Embed Size (px)
DESCRIPTION
Enrollment, Marketing & Outreach for Coverage Expansions. The Louisiana Experience State Coverage Initiatives National Workshop New Orleans, LA January 25, 2007 J. Ruth Kennedy La. Dept of Health & Hospitals. Overview of Louisiana Strategies. - PowerPoint PPT Presentation
Citation preview
Enrollment, Marketing & Outreach for Coverage
Expansions
The Louisiana Experience
State Coverage InitiativesNational Workshop
New Orleans, LAJanuary 25, 2007
J. Ruth KennedyLa. Dept of Health & Hospitals
2
Overview of Louisiana Strategies
Engaging eligibility employees in outreach, marketing, & enrollment
Successfully reducing procedural closures as renewal
Major organizational change in our eligibility operations
3
The Importance of Informing Families
Children will not be helped if we don’t intervene. Parents are either unconcerned or unaware. --LA Congressman Rodney Alexander
4
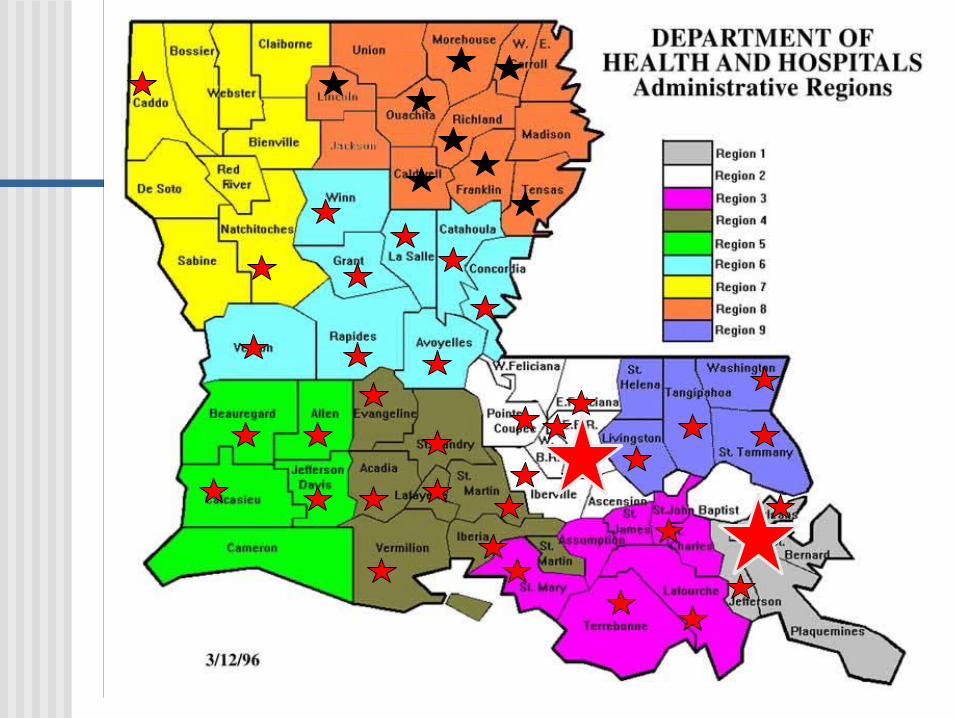
Louisiana Eligibility Administrative Overview Eligibility is determined by state Medicaid
agency employees Medicaid Analysts process only Medicaid
and SCHIP cases Approximately 50 local eligibility offices Medicaid Program has direct line authority
over 844 eligibility employees
5
6
Medicaid Eligibility Staff are Major Players in Outreach
843+ local Medicaid managers, supervisors, eligibility caseworkers, and clerical staff
Brainstorming and implementing Regional Outreach Plans
Organizing and conducting launch meetings Telling friends, family, neighbors, and
acquaintances about LaCHIP Distribution of application form and holders in
their communities
7
Connecting the Dots . . . Why Health Coverage Matters
Health CareAccess
EducationalOutcomes
Poverty Rate in
Louisiana
8
HCFA’s 2000 Summation of LaCHIP Outreach Efforts
. . .the State has been both aggressive and innovative inmarketing the program and enrolling eligible children. Thestate has worked arduously in establishing an effectivegrassroots eligibility outreach network and has taken fulladvantage of vital partnership opportunities, such as withthe Robert Wood Johnson grantee. As a result the State enrolled a significant number of previously uninsured children and exceeded its established enrollment goals. The State has also substantially reduced the number of uninsured children by identifying and enrolling eligible Medicaid children. --Draft Review of Louisiana’s LaCHIP Program Dated 8/16/00
9
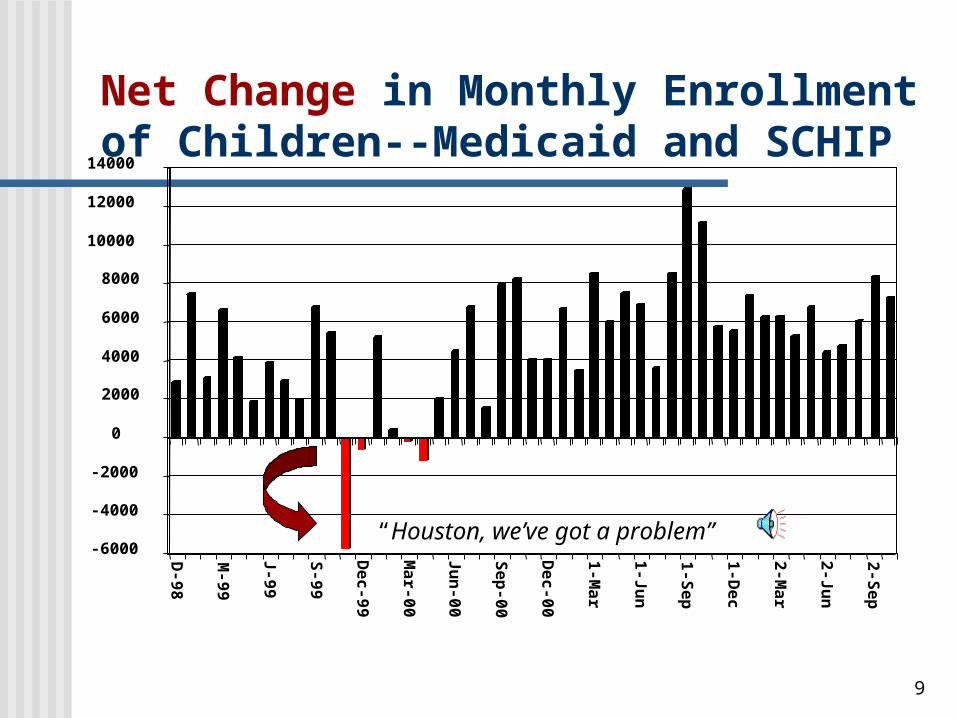
Net Change in Monthly Enrollment of Children--Medicaid and SCHIP
“Houston, we’ve got a problem” -6000
-4000
-2000
0
2000
4000
6000
8000
10000
12000
14000
D-98
M-99
J-99
S-99
Dec-99
Mar-00
Jun-00
Sep-00
Dec-00
1-Mar
1-Jun
1-Sep
1-Dec
2-Mar
2-Jun
2-Sep
10
A “Hole in the Bucket” or Renewal Woes
New enrollees can be exceeded by closures at renewalMany closures for “procedural” reasons
Failure to return renewal formFailure to submit essential verificationUnable to locate
Problem more pronounced for “traditional” Medicaid children
11
“Closing the Door” on Procedural Closures at Renewal Matters
Essential to “maintain the gains”
More costly to process applications than renewals
Protects investment in outreach & marketing
12
Our Recipe for “Closing the Door” on Procedural Closures Simplify the renewal process
Renewal form Verification requirements
Ex Parte renewals when possible Aggressive follow-up when renewal form
is not received Telephone renewals Automated Voice Response renewals Web based renewals [Coming Soon!]
13
Spotlight on Retention Began in 2001
A “new name”—name for process formerly known as “redetermination” changed to “renewal”
New simplified Renewal Form Ex parte renewals mandated for
children with active Food Stamp cases
Involved local offices in identifying solutions
14
Ex Parte Renewal Defined “Action by one party
without the involvement of the other”
Described in 4/7/00 State Medicaid Director’s Letter
Heavy reliance on other computer systems for verification Food Stamps TANF Child Support More than 60% of Title 19 Medicaid
children are extended 12 months using exparte renewal
15
“Ex Parte” --New Eligibility Vocabulary Word
It’s an adjective! CMS advised that we should do ex parte
renewals. It’s a verb!
Is there any way you can possibly ex parte it?
It’s a noun! I did 8 ex partes yesterday.
16
Aggressive Follow-up When Renewal Form in Not Received Incorporated into policy and procedures
since July 2001 Phone calls must be attempted and
documented Efforts to find new address and locate
family Other computer systems Internet Schools, medical providers
Major losses when temporarily discontinued from 7/06 to 11/06
17
Telephone Renewals Benefit Families and the Agency
Federal regulations require annual review—not signed form
Implemented 11/03 as option when ex parte can’t be done
Two types of telephone renewals In lieu of mailing a Renewal Form At follow-up when Renewal Form is
not returned Key to our getting procedural
closures below 5% Reduces administrative cost—
postage, paper, staff time
18
Automated Voice Response (AVR) Renewals
Families can renew anytime—off-cycle or “rolling” renewals encouraged
Option available when calling the LaCHIP toll-free hotline
“To renew by phone now, Press 3” Data retrieved daily & electronically
routed to local eligibility offices Reminder flyers advise of this 24/7
renewal option
19
Local Office Involvement in Developing Retention Plans
Participating in workgroup resulted in greater awareness of the problem (education/training)
Front-line staff have unique insights and proposed excellent strategies
Ownership and buy-in was achieved“I think one of the highlights staff enjoyed was being able to come up with a renewal plan, and then watch their ideas at work”
-- Debbie Falgout, Medicaid Analyst SupervisorThibodaux, Louisiana
20
Examples of Local Initiatives to Improve Retention Supervisory review of all procedural closures at
renewal Not requesting ANY verifications at renewal Adding a “drop box” outside the building for
after hours convenience to return renewal forms, verifications
Additional “reminders” e.g. fluorescent pink reminder flyer prior to advance notice of closure
Enclosing another renewal form/SASE with advance notice of closure
Using US Postal Return Service Telephone surveys of families who failed to
return the renewal form
21
Ongoing Evaluation of Policies, Procedures and Practices Some policies and procedures have
unintended consequences, or in retrospect prove to be unnecessary; Example: policy to hold renewals and not
close them for procedural reasons until deadline day for closures
“Best practices” need to be identified, documented and shared with other offices
Good renewal outcomes by regions and offices deserve acknowledgement and recognition
22
“Organizational Change” Can Be Achieved in Eligibility A key prerequisite to success
of other marketing and outreach efforts
Caseworkers “open” and “close” the door
Major changes in expectations of caseworkers Passive Pro-active
23
Training for Managers Regarding Change in Focus
From strong emphasis on quality control, error reduction, thorough case documentation . . .
. . . To removing barriers, making enrollment process “user friendly”, enrolling eligible children and families, assuring loss of cash does not translate to loss of Medicaid as well.
24
How Much is Too Much?
25
“New Thinking” in Local Offices “What is making a difference is staff has
changed their way of thinking and they do bend over backwards to help the recipient. The mindset is that the applicant or recipient is our number one priority. . . .the Analyst continues to extend time when the recipient states he or she needs more time to get the information in. The Analyst will help the recipient to gather information or documentation whenever possible.”
--Margo Joseph, Medicaid Area ManagerLaPlace, Louisiana
26
Organizational Change“A Long Hard Row to Hoe”
“The “old” way of thinking was that if “they” wanted the services “they” should be expected to do the legwork. Now [caseworkers] get forms completed and information verified [themselves], which, in the long run, actually saves time. But changing old habits has been a long, hard row to hoe.”
“The “old” way of thinking was that if “they” wanted the services “they” should be expected to do the legwork. Now [caseworkers] get forms completed and information verified [themselves], which, in the long run, actually saves time. But changing old habits has been a long, hard row to hoe.”
27
Our “Who Moved the Cheese?” Training Remain Relevant They have moved
the cheese The quicker you let
go of old cheese, the sooner you can enjoy new cheese
They keep moving the cheese so be ready to change quickly!
28
Lessons Learned from our Eligibility Transformation
Incremental changes rather than “big bang” approach”
Dual focus—administrative as well as health & social
Attention to messaging; internal as well as external marketing
Establish high expectations for staff Empowerment of state government
employees Expect initial pushback
29
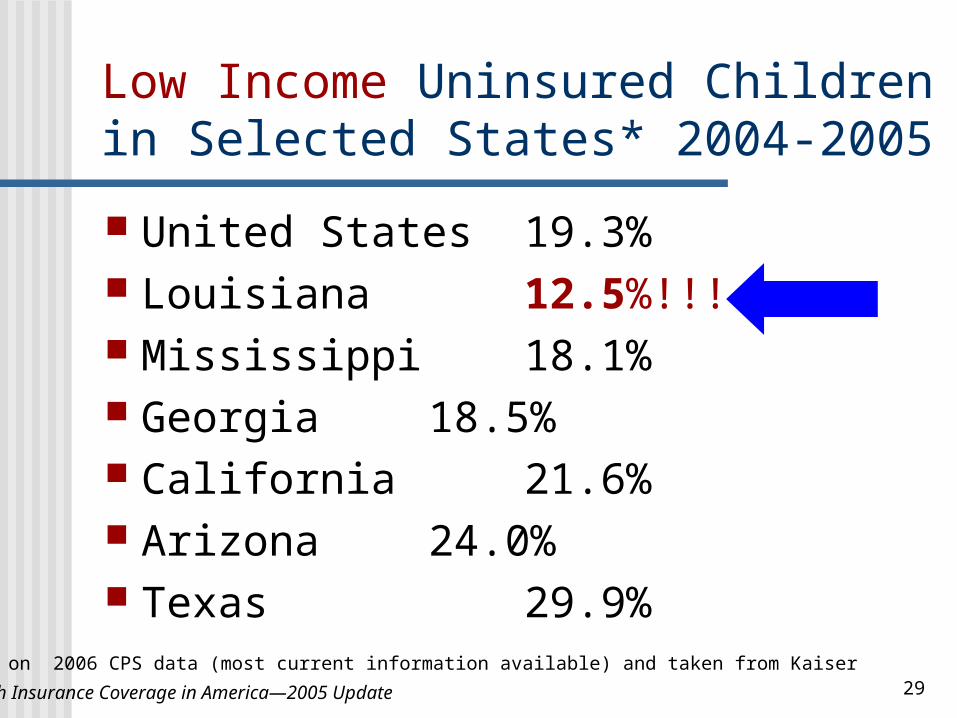
Low Income Uninsured Children in Selected States* 2004-2005
United States 19.3% Louisiana 12.5%!!! Mississippi 18.1% Georgia 18.5% California 21.6% Arizona 24.0% Texas 29.9%
•Based on 2006 CPS data (most current information available) and taken from Kaiser
• Health Insurance Coverage in America—2005 Update
30
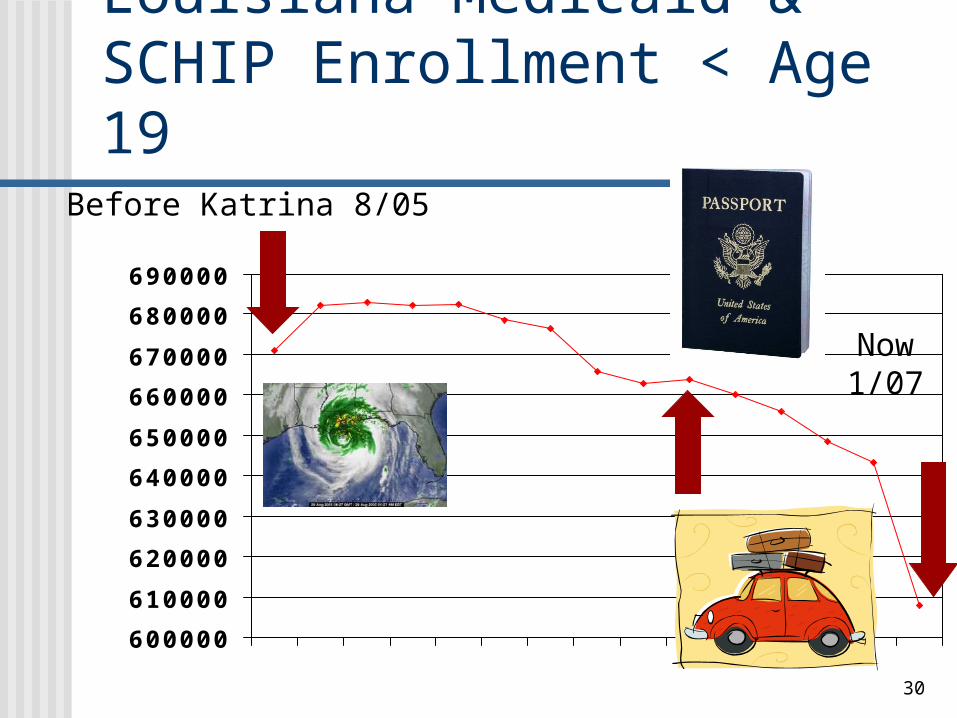
Louisiana Medicaid & SCHIP Enrollment < Age 19
600000
610000
620000
630000
640000
650000
660000
670000
680000
690000
Before Katrina 8/05
Now1/07
31
“Success isn’t Permanent”Challenge of Sustaining Improvements
Reversals being driven at the federal level— DRA citizenship & identify documentation requirements
Vigilant monitoring of enrollment data Dramatic & rapid reduction in children
enrolled since July 2006 Ongoing process improvement and
adjustments are critically important Renewal and retention must continue to be a
major focus
32
Ruth KennedyLaCHIP Director & Medicaid Deputy DirectorLouisiana Department of Health & HospitalsP.O. Box 91030 Baton Rouge, LA 70821-9030Telephone: 225 342 3032Fax: 225 342 9508E-Mail: rkennedy @ dhh.la.gov www.lachip.org
Never doubt that a small group of thoughtful, caring people can change the world Indeed, it is the only thing that ever has !— Dr. Margaret Mead





























