Embed Size (px)
Citation preview
MINI-SYMPOSIUM: PATHOLOGY OF GASTROINTESTINAL LYMPHOMAS
Enteropathy associated T-celllymphoma: a review ofdiagnostic findings andtherapeutic strategiesStuti Shroff
Karthik A Ganapathi
Abstract
Enteropathy associated T-cell lymphoma (EATL) is an uncommon type ofnon-Hodgkin T-cell lymphoma of the intestinal intraepithelial T lympho-
cytes. Frequently presenting as intestinal perforation, ulceration, or a
mass in the jejunum and proximal ileum in the gastrointestinal tract,
EATL carries a poor prognosis with absence of well-defined therapeutic
protocols for management. The WHO recognizes two distinct variants of
EATL, the type I/classical variant and type II/monomorphic variant,
based on different clinical features and histopathologic findings. EATL
type I has a higher incidence in geographic regions with a high prevalence
of celiac disease such as Northern Europe and is rare in the Asian popu-
lation, in whom celiac disease is also rare. EATL type II can occur sporad-
ically, has a higher incidence in Asian populations, with no definite
association with celiac disease. This review aims to summarize the clini-
copathologic findings of EATL and current approaches to management.
Keywords enteropathy associated T-cell lymphoma; intraepithelial lym-
phocytes; refractory celiac disease
Introduction
The first association between malabsorption and intestinal lym-
phoma was made in 1937 by Fairley and Mackie.1 It was believed
for several years that malabsorption was the sequelae of intes-
tinal lymphoma. This perception changed in 1962 when Gough
et al. described a series of three patients who developed intestinal
lymphoma as a complication of malabsorption.2 In 1978 Isaacson
et al. first suggested,3 and later in 1985, demonstrated that the
intraepithelial T cells were the cells of origin for this celiac dis-
ease associated lymphoma.4 The term enteropathy associated T-
cell lymphoma (EATL) was introduced by O’Farrelly et al. in
1986 to distinguish it from an uncomplicated form of celiac
disease.5
Formerly known as enteropathy-type-T-cell lymphoma, en-
teropathy associated T-cell lymphoma is a rare form of non-
Hodgkin lymphoma. With an annual incidence of 0.5e1 per
million in the Western countries,6 and comprising 10e25% of
Stuti Shroff MD PhD Assistant Professor Department of Pathology and
Laboratory Medicine, Hospital of the University of Pennsylvania,
Philadelphia, PA, USA. Conflicts of interest: none.
Karthik A Ganapathi MD PhD Clinical Fellow Department of Pathology,
National Cancer Institute, National Institutes of Health, Bethesda, MD,
USA. Conflicts of interest: none.
DIAGNOSTIC HISTOPATHOLOGY 20:4 151
all primary lymphomas of the intestine, EATL is the most
common primary gastrointestinal T-cell lymphoma. The inci-
dence of EATL varies geographically. It is often, but not al-
ways, associated with celiac disease and follows the frequency
of celiac disease worldwide. Though uncomplicated celiac
disease has a higher incidence in the female population, a
population based study in the Netherlands revealed that EATL
affects men more frequently than women. Patients affected by
EATL typically present in the age range of 50e70 years with a
mean age of 64 years. The peak incidence is in the seventh
decade of life.7
Though EATL can involve any part of the gastrointestinal
tract, such as the stomach, duodenum and colon, the jejunum
and proximal ileum are the most common sites of involvement.
Extra-intestinal involvement, though reported, is rare. Patients
can present with celiac-disease related symptoms such as
malabsorption, abdominal pain, and weight loss. The first pre-
sentation in several cases, however, is perforation or obstruction
of the small intestine, with the diagnosis being made at the time
of laparotomy.
The WHO recognizes two variants of EATL, each with
different genetic alterations and histomorphologic findings.
A. Type I or classical variant
The classical or type I variant is the more common variant of
EATL, comprising 66e90% of the cases.8,9 It is characterized by
strong association to celiac disease and is most frequent in in-
dividuals with the celiac-disease associated human leukocyte
antigen (HLA) DQA1*0501, DBQ1*0201 genotypes. Additional
HLA-DR/DQ alleles may increase the risk of lymphoma in these
patients. Type I or classic EATL is also characterized by chro-
mosomal aberrations with a gain in the 9q region or a deletion in
the 16q region.10
Celiac disease is an immune-mediated gluten sensitive enter-
opathy induced as a result of consumption of Triticeae glutens in
genetically susceptible individuals. Ingestion of gluten found in
wheat, barley and rye leads to intraepithelial lymphocytosis with
epithelial damage, expansion of lamina propria, villous atrophy
and crypt hyperplasia. The histologic findings are supported by
detection of circulating serum IgA autoantibodies against trans-
glutaminase and endomysium.
Refractory celiac disease (RCD) with or without mucosal ul-
ceration may precede EATL. RCD is defined as persistence or
recurrence following a former good response, of clinical and
histologic findings of celiac disease after a rigorous gluten free
diet for a period of greater than 12 months. Two subtypes of RCD
have been identified, RCD I and RCD II. Individuals with RCD I
demonstrate less than 20% intraepithelial lymphocytes. These
intraepithelial lymphocytes have a normal phenotype and are
polyclonal. Patients with RCD II have greater than 20% intra-
epithelial lymphocytes with aberrant expression of CD3, CD4 and
down-regulation of CD8, and monoclonal gT cell receptor rear-
rangements. This aberrant T cell phenotype has also been
demonstrated in the enteropathic mucosa adjacent to the tumor
in EATL, type I, suggesting that RCD II is likely a precursor, and
may represent an intraepithelial cryptic T cell lymphoma or an
in-situ lesion of EATL, type I. Additional support for RCD II as the
precursor lesion for EATL, type I, is that the intraepithelial
lymphocytes both in RCD II and EATL, type I, harbor gains of
chromosome 1q and 5q.11
� 2014 Elsevier Ltd. All rights reserved.
MINI-SYMPOSIUM: PATHOLOGY OF GASTROINTESTINAL LYMPHOMAS
Studies have shown that the interval of time between the
diagnosis of celiac disease and the onset of type I EATL is vari-
able. Most patients with type I EATL have adult-onset celiac
disease. The diagnosis of celiac disease in some patients is in the
same clinical episode as the diagnosis of type I EATL. In other
individuals this interval can be more than 5 years.12
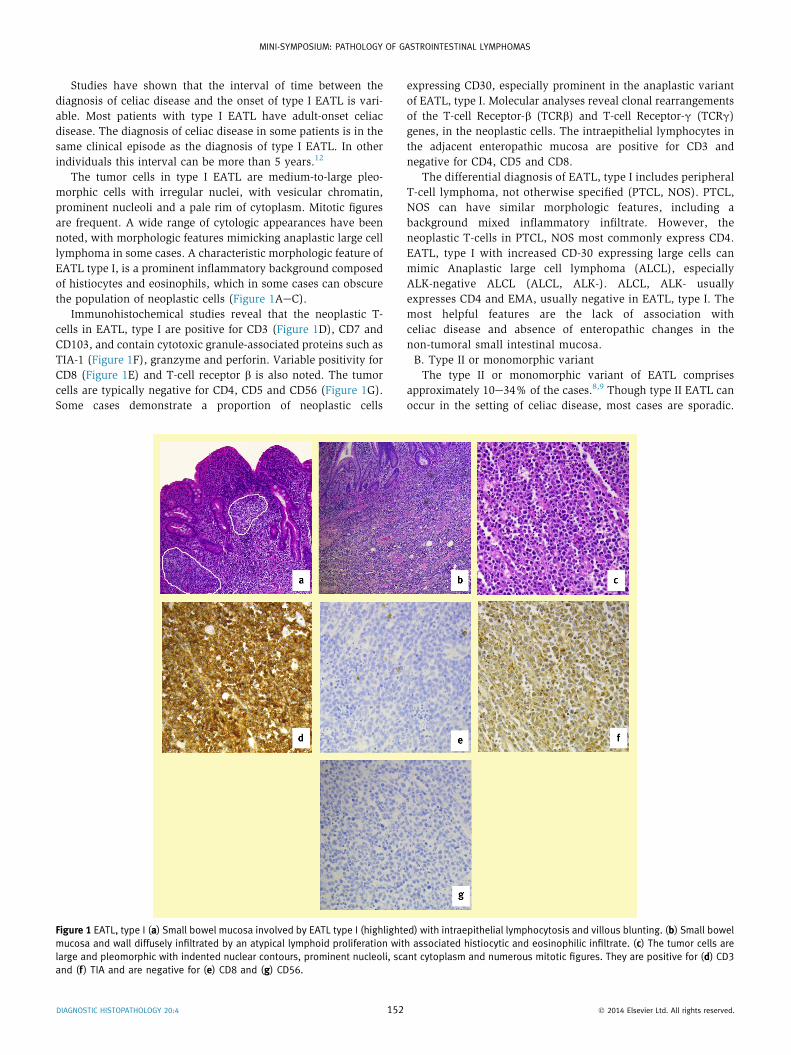
The tumor cells in type I EATL are medium-to-large pleo-
morphic cells with irregular nuclei, with vesicular chromatin,
prominent nucleoli and a pale rim of cytoplasm. Mitotic figures
are frequent. A wide range of cytologic appearances have been
noted, with morphologic features mimicking anaplastic large cell
lymphoma in some cases. A characteristic morphologic feature of
EATL type I, is a prominent inflammatory background composed
of histiocytes and eosinophils, which in some cases can obscure
the population of neoplastic cells (Figure 1AeC).
Immunohistochemical studies reveal that the neoplastic T-
cells in EATL, type I are positive for CD3 (Figure 1D), CD7 and
CD103, and contain cytotoxic granule-associated proteins such as
TIA-1 (Figure 1F), granzyme and perforin. Variable positivity for
CD8 (Figure 1E) and T-cell receptor b is also noted. The tumor
cells are typically negative for CD4, CD5 and CD56 (Figure 1G).
Some cases demonstrate a proportion of neoplastic cells
Figure 1 EATL, type I (a) Small bowel mucosa involved by EATL type I (highlight
mucosa and wall diffusely infiltrated by an atypical lymphoid proliferation wit
large and pleomorphic with indented nuclear contours, prominent nucleoli, sca
and (f ) TIA and are negative for (e) CD8 and (g) CD56.
DIAGNOSTIC HISTOPATHOLOGY 20:4 152
expressing CD30, especially prominent in the anaplastic variant
of EATL, type I. Molecular analyses reveal clonal rearrangements
of the T-cell Receptor-b (TCRb) and T-cell Receptor-g (TCRg)
genes, in the neoplastic cells. The intraepithelial lymphocytes in
the adjacent enteropathic mucosa are positive for CD3 and
negative for CD4, CD5 and CD8.
The differential diagnosis of EATL, type I includes peripheral
T-cell lymphoma, not otherwise specified (PTCL, NOS). PTCL,
NOS can have similar morphologic features, including a
background mixed inflammatory infiltrate. However, the
neoplastic T-cells in PTCL, NOS most commonly express CD4.
EATL, type I with increased CD-30 expressing large cells can
mimic Anaplastic large cell lymphoma (ALCL), especially
ALK-negative ALCL (ALCL, ALK-). ALCL, ALK- usually
expresses CD4 and EMA, usually negative in EATL, type I. The
most helpful features are the lack of association with
celiac disease and absence of enteropathic changes in the
non-tumoral small intestinal mucosa.
B. Type II or monomorphic variant
The type II or monomorphic variant of EATL comprises
approximately 10e34% of the cases.8,9 Though type II EATL can
occur in the setting of celiac disease, most cases are sporadic.
ed) with intraepithelial lymphocytosis and villous blunting. (b) Small bowel
h associated histiocytic and eosinophilic infiltrate. (c) The tumor cells are
nt cytoplasm and numerous mitotic figures. They are positive for (d) CD3
� 2014 Elsevier Ltd. All rights reserved.
MINI-SYMPOSIUM: PATHOLOGY OF GASTROINTESTINAL LYMPHOMAS
The frequency of HLA-DQ2/HLA-DQ8 in Caucasian patients with
this variant EATL is 30e40%, which is comparable to the normal
frequency HLA-DQ2/HLA-DQ8 in the Caucasian population.8
EATL type II is more common in the Asian population from
Japan and Taiwan, in whom celiac disease is rare.10,13 The eti-
ology of EATL type II in this population remains unknown.
Chromosomal aberrations with a gain in the 9q region or a
deletion in the 16q region have also been reported, however, this
lymphoma more frequently demonstrates gains in the 8q24
(MYC) region.10 Unlike RCD II and EATL type I, EATL type II
rarely demonstrates gains of chromosome 1q and 5q.10
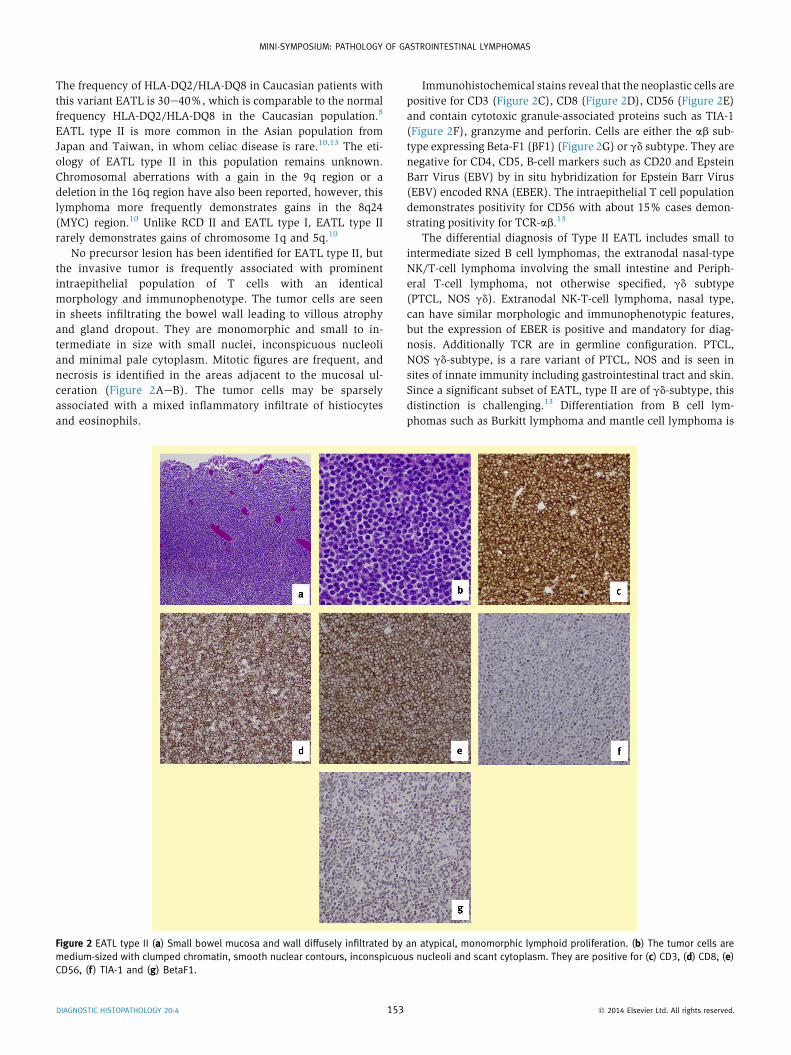
No precursor lesion has been identified for EATL type II, but
the invasive tumor is frequently associated with prominent
intraepithelial population of T cells with an identical
morphology and immunophenotype. The tumor cells are seen
in sheets infiltrating the bowel wall leading to villous atrophy
and gland dropout. They are monomorphic and small to in-
termediate in size with small nuclei, inconspicuous nucleoli
and minimal pale cytoplasm. Mitotic figures are frequent, and
necrosis is identified in the areas adjacent to the mucosal ul-
ceration (Figure 2AeB). The tumor cells may be sparsely
associated with a mixed inflammatory infiltrate of histiocytes
and eosinophils.
Figure 2 EATL type II (a) Small bowel mucosa and wall diffusely infiltrated by
medium-sized with clumped chromatin, smooth nuclear contours, inconspicuo
CD56, (f ) TIA-1 and (g) BetaF1.
DIAGNOSTIC HISTOPATHOLOGY 20:4 153
Immunohistochemical stains reveal that the neoplastic cells are
positive for CD3 (Figure 2C), CD8 (Figure 2D), CD56 (Figure 2E)
and contain cytotoxic granule-associated proteins such as TIA-1
(Figure 2F), granzyme and perforin. Cells are either the ab sub-
type expressing Beta-F1 (bF1) (Figure 2G) or gd subtype. They are
negative for CD4, CD5, B-cell markers such as CD20 and Epstein
Barr Virus (EBV) by in situ hybridization for Epstein Barr Virus
(EBV) encoded RNA (EBER). The intraepithelial T cell population
demonstrates positivity for CD56 with about 15% cases demon-
strating positivity for TCR-ab.13
The differential diagnosis of Type II EATL includes small to
intermediate sized B cell lymphomas, the extranodal nasal-type
NK/T-cell lymphoma involving the small intestine and Periph-
eral T-cell lymphoma, not otherwise specified, gd subtype
(PTCL, NOS gd). Extranodal NK-T-cell lymphoma, nasal type,
can have similar morphologic and immunophenotypic features,
but the expression of EBER is positive and mandatory for diag-
nosis. Additionally TCR are in germline configuration. PTCL,
NOS gd-subtype, is a rare variant of PTCL, NOS and is seen in
sites of innate immunity including gastrointestinal tract and skin.
Since a significant subset of EATL, type II are of gd-subtype, this
distinction is challenging.13 Differentiation from B cell lym-
phomas such as Burkitt lymphoma and mantle cell lymphoma is
an atypical, monomorphic lymphoid proliferation. (b) The tumor cells are
us nucleoli and scant cytoplasm. They are positive for (c) CD3, (d) CD8, (e)
� 2014 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: PATHOLOGY OF GASTROINTESTINAL LYMPHOMAS
made on clinical presentation and immunohistochemistry. Bur-
kitt lymphoma is more common in the younger age group, and
mantle cell lymphoma involving the bowel presents more
frequently as polyps rather than ulcerative or tumoral lesions.
Immunohistochemistry for B-cell markers such as CD20, CD10
and cyclin-D1 also aids in the differentiation of these cases.
Clinical presentation and diagnosis
EATL often presents with multifocal masses that ulcerate and
invade the wall of the small intestine. Jejunum and proximal
terminal ileum are the most commonly involved sites in the
gastrointestinal tract. Abdominal pain, weight loss, diarrhea, and
symptoms of bowel obstruction are noted in some cases.
Involvement of the distal small intestine, ileocecal region and
colon are more frequent in type II EATL compared to EATL
type I. Extraintestinal involvement by EATL can be seen in the
mesenteric, paraaortic or iliac lymph nodes.9
In patients who present in an emergency scenario with a
perforation, the diagnosis is usually made at the time of laparot-
omy. In other patients, the diagnosis of the ulcerative or tumoral
lesions of EATL is made with the help of imaging techniques such
as CT scan combined with 18F-fluorodeoxyglucose positron
emission tomography (18F-FDG-PET) scan. Video capsule
enteroscopy (VCE) and magnetic resonance enteroclysis (MRE)
are additional diagnostic modalies for examination of the small
intestine and can be used to monitor tumor size following
chemotherapy.8 Double-balloon enteroscopy (DBE), first
described by Yamamoto et al., allows for a detailed examination of
the small bowel and identification of diminutive small intestine
lesions.14,15 On histologic examination, features of celiac disease
such as intraepithelial lymphocytosis, crypt hyperplasia and
villous hypertrophy are noted in the non-tumoral mucosa of the
adjacent small intestine in EATL type I.
Therapeutic options
There are no established standardized therapeutic protocols for
the treatment of EATL. For disease localized to a small segment
of bowel, surgical resection is the first modality of management,
followed by chemotherapy. Numerous different chemothera-
peutic regimens containing anthracycline have been adminis-
tered. Relapses after administration of CHOP
(cyclophosphamide, doxorubicin, vincristine, prednisone),
ACVBP (doxorubicin, cyclophosphamide, vindesine, bleomycin,
prednisone) and CHOP-like chemotherapeutic regimens are
frequent.9 IVE (ifosfamide, etoposide, epirubicin), followed by
high-dose methotrexate with folinic acid rescue and BEAM
(carmustine, etoposide, cytarabine, melphalan) followed by
consolidative autologous stem cell transplantation regimens have
also been administered with better survival, albeit limited suc-
cess.16,17 Radiation is indicated in patients with bulky disease or
with incomplete resection.
Prognosis
Despite numerous therapeutic regimens, the prognosis both
subtypes of EATL remains poor, since patients present with
multifocal and advanced stage disease with complications of
intestinal perforation at the time of presentation. Additionally, a
DIAGNOSTIC HISTOPATHOLOGY 20:4 154
significant proportion of patients do not complete their chemo-
therapeutic regimen or do not receive radiotherapy secondary to
poor nutritional status, performance status impairment, other
complications or rapid disease progression despite therapy.18,19
In a study of 62 patients by Delabie et al. the median overall
survival was 10 months and the median failure-free survival was
only 6 months.9 Recurrences are frequent and most common in
the small intestine. The 5-year overall survival is reportedly 20%,
however, the failure-free survival at 5 years is low at 4%.9
Conclusion
In summary, EATL is a rare type of aggressive non-Hodgkin T-
cell lymphoma with two distinct histologic subtypes. The classic
and monomorphic variants of EATL have different histo-
morphologic features and precursor lesions. Despite numerous
therapeutic regimens, the prognosis of EATL is poor with un-
satisfactory survival outcomes. A
REFERENCES
1 Fairley NH, Mackie FP. Clinical and biochemical syndrome in lym-
phadenoma. Br Med J 1937; 1. 375e404.4.
2 Gough KR, Read AE, Naish JM. Intestinal reticulosis as a complication
of idiopathic steatorrhoea. Gut 1962; 3: 232e9.
3 Isaacson P, Wright DH. Malignant histiocytosis of the intestine. Its
relationship to malabsorption and ulcerative jejunitis. Hum Pathol
1978; 9: 661e77.
4 Isaacson PG, O’Connor NT, Spencer J, et al. Malignant histiocytosis of
the intestine: a t-cell lymphoma. Lancet 1985; 2: 688e91.
5 O’Farrelly C, Feighery C, O’Briain DS, et al. Humoral response to wheat
protein in patients with coeliac disease and enteropathy associated t
cell lymphoma. Br Med J (Clin Res Ed) 1986; 293: 908e10.
6 Catassi C, Bearzi I, Holmes GK. Association of celiac disease and
intestinal lymphomas and other cancers. Gastroenterology 2005;
128: S79e86.
7 Verbeek WH, Van De Water JM, Al-Toma A, Oudejans JJ, Mulder CJ,
Coupe VM. Incidence of enteropathy-associated t-cell lymphoma: a
nation-wide study of a population-based registry in the Netherlands.
Scand J Gastroenterol 2008; 43: 1322e8.
8 van de Water JM, Cillessen SA, Visser OJ, Verbeek WH, Meijer CJ,
Mulder CJ. Enteropathy associated t-cell lymphoma and its precursor
lesions. Best Pract Res Clin Gastroenterol 2010; 24: 43e56.
9 Delabie J, Holte H, Vose JM, et al. Enteropathy-associated t-cell
lymphoma: clinical and histological findings from the international
peripheral t-cell lymphoma project. Blood 2011; 118: 148e55.
10 Deleeuw RJ, Zettl A, Klinker E, et al. Whole-genome analysis and HLA
genotyping of enteropathy-type t-cell lymphoma reveals 2 distinct
lymphoma subtypes. Gastroenterology 2007; 132: 1902e11.
11 Verkarre V, Romana SP, Cellier C, et al. Recurrent partial trisomy 1q22-
q44 in clonal intraepithelial lymphocytes in refractory celiac sprue.
Gastroenterology 2003; 125: 40e6.
12 Ilyas M, Niedobitek G, Agathanggelou A, et al. Non-hodgkin’s lym-
phoma, coeliac disease, and epstein-barr virus: a study of 13 cases
of enteropathy-associated t- and b-cell lymphoma. J Pathol 1995;
177: 115e22.
13 Chan JK, Chan AC, Cheuk W, et al. Type ii enteropathy-associated t-cell
lymphoma: a distinct aggressive lymphomawith frequent gammadelta
t-cell receptor expression. Am J Surg Pathol 2011; 35: 1557e69.
� 2014 Elsevier Ltd. All rights reserved.

MINI-SYMPOSIUM: PATHOLOGY OF GASTROINTESTINAL LYMPHOMAS
14 Yamamoto H, Sekine Y, Sato Y, et al. Total enteroscopy with a
nonsurgical steerable double-balloon method. Gastrointest Endosc
2001; 53: 216e20.
15 Matsumoto T, Nakamura S, Esaki M, et al. Double-balloon endoscopy
depicts diminutive small bowel lesions in gastrointestinal lymphoma.
Dig Dis Sci 2010; 55: 158e65.
16 Bishton MJ, Haynes AP. Combination chemotherapy followed by
autologous stem cell transplant for enteropathy-associated t cell
lymphoma. Br J Haematol 2007; 136: 111e3.
DIAGNOSTIC HISTOPATHOLOGY 20:4 155
17 Jantunen E, Boumendil A, Finel H, et al. Autologous stem cell trans-
plantation for enteropathy-associated t-cell lymphoma: a retrospec-
tive study by the EBMT. Blood 2013; 121: 2529e32.
18 Daum S, Ullrich R, Heise W, et al. Intestinal non-hodgkin’s lym-
phoma: a multicenter prospective clinical study from the German
study group on intestinal non-hodgkin’s lymphoma. J Clin Oncol
2003; 21: 2740e6.
19 Ferreri AJ, Zinzani PL, Govi S, Pileri SA. Enteropathy-associated t-cell
lymphoma. Crit Rev Oncol Hematol 2011; 79: 84e90.
� 2014 Elsevier Ltd. All rights reserved.