Embed Size (px)
Citation preview

180
EP16
EP16 – Nurse Autonomy is supported and promoted through the organization’s governance structure for shared decision-making. Provide one example, with supporting evidence, of clinical autonomy that demonstrates the authority and freedom of nurses to make nursing care decisions (within the full scope of their practice) in the clinical care of patients. And Provide one example, with supporting evidence, of organizational autonomy that demonstrates the authority and freedom of nurses to be involved in broader unit, service line, organization or system decision-making processes pertaining to patient care, policies and procedures, or work environment. Example 1: Clinical Autonomy: Clinical Nurse Pat Sites, RN, Autonomously Coordinates Care for Patients Receiving Anticoagulant Therapy There are many patient populations that require anticoagulation as a therapeutic intervention. The complexity of dosing and monitoring requirements makes these high-risk medications. Managing patients on anticoagulant therapy is challenging and associated with adverse drug events. Oversight of this practice at UVA is achieved with an interprofessional Anticoagulation Committee. This committee is divided into two subcommittees: inpatient and outpatient. Shared leadership and overlapping membership ensure consistent practices across the continuum of care. Nurses, physicians, pharmacists, laboratory workers and informaticists work together to create tools for the most efficient and effective care for patients receiving anticoagulant therapy. Pat Sites, RN, Clinician II, in the University Physicians of Charlottesville (UPC) Clinic, is one of several nurses who provide focused care in the outpatient management of patients on anticoagulant medications. Three days a week, Sites coordinates care for patients discharged from the hospital on these medications or initiated on therapy in the ambulatory setting. Her autonomous clinical practice is guided by protocols (Exhibit EP16.a: Outpatient Anticoagulation Clinic Protocol) developed to direct the standardized care of this patient population. When a patient is started on warfarin, Sites receives a notification from the physician managing the patient’s care. The physician provides orders dictating the therapeutic range for therapy based on the patient’s unique condition and evaluation. The protocol order then provides the structure that Sites uses to make decisions about his or her therapy, monitoring and follow-up.
181
EP16
When Sites receives a patient, she spends significant time educating him or her about his or her specific need for anticoagulation so that he or she understands the importance of adhering to the regimen. Providing education about dosing, side effects, precautions and monitoring is facilitated with standardized patient education materials. (Exhibit EP16.b: PE16021 Info Warfarin Color) The first goal is to achieve therapeutic levels of the medication. Each patient’s response to anticoagulants is unique, and careful monitoring is critical. Following the initial appointment, Sites typically sees the patient again in three days to check blood levels, assess the patient and provide additional education. Close follow-up occurs until the patient achieves therapeutic levels, and then appointments are scheduled to maintain adequate therapy and monitoring. Some patients require “bridge therapy” as they transition off of one type of anticoagulant, such as low molecular weight heparin, to oral medication, such as warfarin. In these cases, the protocol guides the process, and Sites manages the care and instructs the patient on transition and injections. Assessment of patients on anticoagulant therapy includes bleeding, diet changes, medication compliance and possible interfering factors if blood levels are not at target, as well as overall health and well-being. Sites tracks more than 180 patients in various stages of therapy. If patients are not following their appointment schedule, she reaches out to them to provide guidance and assists as needed. Recently, Sites began caring for a patient with atrial fibrillation who was awaiting a corrective ablation. The patient was initiated on anticoagulant therapy to prevent blood clots. The patient lived more than two hours away from UVA. In the process of working toward therapeutic levels, the patient experienced a fall in her home. She was injured and admitted to her local hospital. The family called Sites and informed her of the situation. Sites reached out to the physicians caring for the patient, and they collaborated to develop a plan to maintain the anticoagulant therapy goals. Sites consulted with the physicians by phone and informed them of the next steps according to the anticoagulation protocol to ensure that her patient’s course was not interrupted. Following the patient’s hospitalization, Sites resumed routine follow-up with her. Exhibit EP16.c is an example of documentation reflective of her care and inclusion of the patient’s husband. (Exhibit EP16.c: Sample Anticoagulant Epic Note) In addition to managing patients autonomously, Sites and her anticoagulation nurse colleagues are participating in a design / redesign of the Epic tools. Examples include creating an online anticoagulation referral form (delineating reason for anticoagulation, therapeutic INR range and duration of therapy) and standardizing warfarin education documentation between the inpatient and outpatient setting. The anticoagulation nurses

182
EP16
are making decisions in partnership with Cindy Westley, MSN, RN-BC, CNL, Nurse Informaticist, working with anticoagulation-related issues to enhance documentation and communication across settings. These changes are presented to UVA Anticoagulation Committee for review and approval. The ultimate goals focus on patient safety and efficiency of care. As the primary users of the aspects of documentation specific to anticoagulation therapy and monitoring, the anticoagulation nurses’ expert perspectives are being incorporated into the design changes. Mary Stack, MSN, RN, FNP-BC, Advanced Practice Nurse 1-NP, in the University Medical Associates (UMA) Clinic, provides direct patient care with the added ability to prescribe and address anticoagulation-related issues. When patients who do not have primary care providers (PCP) are discharged from the hospital, Stack serves as a transition provider, managing anticoagulation needs until their initial PCP visit. For patients still in the hospital, she assists with discharge planning when difficult situations arise. She provides anticoagulation management education to outpatient nurses and serves as a resource to nursing and medical staff. Participants: EP16 Table 1: Participants, Anticoagulation Nursing Team
Name Discipline Title Department Patricia Sites Nursing RN Clinician II UPC Clinic Mary Stack Nursing Advanced
Practice Nurse 1-Nurse Practitioner
UMA Clinic
Marsha Tarbert Nursing RN Clinician II UMA Clinic Lee McDaniel Nursing RN Clinician II Internal Medicine at
Orange Example 2: Organizational Autonomy: Clinical Nurses Lead and Participate in the Local and Organizational Structures and Processes that Support Patients Experiencing ST-segment Elevation Myocardial Infarctions UVA Emergency Department (ED) provides comprehensive, expert care for the local and regional community, including transfer patients from other facilities. Building systems and processes to provide standardized, coordinated care requires interprofessional planning and teamwork. The care of patients experiencing STEMI (ST-segment elevation myocardial infarction) events provides an example of the key role that nurses play in broad decision-making processes. STEMI patients depend on the successful coordination of care in a

183
EP16
continuum from prehospitalization through admission. Nurses are responsible for care delivery at every phase and are integral to the planning, development, education and implementation of the processes. There are two key interprofessional committees that design and oversee care related to cardiovascular emergencies: the Acute Coronary Syndrome (ACS) Quality Support Team (QST) and the Chest Pain Steering Committee. The ACS QST is co-chaired by Barbara Craighead, BSN, RN, Clinician IV, in the Emergency Department, and Nancy Fauber, MSN, RN, Quality Improvement Coordinator, in the Cardiac Catheterization Lab, and includes representatives from Emergency Medical Services (EMS), the Emergency Department, Cardiac Cath Lab, Pharmacy, and acute and critical care cardiology nursing units. (Exhibit EP16.d: ACS QST Mission and Goals 2013-2014) The purpose of this group is to continuously improve the quality of patient care and the effectiveness and efficiency of services, systems and processes related to the delivery of patient care for adult cardiology patients with the diagnoses of ST elevation MI, non-ST elevation MI, and unstable angina. Each STEMI case is reviewed to evaluate protocols and process improvement across the continuum of care. The Chest Pain Steering Committee is a large interprofessional group whose scope is specific to the ED care but broader in nature. This committee is co-chaired by Craighead and David R. Burt, MD, and addresses many aspects of practice, education and research related to cardiac care. Examples of topics for this group include Chest Pain Center orientation, protocol and tool development, medication changes, ACTION registry data and outreach to EMS. ACTION, a “Get With The Guidelines” registry, is a risk-adjusted, outcomes-based quality improvement program. It focuses on high-risk STEMI / NSTEMI patients and helps hospitals apply American College of Cardiology / American Heart Association (ACC / AHA) clinical guideline recommendations. Each of these committees includes nurses who contribute to planning and decision-making. Craighead’s leadership on both committees allows for continuity and coordination of work. Her expertise, longstanding participation and leadership are valued and respected. Craighead has cultivated strong partnerships that have contributed to the success of the UVA STEMI program. The strength of the collaborative leadership in the ED also contributes to the success of the STEMI program. An “all hands on deck” approach ensures that patients get what they need. All ED team members are trained in the STEMI protocol. Security guards, ED registration personnel, patient care technicians and nurses are trained to screen for symptoms of chest pain, which patients may exhibit in the ED waiting
184
EP16
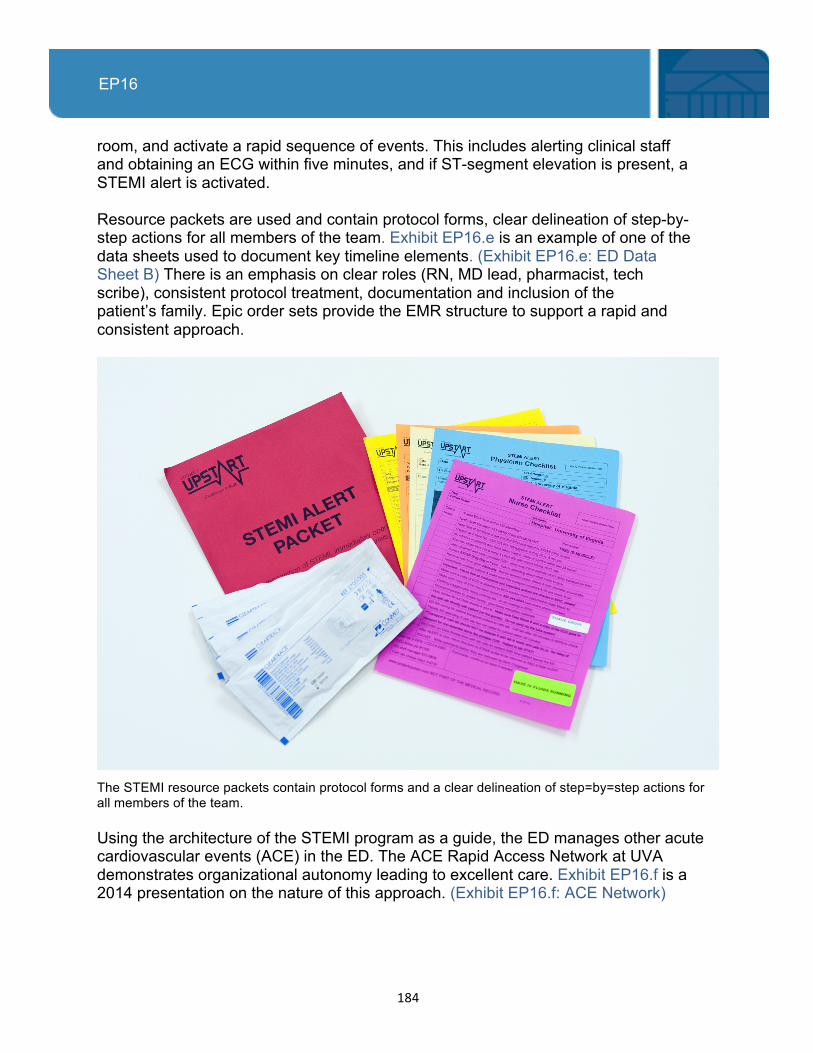
room, and activate a rapid sequence of events. This includes alerting clinical staff and obtaining an ECG within five minutes, and if ST-segment elevation is present, a STEMI alert is activated. Resource packets are used and contain protocol forms, clear delineation of step-by-step actions for all members of the team. Exhibit EP16.e is an example of one of the data sheets used to document key timeline elements. (Exhibit EP16.e: ED Data Sheet B) There is an emphasis on clear roles (RN, MD lead, pharmacist, tech scribe), consistent protocol treatment, documentation and inclusion of the patient’s family. Epic order sets provide the EMR structure to support a rapid and consistent approach.
The STEMI resource packets contain protocol forms and a clear delineation of step=by=step actions for all members of the team. Using the architecture of the STEMI program as a guide, the ED manages other acute cardiovascular events (ACE) in the ED. The ACE Rapid Access Network at UVA demonstrates organizational autonomy leading to excellent care. Exhibit EP16.f is a 2014 presentation on the nature of this approach. (Exhibit EP16.f: ACE Network)
185
EP16
The ACE emergencies treated through this approach include:
• STEMI (ST-segment elevation myocardial infarction) • Stroke: Acute ischemic CVA • Sudden Cardiac Arrest (SCA) with spontaneous return of circulation (SROC) • Aortic emergencies (AE): Ruptured AAA and dissection
An example of the success of the STEMI alert process is found in the case of a patient who arrived in the ED on June 29, 2014. With a chief complaint of chest pain, he triggered a rapid assessment by Tonya Showalter, RN, CEN, Clinician III. Exhibit EP16.g: STEMI Checklist Documentation is the documentation of the checklist elements as they were completed for this patient in the ED. Only 72 minutes elapsed from the time that patient arrived in the facility to the time the cardiac catheterization sheath was removed following a successful procedure. Implementation of the Inpatient STEMI Alert – March 2014
The hospital Patient Safety Committee identified opportunities for improvement with the internal STEMI response system. While rare, unrecognized STEMIs experienced by inpatients can be a catastrophic event. The ACS QST was tasked with developing a program to disseminate the successful principles and practices from the ED to adult inpatients who exhibit STEMI symptoms. The ACS QST identified key strategies for implementation success: 1. Collaborate with acute cardiology inpatient units to develop a guideline for response
to cardiac critical events such as chest pain. 2. Determine who will be responsible for obtaining emergency ECGs on any unit
throughout the hospital. 3. Ensure education and hands-on training are provided to those who will obtain ECGs
and that a mechanism is in place for ongoing competency. 4. Collaborate with hospital Patient Safety Committee to implement the guideline
across the hospital. 5. Insure technical logistics are in place, such as protocol orders for emergency ECGs
and automatic upload of ECGs into Epic. 6. Review / analyze data on inpatient STEMI cases with focus on early recognition /
action steps. Nursing input in the development of a guidance document to achieve these strategies spanned many nursing and interprofessional committees. The workflow of the acute care nurse as well as the Medical Emergency Team (MET – a rapid response team composed of RNs) nurses was considered.

186
EP16
The committee incorporated the strategies into a Clinical Practice Guideline. In March 2014, the Emergency Management of Suspected Cardiac Event guideline was presented by Craighead and Dr. Burt to the Patient Care Committee. The committee approved the guideline for full implementation. The inpatient STEMI alert activates the assessment and response to rapidly bring the necessary resources to the patient. Necessary education included ECG competency demonstration at the April 2014 skills days. (Exhibit EP16.h: Inpatient STEMI Guideline) Nurses played a critical role in the organizational development of the STEMI alert system at UVA and its dissemination nationwide, as well as within the whole inpatient system of our institution. Nurse leadership on key organizational committees has facilitated a robust rapid action system that delivers quantifiable improvements to our patients’ care and outcomes. Participants: EP16 Table 2: Participants, ACS QST and Chest Pain Steering Committees Name Discipline Title Department Mark Adams Nursing RN Clinician IV CCU Yasir Akhtar Physician Resident
Physician Medicine/Cardiology
Kirk Barbieri Information Technology
Director Specialty IT and Outcomes
Information Technology
Will Barnhardt Project Coordinator
Project Coordinator
Emergency Services
Lea Becker Research Clinical Research Coordinator Senior
Department of Emergency Medicine
Erin Berry Scribe Scribe ED Karen Braden Nursing Quality
Improvement Coordinator
ED
Michael Bradley Patient Care Technician
Patient Care Technician
ED
Mercy Bradshaw Nursing RN Clinician III ED Myra Brent-McGarry
Nursing Quality Improvement Coordinator
Cardiac Catheterization Lab
David Burt Physician Assistant Professor of Emergency Medicine
Emergency Medicine

187
EP16
Barbara Craighead
Nursing RN Clinician IV ED
Kerriann Dooley Nursing RN Clinician II ED Elaine Dube Nursing Registered Nurse Neuro ICU Steven Dunn Pharmacist Pharmacy Clinical
Coordinator Pharmacy
Nancy Fauber Nursing Quality Improvement Coordinator
Heart and Vascular Center
Suzanne Fuhrmeister
Nursing Advanced Practice Nurse 1-Clinical Nurse Specialist
4 East
Chris Ghaemmaghami
Physician Associate Professor of Emergency Medicine
Emergency Medicine
John Gilday Nursing RN Administrative Coordinator
Emergency Services
Larry Gimple Physician Professor of Medicine
Cardiology
Jenny Hamby Nursing Nursing Education Coordinator II
ED
Tina Hardison Pharmacy Pharmacy Clinical Coordinator
Pharmacy
Patricia Higgins Nursing Director ED Meghan Hinger Nursing Manager ED Jon Howard Nursing RN Administrative
Coordinator Emergency Services
Marian Lawson Nursing Manager, Heart and Vascular Center Quality
Heart Center
Lewis Lipson Physician Associate Professor
Cardiovascular Medicine
Bob Melady Nursing RN Clinician IV ED Chris Miller Nursing RN Clinician I ED Blee Moffett Nursing Manager Medical Emergency
Team Matt Mrazek Nursing RN Clinician I 4 East Karen Partlow Pharmacy Pharmacy
Resident Interns and Residents
Mike Ragosta Physician Professor of Cardiology

188
EP16
Medicine Michael Salerno Nursing RN Clinician II ED Nicole Shifflett Patient Care
Technician Patient Care Technician
ED
Joshua Stanton Physician Instructor of Emergency Medicine
Emergency Medicine
Christopher Stokes
Physician Resident Physician
Emergency Medicine
Joan Tepper Nursing Nurse Manager 4 East Julian Wiebe-Johnson
Nursing Clinician II ED
Sandy Weaver Nursing Procedure Coordinator
Heart and Vascular Center
March Winstead Emergency Preparedness and Response
Emergency Preparedness and Response Coordinator
Emergency Services
Greg Wozneak Nursing Director Heart Center