Embed Size (px)
DESCRIPTION
Â
Citation preview

EXAMINING THE ROLES OF MOTHER LEADER GROUPS IN THE
LIRA USAID CHILD SURVIVAL PROJECT
NORTHERN UGANDA.LIRA USAID CHILD SURVIVAL PROJECT

AUTHORS1. Aguze George 2. Lydia Akulo 3. Dr Isaac Odongo 4. Omoo Henry

ISSUES;Although child mortality has been on the decline, Uganda remains a high priority country for child survival.
A new report shows that Uganda is one of 24 developing countries where 100 deaths per 1,000 live births are still registered.

ISSUES CONT---Currently, the < 5s mortality rate is 131
per 1,000 live births, the highest rate in East Africa as compared to Kenya 107 per 1,000 live births, Tanzania, 122 and Rwanda 23 per 1,000 live births
The major causes are :- Malaria, Pneumonia, diarrhea, Malnutrition and HIV/AIDS.
Dr Jane Achan President of the Uganda paediatric Association Kampala September 2013

DESCRIPTIONIn September 2009, Medical Teams International -Uganda received a grant from USAID to implement,a 4 year Child survival project in 3 selected sub counties of Aromo, Ogur and Lira in Erute North HSD.
The project overall aim aligned with MOH goal to reduce child morbidity and mortality in Uganda.

DESCRIPTION CONT----- Specific objectives related to ;
1) Making communities assume responsibility for their own health through strengthening community capacity (VHTs, PDCs, HSD)
2) Improved health (C-IMCI) and child care (ECD) behaviors among mothers of children <5 years
3) Improved quality of health facility services through strengthened IMCI and MNC capacity
4) Strengthened institutional capacity of MTI and DHO to implement effective and efficient child survival activities.

PROJECT LEVEL OF EFFORTS

STRATEGIES USED:
Targeted behavior change at the household level.
The project assumed that key family practices, and subsequently health status, will be improved at the household level by building the capacity of Village Health Teams in Community-based Integrated Management of Childhood Illness (C-IMCI) using a social and behavior change approach.

Community mobilization Through capacity building of
community organizations and leaders including planning and evaluation, and activities for sustainable positive health outcomes.

Quality of care and access at the clinic levelBy implementing IMCI through training,
mentoring, supportive supervision for health facility staff and strengthening of referral and logistics systems.

Institutional capacity building for MTI and partners focusing on improved program quality and technical skills, strengthened project monitoring and evaluation, and institutionalization and dissemination of lessons learned.

WHY LEAD MOTHER GROUPS Initially our primary focus in the community
were the Village Health Teams, PDCs and local leaders. The MTE KPC showed significant improvements in some indicators while others had not improved.
Bottle necks to the project were identified, key among others was that there are only two instead of the mandated five VHTs per village and there are many demands on their time by government programs and other NGOs.

Though we had trained 560 VHTs for project support, there was no additional funding to train more VHTs.
The MTE recommended an innovative approach. Additional 1,128 up from 300 Mother Leader groups were identified and trained to compliment the roles of the VHTs.
These are young mothers who are energetic, chosen by the community and able to influence to fellow mothers to seek health services for their children.

The training of the Mother Leader Groups was meant to provide needed support to VHTs in reaching every household with a pregnant woman or children under two with key messages on maternal newborn care, complementary feeding, and optimal breastfeeding.

While supporting behavior change in these interventions, the MLGs were also mentored to promote sanitation and monitor child health cards to minimize immunization drop-outs.

METHODS To determine the desired change that could
have been brought by the Lead Mother Groups.
A simple comparative study was set out to examine the Roles of Mother Leader Groups in the Lira USAID Child Survival project as compared to the VHTs.

The study was interested in looking at the trend of at least 4 indicators; OPD utilization (Utilization of OPD per capita) immunization (DPT3 coverage), deliveries at health units (% deliveries at Health facilities) and 4th ANC attendance (Proportion of pregnant women who visited ANC Clinics 4 times during their pregnancy)

We conducted a panel review of the HMIS, HSD Annual reports of fiscal years 2009/10- 2012/13 ,KPC FE preliminary reports and interviews with the health service providers to help determine whether the participation of the lead mother groups improved the above indicators.

EXPERIENCE By the end of the project all the
parameters had significantly improved.
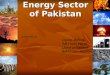
OPD utilization improved from 0.1 in 2010/11 to 0.6 in 2012/13 in Aromo Health centre.
In Ogur HCIV there was also a positive trend, the utilization increased by 0.2

In Aromo HC III, there was a remarkable change in 4th ANC attendance with a steady increase throughout the years but more realized in the 2011/12-2012/13 where the MLGs were actively working.
The same trend is also observed for DPT3 coverage with a record high of 87% in 2012/13.
Note worthy Bar Apwo and Ogur Health Centre IV had a significant improvement in the DPT 3 coverage up to 111% in 2012/13 from 87% and 93% respectively in 2011/12.

TREND OPD UTILISATION OVER YEARS

TREND OF DPT3 COVERAGE

DELIVERY UNDER SKILLED ATTENDANCE

KEY LESSONS LEARNT:
The involvement of the Lead mother groups in the Child Survival project complimented the roles of VHTs and improved mobilization for the CSP services.
The use of a well trained and motivated Mother Lead Groups is a better strategy for the success of a child survival project.
Mother Leader Groups are specific and devote their time in supporting fellow peers

Mothers tend to listen to the mother leader groups better as compared to the Village Health Teams
The communities and local leaders as well as health workers appreciated the role of the Mother Leader Groups in giving timely health education regarding maternal and child health issues and increasing early health seeking behaviors among women.

CONCLUSION
The involvement of the Mother leader groups in the USAID Lira child survival project ;
Improved community mobilization and early seeking health behavior,
Increased access to child survival services among women in Erute North Health Sub district.

RECOMMENDATIONS: For the success and sustainability of future Child Survival project we recommend the following:
The “Leader Mother groups” is a better community focus for Child Survival project.

MoH should consider investing in building the capacity of Lead Mother Groups to compliment the roles of VHTs in Maternal and Child Health programming.
This Innovation “The Lead Mother Groups” should be replicated in other USAID Child survival and Health grants program as a “best practice”.