Embed Size (px)
Citation preview

Enteral nutrition for preterm infants:
translating ESPGHAN guidelines into practice
Innovating for life.
ovnnI
ro fgntiaov
.eif lr
Sponsored by
Cow & Gate, White Horse Business Park, T
Sponsored by
Cow & Gate, White Horse Business Park, T
in association with
iltshire BA14 0XQ United Kingdom phone: 08457 623 624rowbridge, WCow & Gate, White Horse Business Park, T
in association with
iltshire BA14 0XQ United Kingdom phone: 08457 623 624
iltshire BA14 0XQ United Kingdom phone: 08457 623 624
The survival of preterm infants has increased dramatically over thelast two decades due to advances in obstetric and neonatal medicine,and advanced nursing care based on years of experience and a strongresearch base. Increasing survival, duration and complexity ofintensive care means that nutritional management becomesincreasingly important. It is therefore vital that all health professionalsworking in neonatal care understand how to translate nutritionalresearch, knowledge and recommendations into everyday practice.
A D VA N C E S I N P R A C T I C E – 8
infant
Improved obstetric management and the use ofantenatal steroids mean that babies are nowhealthier at birth than ever before. Technologicalimprovements in respiratory support, includingbetter ventilators and surfactants, have haddramatic impacts on reducing early respiratorydeaths. Promoting and achieving good nutritionalstatus is the keystone upon which other systemsdepend. Nutritional status determines risks ofnecrotising enterocolitis (NEC)1, blood streaminfections, growth and cognitive outcome2. Recentevidence also highlights that nutrition in early lifehas long-term effects, and directly relates to thechances of developing later life diseases such ashypertension, heart disease and type 2 diabetes.
PRETERM INFANTS HAVE UNIQUE NEEDS
Preterm infants do not benefit from the later stagesof pregnancy when optimal nutrient stores arenormally established. This is true for every majornutrient, from protein and energy, to minerals andvitamins3,4. Adipose tissue, the major energy store interm infants, is extremely limited in preterm babies.Preterm babies do not have any significant ‘energy’stores, and must rely on small amounts of fat,carbohydrate (eg glycogen) and protein. Limited fatstores mean that the largest ‘energy’ store isprotein in muscles and other organs. Use of bodyprotein for energy will impair function. Estimates
suggest a 1000g baby only has sufficient energy for2-3 days before death would result withoutexogenous dietary supply.
The preterm brain is extremely vulnerable to under-nutrition. There are few controlled trials, but thoseand observational studies suggest that sub-optimalmacronutrient supply (protein and energy) in earlylife will result in ~5-10 IQ point deficit in laterchildhood. Breast milk is the best form of nutrition:aside from reducing the incidence of NEC andinfections, it is estimated to improve cognitiveoutcome by the equivalent of 4-6 IQ points. Thereare few other interventions in neonatal practicewith that magnitude of effect.
NUTRIENT INTAKES
It is not possible to determine the precise dailyintake of nutrients that any individual baby needs,so recommendations are based on many differenttypes of evidence. Expressed breast milk (EBM) isthe best milk for all preterm babies, but alone willnot meet the nutrient needs of most very pretermbabies. Many will therefore benefit from the use ofbreast milk fortifiers (BMF). Despite support fromnursing staff and lactation specialists, manymothers chose not to initiate expression, or find itdifficult to maintain EBM supply during the manyweeks of neonatal care. Specialised formulae aretherefore required as the nutrient composition in
Volume 7 Issue 6 2011, Pages 187-90 © 2011 Stansted News Limited
Enteral nutrition for preterm infants:translating ESPGHAN guidelines intopractice
Written by
Nicholas D Embleton BSc MD FRCPCH, Consultant Neonatal Paediatrician.Newcastle Neonatal Service, Royal Victoria Infirmary, Newcastle-upon-Tyne.
fed infants. The current recommendation is for aprotein intake of 3.5-4g/kg/d for babies 1-1.8kg inweight: higher intakes are likely to be safe andmight well be needed in the smallest infants, and inthose where support of ‘catch-up’ growth is needed.The composition of many fortifiers and formulaeover the last few years may not have adequatelymet protein needs in all babies. Increasing the milkvolume intake is often not possible (for exampledue to high gastric aspirates) and might beinappropriate if it also results in excess energyintake. Newer formulae and BMF compositions willhelp address this problem, as will innovativeproducts such as protein supplements.
ENERGY AND FAT INTAKES
Although the proportion of energy intake providedby carbohydrates (eg glucose and polysaccharidesetc) is quite tightly defined (10.5-12g/100kcal),there are no studies that allow precisedetermination of the optimal carbohydrate intake.
Dietary lipids provide the remainder of energyintakes, but also provide essential fatty acids andfat soluble vitamins. Lipids are essential for all cellmembranes. There are very high levels of long-chain polyunsaturated fatty acids in the brain andretina. The essential fatty acids alpha-linolenic andlinoleic acids, must be provided in the diet, and areneeded for the production of docosahexaenoic acid(DHA) and arachidonic acid (AA). Clinical trialsexamining the effects of additional DHA and AA informula suggest benefits on early visual and braindevelopment, and possibly immune effects, butthere are few data showing unequivocal long-termbenefit. Breast milk is an excellent source ofessential dietary lipids.
CALCIUM, PHOSPHORUS AND VITAMIN D
It is difficult to match the in-utero accretion ofminerals in preterm infants. ESPGHAN providerecommendations for formula composition, andrecommendations on the calcium to phosphorusratio. In clinical practice very few babies needadditional calcium if they receive a modern pretermformula or breast milk with added BMF.Phosphorus depletion is much more common,particularly in babies on unfortified breast milk.
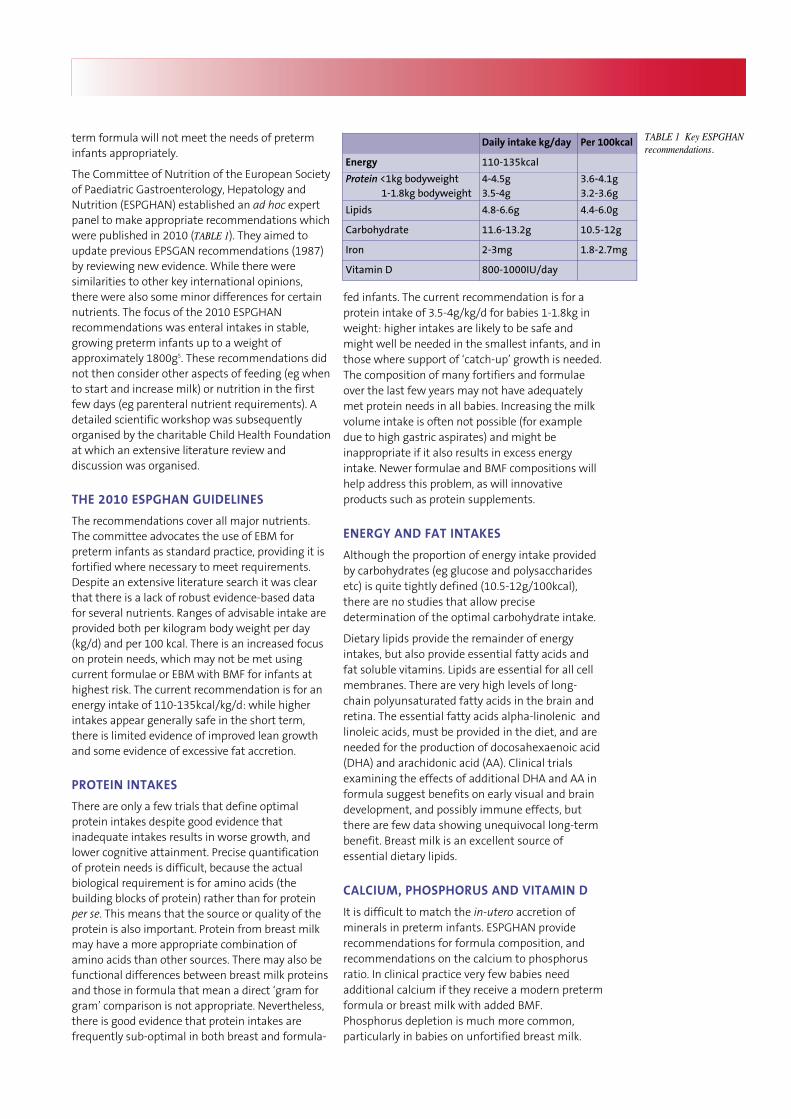
TABLE 1 Key ESPGHANrecommendations.
term formula will not meet the needs of preterminfants appropriately.
The Committee of Nutrition of the European Societyof Paediatric Gastroenterology, Hepatology andNutrition (ESPGHAN) established an ad hoc expertpanel to make appropriate recommendations whichwere published in 2010 (TABLE 1). They aimed toupdate previous EPSGAN recommendations (1987)by reviewing new evidence. While there weresimilarities to other key international opinions,there were also some minor differences for certainnutrients. The focus of the 2010 ESPGHANrecommendations was enteral intakes in stable,growing preterm infants up to a weight ofapproximately 1800g5. These recommendations didnot then consider other aspects of feeding (eg whento start and increase milk) or nutrition in the firstfew days (eg parenteral nutrient requirements). Adetailed scientific workshop was subsequentlyorganised by the charitable Child Health Foundationat which an extensive literature review anddiscussion was organised.
THE 2010 ESPGHAN GUIDELINES
The recommendations cover all major nutrients.The committee advocates the use of EBM forpreterm infants as standard practice, providing it isfortified where necessary to meet requirements.Despite an extensive literature search it was clearthat there is a lack of robust evidence-based datafor several nutrients. Ranges of advisable intake areprovided both per kilogram body weight per day(kg/d) and per 100 kcal. There is an increased focuson protein needs, which may not be met usingcurrent formulae or EBM with BMF for infants athighest risk. The current recommendation is for anenergy intake of 110-135kcal/kg/d: while higherintakes appear generally safe in the short term,there is limited evidence of improved lean growthand some evidence of excessive fat accretion.
PROTEIN INTAKES
There are only a few trials that define optimalprotein intakes despite good evidence thatinadequate intakes results in worse growth, andlower cognitive attainment. Precise quantificationof protein needs is difficult, because the actualbiological requirement is for amino acids (thebuilding blocks of protein) rather than for proteinper se. This means that the source or quality of theprotein is also important. Protein from breast milkmay have a more appropriate combination ofamino acids than other sources. There may also befunctional differences between breast milk proteinsand those in formula that mean a direct ‘gram forgram’ comparison is not appropriate. Nevertheless,there is good evidence that protein intakes arefrequently sub-optimal in both breast and formula-
Daily intake kg/day Per 100kcal
Energy 110-135kcal
Protein <1kg bodyweight1-1.8kg bodyweight
4-4.5g3.5-4g
3.6-4.1g3.2-3.6g
Lipids 4.8-6.6g 4.4-6.0g
Carbohydrate 11.6-13.2g 10.5-12g
Iron 2-3mg 1.8-2.7mg
Vitamin D 800-1000IU/day

PRE- AND PROBIOTICS
Human breast milk contains high levels ofoligosaccharides, especially in colostrum and earlymilk. Most of these resist digestion in the smallbowel, and reach the large bowel where they arefermented. Here they promote the growth ofcertain ‘healthy’ bacteria (probiotic bacteria) suchas bifido-bacteria or lactobacillus. While it is notpossible for milk formulae to match theoligosaccharide composition of breast milk, theaddition of prebiotics such as galacto-oligosaccharide and fructo-oligosaccharideincreases faecal bifido-bacteria counts, reducesstool hardness, and may also affect feed tolerance6.There are also preliminary data suggesting effectson immune function, but there are no controlledtrials showing reduction in rates of sepsis or NEC.Although the literature surrounding the use ofprobiotics in preterm infants as prophylaxis againstNEC is encouraging, routine use is highlycontentious7. ESPGHAN stated further data wererequired before probiotics could be consideredessential dietary components.
CHALLENGES AND INNOVATIONS
Promoting good nutritional status is a keycomponent of neonatal care. Use of breast milkmust be encouraged, macronutrient intakes needoptimising and micronutrient intakes need carefulconsideration. Modern milk formulae and BMF arebeing adapted to meet the changing needs ofpreterm babies and help overcome some of thedifficulties faced in the past. The updated ESPGHANguidelines are just the start. It is important that allthose working in neonatal care are aware of thenutrient needs of preterm infants, and how thesecan be met using EBM and innovative products. Anincreased focus on the role of inadequate proteinintakes has encouraged a re-formulation of someexisting products and highlighted the need for newproducts such as protein supplements.
REFERENCES1. Lucas A et al. Breast milk and necrotising enterocolitis. Lancet
1990;336:1519-23.2. Lucas A et al. Breast milk and subsequent intelligence quotient
in children born preterm. Lancet 1992;339:261-64.3. Embleton ND. Optional protein and energy intakes in preterm
infants. Early Hum Dev 2007;83:831-37.4. Tsang R et al. Nutrition of the Preterm Infant, scientific basis and
practical guidelines. Second edition. Cincinnati, Ohio: DigitalEducational Publishing Inc. 2005.
5. Agostoni C et al. Enteral nutrient supply for preterm infants:Commentary from ESPGHAN Committee on Nutrition. JPGN2010;50:85-91.
6. Knol J et al. Increase of faecal bifidobacteria due to dietaryoligosaccharides induces a reduction of clinically relevantpathogen germs in the faeces of preterm formula-fed infants.Acta Paediatrica 2005;94 (suppl 449):31-33.
7. Embleton N et al. Probiotics decrease the incidence of NEC anddeath – so why aren’t we using them? Infant 2011;7:20-24.
A D VA N C E S I N P R A C T I C E – 8
Unlike macronutrients (protein, fat, carbohydrate)the plasma phosphate level is a simple way ofassessing dietary phosphate adequacy.
Vitamin D is involved in a bewildering array ofphysiological processes including neurologicalfunction and bone mineralisation. While skinsynthesis of vitamin D is of major importance inchildren and adults, preterm infants are solelydependent on dietary sources and recommen-dations assume no contribution from skinsynthesis. Vitamin D undergoes hepatic and renalconversion into the active form, which in turnpromotes mineral absorption from the gut, andfacilitates adequate bone formation. Althoughthere are many different forms (vitamin D2 andvitamin D3 are the major forms) recommendationsare only for vitamin D and are provided ininternational units (IU). The ESPGHANrecommendation of 800-1000 IU per day is theonly nutrient for which a daily intake as opposed toa per kg per day intake is made. In order to meetthis at low intake volumes without providingexcessive intakes when volume consumption ishigh, it is necessary to use a vitamin supplement inthe first few months. Additionally, an increasedrecognition of the high prevalence of vitamin Dinadequacy in the general population has led torecommendations that supplemental vitamin Dcontinues to be provided during infancy.
IRON
Iron deficiency results not only in anaemia, but alsoin worse cognitive outcome. However, iron is toxic,and while intestinal uptake can be down-regulated,humans possess no mechanism for excretion ofexcess iron. Free iron increases oxidant damage,may increase the risk of retinopathy of prematurity(ROP) and increases the risk of bacterialproliferation. A careful balance is therefore required.Although iron is essential from birth, gut re-absorption and blood transfusions in the mostpreterm infants mean that supplemental iron israrely required in the first 2-4 weeks unless bloodloss (including that from frequent blood tests) isexcessive. Preterm formula will meet ironrequirements, but additional iron will be needed forinfants who have not been recently transfused andwhere their sole dietary intake is from EBM. It isimportant to note that BMFs available in the UK donot contain additional iron – this is the only majornutrient where intakes in BMF-supplementedinfants do not match those fed on preterm formula.Although ESPGHAN recommendations are forsupplemental iron from 2-4 weeks of age, inpractice few infants need additional iron before 4-6weeks of age. Given that most infants <28 weeks’gestation receive at least one blood transfusion,many practitioners find that extra iron need only bestarted in the weeks just prior to hospital discharge.
Conflict of intereststatement
Dr Embleton supports the use
of breast milk and does not
endorse any specific company
or product. His research
studies have received support
from infant formula
manufacturers but he has no
personal or financial
relationship with any
commercial organisation.
Infant has donated an
honoraria for the writing of
this article to charity.





























