Embed Size (px)
Citation preview

Environmental Factors in Coronary Heart DiseaseAn Epidemiologic Study at Agra (India)
By KRISHNA S. MATHUR, M.D.. F.R.C.P.
CORONARY heart disease, emergiing fromobscurity in the early years of the cen-
tury, has become the most serious and imme-diate health problem in manv countries. InNew England the incidence has risen from 37per cent of 2,314 cardiac patients in 1928'to 48.5 per cent among 3,000 heart patients in1951.2 A review of a series of 1,284 consecu-tive hearts examined by the injection-plus-dis-section technic of Schlesinger, at the BethIsrael Hospital, Boston, during the decade1941 to 1950 revealed myocardial infarctionon gross and histologic examinlation of themyocardium in 268 or 20.6 per cent and oc-clusion of coronary arteries in 342 or 26.6per cent of the hearts.3
Comparable statistics on the subject are notavailable in India but the disease has appar-ently assumed menacing proportions and canbe presumed to be on the increase. Sanjivi,4Vakil,5 Samaini,6 and Padmavati7 have re-ported incidences of 11.8 to 13.5 per cent intheir hospital series of cardiac eases. In a sim-ilar study of heart cases in private practiceVakil8 found the frequency to be 26 per cent.Recently Malhotra9 reported an incidenee of28.3 per cent in combined hospital and privateseries.A most striking and potenitially importanit
fact about this disease is its geographic varia-bility, i.e., the great differences in its incidenceand mortality in different populations. It hasbeen reported, for example, that middle-agedinen in the United States, Great Britain, andFinland are more prone to die of coronaryheart disease than are men of the same age inNorway or Denmark, and are several timesmore prone than are men in Italy or Portu-gal; the disparity is even greater when com-From the Department of Medicine, Sarojini Naidu
Medical College, Agra, India.
684
parison is made with middle-aged men inJapan, with the Bantu in South Africa, theMayan Indians in Guatemala, the Navajosin New Mexico, the Jews in Yeman, the na-tives in Okinawa, the Negroes in Nigeria, andso on. Gordon'0 observed that the death ratefrom arteriosclerotic heart disease is loweramong Japanese in the United States thanamnong white Americaln men of the same agegroup, and it is still lower amiong Japanese inHawaii and in Japan.
These observations indicate the need forniew epidemiologic data that emphasize differ-ences of race, culture, ways of life, stress andstrain, and dietary habits. It is the purposeof this paper to determine the role of environ-mental and nutritional factors in the genesisof coronary heart disease froin an analysis ofcase records of patients treated in hospitalsand private practice as well as field surveysof the gen-eral population belonging to differ-eut socioeconomic groups. Such an approachmay supply a few clues to investigators, whomay then study these probleins in the labora-tory.
MaterialThese studies have been conducted at Agra, one
of the 3 big medical centers of Uttar Pradesh-the biggest state of India. The patients are drawnto this center not only from the rural and urbanpopulation of Agra, but from most of the sur-rounding western districts of the State.The nmaterial for these investigations has been
obtained from 2 sources: (1) ease records ofcoronary heart disease patients, and (2) surveysof the general population.
1. The clinical material for this studv wasdrawn from both hospital and private cases ofcoronary heart disease seen by the author" fromJanuary 1946 to August 1957. There were 553cases of coronary heart disease among 3,273 cardi-ae patients during this period. These included401 or 35.2 per cent of 1,127 private and 152 or7 per cent of 2,145 hospital cardiac cases, giving
Circulation, Volume XXI, May 1960
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
ENVIRONMENT AND CORONARY DISEASE
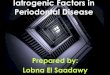
an over-all incidence of 16.9 per cent in the com-bined private and hospital series. Of these 553patients, 391 or 71 per cent were cases of myo-cardial infaretion, 133 or 24 per cent were anginapectoris, and 27 or 5 per cent were cases of coro-nary failure.
The peak age incidence in the present series was45 to 55 years (table 1). About two thirds of allcases between 40 and 60 years, 12.3 per cent werebelow 40 years, and the youngest was 18 years old.
There were 492 men (89 per cent) and 61women (11 per cent), the sex ratio being 8:1 Thesex difference was less marked after the age of45 years.The constitution of the patients was classified
as ectomorphic in 39 per cent, mesomorphic in 51.3per cent, and endomorphic in 9.7 per cent. Hyper-tension was present in 50.2 per cent, diabetes in13 per cent; and the serologic test for syphiliswas positive in 3.8 per cent.A family history of coronary heart disease was
available in 7.4 per cent, of hypertension in 3.8per cent, and of diabetes in 2 per cent of thecases. These figures do not reflect the true familialincidence of these diseases, since most of themhad been treated by practitioners of indigenousmedicine who did not diagnose these diseases, andsome others were ignorant of the cause of deathamong their close relatives.
2. The data concerning the general populationhave been obtained from records of a planned fieldsurvey12 of the incidence of coronary heart dis-ease including clinical and electrocardiographicstudies, detailed analysis of the dietary pattern,and estimation of the blood lipids among 1,056persons of the general population over the ageof 25 years belonging to different socioeconomicgroups.
In deciding on the socioeconomic classification,consideration was given to vocation, education,status in society, and income. Doctors, lawyers,university professors, high government officials,and businessmen with a monthly income over Rs.500 per month were classed as that "high-socio-economic group"; clerks, school teachers, pettyofficers, shopkeepers with income levels betweenRs. 100 and Rs. 500 per month were classed asthe "middle-socioeconomic group"; and industrial,manual, and agricultural workers with less thanRs. 100 as their monthly wages were grouped to-gether as belonging to the "low-socioeconomicgroup."
During the course of the present investigations216 of the high-, 350 of the middle-, and 480persons of the low-socioeconomic group werestudied. In the last category were included 230industrial, 121 manual, and 129 agricultural
Circulation, Volume XXI, May 1960
Table 1Age Distribution of 553 Cases ofDisease
Coronary Heart
Age group(years) Number Percentage
Below 20 1 0.121-25 4 0.726-30 10 1.831 35 22 4.036-40 32 5.841-45 67 12.146-50 101 18.351-55 113 20.456-60 76 13.761-65 64 11.566-70 39 7.171-75 18 3.276-80 4 0.7
Over 80 2 0.3
workers. Eleven cases of coronary heart diseasewere encountered, giving an over-all incidence of1.04 per cent.
ObservationsUrban Versus Rural
Of the 553 cases of coronary heart diseaseseen by the author 488, or 88.2 per cent, werefrom Agra and neighboring cities and towns,while the remaining 67 patients, or 11.8 percent, came from villages.One explanation may be that patients from
rural areas are less likely to travel to Agrafor an episode of chest pain, unless compli-cations arise, whereas the city dwellers beingconscious about heart attacks consult physi-cians on minor suspicion. The figures wouldnot then give convincing proof of the relativefrequency of coronary heart disease in urbanand rural populations. The answer will comefrom field surveys. Although our experienceof field studies in villages is limited, our im-pression is that the incidence is low in ruralpopulations.Socioeconomic Status
The incidence of coronary heart disease was35.2 per cent of all cardiac cases in privatepractice and 7 per cent of cardiac patientsadmitted to the hospital. The majority of theformer belong to the high-socioeconomic groupand the majority of the latter come from thelow-socioeconomic group. On further analysis
685
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

6MATHUR
Table 2Incidenscje of Coronary Heart Disease in DifferentSocioeconomic. Groups of the General Populationl
Number CoronarySocioeconomic group studied heart disease Percentage
HighMiddleLow
216350480
9
O
4.00.60
Industrial -230Manual -121Agriculturnll 1 .9
it was observed that of the 353 cases of coro-
nary heart disease 63.3 per cenlt belonged tothe high-, 25 per cent belonged to the middle-.and 11.7 per cent to the low-socioeconiomicgroup.
In the field studies among 1,056 unselectedindividuals, the incidence of coronary heartdisease was 4.1 per cent in the high groul,and 0.57 per cent in the middle group. Nocase was encountered among 480 industrial,manual, and agricultural workers (table 2).
These observations emphasize the markedpreponderance of coronlary heart disease inthe privileged class of society in contrast tothe socioeconomically backward class, whichenjoys a relative immunity fromn this disease.Diet
Of the 553 cases 62.2 per cent were vege-
tarians and 37.8 per celnt were nonvegetarians.But this question is unimportant in India be-
cause, with few exceptions, the so-called noni-
vegetarianis in India take meat only 2 or 3
times a week.We have therefore studied the nutritional
status of 102 consecutive cases of coronarv
heart disease with regard to daily intake offat, proteins, carbohydrate, cholesterol, totalcalories, amid percentage of calories from fatand compared themii with similar studies car-
ried out in field surveys ainonog normal per-
sons belonging to various socioeconlomicgroups.13 The focal point of interest in thediet has been the relationship of dietary fatto eoronary heart disease.The maximum incidence of coronary heart
disease in the field survey was found in per-
soIns of the high-socioeconomic group who
consume the highest amoulit of total dietary-
fat and derive the highest pereentage of cal-ories from dietary fat. Memnbers of the high-socioeconomic group consumed 86.3 per cenitof saturated fat versus 77.7 per cent by thosein the middle and 52.1 per cent in the lowgroups.The fat intake, percentage of fat calories.
and saturated fat in the dietarv pattern ofcoronary cases are similar to the high-socio-econiomic group of society, which bears thenaximum burden of coroniary heart disease.
Serum LipidsStudies of serum lipid in the field survey
gave the highest values of serumn cholesterolin the high-socioeconomic group and lowestin the low-socioeconomnic group; this was alsotrue for the values of seruim lipid phosphorus.The cholesterol/'phospholipid ratio in the 3groups did niot differ significantly froim on-eto another. A gradual rise in serum cholesterolwas also observed with age from 20 to 50years, after which a slight fall occurred. 14
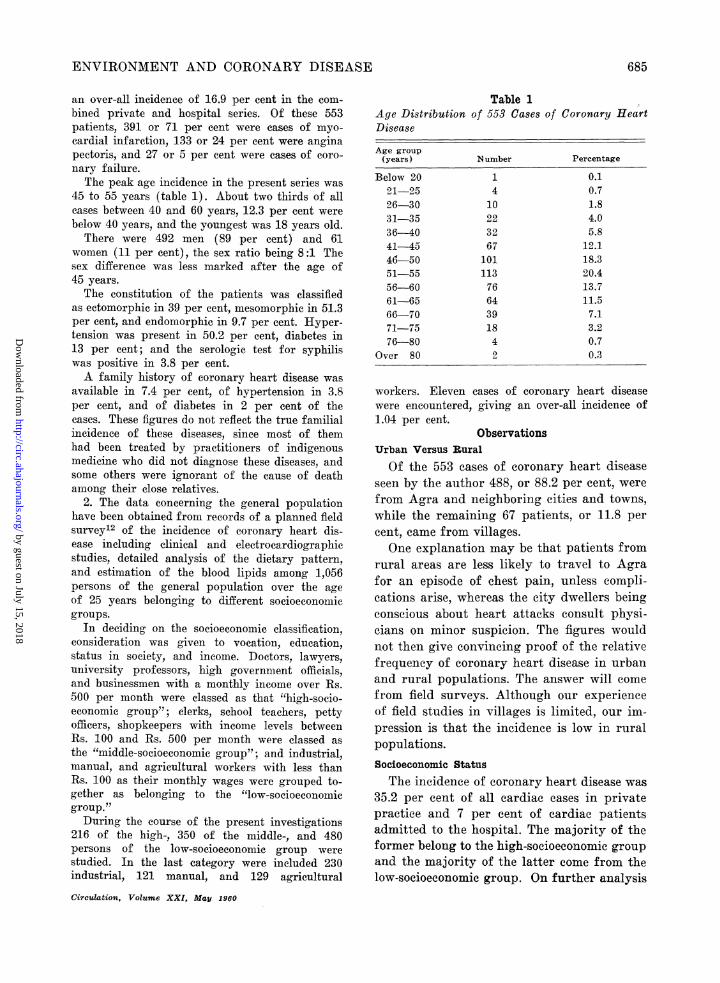
Eighty normal controls were drawn fromthis study anid matched according to age, sex,and socioeconomic status with 80 cases of cor-onary heart disease, and their serumn lipidswere compared.15The mean values of total serum cholesterol,
serum lipid phosphorus, anid cholesterol/phospholipid ratio were significantly higherin the coroniary group than in the controlgroup. In cases of coronary heart disease, therise in total serum cholesterol was greater thanthe rise in serum lipid phosphorus. There wasa considerable overlap of values between thecoronarv group and the normal group butvery high values were infrequent in normalindividuals.
It is considered that determination ofserum cholesterol is a reliable and simple pro-cedure for identifying persons with grossdisturbance of lipid metabolism, which isblamed as one of the factors in coronary heartdisease.
Physical Activity
Business executives formned the largest per-centage of 553 patients with coronary heartdisease, with doctors, landlords, anid high gov-
Circulation, Volume XXI, May 1960
686
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from

ENVIRONMENT AND CORONARY DISEASE
ernment officials following in order. Shop-keepers, clerks, alnd petty officers accountedfor a smaller group of such patients. Theminimum niumber of cases were found anmonglaborers and farmers. The results of the fieldsurvey confirmed the observations made inthe hospital wards and private practice.
In an evaluation- of the amount of physicalactivity involved in each case, it was roughlyassumed that the higher strata of society,which bear the maximum burden of coronaryheart disease, did little manual work inmarked conitrast to the poorer sections of so-ciety, whose work and nmode of life demandgreater amount of physical work.Stress and Strain
It is difficult to assess the part played bystress aiid strain on the incidence of coronaryheart disease in an epidemiologie study ofthis nature. The emotional tempo of life hasgone up considerably during the last 2 dee-ades, and this is more evident in the big cities.The poor Ilndian villager is quite removedfrom this tension and relaxes more comnpletelywhen away from his work; that may partlyexplain his relative protection from coronaryheart disease.Smoking and Alcohol
Our studies fail to establish any relationof smoking or alcohol to coronary heart dis-ease. Of 553 cases, only 149 or 26.9 per centsmoked and 62 or 11.2 per cent took alcohol,most of them moderately.
DiscussionPublished reports on coronary heart disease
from India are few.6' 8 9, 16 Their observationson the relationship of age, sex, and body buildto its frequency are similar. Its high incidencein upper class and urban population has beenreported. The conclusion drawin by Malhotra9that vegetarians were no less predisposed tocoronary heart disease than nonvegetarianshas not much significance. Environmentalfactors with special reference to socioeconomiestatus and their relationship to the dietarypattern and blood lipids in cases of coronaryheart disease as against the normal populationCirculation, Volume XXI, May 1960
Table 3Dietary Factors in Different Socioeconomic Groupsof General Population andHeart Disease
Cases of Coronary
Daily Percentagefat intake calories Percentage(Gm.) from fats saturated fat
Coronary heartdisease
High-socio-economic group
Middle-socio-economie group
Low-socio-economic groupInidustrial
ManualAgricultural
69.1+29.1 29.1± 4.2 82.8+ 9.6
77.1+25.8 32.8± 9.4 86.5±17.9
60.8±22.8 20.9± 8.6 77.7±15.3
51.8+19.3
40.4+14.2
56.6+ 6.9
are being presented fromtime.
15.1±13.816.9± 4.9
22.4± 5.7
52.1+16.0
49.0±14.359.6±24.3
India for the first
A recent development in India has beenthe field studies of general population such asthe one reported here. The only other parallelstudy is being conducted by Padmavati etal.17 at Delhi. She reported an incidence of 4per cent in the high-socioeconomic group incontrast to 0.5 per cent in the rural popula-tion of Nazafgarh, and 0.17 per cent in theindustrial workers. The corresponding inci-dence in the high-socioeconomic group in thepresent series was 4.1 per cent in the surveyof the general population.
It seems clear from the studies on patientsand the general population that coronaryheart disease has a predilection for the privi-leged class of society in great contradistinc-tion to individuals of low-socioeconomicgroup, who enjoy relative immunity from thisdisease. How these socioeconomic factors op-erate has been a baffling question in the highlycomplicated problem of coronary heart dis-ease.The answer to the relationship of diet to
coronary heart disease has been sought inepidemiologic surveys, clinical studies, andmetabolic ward experiments. The highest in-cidence of coronary heart disease has beenobserved in members of the high-socioeconomicgroup, who consume the highest amount of
687
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
MATHUR
Table 4Mean Lipid Values in Cases of Coronary HeartDisease and Normal Controls
CoronarySerum lipids heart disease Normal
Total serum
cholesterol (mg. %)
Serum lipidphosphorus (mg. %)
C/P ratio
218±52.4(114-350)9.46+1.92
(5.3-14)24.1±3.21(19.8-29.4)
182.6±38.2(96-275)
8.44±2.49(5-11)
21.7± 2.18(17-27.2)
dietary fat, the highest percentage of fat cal-ories and saturated fat. But on subgrouping-of each socioeconomic group on the basis ofdietary fat intake, it was observed that the
serum lipid level did not show a correspond-ing rise with the rise in dietary fat consump-
tion.13
Although the total quantity of fat, percent-
age of calories contributed by fat, andpercentage of saturated fat may have an im-portant relationship with coronary heartdisease, other factors like total caloric intake,relative rate of calorie expenditure, physicalactivity, emotional status, and hormonal in-fluences cannot be easily isolated from theproblem of excessive fat intake. Consequelntlythe epidemiologic studies do not give a coni-
vincing answer to the relationship of dietaryfat-and coronary heart disease.
In India the dietary habits of people havenot changed significantly during the lastdeeade or two, but with the advance of mod-ernization, industrialization, and urbaniza-tion, physical labor has been curtailed con-
siderably, and people are exposed to greaterstress and strain. These may be importalntfactors in the increasing inicidence of coronary
heart disease.Summary
Various factors relating to coronary heartdisease were investigated in 2 groups of pa-
tients: 553 patients with clinical coronary
heart disease and 1,056 persons selected in a
field survey of the general population.The incidence of coronary disease was high
in the urban population, in the upper socio-economic classes, and in persons with highest
amounts of total dietary fat and highest per-centage of calories from dietary fat. Totalserum cholesterol, serum phospholipid, andcholesterol/phospholipid ratio were hiaher inthe coronary group.
Finally, it seemed that physical activitywas less and emotional stress and straingreater in the patienlts with coronary disease.No relation between coronary disease and
smoking or alcohol was established.
Summario in InterlinguaVarie factores relationate a morbo cardiac coronari
esseva investigate in 2 gruppos de patientes.Le prime consisteva de 553 patientes con clinicamentemanifeste morbo cardiac coronari, le secunde con-sisteva de 1.056 subjectos seligite in un investigationprofilatori del population general.Le incidentia de morbo coronari esseva alte in le
population urban, in le classes socio-economicamentesuperior, e in gruppos de subjectos con le plus altetotales de grassia dietari e le plus alte procentagesde calorias ab grassia deitari. Le valores pro choles-terol total del sero, pro phospholipido seral, e pro leproportion de cholesterol a phospholipido esseva plusalte in le gruppo coronari.
Finalmente, ii pareva que le activate physic esseva
inferior e que le stress emotional esseva superior in le
patientes con morbo coronari.Nulle relation esseva constatate inter morbo coro-
nari e le uso de taboco e de alcohol.
References1. WHITE, P. D., AND JONES, T.: Heart disease
and disorders in New England. Am. Heart J.
3: 302, 1928.2. WHITE, P. D.: Heart Disease. Ed. 4. New York,
The Macmillan Company, 1951.3. MATHUR, K. S.: Coronary artery occlusion.
Indian J. MI. Sc. 13: 7, 1959.
4. SANJIVI, K. S.: Heart Disease in South India.
Proceedings of the Annual Conference of As-
sociation of Physicians of India, 1946.5. VAKIL, R. J.: An aetiological study of heart
disease in Bombay. Indian J. M. Sc. 2: 465,1948.
6. SAMrANI, 0. T.: Coronary heart disease in lowincome population in India. Indian Heart J.8: 104, 1956.
7. PADMAVATI, S.: A five year survey of heartdisease in Delhi. Indian Heart J. 10: 33,1958.
8. VAKIL, R. J.: Statistical observations on cases
of coronary thrombosis. The Indian Physi-cian 2: 331, 1952.
Circulation, Volume XXI, Mao 1960
688
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
ENVIRONMENT AND CORONARY DISEASE
9. MALHOTRA, R. P., AND PATHANIA, N. S.: Someaetiological aspects of coronary heart disease.Brit. M. J. 2: 528, 1958.
10. GORDON, T.: Mortality experience among theJapanese in the United States, Hawaii andJapan. Pub. Health Rep. 72: 543, 1957.
11. MATHUR, K. S.: The problem of heart disease inIndia. Am. J. Cardiology. In press.
12. -, AND WAHI, P. N.: Study of Environmentaland nutritional factors affecting the incidenceof atherosclerosis and coronary heart disease.Annual Report of I.C.M.R., 1958.
13. , -, MALHOTRA, K. K., SHARMA, R. D., ANDSRIVASTAVA, S. K.: Dietary fats, serum choles-terol and serum lipid phosphorus in differentsocio-economic groups in Utter Pradesh (In-
dia). J. In dian M. A. In press.14. MATHUR, K. S., WAHI, P. N., AND MALHOTRA,
K. K.: Effect of Indian dietary fat on bloodcoagulability anid serum lipids in normals andin cases of myocardial infaretion. IndianJ. M. Research. In press.
15. -, MALHOTRA, K. K., AND SIIARMA, R. D.: Serumlipids in coronary heart disease. Indian HeartJ. 12: 28, 1960.
16. WIG, K. L., AND MALHOTRA, R. P.: Coronaryartery disease in the young. Indian Heart J.3: 231, 1951.
17. PADMAVATI, S., GUPTA, S., AND PANTULU, G. V.A.: Dietary fat, serum cholesterol levels andincidence of atherosclerosis and hypertensionin Delhi. Indian J. M. Research 46: 245, 1958.
An Awareness of the History of MedicineA physician is inevitably wrapped in the fabric of the history of medicine, for in his
daily undertakings he comes face to face with the experience of his predecessors whoeffectively pursued the art and the science of both practice and research. The observationaland constructive methods that he uses in creating a case through careful history takingmay bring to his mind, if he is well oriented, the contributions of Plato, Aristotle, Hip-pocrates, Galen, Maimonides, Vesalius, Harvey, Leeuwenhoek, Boyle, Pasteur, Virchow,Sydenham and many others.
It is a way of building a bridge between the practice of medicine and the humanity ofscience. There are distinguished physicians today who, though preoccupied with immedi-ately practical or scientific problems, reap a sense of deep personal satisfaction in follow-ing the long course of medical history back through the Renaissance and the Mtiddle Agesto Greco-Roman periods of thought and action. . . . The exercise of the intellect in thismanner will focus his attention on the deductive and inductive methods, the dogmas, thetenuous speculations, the working hypotheses and the experiments themselves that led tothe growth or the retardation of medical history.
Paul, the apostle, in his first epistle to the Thessalonians uttered the well known thought,"Prove all things; hold fast that which is good." This counsel is particularly applicableto those who tend to worship the present and to scorn the past. The present may indeedrepresent the high, immediate mountain view of medicine, but for all that the valleys ofthe past and the smaller mountain ranges that confine them are willy-nilly part of thepresent. A nmere awareness of Greek, Hebraic, Arabic and Christian traditions as theyrelate to the present will give a physician a sense of pride in his calling and a feeling ofbeing nearly complete in his total capabilities as he concerns himself with ethics, scientificeducation or patient-physician relations.-Editorial. New England Journal of Medicine257: 290, 1957. (Reprinted with permission of the Publishers.)
Circulation, Volume XXI, May 1960
689
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from
KRISHNA S. MATHURAgra (India)
Environmental Factors in Coronary Heart Disease: An Epidemiologic Study at
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1960 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.21.5.684
1960;21:684-689Circulation.
http://circ.ahajournals.org/content/21/5/684located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 15, 2018http://circ.ahajournals.org/
Dow
nloaded from