral challenge (5,116).
Figure 3. Schematic illustration of IgE-tests: 1. Measurement of free
circulating food allergen specific IgE-antibodies in patient sera and 2. Skin
prick test measuring the effects of mast cell degranulation in the subcutaneous
tissue following allergen exposure through a disrupted skin barrier.

18
Most commonly when performing a diagnostic food elimination, a single
suspected food allergen is eliminated from the child’s diet over a limited
period of time. The duration of the food elimination is determined by the
type and severity of symptoms, though an elimination period of 2-4 weeks is
usually sufficient (116,132). Even if the child’s symptoms resolve during the
elimination period, a food allergy diagnosis cannot be established until a
food challenge has been performed, resulting in recurrence of symptoms
(116,123,132).
In most cases of food allergy where the food-induced symptoms are benign,
the diagnostic food challenge can be performed at home. However, if the
parents are not properly instructed and motivated the diagnostic
elimination/provocation test is often not completed and the child remains on
an elimination diet (133). Therefore, the advice on food elimination should
always be evaluated (132). Children with severe food allergic reactions
should be followed by a pediatrician and food challenges, when appropriate,
should be performed in a hospital setting (5,116).
Open challenges
Open challenges are most commonly used in clinical practice. Without
blinding and the use of placebo the open challenge is easier to perform and
less time consuming. It is, however, limited by the chance of bias, which may
result in falsely positive outcomes (116,134). The risk of false positive results
is highest if the patient is anxious about the challenge and if the patient’s
previous symptoms have been late onset and/or subjective (132).
During a food challenge the food is introduced in gradually increasing doses,
usually aiming at a final dose close to a portion size of the challenge food. In
most cases a standardized challenge schedule is used, though the food
amounts and dose intervals might need to be adjusted according to the
severity and eliciting doses of previous reactions (5,123).
Blinded challenges
In a single-blinded challenge the serving of challenge food or placebo is
blinded to the patient but not to the personnel responsible for the testing.
This procedure might reduce the risk of bias on the part of the patient, but
can still affect the observer in the interpretation of the challenge outcome
(132,135).

19
Therefore, the double-blind placebo-controlled food challenge (DBPCFC) is
considered gold standard in diagnosing food allergy and it is the preferred
method for research protocols (5,116,135). Double-blind challenges reduce
the patient and observer bias to a minimum and is particularly useful in
diagnosing or ruling out adverse reactions to food presenting with delayed,
chronic or subjective symptoms (132,136).
However, since the DBPCFC is time and labor consuming it is rarely used in
daily clinical practice (116). Also, even though several elaborate guidelines
have been published during recent years the procedure of DBPCFC has not
yet been fully standardized and there is still a lack of validated DBPCFC
recipes (114,136).
Complementary diagnostic tests and future prognostic biomarkers
The discovery of new food allergy phenotypes brings about the need of new
diagnostic methods (64). Some old diagnostic methods are being tested for
new and more specific purposes and new diagnostic methods are being
developed following deeper understanding of the background mechanisms of
food allergy (126,138). Also, since DBPCFCs are time and labor consuming
and puts the patient at risk of an allergic reaction, there is an ongoing search
for easily available objective prognostic markers that would make double-
blind challenges superfluous (131).
In conclusion:
Even though a thorough clinical history and the easily available IgE-tests
might be helpful, they are usually not sufficient to diagnose or rule out a
food allergy. An oral challenge is usually necessary to establish a food
allergy diagnosis and the double-blind placebo-controlled food challenge
(DBPCFC) is considered gold standard. Since DBPCFCs are costly and
time consuming they are rarely used in daily clinical practice. Also, the
procedure of DBPCFC has not yet been fully standardized and there is still
a lack of validated DBPCFC-recipes.

20
Endoscopy
Since many years endoscopy has been used to diagnose inflammatory
diseases in the gastrointestinal tract. The possibility to take biopsies and
visualize the site of inflammation has contributed to the understanding of
different phenotypes of gastrointestinal allergies, their distribution and
immunological mechanisms (92,111). For some types of food allergy i.e.
eosinophilic esophagitis, endoscopy is essential for the diagnosis (137). In
the future, endoscopy will probably be more commonly used for
measurement of diagnostic markers on site (6,64,122,138).
However, diagnosis by endoscopic methods are invasive and especially for
children, not easily available. Establishing a food allergy diagnosis through
biopsies from the intestinal mucosa also requires access to experienced
pathologists. So far, the fairly extensive resources necessary for endoscopic
investigations has limited its use to the larger University hospitals (6,92).
Inflammatory and regulatory makers in faeces
Using endoscopic methods, signs of allergic inflammation can often be
detected where the vulnerable intestinal mucosa has been exposed to the
culprit food allergen (111). A less invasive upcoming diagnostic method is to
determine decomposing products from an intestinal allergic inflammation by
analyzing stool samples (112). Previous studies have shown that eosinophils
are activated in food allergic intestinal inflammation (139) and that
eosinophil-derived neurotoxion (EDN) also known as eosinophilic protein X
(EPX), one of the major proteins released by eosinophils, might be used as a
marker of food allergic reactions (139,140).
It has also been shown that measurement of the cytosolic,
immunomodulatory protein calprotectin in faeces can be a helpful tool in the
follow-up of response to treatment and determination of reoccurrence of
cow’s milk allergy (141). In addition, the antibiotic peptide human beta-
defensin 2 (HBD2) and secretory IgA have been investigated in stool samples
as possible markers of food-induced inflammation and tolerance in the gut
mucosa (142,143).
Atopy patch tests
Patch tests are commonly used to identify delayed-type immune reactions to
allergens (138). In a patch test the allergen is placed in a small chamber,
which is then applied to the skin of the patient for 48 hours. The test reaction
is measured after 48 and 72 hours respectively.

21
In atopy patch testing, the same method is performed using food antigens,
usually fresh foods (144). Atopy patch testing was first used in studies of
patients with eczema, where it was found to be a useful tool in diagnosing
food allergy (145). The test has also been shown to be helpful in identifying
food triggers in children with gastrointestinal allergy i.e. FPIES and
eosinophilic esophagitis (146,147). Nevertheless, the roles of atopy patch
testing in food allergy diagnosis is conflicting and large-scale clinical studies
are lacking. Also, the use of fresh foods as allergen extracts in patch testing
has not been standardized and neither has the method of reading the test
results, making it dependent on the skills of the investigator (148).
Serological tests
As previously discussed, the available tests measuring specific IgE to
allergenic molecules in foods are rapidly increasing (126). Studies of patients
allergic to nuts and peanuts have showed that IgE-sensitization to storage
proteins more often correlate to the presence of allergy symptoms, while
cross-sensitizations to pollen allergens are usually asymptomatic or causes
local, benign symptoms (120). With a more widespread availability, the use
of molecular allergen analyses to determine the relevance of food
sensitization will probably increase, as will our understanding of the
relationships between food allergen IgE-sensitization and symptoms (149).
The occurrence of food-specific IgG is thought to indicate previous exposure
to the food and the presence of tolerance, though the role of specific IgG in
the mechanism of tolerance development is not yet fully understood (88).
During oral and sublingual desensitization therapy, clinical improvement
has been associated with a decrease in specific IgE and an increase in
allergen specific IgG4 (150). In addition, specific IgG4 has been shown to
inhibit peanut-induced basophil and mast cell activation in children that are
sensitized but clinically tolerant to major peanut allergens (151). However,
the level of increased specific IgG4 does not correlate well with the degree of
improvement or severity of the allergic disease which limits the use of
specific IgG4 as a sole marker of tolerance development (5).
In addition to being detectable in stool samples, the immunomodulatory
protein calprotectin can also be measured in sera. Calprotectin is a cursor of
neutrophil inflammation and elevated serum calprotectin levels have been
shown to be a useful marker of some rheumatic diseases (152). Recently it
has also been suggested as a possible biomarker of neonatal sepsis (153). To
our knowledge, no studies have so far been published investigating the levels
of serum calprotectin in children with suspected food allergy.

22
Basophil activation tests
In cellular allergy testing, an allergic response is induced in vitro (126). The
most common cellular allergy test is the basophil activation test (BAT), an
upcoming tool for the diagnosis of IgE-mediated food allergy (154,155).
During a BAT, allergen-induced changes in the expression of proteins on the
surface of basophils are detected using flow cytometry (126). Studies have
shown that BAT might be superior to IgE-tests and clinical history in
distinguishing a symptomatic peanut allergy from tolerance, especially in
ambiguous cases (156,157). The BAT has also been shown to complement
more established allergy tests in improving the diagnostic sensitivity (158).
In addition, measurement of basophilic sensitivity as activation at graded
dilutions of allergens (CD-sens) offers the possibility of monitoring
treatment with anti-IgE and oral tolerance induction in children with severe
food allergy (154,159). Up to now performing BATs requires a fairly rapid
and costly processing of the collected samples and expertise in performing
and interpreting the tests. Increased availability and standardization of
methods are necessary for a more wide-spread use of BATs (155).
In conclusion:
New diagnostic test and prognostic markers are emerging, hopefully
facilitating future food allergy diagnostics. Analyses of IgE-sensitization
to molecular allergens and cellular allergen tests appear promising in
improving the diagnosis of symptomatic IgE-mediated allergies while
an increased use of endoscopy brings about the possibility of sampling
diagnostic markers on the site of inflammation. In addition,
decomposing products emanating from local allergic inflammation in
the intestinal mucosa may be detectable in stool samples from food
allergic children.

23
Cytokines
Food allergic children have a cytokine response pattern with increased
expression of Th2-related cytokines e.g. IL-4, IL-5 and IL-13 and reduced
production of the Th1-related cytokine IFN-γ (106,110,160). These, and other
cytokines including the regulatory cytokine IL-10, have been examined as
possible prognostic markers using in vitro stimulation of peripheral blood
mononuclear cells (PBMC) with relevant food allergens and more seldom in
vivo with oral food challenges (103,161,162).
After stimulation of PBMCs with specific food allergens, the expression of
the Th2 cytokine pattern is enhanced and the expressed levels of the
regulatory cytokine IL-10 diminished in children with symptomatic IgE-
mediated allergy compared to tolerant children (107,161). Due to its active
role in tolerance development, IL-10 has been discussed as a possible
biomarker for symptomatic IgE-mediated food allergy (101) and so has the
Th2-related cytokine IL-13 (163,164).
In conclusion:
Following stimulation with relevant food allergens, decreased
expression of regulatory cytokines and increased levels of Th2-related
and pro-inflammatory cytokines have been detected in blood samples
from children with symptomatic food allergy compared to tolerant
children. Some cytokines, including the regulatory cytokine IL-10 and
the Th2-related cytokine IL-13 have been suggested as possible
prognostic markers of a symptomatic IgE-mediated food allergy.

24

25
Objectives
The main objective of the project in this thesis was to examine the clinical
epidemiology of food hypersensitivity in a population-based cohort of
schoolchildren in Northern Sweden followed from age 7-8 to 11-12 years of
age.
The specific aims were:
- To validate new recipes for double-blind placebo-controlled
challenges with cow’s milk, hen’s egg, soy, cod and wheat (Paper I).
- To investigate the incidence and remission of parentally reported
food hypersensitivity in a population based cohort followed from 8
to 12 years of age (Paper II).
- To assess the prevalence of allergy to cow’s milk, hen’s egg, cod and
wheat among 11-12-year old Swedish children using reported data,
clinical investigations and double-blind placebo-controlled food
challenges (Paper III).
- To describe the food hypersensitivity phenotypes among Swedish 11-
12-year old children reporting hypersensitivity to cow’s milk and to
analyze how the different phenotypes correlated to body mass index
(BMI), living conditions, allergic sensitization, allergic heredity and
physician diagnosed asthma, rhinitis and eczema (Paper IV).
- To investigate the spontaneous cytokine mRNA expression in
peripheral mononuclear cells from children with possible food
allergy and healthy controls before and after a double-blind placebo-
controlled food challenge series. Also, to investigate inflammatory
markers in stool samples from children with possible food allergy
before and after the completed food challenge and in relation to the
challenge outcome (Paper V).

26
27
Materials and methods
The first part of this study emanated from a clinical need of improving the
methods for diagnosing or ruling out food allergy in our pediatric patients.
At the time of the study, there were very few validated recipes for DBPCFC.
To allow a wider spread of our developed recipes for double-blind challenges
with the foods; cow’s milk, hen’s egg, soy, cod and wheat and to be able to
use them in research protocols, we decided to perform a study with the aim
of validating these recipes.
1. Method: Paper I
Study population
Whole school classes in the town of Umeå were invited to participate in our
test panels. Apart from validating our DBPCFC recipes we also wanted to
investigate whether the taste and texture of the challenge substances were
acceptable for children of different ages. We therefore invited children from
two different age groups; classes 2 and 3 (8-10 years of age) and class 8 (14-
15 years of age). Children were excluded from the study if they had a
hypersensitivity to the food that was tested.
We aimed to invite around 50 children in each age group (165). During the
study, the recipes for milk and wheat had to be improved due to detectable
differences between the active and placebo substances. New school classes
were thus invited as test panels for the sensorial testing of the improved milk
and wheat DBPCFC recipes. In all, 275 children (81 % of invited) participated
in the testing of at least one DBPCFC recipe.
Sensorial testing
Triangle tests were used for the sensorial testing (165,166). In a Triangle test
the panelists are served three samples in coded covered mugs/canisters with
a straw, whereof two samples are identical and one is odd (Figure 4). The
task of the panelists is to pick out the odd sample. The Triangle test is a
forced-choice procedure, meaning that the test panelist has to choose a
sample whether or not a perceivable difference is detected (165).

28
Statistical analysis
To determine whether there was a statistically significant detectable
difference between our active and placebo substances the numbers of correct
responses were calculated and compared to the total number of participants.
Further, p-values were calculated with a standard binomial distribution and
a p-value <0.05 was considered statistically significant. One-sided testing
was used, since the outcome of interest was whether the odd sample could be
detected with significant frequency. The minimum numbers of correct
responses to conclude a difference were calculated according to the formula:
[x= (n/3) +1.64√ (2n/9)] (165).
Figure 4. Arrangement of covered, coded cups with test substances and a
worksheet for the performance of a Triangle test.

29
Method: The OLIN studies
The four remaining papers in this thesis are the results from a collaboration
project between the Department of Clinical Sciences, Pediatrics, Umeå
University and the Obstructive Lung disease In Northern Sweden (OLIN)
studies. For 30 years, the OLIN-studies have pursued epidemiological,
population based research with focus on obstructive lung disease and
allergies in adults and children in Norrbotten, in the north of Sweden and
the studies has so far resulted in more than 250 original scientific papers and
14 doctoral theses.
Study population
This project is based on the second pediatric OLIN cohort recruited in 2006.
When recruited, the cohort consisted of all children in classes 1 and 2 (aged
7-8 years, medium age 8 years) in 3 municipalities in Northern Sweden;
Luleå and Piteå located by the coast of the Baltic Sea and Kiruna located in
the innermost parts of the Norrbotten County (Figure 5). The children
invited to this cohort study composed almost 60% of all children in this age
group in Norrbotten County in 2006. In 2010, there was a study follow-up,
using the same methods. This time, all children in classes 5 and 6 (aged 11-12
years, medium age 12 years) in the same three municipalities were invited to
participate in the study (27).
Fig. 5. Study area

30
Questionnaires
Procedure
The parental questionnaire included the International Study of Asthma and
Allergies in Childhood (ISAAC) core questions (167) with added questions
about symptoms, physician diagnosis, medication and possible determinants
of asthma, rhinitis and eczema. This questionnaire has been used in the
OLIN cohort studies since 1996 (27,168-170). In 2006, queries about allergy
/hypersensitivity to foods were added to the questionnaire (36). The parental
questionnaires were distributed by school personnel.
Participants
When the cohort was recruited in 2006, the parents of 2585 children, 96% of
invited, participated in the questionnaire. At the 2010 study follow-up, the
parents of 2612 children, 96% of invited, answered the questionnaire,
whereof whom 2378 (89% of the original cohort) also had participated at
study start (Figure 6).
Skin Prick Tests
Procedure
The SPT followed the European Academy of Allergology and Clinical
Immunology (EACCI) recommendations (171). The Solu-Prick panel
included: birch, timothy, mugwort, cat, dog, horse, two house dust mite
extracts (Dermatophagoides pteronyssius and farinae) and two mold extracts
(Claudosporium and Alternaria) (ALK, Denmark).
The potency of the extracts was 10 histamine equivalent prick (HEP) except
for the two molds, which were 1:20 w/v. Histamine 10 mg/ml and glycerol
were used as the positive and negative controls. A positive test was defined
as at least one wheal ≥3mm in diameter, recorded after 15 minutes.
Participants
In 2006, the 1895 children from the two municipalities Luleå and Kiruna
were invited to the SPT and 1700 (90%) participated. At the 2010 study
follow-up, 1657 children (86% of invited) participated in the SPT, whereof
1450 (77 % of the children invited in 2006) also had participated in the skin
prick testing at study start in 2006 (Figure 6).

31
Child interview
Procedure
At the 2010 follow-up, all children in the two municipalities Luleå and
Kiruna were also invited to a short interview, hence called Child interview,
including questions about perceived allergy/hypersensitivity and avoidance
of the basic foods; milk, egg, cod and wheat. The interviews were performed
at the children’s schools along with the skin prick tests and assessment of
BMI.
Participants
A total of 1824 11-12 year old children (98% of invited) participated in the
Child interview (Figure 6).
Serological tests
Procedure
Serum samples were analyzed using an fx5 ImmunoCAP food screening test
(ThermoFisher Diagnostics, Uppsala, Sweden) including cow’s milk, hen’s
egg, cod, soy, wheat, and peanut. If the screening test was positive, specific
IgE was analyzed separately for all of the included foods. An ImmunoCAP
inhalant allergen screening was also conducted (ThermoFisher Diagnostics,
Uppsala, Sweden) and included the following allergens: birch, timothy,
mugwort, cat, dog, horse, dust mites (Dermatophagoides pteronyssius and
farinae), and Claudosporium.
An IgE serum level > 0.35 kU/L was considered positive for all of the IgE
tests. Further, tissue transglutaminase A (tTGA) was measured in serum as a
marker of celiac disease using the EliATM CelikeyTM IgA test (ThermoFisher
Diagnostics, and a tTGA serum level < 7 U/L was considered negative.
Participants
At the 2010 follow-up all children in Kiruna and 25% randomly selected
children from Luleå were invited to donate blood samples for analyses of
specific IgE-tests and tTGA. Of 997 invited, 695 children (71 %) participated
in the blood sampling.

32
Statistical analyses
The statistical analyses were performed using the Statistical Package for
Social Science Software 21 (SPSS Inc, Chicago, IL, USA). In Papers II-V, the
Chi square test, and Fisher’s exact test when appropriate, or bivariate logistic
regression was used for bivariate comparison of categorical variables.
Multivariate regression models were used in Paper II and IV when adjusting
for possible confounding factors. The multivariate regression models
included the variables that were significant or borderline significant in the
bivariate analyses. When comparing continuous variables between groups,
the Student’s T-test or ANOVA was used if the variable was normally
distributed and the Mann-Whitney test or the Kruskal-Wallis 1-way ANOVA
if not. In all papers, a 95% confidence interval (CI) was used and a p-value <
0.05 was considered statistically significant.

33
Definitions
Paper II:
▫Any FHS - was defined as questionnaire-reported symptoms to at least one
of the specific foods: cow’s milk, hen’s egg, fish, wheat, soy, kiwi, orange,
apple, raw carrots, banana, nuts, peanuts and almonds.
▫Non-milk FHS - was defined as questionnaire-reported symptoms to one or
more of the specific foods; hen’s egg, fish, wheat, soy, kiwi, orange, apple,
raw carrots, banana, nuts, peanuts and almonds, cow’s milk excluded.
▫Milk FHS - was defined as questionnaire-reported symptoms to cow’s milk
only.
Paper III:
▫Reported food allergy - was defined as reported allergy or hypersensitivity
to and complete avoidance of one or more of the foods; cow’s milk, hen’s egg,
fish, or wheat in the Child interview (children in Luleå and Kiruna) or in the
parental questionnaire (children in Piteå). Children were not included in this
definition if they had a questionnaire-reported physician diagnosed celiac
disease.
Paper III-V:
▫FHS phenotypes – were based on data collected from the structured
interviews and analyses of food specific IgE and tTGA. The food
hypersensitivity phenotypes were determined by the following preset
criteria:
▫IgE-mediated food/milk allergy phenotype – was defined as the fulfilled
mandatory criteria:
A positive food specific IgE-test – provided exposure to the culprit
food within the last two years
Symptoms triggered by less than 100 ml of milk or less than a
portion size of egg, cod or wheat products
…and at least two fulfilled secondary criteria:
Onset before five years of age – provided that the food had been
introduced in the child’s diet prior to that age
First symptom within 15 minutes of exposure
Symptoms from more than one organ system
Symptoms triggered by treasure amounts of the culprit food

34
Symptoms triggered by skin exposure
Symptoms triggered by airborne exposure
Anaphylaxis / exercise induced anaphylaxis
▫Non-IgE mediated food/milk allergy phenotype– was defined as the
fulfilled mandatory criteria:
A negative food specific IgE-test
Symptoms triggered by less than 100 ml of milk or less than a
portion size of egg, cod or wheat products
No celiac disease
…and at least two fulfilled secondary criteria:
Onset before five years of age – provided that the food had been
introduced in the child’s diet prior to that age
First symptom more than 1 hour after exposure
Symptoms from more than one organ system
Symptoms triggered by treasure amounts of the culprit food
▫Suspected food allergy – was defined as all but one fulfilled criteria for the
IgE-mediated or non-IgE mediated allergy phenotypes.
▫Outgrown food/milk allergy phenotype – was defined as a convincing
history of an IgE-mediated or non-IgE mediated allergy, and continued
avoidance of the culprit food despite tolerance of at least 100 ml of milk or a
portion size of egg, cod or wheat products without symptoms.
▫Probable lactose intolerance phenotype – was defined as fulfilled
mandatory criteria:
Symptom onset after five years of age
Symptoms limited to flatulence, stomach-ache and/or diarrhea
Symptoms triggered by 100 ml of milk or more
Symptom-free on a lactose free/reduced diet
No milk allergy
No Celiac disease
▫Suspected lactose intolerance – was defined as all but one fulfilled
mandatory criteria for the probable lactose intolerance phenotype.
▫Celiac disease phenotype - was defined as a reported physician diagnosis of
Celiac disease and/or a positive tTGA-test.

35
▫Non-definable phenotype – was defined as avoidance of milk, egg, cod or
wheat but did not fulfil the criteria for any of the listed phenotypes or
declined donation of food specific IgE and/or tTGA, which were essential for
the FHS phenotyping.
▫Discontinued elimination diet – was defined as reported food allergy at the
Child interview (children in Luleå and Kiruna) or in the parental
questionnaire (children in Piteå) and cancellation of the food avoidance prior
to the structured interview.
Paper II-V:
▫Allergic heredity – was defined as questionnaire-reported parental asthma,
rhinitis and/or eczema.
▫FHS heredity – was defined as questionnaire-reported parental food
hypersensitivity
▫Allergic sensitization – was defined as at least one positive SPT or positive
IgE screen test.
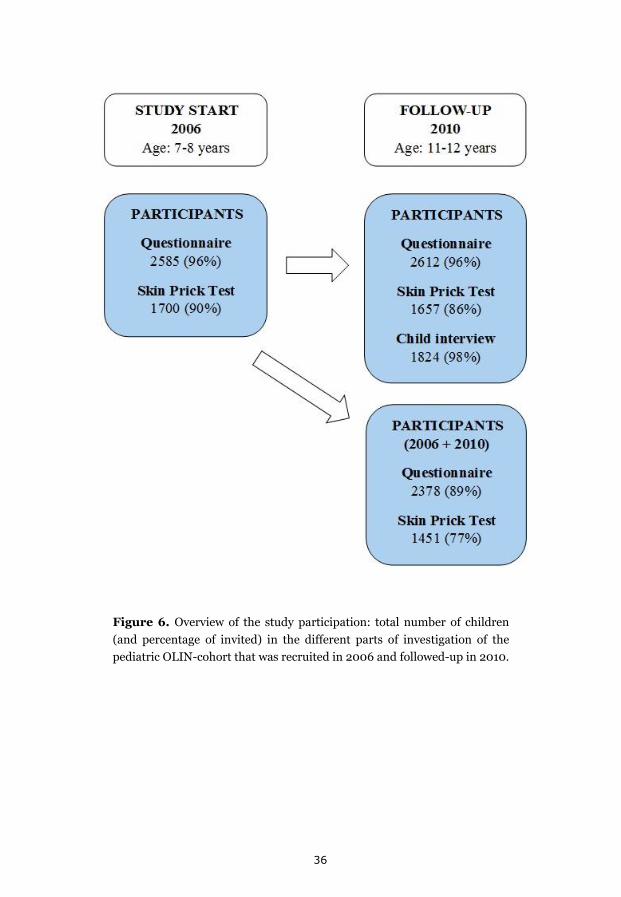
36
Figure 6. Overview of the study participation: total number of children
(and percentage of invited) in the different parts of investigation of the
pediatric OLIN-cohort that was recruited in 2006 and followed-up in 2010.

37
2. Method: Paper II
Study population
The main objective of Paper II was to investigate the incidence and
remission of parentally reported food hypersensitivity between 7-8 and 11-12
years of age. For this longitudinal study we included the 2378 children (89%
of invited) from the OLIN cohort who participated both at study start and at
the 2010 follow-up (Figure 6).
Questionnaires and Skin prick tests
Questionnaire data regarding parentally reported hypersensitivity to foods at
age 7-8 years and 11-12 years were collected. Variables from the parental
questionnaire and SPT results analyzed as possible risk factors for incidence
and remission of reported hypersensitivity to foods were collected from the
2006 investigation when the children were 7-8 years of age.
Serological tests
Among the serological analyses collected from the random population
sample, results from the fx5 ImmunoCAP food screen test (ThermoFisher
Diagnostics, Uppsala, Sweden) were available for 652 children (71% of
invited) of those who had participated in the questionnaire both at study
start and study follow-up. The presence of a positive IgE to any of the foods;
milk, egg, cod, wheat, soy and peanut was analyzed in relation to parentally
reported hypersensitivity to the corresponding food.
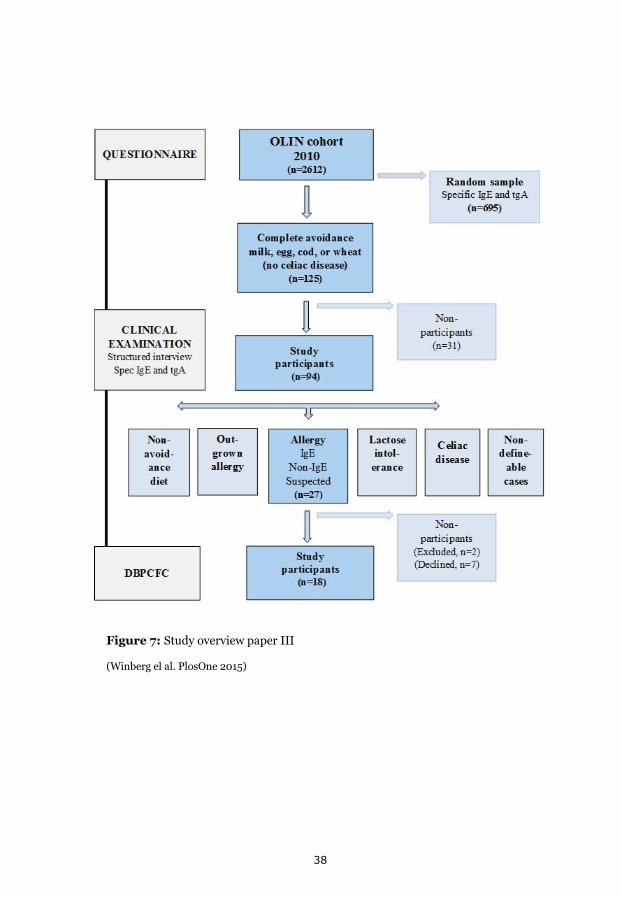
38
Figure 7: Study overview paper III
(Winberg el al. PlosOne 2015)
39
3. Method: Paper III
Study population
The main objective of Paper III was to assess the prevalence of allergy to
cow’s milk, hen’s egg, cod and wheat at 11-12 years of age. In this cross-
sectional study we included all of the 2612 children who participated in the
2010 questionnaire (Figure 6). A study overview is presented in Figure 7.
Questionnaires and Child interviews
The inclusion criteria for invitation to the clinical investigation was a
reported allergy to the basic foods; milk, egg, cod or wheat, defined as:
- Reported allergy/hypersensitivity to milk, egg, cod or wheat
- Complete avoidance of the culprit food
- No physician diagnosed celiac disease
The children from the two municipalities Luleå and Kiruna were included
according to their answer to the Child interview question:
“To what extent do you avoid the following foods; cow’s milk, hen’s egg,
fish, or wheat, due to allergy/ hypersensitivity?” The possible answer
alternatives for each food were; not at all, partially or completely.
Since the children in the municipality of Piteå were not invited to the Child
interviews and SPTs, these children were included according to the answer to
the following question in the parental questionnaire:
“To what extent does your child avoid the following foods; cow’s milk, hen’s
egg, fish, or wheat, due to allergy/ hypersensitivity?” The possible answer
alternatives for each food were; not at all, partially or completely.
Data on celiac disease was collected from the parental questionnaire query:
“Has your child been diagnosed by a physician as having celiac disease?”
40
Clinical examinations
The children with reported allergy were invited to a clinical examination,
including:
- A structured interview (Supplemental file)
- A physical examination
- Blood samples for analysis of tTGA , food specific IgE, an IgE food
screen test and an IgE inhalant screen test
The clinical examination included measurement of length (cm) and weight
(kg) and a clinical investigation including inspection of ears, mouth and skin,
auskultaion of heart and lungs and palpation of abdomen, thyroid and
nodular glands. All clinical examinations were performed by the same
pediatric allergist (AW).
Food hypersensitivity phenotypes
According to the results from the clinical examinations, children were sorted
into the following food hypersensitivity phenotypes according to preset
criteria (see Definitions):
- Current food allergy
o IgE-mediated allergy
o Non-IgE-mediated allergy
o Suspected allergy
- Outgrown food allergy
- Lactose intolerance
- Celiac disease
- Non-definable cases/ Non-avoidance diet
Double-blind placebo-controlled food challenges
The DBPCFC was performed as a 3-session challenge series, the sessions set
one week apart (Figure 9). At two of the challenge sessions the test substance
contained the challenge food and at one session the test substance was free
of the challenge food (placebo).
The serving order was drawn by lot and unknown to both the patients and
the personal undertaking the challenges (AW and ÅS). The test substances
were prepared immediately prior to the challenge session and the same
dietician (LN) was responsible for the preparation during all the challenge
series. The DBPCFC recipes used were those previously validated in Paper I.

41
Due to safety reasons, the DBPCFC series were performed in a hospital
setting. The test substance was served in increasing doses 30 minutes apart
and the child remained for observation for 2 hours after the completed
challenge. The test session was aborted at the dose step where the child
developed clear, objective symptoms or when all dose steps had been
completed. If the symptoms were severe, the whole challenge series was
terminated. Following each challenge session, the child performed a 3-day
symptom diary.
The DBPCFC code was broken at a follow-up visit one week after the
completed challenge series. The same pediatric allergist (AW) and study
nurse (ÅS) were responsible at all challenge-sessions and follow-up visits. A
DBPCFC series was considered positive if the child during or following the
challenge sessions with active substance developed symptoms that were
objective and/or repeatable.

42
Figure 8. Study overview paper IV

43
4. Method: Paper IV
Study population
The low prevalence of challenge-proven allergy to basic foods initiated
further examination of the children reporting partial milk avoidance, as we
had only included children reporting complete milk avoidance in Paper III.
For this cross-sectional study we included all 1824 children (98% of invited)
from the 2010 follow-up who had participated in the Child interview (Figure
6). The main aim of this study was to investigate the milk hypersensitivity
phenotypes among children reporting milk avoidance due to perceived
hypersensitivity and whether the phenotypes were different between
children reporting complete or partial milk avoidance.
Child interviews, structured interviews and serological tests
The inclusion criterion was a report of milk avoidance, partially or
completely, due to perceived milk hypersensitivity. The inclusion was based
on the following question from the Child interview:
“To what extent do you avoid the following foods; cow’s milk, hen’s egg,
fish, or wheat, due to allergy/ hypersensitivity?” The possible answer
alternatives for each food were; not at all, partially or completely.
Children with physician-diagnosed celiac disease were not invited to the
structured interview. Data on celiac disease was collected from the parental
questionnaire query:
“Has your child been diagnosed by a physician as having celiac disease?”
Children participating in the child interview were also invited to assessment
of BMI and 1808 children (97% of invited) participated in measurement of
both length and weight.
Data regarding living conditions, allergic sensitization, allergic heredity and
physician-diagnosed asthma, rhinitis and eczema were collected from the
2010 parental questionnaire.

44
The structured interviews were performed 6-12 months after the Child
interview.
- Children reporting complete milk avoidance were invited to the
Clinical examination described in Paper III, which included a
structured face-to-face interview.
- Children reporting partial milk avoidance were invited to the same
structured interview but over telephone.
Children, who at the time of the telephone interview still avoided milk, were
invited to donate blood for analyses of tTGA, milk specific IgE, an IgE food
screen test and an IgE inhalant screen test (ThermoFisher Diagnostics,
Uppsala, Sweden). Results from analyses from the same tests were already
available for the children reporting complete milk avoidance who
participated in the Paper III study.
Food hypersensitivity phenotypes
According to the results from the structured interviews and blood sample
analyses, the children were sorted into the following milk hypersensitivity
phenotypes according to preset criteria (see Definitions):
- Current milk allergy
o IgE-mediated allergy
o Non-IgE-mediated allergy
- Outgrown milk allergy
- Probable lactose intolerance
- Celiac disease
- Non-definable cases
- Discontinued milk avoidance
The prevalence of the different milk hypersensitivity phenotypes was
compared between children reporting complete and partial milk avoidance.
In addition, the association between the different milk hypersensitivity
phenotypes and BMI, living conditions, allergic sensitization, allergic
heredity and physician diagnosed asthma, rhinitis and eczema was analyzed.

45
5. Method: Paper V
Since DBPCFC are time and labor consuming and put the child at risk of an
allergic reaction, there is ongoing search of objective, prognostic markers
that could predict the food challenge otcome. We examined the spontaneous
cytokine mRNA expression of PMBCs, quantified for a panel of 15 cytokines
discriminating between a humoral Th2-, cytotoxic Th1-, regulatory Th3/Tr1-
and inflammatory responses in children with suspected food allergy and
helathy controls before and one week after a completed food challenge-
series. In addition, inflammatory and regulatory biomarkers in faeces were
analyzed in children with suspected food allergy. The main objective was to
investigate whether the included biomarkers had the potential of
determining the challenge outcome.
Study population
We included all 18 children with suspected food allergy who participated in
the DBPCFC series in Paper III. Complete analyzable blood samples were
available from 17 of these children.
In addition, 7 children without any allergies randomly selected from the
OLIN cohort participants living in Luleå, were invited to participate in a
DBPCFC series with egg. All of the invited controls participated in the
challenge series and complete blood samples were available from 6 of these
children.
Serum sampling and serological tests
Blood samples for the analyses of expressed cytokine mRNA patterns were
collected immediately before the first challenge session (baseline samples)
and one week after the last session (post challenge samples) (Figure 9). Sera
for analysis of food specific IgE and IgG4 (ThermoFisher Diagnostics,
Uppsala, Sweden) were collected from all children at baseline and from
children with suspected food allergy post challenge.
Cytokine expression in PBMCs
Peripheral blood mononuclear cells (PBMC) were isolated using Ficoll-paque
gradient centrifugation. Then, using quantitative real time polymerase chain
reaction (qRT-PCR), a cytokine gene expression analysis was made.

46
The messenger ribonucleic acid (mRNA) expression of the 12 included
cytokines were analyzed as markers of T-cell response; IFN-γ as a marker of
Th1-response, IL-4, IL-5 and IL-13 as markers of Th2-response, TGF-β and
IL-10 as markers of T-regulatory response, IL17-A as a marker of Th-17
response, IL-2 and IL-15 as markers of T-cell proliferation and TNF α, IL-1β,
IL-6 and IL-8 as markers of pro-inflammatory response. The expression of
the different cytokines at baseline and post challenge was then analyzed
according to DBPCFC outcomes and in relation to the control group.
Figure 9. Study overview of paper 5 and analyzed cytokine mRNA
expression in peripheral blood mononuclear cells including hallmark
cytokines for the humoral allergy-promoting T helper (Th) 2 response,
cellular cytotoxicity-promoting Th1 response, inflammatory-, and T
regulatory responses.
47
Biomarkers in stool samples
The 18 children with suspected food allergy were also invited to donate stool
samples at baseline and post challenge. From the complete stool samples
available from 12 of these children, five fecal markers where quantified using
enzyme-linked immunosorbent assay (ELISA) methods (Immundiagnostik,
Bensheim, Germany): PhiCal®Calprotectin, EDN (Eosinophil-derived
neurotoxin), sIgA (Secretory IgA), HBD-2 (human β-Defensin-2) and α1-
Antitrypsin. The levels of the different fecal markers at baseline and post
challenge were then analyzed according to DBPCFC outcomes.
48

49
Results
Validation of new DBPCFC recipes (Paper I)
In this study we aimed to validate new recipes for low-dose double-blind
placebo-controlled food challenges in school children, by investigating if
there were any sensory differences between the active materials containing
cow’s milk, hen’s egg, soy, wheat or cod, and the placebo materials. The
challenge materials contained the same amino acid based product Elemental
028 extra liquid orange/pineapple flavour (Nutricia, Liverpool, England),
with or without added food allergens. Further, to match the sensorial
properties of the challenge foods, supplementary ingrediants had been added
to the different test materials. The test panels consisted of 275 school
children, aged 8-10 and 14-15 years respectively, from five Swedish schools.
Each participant tested at least one recipe.
Standardized blinded triangle tests were performed to investigate if any
sensory differences could be detected between the active and placebo
materials. In our final recipes, no significant differences could be detected
between the active and placebo materials for any challenge food (p>0.05).
These results remained after stratification for age and gender. The taste of
challenge materials was acceptable to the children in both age groups and no
unfavourable side effects related to test materials were observed.
Main results:
New recipes for low-dose double-blind placebo-controlled food
challenges for milk, egg, cod, wheat and soy were validated regarding
detectable differences between the active and placebo substances. The
taste and texture of the test substances were accepted by the children in
the test panels, i.e. at 8-10 and 14-15 years of age.

50
Incidence and remission of food hypersensitivity (Paper II)
Prevalence, incidence and remission
In this longitudinal study, we investigated parentally reported FHS in a
population based cohort of schoolchildren, followed from 8 to 12 years of
age. The prevalence of reported hypersensitivity to any food increased from
21% at 8 years to 26% at 12 years of age (p< 0.001). During the same 4-year-
period, the prevalence of reported hypersensitivity to the basic foods: milk,
egg, cod and wheat increased from 10 % to 15 % (p<0.001) and the
prevalence of reported milk hypersensitivity from 9 % to 13 % (p<0.001)
(Figure 10). The cumulative incidence of reported FHS was high (15%), as
was remission (33%). This pattern was recognizable for hypersensitivity to
many of the 13 common foods investigated, but it was particularly evident
for hypersensitivity to cow’s milk.
Figure 10. Comparison of prevalence of food hypersensitivity, asthma, rhinitis
and eczema respectively, at the age of 7-8 and 11-12 years of age.

51
Factors associated with incidence and remission
Female sex, allergic heredity, current rhinitis and allergic sensitization were
associated with the incidence of any FHS. Allergic sensitization was
negatively associated with remission. While the factors associated with the
incidence and remission of non-milk FHS were similar to the factors
associated with any FHS, the risk factor patterns for milk hypersensitivity
were different. Female sex and allergic heredity were associated with the
incidence of milk FHS and living in Kiruna was negatively associated with its
remission, though no association was found to other atopy related conditions
(Figure 11).
Figure 11. Association of listed variables at 8 years of age to the incidence of
non-milk FHS and milk FHS presented as odds ratios (OR) and 95% confidence
intervals (CI).

52
Reported FHS and IgE- sensitization
Among the 652 children (71% of invited) who participated in the serological
tests, parentally reported hypersensitivity to the foods; milk, egg, cod, wheat,
soy and peanut were analyzed in relation to the presence of a positive IgE-
test to the culprit food. Generally, the agreement between reported food
hypersensitivity and IgE-sensitization to the implicated food was poor. This
was particularly true for the foods: milk, wheat and soy. However, even for
peanut, only one third of the peanut sensitized children reported symptoms
and only one third of the children with reported hypersensitivity to peanut
had a positive IgE-test.
Main results:
There was a high incidence as well as a high remission of reported food
hypersensitivity from age 8 to 12 years of age. Risk factors associated
with incidence and remission were different for milk hypersensitivity
and hypersensitivity to foods other than milk. The agreement between
reported symptoms to milk, egg, cod, wheat, soy and peanut and IgE-
sensitization to the culprit food was poor.

53
Assessment of allergy to milk, egg cod and wheat (Paper III)
In this cross-sectional study we investigated the prevalence of allergy to the
basic foods; milk, egg, cod and wheat among 11 to 12-year-old children in a
population based cohort using;
1. Reported data
2. Clinical investigations (structured interviews, physical examinations
and analyses of serum specific IgE and a celiac screening test)
3. A double-blind placebo-controlled food challenge series.
The prevalence of reported hypersensitivity to cow’s milk, hen’s egg, cod,
and/or wheat among the 11 to 12 year olds was 14.7% and the prevalence of
reported allergy to these foods according to our definition was 4.8% (Figure
12).
The 125 children with reported allergy to milk, egg, cod and wheat were
invited to the clinical examination and 94 (75%) participated. Based on the
results, children were categorized into the following FHS phenotypes:
current allergy (29%), outgrown allergy (19%), lactose intolerance (40%)
and unclear (12%). Among children categorized as having a current allergy,
positive food (63%) or inhalant (74%) allergen screen test were common, as
were reported physician diagnoses of asthma (52%), rhinitis (44%), and
eczema (67%). Assuming a similar distribution among the non-participants,
the prevalence of allergy to milk, egg, cod and wheat according to the clinical
examination was 1.4% (Figure 12).
The 27 children categorized as current food allergy were then considered for
further evaluation with a DBPCFC series. Two of these children fulfilled
preset exclusion criteria and were therefore not included. Of 25 invited, 18
children (72%) participated in a total of 20 challenge series with milk, egg or
cod. Thus, 2 children participated in 2 challenge series with different basic
foods.
Out of the 20 DBPCFCs, 9 were considered positive. All but one child with a
positive challenge outcome were IgE-sensitized to the culprit food. Four of
the nine children with positive challenge outcomes reacted with an
anaphylaxis. Only one of these children had previously been prescribed an
epinephrine auto-injector and none of these children were on daily
treatment for their concomitant asthma. Assuming a similar distribution of

54
positive DBPCFC outcomes among the non-participants, the food allergy
prevalence following DBPCFC was 0.6% (Figure 12).
Main results:
The prevalence of reported allergy to cow’s milk, hen’s egg, cod, or wheat
was 4.8%, whereas the prevalence according to preset diagnostic criteria
was 1.4%. This figure was further halved when possible food allergy was
evaluated with double-blind placebo-controlled food challenges. The
majority of children with reported allergy to basic foods were categorized
as other food hypersensitivity phenotypes, the most common being
probable lactose intolerance and outgrown food allergy.
Figure 12: Prevalence of reported food hypersensitivity and allergy to the basic
foods; milk, egg cod and wheat according to reported data, clinical investigation
and double-blind placebo-controlled food challenges.

55
Milk hypersensitivity phenotypes (Paper IV)
In this cross-sectional study we investigated the milk hypersensitivity
phenotypes among 11-12-year old children with self-reported milk avoidance
due to perceived milk hypersensitivity. Of the whole study sample, n=1824,
the prevalence of self-reported milk hypersensitivity was 14.5% (n=265). Of
these, 193 children (73%) reported partial milk avoidance and 72 children
(27%) reported complete avoidance of milk. Among the 265 children with
reported milk hypersensitivity, 236 (89%) participated in a structured
interview.
Only 3 % of the 11 to 12-year-olds with self-reported milk hypersensitivity
were categorized as current milk allergy; of whom all had reported complete
milk avoidance. The most common milk hypersensitivity phenotype was
probable lactose intolerance (40%) followed by outgrown milk allergy
(23%).
Figure 13. Distribution of the different milk hypersensitivity phenotypes
among children reporting complete and partial milk avoidance

56
Children with outgrown milk allergy had a convincing history of milk allergy
but tolerated at least 100 ml of milk without any symptoms at the time of the
evaluation. Despite this, they had remained on an elimination diet. At the
time of the structured interview, 30 % of the children had discontinued their
milk elimination diet. All children with discontinued elimination diet had
previously reported partial milk avoidance. Except for the phenotypes
current milk allergy and discontinued milk avoidance, the distribution of
the different milk hypersensitivity phenotypes was similar between children
reporting complete and partial milk avoidance (Figure 13).
Figure 14. Association of the listed variables to milk allergy, current
or outgrown expressed as odds ratios (OR) with 95% confidence
intervals (CI).

57
Children with current or outgrown milk allergy had a lower BMI (OR 0.82,
95% CI 0.80-0.98) compared to children with no milk avoidance. Also,
among children with milk allergy the variables female sex, physician
diagnosed eczema and heredity for food hypersensitivity were more common
compared to children not avoiding milk (Figure 14). In contrast, children
with probable lactose intolerance were less often sensitized to aeroallergens
and food allergens compared to children with no reported milk
hypersensitivity.
Only 9% of the children currently avoiding milk reported that they in
previous health care contacts had ever been referred to a dietician for
nutritional advice and only 2% reported that their milk hypersensitivity
diagnosis had been established by an oral challenge.
Main results:
Even though the prevalence of reported milk hypersensitivity among
the 11-12 year olds was as high as 14.5%, only 3% of them were
categorized as current milk allergy. The most common milk
hypersensitivity phenotypes were probable lactose intolerance and
outgrown milk allergy. Current and outgrown milk allergy was
associated with other atopic disorders and lower BMI. Only 9 % of the
children currently avoiding milk reported that they had ever been
referred to a dietician for nutritional advice and only 2% had a milk
hypersensitivity diagnosis established by an oral challenge.
58
If only immunology was this simple…

59
Biomarkers in blood and stool samples (Paper V)
Here, we analyzed the spontaneous cytokine mRNA expression pattern of
PMBCs before and one week after a completed DBPCFC series with milk, egg
or cod in 12-13 year old children with suspected food allergy and in age-
matched healthy controls. Blood samples were available from 17 children
with suspected food allergy; 9 children with negative challenge outcomes and
8 with positive challenge outcomes. Of the children with positive challenge
outcomes, 3 had reacted with anaphylaxis during challenge. In addition, 7
children from the OLIN cohort without any allergies participated in a
DBPCFC series with egg and blood samples were available from 6 of these
controls.
Further, inflammatory and regulatory biomarkers in faeces were analyzed in
children with suspected food allergy before and one week after the DBPCFC
series. Stool samples were available for 12 children, 6 with positive and 6
with negative challenge outcomes.
Figure 15. Median mRNA expression of the cytokines IL-13 and IL-10 at
baseline and post challenge in children with positive and negative
challenge outcomes and in controls.

60
At baseline, children with suspected food allergy expressed higher mRNA
levels of the Th2-related cytokine IL-13 compared to controls. The baseline
mRNA level of IL-13 was higher in children with a positive challenge
outcome compared to children with a negative challenge outcome. The
baseline levels of the regulatory cytokine IL-10 were similar in the controls
and in children with a negative challenge outcome, though significantly
higher among children with a positive challenge otcome, i.e. challenge-
proven food allergy (Figure 15).
Post challenge, children with suspected food allergy expressed higher mRNA
levels of the pro-inflammatory cytokines IL-1β and IL-6 compared to
controls but there were no significant differences detected in the post
challenge cytokine mRNA profiles between children with positive and
negative food challenges.
Figure 16. Median values of fecal markers at baseline and post challenge
among children with a positive (n=6) and negative (n=6) challenge outcome.

61
Three of the children in our study reacted with anaphylaxis during DBPCFC.
Compared to healthy controls, children with anaphylaxis expressed 10-fold
higher mRNA levels of the Th2-related cytokines IL-4 and IL-13 at baseline
and 30-100 fold higher levels of the pro-inflammatory cytokines IL-1β and
IL-6 post challenge. Children with anaphylaxis also expressed a 10-fold
higher post challenge mRNA level of the regulatory cytokine IL-10 compared
to controls. As opposed to this finding, the post challenge mRNA level of the
regulatory cytokine TGF-β1 was decreased among children with anaphylaxis
compared to healthy controls. Due to the low number of children with
anaphylaxis, no statistical analyses were performed on this subgroup.
The levels of calprotectin and EDN in feces were higher among the children
with a positive food challenge compared to children with a negative
challenge outcome both at baseline and post challenge, though the
differences did not reach statistical significance (Figure 16). There were no
detectable differences between children with challenge-proven allergy and
children with a negative challenge outcome for the fecal biomarkers: sIgA, β-
Defensin-2 and α1-Antitrypsin.
Main results:
At baseline, children with suspected food allergy had elevated
expression levels of the Th2-associated cytokine IL-13 compared to
controls. IL-13 mRNA and mRNA for the regulatory cytokine IL-10 were
higher in challenge-proven food allergy compared to the cytokine levels
seen in negative challenges. Post challenge, IL-1β and IL-6 mRNA were
elevated in the allergic children compared to controls. Fecal calprotectin
and EDN levels were higher in challenge proven food allergy compared
to a negative challenge although not statistically significantly.

62

63
Discussion
Discussion of methodology
Sensory testing
There are two types of sensorial differentiation tests; Overall difference tests
that are designated to show whether subjects can detect any difference
between samples and Attribute difference tests where different samples are
ranked according to one or more attributes i.e. sweetness (166). Since our
aim was to investigate whether children in different age groups could detect
any sensorial difference between the active and placebo materials of our
recipes, we choose to use the Overall difference test called Triangle test.
Compared to the alternative Overall difference test called Duo-trio-test, the
Triangle test is statistically more efficient (165,166).
It has been suggested that for sensorial testing, professional adult panelists
should be used (166,172). However, since a secondary aim of our validation
study was to examine whether the taste and texture of our test samples were
acceptable to children of different ages, we chose to include children aged 7-
10 years and 14-15 years in our test panels. To increase the validity of the
tests, we used large test panels. In a triangle test, a test panel of at least 25-
30 people is required to obtain the requisite sensitivity of the test (165,172).
We therefore aimed to invite around 50 children in each age group. Further,
before starting the study tests the participating children were educated in the
triangle test technique using two different kinds of fruit juices.
Epidemiologic study design
A major strength of our project including Papers II-V, is the longitudinal and
population-based design and the high participation-rates, supporting the
representativeness of the population i.e. the internal validity. The internal
validity describes to what extent the study outcome defines the true situation
in the study population, while external validity describes whether the results
of the study are applicable to other populations or settings (173).
Since the investigated cohort represent almost 60% of the children in
Norrbotten County, we have reason to believe that our findings are
representative for schoolchildren in the North of Sweden.
64
Supported by the findings of others (16,32,35,38), we also think that our
results might be applicable to children in other parts of Sweden and perhaps
even to children with similar socio-economic conditions in other parts of the
Western world, even though the very high percentage of Caucasians in our
cohort could affect the prevalence of FHS (32,65).
The relatively large study cohort and the commonness of the investigated
conditions, support the reliability of our studies. The pediatric cohort was
originally recruited for investigating prevalence of asthma, rhinitis, eczema
and allergic sensitization and for this the power of the study was excellent.
The calculated power for investigating incidence and remission of these
conditions was also satisfactory.
In line with this, the power of our questionnaire studies investigating
prevalence, incidence and remission of reported food hypersensitivity was
good. Even though the participation in the structured interviews and clinical
examinations were somewhat lower, 89% and 75% respectively, the very high
participation (96-97% of invited) in the parental questionnaires allowed us
to perform non-responder analyses based on questionnaire data. In Paper III
and IV these analyses did not show any significant differences for variables
like: sex, living conditions, older siblings, parental smoking, allergic
heredity, allergic sensitization and physician diagnosed asthma, rhinitis and
eczema between participants and non-participants in the structured
interviews and clinical examinations. Thus the study participants were
representative of the entire cohort.
A possible limitation with the population-based design, was that despite a
large cohort, the high participation rate and a high prevalence of reported
hypersensitivity to the basic foods: milk, egg, cod and wheat in the entire
cohort, the final prevalence of current food allergy following clinical
examination was low. As a consequence, a small group of children were
finally invited to the DBPCFC series, affecting the power in the analyses of
the challenge outcomes in Paper III and more so in the statistical analyses of
biomarkers in Paper V. The findings of the latter study therefore needs to be
verified by larger studies, by either inviting a larger cohort or by inviting
study participants from a hospital material (173).

65
In Paper II we investigated the cumulative incidence of reported food
hypersensitivity i.e. the onset of new cases with time, and the remission i.e.
the number of study participating recovering with time (173), between the
ages 7-8 and 11-12 years. A longitudinal study design, where a cohort is
followed over time, is preferable when examining incidence or remission of a
condition. In Papers III and IV, we used cross-sectional studies to
investigate the prevalence of allergy to basic foods and other food
hypersensitivity phenotypes at 11-12 years of age. Prevalence is a measure of
the percentage of individuals affected by a condition or exposure at a certain
point of time. Combining longitudinal and cross-sectional data on FHS
rendered a broader picture and a better understanding of the investigated
condition and was a major strength of our study.
Reported data
A significant part of this work is based on reported data, making it
susceptible to information bias (175). Bias stands for a systematic error that
causes distortion of the study, which might affect the study outcome
(173,174). Information bias is caused by measurement errors and can arise
when some people are more or less inclined to report the presence of a
disease or an exposure, defined as reporting bias, or if certain people are
more or less prone to remember conditions and exposures of the past,
defined as recall bias (175). Information bias may also occur if different
questionnaires or study methods are used at different study occasions, when
using study methods that are highly dependent on the investigator or when
the same reported data are collected from different individuals, e.g. children
and either of their parents.
In our study we used a comprehensive questionnaire, which was almost
identical at study start and follow-up. The questionnaire has also been used
in previous OLIN-studies since 1996 (27,168-170). Further, the clinical
examinations in Paper III were all performed by the same pediatric allergist
(AW). We did not, however, have access to the children’s medical journals to
verify reported data on food hypersensitivity diagnoses and previous
diagnostic tests, wich could have added further information and reduced the
risk of report bias.
In Paper III, the inclusion criteria for the children in the two municipalities
Luleå and Kiruna and the municipality of Piteå differed. The children in
Luleå and Kiruna were included according to self-reported FHS at the Child
interview, while children in Piteå were included according to parentally
reported FHS.
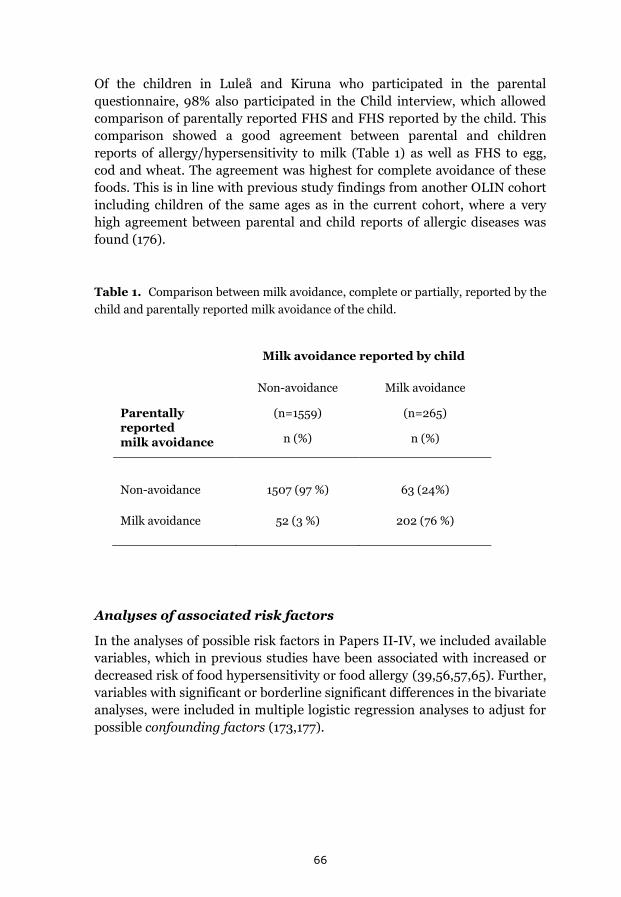
66
Of the children in Luleå and Kiruna who participated in the parental
questionnaire, 98% also participated in the Child interview, which allowed
comparison of parentally reported FHS and FHS reported by the child. This
comparison showed a good agreement between parental and children
reports of allergy/hypersensitivity to milk (Table 1) as well as FHS to egg,
cod and wheat. The agreement was highest for complete avoidance of these
foods. This is in line with previous study findings from another OLIN cohort
including children of the same ages as in the current cohort, where a very
high agreement between parental and child reports of allergic diseases was
found (176).
Table 1. Comparison between milk avoidance, complete or partially, reported by the
child and parentally reported milk avoidance of the child.
Milk avoidance reported by child
Parentally reported
milk avoidance
Non-avoidance
(n=1559)
n (%)
Milk avoidance
(n=265)
n (%)
Non-avoidance 1507 (97 %) 63 (24%)
Milk avoidance 52 (3 %) 202 (76 %)
Analyses of associated risk factors
In the analyses of possible risk factors in Papers II-IV, we included available
variables, which in previous studies have been associated with increased or
decreased risk of food hypersensitivity or food allergy (39,56,57,65). Further,
variables with significant or borderline significant differences in the bivariate
analyses, were included in multiple logistic regression analyses to adjust for
possible confounding factors (173,177).

67
Confounding factors are sometimes regarded as sources of bias (173,174). A
confounding factor is an extraneous variable that is correlated with the
investigated variable of interest as well as with the outcome. If an existing
confounding factor is not regarded in the analyses, a false association
between the investigated variable and the outcome might appear. Despite the
use of multiple logistic regressions, it is often difficult to rule out all possible
confounding factors, since many confounding factors are still unknown
(173).
It has been suggested, though not established, that when analyzing many
possible risk factors, the p-value should be diminished in order to reduce the
risk of significant associations appearing by chance (173,177). However, the
tested variables in our study were not included by chance but selected
according to previous study findings (39,56,57,65), suggesting these
variables as possibly associated to our study outcomes.
IgE-tests
The current project was part of a larger longitudinal population-based study,
investigating prevalence and associated risk factors for atopy related
conditions i.e. asthma, rhinitis, eczema and allergic sensitization. To
determine the prevalence of allergic sensitization, the children in the two
municipalities Kiruna and Luleå were invited to a SPT with 10 common
airborne allergens. Further, all children in Kiruna and 25% randomly
selected from Luleå were invited to donate blood for serological analyses and
695 children (71% of invited) participated. To facilitate participation, the
SPTs were performed at the children’s schools.
For the benefit of our project, it would have been preferable to add common
food allergens, especially milk, egg, cod and wheat to the SPT panel and this
was also discussed prior to study start. However, even though SPT with food
allergens are considered to be a safe procedure in recent management
guidelines (178), anaphylactic reactions during SPT with food allergens have
been described. During my 15 years practice as a pediatric allergist I have
witnessed two cases of anaphylaxis caused by SPT with food allergens, one
triggered by hen’s egg and the other by cod. Since severe reactions due to
SPT with food allergens are rare and when early recognized, fairly easily
treated, we would not have considered this a problem if the study SPT had
been performed in a health care facility. However, in this study SPTs were
made on 1700 children and performed at the children’s schools, some
located very far from a Health Care Center. During these circumstances we
could not guarantee the tests to be completely safe for the study participants.

68
In a previous pediatric OLIN cohort study the correlation between a positive
SPT and a specific IgE > 0.35 KU/L to aeroallergens included in the SPT was
validated and found to be excellent (179). Therefore, instead of including
foods in our SPT panels, food-specific IgE-analyses were added to the
serological tests in the random population sample (n=695).
With the exception of Paper V, specific IgE was only analyzed to the crude
food allergens. Before study start, analyses of specific IgE to allergen
molecules were also discussed for Papers II-IV. We did not, however,
prioritize this since by that time, only a few IgE-tests for molecular allergens
in foods were commercially available and the knowledge about their
usefulness in food allergy diagnostics was limited (126). There is however a
need for population based studies investigating the prevalence of IgE-
sensitization to these newly discovered allergenic molecules and how they
relate to the presence of allergic symptoms, for food allergens as well as
inhalant allergens (180). There is also a need for clinical research
investigating whether patterns and levels of IgE-sensitization to different
molecular food allergens might be useful in predicting food challenge
outcomes (126).
Validation of reported data
Another major strength of this project is the validation of reported data on
allergy to milk, egg, cod and wheat, first with the more easily available
clinical examinations and serological tests and then further with DBPCFCs
(135,178). The FHS phenotyping following the clinical examination and
serological tests, was useful for identifying the children with current food
allergy who were invited for further evaluation with a DBPCFC series. The
categorization also gave us a good overview of the distribution of FHS
phenotypes underlying reported hypersensitivity to milk, egg, cod and wheat
in the examined cohort.
Previous studies have reported that the prevalence of perceived food allergy
exceeds that of challenge-proven allergy (9,15,16) and the use of DBPCFC
renders the lowest prevalence (9,135). However, even though considered
gold standard for diagnosing food allergy, DBPCFC are rarely used in daily
clinical practice and until recently, few population based studies have
validated reported food allergy with double-blind challenges (15,16,181).
In Paper III, we used a DBPCFC series to validate reported allergy to milk,
egg, cod and wheat. Since our resources were limited, we chose to focus on
these four basic foods due to the high reported prevalence of FHS to milk,
egg, cod and wheat in this cohort (36), the possible negative nutritional

69
effects of elimination of these foods (182-184) and the lack of knowledge
about the phenotypes underlying perceived FHS to milk, egg, cod, and wheat
in schoolchildren (4,12). The omitted validation of the other FHS phenotypes
could be considered a study limitation, as could the exclusion of allergies to
other foods. However, validating all FHS phenotypes or including
hypersensitivity to more foods was not possible in our project. Instead, this
will be an eligible task for future population based studies on food
hypersensitivity.
The DBPCFC methodology
When we planned this study, very few validated recipes for DBPCFC in
children were available, whereof the wheat recipe required baking and no
validated recipe at all was available for cod (185). Therefore we developed
our own DBPCFC recipes, which were successfully validated regarding
detectable sensorial differences between the active and placebo substances in
a separate cohort of healthy schoolchildren (n=275) in Paper I.
The recipes all contained the same liquid amino acid based product with
supplementary ingredients to disguise the taste and texture of the challenge
food. The use of a liquid test substance made it easy to prepare and easy to
dose. The limitation was the difficulty to hide a large enough amount of
challenge food in a drinkable amount of test substance. Therefore, the doses
of allergenic food given during the DBPFC sessions were low, ranging from
2.0-2.4 g of food protein. The challenge foods, except for cod, was used in
raw form in order to keep their allergenicity (186) and to increase the
sensitivity of the test, the DBPCFC was performed as a 3-session challenge
series including two challenge occasions with active substance (114,187).
Cytokine mRNA expression in PBMC
In Paper V, we chose to measure cytokine mRNA expression profiles in
PBMCs instead of measuring levels of biologically active cytokine proteins. The rationale for this decision was the high sensitivity and specificity of qRT-
PCR as a method and access to a well-established qRT-PCR for measurement
of cytokine mRNA expression. Importantly, a previous study by our group,
showed an excellent correlation between the levels of cytokine mRNA
measured by this method and detected levels of corresponding cytokines at
the protein levels (188).
The strengths of the study in Paper V, were the broad palette of cytokines
and fecal markers analyzed before and after in vivo stimulation with relevant
food allergens and the well-defined study participants. A study weakness was

70
that the study groups were small and the children heterogeneous according
to type of food allergy, symptom severity, challenge food and the serving
order of test samples during the DBPCFC series. The limited number of
participants was due to a low prevalence of allergy to basic foods, even
though we initially invited all children with reported allergy to milk, egg, cod
and wheat from a large population-based cohort with a high prevalence of
reported FHS to these foods. The difference in the serving order of active and
placebo substances was a consequence of serving orders being drawn by lot,
which was necessary to achieve a double-blind food challenge series (135).
The transport time was an important issue in our study, since the food
challenges were performed in hospitals 250-500 km from the laboratory that
performed the cytokine analyses. Thus, for practical and logistic reasons, the
post challenge samples in our study were collected one week after the
completed challenge series. The optimal time for measuring post challenge
biomarkers is a matter of discussion. The mRNA expression of different
cytokines peaks at different time intervals, which are different depending on
the detection method used. A Polish study investigating cytokine protein
levels in sera, showed a significant increase in the levels of IL-4 and IL-5
following double-blind challenges with active substance but not with placebo
in children with asthma and IgE-mediated food allergy. The maximum
secretion for these cytokines were seen after 24 hours (162). In contrary, the
levels of fecal inflammatory markers and specific IgE and IgG4 are likely to
peak weeks after allergen exposure (87,90,141,142).
Analyses of fecal biomarkers
For the analyses of inflammatory and tolerogenic markers fecal markers we
used commercially available ELISA methods (Immundiagnostik, Bensheim,
Germany). The ELISA method is the conventional method used for detecting
fecal calpotectin levels in inflammatory bowel disease, though other, more
repid tests are emerging on the market. A previous study showed that the
sensitivity and specificity is somewhat different in different methods of
measuring fecal calprotetin and that the same detection method therefore
should be used when comparing fecal levels of calprotectin at different time
intervals or between individuals (189).

71
Discussion of main results
Epidemiology of food hypersensitivity
The prevalence of parentally reported FHS in this population-based cohort
in Northern Sweden was high, 21%, at 7-8 years of age and even higher, 26%,
at 11-12 years of age. Although the majority of children with allergies to basic
foods i.e. milk and egg develop tolerance before school age (5,15) and lactose
intolerance is thought to be uncommon among Swedish schoolchildren (31),
the prevalence of reported hypersensitivity to milk, egg, cod and wheat
increased from 10% at 7-8 years of age to almost 15% at 11-12 years of age.
The prevalence of reported FHS to basic foods found in this study was high
compared to other studies on older schoolchildren and adolescents (9,11,16).
According to our definition, the prevalence of reported allergy to the basic
foods: milk, egg, cod and wheat at 11-12 years of age was 4.8%. When
validated with a clinical examination and analyses of food specific IgE and a
celiac screen test, the prevalence of current allergy to these foods was 1.4%.
This prevalence was further halved following a DBPCFC series. The
prevalence of challenge-proven allergy to milk, egg, cod and wheat of 0.6%
was consistent or somewhat lower compared to the few other studies using a
similar study approach (9,16,181) and 25-fold lower than the prevalence of
reported hypersensitivity to these foods in our study cohort.
In Papers III and IV we showed that current food allergy was an uncommon
cause of reported hypersensitivity to milk, egg, cod and wheat. The most
common FHS phenotypes were probable lactose intolerance followed by
outgrown allergy. At the time of the evaluation, children with outgrown
allergy could tolerate a portion size of the culprit food without any
symptoms, but they had nevertheless remained on an elimination diet. This
is consistent with previous studies, showing that many children with food
allergy keep avoiding the culprit food even after they have become tolerant
(133).
In Paper IV we also showed that milk allergy, current or outgrown, was
associated with a lower BMI compared to children not avoiding milk. A
possible reason for this finding is that children with milk allergy had
eliminated dairy products since very early life and still were avoiding them,
even though children with outgrown milk allergy probably did not have to.
This finding is in line with other studies showing that a milk eliminated diet
due to allergy may lead to impaired growth and lower intake of important
nutrients like vitamin D (182-184, 190).

72
Of the children in Paper IV still avoiding milk, 43% reported that their milk
hypersensitivity had been diagnosed by a physician and a previous physician
diagnosis was more common among children who were categorized as
having milk allergy. Only 2 % of the children reported that their milk
hypersensitivity had been established by an oral challenge and 9% of the
children still avoiding milk, reported that they had ever been referred to a
dietician for nutritional advice. Together, these data supports previous
findings that food hypersensitivity diagnoses given early in life may have
dietary and nutritional consequences in adolescence (189,191) and pinpoints
the importance of following up and properly evaluating medical advice given
regarding elimination of basic foods (5,192,193).
In Paper III, four out of nine children with a positive challenge outcome
reacted with anaphylaxis. The food-specific IgE among these children were
moderately elevated, ranging from 3.3-13.1 kU/L. This is consistent with the
findings of others, showing that food allergy severity cannot be determined
by the level of specific IgE (90,122,128). None of the children who reacted
with anaphylaxis had reported previous anaphylactic reactions to the
challenge food and only one of them had been prescribed an epinephrine
auto-injector. None of these children were on daily medication for their
concomitant asthma. These findings highlight the importance of recurrent
evaluations of children with suspected food allergy (5,116).
By the time of the structured interviews in Paper IV, 30% of the children
reporting milk avoidance due to perceived hypersensitivity at the Child
interview, had discontinued their milk-eliminated diet. All of these children
had previously reported partial milk avoidance. Stated reasons for
discontinuing the milk elimination diet were that the children had tried to
eliminate milk during a period, seeking alleviation for various symptoms, but
had found that the elimination diet did not result in any improvement or
that they were symptom-free independently of diet. This high prevalence of
discontinued milk elimination was in line with our findings in Paper II,
where we found a high incidence (15%) as well as a high remission (33%) of
parentally reported FHS between 7-8 years to 11-12 years of age. This pattern
was recognizable for hypersensitivity to many of the investigated foods, but
was most obvious for reported hypersensitivity to milk.
Reported hypersensitivity to milk had different symptom patterns as well as
different associated risk factors compared to non-milk FHS. In Paper II,
incidence of non-milk FHS was associated with allergic heredity as well as
current rhinitis and allergic sensitization, while asthma and allergic
sensitization were negatively associated with the remission of non-milk FHS.
73
Similar relationships between atopy related conditions and prevalence of
FHS have been found by others (35,37), although there is a lack of
population-based studies investigating risk factors associated with incidence
and remission of FHS in older schoolchildren and adolescents (15,19).
Neither incidence nor remission of milk FHS were associated with any other
atopy-related conditions. A possible explanation for this finding could be
that the current allergy phenotype was more common among children with
non-milk FHS compared to children with milk FHS (20,194). In Paper IV,
where children avoiding milk due to perceived hypersensitivity were sorted
into different milk hypersensitivity phenotypes, only 3% of these children
were categorized as current milk allergy and 23% as outgrown milk allergy.
The most common phenotype was probable lactose intolerance. While milk
allergy, current or outgrown, was associated with a number of atopy related
variables, children in the probable lactose intolerance phenotype were less
sensitized to aeroallergens and food allergens compared to children not
avoiding milk.
Female sex was associated with incidence of any FHS, non-milk FHS and
milk FHS. It was also associated with milk avoidance due to perceived
hypersensitivity as well as having a milk allergy phenotype at 11-12 years of
age. This is in line with the findings of others, showing that while IgE-
sensitization to food allergens and food allergy is more common among
younger boys than girls, food allergy is more common among adolescent
girls and women compared to men (59,66). The reason for this shift is
unknown, but thought to be related to hormonal factors (67). In addition,
previous studies have shown that women more often report symptoms of
lactose intolerance than men (70,72).
In Paper II, we also investigated the relationship between IgE-sensitization
to milk, egg, soy, cod, wheat and peanut and parentally reported symptoms
to the corresponding food in their child. Generally, there was a poor
agreement between reported symptoms and a positive specific IgE to the
culprit food and the agreement was weakest for milk, soy and wheat. This is
consistent with other studies (90, 195) as well as with our findings in Paper
III and IV showing that current IgE-mediated allergy was an uncommon
course of reported hypersensitivity to basic foods in this cohort of 11-12 year
olds.
Diagnosing food allergy
In this project, we successfully validated recipes for low-dose DBPCFC with
cow’s milk, hen’s egg, soy, cod and wheat in children. These recipes were

74
then used in DBPCFC series for validating reported allergy to basic foods,
but the validation of our recipes has also allowed a spread of these recipes in
order to facilitate the use of DBPCFC in daily clinical practice. It has been
shown in previous studies that the performance of an oral food challenge can
reduce the fear of future adverse reactions to the culprit food but may also
improve quality of life in families with children with suspected food allergy
(196). Even though DBPCFCs are considered gold standard for diagnosing or
ruling out food allergy, the methodology has not yet been fully standardized
(135,136). The access to validated DBPCFC recipes may facilitate such a
standardization, which will make results from studies using DBPCFCs easier
to compare.
Since DBPCFCs are time and resource consuming, there is a search of
objective prognostic markers that could predict challenge outcome and
thereby make DBPCFCs superfluous. In Paper V, we showed that the
baseline mRNA levels of the Th2-related cytokine IL-13 were higher in
children with challenge-proven food allergy compared to children with a
negative challenge outcome compared to healthy controls. It has been shown
in other studies that high levels of IL-13 are expressed after stimulation of
PBMCs with relevant food allergens in food allergic patients and that the IL-
13 level decreases after tolerance development (163,164). In addition,
Metcalfe et al recently showed that an elevated egg-specific Th2 cytokine
response – of IL-13 and IL-5 in particular – at 4 months of age could predict
egg allergy at 12 months of age (161), which could be in line with our
findings.
Further, we showed that the expressed mRNA level of the regulatory
cytokine IL-10 at baseline was higher among children with challenge-proven
food allergy compared to children with a negative challenge outcome. Higher
IL-10 levels have been shown following stimulation of PBMCs with cow’s
milk protein in children with IgE-mediated cow’s milk allergy compared to
children with non-IgE mediated milk allergy (163,197) and in children
during tolerance development compared to children with symptomatic food
allergy (164).Previous studies have also shown that after stimulation of
PBMCs with specific food allergens the expression of the Th2 cytokine
pattern is enhanced and the expressed levels of the regulatory cytokine IL-10
diminished in children with symptomatic IgE-mediated allergy compared to
children who have developed tolerance (107,161). Due to its active role in
tolerance development, IL-10 has been discussed as a possible biomarker for
symptomatic IgE-mediated food allergy (101). However, since data are not
univocal and study results vary with study population and investigated food
(108,164,198) it has been suggested that analyzing IL-10 as part of a broader
Th2-profile would be preferable (103,199,200).

75
In Paper V, we also investigated the fecal levels of EDN as a marker of
eosinophilic inflammation and calprotectin as a marker of neutrophilic
inflammation of the gastrointestinal tract, in relation to DBPCFC outcome.
The baseline levels of EDN and the baseline and post challenge levels of fecal
calprotectin were almost twice as high among children with a positive
compared to a negative challenge outcome, although none of these
differences reached statistical significance. This was probably due to a lack
of power caused by the low number of participants toghether with the large
natural variance in faecal calprotectin levels (141,189). Our findings are,
however, in line with the results from other studies showing that fecal levels
of EDN might be used as a marker of food allergic reactions (139,140) and
that measurement of fecal calprotectin can be a helpful tool in the follow-up
of response to treatment and determination of reoccurrence of cow’s milk
allergy (141,142).
Ethical considerations
The benefit of our study participants was the possibility to be diagnosed or
freed from a suspected allergy to basic foods by the use of gold standard
methods (5,116). To secure the safety of our study participants during
DBPCFC, the double-blind challenges were performed in a hospital setting
with drugs and equipment for the treatment of allergic symptoms, including
anaphylaxis, immediately available. Also, the same experienced allergist
(AW) and allergy nurse (AS) were responsible at all challenge occasions.
Before each challenge occasion, an intravenous line was set in case of need to
administer intravenous drugs or rehydration fluids. This intravenous line
was also used for blood sampling when appropriate, to avoid unnecessary
venous punctures. Children with positive tTGA-tests and no previous
diagnosis of celiac disease, were informed about the test result and referred
to a pediatric clinic for further investigation.
The children participating in the validation of our DBPCFC recipes and the
analyses of cytokine mRNA expressions, had no immediate personal benefits
of participating in the study, neither were they exposed to any health-related
risks caused by their participation, except for the discomfort of donating
blood samples in Paper 5. These children have, however, contributed to
research that will hopefully improve future diagnostics and care-taking of
children with suspected food allergy and consequently decrease unnecessary
food avoidance.
76

77
Personal point of closure
I have learned a lot during these years of doctoral studies, adding new
dimensions to my clinical work. A better understanding of food
hypersensitivity in schoolchildren, its prevalence, clinical expressions and
underlying phenotypes has increased the interest and engagement in our
allergy team to disentangle the cause of adverse reactions to foods in our
pediatric patients and to improve our diagnostic methods. The most
significant lessons I have learned during this project were that perceived
food hypersensitivity to basic foods was even more common, and that the
percentage of children with current allergy to these foods lower, than I first
thought. Further, that medical advice on food avoidance early in life, may
have nutritional consequences in adolescence.
Even though I find our attempts to diagnose or free children with suspected
food hypersensitivity important, this study has made me realize that to
achieve significant changes, we have to start much earlier on. Since most
children with allergies to basic foods develop tolerance before school age and
since the older the child the more difficult it is for them to accept new tastes
and textures, we must become better at evaluating diagnostic elimination
diets and at following-up children with suspected food hypersensitivity to
avoid unnecessary food avoidances. It is of course not necessary for everyone
to eat all kinds of foods, but since I believe it to be a good start of a healthy
relationship to food, I want as many children as possible to have the
opportunity to do so. Following-up and properly diagnosing children with
suspected food hypersensitivity will also diminish the risk of children with
severe food allergy being disbelieved and thereby liable to risks of
unnecessary exposure to the culprit food.
Our developed recipes for double-blind challenges in children have been
used frequently in our daily clinical practice and the validation of these
recipes has allowed a spread to other clinics in the country. Further, we have
gained knowledge about how schoolchildren experience food hyper-
sensitivity and food avoidance, which has facilitated improvement of our
patient follow-ups. The upcoming theses of my friend and colleague Åsa
Strinnholm, will contribute additional knowledge on quality of life in
adolescents with perceived food allergy. Also, continuous studies and new
research from the OLIN group and the department of Pediatrics, Umeå
University will contribute to future knowledge on epidemiology and risk
factors of food hypersensitivity – and I will probably not be able to keep my
fingers out of that jar…

78

79
Acknowledgements
Thank You…
To Our Study Participants
…to all of the families answering our Call
Without you this Work would be nothing at all
To the OLIN family
…for selflessly sharing your research skills
…for dragging and pushing me over the hills
To the OLIN “study personnel”
…you´re the true heroes – one must understand
Collectors of data from “Nowhereland”
To Annika and Anette
at the department of Food and Nutrition
…for successfully blindfolding class after class
…for the excellent taste of working with us
To Lucia, Olga, Ivan, Ignacio, Catharina and Agneta
at the department of Immunology
…for handling our samples – and doing it well
…for teaching me methods I hardly can spell

80
Thank You…
To Catarina, Yvonne and the other amazing ladies
at the “Pediatric Research Unit”
…for always having a hand to lend
…for being the pillars upon who we depend
To Ulla, Karin, Elisabeth, Carina, Tove and Marlene
…for unvaluable help and for keeping all
the “beg, steel and borrowing” under control
To my PhD-student collegues
…for the scanning of papers – for wrongs and for rights
…for fellowship, fun and “Falafel-fights”
To Helena, the best (looking) Statistician ever
…for making logaritms natural, p less bizarre
A statistical lifeboat – that´s what you R
To the best Co-authors ever
…for forbearance and patience, for taking your time
with all of my synonyms – preferably in rhyme
To Christina and Eva, the best Supervisors ever
…for friendship and wisdom – for letting me thrive
For parts of this journey you´ve kept me alive
To Åsa and Lisbeth, my Partners in crime:
…for being my “Sisters in Arms” through the years
rumbling the country – like three musketeers

81
Thank You…
To Per Erik, the best Boss ever
…for all of the hours of research I got
…for believing in me when I – frankly – did not
To my Colleagues at the department of Pediatrics
…for lightening the burdens, for fun of all sorts
…for vivid discussions and friendly supports
To the best Allergy team ever
…my Backbone and Strength – I depend on you all –
to keep everything strictly under control
To the best Pulmonary and Respiratory teams ever
…your cunning and skills reassure that I might
have a nightmare-free, pressure-less sleep every night
To my Mentors: Christian and Stig
…for the sake of deliberately befooling me
into the path of Allergology
To my Gurus: Olle, Solveig and Sten-Erik
…for the answering of questions – giant or small -
whenever I needed a friend to call
To the “Children´s choir”
(or “kväkare utan gränser” or “the unreal group”)
…for the music and also – for good and for worse –
the art of preforming without a rehearse

82
Thank You…
To old and new aquaintances
…to all of the fabulous friends that I´ve got
You´re the “treasure of life” – and I love you a lot
To Karl-Gunnar, Ing-Britt, Pentti, Leena, Per and Ina
…for all your support, all the strings you´ve unnerved
You are Relatives better than I have deserved
To my Brother Olle
…you´re a piece of me missing, distant but near
You´re a part of this too – even though you´re not here
To Mikael, Kalle, Emil and Gustav
…my Husband, my Children – my dear Family
Through all of these Chapters you´ve been there for me
Without your sweet loving – where would I be?

83
Funding
This thesis was funded by:
The Swedish Research Council
The Swedish Heart and Lung Foundation
VISARE Norr
The Swedish Asthma and Allergy Foundation
ALF - a regional agreement between Umeå University and Väster-botten and Norrbotten County Council
FoU - the State Government funding for Health Care research
Norrbotten County Council
The Swedish Society of Medicine
Insamlingsstiftelsen
The Sven Jerring Foundation
The Kempe Foundation
The Oskar foundation
The Anerska Foundation
The Kjerstin Hejdenberg Foundation
Stiftelsen Samariten
BLF – the section for Allergology
Nutricia AB is acknowledged for providing DBPCFC test material
ThermoFisher Diagnostics, Uppsala, Sweden provided funding for parts of the IgE tests and tTGA analyses
84
References
1.Prescott SL, Pawankar R, Allen KJ, Campbell DE, Sinn J, Fiocchi A, et al. A global survey of changing patterns of food allergy burden in children. World Allergy Organ J 2013;6(1):21.
2.Johansson SG, Bieber T, Dahl R, Friedmann PS, Lanier BQ, Lockey RF, et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol 2004;113(5):832-6.
3.Sicherer SH, Sampson HA. Food allergy. J Allergy Clin Immunol 2010;125(2 Suppl 2):S116-25.
4.Nowak-Wegrzyn A, Sampson HA. Adverse reactions to foods. Med Clin North Am. 2006;90(1):97-127.
5.Burks AW, Tang M, Sicherer S, Muraro A, Eigenmann PA, Ebisawa M, et al. ICON: food allergy. J Allergy Clin Immunol 2012;129(4):906-20.
6.Nowak-Wegrzyn A, Katz Y, Mehr SS, Koletzko S. Non-IgE-mediated gastrointestinal food allergy. J Allergy Clin Immunol 2015;135(5):1114-24.
7.Wilt TJ, Shaukat A, Shamliyan T, Taylor BC, MacDonald R, Tacklind J, et al. Lactose intolerance and health. Evid Rep Technol Assess 2010(192):1-410.
8.Mills EN, Mackie AR, Burney P, Beyer K, Frewer L, Madsen C, et al. The prevalence, cost and basis of food allergy across Europe. Allergy. 2007;62(7):717-22.
9.Rona RJ, Keil T, Summers C, Gislason D, Zuidmeer L, Sodergren E, et al. The prevalence of food allergy: a meta-analysis. J Allergy Clin Immunol 2007;120(3):638-46.
10.Enroth S, Dahlbom I, Hansson T, Johansson A, Gyllensten U. Prevalence and sensitization of atopic allergy and coeliac disease in the Northern Sweden Population Health Study. Int J Circumpolar Health. 2013;5(72).
11.Osterballe M, Mortz CG, Hansen TK, Andersen KE, Bindslev-Jensen C. The prevalence of food hypersensitivity in young adults. Pediatr Allergy Immunol 2009;20(7):686-92.
12.Sicherer SH, Sampson HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol 2014;133(2):291-307.
85
13.Prescott S, Allen KJ. Food allergy: riding the second wave of the allergy epidemic. Pediatr Allergy Immunol 2011;22(2):155-60.
14.Nwaru BI, Hickstein L, Panesar SS, Muraro A, Werfel T, Cardona V, et al. The epidemiology of food allergy in Europe: a systematic review and meta-analysis. Allergy 2014;69(1):62-75.
15.Schoemaker AA, Sprikkelman AB, Grimshaw KE, Roberts G, Grabenhenrich L, Rosenfeld L, et al. Incidence and natural history of challenge-proven cow's milk allergy in European children - EuroPrevall birth cohort. Allergy 2015;70(8):963-72.
16.Nwaru BI, Hickstein L, Panesar SS, Roberts G, Muraro A, Sheikh A. Prevalence of common food allergies in Europe: a systematic review and meta-analysis. Allergy 2014;69(8):992-1007.
17.Allen KJ, Koplin JJ. The epidemiology of IgE-mediated food allergy and anaphylaxis. Immunol Allergy Clin North Am 2012;32(1):35-50.
18.Eller E, Kjaer HF, Host A, Andersen KE, Bindslev-Jensen C. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy 2009;64(7):1023-9.
19.Venter C, Pereira B, Voigt K, Grundy J, Clayton CB, Higgins B, et al. Prevalence and cumulative incidence of food hypersensitivity in the first 3 years of life. Allergy 2008;63(3):354-9.
20.Elizur A, Rajuan N, Goldberg MR, Leshno M, Cohen A, Katz Y. Natural course and risk factors for persistence of IgE-mediated cow's milk allergy. J Pediatr 2012;161(3):482-7.
21.Skripak JM, Matsui EC, Mudd K, Wood RA. The natural history of IgE-mediated cow's milk allergy. J Allergy Clin Immunol 2007;120(5):1172-7.
22.Kattan JD, Cocco RR, Jarvinen KM. Milk and soy allergy. Pediatr Clin North Am 2011;58(2):407-26.
23.Ho MH, Wong WH, Heine RG, Hosking CS, Hill DJ, Allen KJ. Early clinical predictors of remission of peanut allergy in children. J Allergy Clin Immunol 2008;121(3):731-6.
24.Hourihane JO. Peanut allergy. Pediatr Clin North Am 2011;58(2):445-58.
25.Geroldinger-Simic M, Zelniker T, Aberer W, Ebner C, Egger C, Greiderer A, et al. Birch pollen-related food allergy: clinical aspects and the role of allergen-specific IgE and IgG4 antibodies. J Allergy Clin Immunol 2011;127(3):616-22.

86
26.Warm K, Backman H, Lindberg A, Lundbäck B, Rönmark E. Low incidence and high remission of allergic sensitization among adults. J Allergy Clin Immunol 2012;129(1):136-42.
27.Rönmark E, Bjerg A, Perzanowski M, Platts-Mills T, Lundbäck B. Major increase in allergic sensitization in schoolchildren from 1996 to 2006 in northern Sweden. J Allergy Clin Immunol 2009;124(2):357-63, 63.
28.Allen KJ, Davidson GP, Day AS, Hill DJ, Kemp AS, Peake JE, et al. Management of cow's milk protein allergy in infants and young children: an expert panel perspective. J Paediatr Child Health. 2009;45(9):481-6.
29.Katz Y, Goldberg MR, Rajuan N, Cohen A, Leshno M. The prevalence and natural course of food protein-induced enterocolitis syndrome to cow's milk: a large-scale, prospective population-based study. J Allergy Clin Immunol 2011;127(3):647-53.
30.Ingram CJ, Mulcare CA, Itan Y, Thomas MG, Swallow DM. Lactose digestion and the evolutionary genetics of lactase persistence. Hum Genet 2009;124(6):579-91.
31.Vuorisalo T, Arjamaa O, Vasemägi A, Taavitsainen JP, Tourunen A, Saloniemi I. High lactose tolerance in North Europeans: a result of migration, not in situ milk consumption. Perspect Biol Med 2012;55:163-74.
32.Almon R, Engfeldt P, Tysk C, Sjöstrom M, Nilsson TK. Prevalence and trends in adult-type hypolactasia in different age cohorts in Central Sweden diagnosed by genotyping for the adult-type hypolactasia-linked LCT -13910C > T mutation. Scand J Gastroenterol 2007;42(2):165-70.
33.Carroccio A, Montalto G, Cavera G, Notarbatolo A. Lactose intolerance and self-reported milk intolerance: relationship with lactose maldigestion and nutrient intake. Lactase Deficiency Study Group. J Am Coll Nutr 1998;17(6):631-6.
34.Paajanen L, Korpela R, Tuure T, Honkanen J, Järvelä I, Ilonen J, et al. Cow milk is not responsible for most gastrointestinal immune-like syndromes--evidence from a population-based study. Am J Clin Nutr 2005;82(6):1327-35.
35.Östblom E, Lilja G, Pershagen G, van Hage M, Wickman M. Phenotypes of food hypersensitivity and development of allergic diseases during the first 8 years of life. Clin Exp Allergy 2008;38(8):1325-32.
87
36.Strinnholm Å, Winberg A, West C, Hedman L, Rönmark E. Food hypersensitivity is common in Swedish schoolchildren, especially oral reactions to fruit and gastrointestinal reactions to milk. Acta Paediatr 2014;103(12):1290-6.
37.Soost S, Leynaert B, Almqvist C, Edenharter G, Zuberbier T, Worm M. Risk factors of adverse reactions to food in German adults. Clin Exp Allergy 2009;39(7):1036-44.
38.Sandin A, Annus T, Björksten B, Nilsson L, Riikjarv MA, van Hage-Hamsten M, et al. Prevalence of self-reported food allergy and IgE antibodies to food allergens in Swedish and Estonian schoolchildren. Eur J Clin Nutr 2005;59(3):399-403.
39.Tan TH, Ellis JA, Saffery R, Allen KJ. The role of genetics and environment in the rise of childhood food allergy. Clin Exp Allergy 2012;42(1):20-9.
40.Fuertes E, Standl M, von Berg A, Lehmann I, Hoffmann B, Bauer CP, et al. Parental allergic disease before and after child birth poses similar risk for childhood allergies. Allergy 2015;70(7):873-6.
41.Hong X, Tsai HJ, Wang X. Genetics of food allergy. Curr Opin Pediatr 2009;21(6):770-6.
42.West CE, Renz H, Jenmalm MC, Kozyrskyj AL, Allen KJ, Vuillermin P, et al. The gut microbiota and inflammatory noncommunicable diseases: associations and potentials for gut microbiota therapies. J Allergy Clin Immunol 2015;135(1):3-13.
43.Wold AE. The hygiene hypothesis revised: is the rising frequency of allergy due to changes in the intestinal flora? Allergy. 1998;53:20-5.
44.Laursen MF, Zachariassen G, Bahl MI, Bergström A, Host A, Michaelsen KF, et al. Having older siblings is associated with gut microbiota development during early childhood. BMC Microbiol. 2015;15(154):015-0477.
45.Campbell BE, Lodge CJ, Lowe AJ, Burgess JA, Matheson MC, Dharmage SC. Exposure to 'farming' and objective markers of atopy: a systematic review and meta-analysis. Clin Exp Allergy 2015;45(4):744-57.
46.Amberbir A, Medhin G, Abegaz WE, Hanlon C, Robinson K, Fogarty A, et al. Exposure to Helicobacter pylori infection in early childhood and the risk of allergic disease and atopic sensitization: a longitudinal birth cohort study. Clin Exp Allergy 2014;44(4):563-71.

88
47.Lynch SV, Wood RA, Boushey H, Bacharier LB, Bloomberg GR, Kattan M, et al. Effects of early-life exposure to allergens and bacteria on recurrent wheeze and atopy in urban children. J Allergy Clin Immunol 2014;134(3):593-601.
48.Pyrhönen K, Näyhä S, Hiltunen L, Läärä E. Caesarean section and allergic manifestations: insufficient evidence of association found in population-based study of children aged 1 to 4 years. Acta Paediatr 2013;102(10):982-9.
49.West CE, Jenmalm MC, Prescott SL. The gut microbiota and its role in the development of allergic disease: a wider perspective. Clin Exp Allergy 2015;45(1):43-53.
50.Koplin JJ, Dharmage SC, Ponsonby AL, Tang ML, Lowe AJ, Gurrin LC, et al. Environmental and demographic risk factors for egg allergy in a population-based study of infants. Allergy. 2012.
51.Sharief S, Jariwala S, Kumar J, Muntner P, Melamed ML. Vitamin D levels and food and environmental allergies in the United States: results from the National Health and Nutrition Examination Survey 2005-2006. J Allergy Clin Immunol 2011;127(5):1195-202.
52.Allen KJ, Koplin JJ, Ponsonby AL, Gurrin LC, Wake M, Vuillermin P, et al. Vitamin D insufficiency is associated with challenge-proven food allergy in infants. J Allergy Clin Immunol 2013;131(4):1109-16.
53.Magnusson J, Kull I, Westman M, Håkansson N, Wolk A, Melen E, et al. Fish and polyunsaturated fat intake and development of allergic and nonallergic rhinitis. J Allergy Clin Immunol 2015. Epub 2015/07/15.
54.Lack G, Plaut M, Sayre PH. Peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015;372(22):2165-6.
55.Palmer DJ, Metcalfe J, Makrides M, Gold MS, Quinn P, West CE, et al. Early regular egg exposure in infants with eczema: A randomized controlled trial. J Allergy Clin Immunol. 2013;132(2):387-92.
56.Lack G. Update on risk factors for food allergy. J Allergy Clin Immunol 2012;129(5):1187-97.
57.Ben-Shoshan M, Soller L, Harrington DW, Knoll M, La Vieille S, Fragapane J, et al. Eczema in early childhood, sociodemographic factors and lifestyle habits are associated with food allergy: a nested case-control study. Int Arch Allergy Immunol 2015;166(3):199-207.
58.Just J, Deslandes-Boutmy E, Amat F, Desseaux K, Nemni A, Bourrat E, et al. Natural history of allergic sensitization in infants with early-onset atopic
89
dermatitis: results from ORCA Study. Pediatr Allergy Immunol 2014;25(7):668-73.
59.Liu AH, Jaramillo R, Sicherer SH, Wood RA, Bock SA, Burks AW, et al. National prevalence and risk factors for food allergy and relationship to asthma: results from the National Health and Nutrition Examination Survey 2005-2006. J Allergy Clin Immunol 2010;126(4):798-806.
60.Pinart M, Benet M, Annesi-Maesano I, von Berg A, Berdel D, Carlsen KC, et al. Comorbidity of eczema, rhinitis, and asthma in IgE-sensitised and non-IgE-sensitised children in MeDALL: a population-based cohort study. The Lancet Respir Med 2014;2(2):131-40.
61.Santos A, Dias A, Pinheiro JA. Predictive factors for the persistence of cow's milk allergy. Pediatr Allergy Immunol. 2010;21(8):1127-34.
62.Pyrhönen K, Hiltunen L, Kaila M, Näyhä S, Läärä E. Heredity of food allergies in an unselected child population: an epidemiological survey from Finland. Pediatr Allergy Immunol 2011;22(1 Pt 2):e124-32.
63.Goldberg M, Eisenberg E, Elizur A, Rajuan N, Rachmiel M, Cohen A, et al. Role of parental atopy in cow's milk allergy: a population-based study. Ann Allergy Asthma Immunol 2013;110(4):279-83.
64.Ashley S, Dang T, Koplin J, Martino D, Prescott S. Food for thought: progress in understanding the causes and mechanisms of food allergy. Curr Opin Allergy Clin Immunol 2015;15(3):237-42.
65.Kumar R, Tsai HJ, Hong X, Liu X, Wang G, Pearson C, et al. Race, ancestry, and development of food-allergen sensitization in early childhood. Pediatrics 2011;128(4):e821-9.
66.DunnGalvin A, Hourihane JO, Frewer L, Knibb RC, Oude Elberink JN, Klinge I. Incorporating a gender dimension in food allergy research: a review. Allergy 2006;61(11):1336-43.
67.Chen W, Mempel M, Schober W, Behrendt H, Ring J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy 2008;63(11):1418-27.
68.Allen KJ, Martin PE. Clinical aspects of pediatric food allergy and failed oral immune tolerance. J Clin Gastroenterol 2010;44(6):391-401.
69.Haberkorn BC, Ermens AA, Koeken A, Cobbaert CM, van Guldener C. Improving diagnosis of adult-type hypolactasia in patients with abdominal complaints. Clin Chem Lab Med 2011;50(1):119-23.
90
70.Baadkar SV, Mukherjee MS, Lele SS. Study on influence of age, gender and genetic variants on lactose intolerance and its impact on milk intake in adult Asian Indians. Ann Hum Biol 2014;41(6):548-53.
71.Rasinperä H, Saarinen K, Pelkonen A, Järvelä I, Savilahti E, Kolho KL. Molecularly defined adult-type hypolactasia in school-aged children with a previous history of cow's milk allergy. World J Gastroenterol 2006;12(14):2264-8.
72.Barr SI. Perceived lactose intolerance in adult Canadians: a national survey. Appl Physiol Nutr Metab 2013;38(8):830-5.
73.Kaiko GE, Horvat JC, Beagley KW, Hansbro PM. Immunological decision-making: how does the immune system decide to mount a helper T-cell response? Immunology 2008;123(3):326-38.
74.Houghteling PD, Walker WA. From Birth to "Immunohealth," Allergies and Enterocolitis. J Clin Gastroenterol 2015;49(1):S7-S12.
75.Annunziato F, Romagnani P, Cosmi L, Lazzeri E, Romagnani S. Chemokines and lymphopoiesis in human thymus. Trends Immunol 2001;22(5):277-81.
76.Rothenberg EV. Stepwise specification of lymphocyte developmental lineages. Curr Opin Genet Dev 2000;10(4):370-9.
77.Mosmann TR, Kobie JJ, Lee FE, Quataert SA. T helper cytokine patterns: defined subsets, random expression, and external modulation. Immunol Res 2009;45(2-3):173-84.
78.Akdis M, Verhagen J, Taylor A, Karamloo F, Karagiannidis C, Crameri R, et al. Immune responses in healthy and allergic individuals are characterized by a fine balance between allergen-specific T regulatory 1 and T helper 2 cells. J Exp Med 2004;199(11):1567-75.
79.Schmidt-Weber CB, Akdis M, Akdis CA. TH17 cells in the big picture of immunology. J Allergy Clin Immunol 2007;120(2):247-54.
80.Hinks TS, Zhou X, Staples KJ, Dimitrov BD, Manta A, Petrossian T, et al. Innate and adaptive T cells in asthmatic patients: Relationship to severity and disease mechanisms. J Allergy Clin Immunol 2015;136(2):323-33.
81.79.Akdis M, Blaser K, Akdis CA. T regulatory cells in allergy: novel concepts in the pathogenesis, prevention, and treatment of allergic diseases. J Allergy Clin Immunol 2005;116(5):961-8.
91
82.Palomares O, Martin-Fontecha M, Lauener R, Traidl-Hoffmann C, Cavkaytar O, Akdis M, et al. Regulatory T cells and immune regulation of allergic diseases: roles of IL-10 and TGF-beta. Genes Immun 2014;15(8):511-20.
83.Pandiyan P, Zhu J. Origin and functions of pro-inflammatory cytokine producing Foxp3(+) regulatory T cells. Cytokine 2015;76(1):13-24.
84.Huang W, August A. The signaling symphony: T cell receptor tunes cytokine-mediated T cell differentiation. J Leukoc Biol 2015;97(3):477-85.
85.Zhang H, Kong H, Zeng X, Guo L, Sun X, He S. Subsets of regulatory T cells and their roles in allergy. J Transl Med 2014;12(125):1479-5876.
86.Yao Y, Vent-Schmidt J, McGeough MD, Wong M, Hoffman HM, Steiner TS, et al. Tr1 Cells, but Not Foxp3+ Regulatory T Cells, Suppress NLRP3 Inflammasome Activation via an IL-10-Dependent Mechanism. J Immunol 2015;195(2):488-97.
87.Kumar S, Verma AK, Das M, Dwivedi PD. Molecular mechanisms of IgE mediated food allergy. Int Immunopharmacol 2012;13(4):432-9.
88.Kim EH, Burks W. Immunological basis of food allergy (IgE-mediated, non-IgE-mediated, and tolerance). Chem Immunol Allergy 2015;101:8-17.
89.Eigenmann PA. Mechanisms of food allergy. Pediatr Allergy Immunol 2009;20(1):5-11.
90.Sicherer SH, Wood RA. Allergy testing in childhood: using allergen-specific IgE tests. Pediatrics 2012;129(1):193-7.
91.Lorenz AR, Scheurer S, Vieths S. Food allergens: molecular and immunological aspects, allergen databases and cross-reactivity. Chem Immunol Allergy 2015;101:18-29.
92.Heine RG. Gastrointestinal food allergies. Chem Immunol Allergy 2015;101:171-80.
93.MacDonald TT, Di Sabatino A. The immunologic basis for gastrointestinal food allergy. Current opinion in gastroenterology. 2009;25(6):521-6.
94.Bergmann MM, Eigenmann PA. Food allergy in childhood (infancy to school age). Chem Immunol Allergy 2015;101:38-50.
95.O'Shea JJ, Gadina M, Kanno Y. Cytokine signaling: birth of a pathway. J Immunol 2011;187(11):5475-8.

92
96.Galli SJ, Tsai M, Piliponsky AM. The development of allergic inflammation. Nature 2008;454(7203):445-54.
97.Akdis CA, Akdis M. Mechanisms of immune tolerance to allergens: role of IL-10 and Tregs. J Clin Invest 2014;124(11):4678-80
98.Wisniewski J, Agrawal R, Woodfolk JA. Mechanisms of tolerance induction in allergic disease: integrating current and emerging concepts. Clin Exp Allergy 2013;43(2):164-76.
99.Stanic B, van de Veen W, Wirz OF, Ruckert B, Morita H, Sollner S, et al. IL-10-overexpressing B cells regulate innate and adaptive immune responses. J Allergy Clin Immunol 2015;135(3):771-80.
100.Till S. Mechanisms of immunotherapy and surrogate markers. Allergy 2011;66 Suppl 95:25-7.
101.Alonso R, Pineda F, Enrique E, Tella R, Cistero-Bahima A. Usefulness of serum interleukin-10 in determining food tolerance. Allergy 2007;62:710-1.
102.Sommanus S, Kerddonfak S, Kamchaisatian W, Vilaiyuk S, Sasisakulporn C, Teawsomboonkit W, et al. Cow's milk protein allergy: immunological response in children with cow's milk protein tolerance. Asian Pac J Allergy Immunol 2014;32(2):171-7.
103.Tiemessen MM, Van Ieperen-Van Dijk AG, Bruijnzeel-Koomen CA, Garssen J, Knol EF, Van Hoffen E. Cow's milk-specific T-cell reactivity of children with and without persistent cow's milk allergy: key role for IL-10. J Allergy Clin Immunol 2004;113(5):932-9.
104.Lee JH, Noh J, Noh G, Choi WS, Cho S, Lee SS. Allergen-specific transforming growth factor-beta-producing CD19+CD5+ regulatory B-cell (Br3) responses in human late eczematous allergic reactions to cow's milk. J Interferon Cytokine Res 2011;31(5):441-9.
105.Jacob CM, Pastorino AC, Okay TS, Castro AP, Gushken AK, Watanabe LA, et al. Interleukin 10 (IL10) and transforming growth factor beta1 (TGFbeta1) gene polymorphisms in persistent IgE-mediated cow's milk allergy. Clinics 2013;68(7):1004-9.
106.Williams CM, Rahman S, Hubeau C, Ma HL. Cytokine pathways in allergic disease. Toxicol Pathol 2012;40(2):205-15.
107.Schade RP, Van Ieperen-Van Dijk AG, Van Reijsen FC, Versluis C, Kimpen JL, Knol EF, et al. Differences in antigen-specific T-cell responses between infants with atopic dermatitis with and without cow's milk allergy: relevance of TH2 cytokines. J Allergy Clin Immunol 2000;106(6):1155-62.
93
108.Scott-Taylor TH, Hourihane JB, Harper J, Strobel S. Patterns of food allergen-specific cytokine production by T lymphocytes of children with multiple allergies. Clin Exp Allergy 2005;35(11):1473-80.
109.Neaville WA, Tisler C, Bhattacharya A, Anklam K, Gilbertson-White S, Hamilton R, et al. Developmental cytokine response profiles and the clinical and immunologic expression of atopy during the first year of life. J Allergy Clin Immunol 2003;112(4):740-6.
110.Tomicic S, Fälth-Magnusson K, Böttcher MF. Dysregulated Th1 and Th2 responses in food-allergic children--does elimination diet contribute to the dysregulation? Pediatr Allergy Immunol 2010;21(4 Pt 1):649-55.
111.Sampson HA. Food allergy: immunology of the GI mucosa towards classification and understanding of GI hypersensitivities. Pediatr Allergy Immunol 2001;12 Suppl 14:7-9.
112.Saarinen KM, Sarnesto A, Savilahti E. Markers of inflammation in the feces of infants with cow's milk allergy. Pediatr Allergy Immunol 2002;13(3):188-94.
113.Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics 2011;128(1):e9-17.
114.Niggemann B, Beyer K. Pitfalls in double-blind, placebo-controlled oral food challenges. Allergy 2007;62(7):729-32.
115.Kleiman J, Ben-Shoshan M. Food-dependent exercise-induced anaphylaxis with negative allergy testing. BMJ Case Rep 2014;2014.
116.Nowak-Wegrzyn A. Food allergy guidelines and beyond. Immunol Allergy Clin North Am 2012;32(1):xv-xix.
117.Pesek RD, Jones SM. Anaphylaxis in food allergy. Chem Immunol Allergy 2015;101:191-8.
118.Panesar SS, Javad S, de Silva D, Nwaru BI, Hickstein L, Muraro A, et al. The epidemiology of anaphylaxis in Europe: a systematic review. Allergy 2013;68(11):1353-61.
119.Hofmann A, Burks AW. Pollen food syndrome: update on the allergens. Curr Allergy Asthma Rep 2008;8(5):413-7.
120.Asarnoj A, Nilsson C, Lidholm J, Glaumann S, Östblom E, Hedlin G, et al. Peanut component Ara h 8 sensitization and tolerance to peanut. J Allergy Clin Immunol 2012;130(2):468-72.

94
121.Järvinen KM, Nowak-Wegrzyn A. Food protein-induced enterocolitis syndrome (FPIES): current management strategies and review of the literature. J Allergy Clin Immunol 2013;1(4):317-22.
122.Soares-Weiser K, Takwoingi Y, Panesar SS, Muraro A, Werfel T, Hoffmann-Sommergruber K, et al. The diagnosis of food allergy: a systematic review and meta-analysis. Allergy 2014;69(1):76-86.
123.Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S, et al. Diagnostic approach and management of cow's-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines J Pediatr Gastroenterol Nutr 2012;55(2):221-
124.Skypala IJ, Venter C, Meyer R, deJong NW, Fox AT, Groetch M, et al. The development of a standardised diet history tool to support the diagnosis of food allergy. Clin Transl Allergy 2015;5:7.
125.Mehl A, Niggemann B, Keil T, Wahn U, Beyer K. Skin prick test and specific serum IgE in the diagnostic evaluation of suspected cow's milk and hen's egg allergy in children: does one replace the other? Clin Exp Allergy 2012;42(8):1266-72.
126.Borres MP, Sato S, Ebisawa M. IgE-related examination in food allergy with focus on allergen components. Chem Immunol Allergy 2015;101:68-78.
127.Sampson HA, Ho DG. Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents. J Allergy Clin Immunol 1997;100(4):444-51.
128.Bousquet J, Anto JM, Bachert C, Bousquet PJ, Colombo P, Crameri R, et al. Factors responsible for differences between asymptomatic subjects and patients presenting an IgE sensitization to allergens. A GA2LEN project. Allergy 2006;61(6):671-80.
129.Komata T, Söderström L, Borres MP, Tachimoto H, Ebisawa M. The predictive relationship of food-specific serum IgE concentrations to challenge outcomes for egg and milk varies by patient age. J Allergy Clin Immunol 2007;119(5):1272-4.
130.Shreffler WG. Microarrayed recombinant allergens for diagnostic testing. J Allergy Clin Immunol 2011;127(4):843-9.
131.Crameri R. The crux with a reliable in vitro and in vivo diagnosis of allergy. Allergy 2013;68(6):693-4.
132.Wood RA. Diagnostic elimination diets and oral food provocation. Chem Immunol Allergy 2015;101:87-95.

95
133.Eigenmann PA, Caubet JC, Zamora SA. Continuing food-avoidance diets after negative food challenges. Pediatr Allergy Immunol 2006;17(8):601-5.
134.Bird JA, Lack G, Perry TT. Clinical management of food allergy. J Allergy Clin Immunol Pract 2015;3(1):1-11.
135.Nowak-Wegrzyn A, Assa'ad AH, Bahna SL, Bock SA, Sicherer SH, Teuber SS. Work Group report: oral food challenge testing. J Allergy Clin Immunol 2009;123(6 Suppl):S365-83.
136.Venter C. Food hypersensitivity: diagnosing and managing food allergies and intolerances. J Allergy (Cairo) 2012;2012:576017.
137.Papadopoulou A, Koletzko S, Heuschkel R, Dias JA, Allen KJ, Murch SH, et al. Management guidelines of eosinophilic esophagitis in childhood. J Pediatr Gastroenterol Nutr 2014;58(1):107-18.
138.Matsumoto K. Non-IgE-related diagnostic methods (LST, patch test). Chem Immunol Allergy 2015;101:79-86.
139.Majamaa H, Laine S, Miettinen A. Eosinophil protein X and eosinophil cationic protein as indicators of intestinal inflammation in infants with atopic eczema and food allergy. Clin Exp Allergy 1999;29(11):1502-6.
140.van Odijk J, Peterson CG, Ahlstedt S, Bengtsson U, Borres MP, Hulthen L, et al. Measurements of eosinophil activation before and after food challenges in adults with food hypersensitivity. Int Arch Allergy Immunol 2006;140(4):334-41.
141.Beser OF, Sancak S, Erkan T, Kutlu T, Cokugras H, Cokugras FC. Can Fecal Calprotectin Level Be Used as a Markers of Inflammation in the Diagnosis and Follow-Up of Cow's Milk Protein Allergy? Allergy Asthma Immunol Res 2014;6(1):33-8.
142.Merras-Salmio L, Kolho KL, Pelkonen AS, Kuitunen M, Mäkelä MJ, Savilahti E. Markers of gut mucosal inflammation and cow's milk specific immunoglobulins in non-IgE cow's milk allergy. Clin Transl Allergy 2014;4(1):2045-7022.
143.Kim JS, Sampson HA. Food allergy: a glimpse into the inner workings of gut immunology. Curr Opin Gastroenterol 2012;28(2):99-103.
144.Turjanmaa K, Darsow U, Niggemann B, Rance F, Vanto T, Werfel T. EAACI/GA2LEN position paper: present status of the atopy patch test. Allergy 2006;61(12):1377-84.
96
145.Niggemann B, Reibel S, Wahn U. The atopy patch test (APT)-- a useful tool for the diagnosis of food allergy in children with atopic dermatitis. Allergy 2000;55(3):281-5.
146.Canani RB, Buongiovanni A, Nocerino R, Cosenza L, Troncone R. Toward a standardized reading of the atopy patch test in children with suspected cow's milk allergy-related gastrointestinal symptoms. Allergy 2011;66(11):1499-500.
147.Nocerino R, Granata V, Di Costanzo M, Pezzella V, Leone L, Passariello A, et al. Atopy patch tests are useful to predict oral tolerance in children with gastrointestinal symptoms related to non-IgE-mediated cow's milk allergy. Allergy 2013;68(2):246-8.
148.Mehl A, Rolinck-Werninghaus C, Staden U, Verstege A, Wahn U, Beyer K, et al. The atopy patch test in the diagnostic workup of suspected food-related symptoms in children. J Allergy Clin Immunol 2006;118(4):923-9.
149.Scala E, Alessandri C, Bernardi ML, Ferrara R, Palazzo P, Pomponi D, et al. Cross-sectional survey on immunoglobulin E reactivity in 23,077 subjects using an allergenic molecule-based microarray detection system. Clin Exp Allergy 2010;40(6):911-21.
150.Burton OT, Logsdon SL, Zhou JS, Medina-Tamayo J, Abdel-Gadir A, Noval Rivas M, et al. Oral immunotherapy induces IgG antibodies that act through FcgammaRIIb to suppress IgE-mediated hypersensitivity. J Allergy Clin Immunol 2014;134(6):1310-7.
151.Santos AF, James LK, Bahnson HT, Shamji MH, Couto-Francisco NC, Islam S, et al. IgG4 inhibits peanut-induced basophil and mast cell activation in peanut-tolerant children sensitized to peanut major allergens. J Allergy Clin Immunol 2015;135(5):1249-56.
152.Mariani A, Marsili M, Nozzi M, Faricelli R, Chiarelli F, Breda L. Serum calprotectin: review of its usefulness and validity in paediatric rheumatic diseases. Clin Exp Rheumatol 2015;33(1):109-14.
153.Decembrino L, De Amici M, Pozzi M, De Silvestri A, Stronati M. Serum Calprotectin: A Potential Biomarker for Neonatal Sepsis. J Immunol Res 2015;147973(10):26.
154.Hoffmann HJ, Santos AF, Mayorga C, Nopp A, Eberlein B, Ferrer M, et al. The clinical utility of basophil activation testing in diagnosis and monitoring of allergic disease. Allergy 2015. E-pub:2015/07/23
155.Patil SU, Shreffler WG. BATting above average: basophil activation testing for peanut allergy. J Allergy Clin Immunol 2014;134(3):653-4.
97
156.Glaumann S, Nopp A, Johansson SG, Borres MP, Nilsson C. Oral peanut challenge identifies an allergy but the peanut allergen threshold sensitivity is not reproducible. PloS One 2013;8(1):e53465.
157.Santos AF, Douiri A, Becares N, Wu SY, Stephens A, Radulovic S, et al. Basophil activation test discriminates between allergy and tolerance in peanut-sensitized children. J Allergy Clin Immunol 2014;134(3):645-52.
158.Nilsson N, Nilsson C, Hedlin G, Johansson SG, Borres MP, Nopp A. Combining analyses of basophil allergen threshold sensitivity, CD-sens, and IgE antibodies to hydrolyzed wheat, omega-5 gliadin and timothy grass enhances the prediction of wheat challenge outcome. Int Arch Allergy Immunol 2013;162(1):50-7.
159.Nopp A, Johansson SG, Ankerst J, Palmqvist M, Öman H. CD-sens and clinical changes during withdrawal of Xolair after 6 years of treatment. Allergy 2007;62(10):1175-81.
160.Sicherer SH, Wood RA, Stablein D, Burks AW, Liu AH, Jones SM, et al. Immunologic features of infants with milk or egg allergy enrolled in an observational study (Consortium of Food Allergy Research) of food allergy. J Allergy Clin Immunol 2010;125(5):1077-83.
161.Metcalfe JR, D'Vaz N, Makrides M, Gold MS, Quinn P, West CE, et al. Elevated IL-5 and IL-13 responses to egg proteins predate the introduction of egg in solid foods in infants with eczema. Clin Exp Allergy 2015;6(10):12608.
162.Krogulska A, Wasowska-Krolikowska K, Polakowska E, Chrul S. Cytokine profile in children with asthma undergoing food challenges. J Investig Allergol Clin Immunol 2009;19(1):43-8.
163.Vocca I, Canani RB, Camarca A, Ruotolo S, Nocerino R, Radano G, et al. Peripheral blood immune response elicited by beta-lactoglobulin in childhood cow's milk allergy. Pediatr Res 2011;70(6):549-54.
164.Dang TD, Tang ML, Koplin JJ, Licciardi PV, Eckert JK, Tan T, et al. Characterization of plasma cytokines in an infant population cohort of challenge-proven food allergy. Allergy 2013;68(10):1233-40.
165.International Standardization Organization. Report No. ISO 4120:2004. Sensory analysis. Methodology. Triangular test. Second edition 2004/06/15
166.Meilgaard MC, Civille, GV, Carr BT. Sensory evaluation techniques. 4th edition: CRC Press Inc: Boca Raton, FL.: 2007.

98
167.Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, et al. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Resp J 1995;8(3):483-91.
168.Bjerg A, Sandström T, Lundbäck B, Rönmark E. Time trends in asthma and wheeze in Swedish children 1996-2006: prevalence and risk factors by sex. Allergy 2010;65(1):48-55.
169.Rönmark E, Jonsson E, Platts-Mills T, Lundbäck B. Different pattern of risk factors for atopic and nonatopic asthma among children--report from the Obstructive Lung Disease in Northern Sweden Study. Allergy 1999;54(9):926-35.
170.Rönmark E, Lundbäck B, Jonsson E, Platts-Mills T. Asthma, type-1 allergy and related conditions in 7- and 8-year-old children in northern Sweden: prevalence rates and risk factor pattern. Resp Med 1998;92(2):316-24.
171.Dreborg S. The skin prick test in the diagnosis of atopic allergy. J Am Acad Dermatol 1989;21(4 Pt 2):820-1.
172.Calle-Alonso F, Pérez CJ. A Statistical Agreement-Based Approach for Difference Testing. J Sensory Studies 2013;28(5):358-69.
173.Greenberg R. Medical epidemiology. 4C edition: New York: Lange Medical Books/McGraw-Hill 2005.
174.Howe CJ, Cain LE, Hogan JW. Are all biases missing data problems? Curr Epidemiol Rep 2015;2(3):162-71.
175.Mortz CG, Andersen KE, Bindslev-Jensen C. Recall Bias in Childhood Atopic Diseases Among Adults in The Odense Adolescence Cohort Study. Acta Derm Venereol 2015;28(10):00015555-2128.
176.Hedman L, Bjerg A, Perzanowski M, Rönmark E. Good agreement between parental and self-completed questionnaires about allergic diseases and environmental factors in teenagers. J Clin Epidemiol 2010;63(7):783-9.
177.Pagano M, Gauvreau K. Principles of biostatistics. 2th edition: Pacific Grove: Duxbury; 2000.
178.Boyce JA, Assa'ad A, Burks AW, Jones SM, Sampson HA, Wood RA, et al. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report. J Allergy Clin Immunol 2010;126(6):1105-18.

99
179.Rönmark E, Perzanowski M, Platts-Mills T, Lundbäck B. Four-year incidence of allergic sensitization among schoolchildren in a community where allergy to cat and dog dominates sensitization: report from the Obstructive Lung Disease in Northern Sweden Study Group. J Allergy Clin Immunol 2003;112(4):747-54.
180.Bjerg A, Winberg A, Berthold M, Mattsson L, Borres MP, Rönmark E. A population-based study of animal component sensitization, asthma, and rhinitis in schoolchildren. Pediatr Allergy Immunol 2015;26(6):557-63.
181.Kaya A, Erkocoglu M, Civelek E, Cakir B, Kocabas CN. Prevalence of confirmed IgE-mediated food allergy among adolescents in Turkey. Pediatr Allergy Immunol 2013;24(5):456-62.
182.Persson K, Öhlund I, Nordström L, Winberg A, Rönmark E, West CE. Vitamin D deficiency at the Arctic Circle - a study in food-allergic adolescents and controls. Acta Paediatr. 2013;102(6):644-9.
183.Meyer R, De Koker C, Dziubak R, Venter C, Dominguez-Ortega G, Cutts R, et al. Malnutrition in children with food allergies in the UK. J Hum Nutr Diet 2013. E-pub: 2013/08/14
184.Mehta H, Ramesh M, Feuille E, Groetch M, Wang J. Growth comparison in children with and without food allergies in 2 different demographic populations. J Pediatr 2014;165(4):842-8.
185.Vlieg-Boerstra BJ, Bijleveld CM, van der Heide S, Beusekamp BJ, Wolt-Plompen SA, Kukler J, et al. Development and validation of challenge materials for double-blind, placebo-controlled food challenges in children. J Allergy Clin Immunol 2004;113(2):341-6.
186.Nowak-Wegrzyn A, Fiocchi A. Rare, medium, or well done? The effect of heating and food matrix on food protein allergenicity. Curr Opin Allergy Clin Immunol 2009;9(3):234-7.
187.Vlieg-Boerstra BJ, van der Heide S, Bijleveld CM, Kukler J, Duiverman EJ, Dubois AE. Placebo reactions in double-blind, placebo-controlled food challenges in children. Allergy 2007;62(8):905-12.
188.West CE, Hernell O, Andersson Y, Sjöstedt M, Hammarström ML. Probiotic effects on T-cell maturation in infants during weaning. Clin Exp Allergy 2012;42(4):540-9.
189.Kolho KL, Turner D, Veereman-Wauters G, Sladek M, de Ridder L, Shaoul R, et al. Rapid test for fecal calprotectin levels in children with Crohn disease. J Pediatr Gastroenterol Nutr 2012;55(4):436-9.

100
190.Robbins KA, Wood RA, Keet CA. Milk allergy is associated with decreased growth in US children. J Allergy Clin Immunol 2014. Epub 2014/10/15.
191.Nachshon L, Goldberg MR, Schwartz N, Sinai T, Amitzur-Levy R, Elizur A, et al. Decreased bone mineral density in young adult IgE-mediated cow's milk-allergic patients. J Allergy Clin Immunol 2014;134(5):1108-13.
192.Meyer R, Venter C, Fox AT, Shah N. Practical dietary management of protein energy malnutrition in young children with cow's milk protein allergy. Pediatr Allergy Immunol 2012;23(4):307-14.
193.Nowak-Wegrzyn A, Groetch M. Nutritional aspects and diets in food allergy. Chem Immunol Allergy 2015;101:209-20.
194.Kokkonen J, Haapalahti M, Tikkanen S, Karttunen R, Savilahti E. Gastrointestinal complaints and diagnosis in children: a population-based study. Acta Paediatr 2004;93(7):880-6.
195.Peters RL, Gurrin LC, Allen KJ. The predictive value of skin prick testing for challenge-proven food allergy: a systematic review. Pediatr Allergy Immunol 2012;23(4):347-52.
196.Kemp AS, Allen CW, Campbell DE. Parental perceptions in egg allergy: does egg challenge make a difference? Pediatr Allergy Immunol 2009;20(7):648-53.
197.Sutas Y, Kekki OM, Isolauri E. Late onset reactions to oral food challenge are linked to low serum interleukin-10 concentrations in patients with atopic dermatitis and food allergy. Clin Exp Allergy 2000;30(8):1121-8.
198.Lotoski LC, Simons FE, Chooniedass R, Liem J, Ostopowich I, Becker AB, et al. Are plasma IL-10 levels a useful marker of human clinical tolerance in peanut allergy? PLoS One 2010;5(6):0011192.
199.Krogulska A, Borowiec M, Polakowska E, Dynowski J, Mlynarski W, Wasowska-Krolikowska K. FOXP3, IL-10, and TGF-beta genes expression in children with IgE-dependent food allergy. J Clin Immunol 2011;31(2):205-15.
200.Savilahti EM, Karinen S, Salo HM, Klemetti P, Saarinen KM, Klemola T, et al. Combined T regulatory cell and Th2 expression profile identifies children with cow's milk allergy. Clin Immunol 2010;136(1):16-20.

101
Supplement
Questions from structured interviews considered in Paper III and/or Paper IV.
1. Was your child breastfed?
□ No
□ Yes
If yes, for how long?
□ < 3 months □ 3-6 months
□ 6-12 months □ >12 months
2. Did your child suffer from any symptoms during breastfeeding?
□ No
□ Yes
If yes, what kind of symptom/s?
□ Colic □ Gastrointestinal
□ Eczema □ Urticaria
□ Respiratory □ other: _____________
3. At what age was your child introduced to taste portions?
□ 3-6 months □ 6-12 months
□ >12 months
4. Did your child suffer from any symptoms during introduction of
taste portions?
□ No
□ Yes
If yes, what kind of symptom/s?
□ Colic □ Gastrointestinal
□ Eczema □ Urticaria
□ Respiratory □ Other: ______________
5. Has your child had a growth deviation?
□ No
□ Yes
If yes, which type of growth deviation?
□ Length □ Weight
□ Head circumference

102
6. Parental allergy/atopy related conditions?
□ No
□ Yes, mother
If yes, what type of allergy/atopy related condition in mother?
□ Asthma
□ Rhino-conjunctivitis
□ Eczema
□ Gastrointestinal
□ Allergy to airborne allergen/s, which?
________________________________
□ Food hypersensitivity;
□ During childhood
□ In adulthood
To which food/foods? -
______________________
□ Yes, father
If yes, what type of allergy/atopy related condition in father?
□ Asthma
□ Rhino-conjunctivitis
□ Eczema
□ Gastrointestinal
□ Allergy to airborne allergen/s, which?-
________________________________
□ Food hypersensitivity;
□ During childhood
□ In adulthood
To which food/foods? -
______________________
7. Other parental (mother or father) diseases/conditions?
a. Celiac disease
□ Yes □ No
b. Diabetes Mellitus type 1
□ Yes □ No
c. Inflammatory bowel disease
□ Yes □ No
d. Thyroid disease
□ Yes □ No
e. Gastritis/Esophagitis
□ Yes □ No
f. Irritable bowel disease
□ Yes □ No

103
8. Atopy related diseases/conditions in child (except for food
hypersensitivity)
a. Asthma
□ Yes, now □ Yes, before □ No, never
b. Rhino-conjunctivitis
□ Yes, now □ Yes, before □ No, never
c. Eczema
□ Yes, now □ Yes, before □ No, never
d. Allergy
□ Yes, now □ Yes, before □ No, never
If yes, what kind of allergy?
□ Birch pollen
□ Grass pollen
□ Ragweed
□ Furred animals
□ Bee/Wasp
□ Drugs, type: ______________________
9. Other diseases/conditions in child?
a. Celiac disease
□ Yes □ No
b. Diabetes Mellitus type 1
□ Yes □ No
c. Inflammatory bowel disease
□ Yes □ No
d. Thyroid disease
□ Yes □ No
e. Gastritis/Esophagitis
□ Yes □ No
f. Irritable bowel disease
□ Yes □ No
10. Has the child ever had anaphylaxis caused by food?
□ No
□ Yes
If yes, by what food trigger/s?
__________________________________________
At what age/s?
______________________________________

104
Questions on symptoms caused by the specific foods: milk, egg,
cod and wheat.
If the child reported hypersensitivity to more than one of these foods, the
questions were asked separately for the different foods.
11. Current symptoms caused by intake of milk/egg/cod/wheat:
□ Airways: □ Rhinitis □ Asthma □ Laryngospasm
□ Heart/circulation (decreased blood pressure/ circulatory failure)
□ Eyes (conjunctivitis/kerato-conjunctivitis)
□ Oral: □ Itching □ Aphtae □ Lip swelling
□ Itching/bloated feeling of the throat
□ Skin: □ Eczema □ Urticaria □ Angioedema
□ Gastrointestinal: □ Vomiting □ Diarrhea □ Constipation
□ Flatulence □ Stomach ache
□ Affected growth
□ Other/s:
_______________________________________________
_______________________________________________
_______________________________________________
12. Symptoms caused by intake of milk/egg/cod/wheat at symptom
onset:
□ Airways: □ Rhinitis □ Asthma □ Laryngospasm
□ Heart/circulation (decreased blood pressure/ circulatory failure)
□ Eyes (conjunctivitis/kerato-conjunctivitis)
□ Oral: □ Itching □ Aphtae □ Lip swelling
□ Itching/bloated feeling of the throat
□ Skin: □ Eczema □ Urticaria □ Angioedema
□ Gastrointestinal: □ Vomiting □ Diarrhea □ Constipation
□ Flatulence □ Stomach ache
□ Affected growth
□ Other/s:
_______________________________________________
_______________________________________________
_______________________________________________
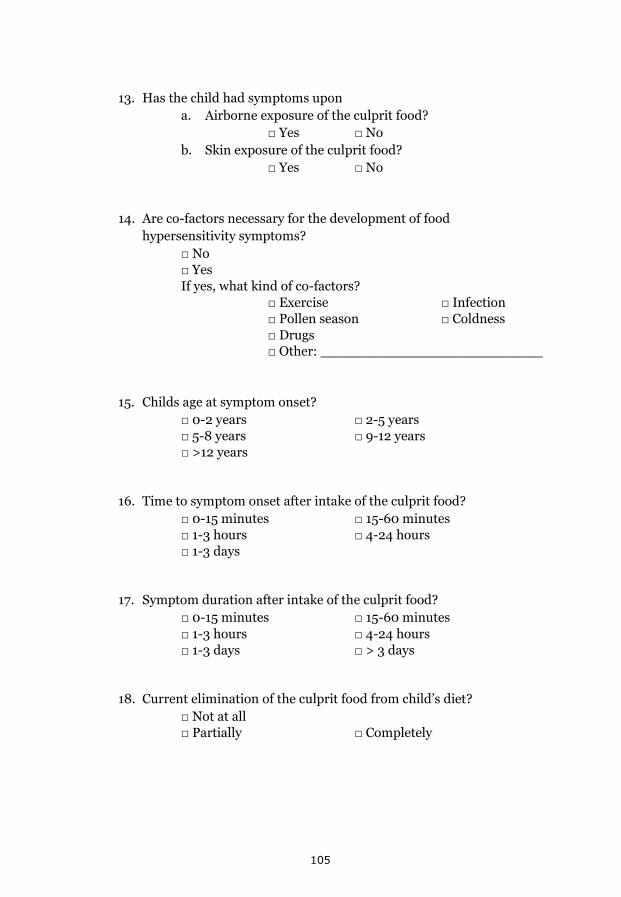
105
13. Has the child had symptoms upon
a. Airborne exposure of the culprit food?
□ Yes □ No
b. Skin exposure of the culprit food?
□ Yes □ No
14. Are co-factors necessary for the development of food
hypersensitivity symptoms?
□ No
□ Yes
If yes, what kind of co-factors?
□ Exercise □ Infection
□ Pollen season □ Coldness
□ Drugs
□ Other: __________________________
15. Childs age at symptom onset?
□ 0-2 years □ 2-5 years
□ 5-8 years □ 9-12 years
□ >12 years
16. Time to symptom onset after intake of the culprit food?
□ 0-15 minutes □ 15-60 minutes
□ 1-3 hours □ 4-24 hours
□ 1-3 days
17. Symptom duration after intake of the culprit food?
□ 0-15 minutes □ 15-60 minutes
□ 1-3 hours □ 4-24 hours
□ 1-3 days □ > 3 days
18. Current elimination of the culprit food from child’s diet?
□ Not at all
□ Partially □ Completely

106
19. If hypersensitivity to milk: does lactose-free products trigger
symptoms?
□ No
□ Yes
If yes, at what dose?
__________________________________
20. If hypersensitivity to milk: What replacement products does the
child eat/drink?
□ Lactose free/reduced products
□ < 1 dl/day □ 1-3 dl/day □ >1 dl/day
□ Soy products
□ < 1 dl/day □ 1-3 dl/day □ >1 dl/day
□ Oat products
□ < 1 dl/day □ 1-3 dl/day □ >1 dl/day
□ Rice products
□ < 1 dl/day □ 1-3 dl/day □ >1 dl/day
□ Calcium supplement
□ Other:
_________________________________________
21. If hypersensitivity to fish, what kind of fish causes symptoms?
□ Cod fish □ Salmon
□ Shell fish
22. Physician diagnosis of celiac disease?
□ No
□ Yes
If yes, at what age?
__________________________________________
23. If hypersensitivity to wheat: does other grains cause symptoms?
□ No
□ Yes
If yes, what kind of grains?
□ Barley □ Rye □ Oats

107
24. At what age was the culprit food introduced in the child’s diet?
□ < 3 months □ Through breastmilk □ Own diet
□ 3-6 months □ Through breastmilk □ Own diet
□ 6-12 months □ Through breastmilk □ Own diet
□ > 12 months □ Through breastmilk □ Own diet
25. Amount and type of trigger food necessary to cause symptoms:
a. Milk □ Baked milk:
□ Treasure amount □ Table spoon
□ < 1 dl □ >1 dl
□ Raw (pasteurized) milk:
□ Treasure amount □ Table spoon
□ < 1 dl □ >1 dl
b. Egg □ Baked egg:
□ Treasure amount
□ Tablespoon of muffin
□ Whole muffin
□ Pancake
□ Boiled/fried egg
□ Raw egg
□ Treasure amount
□ Tablespoon of sponge
c. Cod □ Cooked cod:
□ Treasure amount □ Tea spoon
□ Table spoon □ Portion size
□ Raw cod (sushi, pickled herring):
□ Treasure amount □ Tea spoon
□ Table spoon □ Portion size
d. Wheat □ Baked wheat:
□ Treasure amount
□ Tea spoon of bread
□ Table spoon of bread
□ Portion size
□ Repeated exposure
□ Raw wheat

108
26. When was the child last exposed to the culprit food?
□ < 3 months □ 3-6 months
□ 6-12 months □ 1-2 years
□ >2 years
27. How long ago did the child last have a reaction due to intake of the
culprit food?
□ < 3 months □ 3-6 months
□ 6-12 months □ 1-2 years
□ >2 years
28. Has the child been diagnosed with hypersensitivity to the culprit
food through a previous health care contact?
□ No
□ Yes
If yes, by whom?
□ By a physician
□ By a child health care nurse
□ Other:__________________________
29. Has the child performed any investigations/diagnostic test before
the food hypersensitivity diagnosis?
□ No
□ Yes
If yes, what kind of investigation/test?
□ Clinical history
□ Positive □ Negative
□ Specific IgE/Skin prick test
□ Positive □ Negative
□ Oral challenge
□ Positive □ Negative
□ Lactose challenge
□ Positive □ Negative
□ Gene test (lactase down-regulating gene)
□ Positive □ Negative
□ Other: ___________________________
30. Has the child ever been referred to a dietician for nutritional advice
due to the food hypersensitivity?
□ No
□ Yes