Embed Size (px)
Citation preview

Virology 411 (2011) 288–305
Contents lists available at ScienceDirect
Virology
j ourna l homepage: www.e lsev ie r.com/ locate /yv i ro
Review
Enterovirus infections of the central nervous system
Ross E. Rhoades, Jenna M. Tabor-Godwin, Ginger Tsueng, Ralph Feuer ⁎Cell & Molecular Biology Joint Doctoral Program, Department of Biology, San Diego State University, San Diego, CA, 92182-4614, USA
⁎ Corresponding author. Cell & Molecular Biology JoinUSA. Fax: +1 619 594 0777.
E-mail address: [email protected] (R. Feuer)
0042-6822/$ – see front matter © 2011 Elsevier Inc. Aldoi:10.1016/j.virol.2010.12.014
a b s t r a c t
a r t i c l e i n f oArticle history:Received 7 December 2010Accepted 8 December 2010Available online 20 January 2011
Keywords:EnterovirusesCNS
Enteroviruses (EV) frequently infect the central nervous system (CNS) and induce neurological diseases.Although the CNS is composed of many different cell types, the spectrum of tropism for each EV isconsiderable. These viruses have the ability to completely shut down host translational machinery and areconsidered highly cytolytic, thereby causing cytopathic effects. Hence, CNS dysfunction following EV infectionof neuronal or glial cells might be expected. Perhaps unexpectedly given their cytolytic nature, EVs mayestablish a persistent infection within the CNS, and the lasting effects on the host might be significant withunanticipated consequences. This review will describe the clinical aspects of EV-mediated disease,mechanisms of disease, determinants of tropism, immune activation within the CNS, and potential treatmentregimes.
© 2011 Elsevier Inc. All rights reserved.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Polioviruses (PVs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Coxsackieviruses (CVs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Enterovirus-71 (EV-71) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Echoviruses (ECHO-Vs) and parechoviruses (P-ECHO-Vs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Theiler's murine encephalomyelitis virus (TMEV) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 289Molecular biology of enteroviruses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290Enteroviruses and autophagy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290Host cell translational shutdown following enterovirus infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 290Virus entry — cell receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291Coxsackievirus infection of neural progenitor and stem cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291Enterovirus dissemination — hitch-hiking on migratory immune cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 291Routes of enterovirus entry into the CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292Enterovirus quasispecies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293Enterovirus tropism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294IRES trans-acting factors (ITAFs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294Immune responses to enteroviruses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294Innate immune response following enterovirus infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295Adaptive immune response following enterovirus infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295Enterovirus persistence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296Pathophysiology of enterovirus infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296Clinical diagnosis of enterovirus infection of the CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297Contributions of apoptosis to enterovirus disease in the CNS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297Potential behavior and memory dysfunction following enterovirus infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297Antiviral drugs to treat enterovirus infections — RNAi based approaches . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 298Antiviral drugs to treat enterovirus infections — ribavirin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 298Antiviral drugs to treat enterovirus infections — pleconaril . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Intra-venous immunoglobulins to treat enterovirus infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299
t Doctoral Program, Department of Biology, San Diego State University, 5500 Campanile Drive; San Diego, CA 92182-4614,
.
l rights reserved.

289R.E. Rhoades et al. / Virology 411 (2011) 288–305
Vaccines against enteroviruses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Poliovirus vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 299Enterovirus-71 vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300Coxsackievirus vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 300Gene delivery in the CNS utilizing enterovirus-based vectors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301Conclusions and future perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 301
Introduction
Enterovirus (EV) infections are a significant cause of morbidity andmortality throughout the world. The EV genus is part of thepicornavirus family and includes such notable members as poliovirus(PV), coxsackievirus (CV), and enterovirus-71 (EV-71). EVs have beenassociated with many human diseases, including myocarditis (Klingelet al., 1992), pancreatitis (Ramsingh, 2008), and chronic inflammatorymyopathy (Tam and Messner, 1999). Diseases caused by EV are notrestricted to the well-known scourge of mankind throughout history,recognized as poliomyelitis. Many non-polio human EVs are quitecommon, causing an estimated 10–15 million or more symptomaticinfections in the US alone. Non-polio EVs are known to target thecentral nervous system (CNS) and are responsible for numerousclinical manifestations, including encephalitis, and meningitis(Michos et al., 2007). The long-term consequences of EV infectionupon the CNS are largely unknown. However, these viruses are knownto persist, and the presence of viral RNA by itself has been shown to bepotentially pathogenic in some cases. Also, EVs have been linked toautoimmune-like diseases, including diabetes, chronic inflammatorymyopathy, and chronic myocarditis, perhaps in part due to the long-term presence of viral material. Therefore, EVs may be able to persistwithin the CNS potentially causing lasting neuropathology.
The original classification of enteroviruses included the fourgroups: Polioviruses (PVs), Coxsackie A viruses, Coxsackie B viruses,and ECHO (Enteric Cytopathic Human Orphan) viruses. However, thesignificant level of phylogenetic overlap among the four groups hasled to a new classification system of consecutive numbers for themore recently isolated viruses (such as Enterovirus-71, Enterovirus-72, etc.) (Oberste et al., 2002). Our review will cover the mostcommon and more extensively studied types of enteroviruses.However, the large number of circulating strains in human popula-tions alone suggests a potential role for these viruses for unknown orunappreciated human diseases (Victoria et al., 2009). Also, vaccinedesign against enteroviruses may be difficult based on significant EVgenetic variability.
Polioviruses (PVs)
Polioviruses (PVs) are perhaps the most studied and character-ized of the enteroviruses, especially given the clinical consequencesof infection which can infect motor neurons of the anterior horn ofthe spinal cord and lead to paralytic poliomyelitis in humans.Although the advent of polio vaccination has proven effective ingreatly reducing the incidence of disease, some cases still occur andthese cases appear to be on the rise; outbreaks following wild PVimportations into previously polio-free countries continue to be anongoing risk (MMWR, 2010). Over the years, basic research on PV hasrevealed the mechanics of protein translation and viral replication,immune activation, vaccine development, and viral populationdynamics (Cameron et al., 2010; Pfeiffer, 2010). These discoverieshave provided valuable information for the ongoing research of non-polio enteroviruses which continue to cause encephalitis and meningitisin humans.
Coxsackieviruses (CVs)
Coxsackieviruses (CVs) may cause severe morbidity and mortality,particularly in the very young (Romero, 2008; Tebruegge and Curtis,2009). CV infection during pregnancy has been linked to an increasein spontaneous abortions, fetal myocarditis (Ornoy and Tenenbaum,2006), and neurodevelopmental delays in the newborn (Euscher et al.,2001). Infants infected with CV have been shown to be extremelysusceptible to myocarditis, meningitis and encephalitis with asubsequent mortality rate as high as 10%. Also, a number of delayedneuropathologies have been associated with previous CV infection,including schizophrenia (Rantakallio et al., 1997; Suvisaari et al.,2003), encephalitis lethargica (Cree et al., 2003), and amyotrophiclateral sclerosis (Woodall and Graham, 2004; Woodall et al., 1994). Ofnote, few studies have been done to determine the lastingconsequences of CV infection upon surviving individuals despite therelatively common occurrence of CV meningo-encephalitis in infants.
Enterovirus-71 (EV-71)
Enterovirus-71 (EV-71) is amajor public health issue acrossAsia andof increasing concern globally, causing hand foot and mouth diseasewith potential neurological complications (Solomon et al., 2010). Thebrain stem is themost likely target for infection, and infectionmay causeserious clinical disease and psychological disorders in young children(Lee et al., 2009). New outbreaks of EV-71 have occurred across Asia,perhaps due to the ability of the virus to rapidly evolve (Solomon et al.,2010).
Echoviruses (ECHO-Vs) and parechoviruses (P-ECHO-Vs)
Echoviruses (ECHO-Vs) were first isolated from the feces ofasymptomatic patients; however, these viruses are now recognizedto be associated with various human diseases, including asepticmeningitis. ECHO-Vs are highly infectious and preferentially targetinfants and young children. These viruses can cause amild, nonspecificillness similar to that of CVs. Also, parechoviruses (P-ECHO-Vs) havebeen found to be associated with encephalitis and white matter injuryin neonates (Gupta et al., 2010; Verboon-Maciolek et al., 2008a), withsimilarities to EV infections (Verboon-Maciolek et al., 2008b).Although originally described as ECHO-V-22 and ECHO-V-23, theirdistinct genetic features have led to their re-classification (Harvala andSimmonds, 2009).
Theiler's murine encephalomyelitis virus (TMEV)
Although the picornavirus, Theiler's murine encephalomyelitisvirus (TMEV), is designated a cardiovirus by phylogenetic analyses,much can be learned from the existing literature on TMEV and CNSdisease. Also, many similarities exist between EVs and TMEV in termsof their molecular biology, tropism, ability to persist, and induction ofneuropathology. Therefore, we have included relevant information onTMEV and CNS pathology in this review. Two main subtypes of TMEVare studied in animal models. The strain GDVII produces acuteencephalomyelitis quickly in mice. The DA, WW, or BeAn strains

290 R.E. Rhoades et al. / Virology 411 (2011) 288–305
persist within the CNS and induce demyelinating plaques similar tothose seen in multiple sclerosis. More detailed reviews of TMEVtropism, immune response, persistence, and demyelination have beenpublished by other research groups (Brahic et al., 2005; Lipton et al.,2005; Oleszak et al., 2004; Olson et al., 2005; Rodriguez, 2007).
Molecular biology of enteroviruses
To better understand EV infection of the CNS and potentialconsequences upon glial or neuronal host cells, a full comprehensionof EV structure and molecular biology is essential. EVs consist oficosahedral, non-enveloped viruses of approximately 30 nm indiameter. These viruses generally have the proclivity to survive acidicenvironment, enabling their passage through the stomach followingfecal/oral transmission and eventual invasion into the small intestine.The viral capsid contains the positive-strand RNA genome, ranging insize from ~7.2 to 8.5 kb. The viral genome includes several cis-actingRNA elements which play a role in replication and/or translation.These cis-acting elements include the 5′ and 3′ nontranslated regions(NTRs), the cis-acting replication element (CRE) and the 3′ poly(A)tail (Steil and Barton, 2009).
A single open reading frame (ORF) within the NTRs encodes a longviral protein which undergoes post-translational cleavage into themature viral proteins. These viral proteins include the four structuralproteins, VP1–4 which comprise the viral capsid, and seven non-structural proteins (2A–C and 3A–D) including the primer- and RNA-dependent RNA polymerase (3DPol) (Kitamura et al., 1981). Inaddition, one of the viral proteins 3B (also known as VPg) covalentlyattaches to the 5′ end of the viral genome. VPg plays an essential rolein viral replication by acting as a primer for RNA synthesis. UtilizingPV as a model, VPg has been shown to undergo uridylylation toVPgpUpU by 3DPol using adenosine residues in the stem-loopstructure of CRE, located in the 2C region of the EV ORF, as a template(Goodfellow et al., 2000; Paul et al., 2003). Recent elucidation by NMRsuggests that VPg undergoes a structural change upon uridylylationwhich allows viral replication to be more efficient and selective(Schein et al., 2010). Since uridylylation is not observed during hostcell transcription, this process may be a unique therapeutic targetagainst EV infections, given that point mutations that blockuridylylation may prevent viral growth (Paul et al., 1998). WhileVPg plays a role in both positive- and negative-strand RNA synthesis,it is still unknown how approximately 40 to 70 copies of positive-strand genome are produced for every negative-strand genomeduring an EV infection (Novak and Kirkegaard, 1991). Intriguingly,this ratio decreases upon the establishment of CVB3 persistencewithin the CNS suggesting that a double-stranded RNA genomicstructuremight assist in virus stability during persistence (Feuer et al.,2009).
Despite the unanswered questions with regards to the ratio of EVpositive to negative strand synthesis during both acute and persistentinfection, many other aspects of their translation and replication arewell understood. For example, the well-characterized internal ribo-some entry site (IRES) in the 5′ NTR directly interacts with host cellribosomes to initiate translation of the viral genome upon enteringthe cell (Pelletier and Sonenberg, 1988). Immediate translation isnecessary in order to produce the primer- and RNA-dependent RNApolymerase needed for viral replication, as well as the other viralproteins that facilitate replication. The viral genome is translated intoa ~250-kDa polyprotein, which undergoes a series of cleavages atpredetermined cleavage sites carried out by the viral proteases 2Apro
and 3CDpro. During proteolytic processing, several precursor proteinintermediates also play important roles during viral infection.
Only after viral protein translation is completed does negative-strand replication begin since translation and replication cannot occurat the same time (Gamarnik and Andino, 1998). A ternary complexthen forms to facilitate both positive- and negative-strand synthesis at
the 5′ cloverleaf structure of the 5′NTR that includes the host poly(rC)binding protein (PCBP) and the viral precursor protein 3CD (Vogt andAndino, 2010). This complex associates with poly(A) binding protein1 (PABP1), which is bound to the poly(A) tail of the genome, andcauses the genome to circularize during negative-strand synthesis(Herold and Andino, 2001). Further analysis of the crystal structure of3CD has shown that the N-terminus is in close proximity to the VPgbinding site, and that 3CD may be involved in the uridylylationreaction as part of the replication complex (Marcotte et al., 2007).Moreover, 3AB (also the VPg precursor protein) is a membrane boundprotein (Fujita et al., 2007), thus providing a spatial link between viralreplication on host membranes, viral priming and the replicationcomplex.
Enteroviruses and autophagy
Interestingly, EVs have been shown to benefit from, and induce thecellular degradation process known as autophagy (Huang et al., 2009;Suhy et al., 2000; Wong et al., 2008). It is thought that EVs use theautophagosome membrane as a scaffold for viral replication. A recentpublication has shown an increase in viral replication linked to theinduction of autophagy during CV infection in rat primary neurons(Yoon et al., 2008). Autophagy is known to play an important role inpreventing cellular damage in neurons, and this normal cellularprocess has recently been shown to be highly upregulated in neuronsduring short-term fasting (Alirezaei et al., 2010; Simonsen et al.,2008).
However, it still remains to be determined if EVs use autophagy forviral replication in all cell types within the CNS. For example, giventheir unique and critical role in development and CNS cellularhomeostasis, neural stem cells might respond differently anduniquely to microbial infection. Furthermore, it will be important toelucidate whether autophagy plays a role in the establishment of viralpersistence in the CNS. The induction or inhibition of autophagy incells harboring viral material may alter EV persistence. Autophagyinhibitors have been shown to preferentially decrease extracellular ascompared to intracellular PV production, thus providing an attractivemodel for non-cytolytic virus release from the cell (Jackson et al.,2005). Also, one might expect that an increase in the level ofautophagy which might recycle organelles or other cellular compo-nents associated with EV persistence may hasten viral RNAdegradation.
Host cell translational shutdown following enterovirus infection
In addition to their roles in viral replication and post-translationalprocessing, several viral proteins have profound effects on the hostcell during the course of infection effectively modulating cellulartranscription, translation and protein secretion. Host cell transcriptionis suppressed by the viral protease 3C, which is carried into thenucleus by the nuclear localization signal located on 3D when in itsprecursor form (Sharma et al., 2004). Additionally, the 3C protein ofEV-71 has recently been shown to block polyadenylation of hostmRNA by cleaving a critical factor needed for this process (Weng et al.,2009). In turn, viral protease 2A halts host cell cap-dependenttranslation by cleaving eIF4G, which in a clever twist also enhancesthe translation of viral mRNA by stabilizing polysomes (Etchison et al.,1982; Kempf and Barton, 2008). Furthermore, viral proteins 2B and 3Ainhibit host cell protein secretion, as plasma membrane and secretoryprotein transport are halted (Doedens and Kirkegaard, 1995).
In general, the host cell most likely faces a grim ultimate fate duethe cytolytic nature of EVs. Viral protein 2B is a highly efficientviroporin which can permeabilize the host cell membrane, as well asthose of nearby cells (Madan et al., 2010). However, the pathwaysactivated in the cell during infection can be somewhat contradictory.In what is thought to be an attempt by the virus to keep the cell alive

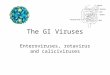
Fig. 1. Neural progenitor and stem cells grown in culture are highly susceptible tocoxsackievirus infection. NPSCs were isolated from the cortices of one day-old C57 BL/6mice, cultured to form neurosphere aggregates, and infected with eGFP-CVB3(moi=0.1). Infected neurospheres were observed over time by fluorescencemicroscopy. Virus protein expression (green) was readily observed by day 1 PI. Anincrease in viral protein expression was seen until day 4 PI. By day 6 PI, virus proteinlevels were reduced, and signs of cytopathic effect (cpe) were readily observed at ahigher magnification (not shown).
291R.E. Rhoades et al. / Virology 411 (2011) 288–305
long enough to complete viral replication and eventually escape itscellular confinements, EVs induce both anti-apoptotic (3A and 2Bproteins) and pro-apoptotic effects (VP2, 2A and 3C proteins) on thehost cell (Whitton et al., 2005). Furthermore, viral protein synthesis,which is boosted by 2A, has been shown to be necessary for apoptosis(Shih et al., 2008). With several reports demonstrating apoptosis inneurons after EV infection, and the role of 2A in regulating translation,it is interesting to speculate that shutoff of host cell translation by EVsmay directly cause apoptotic cell death in neurons. We have shownthat CVB3 induced apoptosis within pyramidal neurons in thehippocampus (Feuer et al., 2003). In contrast, TMEV may indirectlyinduce apoptosis of nearby pyramidal neurons in the hippocampus innon-cell autonomous manner (Buenz et al., 2009).
Virus entry — cell receptors
EVs use a wide array of receptors and entry mechanisms to invadethe host cell. In particular, EV-71 has been shown to use severalreceptors, including sialylated glycans, P-selectin glycoprotein ligand-1and Scavenger receptor B2 (Nishimura et al., 2009; Yamayoshi et al.,2009; Yang et al., 2009). CVB can utilize both decay accelerating factor(DAF) and the coxsackievirus and adenovirus receptor (CAR) for viralentry, depending on the target cell. For example in polarized cells, CVBelicits a unique strategy by binding to DAF at the apical surface of thecell, followed by CAR binding within the tight junctions in a caveolin-dependent, dynamin-independent manner (Coyne and Bergelson,2006). Whereas in non-polarized cells, CVB only appears to utilizeCAR for entry and undergoes dynamin-dependent and caveolin-independent entry (Patel et al., 2009).
While some EVs are capable of utilizingmultiple receptors, PV usesonly one, CD155, an adhesion molecule also known as the human PVreceptor (hPVR). In an in vitro blood-brain barrier (BBB)model, PV hasbeen show to enter human brain microvascular endothelial cells(hBMECs) using hPVR in a dynamin and caveolin-dependent manner(Coyne et al., 2007). However, when using non-CNS specificimmortalized cells lines, PV entry was found to be caveolin-independent. Both reports found tyrosine kinases to be essential forentry (Brandenburg et al., 2007). These studies illustrate theimportance of characterizing EV entry in multiple CNS cell types,since key differences may exist in different model systems ofinfection. Similarly, care must be taken in making generalizedconclusions of virus entry based on in vitro cell culture models.
Undoubtedly, receptor expression on potential target cells definesthe first barrier to virus entry. A recent study has shown a linkbetween decreased CAR expression in differentiated primary neuronsand a reduction in CVB3 infection, suggesting that susceptibility toinfection may diminish as the level of virus receptor decreases duringthe differentiation process (Ahn et al., 2008). Similarly, PV infectionand tissue tropism was largely found to be restricted by hPVRexpression in the CNS of hPVR promoter-driven beta-galactosidasetransgenic mice (Gromeier et al., 1995). Analysis of receptordistribution in hPVR promoter-driven beta-galactosidase transgenicmice during development showed high levels of protein expression inthe spinal cord anterior horn motor neurons which are known toharbor infection in the mature CNS (Gromeier et al., 2000). Althoughsome EV receptors may be widely expressed in tissues including theCNS, additional cellular determinants may ultimately control tropism.For example, CAR expression is relatively widespread in the murineneonatal CNS (Honda et al., 2000; Hotta et al., 2003; Venkatramanet al., 2005) and utilized by adenovirus— a DNA virus with substantialtropism differences as compared to CVB3. Yet, early CVB3 infection islargely restricted to neural progenitor and stem cells (NPSCs) (Fig. 1)or infiltrating myeloid cells during early infection (Feuer et al., 2005)(Fig. 2). The proliferative status of these cells may provide anadditional level of susceptibility to infection (Feuer et al., 2002,2003, 2005; Feuer and Whitton, 2008).
Coxsackievirus infection of neural progenitor and stem cells
What might be the benefit of CVB3 targeting NPSCs for infection?We expect that the benefits may be many fold in terms of viralreplication, persistence, dissemination, and transmission. First, NPSCsactively proliferate not only during neonatal development, but alsooccasionally within the adult host. Infection of NPSCs may assist inexpanding the tropism of CVB3 upon their differentiation into thethree neural lineages — neurons, astrocytes, and oligodendrocytes.Previously, we determined that CVB3 preferentially replicates withinactively proliferating cells (Feuer et al., 2002). Hence, NPSCs may beconsidered ideal host cells for infection.
Second, NPSCs migrate upon their differentiation into particularregions within the CNS, including the hippocampus and the olfactorybulb. The olfactory bulb might be considered an escape route for thevirusupon anterograde transport across the olfactoryneuroepithelium.Third, NPSCs might be altered upon their differentiation into neurons.Alterations in neuronal function may lead to behavioral modificationswithin the host, whichmay act tomaximize virus transmission. Fourth,targeting of NPSCs might be a strategy of CVB3 to establish persistentinfection with sporadic reactivation whenever quiescent stem cellsbecomeactivated to generate downstreamprogenitor cells (Fig. 3). Themajority of primary neural stem cells at any moment in time might beexpected to remain within a quiescent state. Therefore, CVB3replication may be temporarily arrested in the host cell until a laterpoint in time when the production of virions may be of benefit to viraltransmission, perhaps through the olfactory neuroepithelium. Finally,normal immune responses may be suppressed within neurogenicregions, either due to the immunoprivileged status of the CNS, orpotentially reduced antiviral responses in these crucial neural stemcells.
Enterovirus dissemination — hitch-hiking on migratoryimmune cells
Perhaps surprisingly, polarized epithelial cells are not consideredprimary target cells for CVB3 infection in vivo, despite their expression

Fig. 2. Induction of CCL12 and the progressive extravasation of infectedmyeloid cells through the basement membrane as determined by confocal microscopy and Imaris 3D analysis.One day-old C57 BL/6 mice were intra-cranially infected with a recombinant coxsackievirus B3 expressing eGFP (eGFP-CVB3; 10E7 pfu). The brains were harvested 12 h later andinspected by confocal fluorescence microscopy. Myeloid cells responding to CVB3 infection were observed entering through the tight junctions of the choroid plexus epithelium. Asthese myeloid cells entered the lateral ventricle, they expressed high levels of viral protein (green). Also, the chemokine CCL12 (red), a potential chemoattractant molecule forinfiltrating myeloid cells, was expressed within the choroid plexus and surrounding subventricular zone. The kinetics of myeloid cell migration through the basement membrane(outlined by laminin staining in red) was observed by confocal microscopy and IMARIS 3D analysis. Immunofluorescence images showed infected myeloid cell migration (green)through the tight junctions of the choroid plexus epithelium. Gray scale images of all three colors (virus-green; laminin-red, DAPI-blue) at 12 h PI revealed the intensity andorganization of the myeloid cell infiltration in greater detail. In order to better visualize myeloid cell entry, IMARIS 3D with diminishing laminin label (diminishing red) was carriedout, and the methodology revealed the extravasation of infected myeloid cells through the basement membrane (white arrow). Original images were obtained with a 63× Plan-Aprochromat objective at 0.3 μm interval step slices.
292 R.E. Rhoades et al. / Virology 411 (2011) 288–305
of intrajunctional proteins. Rather, the major targets of infection havebeen found to include the acinar cells of the pancreas, cardiomyocytes,activated lymphocytes within the marginal regions of the spleen,infiltrating nestin+myeloid cells, proliferating NPSCs, and immatureneurons of the CNS. Instead, targeting of intrajunctional proteins suchas CAR by CVB3 might be a sophisticated viral strategy to specificallyinfect migratory immune cells as they undergo diapedesis through thetight junctions. In this regard, we have recently shown the ability ofCVB3 to infect nestin+myeloid cells upon their infiltration across thetight junctions of the choroid plexus epithelial cells comprising theblood-cerebral spinal fluid-barrier in response to early CNS infection(Tabor-Godwin et al., 2010). These infected myeloid cells eventuallymigrate into the parenchyma of the brain, thereby assisting in virusdissemination.
The benefits to virus dissemination by targeting intrajunctionalproteins may be many fold; first, virions temporarily attached tosequestered intrajunctional proteins might find themselves in aperfect location to “hitch-hike” onto a migratory immune cell as thesecells enter sites of inflammation or injury in response to earlyinfection. Second, immune cells responding to inflammation or injurytend to be highly activated or undergoing proliferation, and each virusmay induce unique chemokine profiles early after infection to attracttheir immune cells of choice. CVB3 has been shown previously topreferentially replicate within activated or proliferating cells. Third,virions carried internally by immune cells might temporarily shieldthe virus from neutralizing antibodies upon dissemination. Neutral-izing antibodies are thought to play a major role in limiting EV
infections, and hypogamma-globulinemic patients deficient in hu-moral immunity are highly susceptible to EV infection. Perhaps notsurprisingly, other viruses have been shown to bind to intrajunctionalproteins (Bergelson, 2009), suggesting that the proposed mechanismabove might be a general feature of virus dissemination within thehost. Therefore, rather than being a hindrance to virus entry — whichmight be expected for receptors sequestered within highly inacces-sible areas— virus evolutionmay have optimized virion attachment tointrajunctional proteins to maximize viral spread using immunetarget cell “Trojan horses” which become infected during theirmigration across tight junctions. Supporting this hypothesis, evidencefor viral targeting of lymphocytes or monocytes for spread intoprimary target organs and maximal viral replication has beendescribed for CVB3 (Mena et al., 1999) and other viruses (Nodaet al., 2006).
Routes of enterovirus entry into the CNS
Since EVs, such as PV, are transmitted via the fecal–oral route ofinfection, a detailed understanding of how the virus travels from thegut to the brain is essential in designing strategies to limit EV disease.Despite the extensive research that has been performed to understandCNS invasion, many questions remain. Multiple pathways mayactually work in combination to complete this phenomenon. Thetwomainmodels of PV entry into the CNS both involve viremia, or thepresence of virus in the blood, after the virus has replicated in thelymphatic tissues of the gastrointestinal tract. One hypothesis simply

Fig. 3. Potential reactivation of a persistent coxsackievirus infection within quiescentneural stem cell. Coxsackieviral RNA (squiggly green lines) may persist in a latent statewithin quiescent type B neural stem cells in the CNS. Following cellular divisionreactivation of viral RNA may lead to viral protein expression and sporadic infectiousvirus production. The production of infectious virions may infect nearby progenitorcells. Alternatively, asymmetric division of infected type B stem cells may generatedownstream progenitor cells or immature neurons that remained infected and migrateto other regions of the CNS. The outcome over the long-term of continuous virusreactivation may be virus-mediated neuropathology and virus dissemination.
293R.E. Rhoades et al. / Virology 411 (2011) 288–305
proposes the direct movement of the virus through the blood-brain-barrier (BBB) in an hPVR-independent manner (Yang et al., 1997).Perhaps direct entry across the BBB via early PV infection of hBMECsmay occur first, thus weakening or exposing the BBB and allowing forsecondary virus entry into the CNS regardless of receptor expression.
A secondmodel of EV entry proposes PV spread frommuscle to theCNS along neural pathways (Ren and Racaniello, 1992). These neuralpathways were more clearly defined by Gromeier and Wimmer in1998 as retrograde axonal transport of the virus from damaged
muscle to the CNS (Gromeier and Wimmer, 1998). Since muscleinjury has been shown to induce neurological PV infection, the modelis typically referred to as “provocation poliomyelitis”. Initially, it wasproposed that hPVR was necessary for retrograde axonal transport ofthe virus along microtubules (Ohka et al., 2004). However morerecently, retrograde transport has been shown to occur independentlyof the hPVR (Ohka et al., 2009).
Another emerging model of CNS entry involves the use of EV-infected immune cells invading the CNS in a “Trojan horse” fashion, asdescribed above. Of note, PV has been shown to infect monocytes,macrophages and dendritic cells in an hPVR-dependent manner(Freistadt et al., 1993; Wahid et al., 2005). In addition, lymphocytesmay play a role in monocyte infection by inducing their activation andfacilitating viral replication (Eberle et al., 1995). Further investigationhas revealed a possible link between PV pathogenesis in the CNS andmonocyte infection, as neurovirulent strains were found to replicatemore efficiently in monocytes (Freistadt and Eberle, 1996). Asdescribed above, CVB3 and also EV-71 have been shown to replicatein immune cells, B-lymphocytes, T-lymphocytes and cells of themyeloid lineage (Haddad et al., 2004; Vuorinen et al., 1996). Ourlaboratory has recently revealed the rapid infiltration of a novelpopulation of nestin+myeloid cells into the neonatal CNS followingCVB3 infection (Tabor-Godwin et al., 2010). These cells are highlysusceptible to CVB3 infection and move into the brain parenchymaover time, suggesting a role in viral dissemination. The growingnumber of studies demonstrating EV infection of immune cellssuggests that further investigation of the “Trojan horse” model ofCNS invasion may be warranted.
Enterovirus quasispecies
Another essential factor in CNS invasion may be the involvementof EV quasispecies, or genotypic variants of virus populations, due tomutational errors accumulated during viral replication. These errorsresult from the low fidelity of the RNA-dependent RNA polymerasewhereby at least one incorrect nucleotide is incorporated per genomeduplication (Ward and Flanegan, 1992; Ward et al., 1988). Othercontributing factors during viral replication may also increase viraldiversity. For example, a recent in vitro study performedwith PV 3DPol
found that the replication fidelity may be relatively high; yet otherevents during replication, such as template switching, may actuallycontribute to the errors found in the genome (Freistadt et al., 2007).
Regardless of the nature of mutation rate, the existence of a swarmof viral variants, or a quasispecies cloud, has been shown to contributeto EV spread to the CNS. Recent elegant work utilizing a PV variantencoding a mutation in 3DPol isolated during serial passage in thepresence of ribavirin has revealed the critical nature of viralquasispecies in contributing to invasion of the CNS. The PV isolate(G64S) was shown to increase the fidelity of the viral polymerase anddecrease quasispecies diversity (Vignuzzi et al., 2006). The G64S PVisolate was less neurovirulent than wild type virus, and CNS invasionfailed to occur unless the isolate was co-inoculated in combinationwith a diverse quasispecies population. These intriguing resultsdemonstrated that cooperation between variants within a viralpopulation was necessary for CNS invasion and the ensuingneuropathology. Cooperation among viral genotypes might includeevasion of the immune response simultaneously with CNS invasion.
Genetic bottleneck effects have also been observed as viral variantsenter the CNS. As thefirst fewviruses enter cellular routes into the CNS,antiviral responses become initiated which block entry for theremaining variants (Pfeiffer and Kirkegaard, 2006). This antiviralgenetic bottleneck effect, also referred to as the “burned-bridge”model, may contribute to the rare transmission of PV into the CNSwhich occurs in approximately 1 to 2% of cases (Gromeier andWimmer, 1998). Later studies have added to the “burned-bridge”modelwherebymultiple barriersmay contribute to genetic bottleneck

294 R.E. Rhoades et al. / Virology 411 (2011) 288–305
effects of quasispecies. These barriers whichmay limit neurovirulenceinclude the integrity of the gut, the induction of a protective innateimmune response, and inefficiency in neuronal transport of virus (Kusset al., 2008; Lancaster and Pfeiffer, 2010). Thus, EV entrance into thebrain appears to be a complicated interplay not only between the virusand the host, but also among viral variants within the quasispeciespopulation.
Enterovirus tropism
EVs are routinely neurotropic, yet each member of the virus genustargets different regions of the CNS (Table 1). A recent in vivo study byNagata et al. examined the localization of PV and EV-71 followingintravenous infection of monkeys. The authors identified PV-inducedlesions primarily within the pyramidal tract of the CNS causing a totalloss of motor neurons in the anterior horn of the spine. In contrast, EV-71 induced only limited damage in both the extrapyramidal andpyramidal tracts, leaving many motor neurons in the anterior horn ofthe spine intact (Nagata et al., 2004). Furthermore, the authors wereable to isolate PV from the entire CNS, including the dorsal rootganglia and the trigeminal. In contrast, EV-71 could not be isolatedfrom either of the latter two regions of the CNS. These results illustratethe broad range of neuronal target cells for PV, as compared to themore restricted neuronal targets for EV-71.
In yet another example of neuronal targeting of a picornavirus,TMEVwas shown to initially infect gray matter regions of the CNS, yetvirus persisted in the white matter following acute infection(Roussarie et al., 2007). Echovirus type 1 (ECHO-1-V) has beenshown to cause cellular necrotic lesions in the cerebral cortices oftransgenic mice expressing human integrin very late antigen 2,leading to paralysis and wasting (Hughes et al., 2003). In contrast,early CVB3 infection was found to be localized to specific neurogenicregions of the brain, including the subventricular zone (SVZ) (Feueret al., 2005).
Each EV genus member clearly prefers distinct regions of the CNS.Yet, what factors determine preferential tropism at the cellular level?Tropism at the cellular level can be viewed as an interplay of at leastthree general factors: the ability of the virus to infect and replicate inthe specific host tissues; the capability of the host cell to clear thevirus; and the capacity of the virus to avoid clearance by the host.Potential differences in the magnitude of the interferon α/β responsemay greatly influence PV tissue tropism (Ida-Hosonuma et al., 2005;Yoshikawa et al., 2006). The tropism of PV for neurons has previouslybeen shown to be also determined by the PV Internal Ribosomal EntrySite (IRES) (Kauder and Racaniello, 2004). Kauder et al. initially foundthat the tropism of PV towards nervous tissues could not be fullyexplained by organ-specific differences in IRES-mediated translationwithin age-matched samples. They investigated alterations in PVtropism by generating recombinant viruses engineered to contain theIRES from human rhinovirus (Kauder et al., 2006). In this manner, theinvestigators observed IRES-mediated, organ-specific translationaldifferences between EVs in adult versus neonatal infection. Theyconcluded that these differences might be attributed to IRES trans-acting Factors (ITAFs) differentially expressed in various cell types,including neurons.
Table 1Enterovirus tropism in the CNS.
Virus CNS localization Cell types i
Poliovirus Entire CNS Neurons, asEnterovirus-71 CNS — but not dorsal root ganglia or trigemina Neurons anCoxsackievirus Choroid plexus, neurogenic regions (SVZ and SGZ),
hippocampus, cortexNestin+m
TMEV Gray matter (acute) white matter (persistence) Neurons, as
IRES trans-acting factors (ITAFs)
ITAFs have been found to play a key role in EV IRES-mediatedtranslation initiation. Some IRESs require specific ITAFs, while othersrequire few additional proteins (Fitzgerald and Semler, 2009). Hence,tissue specific ITAFs may help to explain the tropism of EVs towardsparticular tissue types. Neurons may be more susceptible to infectiondue to the availability of specific ITAFs needed to initiate IRES-mediated translation. Investigation of TMEV and FMDV IRESssuggested that cell-specific differences in ITAFs may explain whysome viruses are able to replicate in neurons, while others cannot(Pilipenko et al., 2000). Furthermore, translation initiation of differentEVs IRES may depend on a combination of different ITAFs andeukaryotic initiation factors which may have different cell-specificlevels of abundance (Boussadia et al., 2003). Recently, the FarUpstream Element (FUSE) binding protein (FBP2), originally identi-fied to associate with a protein complex involved in intronic c-srcneuronal specific silencing enhancer, was discovered as a critical ITAFfor EV-71 infection (Lin et al., 2009a).
While the IRES and ITAFs have largely been associated with viralreplication inneurons, EVs are capable of infectingother cell types in theCNS. For example, PV can infect astrocytes and oligodendrocytes(Couderc et al., 2002). Also, it has been known for some time that TMEVcan infect astrocytes, yet persist in oligodendrocytes (Rodriguez et al.,1983). EV-71 has been found to readily infect and replicate inastrocytoma cultures (Kung et al., 2007) and cultures of rat brainastrocytes (Tung et al., 2010). We have shown that CVB3 preferentiallyinfects NPSCs (Feuer and Whitton, 2008), and more recently, a novelpopulation of nestin+myeloid cells infiltrating into the CNS (Tabor-Godwin et al., 2010). Parechoviruses (P-ECHO-Vs) are suspected to betaken up by microglia which leads to the activation of these residentimmune cells (Volpe, 2008). Also, microglia, and glial cells may bepotential sites of EV persistence. For example, macrophages andmicroglia have been found to be the main reservoir for harboringTMEV during persistent infection (Roussarie et al., 2007). RespiratoryEV, including rhinoviruses (RVs), have not been historically found toinfect theCNS.However, a recent study suggested that recombinationofrespiratory EV to genetically similar viruses, such as CV and PV, mayeventually lead to respiratory EVs with tropism for the central nervoussystem (Tapparel et al., 2009). This possibility is not implausible,especially with the recent findings suggesting the contribution of viralvariants or quasispecies to PV spread into the CNS (Vignuzzi et al.,2006).
Immune responses to enteroviruses
The immune response plays a critical role in protecting the hostfrom viral pathogens by both modulating the release of chemokinesand inflammatory cytokines for leukocyte recruitment, and bydirectly fighting infection via the interferon response. An informativereview of chemokine induction in response to neurotropic infectionshas recently been published by Hosking and Lane (2010). Thesechemoattractant molecules may be especially critical to combatingmicrobes within immunoprivileged sites, such as the CNS. We havedemonstrated the induction of numerous chemokines in the CNSfollowing CVB3 infection. One particular chemokine, CCL12, may play
nfected — acute Cell types infected — persistence
trocytes, and oligodendrocytes Neuronsd astrocytes Persistence documented; site unknownyeloid cells, NPSCs, and neurons NPSCs (in culture)
trocytes, and oligodendrocytes Macrophages, microglia, and oligodendrocytes

295R.E. Rhoades et al. / Virology 411 (2011) 288–305
an essential role in the recruitment of nestin+myeloid cells thatinfiltrate across the blood-CSF-barrier and become infected upon theirentry through the choroid plexus (Tabor-Godwin et al., 2010).“Bystander” casualties suffered upon activation of cytolytic T cellsduring an adaptive immune response within the CNS may bepotentially more devastating to neurons than a viral infection itself.Thus, the host may restrict or control immune responses in responseto a viral infectionwithin immunoprivileged sites; this restrictionmaypartly explain why certain viruses may preferentially target the CNS.
Innate immune response following enterovirus infection
The innate immune response begins with the recognition of thevirus by cytoplasmic sensors. EVs have been shown to activateessential innate immune response molecules, including Toll-likeReceptor 3 (TLR3), Retinoic Acid Inducible Gene I (RIG-I), andMelanoma Differentiation-Associated Gene 5 (MDA5). TLR3 is locatedon the membrane of endosomes or the plasma membrane andrecognizes double-stranded RNA, a structure generally observedduring viral replication of all RNA viruses. Recent studies suggestthat TLR3 plays a strong role in cardioprotection against EV infectionsand may depend on autophagic processes (Gorbea et al., 2010).Studies of the recognition of EVs by cytoplasmic sensors of the innateimmune response have largely centered on DExD/H-box-containingRNA helicases, such as RIG-I and MDA5. In examining encephalo-myocarditis virus (EMCV) induction of the type I interferon (IFN)response in mouse embryonic fibroblasts, Kato et al. concluded thatMDA5, but not RIG-I, was critical for picornavirus detection (Katoet al., 2006). However, this does not mean that RIG-I is excluded frompicornavirus detection. By utilizing MDA-5 knockout mice, Papon etal. observed that RIG-I was also useful in detecting EMCV (Papon et al.,2009). Both of these sensors may play important roles in EV detectionby the host. EVs may circumvent the action of these molecules byencoding proteins that affect their signaling pathways.
Once a pathogen is recognized, the innate immune response mayplay a substantial role in initiating virus-mediated neuropathologyfollowing EV infections. For example, the severity of echovirus and EVinfections in the CNS have been associatedwith higher systemic levelsof proinflammatory cytokines like IL-6, IL-1β, and TNF, which can leadto greater cytokine-induced tissue destruction (Lin et al., 2003; Liuet al., 2005). Also, CV activation of the inflammatory response hasbeen shown to cause extensive infiltration of leukocytes into the CNSthereby causing inflammatory lesions and contributing to neuropa-thology associated with the virus (Feuer et al., 2009).
In addition to the potentially harmful inflammatory responsestriggered within the CNS, EV infections may also initiate the type I IFNresponse pathway. TLR-3, RIG-1, and MDA5 are all able to induce thetype I IFN response. TLR-3 induces the production of type I IFNs byactivating the transcription factors Interferon Regulatory Factor 3(IRF3), NF-κB, and AP-I through the adaptor protein TIR-domain-containing Adapter Inducing Interferon β (TRIF) (Matsumoto andSeya, 2008; Wilkins and Gale, 2010). The RIG-I and MDA-5 pathwaysare distinct and independent of the TLR-3 pathway. RIG-I and MDA-5both interact with the adaptor molecule IPS-1 through their CARDdomains. IPS-1 transfers the activation signal to downstream kinases,which in turn activate IRF-3 and other transcription factors involvedin type I IFN induction (Kato et al., 2006). Malathi et al. determinedthat the helicase activity of RIG-I and MDA5 may have importantautoregulatory roles and work in concert with Endoribonuclease L(RNase L) to produce small self RNA cleavage products that caninteract with RIG-I or MDA5, thereby amplifying the signal (Malathiet al., 2007).
Following their induction, type I IFNs bind to their receptors eitheron the same cell or on neighboring cells. Binding of type I IFNs to theirreceptor induces the transcription of antiviral miRNAs and IFNStimulated Genes (ISGs) through the JAK/STAT pathway. Many of
these ISGs encode antiviral products or serve to further upregulate thetype I IFN pathway. For example, RNase L is an ISG that contributes tothe amplification of the type I IFN response, but also cleaves viral RNAand inhibits their translation. Furthermore, the antiviral activity ofRNase L has been found to have a protective role in the CNS againstcoronavirus-induced demyelination. In comparing wildtype andRNase L−/− mice, Ireland et al. found that RNase L deficienciesincreased demyelination and axonal damage in the brain followinginfection, and affected the regulation apoptosis (Ireland et al., 2009).Additional ISGs encode products that can inhibit specific viruses.Additionally, IFN-β has been found to modulate the expression ofantiviral microRNAs in response to RNA viruses, including hepatitis C(Pedersen et al., 2007). Hence, it is reasonable to suspect that type IIFN-induced antiviral miRNAs might play an important role in hostdefense against EVs in the CNS.
EVs have evolved a surprising number of mechanisms for under-mining the host innate immune response, attacking at different stagesof the IFN induction and response pathways. EV and cardiovirus (suchas TMEV) proteins may counter-act host defenses (Agol and Gmyl,2010). The ability to evade the host antiviral response may be animportant contributing factor not only for maximizing acute infection,but also for the successful establishment of viral persistence. PV,rhinovirus (RV), and EV have been found to reduce RIG-I levels anddisrupt RIG-I mediated interferon signaling (Barral et al., 2009). Areduction in RIG-I levels has been attributed to the activity of the PV3C protease. PV and RV type-1a have also been observed to cleaveMDA5 through a caspase and proteasome-dependent mechanism(Barral et al., 2007). Since RIG-I signaling induces further RIG-Iexpression, and MDA5 provides secondary protection against viralinfection in the host cell, EVs may also target the downstreamsignaling pathways for these molecules. The 3C protease of EV-71 hasalso been found to disrupt RIG-I signaling through a protease-independent fashion. Instead of cleaving, 3C protease binds to RIG-Iand prevents the recruitment of IPS-1 (Lei et al., 2010). In contrast,RV-14 attenuates the type I interferon response by targeting theactivation of IRF-3 upon identification by MDA5 (Kotla et al., 2008).Similarly, TMEV has been found to inhibit IRF-3 dimerization (Ricouret al., 2009).
Once the antiviral response has been initiated, viruses havedeveloped ways to combat these protective actions. PV and RV havebeen found to cleave Nup62 (Park et al., 2010) and degrade Nup153and Nup98 (Park et al., 2008). By altering the nucleus by degradingnuclear pore complex proteins, viruses can affect host mRNA andprotein localization, and shut down host protective factors. Thehyperphosphorylation of Nup98 by the L protein during TMEVinfection has been shown to block host mRNA export from thenucleus (Ricour et al., 2009). Herpesvirus genomes have been foundto encode miRNAs suggesting that they exploit the host miRNAmachinery to regulate the expression of host and viral genes (Pfefferet al., 2005). Although this mechanism has not been demonstrated forEVs, Pelletier et al. have found that cells exposed to and cured of PVusing RNAi respond more quickly to RNAi treatment, as compared tocells never having been exposed to PV (Pelletier et al., 2010). Theseintriguing results suggest that cellular miRNA processing machineryplays an antiviral role during EV infections, as well. Furthermore, cellswhich have successfully cleared the virus may be permanently alteredto better respond to future viral infections.
Adaptive immune response following enterovirus infection
Numerous clinical case reports involving patients suffering fromencephalitis due to EV document the importance of neutralizingantibodies in controlling infection (Xie et al., 2010). The significantcontribution of a neutralizing antibody response in controllinginfection is also shown by studies describing individuals sufferingfrom agammaglobulimia. The absence of neutralizing antibodies in

296 R.E. Rhoades et al. / Virology 411 (2011) 288–305
agammaglobulimic patients results in an increased susceptibility toEV infections of the CNS that can lead to chronic neuropathies(Misbah et al., 1992). Experiments evaluating CVB3 infection in micelacking B cells (BcKO mice) indicate that antibodies are critical forviral clearance (Mena et al., 1999). The role of B cells in controllingCVB3 infection may be more complex by evidence suggesting B cellsmay contribute to virus dissemination via the “Trojan horse”hypothesis. Early after infection in normal mice, high levels of viralRNA was observed in proliferating lymphocytes located within themarginal zone of the spleen.
Macrophages and microglia may be involved in EV clearancewithin the CNS. These phagocytic cells are thought to be earlyresponders to viral infection. The presence of activated microglia andmacrophages in response to CVB3 infection has been observed in ourneonatal mouse model (Feuer et al., 2009). By confocal microscopy,Iba1+ macrophages/microglia within the CNS were shown activelyengulfing virally-infected cells.
T cells also play a critical role in the adaptive immune response toEV infection in the CNS; however, bystander damage following theiractivation may be significant. Much work in understanding T cellresponses to picornavirus infection in the CNS and the ensuingimmune-mediated pathology has been described for TMEV duringacute and persistent infection. A highly detailed and informativereview on TMEV-induced molecular mimicry model of multiplesclerosis has been published (Olson et al., 2005). Infiltration of CD4+
and CD8+ lymphocytes within the CNS has also been shown followingEV infection (Lin et al., 2009b). Exacerbation of virally-inducedmorbidity may occur in mice deficient in CD4+ and CD8+ lympho-cytes, indicating that T cells are necessary to combat infection. Incontrast, some EVs such as CVB3, have evolved ways to escapedetection by CD8+ T cells via the inhibition of antigen presentation bytheMHC class I pathway (Kemball et al., 2009). Therefore, activation ofthe T cell response may vary greatly, depending upon the EV genus(Slifka et al., 2001).
Enterovirus persistence
Although EV possess multiple mechanisms by which they canevade the host immune response, their success is not absolute, andthe struggle between the host and virus can last for very long periodsof time. EV persistence appears to be the product of the ongoingattempt of the host to eliminate or suppress virus replication, and thevirus' struggle to remain intact in a hostile cellular environment.Under the selective pressures generated by a successful host immuneresponse, sometimes the best defense for the virus is simply tomutate. As described above, errors in EV replication can lead to theexistence of viral quasispecies (Domingo et al., 2008) which maybroaden the tropism of EV (Vignuzzi et al., 2006), assist in evasionfrom the immune response, and lead to persistence. Thus, perhaps itcomes as no surprise that EVs may persist in the CNS and avoidclearance by the host.
EV-71, PV, CVB3, and TMEV all havemechanisms formitigating thehost innate immune response. These viruses have been observed topersist long after the initial infection. Evidence of EV-71 persistence ina clinical setting has been observed by the continued detection ofvirus sequences in the excretions and secretions of patients long afterthe detection of the initial infection (Han et al., 2010). Whether or notthe CNS is a potential site of the EV-71 persistence has not yet to bedetermined. In the case of TMEV, virus has been found to persist inoligodendrocyte cell cultures, but the main reservoir for persistentTMEV may be macrophages (Roussarie et al., 2007). Upon infection,TMEV is transferred from the neuronal axon to the oligodendrocyte ina myelin-mediated fashion; following the ingestion of infectedoligodendrocytes, macrophages become the primary reservoir forTMEV persistence.
PV has previously been demonstrated to persist in primary neuralcell cultures (Colbere-Garapin et al., 1998). PV persistence andreactivation has been a suspected cause of Post-Polio Syndrome(PPS) (Baj et al., 2007). Indeed PV RNA could be detected in somepatients with PPS, though the persistent virus may be very differentfrom the wild type strain (Baj et al., 2007). The low viral load and theunclear mechanism of reactivation for mutated virus in PPS patientsmost likely fuel the controversy regarding the potential contributionof persistent PV material to recurring disease. Perhaps PV persists inan attenuated form in peripheral nervous tissues of the host at lowreplication rates; a reactivation event, such as injury, might triggerhigher levels of viral replication with ensuing neurological sequelae.Injury-mediated retrograde axonal transport of PV has been demon-strated to carry PV into the CNS (Gromeier and Wimmer, 1998), andmay be a mechanism by which PV can be transported from sites ofpersistence back to the CNS.
CV persistence in the heart has been the subject of muchinvestigation, and its persistence in the CNS has only recently beendescribed (Feuer et al., 2009). In the heart, CV persistence is associatedwith chronic myocarditis and dilated cardiomyopathy (Chapman andKim, 2008). The host innate immune response, in particular the type IIFN response, is extremely critical for controlling CV infection of theheart (Deonarain et al., 2004). The type I IFN response might alsocreate selective pressures resulting in viral genomemutations (Kim etal., 2005b), attenuation of CV, and persistence in the heart. Genomedeletions in the 5′ UTR of CVB3 were recently observed upon passageof CVB3 in primary heart cell cultures. These deletionswere associatedwith a reduction in cytopathic effects (cpe) without reductions in viraltiters (Kim et al., 2008). Similarly, persistent CVB3 RNA was detectedin the CNS of mice following neonatal infection for up to 90 days post-infection (PI), as determined by nested RT-PCR, in the absence ofinfectious virus by plaque assay (Feuer et al., 2009). Our most recentresults suggest that CVB3-infected neurospheres, or NPSCs grown inculture as free-floating structures, may support a persistent or carrier-state infection (manuscript submitted). Based on these results, wehypothesize that neurogenic regions of the CNS may be potential sitesof CVB3 persistence in vivo. Perhaps CVB3 reactivation is inducedupon occasional proliferation and asymmetric division of resting orquiescent type B neural stem cells harboring persistent virus withinthe CNS (Fig. 3), thereby leading to intermittent replication of virus.
The possible persistence and reactivation of EV in a clinical settingis of profound importance, especially with the addition of immuno-suppressive drugs, such as Rituximab, given to patients suffering fromB cell lymphomas. Immunosuppression, especially with drugs target-ing the humoral immune response, may lead to reactivation/increasedreplication of persistent EV in the CNS with potentially dangerousneurological complications (Schilthuizen et al., 2010; Servais et al.,2010).
Pathophysiology of enterovirus infection
EV infection of the CNS has been associated with acute flaccidparalysis (Solomon and Willison, 2003), acute disseminating myelitisand acute transverse myelitis (Agin et al., 2010; Minami et al., 2004).Aseptic meningitis and encephalitis can also result from EV infection(Dalwai et al., 2010; Lewthwaite et al., 2010). Further evidenceindicating the extensive distribution and diversity of EVs associatedwith human disease is demonstrated by a recent informativepublication by Victoria et al. (2009). Their metagenomic analysessuggested the presence of circulating human EV species A (HEV-A)through HEV-C, including other members of the Picornaviridae, suchas P-ECHO-Vs, rhinoviruses, and human cardioviruses in South Asianchildren suffering from acute flaccid paralysis. Metagenomic analysismay be a highly informative technique in determining the distributionand number of circulating EVs in human populations.

Fig. 4. Increased susceptibility of young mice to coxsackievirus infection andsubsequent CNS pathology. Neonatal SJL mice (days 1, 2, or 6 post-birth) were intra-cranially infected with 100 pfu CVB3. The brains of infected mice were harvested ondays 11, 15 or 33 post-infection, respectively. De-paraffinized sections of the brainswere stained with hematoxylin and eosin and inspected by microscopy for lesions andinflammatory cells. (A) One day-old mice suffered the greatest level of neuropathologyfollowing infection. Lesions were observed within the cortex and hippocampus (blackarrows). (B) A higher magnification of (A) revealed the loss of pyramidal neurons in thehippocampus and the presence of inflammatory cells (black arrows). (C) In contrast,two day-old mice infected with an identical amount of CVB3 showed reduced signs ofneuronal loss restricted to the CA3 and CA4 field of the hippocampus (black arrow). Thepresence of immune cell enriched perivascular cuffs were observed near thehippocampus (black arrow). (D) Six day-old mice infected with CVB3 showed littleor no signs of CNS disease.
297R.E. Rhoades et al. / Virology 411 (2011) 288–305
Clinical diagnosis of enterovirus infection of the CNS
A variety of differing techniques have been used in the clinicaldiagnosis of EV infections of the CNS (Table 2); a comprehensivedescription of which is beyond the scope of this review. TheGreeneChip pioneered by Ian Lipkin represents the technologicalforefront of pathogen identification, but has yet to be employed in thecontext of EV infections of the CNS (Hunter, 2008). Diagnosis viaselective culture using transgenic cell lines is limited and hinderedprimarily by the absence of cell lines supporting strain-specificreplication (Leland and Ginocchio, 2007). In contrast, moleculartechniques, such as RT-PCR, represent a sensitive and precisemethodology for identification of EV CNS infection. Cerebrospinalfluid (CSF) from afflicted patients is the preferred source of clinicalsample upon which these techniques can be performed. Genomicanalysis using RT-PCR can be completed within 24 h of samplecollection (Romero, 1999). RT-PCR diagnosis of enteroviral meningitishas been performed using primers recognizing a conserved regionwithin the 5′ UTR (Rotbart, 1990). While genus level identification ofEVs is clinically relevant and can be used to guide antiviral regimes,strain-specific genotyping is required in some instances. RT-PCRcharacterization of the VP1 region has lead to strain-specificphylogenetic classification (Mirand et al., 2008). Sequencing of theVP4 and VP2 regions was performed in instances where moleculartyping using the VP1 region was inconclusive. These studies indicatethat RT-PCR is an effective and clinically feasible technique for theidentification of the specific EV strain present in clinically obtainedCSF samples.
Quantitative Real-Time PCR (qRT-PCR) may be a more sophisti-cated molecular method utilized to detect the amount of EV in clinicalCSF samples (Dierssen et al., 2008). The majority of qRT-PCR assaysidentifying EV use the primer pair designed by Robart et al. in 1990,although variations of these primers do exist (Rotbart, 1990). Alimitation of the technique involves the absence of amplificationcurves for samples containing mutations in the probe binding region(Hymas et al., 2008).
Contributions of apoptosis to enterovirus disease in the CNS
We have previously described the induction of CNS lesions (Fig. 4),inflammation, and apoptosis within CVB3-infected neurons in thecortex and hippocampus (Feuer et al., 2003). TUNEL staining showedcolocalization of infection and apoptosis within the CNS following ICinoculation of our neonatal mouse model with a recombinant CVB3expressing eGFP (eGFP-CVB3). A direct overlap of infection andactivated caspase-3 protein revealed infected cells undergoing earlystage apoptosis. Also, infection of virally-infected neuronal precursorcells contributed to the generation of lesions within the CNS. We alsorecently revealed the induction of apoptosis in the choroid plexus(Tabor-Godwin et al., 2010) following CVB3 infection. These resultssuggest that EV may compromise the function of the choroid plexus,an essential organ involved in CSF production and immune regulation.
Table 2Methods used to identify and classify enterovirus CNS infections.
Technique Method of identification Host iso
Tissue culture (Leland, 2008) Presence of cellularcytopathic effect
Cerebra
Reverse-transcription polymerase chainreaction+genomic sequence (Romero, 1999)
Genomic amplification Cerebra
Quantitative real time PCR (Dierssen, 2008) Genomic amplification Cerebra
Immunohistochemistry Visualization using virallyspecific antibodies
Centralsystem
In situ hybridization Visualization using virallyspecific probes
Centralsystem
The observation of hydrocephalus in mice following CVB3 infectionmay be related to choroid plexus dysfunction following infection.Reports also indicate that PV infection may be associated withinduction of apoptosis in the CNS (Girard et al., 1999). DNAoligonucleosomal laddering and enzyme-linked immunosorbent(ELISA) assays performed upon CNS samples obtained from miceexhibiting paralytic poliomyelitis indicated the presence of cellsundergoing apoptosis. These studies indicate that EVs are capable ofinducing apoptosis within the CNS.
Potential behavior and memory dysfunction followingenterovirus infection
The presence of infected neurons and ongoing apoptosis in thehippocampus and other regions of the CNS is highly suggestive thatmemorydysfunction or behavior changesmight be expected followingEV infection. Previous studies have suggested a link between EV
late Tools Specificity
l spinal fluid Selective cell lines Genus
l spinal fluid Enterovirus specific primers—majorityamplify 5′ UTR (Rotbart, 1990)
Serotype — nucleotidemutations (Mirand, 2008)
l spinal fluid Enterovirus specific primers —majority amplify 5′ UTR
Genus
nervoustissue
Visualization/microscopy Cellular localization
nervoustissue
Visualization/microscopy Cellular localization

298 R.E. Rhoades et al. / Virology 411 (2011) 288–305
infection early in childhood and the development of schizophrenia(Rantakallio et al., 1997; Suvisaari et al., 2003). EV infection of the CNSoccurring during childhood is also associated with long termneuropathies including delayed neurodevelopment and reducedcognition (Chang et al., 2007). Clinical examination of placentalsamples from newborns exhibiting neurodevelopmental defects hasrevealed the presence of EV within the tissue (Euscher et al., 2001).EV-71 has specifically been implicated as the causative agent ofdevelopmental defects in the CNS (Huang et al., 2006). Infection ofpregnant mice with polyinosinic–polycytidylic acid, a compound thatmimics replicating virus, may lead to inhibition of embryonic neuronalstem cell development (De et al., 2010). Therefore, developmentaldefects observed following EV infection of the CNSmight be attributed,at least in part, to the abrogation of normal stem cell replicationwithinthe brain.
Experiments using the Morris water maze as an indicator ofmemory formation found that mice infected with TMEV which alsocan target the hippocampus exhibited a spatial learning deficit (Buenzet al., 2006). The deficit was correlated with the extent of damage tothe hippocampus resulting from TMEV infection. We are currentlyexamining the consequences of CVB3 infection on CNS developmentand spatialmemory dysfunction.We expect that lasting consequenceson brain function may result following persistent CVB3 infection.These studies may be highly significant in a clinical setting, especiallygiven that EV infections comprise the great majority of asepticencephalitis infections in humans.
Antiviral drugs to treat enterovirus infections — RNAibased approaches
The idea that RNAi may act as a potent natural antiviral againstRNA viruses in mammalian cells was first shown in 2003 (Gitlin andAndino, 2003). Since then, RNAi has proven to effectively inhibit EVreproduction both in vitro and in vivo in a variety of cell and mouselines in Table 3. Mechanistically, siRNAs inhibit the production ofinfectious virions via Dicer recognition of the viral dsRNA formedduring genomic replication (Aliyari and Ding, 2009). Targeted RNAsare subsequently degraded, effectively hindering the formation ofnascent virions.
The vast majority of siRNAs developed against EV focus upon thedegradation of mRNAs coding for the viral RNA-dependent RNApolymerase (RdRp) and proteases. For example, siRNAs directedagainst protease 2A were the most effective in the inhibition of CVB3infection in HeLa cells andmurine cardiomyocytes (Yuan et al., 2005).Interferon receptor knock-out mice transfected with siRNAs targetingCVB3 protease 2A exhibited increased survival time and attenuatedviral replication when challenged with CVB3 (Merl et al., 2005). The19-mer siRNAs targeting the viral 3Cpro region of coxsackievirus B4(CVB4) were effective in decreasing viral replication in rhabdomyo-carcoma cells (Tan et al., 2010). siRNAs targeted against the 3DPol ofEV-71 has also proven protective against this virus in vivo (Tan et al.,2007). Prophylactic treatment of suckling mice with siRNAs prior toviral inoculation decreased the level of hind limb paralysis and weightloss associated with EV-71 infection. Also, RT-PCR and western blots
Table 3Compounds used to treat enterovirus infections.
Compound Target Stage of development BBB penetra
Ribavirin(Li, 2008)
Viral genome Patient prescription Conflicting re(Hosoya 200
Pleconaril(Pevear, 1999)
VP1 protein ofnucleocapsid
Clinical-phase III–IV(Webster, 2005,Desmond 2006)
Yes(Schmidtke,
RNAi (multipleformulations)
Viral genome —majority targetprotease 2A+3C or polymerase3D (Yuan, 2005; Tan, 2010, 2007)
In vitro/in vivo(Li, 2008)
Undocumen
demonstrated a decrease in viral replication and viral proteinexpression levels within the intestines of siRNA-treated mice.
EVs are especially prone to the formation of escape mutants due tothe absence of an RdRp proofreading mechanism. The low fidelity ofthe RdRp increases the likelihood of mutants escaping the therapeuticeffects of RNAi. The formation of escape mutants resistant to anti-CVsiRNAs has been documented (Merl and Wessely, 2007). PV escapevariants against siRNAs evolve to incorporate a single nucleotidemutation located in the center of the targeted RNA (Gitlin et al., 2002).One strategy to combat this phenomenon may be the simultaneousadministration of multiple siRNAs. The administration of a cocktailconsisting of three distinct siRNAs may reduce the number of escapemutant progeny to extremely low levels (Merl and Wessely, 2007).Targeting receptors of viral entry with RNAi may be another strategyof effectively inhibiting EV replication. siRNAs directed againstmurineCAR (mCAR) decreased CVB3 titers in mice (Werk et al., 2005). RNAidegradation of host genes constitutes a unique approach which maymitigate the formation of potential viral escape mutants by affectingcellular targets, as opposed to viral targets.
The development of therapeutic siRNAs symbolizes a novel and asof yet, undeveloped candidate for the treatment of EV infections of theCNS (Vaishnaw et al., 2010). However, RNAi as antiviral therapy hasyet to be employedwithin the CNS. Once the hurdle of delivering RNAitherapeutic constructs to the CNS has been overcome, siRNAs couldpotentially be used to treat life-threatening EV infections. EVinfections of the CNS rarely occur in the absence of infection ofperipheral tissues outside the brain. Therefore, even if a therapeuticagent has not been demonstrated to hinder virus production withinthe CNS per se; by inhibiting replication in other tissues, an siRNA-based drug might impede virus growth and the eventual progressionof disease into the CNS. In summation, RNAi represents an immatureyet powerful tool that should not be overlooked in the development oftherapeutics designed to treat EV infections of the CNS.
Antiviral drugs to treat enterovirus infections — ribavirin
Ribavirin (1-(_-d-ribofuranosyl)-1H-1,2,4-triazole-3-carboxamide)was first synthesized in 1972 by ICN pharmaceuticals. Currently underclinical development as a broad-spectrum antiviral, ribavirin has beenshown to inhibit the replication of a variety of EVs. Ribavirin, anucleoside analog, may act as amutagen via incorporation into the viralRNA genome (Crotty and Andino, 2002; Crotty et al., 2000, 2001). Thepresence of ribavirin may force the afflicted virus into “Errorcatastrophe” by generating a highly variable noninfectious quasispeciesswarm and thereby causing lethal mutagenesis (Vignuzzi et al., 2006).Ribavirin has been found to inhibit both in vitro and in vivo EV-71replication (Li et al., 2008). Human neuronal and mouse neuronal celllines treated with ribavirin showed decreased signs of cpe followingEV-71 infection. Also, ribavirin-treated mice exhibited decreasedmortality, morbidity, and paralysis rates when challenged with EV-71(Li et al., 2008).
There are conflicting reports on the ability of ribavirin to crossthe BBB; a necessary criterion when dealing with the treatment ofEV infections of the CNS. Upon treatment of subacute sclerosing
tion Resistance Mechanism
ports1+Honda 1994)
Yes (Poliovirus Isolates)(Vignuzzi, 2005+Pfeiffer 2003)
Nucleoside analog— genomicincorporation— error catastrophe
2009)Yes (CVB3 Nancy Strain)(Schmidtke, 2005)
Conformational change of VP1protein — receptor attachment —genomic uncoating (Chen, 2008)
ted Yes (Coxsackie+Poliovirus Isolates)(Merl, 2007; Gitlin, 2002)
Viral RNA degradation via Dicerrecognition (Aliyari, 2009)

299R.E. Rhoades et al. / Virology 411 (2011) 288–305
panencephalitis (SSPE), a neurological disease caused by persistentmeasles infection, only direct intracranial (IC) and not IP administra-tion of RBV diminished the effects of this virus (Honda et al., 1994).Combining the drugwith the lipophylic carriermolecule, cyclodextrin,may increase the concentration within the CNS following IP injection(Jeulin et al., 2009). Ribavirin has also been combined with IFN-αtherapy to treat SSPE (Hosoya et al., 2001). Patients receivedintravenous (IV) ribavirin, as well as intraventricular IFN-α treatment.Upon treatment with ribavirin (20 mg/kg), high performance liquidchromatography quantification indicated that the compound waspresent within the cerebral spinal fluid of one patient at aconcentration of 7.5 μg/ml, a concentration shown to inhibit thereplication of SSPE in both tissue culture and mouse studies (Hosoyaet al., 1989; Ishii et al., 1996). Therefore, ribavirin may be capable ofcrossing the blood brain barrier (BBB) in sufficient quantities and toinhibit viral replication. In our neonatal model of CVB3 infection, IPadministration of ribavirin led to brain wet weight recovery(manuscript in preparation) indicating that the compound may crossthe BBB in effective quantities to reduce CVB3 replication duringpersistent infection.
EV resistance may necessitate the development of new antiviraldrugs to combat these nefarious pathogens. Resistance againstribavirin by PV has been recently observed (Vignuzzi et al., 2006).PV may combat the effects of ribavirin via a single point mutation inthe RdRp, effectively increasing the fidelity and lowering the viralgenomic mutation rate (Pfeiffer and Kirkegaard, 2003). Intriguingly,the emergent ribavirin-resistant quasispecies swarm may be lessadaptable to a changing environment.
Antiviral drugs to treat enterovirus infections — pleconaril
Pleconaril,3-(3,5-dimethyl-4((3-(3-methyl-5-isoxazolyl)propyl]oly)phenyl)-5-(trifluoromethyl)-1,2,4-oxadiazole is currently licensedby Schering Plough and has been developed as an anti-picornaviral drugwith demonstrated efficacy against many EVs (Pevear et al., 1999).Pleconaril is able to cross the BBB and remain within the CNS atconcentrations that inhibit EV replication (Schmidtke et al., 2009). Themechanism of action for pleconaril against viral pathogens is two-fold;the compound inhibits both viral attachment to the cognate receptorand uncoating of the nucleocapsid during replication (Chen et al.,2008b). Pleconaril inhibits viral attachment by binding to the VP1protein present in the canyon floor or ‘pocket’ of the nucleocapsid andinducing a conformational change in the protein. This conformationalchange synergistically inhibits the release of the viral RNA from thenucleocapsid, effectively hindering replication. Tissue culture andanimal challenge studies testing the susceptibility of clinical EV isolatesto the drug have demonstrated antiviral activity (Pevear et al., 1999).Also, numerous case studies evaluating the efficacy of pleconaril to treatclinically ill patients including immunocompromised individuals havebeendescribed (Desmondet al., 2006;Webster, 2005). A previous studyhas suggested that the Nancy strain of CVB3 may be resistant topleconaril (Schmidtke et al., 2005). This resistance was found to be dueto a pointmutation at amino acid 1092 of the CVB3 open reading frame.Resistance was associated with a leucine at this position, whereasisoleucine and valine were associated with susceptibility to pleconaril.In summation, these studies demonstrate that pleconaril may be avaluable compound in the treatment of some EV infections of the CNS.
Intra-venous immunoglobulins to treat enterovirus infections
The standard therapy for aseptic meningitis caused by EV infectioncontinues to be intra-venous immunoglobulin (IVIg) treatment,although the efficacy has not been proven (Abzug, 2004). IVIg istypically prepared from pools of plasma samples from healthy donors(Cheng et al., 2008). This passive immunization-based therapy mightneutralize infectious virus circulating within the host, in addition to
other non-specific inflammatory mechanisms (Ooi et al., 2010). Fig. 5illustrates the mechanism of action for each of the antiviralcompounds and IVIg, described above. In addition, novel antiviraltherapies against EVs continue to be developed (Wu et al., 2010).
Vaccines against enteroviruses
The historical Salk and Sabin vaccines against PV demonstrate theeffectiveness of immunization in protecting the host against EVinfections. Many effective vaccines stimulating both the innate andadaptive immune response have been designed to combat theremaining clinically relevant EVs. To combat EV infection, the adaptiveimmune response employs both T cells and antibodies in the clearanceof the virus. Therefore, the most successful vaccines activate bothhumoral and cell-mediated immunity and induce lasting viral immu-nity. The administration of novel vaccines to patients comes withpotential risks, extensive and costly clinical studies, and a potentiallyapprehensive public. Unfortunately, acceptance of EV-based vaccines tothe public may not materialize unless the potential diseases caused bythese pathogens become much more widely appreciated. That said,ongoing EV vaccine studiesmay help us improve the efficacy and safetyof potential vaccine candidates, especially if EV transmission and/ordisease manifestations increase in the general population in the future.Also “therapeutic vaccines”, those vaccines given after initial infection,might bemore readily accepted in patients suffering fromEV-mediateddisease. “Therapeutic vaccines” could be envisioned which mayenhance or redirect an ongoing immune response in order to reduceviral load during early infection, or after the establishment of viralpersistence.
Poliovirus vaccines
Attenuation of EVs through mutations in the genome hashistorically led to efficient vaccine production. Perhaps the mostwell-known attenuated form of PV is that used for the Sabin vaccine,which has decreased neurovirulence in part controlled by two stemloops in the viral IRES (Gromeier et al., 1999). Another mutation thatcan cause CNS attenuation is located between the 5′NTR cloverleaf andIRES and reduces the binding of polypyrimidine tract-binding protein(Guest et al., 2004). Other studies havemade recombinant viruses thatuse the IRES from human rhinovirus type 2 (HRV2) to attenuateneurovirulence in the Sabin vaccine strain of PV as well as in herpessimplex virus type 1 (Campbell et al., 2007; Gromeier et al., 1996).Somewhat alarmingly, a vaccine-derived PV and coxsackievirus A17recombinant has been generated in the laboratory, thus illustrating thepossibility of such events occurring naturally (Jegouic et al., 2009).
Mutations causing changes in virulence and/or attenuation canalso exist in other regions of the genome. Recent publications haverevealed Sabin vaccine strains that in rare instances caused paralyticpoliomyelitis, havemutations in the capsid protein VP1 representing amutational hot-spot (Blomqvist et al., 2010; Rahimi et al., 2007).Furthermore, defective interfering particles generated through muta-tions in the capsid region of PV in vitro have been used to investigateviral replication (Hagino-Yamagishi and Nomoto, 1989). Newerstudies have used cleavage site mutants to learn more about PVreplication and encapsidation, which appear to be separate steps inthe viral life cycle (Oh et al., 2009).
Both inactivated and attenuated forms of the historical PV vaccineshave been used to induce or confer immunity to the virus. The originalformalin-inactivated form of the vaccine (IPV) was developed byJonas Salk and licensed in 1955 (Salk et al., 1954). In 1963, an orallyadministered live attenuated PV vaccine (OPV) was formulated(Sabin, 1957). The usage of these vaccines and optimized versionshas severely reduced the incidence of poliomyelitis, although thepathogen has yet to be eradicated worldwide. Preference for theadministration of the IPV over the OPV is due to the discovery of

Fig. 5. Antivirals against enteroviruses: mechanisms of action. Pleconaril, ribavirin, intra-venous immunoglobulins (IVIg) and RNAi each inhibit the production of infectious virions atdifferent steps. Pleconaril induces a conformational change in the viral VP1 capsid protein that inhibits both genome uncoating and the binding of the virus to its cognate receptor,CAR. Ribavirin, a nucleoside analog, is incorporated into the viral genome. This incorporation results in viral genomic mutations that lead to “error catastrophe”. Virus-specific IVIgmay bind to virions extracellularly and inhibit the virus from entering the cell. RNAimolecules target the positive sense viral RNA strand leading to Dicer-mediated degradation of theviral genome. However, escapemutants may form that avoid the effects of RNAi. Positive-sense strand viral RNA is shown in black; negative sense strand viral RNA is shown in green.Antiviral compounds are shown in red. The replication complex is shown in blue.
300 R.E. Rhoades et al. / Virology 411 (2011) 288–305
circulating vaccine-derived PVs (cVDPV) associated with the OPV.cVDPVs are virulent PVs derived from the OPV that occur in a smallminority of vaccine recipients. The reversion of cVDPVs fromattenuation to virulence is a direct consequence of the geneticinstability of the vaccine. In 2000, cVDPVs were responsible for a poliooutbreak in the Dominican Republic and Haiti (Olen Kew 2002).Sequencing determined that the cVDPVs were recombinant viruses.The derivation of neurovirulent polio strains from the OPV has led tothe “OPV paradox,” which is based upon the idea that completeeradication of poliomyelitis is contingent upon the elimination of theattenuated form of the vaccine (Dowdle et al., 2003).
Enterovirus-71 vaccines
There have been a variety of effective vaccines designed againstEV-71. A formaldehyde-inactivated whole virus preparation has beenshown to protect mice from encephalomyelitis caused by EV-71infection (Ong et al., 2010). Histopathological examination usingEV-71 specific antibodies revealed an absence of the virus within thebrain stem of immunized mice. Plaque assays using brain stem andspinal cord homogenates confirmed the absence of infectious viruswithin these tissues. Using a unique strategy, transgenic mice weredeveloped to secrete the VP1 capsid protein of EV-71 into milksecretions. When the milk from transgenic animals was fed toneonatal mice, these neonates developed serologically specificantibodies against EV-71 and did not exhibit weight loss whenchallenged with the virus (Chen et al., 2008a). Also, virus-likeparticles, which resemble EV-71 in capsid structure and proteincomposition, have been found to elicit a protective humoral antibodyresponse in animals (Chung et al., 2008). In addition, passive
immunization protected neonatal mice from EV-71 associatedmorbidity when confronted with a lethal dose of virus. A DNA vaccinecoding for VP1 has also been developed (Wu et al., 2001). But incontrast to the aforementioned vaccines, the VP1-based vaccine wasonly partially protective, as shown by a 40% survival rate of miceinoculated with a lethal dose of EV-71 following vaccination.
Coxsackievirus vaccines
As with EV-71, many researchers have developed effectivevaccines against CV, although no clinically available vaccine currentlyexists. Progress has been made using a variety of vaccines strategiesutilizing either DNA plasmids expressing viral proteins, inactivatedvirus, or live attenuated forms of virus. A safe and effective RNAvaccine against CVB3 that produces noninfectious virus has beenrecently produced (Hunziker et al., 2004). Genomic mutation via PCRmutagenesis of the 3CDpro cleavage site present between CVB3proteins 2A and 2B resulted in an RNA viral genome incapable ofproducing infectious virions, yet conferring partial protective immu-nity. RNA-immunized mice exhibited lower viral titers within thepancreas and prolonged survival when challenged with CVB3. RNA-based vaccines are advantageous as compared to DNA vaccines due totheir inability to integrate into host DNA.
Attenuating mutations have also been found in CVB viral capsidproteins, and administering these attenuated viruses was found to beprotective against lethal re-challenge in the pancreas and heart;although the CNS was not examined (Dan and Chantler, 2005).Another successful vaccine in mice designed against CVB3 involvedthe generation of recombinant plasmids expressing capsid proteins.Two independent plasmids encoded the VP1 and VP3 capsid epitopes

301R.E. Rhoades et al. / Virology 411 (2011) 288–305
induced the production of virally specific antibodies following in vivoelectroporation (Park et al., 2009). Although vaccinated micedisplayed a reduction in virally induced heart injury, the inducedantibodies failed to neutralize infectious CVB3 in culture. AttenuatedCVB3 strains have also been used as potential vaccines and mayrepresent the forefront of the field (Kim et al., 2005a). Whether any ofthe aforementioned vaccine candidates are capable of preventing CVpathology within the CNS has yet to be confirmed.
Studies using EVs have also been used as a model system for thedevelopment of innovative vaccine strategies. “High fidelity” RNAviruses isolated upon serial passage in the presence of low concentra-tions of ribavirin might be a general strategy for viral attenuation bydecreasing the level of viral quasispecies (Vignuzzi et al., 2008).Another original approach to vaccine design involved encoding amutant PV that containedhundreds to thousands of under-representedcodon pairs in the PV non-structural proteins (Coleman et al., 2008).This codon-altered PV had the same amino-acid sequence as wild-typePV, yet suffered from a decrease in the virus protein translation rate.Thus, the codon-altered PV could illicit a protective immune responsedespite its attenuation (Wimmer et al., 2009). Both of these approachesgreatly decreased the ability of the attenuated “vaccine strain” to revertto wild-type PV. Importantly both strategies potentially could bedeveloped quickly for emerging RNA viruses, or for other viruseswhereby vaccine development has been deemed problematic.
Gene delivery in the CNS utilizing enterovirus-based vectors
Due to their remarkable ability to infect the CNS, attenuated EVshave been explored for use in gene delivery to cells of the CNS. NovelPV replicons that express green fluorescent protein (GFP) have beenshown to deliver GFP to motor neurons without causing pathogenesis(Jackson et al., 2001). Also, recombinant PVs designed by theGromeier laboratory may be of clinical use for viral gene deliveryinto the CNS, or as oncolytic viruses to target glioblastoma cells andother tumorigenic cells (Goetz et al., 2010). Attenuated CV may alsorepresent an attractive option; our laboratory and others have shownthe feasibility of generating relatively stable recombinant CVsexpressing such gene products as GFP, dsRED, and renilla luciferase(Feuer et al., 2005; Kim et al., 2009). Also with their particular stemcell tropism inmind, attenuated recombinant CVB3may be of value asa viral gene vector specifically for delivery of stem cell modulators,such as transcription factors inducing differentiation, into neural andembryonic stem cells. However, the high number of circulatingantibodies in the population against EVs (Sawyer, 2002) may limittheir use as vectors in vivo; In contrast, in vitro use may be of greatbenefit.
Conclusions and future perspectives
In summary, this review has attempted to cover many of the recentadvances in EV researchwith regard to CNS infection and pathogenesis.EVs are among the most common and medically important humanpathogens, are a frequent cause of CNS disease (Muir and van Loon,1997), and may preferentially cause harm in the very young. Muchremains to be learned regarding factors influencing EV tropism,activation of the immune response following infection, infiltration ofimmune cells into the CNS to combat infection, mechanism ofpathogenesis, and antiviral/vaccine development (Nathanson, 2008).The large number of EV strains circulating in nature hinders the promiseof successful vaccine design against these viruses. The potentialcessation of the globally administered PV vaccine, either due to thesuccessful eradication of poliomyelitis, or due to dwindling WorldHealth Organization resources, may lead to emergence of uncharacter-ized CVs and other related non-polio EVs previously restrained by cross-reacting antibodies generated through yearly immunizations. Theseuncharacterized, yet circulating EV strains with potential CNS tropism
might constitute a new impediment in our control over a devious viralpathogen. Finally, the ability of EVs to persist in the CNS and targetneural stem cells might suggest lasting effects on brain function. Futurestudies might be directed at inspecting possible behavioral alterationsandmemorydysfunction following recovery fromthese challenging, yetsuccessful neurotropic viruses.
Acknowledgments
This workwas supported by the National Institutes of Health (NIH)award R01 NS054108 (to R.F), National Institutes of Mental Health(NIMH) Minority Research Infrastructure Support Program (M-RISP)Faculty Fellow Award R24 MH065515 at San Diego State University(to R.F.), and two Achievement Rewards for College Scientists (ARCS)Foundation Scholarships (to G.T. and J.M.T-G.). No conflicts of interestexist between the subject matter and the authors included in themanuscript.
References
Abzug, M.J., 2004. Presentation, diagnosis, and management of enterovirus infections inneonates. Paediatr. Drugs 6, 1–10.
Agin, H., Apa, H., Unalp, A., Kayserili, E., 2010. Acute disseminated encephalomyelitisassociated with enteroviral infection. Neurosciences (Riyadh.) 15, 46–48.
Agol, V.I., Gmyl, A.P., 2010. Viral security proteins: counteracting host defences. Nat.Rev. Microbiol. 8, 867–878.
Ahn, J., Jee, Y., Seo, I., Yoon, S.Y., Kim, D., Kim, Y.K., Lee, H., 2008. Primary neuronsbecome less susceptible to coxsackievirus B5 following maturation: the correlationwith the decreased level of CAR expression on cell surface. J. Med. Virol. 80 (3),434–440.
Alirezaei, M., Kemball, C.C., Flynn, C.T., Wood, M.R., Whitton, J.L., Kiosses, W.B., 2010.Short-term fasting induces profound neuronal autophagy. Autophagy 6 (6),702–710.
Aliyari, R., Ding, S.W., 2009. RNA-based viral immunity initiated by the Dicer family ofhost immune receptors. Immunol. Rev. 227, 176–188.
Baj, A., Maccari, G., Toniolo, A., 2007. Detection of persistent polioviruses in patientswith the post-polio syndrome. In: Méndez-Vilas, A. (Ed.), Communicating CurrentResearch and Educational Topics and Trends in Applied Microbiology: Formatex,pp. 859–867. edition.
Barral, P.M., Morrison, J.M., Drahos, J., Gupta, P., Sarkar, D., Fisher, P.B., Racaniello, V.R.,2007. MDA-5 is cleaved in poliovirus-infected cells. J. Virol. 81, 3677–3684.
Barral, P.M., Sarkar, D., Fisher, P.B., Racaniello, V.R., 2009. RIG-I is cleaved duringpicornavirus infection. Virology 391, 171–176.
Bergelson, J.M., 2009. Intercellular junctional proteins as receptors and barriers to virusinfection and spread. Cell Host Microbe 5, 517–521.
Blomqvist, S., Savolainen-Kopra, C., Paananen, A., El, B.L., El Maamoon Nasr, E.M.,Firstova, L., Zamiatina, N., Kutateladze, T., Roivainen, M., 2010. Recurrent isolationof poliovirus 3 strains with chimeric capsid protein Vp1 suggests a recombinationhot-spot site in Vp1. Virus Res. 151 (2), 246–251.
Boussadia, O., Niepmann, M., Creancier, L., Prats, A.C., Dautry, F., Jacquemin-Sablon, H.,2003. Unr is required in vivo for efficient initiation of translation from the internalribosome entry sites of both rhinovirus and poliovirus. J. Virol. 77, 3353–3359.
Brahic, M., Bureau, J.F., Michiels, T., 2005. The genetics of the persistent infection anddemyelinating disease caused by Theiler's virus. Annu. Rev. Microbiol. 59 (279–98),279–298.
Brandenburg, B., Lee, L.Y., Lakadamyali, M., Rust, M.J., Zhuang, X., Hogle, J.M., 2007.Imaging poliovirus entry in live cells. PLoS Biol. 5 (7), e183.
Buenz, E.J., Rodriguez, M., Howe, C.L., 2006. Disrupted spatial memory is a consequenceof picornavirus infection. Neurobiol. Dis. 24, 266–273.
Buenz, E.J., Sauer, B.M., Lafrance-Corey, R.G., Deb, C., Denic, A., German, C.L., Howe, C.L.,2009. Apoptosis of hippocampal pyramidal neurons is virus independent in amouse model of acute neurovirulent picornavirus infection. Am. J. Pathol. 175,668–684.
Cameron, C.E., Suk, O.H., Moustafa, I.M., 2010. Expanding knowledge of P3 proteins inthe poliovirus lifecycle. Future Microbiol. 5, 867–881.
Campbell, S.A., Mulvey, M., Mohr, I., Gromeier, M., 2007. Attenuation of herpes simplexvirus neurovirulence with picornavirus cis-acting genetic elements. J. Virol. 81 (2),791–799.
Chang, L.Y., Huang, L.M., Gau, S.S., Wu, Y.Y., Hsia, S.H., Fan, T.Y., Lin, K.L., Huang, Y.C., Lu,C.Y., Lin, T.Y., 2007. Neurodevelopment and cognition in children after enterovirus71 infection. N. Engl. J. Med. 356, 1226–1234.
Chapman, N.M., Kim, K.S., 2008. Persistent coxsackievirus infection: enteroviruspersistence in chronic myocarditis and dilated cardiomyopathy. Curr. Top. Microbiol.Immunol. 323, 275–292.
Chen, H.L., Huang, J.Y., Chu, T.W., Tsai, T.C., Hung, C.M., Lin, C.C., Liu, F.C., Wang, L.C.,Chen, Y.J., Lin, M.F., Chen, C.M., 2008a. Expression of VP1 protein in the milk oftransgenic mice: a potential oral vaccine protects against enterovirus 71 infection.Vaccine 26, 2882–2889.
Chen, T.C., Weng, K.F., Chang, S.C., Lin, J.Y., Huang, P.N., Shih, S.R., 2008b. Developmentof antiviral agents for enteroviruses. J. Antimicrob. Chemother. 62, 1169–1173.

302 R.E. Rhoades et al. / Virology 411 (2011) 288–305
Cheng, M.F., Chen, B.C., Huang, T.S., Hsieh, K.S., Chen, S.N., Liu, Y.C., 2008. Clinicalapplication of reverse-transcription polymerase chain reaction and intravenousimmunoglobulin for enterovirus encephalitis. Jpn J. Infect. Dis. 61, 18–24.
Chung, Y.C., Ho, M.S., Wu, J.C., Chen, W.J., Huang, J.H., Chou, S.T., Hu, Y.C., 2008.Immunization with virus-like particles of enterovirus 71 elicits potent immuneresponses and protects mice against lethal challenge. Vaccine 26, 1855–1862.
Colbere-Garapin, F., Duncan, G., Pavio, N., Pelletier, I., Petit, I., 1998. An approach tounderstanding the mechanisms of poliovirus persistence in infected cells of neuralor non-neural origin. Clin. Diagn. Virol. 9, 107–113.
Coleman, J.R., Papamichail, D., Skiena, S., Futcher, B., Wimmer, E., Mueller, S., 2008. Virusattenuation by genome-scale changes in codon pair bias. Science 320 (5884),1784–1787.
Couderc, T., Guivel-Benhassine, F., Calaora, V., Gosselin, A.S., Blondel, B., 2002. An exvivo murine model to study poliovirus-induced apoptosis in nerve cells. J. Gen.Virol. 83, 1925–1930.
Coyne, C.B., Bergelson, J.M., 2006. Virus-induced Abl and Fyn kinase signals permitcoxsackievirus entry through epithelial tight junctions. Cell 124 (1), 119–131.
Coyne, C.B., Kim, K.S., Bergelson, J.M., 2007. Poliovirus entry into human brainmicrovascular cells requires receptor-induced activation of SHP-2. EMBO J. 26 (17),4016–4028.
Cree, B.C., Bernardini, G.L., Hays, A.P., Lowe, G., 2003. A fatal case of coxsackievirus B4meningoencephalitis. Arch. Neurol. 60, 107–112.
Crotty, S., Andino, R., 2002. Implications of high RNA virus mutation rates: lethalmutagenesis and the antiviral drug ribavirin. Microbes Infect. 4, 1301–1307.
Crotty, S., Maag, D., Arnold, J.J., Zhong, W., Lau, J.Y., Hong, Z., Andino, R., Cameron, C.E.,2000. The broad-spectrum antiviral ribonucleoside ribavirin is an RNA virusmutagen. Nat. Med. 6, 1375–1379.
Crotty, S., Cameron, C.E., Andino, R., 2001. RNA virus error catastrophe: direct moleculartest by using ribavirin. Proc. Natl. Acad. Sci. U. S. A 98, 6895–6900.
Dalwai, A., Ahmad, S., Al-Nakib, W., 2010. Echoviruses are a major cause of asepticmeningitis in infants and young children in Kuwait. Virol. J. 7 (236), 236.
Dan, M., Chantler, J.K., 2005. A genetically engineered attenuated coxsackievirus B3strain protects mice against lethal infection. J. Virol. 79 (14), 9285–9295.
De, M.J., Yaddanapudi, K., Hornig, M., Villar, G., Serge, R., Lipkin, W.I., 2010. Induction ofToll-like receptor 3-mediated immunity during gestation inhibits cortical neuro-genesis and causes behavioral disturbances. MBio. 1, e00176–10.
Deonarain, R., Cerullo, D., Fuse, K., Liu, P.P., Fish, E.N., 2004. Protective role forinterferon-beta in coxsackievirus B3 infection. Circulation 110, 3540–3543.
Desmond, R.A., Accortt, N.A., Talley, L., Villano, S.A., Soong, S.J., Whitley, R.J., 2006.Enteroviral meningitis: natural history and outcome of pleconaril therapy.Antimicrob. Agents Chemother. 50, 2409–2414.
Dierssen, U., Rehren, F., Henke-Gendo, C., Harste, G., Heim, A., 2008. Rapid routinedetection of enterovirus RNA in cerebrospinal fluid by a one-step real-time RT-PCRassay. J. Clin. Virol. 42, 58–64.
Doedens, J.R., Kirkegaard, K., 1995. Inhibition of cellular protein secretion by poliovirusproteins 2B and 3A. EMBO J. 14 (5), 894–907.
Domingo, E., Martin, V., Perales, C., Escarmis, C., 2008. Coxsackieviruses andquasispecies theory: evolution of enteroviruses. Curr. Top. Microbiol. Immunol.323, 3–32.
Dowdle, W.R., De, G.E., Kew, O.M., Pallansch, M.A., Wood, D.J., 2003. Polio eradication:the OPV paradox. Rev. Med. Virol. 13, 277–291.
Eberle, K.E., Nguyen, V.T., Freistadt, M.S., 1995. Low levels of poliovirus replication inprimary human monocytes: possible interactions with lymphocytes. Arch. Virol.140 (12), 2135–2150.
Etchison, D., Milburn, S.C., Edery, I., Sonenberg, N., Hershey, J.W., 1982. Inhibition ofHeLa cell protein synthesis following poliovirus infection correlates with theproteolysis of a 220,000-dalton polypeptide associated with eucaryotic initiationfactor 3 and a cap binding protein complex. J. Biol. Chem. 257 (24), 14806–14810.
Euscher, E., Davis, J., Holzman, I., Nuovo, G.J., 2001. Coxsackie virus infection of theplacenta associated with neurodevelopmental delays in the newborn. Obstet.Gynecol. 98, 1019–1026.
Feuer, R., Whitton, J.L., 2008. Preferential coxsackievirus replication in proliferating/activated cells: implications for virus tropism, persistence, and pathogenesis. Curr.Top. Microbiol. Immunol. 323 (149–73), 149–173.
Feuer, R., Mena, I., Pagarigan, R., Slifka, M.K., Whitton, J.L., 2002. Cell cycle status affectscoxsackievirus replication, persistence, and reactivation in vitro. J. Virol. 76, 4430–4440.
Feuer, R., Mena, I., Pagarigan, R.R., Harkins, S., Hassett, D.E., Whitton, J.L., 2003.Coxsackievirus B3 and the neonatal CNS: the roles of stem cells, developingneurons, and apoptosis in infection, viral dissemination, and disease. Am. J. Pathol.163, 1379–1393.
Feuer, R., Pagarigan, R.R., Harkins, S., Liu, F., Hunziker, I.P., Whitton, J.L., 2005.Coxsackievirus targets proliferating neuronal progenitor cells in the neonatal CNS.J. Neurosci. 25, 2434–2444.
Feuer, R., Ruller, C.M., An, N., Tabor-Godwin, J.M., Rhoades, R.E., Maciejewski, S.,Pagarigan, R.R., Cornell, C.T., Crocker, S.J., Kiosses, W.B., Pham-Mitchell, N.,Campbell, I.L., Whitton, J.L., 2009. Viral persistence and chronic immunopathologyin the adult central nervous system following Coxsackievirus infection during theneonatal period. J. Virol. 83, 9356–9369.
Fitzgerald, K.D., Semler, B.L., 2009. Bridging IRES elements in mRNAs to the eukaryotictranslation apparatus. Biochim. Biophys. Acta 1789, 518–528.
Freistadt, M.S., Eberle, K.E., 1996. Correlation between poliovirus type 1 Mahoneyreplication in blood cells and neurovirulence. J. Virol. 70 (9), 6486–6492.
Freistadt, M.S., Fleit, H.B., Wimmer, E., 1993. Poliovirus receptor on human blood cells: apossible extraneural site of poliovirus replication. Virology 195 (2), 798–803.
Freistadt, M.S., Vaccaro, J.A., Eberle, K.E., 2007. Biochemical characterization of thefidelity of poliovirus RNA-dependent RNA polymerase. Virol. J. 4, 44.
Fujita, K., Krishnakumar, S.S., Franco, D., Paul, A.V., London, E., Wimmer, E., 2007.Membrane topography of the hydrophobic anchor sequence of poliovirus 3A and3AB proteins and the functional effect of 3A/3AB membrane association upon RNAreplication. Biochemistry 46 (17), 5185–5199.
Gamarnik, A.V., Andino, R., 1998. Switch from translation to RNA replication in apositive-stranded RNA virus. Genes Dev. 12 (15), 2293–2304.
Girard, S., Couderc, T., Destombes, J., Thiesson, D., Delpeyroux, F., Blondel, B., 1999.Poliovirus induces apoptosis in the mouse central nervous system. J. Virol. 73,6066–6072.
Gitlin, L., Andino, R., 2003. Nucleic acid-based immune system: the antiviral potential ofmammalian RNA silencing. J. Virol. 77, 7159–7165.
Gitlin, L., Karelsky, S., Andino, R., 2002. Short interfering RNA confers intracellularantiviral immunity in human cells. Nature 418, 430–434.
Goetz, C., Everson, R.G., Zhang, L.C., Gromeier, M., 2010. MAPK signal-integrating kinasecontrols cap-independent translation and cell type-specific cytotoxicity of anoncolytic poliovirus. Mol. Ther. 18, 1937–1946.
Goodfellow, I., Chaudhry, Y., Richardson, A., Meredith, J., Almond, J.W., Barclay, W.,Evans, D.J., 2000. Identification of a cis-acting replication element within thepoliovirus coding region. J. Virol. 74 (10), 4590–4600.
Gorbea, C., Makar, K.A., Pauschinger, M., Pratt, G., Bersola, J.L., Varela, J., David, R.M.,Banks, L., Huang, C.H., Li, H., Schultheiss, H.P., Towbin, J.A., Vallejo, J.G., Bowles, N.E.,2010. A role for Toll-like receptor 3 variants in host susceptibility to enteroviralmyocarditis and dilated cardiomyopathy. J. Biol. Chem. 285, 23208–23223.
Gromeier, M., Wimmer, E., 1998. Mechanism of injury-provoked poliomyelitis. J. Virol.72, 5056–5060.
Gromeier, M., Lu, H.H., Wimmer, E., 1995. Mouse neuropathogenic poliovirus strainscause damage in the central nervous system distinct from poliomyelitis. Microb.Pathog. 18 (4), 253–267.
Gromeier, M., Alexander, L., Wimmer, E., 1996. Internal ribosomal entry sitesubstitution eliminates neurovirulence in intergeneric poliovirus recombinants.Proc. Natl Acad. Sci. USA 93 (6), 2370–2375 %19.
Gromeier, M., Bossert, B., Arita, M., Nomoto, A., Wimmer, E., 1999. Dual stem loopswithin the poliovirus internal ribosomal entry site control neurovirulence. J. Virol.73 (2), 958–964.
Gromeier,M., Solecki,D., Patel,D.D.,Wimmer, E., 2000. Expression of thehumanpoliovirusreceptor/CD155geneduringdevelopment of the central nervous system: implicationsfor the pathogenesis of poliomyelitis. Virology 273 (2), 248–257.
Guest, S., Pilipenko, E., Sharma, K., Chumakov, K., Roos, R.P., 2004. Molecularmechanisms of attenuation of the Sabin strain of poliovirus type 3. J. Virol. 78(20), 11097–11107.
Gupta, S., Fernandez, D., Siddiqui, A., Tong, W.C., Pohl, K., Jungbluth, H., 2010. Extensivewhite matter abnormalities associated with neonatal Parechovirus (HPeV)infection. Eur. J. Paediatr. Neurol. 14, 531–534.
Haddad, A., Nokhbeh, M.R., Alexander, D.A., Dawe, S.J., Grise, C., Gulzar, N., Dimock, K.,2004. Binding to decay-accelerating factor is not required for infection of humanleukocyte cell lines by enterovirus 70. J. Virol. 78 (6), 2674–2681.
Hagino-Yamagishi, K., Nomoto, A., 1989. In vitro construction of poliovirus defectiveinterfering particles. J. Virol. 63 (12), 5386–5392.
Han, J., Ma, X.J., Wan, J.F., Liu, Y.H., Han, Y.L., Chen, C., Tian, C., Gao, C., Wang, M., Dong, X.P.,2010. Longpersistenceof EV71 specific nucleotides in respiratory and feces samples ofthe patients with Hand–Foot–Mouth Disease after recovery. BMC Infect. Dis. 10, 178.
Harvala, H., Simmonds, P., 2009. Human parechoviruses: biology, epidemiology andclinical significance. J. Clin. Virol. 45, 1–9.
Herold, J., Andino, R., 2001. Poliovirus RNA replication requires genome circularizationthrough a protein–protein bridge. Mol. Cell 7 (3), 581–591.
Honda, Y., Hosoya, M., Ishii, T., Shigeta, S., Suzuki, H., 1994. Effect of ribavirin onsubacute sclerosing panencephalitis virus infections in hamsters. Antimicrob.Agents Chemother. 38, 653–655.
Honda, T., Saitoh, H., Masuko, M., Katagiri-Abe, T., Tominaga, K., Kozakai, I., Kobayashi,K., Kumanishi, T., Watanabe, Y.G., Odani, S., Kuwano, R., 2000. The coxsackievirus–adenovirus receptor protein as a cell adhesion molecule in the developing mousebrain. Brain Res. Mol. Brain Res. 77, 19–28.
Hosking, M.P., Lane, T.E., 2010. The role of chemokines during viral infection of the CNS.PLoS Pathog. 6, e1000937.
Hosoya, M., Shigeta, S., Nakamura, K., De, C.E., 1989. Inhibitory effect of selected antiviralcompounds on measles (SSPE) virus replication in vitro. Antivir. Res. 12, 87–97.
Hosoya, M., Shigeta, S., Mori, S., Tomoda, A., Shiraishi, S., Miike, T., Suzuki, H., 2001.High-dose intravenous ribavirin therapy for subacute sclerosing panencephalitis.Antimicrob. Agents Chemother. 45, 943–945.
Hotta, Y., Honda, T., Naito, M., Kuwano, R., 2003. Developmental distribution ofcoxsackie virus and adenovirus receptor localized in the nervous system. Brain Res.Dev. Brain Res. 143, 1–13.
Huang, M.C., Wang, S.M., Hsu, Y.W., Lin, H.C., Chi, C.Y., Liu, C.C., 2006. Long-termcognitive and motor deficits after enterovirus 71 brainstem encephalitis inchildren. Pediatrics 118, e1785–e1788.
Huang, S.C., Chang, C.L., Wang, P.S., Tsai, Y., Liu, H.S., 2009. Enterovirus 71-inducedautophagy detected in vitro and in vivo promotes viral replication. J. Med. Virol. 81(7), 1241–1252.
Hughes, S.A., Thaker, H.M., Racaniello, V.R., 2003. Transgenic mouse model forechovirus myocarditis and paralysis. Proc. Natl. Acad. Sci. U. S. A 100, 15906–15911.
Hunter, P., 2008. Viral vigilance. New surveillance strategies and methods help toidentify dangerous pathogens earlier: a prerequisite for efficient countermeasures.EMBO Rep. 9, 948–950.
Hunziker, I.P., Harkins, S., Feuer, R., Cornell, C.T., Whitton, J.L., 2004. Generation andanalysis of an RNA vaccine that protects against coxsackievirus B3 challenge.Virology 330, 196–208.

303R.E. Rhoades et al. / Virology 411 (2011) 288–305
Hymas, W.C., Aldous, W.K., Taggart, E.W., Stevenson, J.B., Hillyard, D.R., 2008.Description and validation of a novel real-time RT-PCR enterovirus assay. Clin.Chem. 54, 406–413.
Ida-Hosonuma, M., Iwasaki, T., Yoshikawa, T., Nagata, N., Sato, Y., Sata, T., Yoneyama, M.,Fujita, T., Taya, C., Yonekawa, H., Koike, S., 2005. The alpha/beta interferon responsecontrols tissue tropism and pathogenicity of poliovirus. J. Virol. 79, 4460–4469.
Ireland, D.D., Stohlman, S.A., Hinton, D.R., Kapil, P., Silverman, R.H., Atkinson, R.A.,Bergmann, C.C., 2009. RNase L mediated protection from virus induced demyelin-ation. PLoS Pathog. 5, e1000602.
Ishii, T., Hosoya, M., Mori, S., Shigeta, S., Suzuki, H., 1996. Effective ribavirinconcentration in hamster brains for antiviral chemotherapy for subacute sclerosingpanencephalitis. Antimicrob. Agents Chemother. 40, 241–243.
Jackson, C.A., Cobbs, C., Peduzzi, J.D., Novak, M., Morrow, C.D., 2001. Repetitive intrathecalinjections of poliovirus replicons result in gene expression in neurons of the centralnervous system without pathogenesis. Hum. Gene Ther. 12 (15), 1827–1841.
Jackson, W.T., Giddings Jr., T.H., Taylor, M.P., Mulinyawe, S., Rabinovitch, M., Kopito,R.R., Kirkegaard, K., 2005. Subversion of cellular autophagosomal machinery byRNA viruses. PLoS Biol. 3 (5), e156.
Jegouic, S., Joffret, M.L., Blanchard, C., Riquet, F.B., Perret, C., Pelletier, I., Colbere-Garapin, F., Rakoto-Andrianarivelo, M., Delpeyroux, F., 2009. Recombinationbetween polioviruses and co-circulating Coxsackie A viruses: role in the emergenceof pathogenic vaccine-derived polioviruses. PLoS Pathog. 5 (5), e1000412.
Jeulin, H., Venard, V., Carapito, D., Finance, C., Kedzierewicz, F., 2009. Effective ribavirinconcentration in mice brain using cyclodextrin as a drug carrier: evaluation in ameasles encephalitis model. Antivir. Res. 81, 261–266.
Kato, H., Takeuchi, O., Sato, S., Yoneyama, M., Yamamoto, M., Matsui, K., Uematsu, S.,Jung, A., Kawai, T., Ishii, K.J., Yamaguchi, O., Otsu, K., Tsujimura, T., Koh, C.S., Reis eSousa, Matsuura, Y., Fujita, T., Akira, S., 2006. Differential roles of MDA5 and RIG-Ihelicases in the recognition of RNA viruses. Nature 441, 101–105.
Kauder, S.E., Racaniello, V.R., 2004. Poliovirus tropism and attenuation are determinedafter internal ribosome entry. J. Clin. Invest. 113, 1743–1753.
Kauder, S., Kan, S., Racaniello, V.R., 2006. Age-dependent poliovirus replication in themouse central nervous system is determined by internal ribosome entry site-mediated translation. J. Virol. 80, 2589–2595.
Kemball, C.C., Harkins, S., Whitmire, J.K., Flynn, C.T., Feuer, R., Whitton, J.L., 2009.Coxsackievirus B3 inhibits antigen presentation in vivo, exerting a profound andselective effect on the MHC class I pathway. PLoS Pathog. 5, e1000618.
Kempf, B.J., Barton, D.J., 2008. Poliovirus 2A(Pro) increases viral mRNA and polysomestability coordinately in time with cleavage of eIF4G. J. Virol. 82 (12), 5847–5859.
Kim, J.Y., Jeon, E.S., Lim, B.K., Kim, S.M., Chung, S.K., Kim, J.M., Park, S.I., Jo, I., Nam, J.H.,2005a. Immunogenicity of a DNA vaccine for coxsackievirus B3 in mice: protectiveeffects of capsid proteins against viral challenge. Vaccine 23, 1672–1679.
Kim, K.S., Tracy, S., Tapprich, W., Bailey, J., Lee, C.K., Kim, K., Barry, W.H., Chapman, N.M.,2005b. 5′-Terminal deletions occur in coxsackievirus B3 during replication inmurine hearts and cardiac myocyte cultures and correlate with encapsidation ofnegative-strand viral RNA. J. Virol. 79, 7024–7041.
Kim, K.S., Chapman, N.M., Tracy, S., 2008. Replication of coxsackievirus B3 in primarycell cultures generates novel viral genome deletions. J. Virol. 82, 2033–2037.
Kim, Y.J., Yun, S.H., Lim, B.K., Park, K.B., Na, H.N., Jeong, S.Y., Kim, D.S., Cho, Y.J., Jeon, E.S.,Nam, J.H., 2009. Systemic analysis of a novel coxsackievirus gene delivery system ina mouse model. J. Microbiol. Biotechnol. 19 (3), 307–313.
Kitamura, N., Semler, B.L., Rothberg, P.G., Larsen, G.R., Adler, C.J., Dorner, A.J., Emini, E.A.,Hanecak, R., Lee, J.J., van der Werf, S., Anderson, C.W., Wimmer, E., 1981. Primarystructure, gene organization and polypeptide expression of poliovirus RNA. Nature291 (5816), 547–553.
Klingel, K., Hohenadl, C., Canu, A., Albrecht, M., Seemann, M., Mall, G., Kandolf, R., 1992.Ongoing enterovirus-induced myocarditis is associated with persistent heartmuscle infection: quantitative analysis of virus replication, tissue damage, andinflammation. Proc. Natl. Acad. Sci. U. S. A 89, 314–318.
Kotla, S., Peng, T., Bumgarner, R.E., Gustin, K.E., 2008. Attenuation of the type I interferonresponse in cells infected with human rhinovirus. Virology 374, 399–410.
Kung, C.M., King, C.C., Lee, C.N., Huang, L.M., Lee, P.I., Kao, C.L., Kung, C.M., King, C.C., Lee,C.N., Huang, L.M., Lee, P.I., Kao, C.L., 2007. Differences in replication capacitybetween enterovirus 71 isolates obtained from patients with encephalitis andthose obtained from patients with herpangina in Taiwan. J. Med. Virol. 79, 60–68.
Kuss, S.K., Etheredge, C.A., Pfeiffer, J.K., 2008. Multiple host barriers restrict poliovirustrafficking in mice. PLoS Pathog. 4 (6), e1000082.
Lancaster, K.Z., Pfeiffer, J.K., 2010. Limited trafficking of a neurotropic virus throughinefficient retrograde axonal transport and the type I interferon response. PLoSPathog. 6 (3), e1000791.
Lee, T.C., Guo, H.R., Su, H.J., Yang, Y.C., Chang, H.L., Chen, K.T., 2009. Diseases caused byenterovirus 71 infection. Pediatr. Infect. Dis. J. 28, 904–910.
Lei, X., Liu, X., Ma, Y., Sun, Z., Yang, Y., Jin, Q., He, B., Wang, J., 2010. The 3C protein ofenterovirus 71 inhibits retinoid acid-inducible gene I-mediated interferon regulatoryfactor 3 activation and type I interferon responses. J. Virol. 84, 8051–8061.
Leland, D.S., Ginocchio, C.C., 2007. Role of cell culture for virus detection in the age oftechnology. Clin. Microbiol. Rev. 20, 49–78.
Lewthwaite, P., Perera, D., How, O.M., Last, A., Kumar, R., Desai, A., Begum, A., Ravi, V.,Shankar, M.V., Hooi, T.P., Cardosa, M.J., Solomon, T., 2010. Enterovirus 75encephalitis in children, southern India. Emerg. Infect. Dis. 16, 1780–1782.
Li, Z.H., Li, C.M., Ling, P., Shen, F.H., Chen, S.H., Liu, C.C., Yu, C.K., Chen, S.H., 2008.Ribavirin reduces mortality in enterovirus 71-infected mice by decreasing viralreplication. J. Infect. Dis. 197, 854–857.
Lin, T.Y., Hsia, S.H., Huang, Y.C., Wu, C.T., Chang, L.Y., 2003. Proinflammatory cytokinereactions in enterovirus 71 infections of the central nervous system. Clin. Infect. Dis.36, 269–274.
Lin, J.Y., Li, M.L., Shih, S.R., 2009a. Far upstream element binding protein 2 interacts withenterovirus 71 internal ribosomal entry site and negatively regulates viral translation.Nucleic Acids Res. 37, 47–59.
Lin, Y.W., Chang, K.C., Kao, C.M., Chang, S.P., Tung, Y.Y., Chen, S.H., 2009b. Lymphocyteand antibody responses reduce enterovirus 71 lethality in mice by decreasingtissue viral loads. J. Virol. 83, 6477–6483.
Lipton, H.L., Kumar, A.S., Trottier, M., 2005. Theiler's virus persistence in the centralnervous system of mice is associated with continuous viral replication and adifference in outcome of infection of infiltrating macrophages versus oligoden-drocytes. Virus Res. 111, 214–223.
Liu, S.C., Lee, P.I., Lee, C.Y., Wang, J.D., Chiang, B.L., Chou, M.C., 2005. Different cytokinelevels in enterovirus meningitis and encephalitis. Infect. Dis. Clin. Pract. 13.
Madan, V., Redondo, N., Carrasco, L., 2010. Cell permeabilization by poliovirus 2Bviroporin triggers bystander permeabilization in neighbouring cells through amechanism involving gap junctions. Cell. Microbiol. 12 (8), 1144–1157.
Malathi, K., Dong, B., Gale Jr., M., Silverman, R.H., 2007. Small self-RNA generated byRNase L amplifies antiviral innate immunity. Nature 448, 816–819.
Marcotte, L.L., Wass, A.B., Gohara, D.W., Pathak, H.B., Arnold, J.J., Filman, D.J., Cameron, C.E.,Hogle, J.M., 2007. Crystal structure of poliovirus 3CD protein: virally encoded proteaseand precursor to the RNA-dependent RNA polymerase. J. Virol. 81 (7), 3583–3596.
Matsumoto, M., Seya, T., 2008. TLR3: interferon induction by double-stranded RNAincluding poly(I:C). Adv. Drug Deliv. Rev. 60, 805–812.
Mena, I., Perry, C.M., Harkins, S., Rodriguez, F., Gebhard, J., Whitton, J.L., 1999. The role ofB lymphocytes in coxsackievirus B3 infection. Am. J. Pathol. 155, 1205–1215.
Merl, S., Wessely, R., 2007. Anti-coxsackieviral efficacy of RNA interference is highlydependent on genomic target selection and emergence of escape mutants.Oligonucleotides 17, 44–53.
Merl, S., Michaelis, C., Jaschke, B., Vorpahl, M., Seidl, S., Wessely, R., 2005. Targeting 2Aprotease by RNA interference attenuates coxsackieviral cytopathogenicity andpromotes survival in highly susceptible mice. Circulation 111, 1583–1592.
Michos, A.G., Syriopoulou, V.P., Hadjichristodoulou, C., Daikos, G.L., Lagona, E., Douridas,P., Mostrou, G., Theodoridou, M., 2007. Aseptic meningitis in children: analysis of506 cases. PLoS ONE 2, e674.
Minami, K., Tsuda, Y., Maeda, H., Yanagawa, T., Izumi, G., Yoshikawa, N., 2004. Acutetransverse myelitis caused by Coxsackie virus B5 infection. J. Paediatr. Child Health40, 66–68.
Mirand, A., Bailly, J.L., Henquell, C., Peigue-Lafeuille, H., 2008. Rapid enterovirusgenotyping in cerebrospinal fluids: a two-year prospective study in a virologylaboratory setting. Pathol. Biol. Paris. 56, 471–481.
Misbah, S.A., Spickett, G.P., Ryba, P.C., Hockaday, J.M., Kroll, J.S., Sherwood, C., Kurtz, J.B.,Moxon, E.R., Chapel, H.M., 1992. Chronic enteroviral meningoencephalitis inagammaglobulinemia: case report and literature review. J. Clin. Immunol. 12,266–270.
MMWR, 2010. Outbreaks following wild poliovirus importations — Europe, Africa, andAsia, January 2009–September 2010. MMWR Morb. Mortal. Wkly. Rep. 59,1393–1399.
Muir, P., van Loon, A.M., 1997. Enterovirus infections of the central nervous system.Intervirology 40, 153–166.
Nagata, N., Iwasaki, T., Ami, Y., Tano, Y., Harashima, A., Suzaki, Y., Sato, Y., Hasegawa, H.,Sata, T., Miyamura, T., Shimizu, H., 2004. Differential localization of neuronssusceptible to enterovirus 71 and poliovirus type 1 in the central nervous system ofcynomolgus monkeys after intravenous inoculation. J. Gen. Virol. 85, 2981–2989.
Nathanson, N., 2008. The pathogenesis of poliomyelitis: what we don't know. Adv.Virus Res. 71 (1–50), 1–50.
Nishimura, Y., Shimojima, M., Tano, Y., Miyamura, T., Wakita, T., Shimizu, H., 2009.Human P-selectin glycoprotein ligand-1 is a functional receptor for enterovirus 71.Nat. Med. 15 (7), 794–797.
Noda, S., Aguirre, S.A., Bitmansour, A., Brown, J.M., Sparer, T.E., Huang, J., Mocarski, E.S.,2006. Cytomegalovirus MCK-2 controls mobilization and recruitment of myeloidprogenitor cells to facilitate dissemination. Blood 107, 30–38.
Novak, J.E., Kirkegaard, K., 1991. Improved method for detecting poliovirus negativestrands used to demonstrate specificity of positive-strand encapsidation and theratio of positive to negative strands in infected cells. J. Virol. 65 (6), 3384–3387.
Oberste, M.S., Maher, K., Pallansch, M.A., 2002. Molecular phylogeny and proposedclassification of the simian picornaviruses. J. Virol. 76, 1244–1251.
Oh, H.S., Pathak, H.B., Goodfellow, I.G., Arnold, J.J., Cameron, C.E., 2009. Insight intopoliovirus genome replication and encapsidation obtained from studies of 3B–3Ccleavage site mutants. J. Virol. 83 (18), 9370–9387.
Ohka, S., Matsuda, N., Tohyama, K., Oda, T., Morikawa, M., Kuge, S., Nomoto, A., 2004.Receptor (CD155)-dependent endocytosis of poliovirus and retrograde axonaltransport of the endosome. J. Virol. 78 (13), 7186–7198.
Ohka, S., Sakai, M., Bohnert, S., Igarashi, H., Deinhardt, K., Schiavo, G., Nomoto, A., 2009.Receptor-dependent and -independent axonal retrograde transport of poliovirus inmotor neurons. J. Virol. 83 (10), 4995–5004.
Oleszak, E.L., Chang, J.R., Friedman, H., Katsetos, C.D., Platsoucas, C.D., 2004. Theiler'svirus infection: a model for multiple sclerosis. Clin. Microbiol. Rev. 17, 174–207.
Olson, J.K., Ercolini, A.M., Miller, S.D., 2005. A virus-induced molecular mimicry modelof multiple sclerosis. Curr. Top. Microbiol. Immunol. 296 (39–53), 39–53.
Ong, K.C., Devi, S., Cardosa, M.J., Wong, K.T., 2010. Formaldehyde-inactivated whole-virus vaccine protects a murine model of enterovirus 71 encephalomyelitis againstdisease. J. Virol. 84, 661–665.
Ooi, M.H., Wong, S.C., Lewthwaite, P., Cardosa, M.J., Solomon, T., 2010. Clinical features,diagnosis, and management of enterovirus 71. Lancet Neurol. 9, 1097–1105.
Ornoy, A., Tenenbaum, A., 2006. Pregnancy outcome following infections by coxsackie,echo, measles, mumps, hepatitis, polio and encephalitis viruses. Reprod. Toxicol.21, 446–457.

304 R.E. Rhoades et al. / Virology 411 (2011) 288–305
Papon, L., Oteiza, A., Imaizumi, T., Kato, H., Brocchi, E., Lawson, T.G., Akira, S., Mechti, N.,2009. The viral RNA recognition sensor RIG-I is degraded during encephalomyo-carditis virus (EMCV) infection. Virology 393, 311–318.
Park, N., Katikaneni, P., Skern, T., Gustin, K.E., 2008. Differential targeting of nuclear porecomplex proteins in poliovirus-infected cells. J. Virol. 82, 1647–1655.
Park, J.H., Kim, D.S., Cho, Y.J., Kim, Y.J., Jeong, S.Y., Lee, S.M., Cho, S.J., Yun, C.W., Jo, I.,Nam, J.H., 2009. Attenuation of coxsackievirus B3 by VP2 mutation and itsapplication as a vaccine against virus-induced myocarditis and pancreatitis.Vaccine 27, 1974–1983.
Park, N., Skern, T., Gustin, K.E., 2010. Specific cleavage of the nuclear pore complexprotein Nup62 by a viral protease. J. Biol. Chem. 285, 28796–28805.
Patel, K.P., Coyne, C.B., Bergelson, J.M., 2009. Dynamin- and lipid raft-dependent entryof decay-accelerating factor (DAF)-binding and non-DAF-binding coxsackievirusesinto nonpolarized cells. J. Virol. 83 (21), 11064–11077.
Paul, A.V., van Boom, J.H., Filippov, D., Wimmer, E., 1998. Protein-primed RNA synthesisby purified poliovirus RNA polymerase. Nature 393 (6682), 280–284.
Paul, A.V., Peters, J., Mugavero, J., Yin, J., van Boom, J.H., Wimmer, E., 2003. Biochemicaland genetic studies of the VPg uridylylation reaction catalyzed by the RNApolymerase of poliovirus. J. Virol. 77 (2), 891–904.
Pedersen, I.M., Cheng, G., Wieland, S., Volinia, S., Croce, C.M., Chisari, F.V., David, M.,2007. Interferon modulation of cellular microRNAs as an antiviral mechanism.Nature 449, 919–922.
Pelletier, J., Sonenberg, N., 1988. Internal initiation of translation of eukaryotic mRNAdirected by a sequence derived from poliovirus RNA. Nature 334 (6180), 320–325.
Pelletier, I., Saulnier, A., Brisac, C., Jegouic, S., Vabret, N., Tangy, F., Blondel, B., Colbere-Garapin, F., 2010. Enhanced gene silencing in cells cured of persistent virusinfection by RNA interference. J. Virol. 84, 6880–6885.
Pevear, D.C., Tull, T.M., Seipel, M.E., Groarke, J.M., 1999. Activity of pleconaril againstenteroviruses. Antimicrob. Agents Chemother. 43, 2109–2115.
Pfeffer, S., Sewer, A., Lagos-Quintana, M., Sheridan, R., Sander, C., Grasser, F.A., van Dyk,L.F., Ho, C.K., Shuman, S., Chien, M., Russo, J.J., Ju, J., Randall, G., Lindenbach, B.D.,Rice, C.M., Simon, V., Ho, D.D., Zavolan, M., Tuschl, T., 2005. Identification ofmicroRNAs of the herpesvirus family. Nat. Meth. 2, 269–276.
Pfeiffer, J.K., 2010. Innate host barriers to viral trafficking and population diversity:lessons learned from poliovirus. Adv. Virus Res. 77 (85–118), 85–118.
Pfeiffer, J.K., Kirkegaard, K., 2003. A single mutation in poliovirus RNA-dependent RNApolymerase confers resistance to mutagenic nucleotide analogs via increasedfidelity. Proc. Natl Acad. Sci. USA 100, 7289–7294.
Pfeiffer, J.K., Kirkegaard, K., 2006. Bottleneck-mediated quasispecies restriction duringspread of an RNA virus from inoculation site to brain. Proc. Natl Acad. Sci. USA 103(14), 5520–5525.
Pilipenko, E.V., Pestova, T.V., Kolupaeva, V.G., Khitrina, E.V., Poperechnaya, A.N., Agol, V.I.,Hellen, C.U., 2000. A cell cycle-dependent protein serves as a template-specifictranslation initiation factor. Genes Dev. 14, 2028–2045.
Rahimi, P., Tabatabaie, H., Gouya, M.M., Zahraie, M., Mahmudi, M., Ziaie, A., Rad, K.S.,Shahmahmudi, S., Musavi, T., Azad, T.M., Nategh, R., 2007. Characterization ofmutations in the VP(1) region of Sabin strain type 1 polioviruses isolated fromvaccine-associated paralytic poliomyelitis cases in Iran. J. Clin. Virol. 39 (4),304–307.
Ramsingh, A.I., 2008. CVB-induced pancreatitis and alterations in gene expression. Curr.Top. Microbiol. Immunol. 323 (241–58), 241–258.
Rantakallio, P., Jones, P., Moring, J., Von, W.L., 1997. Association between centralnervous system infections during childhood and adult onset schizophrenia andother psychoses: a 28-year follow-up. Int. J. Epidemiol. 26, 837–843.
Ren, R., Racaniello, V.R., 1992. Poliovirus spreads from muscle to the central nervoussystem by neural pathways. J. Infect. Dis. 166 (4), 747–752.
Ricour, C., Delhaye, S., Hato, S.V., Olenyik, T.D., Michel, B., van Kuppeveld, F.J., Gustin, K.E.,Michiels, T., 2009. InhibitionofmRNAexport anddimerizationof interferon regulatoryfactor 3 by Theiler's virus leader protein. J. Gen. Virol. 90, 177–186.
Rodriguez, M., 2007. Effectors of demyelination and remyelination in the CNS:implications for multiple sclerosis. Brain Pathol. 17, 219–229.
Rodriguez, M., Leibowitz, J.L., Lampert, P.W., 1983. Persistent infection of oligoden-drocytes in Theiler's virus-induced encephalomyelitis. Ann. Neurol. 13, 426–433.
Romero, J.R., 1999. Reverse-transcription polymerase chain reaction detection of theenteroviruses. Arch. Pathol. Lab. Med. 123, 1161–1169.
Romero, J.R., 2008. Pediatric group B coxsackievirus infections. Curr. Top. Microbiol.Immunol. 323 (223–39), 223–239.
Rotbart, H.A., 1990. Diagnosis of enteroviral meningitis with the polymerase chainreaction. J. Pediatr. 117, 85–89.
Roussarie, J.P., Ruffie, C., Brahic, M., 2007. The role of myelin in Theiler's viruspersistence in the central nervous system. PLoS Pathog. 3, e23.
Sabin, A.B., 1957. Properties and behavior of orally administered attenuated poliovirusvaccine. J. Am. Med. Assoc. 164, 1216–1223.
Salk, J.E., Krech, U., Youngner, J.S., Bennett, B.L., Lewis, L.J., Bazeley, P.L., 1954.Formaldehyde treatment and safety testing of experimental poliomyelitis vaccines.Am. J. Public Health Nations Health 44, 563–570.
Sawyer, M.H., 2002. Enterovirus infections: diagnosis and treatment. Semin. Pediatr.Infect. Dis. 13, 40–47.
Schein, C.H., Oezguen, N., van der Heden van Noort, G.J., Filippov, D.V., Paul, A., Kumar,E., Braun,W., 2010. NMR solution structure of poliovirus uridylyated peptide linkedto the genome (VPgpU). Peptides 31, 1441–1448.
Schilthuizen, C., Berenschot, H.W., Levin, M.D., 2010. Enteroviral encephalitis in apatient with a marginal zone lymphomatreated with rituximab. Neth. J. Med. 68,221–223.
Schmidtke, M., Hammerschmidt, E., Schuler, S., Zell, R., Birch-Hirschfeld, E., Makarov, V.A.,Riabova, O.B., Wutzler, P., 2005. Susceptibility of coxsackievirus B3 laboratory strains
and clinical isolates to the capsid function inhibitor pleconaril: antiviral studies withvirus chimeras demonstrate the crucial role of amino acid 1092 in treatment. J.Antimicrob. Chemother. 56, 648–656.
Schmidtke, M., Wutzler, P., Zieger, R., Riabova, O.B., Makarov, V.A., 2009. New pleconariland [(biphenyloxy)propyl]isoxazole derivatives with substitutions in the central ringexhibit antiviral activity against pleconaril-resistant coxsackievirus B3. Antivir. Res.81, 56–63.
Servais, S., Caers, J., Warling, O., Frusch, N., Baron, F., De, P.B., Beguin, Y., 2010.Enteroviral meningoencephalitis as complication of Rituximab therapy in a patienttreated for diffuse large B-cell lymphoma. Br. J. Haematol. 150, 379–381.
Sharma, R., Raychaudhuri, S., Dasgupta, A., 2004. Nuclear entry of poliovirus protease–polymerase precursor 3CD: implications for host cell transcription shut-off.Virology 320 (2), 195–205.
Shih, S.R., Weng, K.F., Stollar, V., Li, M.L., 2008. Viral protein synthesis is required forEnterovirus 71 to induce apoptosis in human glioblastoma cells. J. Neurovirol. 14 (1),53–61.
Simonsen, A., Cumming, R.C., Brech, A., Isakson, P., Schubert, D.R., Finley, K.D., 2008.Promoting basal levels of autophagy in the nervous system enhances longevity andoxidant resistance in adult Drosophila. Autophagy 4 (2), 176–184.
Slifka, M.K., Pagarigan, R., Mena, I., Feuer, R., Whitton, J.L., 2001. Using recombinantcoxsackievirus B3 to evaluate the induction and protective efficacy of CD8+ T cellsduring picornavirus infection. J. Virol. 75, 2377–2387.
Solomon, T., Willison, H., 2003. Infectious causes of acute flaccid paralysis. Curr. Opin.Infect. Dis. 16, 375–381.
Solomon, T., Lewthwaite, P., Perera, D., Cardosa, M.J., McMinn, P., Ooi, M.H., 2010.Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect.Dis. 10, 778–790.
Steil, B.P., Barton, D.J., 2009. Cis-active RNA elements (CREs) and picornavirus RNAreplication. Virus Res. 139 (2), 240–252.
Suhy, D.A., Giddings Jr., T.H., Kirkegaard, K., 2000. Remodeling the endoplasmicreticulum by poliovirus infection and by individual viral proteins: an autophagy-like origin for virus-induced vesicles. J. Virol. 74 (19), 8953–8965.
Suvisaari, J., Mautemps, N., Haukka, J., Hovi, T., Lonnqvist, J., 2003. Childhood central nervoussystem viral infections and adult schizophrenia. Am. J. Psychiatry 160, 1183–1185.
Tabor-Godwin, J.M., Ruller, C.M., Bagalso, N., An, N., Pagarigan, R.R., Harkins, S., Gilbert,P.E., Kiosses, W.B., Gude, N.A., Cornell, C.T., Doran, K.S., Sussman, M.A., Whitton, J.L.,Feuer, R., 2010. A novel population of myeloid cells responding to coxsackievirusinfection assists in the dissemination of virus within the neonatal CNS. J. Neurosci.30, 8676–8691.
Tam, P.E., Messner, R.P., 1999. Molecular mechanisms of coxsackievirus persistence inchronic inflammatory myopathy: viral RNA persists through formation of a double-stranded complex without associated genomic mutations or evolution. J. Virol. 73,10113–10121.
Tan, E.L., Tan, T.M., Tak, K.C.V., Poh, C.L., 2007. Inhibition of enterovirus 71 in virus-infected mice by RNA interference. Mol. Ther. 15, 1931–1938.
Tan, E.L., Wong, A.P., Poh, C.L., 2010. Development of potential antiviral strategy againstcoxsackievirus B4. Virus Res. 150, 85–92.
Tapparel, C., Junier, T., Gerlach, D., Van-Belle, S., Turin, L., Cordey, S., Muhlemann, K.,Regamey, N., Aubert, J.D., Soccal, P.M., Eigenmann, P., Zdobnov, E., Kaiser, L., 2009.New respiratory enterovirus and recombinant rhinoviruses among circulatingpicornaviruses. Emerg. Infect. Dis. 15, 719–726.
Tebruegge, M., Curtis, N., 2009. Enterovirus infections in neonates. Semin. Fetal NeonatalMed. 14, 222–227.
Tung, W.H., Lee, I.T., Hsieh, H.L., Yang, C.M., 2010. EV71 induces COX-2 expression viac-Src/PDGFR/PI3K/Akt/p42/p44 MAPK/AP-1 and NF-kappaB in rat brain astrocytes.J. Cell. Physiol. 224, 376–386.
Vaishnaw, A.K., Gollob, J., Gamba-Vitalo, C., Hutabarat, R., Sah, D., Meyers, R., de, F.T.,Maraganore, J., 2010. A status report on RNAi therapeutics. Silence 1, 14.
Venkatraman, G., Behrens, M., Pyrski, M., Margolis, F.L., 2005. Expression of Coxsackie-Adenovirus receptor (CAR) in the developing mouse olfactory system. J. Neurocytol.34, 295–305.
Verboon-Maciolek, M.A., Groenendaal, F., Hahn, C.D., Hellmann, J., van Loon, A.M.,Boivin, G., de Vries, L.S., 2008a. Human parechovirus causes encephalitis with whitematter injury in neonates. Ann. Neurol. 64, 266–273.
Verboon-Maciolek, M.A., Krediet, T.G., Gerards, L.J., de Vries, L.S., Groenendaal, F., vanLoon, A.M., 2008b. Severe neonatal parechovirus infection and similarity withenterovirus infection. Pediatr. Infect. Dis. J. 27, 241–245.
Victoria, J.G., Kapoor, A., Li, L., Blinkova, O., Slikas, B., Wang, C., Naeem, A., Zaidi, S.,Delwart, E., 2009. Metagenomic analyses of viruses in stool samples from childrenwith acute flaccid paralysis. J. Virol. 83, 4642–4651.
Vignuzzi, M., Stone, J.K., Arnold, J.J., Cameron, C.E., Andino, R., 2006. Quasispeciesdiversity determines pathogenesis through cooperative interactions in a viralpopulation. Nature 439, 344–348.
Vignuzzi, M., Wendt, E., Andino, R., 2008. Engineering attenuated virus vaccines bycontrolling replication fidelity. Nat. Med. 14 (2), 154–161.
Vogt, D.A., Andino, R., 2010. An RNA element at the 5′-end of the poliovirus genomefunctions as a general promoter for RNA synthesis. PLoS Pathog. 6 (6), e1000936.
Volpe, J.J., 2008. Neonatal encephalitis and white matter injury: more than justinflammation? Ann. Neurol. 64, 232–236.
Vuorinen, T., Vainionpaa, R., Vanharanta, R., Hyypia, T., 1996. Susceptibility of humanbone marrow cells and hematopoietic cell lines to coxsackievirus B3 infection. J.Virol. 70 (12), 9018–9023.
Wahid, R., Cannon, M.J., Chow, M., 2005. Dendritic cells and macrophages areproductively infected by poliovirus. J. Virol. 79 (1), 401–409.
Ward, C.D., Flanegan, J.B., 1992. Determination of the poliovirus RNA polymerase errorfrequency at eight sites in the viral genome. J. Virol. 66 (6), 3784–3793.

305R.E. Rhoades et al. / Virology 411 (2011) 288–305
Ward, C.D., Stokes, M.A., Flanegan, J.B., 1988. Direct measurement of the poliovirus RNApolymerase error frequency in vitro. J. Virol. 62 (2), 558–562.
Webster, A.D., 2005. Pleconaril— an advance in the treatment of enteroviral infection inimmuno-compromised patients. J. Clin. Virol. 32, 1–6.
Weng, K.F., Li, M.L., Hung, C.T., Shih, S.R., 2009. Enterovirus 71 3C protease cleaves anovel target CstF-64 and inhibits cellular polyadenylation. PLoS Pathog. 5 (9),e1000593.
Werk, D., Schubert, S., Lindig, V., Grunert, H.P., Zeichhardt, H., Erdmann, V.A., Kurreck, J.,2005. Developing an effective RNA interference strategy against a plus-strand RNAvirus: silencing of coxsackievirus B3 and its cognate coxsackievirus–adenovirusreceptor. Biol. Chem. 386, 857–863.
Whitton, J.L., Cornell, C.T., Feuer, R., 2005. Host and virus determinants of picornaviruspathogenesis and tropism. Nat. Rev. Microbiol. 3 (10), 765–776.
Wilkins, C., Gale Jr., M., 2010. Recognition of viruses by cytoplasmic sensors. Curr. Opin.Immunol. 22, 41–47.
Wimmer, E., Mueller, S., Tumpey, T.M., Taubenberger, J.K., 2009. Synthetic viruses: anew opportunity to understand and prevent viral disease. Nat. Biotechnol. 27,1163–1172.
Wong, J., Zhang, J., Si, X., Gao, G., Mao, I., McManus, B.M., Luo, H., 2008. Autophagosomesupports coxsackievirus B3 replication in host cells. J. Virol. 82 (18), 9143–9153.
Woodall, C.J., Graham, D.I., 2004. Evidence for neuronal localisation of enteroviralsequences in motor neurone disease/amyotrophic lateral sclerosis by in situhybridization. Eur. J. Histochem. 48, 129–134.
Woodall, C.J., Riding, M.H., Graham, D.I., Clements, G.B., 1994. Sequences specific forenterovirus detected in spinal cord from patients with motor neurone disease. BMJ308, 1541–1543.
Wu, C.N., Lin, Y.C., Fann, C., Liao, N.S., Shih, S.R., Ho, M.S., 2001. Protection against lethalenterovirus 71 infection in newborn mice by passive immunization with subunitVP1 vaccines and inactivated virus. Vaccine 20, 895–904.
Wu, K.X., Ng, M.M., Chu, J.J., 2010. Developments towards antiviral therapies againstenterovirus 71. Drug Discov. Today 15, 1041–1051.
Xie, J., Jiao, Y., Qiu, Z., Li, Q., Li, T., 2010. Significant elevation of B cells at the acute stagein enterovirus 71-infected children with central nervous system involvement.Scand. J. Infect. Dis.
Yamayoshi, S., Yamashita, Y., Li, J., Hanagata, N., Minowa, T., Takemura, T., Koike, S., 2009.Scavenger receptor B2 is a cellular receptor for enterovirus 71. Nat. Med. 15 (7),798–801.
Yang, W.X., Terasaki, T., Shiroki, K., Ohka, S., Aoki, J., Tanabe, S., Nomura, T., Terada, E.,Sugiyama, Y., Nomoto, A., 1997. Efficient delivery of circulating poliovirus to the centralnervous system independently of poliovirus receptor. Virology 229 (2), 421–428.
Yang, B., Chuang, H., Yang, K.D., 2009. Sialylated glycans as receptor and inhibitor ofenterovirus 71 infection to DLD-1 intestinal cells. Virol. J. 6, 141.
Yoon, S.Y., Ha, Y.E., Choi, J.E., Ahn, J., Lee, H., Kweon, H.S., Lee, J.Y., Kim, D.H., 2008.Coxsackievirus B4 uses autophagy for replication after calpain activation in ratprimary neurons. J. Virol. 82 (23), 11976–11978.
Yoshikawa, T., Iwasaki, T., Ida-Hosonuma, M., Yoneyama, M., Fujita, T., Horie, H.,Miyazawa, M., Abe, S., Simizu, B., Koike, S., 2006. Role of the alpha/beta interferonresponse in the acquisition of susceptibility to poliovirus by kidney cells in culture.J. Virol. 80, 4313–4325.
Yuan, J., Cheung, P.K., Zhang, H.M., Chau, D., Yang, D., 2005. Inhibition of coxsackievirusB3 replication by small interfering RNAs requires perfect sequence match in thecentral region of the viral positive strand. J. Virol. 79, 2151–2159.





![-ravichandran@uiowa.edu] CVS Health (CVS) September … · Through the above service, CVS helps clients in designing ... Improvement, and Modernization ... prescriptions at CVS Pharmacy](https://img.pdfslide.us/doc/110x75/5b5140327f8b9a056a8bdae7/-ravichandranuiowaedu-cvs-health-cvs-september-through-the-above-service.jpg)