Embed Size (px)
DESCRIPTION
Epidemiología de la Tuberculosis miliar y extrapulmonar. Distribución geográfica
Citation preview

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 1/12
Official reprint from UpToDate www.uptodate.com ©2015 UpToDate
AuthorJohn Bernardo, MD
Section EditorC Fordham von Reyn, MD
Deputy EditorElinor L Baron, MD, DTMH
Epidemiology and pathology of extrapulmonary and miliary tuberculosis
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Jul 2015. | This topic last updated: Feb 07, 2014.
INTRODUCTION — Miliary tuberculosis (TB) refers to clinical disease resulting from the hematogenous dissemination of Mycobacterium tuberculosis. The
term “miliary” was coined in 1700 by John Jacobus Manget, who likened the appearance of the involved lung with its surface covered with firm small white
nodules to numerous millet seeds (picture 1). Miliary TB can arise as a result of progressive primary infection or via reactivation of a latent focus with
subsequent spread. Originally a pathologic and then a radiographic description, the term miliary TB is now used to denote all forms of progressive, widely
disseminated hematogenous TB, even if the classical pathologic or radiologic findings are absent.
Tuberculosis may be classified according to site of disease as pulmonary or extrapulmonary; miliary disease has been classified as both an
extrapulmonary and a pulmonary form of TB.
The epidemiology and pathology of miliary TB will be reviewed here. The clinical manifestations, diagnosis, treatment, and prevention of miliary TB are
discussed separately. (See "Clinical manifestations, diagnosis, and treatment of extrapulmonary and miliary tuberculosis".)
EPIDEMIOLOGY — The epidemiology of tuberculosis (TB) and the miliary form of the disease have been altered by the introduction of effective
chemotherapy, the HIV epidemic, and immigration patterns. Of 9945 incident cases reported in the United States in 2012, extrapulmonary TB with no
demonstrated pulmonary involvement accounted for approximately 21 percent of cases (2100 cases). In an additional 1016 cases (10 percent), disease in
pulmonary and extrapulmonary sites was reported; these included 349 cases (3.5 percent of total) with miliary disease [1]. This reflected a minor increase
from 1.8 percent of reported cases in 2006. Worldwide, estimates of its incidence are hampered largely by incomplete reporting and imprecise diagnostic
criteria; it is estimated that miliary TB accounts for 1 to 2 percent of all cases of TB in immunocompetent persons [2].
The epidemiology of miliary disease varies in different case series:
®
®
Prior to the availability of antituberculous therapy, 20 percent of TB autopsy cases at Boston City Hospital had evidence of miliary disease [3]. By the
1970s, with the availability of antituberculous therapy, the incidence had fallen to 0.7 percent [4].
●
Data from the Centers for Disease Control and Prevention (CDC) in the early 1980s (after the availability of antituberculous therapy but prior to the
HIV epidemic) reported 1.3 percent of TB cases had evidence of miliary disease [5].
●
In the midst of the HIV epidemic during the mid 1980s, the percentage of miliary TB was higher among HIV-infected patients than HIV-uninfected
patients (38 versus 8 percent) [6,7]. Risk for developing miliary TB appeared to be highest among patients with the lowest CD4 counts [8].
●
In a public health clinic in Ireland in the 1990s, miliary disease accounted for 4 percent of TB cases [9].●

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 2/12
The HIV epidemic has played a significant role in increasing the prevalence of miliary TB. Between 1999 and 2006 in England and Wales, an almost
fivefold increase in the number of miliary cases was observed (38 to 180 cases); HIV coinfection was most strongly associated with miliary disease [10].
Other factors, such as the emergence of drug-resistant or multidrug-resistant strains, have also contributed [11].
Risk factors — Risk factors for the development of miliary TB include age and underlying medical conditions, especially HIV infection. However, a
significant percentage of cases described in the literature have no demonstrable high-risk condition for dissemination; miliary TB should never be excluded
as a clinical diagnosis because an underlying medical illness is absent.
Age — Infants and young children are highly susceptible to miliary TB, presumably due to their relatively immature immune systems [12-16]. In a
study from Puerto Rico, miliary disease or meningitis occurred more frequently among children <6 years than among children >7 years of age (1 versus
0.4 percent, respectively) [13]. In another series from South Africa, miliary TB accounted for more hospital admissions among children than adults (8
versus 1 percent); 52 percent of cases occurred in children <1 year of age [14].
Miliary TB has been described more frequently among elderly adults in the post-antibiotic era than the pre-antibiotic era; this group is likely at increased
risk due to relative waning of cellular immunity [4]. In addition, the rise of HIV has led to increased prevalence of miliary TB among young adults [17].
Medical conditions — The percentage of patients with miliary TB and some identifiable underlying medical condition in various studies ranged from 38
to 70 percent. The most common conditions include [18-24]:
Weight loss and/or malnutrition are important components of a number of these conditions but have not been addressed separately [18-22].
Other factors — Men outnumber women in most series of miliary TB (table 1); it is uncertain whether this reflects a greater prevalence of TB among
men. It is also uncertain whether African-Americans are more likely to progress from infection to disseminated disease, since control for the relative
contributions of socioeconomic factors, such as living conditions, nutrition, access to care, and comorbidities, is needed for proper data interpretation [25].
PATHOLOGY
Mechanisms of disease — Miliary tuberculosis (TB) can arise as a result of progressive primary infection or via reactivation of a latent focus with
subsequent spread. Rarely, iatrogenic infection can occur.
Progressive primary disease — After establishing a focus of infection in the lung, bacilli can disseminate via the lymphatics and hematogenously
(algorithm 1). There is a predilection for spread to the most vascular organs, such as the liver, spleen, bone marrow, and brain. These distant foci usually
Alcohol abuse●
Malignancy●
Human immunodeficiency virus (HIV) infection●
Corticosteroids or other iatrogenic immunosuppression (eg, TNF-alpha blocking agents)●
Connective tissue disease (with or without iatrogenic immunosuppression)●
Renal failure●
Diabetes●
Pregnancy●

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 3/12
heal by granulomatous encapsulation over weeks to months, containing viable organisms. Failure of these foci to heal early following primary infection
leads to progressive primary disease. Many adult patients with progressive TB have underlying medical or iatrogenic conditions that impair the
development of effective cell mediated immunity intended to contain the primary infection.
Reactivation of a latent focus — Miliary TB may result from reactivation of a latent focus of infection with subsequent erosion into adjoining
lymphatics or blood vessels, leading to dissemination of viable organisms. Reactivation may occur at any time after the primary infection; commonly it
occurs years or decades later, in association with demonstrable waning of specific immune responses, or in the presence of a high risk condition
associated with progressive TB. (See 'Risk factors' above.)
Iatrogenic infection — Rarely, miliary TB may occur as a result of iatrogenic exposure. Disseminated TB has been reported after extracorporeal
shock wave lithotripsy [26,27], urethral catheterization [28], and cardiac valve homograft placement [29]. TB has also been transmitted by solid organ
transplantation [30,31].
Clinicopathologic patterns of disease — Classically, the clinical and pathologic patterns of miliary TB have been divided into three groups: acute miliary
TB, late generalized TB, and anergic (nonreactive) TB. These terms can be confusing because there is considerable overlap among the categories and the
terminology is no longer frequently used. Acute miliary TB is primarily a clinical term; this entity can be seen in the immediate post-primary period or in
immunocompromised children or adults. It is usually observed within the first two to six months following exposure, although progression may be more
rapid in neonates and children under the age of one year [32]. During one TB outbreak in an HIV housing facility in San Francisco, 11 of 30 HIV-infected
residents (37 percent) who were exposed to an infectious pulmonary case of TB developed TB disease within 106 days; in one HIV-infected contact, TB
was diagnosed within four weeks of exposure [33].
Late generalized TB is primarily a pathologic term, referring to hematogenous dissemination without evidence of an active primary focus. Patients with an
acute miliary presentation may in fact have evidence of late generalized disease on histopathology.
Acute miliary tuberculosis — Acute (generalized) miliary TB has a relatively rapid clinical course [3,34]. Prior to the availability of effective
chemotherapy for TB, most cases of acute miliary TB resulted from progressive primary disease. The pathologic hallmark of acute miliary TB is a
caseating granulomatous reaction (picture 2), with a smaller number of organisms than other forms of miliary disease [3,34].
Late generalized tuberculosis — Late generalized TB refers hematogenous spread that occurs after the primary or post-primary period. In one
autopsy series of 100 patients with late generalized TB from 1937 to 1959, patients had relatively chronic, clinically nonspecific presentations [35]. In this
study, late generalized TB was frequently associated with chronic pulmonary TB. Since the availability of chemotherapy for TB, however, foci responsible
for hematogenous spread are extrapulmonary in some cases and are thus more difficult to detect.
A subset of late generalized TB is labeled cryptic miliary TB. This term refers to patients in whom the illness is even more indolent and who may
demonstrate an attenuated histologic response [35,36].
Anergic tuberculosis — Anergic TB is defined histologically by the absence of granulomata. In some cases, microabscesses containing large
numbers of bacilli with a predominantly neutrophilic response are observed, although, in general, anergic TB is relatively difficult to establish based on
histology [37]. Tissue stains and cultures are generally more sensitive diagnostic tools.
Anergic (nonreactive) TB is a relatively uncommon form of miliary disease. The clinical spectrum ranges from overwhelming sepsis to nonspecific or

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 4/12
typhoidal presentations. Most of the described cases are older patients with presumed reactivation TB. Granulomas in immunocompromised patients with
TB may share similar characteristics [38].
Host and pathogen factors — The major determinants of TB dissemination include mycobacterial virulence factors [39] and host immune defenses. The
high susceptibility of infants to miliary TB has led some investigators to speculate that the developing immune system may lack critical elements for
initiating protective responses to M. tuberculosis [15,16]. After initial infection, the development of specific cell-mediated immunity appears to be critical in
limiting disseminated disease. Cytokines, including TNF-alpha, interleukin (IL)-12 and interferon gamma, are essential for granuloma development and
protective immunity to M. tuberculosis [40,41]. (See "Natural history, microbiology, and pathogenesis of tuberculosis" and "Immunology of tuberculosis".)
SUMMARY
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
Miliary tuberculosis (TB) refers to clinical disease resulting from the hematogenous dissemination of Mycobacterium tuberculosis that affects multiple
organs and systems. Miliary TB can arise as a result of progressive primary infection or via reactivation of a previously contained latent focus with
subsequent spread. Miliary TB accounts for approximately 3 percent of incident cases in the United States, with increased representation among
infants and young children and in individuals with concomitant immunosuppression. Extrapulmonary TB accounts for approximately 20 percent of
cases. (See 'Introduction' above and 'Epidemiology' above.)
●
Risk factors for the development of miliary TB include extremes of age and underlying medical conditions. Infants are highly susceptible to miliary
TB, presumably due to their relatively immature immune systems. Elderly adults are also at increased risk for miliary TB due to relative waning of
cellular immunity. Underlying medical conditions conferring increased risk for miliary TB include alcohol abuse, malignancy, HIV infection,
immunosuppression (including chronic corticosteroid use and TNF-alpha inhibitors), connective tissue disease, renal failure, diabetes, and
pregnancy. (See 'Risk factors' above.)
●
After establishing a primary focus of infection in the lung, tuberculous bacilli can disseminate via the lymphatics and hematogenously to the most
vascular organs, such as the liver, spleen, bone marrow, and brain. These distant foci usually heal by granulomatous encapsulation over weeks to
months. Failure of these foci to heal within the first six months after primary infection leads to progressive primary disease. Healed, latent foci can
reactivate at any time after the primary infection; most commonly, reactivation occurs years or decades after primary infection, in association with
waning of cellular immune responses or other risk factors. (See 'Mechanisms of disease' above.)
●
Acute (generalized) miliary TB has a relatively rapid clinical course. This entity can be seen in the immediate post-primary period or as a result of
reactivation of a chronic focus; prior to the availability of anti-TB chemotherapy, most cases resulted from progressive primary disease. The
pathologic hallmark of acute miliary TB is a caseating granulomatous reaction. (See 'Acute miliary tuberculosis' above.)
●
Late generalized TB refers hematogenous spread that occurs after the primary or post-primary period. Prior to the availability of effective TB
chemotherapy, late generalized TB was frequently associated with chronic pulmonary TB. (See 'Late generalized tuberculosis' above.)
●

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 5/12
1. http://www.cdc.gov/tb/statistics/reports/2012/pdf/report2012.pdf (Accessed on January 30, 2014).
2. Sharma SK, Mohan A, Sharma A, Mitra DK. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis 2005; 5:415.
3. CHAPMAN CB, WHORTON CM. Acute generalized miliary tuberculosis in adults. N Engl J Med 1946; 235:239.
4. Alvarez S, McCabe WR. Extrapulmonary tuberculosis revisited: a review of experience at Boston City and other hospitals. Medicine (Baltimore)1984; 63:25.
5. Rieder HL, Kelly GD, Bloch AB, et al. Tuberculosis diagnosed at death in the United States. Chest 1991; 100:678.
6. Shafer RW, Kim DS, Weiss JP, Quale JM. Extrapulmonary tuberculosis in patients with human immunodeficiency virus infection. Medicine(Baltimore) 1991; 70:384.
7. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 5-1999. A 37-year-old man with fever and diffuselymphadenopathy. N Engl J Med 1999; 340:545.
8. Lado Lado FL, Barrio Gómez E, Carballo Arceo E, Cabarcos Ortíz de Barrón A. Clinical presentation of tuberculosis and the degree ofimmunodeficiency in patients with HIV infection. Scand J Infect Dis 1999; 31:387.
9. O'Reilly P, McDonnell T. The spectrum of mycobacterial disease in a Dublin teaching hospital. Ir Med J 1999; 92:299.
10. Kruijshaar ME, Abubakar I. Increase in extrapulmonary tuberculosis in England and Wales 1999-2006. Thorax 2009; 64:1090.
11. Brudney K, Dobkin J. Resurgent tuberculosis in New York City. Human immunodeficiency virus, homelessness, and the decline of tuberculosiscontrol programs. Am Rev Respir Dis 1991; 144:745.
12. Snider DE Jr, Rieder HL, Combs D, et al. Tuberculosis in children. Pediatr Infect Dis J 1988; 7:271.
13. Comstock GW, Livesay VT, Woolpert SF. The prognosis of a positive tuberculin reaction in childhood and adolescence. Am J Epidemiol 1974;99:131.
14. Hussey G, Chisholm T, Kibel M. Miliary tuberculosis in children: a review of 94 cases. Pediatr Infect Dis J 1991; 10:832.
15. Smith S, Jacobs RF, Wilson CB. Immunobiology of childhood tuberculosis: a window on the ontogeny of cellular immunity. J Pediatr 1997; 131:16.
16. Cruz AT, Starke JR. Clinical manifestations of tuberculosis in children. Paediatr Respir Rev 2007; 8:107.
17. Braun MM, Coté TR, Rabkin CS. Trends in death with tuberculosis during the AIDS era. JAMA 1993; 269:2865.
18. Aguado JM, Herrero JA, Gavaldá J, et al. Clinical presentation and outcome of tuberculosis in kidney, liver, and heart transplant recipients in Spain.Spanish Transplantation Infection Study Group, GESITRA. Transplantation 1997; 63:1278.
19. Muñoz P, Palomo J, Muñoz R, et al. Tuberculosis in heart transplant recipients. Clin Infect Dis 1995; 21:398.
20. Sakhuja V, Jha V, Varma PP, et al. The high incidence of tuberculosis among renal transplant recipients in India. Transplantation 1996; 61:211.
21. Nishizaki T, Yanaga K, Soejima Y, et al. Tuberculosis following liver transplantation: report of a case and review of the literature. Transpl Int 1996;9:589.
22. Nagasawa M, Maeda H, Okawa H, Yata J. Pulmonary miliary tuberculosis and T-cell abnormalities in a severe combined immunodeficient patientreconstituted with haploidentical bone marrow transplantation. Int J Hematol 1994; 59:303.
23. Munt PW. Miliary tuberculosis in the chemotherapy era: with a clinical review in 69 American adults. Medicine (Baltimore) 1972; 51:139.
24. Maartens G, Willcox PA, Benatar SR. Miliary tuberculosis: rapid diagnosis, hematologic abnormalities, and outcome in 109 treated adults. Am J

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 6/12
Med 1990; 89:291.
25. Centers for Disease Control. Extrapulmonary tuberculosis in the United States 1969-1973. DHEW publication no CDC 78-8260. Atlanta: Departmentof Health, Education and Welfare, 1978.
26. Morano Amado LE, Amador Barciela L, Rodriguez Fernandez A, et al. Extracorporeal shock wave lithotripsy complicated with miliary tuberculosis. JUrol 1993; 149:1532.
27. Federmann M, Kley HK. Miliary tuberculosis after extracorporeal shock-wave lithotripsy. N Engl J Med 1990; 323:1212.
28. Yekanath H, Gross PA, Vitenson JH. Miliary tuberculosis following ureteral catheterization. Urology 1980; 16:197.
29. Anyanwu CH, Nassau E, Yacoub M. Miliary tuberculosis following homograft valve replacement. Thorax 1976; 31:101.
30. Qunibi WY, al-Sibai MB, Taher S, et al. Mycobacterial infection after renal transplantation--report of 14 cases and review of the literature. Q J Med1990; 77:1039.
31. Miller RA, Lanza LA, Kline JN, Geist LJ. Mycobacterium tuberculosis in lung transplant recipients. Am J Respir Crit Care Med 1995; 152:374.
32. PERRY TL. Natural history and pathogenesis of miliary and meningeal tuberculosis in children; analysis of 163 cases. Pediatrics 1950; 5:988.
33. Daley CL, Small PM, Schecter GF, et al. An outbreak of tuberculosis with accelerated progression among persons infected with the humanimmunodeficiency virus. An analysis using restriction-fragment-length polymorphisms. N Engl J Med 1992; 326:231.
34. Stead WW. Pathogenesis of tuberculosis: clinical and epidemiologic perspective. Rev Infect Dis 1989; 11 Suppl 2:S366.
35. Slavin RE, Walsh TJ, Pollack AD. Late generalized tuberculosis: a clinical pathologic analysis and comparison of 100 cases in the preantibiotic andantibiotic eras. Medicine (Baltimore) 1980; 59:352.
36. Proudfoot AT, Akhtar AJ, Douglas AC, Horne NW. Miliary tuberculosis in adults. Br Med J 1969; 2:273.
37. O'BRIEN JR. Non-reactive tuberculosis. J Clin Pathol 1954; 7:216.
38. de Noronha AL, Báfica A, Nogueira L, et al. Lung granulomas from Mycobacterium tuberculosis/HIV-1 co-infected patients display decreased in situTNF production. Pathol Res Pract 2008; 204:155.
39. Mazurek J, Ignatowicz L, Kallenius G, et al. Divergent effects of mycobacterial cell wall glycolipids on maturation and function of human monocyte-derived dendritic cells. PLoS One 2012; 7:e42515.
40. Altare F, Jouanguy E, Lamhamedi S, et al. Mendelian susceptibility to mycobacterial infection in man. Curr Opin Immunol 1998; 10:413.
41. Jouanguy E, Döffinger R, Dupuis S, et al. IL-12 and IFN-gamma in host defense against mycobacteria and salmonella in mice and men. Curr OpinImmunol 1999; 11:346.
Topic 8029 Version 11.0

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 7/12
GRAPHICS
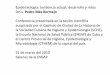
Comparative size of millet seeds
Millet seeds from which the name miliary tuberculosis derives
compared to the size of a dime (right) and a centimeter scale (left).
These correspond to the approximate size of miliary lesions seen on
chest radiograph.
Courtesy of Nesli Basgoz, MD.
Graphic 76174 Version 1.0

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 8/12
Major clinical series of miliary tuberculosis
First
author,
year
Years
includedLocation Inclusion criteria
# of
patients
Percent
male
Race,
percent
Maartens,
1990
1978 to
1987
Groote Schuur
Hospital (community-
based teaching
hospital in South
Africa)
Miliary pattern on CXR plus MTB on culture
from any site; or biopsy or autopsy
evidence of miliary organ involvement with
TB
109 51 African,
45,
mixed,
49,
white, 6
Kim, 1990 1975 to
1988
Duke University
Medical Center and
Durham VA Hospital
Durham, North
Carolina
Discharge diagnosis of disseminated or
miliary TB
38 50 African-
American,
50*
Gelb,
1973
1960 to
1970
UCLA Hospital Los
Angeles, California
Miliary pattern on CXR and one or more: 109 59 African-
American,
811. MTB on culture
2. Biopsy or autopsy showing caseating
granulomas with AFB
3. Clinical presentation and response
consistent with TB
Munt,
1971
1954 to
1970
Sanitorium drawing
from eastern part of
North Carolina
"Acute, diffuse pulmonary and extra-
pulmonary dissemination of TB, usually
associated with a miliary pattern on CXR,
with either MTB by culture or response to
TB therapy"
69 65 African-
American,
87
Proudfoot,
1969
1954 to
1967
Edinburgh, Scotland "Adults diagnosed in Edinburgh as having
disseminated TB"
40 40 Non-
British,
<1
Biehl,
1957
1951 to
1956
Cincinatti General
(city teaching
hospital Cincinatti,
Bacteriologic or pathologic diagnosis of
miliary tuberculosis or probable diagnosis
with response to therapy
68 69 African-
American,
23

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=e… 9/12
Ohio)
CXR: chest radiograph; MTB: Mycobacterium tuberculosis; TB: tuberculosis; AFB: acid-fast bacilli.
* Excluding VA population.
Courtesy of Nesli Basgoz, MD.
Graphic 77719 Version 3.0

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=… 10/12
Pathogenesis of tuberculosis and miliary tuberculosis
TB: tuberculosis.
Courtesy of Nesli Basgoz, MD.
Graphic 66301 Version 3.0

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=… 11/12
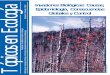
Miliary tuberculosis of the spleen
Miliary tuberculosis of the spleen. The cut surface shows numerous
gray-white granulomas.
Reproduced from: Kumar V, Abbas AK, Fausto N, Mitchell RN. Robbins Basic
Pathology, 8th ed, Saunders Elsevier, Philadelphia 2007. Illustration used
with the permission of Elsevier Inc. All rights reserved.
Graphic 93762 Version 1.0

8/17/2015 Epidemiology and pathology of extrapulmonary and miliary tuberculosis
http://www.uptodate.com.wdg.biblio.udg.mx:2048/contents/epidemiology-and-pathology-of-extrapulmonary-and-miliary-tuberculosis?topicKey=ID%2F8029&elapsedTimeMs=0&source=search_result&searchTerm=… 12/12
Disclosures: John Bernardo, MD Nothing to disclose. C Fordham von Reyn, MD Nothing to disclose. Elinor L Baron, MD, DTMH Nothingto disclose.
Contributor disclosures are review ed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amulti-level review process, and through requirements for references to be provided to support the content. Appropriately referenced content isrequired of all authors and must conform to UpToDate standards of evidence.
Conflict of interest policy
Disclosures