Embed Size (px)
Citation preview
Indian 07. Pediat. 38: m6, ~97 ~
E N Z Y M E S T U D I E S ON WHITE B L O O D CELL~i A N D THEIR SIGNIFICANCE FOR GENETICS*
RICHARD WAGNER* *
Bosr Mass., U.S.A.
T h e a u t h o r e x p r e s s e s h |~ m o s t c o r d i a l c o n g r a t u l a t i o n s to Dr. K.C.
C h a u d h u r l o n t h e o c c a s i o n o f h i s 70~h b i r t h d a y , w i t h h a p p y r e m e m -
b r a n c e s o f t h e l r p r e v i o u s a s s o c i a t l o n at t h e U n l v e r s ~ t a t s K i n d e r k l l n i k
i n V | e n n a ,
Leukocyte enzyme assays provide insight into the mo!ecu!ar basis of some of the glycogen storage diseases (G.S.D.), after evidence that glycogen accumulates in the polymorphonuclear leukocytes (Wagner 1947). It tins been shown that the enzymatic degradation of leukocyte glycogen follows the samepattern as that in the liver (Wagner 1950, Wagner and Reinstein 1950,Wagner andYonrke 1952, 1953, Wagner etal. 1956 1958. One of the most important developments resulting from the study of leukocyte enzymes is the further elucidation of the enzymic basis of type V! G.S.D. Different in- vestigators have obtained remarkably consistent results in the study of leukocyte phosphorylase in hepatic phosphorylase deficiency (cf. Hulsman etal . (1961), Williams and Field (1961), Wallis et al.
(1966), Esmann el aL (1969), and van Creveld and Huijing (1965). All the
*From the Department of Pediatrics, Tufts University School of Medicine, and the New England Medical Centre Hospitals (Boston F]oating Hospital Division), Boston, Mass. 02111. (Address reprint reque,ts to Dr. Richard Wagner, New England Medical Center Hos- pitals, x71 Harrison Avenue, Boston, Mass. o=II L U.S.A.)Supported by General Research Support Grants 27537 and 27316 of the New England Medical Centre Hospitals, Boston, Massachusetts.
** Professor of Pediatrics, Emeritus.
patients studied by these authors showed a marked decrease of phosphorylase activity of the leukocytes. Esmann et al.
(1969) reported a sex linked mode of inheritance.
From our present knowledge, the study of phosphorylase and phosphorylase kinase of the leukocytes in hepatic phosphorylase deficiency appears to be of paramount importance in formulating a patient's diagnosis and prognosis. This type of glycogenosis is the most frequently encountered form (according to Hers (1965) from 30 to 35 per cent of all cases), and it is the most benign. Most patients showing active glucose 6-phos- phatase and amylo- 1,6-glucosidase activity belong to this type. Altogether it has provided the main contribution to our present knowledge of tile genetics of the disease. Huijing and Fernandes (1969) demonstrated this in their studies on X-chromosomal inheritance of liver glycogenosis with phosphorylase kinase deficiency.
In contrast, there are limitations to the biochemical study of liver biopsy specimens. We are occasionally con- fronted with the study of patients who reveal extremely, high values of liver glycogen and in vivo all characteristics of hepatic glycogen depositii~n disease,
\ , V A G N E R - - E N Z Y M E STUDIES ON W H I T E BLOOD CELLS 107
yet show normal enzymatic activity of liver and muscle specimens in vitro. During the past few years we saw eight patients with hepatic glycogenosis who could not be subclassified by liver biopsy. In the following are listed the essential laboratory data of a five-year- old male patient with liver glycogenosis and normal enzyme assay of the phos- phorylitic pathway in the liver biopsy specimen, including glucose 6-phos- phatase, amylo-l,6-glucosidase and phos- phorylase. Leukocytes:
Glycogen concentration (a) 10.4 t~g per 1• 106 (normal
3 to 4 vg/1 • 106 cells) (b) 10.5 /~g. per 1• 106
Phosphoryl ase (a) negligible (b) 2 1 /,m. PO4/min./lx 10" (c) 2.6 #m PO4/min./l• 109
(normal approximately 15 t~mol, phosphate/rain./ i• 109 cells)
Glucose 6-phosphate dehydrogenase (a) 26.4 units (normal 33.3
+ 6.9 units) (b) 18.9 units
Phosphorylase in the mother 4.0/,m. PO~/min./1 •
Phosphorylase in one of two siblings 16.5 tLm. PO4/min/1 • 109
Leukocyte phosphorylase kinase in units/min/mg, protein for the patient 0.14; the mother 0.23 ; and the father 0.34 (normal 0.3-1.2).
Km tbr phosphorylase kinase in units/ ml. for the patient 1667;the mother 500; and the father 135 (normal approxim. 100).
Vmax in units/min/mg, protein for the patient 3 ; the mother 1.7; and the father 2 (normal 1-2).
The patient thus belongs to the sex linked type of glycogen storage disease (type Via) characterized by low phosphorylase and low phosphorylase kinase activity of the leukoeyteys; he is hemizygous deficient. The mother is a heterozygote (Wagner et al. 1971).* Hiujing (1970) demonstrated low phosphorylase kinase activity in the leukocytes due to altered kinetic properties of the enzyme, Km being extremely high in male children and significantly increased in the mothers, indicating low enzyme-substrate affinity.
Although leukocytes do not represent a homogeneous cell population in the peripheral blood, only the phosphorylase assays per 1• 109 mixed leukocytes are recorded It was shown that the poly- morphonuclear leukocytes are the main carriers of enzyme activity, but no correction factor for the proportional share of these cells was introduced. More exact is the expression of enzyme activity per rag. protein. All white blood cells, granuIocytes, lymphocytes and monocytes, and also the blood platelets, have approximately equal specific activity for phosphorylase when expressed per rag. sup'ernatant (cytoplasmic) protein.
Another enzyme included in our study on leukocyte enzymes in GSD is glucose 6-phosphate dehydrogenase (G6PD) (Wagner and Porter 1971). Human leukocytes contain abundant
*The technique for determining leukocyte phosphorylase is the same as m W~gner el al.
(!97 ~ ).
]0[~ INDIAN JOURNAL OF PEDIATRICS
amounts of it anld the polymorphonu- clear leukocyte is its main carrier.
The activity of G6PD is assayed according to Marks' (1958) modification of the method of Kornberg and Horecker (1955) based on the reduction of triphorphopyridine nucleotide (TPN). The reaction mixture is set up directly in the Beckman cuvettes and read at 340/x/x at one minute intervals, usually for twenty minutes. The reaction mixture for the G6PD assay consists of 0.5 ml. of 0.25 M glycylglycine buffer, pH 7:6; 0.5 ml. of 0 1 M magnesium chloride; 0 1 ml. of 0.5 M glncose-6-phosphate, pH 7.6; and 0 .3ml . of2 .3 • 10 ~ a M T P N . The re lume of the cell extract is adjusted to give an increase in optical density of from 0.015 to 0.100, usually equivalent to 2 to 4 • 106 leukocytes. The total
volume is made to 3.0 ml. with distilled water. In the blank the substrate is omitted. The activity is expressed in uni ts- -one enzyme unit equals the change in optical density per minute per 1 • 109 leukocytes. Although the leukocytes were contaminated with some blood platelets, no correction was allowed for their share in the total activity, in general, the activity of 1 • 109 blood platelets is negligible compared with that of the same number of leukocytes.*
G6PD leukocyte activity was studied in 16 cases of hepatic glycogenosis and in one case of fructose intolerance. The normal value is 33.3 +_+_ 6.9 units. Eight yon Gierke cases (with liver glycogen of
* G 6 P D activi ty of isolated h u m a n blood platelets , accord ing to R a m o t e t a l . (1959) a m o u n t s to o.x27 q - 0 . 0 3 8 uni ts . Since the average rat io of blood platelets to leukocytes in our cell suspens ions was found to be 2:*, the share o f platelex activity did not exceed 1.4 to 3 per cent.
VOL. 38, No. 278
from 6.2 to 10.5~ showed normal, or in two instances moderately increased, activity of G6PD, up to 42.8 enzyme units. One patient whose parents were first cousins, revealed all stigmata characteristic of yon Gierke's disease, but did not show in vitro or by histochemical examination the glucose 6-phosphatase defect (termed "functional deficiency of glucose-6-phosphatase" by Senior and Loridan (1968). This case showed G6PD activity almost 100 per cent higher than the norm. One patient with limit dextrinosis showed strikingly low values on repeated examinations. Two female patients with hepatic phosphorylase defect revealed G6PD activity ap- proximately 100 per cent higher than the norm. Three unclassified cases showed G6PD activity within normal limits in two instances, and decreased activity in the third. In one case the glycogen concentration of the liver was 14.9 per cent, but normal activity was
found for phosphorylase, glucose-6- phosphatase, and amylo-1, 6-glucosidase, though unfortunately w e had no determination of leukocyte phosphorylase. Noteworthy for this case is that two brothers had significantly enlarged livers; one brother and also the mother showed an increase of G6PD activity in the leukocytes (46.6 units for the brother and 53.7 for the mother), while the activity in the leukocytes of the patient was markedly decreased (19.8 units). Probably we are dealing with an autosomal recessive aberrat ion, and the patient would be homozygous for the abnormal gone
Two Mauriac patients had low G6PD activity. In the patient with fructose intolerance, G6PD activity was sig~fifi- camly incleased; also liver G6-
,~4rAGNEt~--ENZYME STUDIES ON ~.agHITE BLOOD CELLs 109
phosphatase was far above the norm, 1272 t~g. p/100 rag. liver at pH 6.7 (similar observation by Hers 1965). It is of interest that the two patients with significantly increased G6PD activity were girls who showed a phosphorylase deficiency. This contrasts with the male patient with X-chromosomal inheritance discussed above, whose G6PD activity was rather low. For the two girls leukocyte phosphorylase and phosphory- lase kinase values were not available. Possibly they may be classified as GSD, type VIb (Huijing 1970).
Huijing (1964) found that amylo-l, 6-glucosidase, or debranching enzyme, is present in leukocytes of normal persons; in Ieukocytes of patients with limit dextrinosis (type III) no amylo-1, 6-glucosidase is found. Hoof and Hers (1967) distinguished several subtypes of debranching enzyme deficiency on an enzymic basis. Extensive studies were carried out on patients with type I I I glycogenosis and their families. These investigators included Williams et al.
(1963) and Williams and Field (1968) and Esmann et al. (1969). The latter tbund amylo-1, 6-glucosidase low in the cells of the proband and his mother, whereas the maternal grandparent had normal enzyme activity.
Further scientific knowledge obtained by the use of leukocytes was the proof that branching enzyme deficiency is indeed the cause of type IV GSD, as had been assumed from the abnormal glycogen structure. Enzyme assays in leukocytes of such a patient's relatives suggest autosomal recessive inheritance (Brown and Brown 1966, Fernandes and Huijing 1968, Legum and Nitowsky 1969).
As mentioned above, the classification of liver glycogenosis has certain limita- tions. Studies of the enzymatic activity of the leukocytes appear to contribute to the diagnosis as well as to the detection of the genetic pattern of glycogen storage disease, types III , IV and VI.
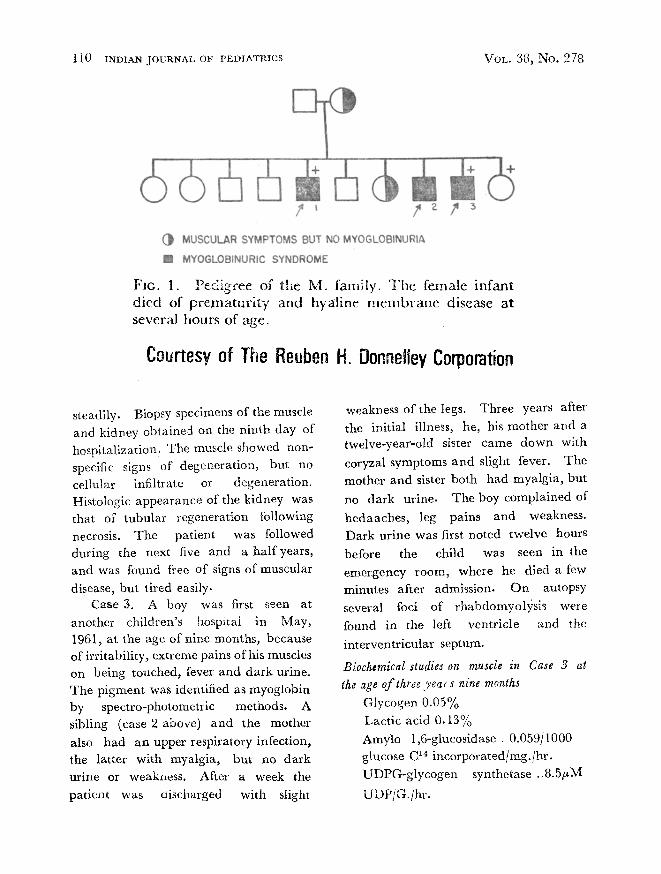
Other disease entities where leukocytes participate in the metabolic error are familial paroxysmal rhabdomyolysis, which is a myoglobinuric syndrome (Fawara et al. 1967) and galactosemia. Some of the particulars of paroxysmal rhabdomyolysis m a y be
seen in Fig. 1. Case 1. A two-and-a-half-year old
boy, in October 1942 was acutely ill with diarrhoea, nausea and headache, associated with weakness of the legs. The urine was not dark. He died after three days from respiratory insufficiency. Diagnosis: acute poliomyelitis. Probably this was rhabdomyolysis, since there were no other cases of poliomyelitis in the small country town. Subsequent experience suggested to the mother of this striking family group that this illness was similar to that of the two siblings described below.
Case 2. A three-and-a-half-year old boy was treated in September, 1959, for an upper respiratory infection with penicillin, triple sulfa drugs and salicylates. Three days later, lethargy, anorexia and severe leg pains appeared and necessitated admission to the Boston Floating Hospital. The urine was dark brown with oliguria and proteinuria 3+ . Seizures were observed on the day of admission. Lumbar puncture revealed normal pressure and cell free fluid. Coxakie virus (A-9) was isolated several weeks later. Tile patient improved
i l0 INDIAN JOURNAL OF PEDIATRICS VOL. 38, No. 278
@ MUSCULAR SYMPTOMS BUT NO MYOGLOIBINURIA
[ ] MYOGLOBiNURIC SYNDROME
FIG. 1. Pedigree of the M. family. T h e female infant died of prematur i~y and hyal ine m e m b r a n e disease at several hours of age.
Ceurtesy of The Reuben H. Donneliey Corporation
steadily. Biopsy specimens of the muscle and kidney obtained on the ninth day of hospitalization. The muscle showed non- specific signs of degeneration, but no cellular infiltrate or degeneration. Histologic appearance of the kidney was that of tubular regeneration following necrosis. The patient was followed during the next five and a half years, and was found free of signs of muscular
disease, but tired easily. Case 3. A boy was first seen at
another children's hospital in May, I961, at the age of nine months, because of irritability, extreme pains of his muscles on being touched, fever and dark urine. The pigment was identified as myoglobin by spectro-photometric methods. A sibling (case 2 above) and the mother also had an upper respiratory infection, the latter with myalgia, but no dark urine or weakness. After a week the patient was discharged with slight
weakness of the legs. Three years after the initial illness, he, his mother and a twelve-year-old sister came down with
coryzal symptoms and slight fever. The mother and sister both had myalgia, but
no dark urine. The boy complained of'
hedaaches, leg pains and weakness. Dark urine was first noted twelve hours
before the child was seen in the emergency room, where he died a few minutes after admission. On autopsy several loci of rhabdomyolysis wele found in the left ventricle and the
interventricular septum.
Biochemical studies on muscle in Case 3 at
the age of three year s nine months
Glycogen 0.05% Lactic acid 0.13% Amylo 1,6-glucosidase . 0.059/1000 glucose C 1~ incorporated/mg./hr, UDPG-glycogen synthetase ..8.5/~M
UDPiG./hr.
W A G N E R - - - E N Z Y M E STUDIES ON W H I T E E L O O D CELLS 1 ~
Phosphorylase .. 156-180~M phosphate /G./min. Phosphorylase (specific activity) 2.18-2.58 Lactic dehydrogenase... 218 units/G. Total protein in homogenates 4.4-4.9 mg./ml. Case 2. White blood cell phosphoryr
lase...23.6 /~M phosphate/min.[109 leukocytes. Mother of the patient: Muscle glycogen ...... 1.3% Muscle lactic acid...0.35% Phosphorylase 154.8 ~M phosphate] G./min.
Phosphorylase (specific activity)...2~ 18 Lac t ic dehydrogenase ..464 units/G. Total protein in homogenate...3.5 mg./ml. Rhabdomyolysis appears to be an
inborn error of glycogen metabolism. Muscle phosphorylase activity, and specific activity corrected for protein
content, are strikingly increased. Also, leukocyte pho;phorylase in Case 2 is almost 60 per cent higher than in the norm (15 to 16). Normal values for muscle phosphorylase activity are usually 75 to 90 /xM phosphate per gm per minute with rare values up to 100/~M. The homogenized material, unlike any
previously examined, exhibited activity in the centrifuged sediment as well as in the supernatant. Lactic dehydrogenase activity was low in Case 3.
One of several other pathological conditions occasionally associated with myoglobinuria is McArdle's myopathy, characterized by d~crea~ed or missing phosphorylase activity, in contrast to the excessive phosphorylase activity in rhabdomyolysis with myoglobinuria.
This might be another example of homeostasis known from other physiologi- cal equilibria. Further studies regarding
muscular phosphorylase activity in
patients with rhabdomyolysis and
myoglobinuria during the patient's well
periods, such as our Case 2, are necessary to answer this question. Our two patients (Cases 2 and 3) belong to
what Korein et al. (1959) have called the
toxic form of myoglobinuria, in contrast to the exertional type.
The mode of inheritance is debatable, whether X-linked or autosomal dominant. In the pedigree of the family
discussed in this article, only the two
boys (Cases 2 and 3) had myoglobinuria. In Case 1 the diagnosis was question- able. The mother and one sister of the boys had only myalgia, but no
myoglobinuria. I f myoglobinurla is considered an essential sign of the full picture, we would label the inheritance
X-linked or autosomal recessive. On
the other hand, i fmyalgia elicitated by an intercurrent infection, as in the case of the mother and one sister, were considered sufficient proof of the same disease entity, the inheritance would be autosomal dominant. Most reports on siblings with myoglobinuria fit into this category, and both male and female subjects are affected. The situation is analagous in ectodermal dysplasia of the anhydrotic type, where the mother of a patient may show absence of the sweat glands in a small area of the skin, without revealing the full picture of the disease. More families with detailed biochemical studies are needed to solve the genetic problem.
112 INDIAN JOURNAL OF PEDIATRICS
Galactosemia is transmitted as an autosomal recessive. The heterozygous carrier of the abnormal gene is detectable
t h r o u g h galactose tolerance tests. Hsia (1960) found decreased P-gal-uridyl-
transferase among parents of galactose- mia patients. During incubation with
galactose, galactosemic leukocytes ac- cumulate more galactose-l-phosphate than do normal leukocytes (Weinberg and
Segal 1960).
S u m m e r y
The application of leukocyte enzyme assays to the diagnosis and study of genetics has been demonstrated in the following errors of metabolism: glycogen storage disease, familial paroxysmal rhabdomyolysis and galactosemia. Under such a programme the activity of
the following enzymes is included: phosphorylase, phosphorylase kinase,
glucose 6-phosphate dehydrogenase,
amylo-1, 6-glucosidase and P-gai-uridyl- transferase. Leukocyte phosphorylase activity is significantly decreased in Hers
disease (type VI glycogenosis). Amylo-1, 6-glucosidasa is lacking in leukocytes of patients with limit dextrinosis, a defect
inherited as an autosomal recessive trait.
Similar inheritance exists in type IV
glycogenosis. Type Via glycogenosis
shows X-chromosomal inheritance, patients being hemizygous deficient and mothers heterozygotes. G6PD has been demonstrated as significantly increased
in two female children with Hers' glycogenosis (possibly VIb) .
Phosphorylase activity ~ was found considerably increased in the skeletal muscle of a patient with familial
paroxysmal rhabdomyolysis, and in the
VOL. 38, No. 278
leukocytes of his brother. The mode of inheritance is debatable, whether X- chromosomal or autosomal dominant. During incubation with galactose, galactosemic leukocytes accumulate more galactose-l-phosphate than do normal
teukocytes.
References
Brown, B.I. and Brown, D.H. (i966). Lack of a-x, 4 glucose: a-I, 4 glucan 6 glucosyltrans- ferase in a case of type IV glycogenosis. Prec. Nat.
Acad. Sci. U.S.A. 56,725. van Creveld, S. and Huijing, E. (1965). Gly-
cogen storage disease. Biochemical and clinical data in sixteen cases. Arner. ft. Med. 38, 554.
Esmann, V., Bobolth, N. and Jorgensen; Jorgen I.B. (1969). Heredity of leukocyte phorphorylase
and ttmylo t, 6.glucosidase deficiency. 07. Pediat.
74, 9 ~ .
Fawara , B.E., Vawter , Gordon, F., Wagner, R., Kevy, Sh. and Porter. E. (I967). Familial p,~roxysmal rhabdomyolysis in children. A myoglobinuric syndrome, Amer. 07. Med. 9 42,
196. Fernandes, J.and FIuijing, F. (x 968). Branching
enzyme deficiency glycogenosis. Arch. Dis. Childh
43, 347. Hers, H,G. (I965). Glycogen storage disease.
Advances Metabol. Disorders, 1, x. H~ia, O. (i969) Inborn Errors of Metabolism Yearbook Medical Publishers, Chicago.
Huijing. F. (1964) Amylo-1, 6-glucosidase activity in normal leukocytes and in leukocytes of patients with glycogen storage disease. Ctin. Chem Acta 2 269
Huijing, F. (197o). Glycogen-~torage disease Type Via: Low phosphorylase kinase activity caused by a low enzyme-substrate affinity. Biochern. et Biophys. Acta 206, 144.
Huijing, F. and Fernandes, J. (1969) X-chro- mosomal inheritance of liver glycogenosis with phosphorylase klnase deficiency. Amer. 07. Human Genera 31 275
Hulsmann, W.C., Oei, T.L. and van Creveld, S. (1961). Phosphorylase activity on leukocytes from patients with glycogen storage disease. Lancet, 2 581:
Korein, 07., Coddon, D.R. and Mowrey, F.H. 0959). The clinical syndrome of paroxysmal
x,VAGNER--ENZYME STUDIES ON WHITE BLOOD CELLS 113
paralytic myoglobinuria. Report of two cases and analytical review of the literature. Neurology,
9, 767 �9 Kornbelg, A. and Horecker, B.L. (1955). In
Methods in Enzymology, Vol. !, p. 323- Academic Press, Inc., New York.
Legum, Cyril P. and Nitowsky, Harold, M. (1969). Studies on leukocyte btancher enzyme activity in a family with type IV glycogenosis.
J . Pedmt 74, 84. Marks, P.A. (1958). Red cell glucose-6- phos-
phate and 6-phosphogluconic dehydrogenases and nucleoside phosphorylase. Sciante, 127, 1388.
Ramot, B., Fisher, L, Szeinberg, A, Adam, A., Sheba, C. and Gafni, D. (1959). A study of subjects with erythrocyte glucose-6-phosphate dehydrogenate deficiency. II. Investigation of leukocyte enzymes. ~,. Clin. Invcr !18 2234.
Senior, B. and Loridan, L. (1968) Studies of liver glyeogenoses, with particular reference to the metabolism of intravenously administered glycerol. New Engl, J . Med 279 958.
Van Hoof, F. and Hers, H.G. (1967) . The subgroups of type I I I glycogenosis. Europ.
J. Biochem. 2, 265. Wagner, Richard. (1947). Glycogen content
of isolated white blood cells in glycogen storage disease Amer. J. Dis. Child. 73 559.
Wagner, R. (195o). Enzyme studies on white blood cells. I. Glycogen degradation. Arch Biochem 26. I'23.
Wagner, R. and Reinstein, S. (195o). Enzyme studies on white blood cells II. Phosphorylating glycogenolysis etc. Arch. Bochem. 29, 260.
Wagner, R. and Yourke, A. (i9~2) Studies on white blood cells I l I : Phosphorylating glycogenolysis and phosphorylated intermediates. Arch. Biochem & Biophys. 39, 174.
Wagner, R. and Yorke, A. (I953). Studies on white blood cells' IV. Glycolysis of added glucose. Hexokinase and adenyl pyrophosphatase activity. Arch. Biochem & Biophys, 44, 415,
Wagner, R, Meyerriecks, N. and Sparaeo, R, (~956) Enzyme studies on white blood cells and blood platelets, V. dehydrogenase activity. Arch. Biochem. & Biophys. 61, 278.
Wagner, R., Meyerriecks, N. and Sparaco, R. (1958). Glycogen storage disease (phosphorylated intermediate in the peripheral blood). 07. Pediat. 53, 683.
Wagner, R ' , Huijing, F. and Porter. F. (I97r). Hepatic glycogenosis due to phopholylase defi- ciency. Limitations of enzyme studies on liver biopsy specimens. Am#r 07. Med. In press.
Wagner, R. and Porter, E. (t971). Glycogen deposition disease and glucose 6-phosphate dehy- drogenase. Unpublished experiments.
Wallis, Patrlcia, G. Sidbury, James B., Jr. and Harris, Ruth, C. (t966). Hepatic phospho- rylase defect. Amer. 07. Dis. Child. 3, o78.
Weinberg, A.N. and Segal, St. (I96o). Effect of galactose-I-phosphate on glucose oxidation by normal and galactoJemic leukocytes. Science 13~, lot 5.
Williams, Christine, and Field, James, B. (I968). Studies in glycogen storage disease. III . Limit dextrinosis: A genetic study, a7 Pediat. 72, 214.
Williams, Hibbard, E. and Field, James, B. (196 0. Low leukocyte phospholylase in hepatic phosphorylase deficient glycogen storage disease.
07. Clin. Invest. 40, 184I. Williams, Hibbard, E., Kendig, Esther, M.
and Field, James B. (i963). Leukocyte de- branching enzyme in glycogen storage disease. a7. Clin. Invest. 42, 656