Embed Size (px)
Citation preview
© 2013 Kilpatrick Companies, LLC. All Rights Reserved.
UnitedHealthcare Enrollment Kit
General Info
Producer: Email:
Phone: Fax:
Group Name: Effective:
Submission Checklist
document/item doc # revised
Product and Benefit Selection Form – Signed by Employer MT-1015728.0 04-18
Employer Application for Small Business – Completed and signed by both Employer and Broker. 275-8892 12-17
Proof of Payroll and Legal Business Documentation Most recent Quarterly Wage & Tax Statement – For 2-9 eligible employee groups
--or--
Participation & Floor Certification – For 10+ eligible employee groups in lieu of TWC report
08-16
Direct Debit Authorization Form – Required for 1 or 2 lives enrolling 100-8513 04-11
Common Law Employee and Fact Attestation Form – If applicable. Required if covering 1099
contractors.
1099 Letter 04-18
Common Ownership Certificate – If applicable. Required if combining subsidiary & affiliated companies. 05-14
PEO Questionnaire – If applicable. Required if group is part of a PEO or Employee Leasing Company. 10-14
First month’s premium check payable to UnitedHealthcare Cannot accept temporary check, personal checks, money orders, or credit cards.
Last billing statement from current carrier[s] – Only needed for ancillary only groups. Medical only
groups do not need to supply prior carrier billing 07-14
Original Proposal – For all lines of coverage selected
Employee Enrollment Forms – Required for all eligible including waivers and declinations. Spreadsheet
Enrollment Available
275-8893 12-15
Contact
Submit Paperwork to Kilpatrick Companies, LLC 1050 Wilcrest Dr. Houston, TX 77042
Call 800-833-8478
Internet www.kilpatrickcos.com

Texas Small Business Groups with 1-50 ATNEProduct and Benefit Selection Form UnitedHealthcare Multi-Choice®
Medical Plan
Package Number _________________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Medical Plan Code ________________ RX Code ________
Billing Type Paper billing Online only/e-Bill Electronic Funds Transfer **Billing cycle – For 15th of the month effective date, please select 1st or 15th of the month billing cycle: 1st 15th
PLEASE NOTE: Please refer to the Health Plan Product Offering for a complete list of the Multi-choice packages available. Please indicate which package and the plans within the package that are being offered to employees. A group may offer multiple plans; however, they must be within the same package.
Dental Plan
Plan Code Not elected
Plan Code Not elected
Vision Plan
Plan Code Not elected
Plan Code Not elected
Signature
TEXAS INSURANCE LAWS REQUIRE ALL CARRIERS IN THE SMALL GROUP MARKET TO ISSUE ANY HEALTH BENEFIT PLAN IT MARKETS IN TEXAS TO SMALL EMPLOYERS OF 1-50 (ATNE) EMPLOYEES INCLUDING A BASIC OR STANDARD HEALTH BENEFIT, UPON THE REQUEST OF A SMALL EMPLOYER TO THE ENTIRE SMALL GROUP, REGARDLESS OF THE HEALTH STATUS OF ANY OF THE INDIVIDUALS IN THE GROUP. The answers provided in this Product and Benefit Selection Form are accurate and complete to the best of my knowledge and belief, and the Insurer shall rely and act upon them accordingly. This Product and Benefit Selection Form must accompany the Employer Application for Small Business. Any person who knowingly and with intent to injure, defraud, or deceive any insurer, files a statement of claim or an application containing any false, incomplete or misleading information is guilty of a felony of the third degree.
Employer Signature Group Name Date Signed
MT-1015728.0 04/27/18 ©2018 United HealthCare Services, Inc. 16-1704-B
Basic Life Amount
Employee: Dependent:
Flat Amounts Not elected Spouse $ Not elected 1x Salary Child(ren) 2x Salary Please indicate salary amount on enrollment form for each employee for multiple of salary life.
Supplemental Coverage
Life/AD&D $ STD/LTD $ (Indicate plan codes)
Life/AD&D $ STD/LTD $ (Indicate plan codes)
Life/AD&D $ STD/LTD $ (Indicate plan codes)
• Complete addendum to Employer Application for Supplemental Life and Disability Lines of Coverage.• Life/AD&D applies to groups with over 10 eligibles; maximum amount is $100,000.• Supplemental Life must be sold with Basic Life.• Please indicate salary amount on enrollment form for each employee for disability and multiple of salary life
Optional State Rider Selection
Please review the offers below and indicate your acceptance or rejection. Additional premium will be charged for the additional benefits chosen.
In Vitro Fertilization
A health benefit that provides pregnancy-related benefits for individuals covered under the plan shall offer and make available to each holder or sponsor of the plan coverage for services and benefits on an expense incurred, service, or prepaid basis for outpatient expenses that arise from in vitro fertilization procedures. Benefits for in vitro fertilization procedures must be provided to the same extent as benefits provided for other pregnancy-related procedures under the plan. The coverage is required only if the patient for the in vitro fertilization procedure is an individual covered under the group health benefit plan; the fertilization or attempted fertilization of the patient’s ocytes is made only with the sperm of the patient’s spouse; the patient and the patient’s spouse have a history of infertility of at least five continuous years’ duration or the infertility is associated with endometriosis, exposure in utero to diethylstilbestrol (DES), blockage of or surgical removal of one or both fallopian tubes, or oligospermia; the patient has been unable to attain a successful pregnancy through any less-costly applicable infertility treatments for which coverage is available under the group health benefit plan; and the in vitro fertilization procedures are performed at a medical facility that conforms to the minimal standards for programs of in vitro fertilization adopted by the American Society for Reproductive Medicine.
In Vitro Fertilization: Accept Reject
Texas plans only
Page 1 of 4
Group’s Legal Name
Group Name to appear on ID card (maximum 30 characters)
Street Address Tax ID
City State Zip Code Names of Owners/Partners (if applicable) Internet access?�� Yes �� No
Contact Person Email Address # of Years in Business
Billing Address (If Different) Telephone Fax
Multi-Location Group* # Locations Address(es) (or list on additional sheet of paper)�� Yes �� No
*If the majority of your employees are not located in your state of application, UnitedHealthcare policies and/or state law may require that yourpolicy be written out of a different state and/or that your benefit plans vary.Organization Type �� Partnership �� C-Corp �� S-Corp �� LLC �� LLP �� Sole Proprietor Medical Benefit Domestic Partner �� Other_________________________________________ Plan Option CoverageDid you have any employees other than yourself and your spouse during the preceding �� Calendar Year �� Yes �� Nocalendar year? �� Yes �� No �� Policy YearWaiting Period for new hires �� 1st of Policy Month following Date of Hire Waiting Period waived
�� 1st of Policy Month following ____ �� months �� days of employment for initial enrollees �� Date of Hire (no waiting period) �� Yes �� No�� ____ �� months �� days of employment following Date of Hire
Classes Excluded: �� None �� Union �� Hourly Nature of Business Industry (SIC) Code�� Non-Management �� Salary
Have Workers’ Comp Workers’ Comp Carrier Name Names of Owners/Partners not covered by Workers’ Comp:�� Yes �� NoNames of Persons currently on COBRA/Continuation, and/or Short/Long Term Disability:�� See Attached List �� None
To avoid processing delays, please make sure you:1 Answer all questions completely and accurately.2 Complete and submit the Product and Benefit Selection Form, if applicable.3 Submit the most recent billing statement listing those currently insured and current status.4 Submit most recent wage and tax information.5 Include a deposit check for any required premiums.6 DO NOT CANCEL YOUR EXISTING COVERAGE UNTIL YOU RECEIVE WRITTEN NOTIFICATION OF APPROVAL.
Employer Application for Small Business
SG.ER.17.TX 4/17 275-8892 12/17
General Information
(DO NOT STAPLE)
Requested Effective Date
Coverage Provided by “UnitedHealthcare and Affiliates”: Medical coverage provided by UnitedHealthcare Insurance Company (PPO, Indemnity) or UnitedHealthcare of Texas, Inc. (HMO)Dental coverage provided by UnitedHealthcare Insurance Company (Indemnity), National Pacific Dental, Inc. (HMO)Life, Short-Term Disability (STD), Long-Term Disability (LTD) Insurance coverage provided by UnitedHealthcare Insurance CompanyVision coverage provided by UnitedHealthcare Insurance Company
Texas
(Waiting period for medicalcoverage cannot exceed 90 days)
UnitedHealthcare Insurance CompanyUnitedHealthcare of Texas, Inc.
National Pacific Dental, Inc.
Notice for Small Employers who select a Consumer Choice plan:You have the option to choose this Consumer Choice of Benefits Health Insurance Plan or Health MaintenanceOrganization health care plan that, either in whole or in part, does not provide state-mandated health benefits normallyrequired in evidences of coverage or accident and sickness policies in Texas. This standard health benefit plan mayprovide a more affordable health plan for you although, at the same time, it may provide you with fewer health planbenefits than those normally included as state-mandated health benefits in Texas. If you choose this standard healthbenefit plan, please consult with your insurance agent to discover which state-mandated health benefits are excludedin this evidence of coverage or policy.
(Does not apply tohealth benefit plans.)
Group Name_________________________________________________________________________________________________________
Page 2 of 4
UnitedHealthcare’s Leave of Absence (LOA) Policy; Eligibility for Medical CoverageIf the employee is on an employer approved leave of absence and the employer continues to pay required medical premiums, the coverage willremain in force for: (1) No longer than 13 consecutive weeks for non-medical leaves (i.e. temporarily laid-off). (2) No longer than 26consecutive weeks for a medical leave. Coverage may be extended for a longer period of time, if required by local, state or federal rules. If the employee’s medical coverage terminates under this LOA policy, the employee may exercise the rights under any applicable Continuationof Medical Coverage provision or the Conversion of Medical Benefits provision described in the Certificate of Coverage.Do you continue medical coverage during a leave of absence (not including state continuation or COBRA coverage)?___ Yes, we continue medical coverage during an approved leave of absence for full time** employees (as defined on page 2).___ No, we do not offer medical coverage during a leave of absence.
General Information (continued)
# Employees # Employees Employer Employer Applying for: Waiving for: % % for Dep
# Eligible Employees Medical Medical Medical# Ineligible Employees Dental Dental DentalTotal # Employees Vision Vision Vision
Basic Life/AD&D Basic Life/AD&D Basic Life/AD&DDep Life Dep Life Dep LifeSupp Life/AD&D Supp Life/AD&D Supp Life/AD&DSupp Dep Life/AD&D Supp Dep Life/AD&D Supp Dep Life/AD&DSTD STD STDLTD LTD LTDOther Other Other
Participation Contribution
# Hours per week to be eligible** ________
**A person is considered aneligible employee if the employeeusually works at least 30 hours perweek.For Disability products theminimum # of work hours per weekto be eligible is 30 hours.
Health Savings Account (if selected): Which bank will be used: �� OptumBank �� Other
Do you currently offer or intend to offer a Health Reimbursement Account (HRA) plan and/or comprehensive supplemental insurancepolicy or funding arrangement in addition to this UnitedHealthcare medical plan? Answers must be accurate whether purchased from UnitedHealthcare or any other insurer or third party administrator. HRA �� Yes �� No If yes, please identify type: �� UnitedHealthcare HRA (any HRA design offered through UnitedHealthcare) �� Other Administrator HRA HRA plans administered by other insurers or third party administrators must comply with UnitedHealthcare HRA design standards.Comprehensive Supplemental Insurance Policy or Funding Arrangement �� Yes �� NoIf you answered "Yes" to either question above, you must choose from the list of UnitedHealthcare HRA-eligible medical plans as shown to youby your broker or agent. Other plans are not eligible for pairing with these arrangements. Purchase of such arrangements at any point duringthe duration of this policy will require you to notify UnitedHealthcare.
Consumer Driven Health Plan Options
�� Yes Subject to ERISA? (Most private sector plans are ERISA plans)�� No If No, please indicate appropriate category:
�� Church (Additional information needed) �� Federal Government�� Indian Tribe – Commercial Business �� Non-Federal Government (State, Local or Tribal Gov.)�� Foreign Government/Foreign Embassy �� Non-ERISA Other ________________________________________
Group Name_________________________________________________________________________________________________________
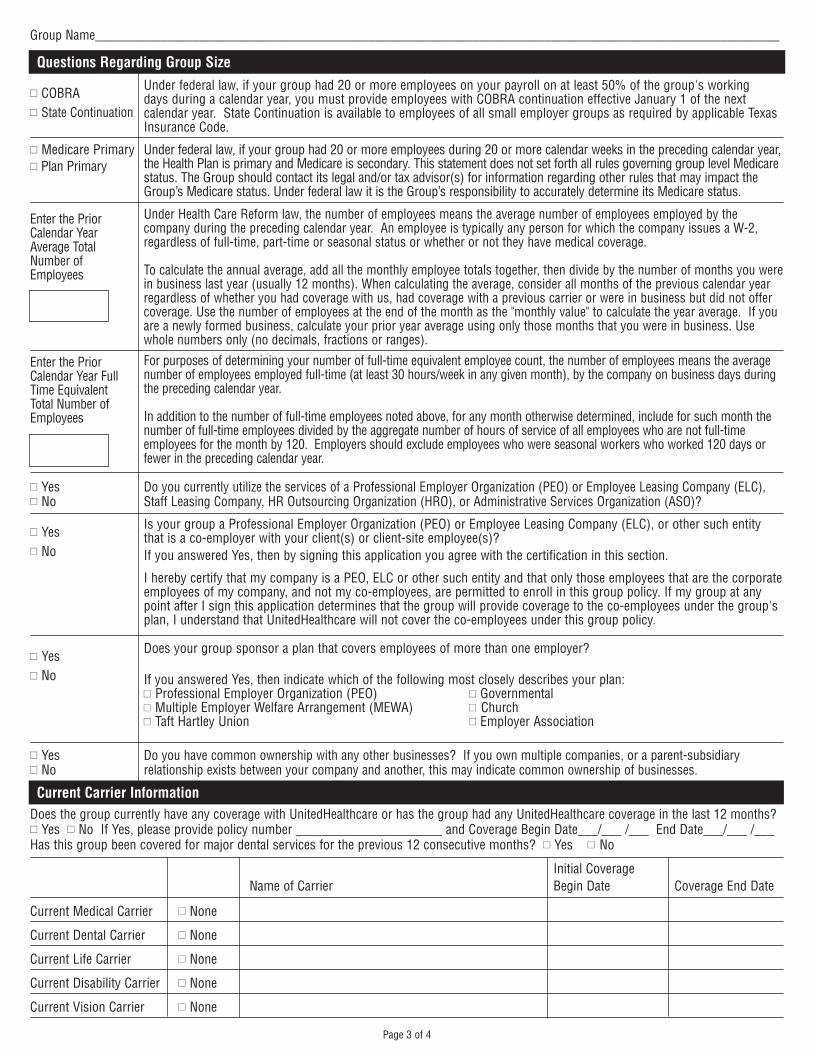
Does the group currently have any coverage with UnitedHealthcare or has the group had any UnitedHealthcare coverage in the last 12 months?�� Yes �� No If Yes, please provide policy number ______________________ and Coverage Begin Date___/___ /___ End Date___/___ /___Has this group been covered for major dental services for the previous 12 consecutive months? �� Yes �� No
Initial CoverageName of Carrier Begin Date Coverage End Date
Current Medical Carrier �� None
Current Dental Carrier �� None
Current Life Carrier �� None
Current Disability Carrier �� None
Current Vision Carrier �� None
Current Carrier Information
Page 3 of 4
�� COBRA Under federal law, if your group had 20 or more employees on your payroll on at least 50% of the group's working
�� State Continuationdays during a calendar year, you must provide employees with COBRA continuation effective January 1 of the nextcalendar year. State Continuation is available to employees of all small employer groups as required by applicable TexasInsurance Code.
�� Medicare Primary Under federal law, if your group had 20 or more employees during 20 or more calendar weeks in the preceding calendar year,�� Plan Primary the Health Plan is primary and Medicare is secondary. This statement does not set forth all rules governing group level Medicare
status. The Group should contact its legal and/or tax advisor(s) for information regarding other rules that may impact the Group’s Medicare status. Under federal law it is the Group’s responsibility to accurately determine its Medicare status.
Under Health Care Reform law, the number of employees means the average number of employees employed by thecompany during the preceding calendar year. An employee is typically any person for which the company issues a W-2,regardless of full-time, part-time or seasonal status or whether or not they have medical coverage.
To calculate the annual average, add all the monthly employee totals together, then divide by the number of months you werein business last year (usually 12 months). When calculating the average, consider all months of the previous calendar yearregardless of whether you had coverage with us, had coverage with a previous carrier or were in business but did not offercoverage. Use the number of employees at the end of the month as the "monthly value" to calculate the year average. If youare a newly formed business, calculate your prior year average using only those months that you were in business. Usewhole numbers only (no decimals, fractions or ranges).
Questions Regarding Group Size
For purposes of determining your number of full-time equivalent employee count, the number of employees means the averagenumber of employees employed full-time (at least 30 hours/week in any given month), by the company on business days duringthe preceding calendar year.
In addition to the number of full-time employees noted above, for any month otherwise determined, include for such month thenumber of full-time employees divided by the aggregate number of hours of service of all employees who are not full-timeemployees for the month by 120. Employers should exclude employees who were seasonal workers who worked 120 days orfewer in the preceding calendar year.
�� Yes Do you currently utilize the services of a Professional Employer Organization (PEO) or Employee Leasing Company (ELC),�� No Staff Leasing Company, HR Outsourcing Organization (HRO), or Administrative Services Organization (ASO)?
�� Yes Is your group a Professional Employer Organization (PEO) or Employee Leasing Company (ELC), or other such entity
�� Nothat is a co-employer with your client(s) or client-site employee(s)? If you answered Yes, then by signing this application you agree with the certification in this section.
I hereby certify that my company is a PEO, ELC or other such entity and that only those employees that are the corporateemployees of my company, and not my co-employees, are permitted to enroll in this group policy. If my group at anypoint after I sign this application determines that the group will provide coverage to the co-employees under the group'splan, I understand that UnitedHealthcare will not cover the co-employees under this group policy.
�� Yes Does your group sponsor a plan that covers employees of more than one employer?
�� No If you answered Yes, then indicate which of the following most closely describes your plan:�� Professional Employer Organization (PEO) �� Governmental�� Multiple Employer Welfare Arrangement (MEWA) �� Church�� Taft Hartley Union �� Employer Association
�� Yes Do you have common ownership with any other businesses? If you own multiple companies, or a parent-subsidiary �� No relationship exists between your company and another, this may indicate common ownership of businesses.
Enter the PriorCalendar YearAverage TotalNumber ofEmployees
Enter the PriorCalendar Year FullTime EquivalentTotal Number ofEmployees
Group Name_________________________________________________________________________________________________________
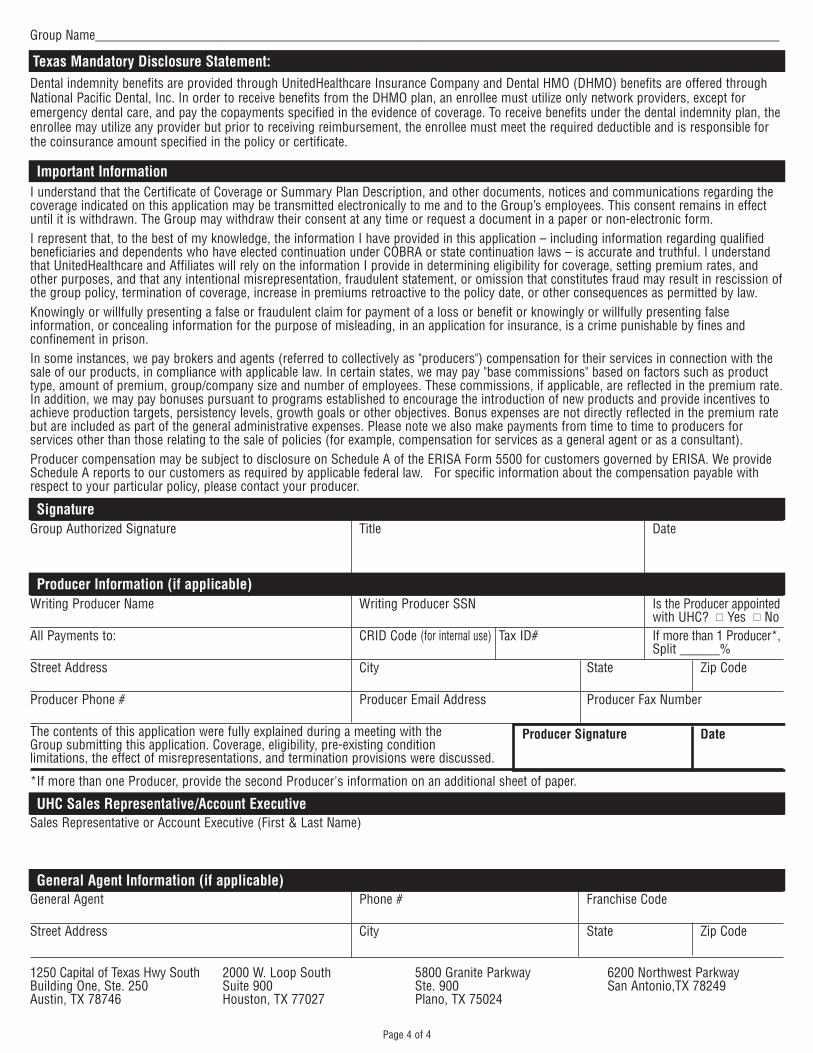
I understand that the Certificate of Coverage or Summary Plan Description, and other documents, notices and communications regarding thecoverage indicated on this application may be transmitted electronically to me and to the Group’s employees. This consent remains in effectuntil it is withdrawn. The Group may withdraw their consent at any time or request a document in a paper or non-electronic form.I represent that, to the best of my knowledge, the information I have provided in this application – including information regarding qualifiedbeneficiaries and dependents who have elected continuation under COBRA or state continuation laws – is accurate and truthful. I understandthat UnitedHealthcare and Affiliates will rely on the information I provide in determining eligibility for coverage, setting premium rates, andother purposes, and that any intentional misrepresentation, fraudulent statement, or omission that constitutes fraud may result in rescission ofthe group policy, termination of coverage, increase in premiums retroactive to the policy date, or other consequences as permitted by law.Knowingly or willfully presenting a false or fraudulent claim for payment of a loss or benefit or knowingly or willfully presenting falseinformation, or concealing information for the purpose of misleading, in an application for insurance, is a crime punishable by fines andconfinement in prison.In some instances, we pay brokers and agents (referred to collectively as "producers") compensation for their services in connection with thesale of our products, in compliance with applicable law. In certain states, we may pay "base commissions" based on factors such as producttype, amount of premium, group/company size and number of employees. These commissions, if applicable, are reflected in the premium rate.In addition, we may pay bonuses pursuant to programs established to encourage the introduction of new products and provide incentives toachieve production targets, persistency levels, growth goals or other objectives. Bonus expenses are not directly reflected in the premium ratebut are included as part of the general administrative expenses. Please note we also make payments from time to time to producers forservices other than those relating to the sale of policies (for example, compensation for services as a general agent or as a consultant). Producer compensation may be subject to disclosure on Schedule A of the ERISA Form 5500 for customers governed by ERISA. We provideSchedule A reports to our customers as required by applicable federal law. For specific information about the compensation payable withrespect to your particular policy, please contact your producer.
Important Information
Group Authorized Signature Title DateSignature
Writing Producer Name Writing Producer SSN Is the Producer appointedwith UHC? �� Yes �� No
All Payments to: CRID Code (for internal use) Tax ID# If more than 1 Producer*,Split ______%
Street Address City State Zip Code
Producer Phone # Producer Email Address Producer Fax Number
The contents of this application were fully explained during a meeting with the Producer Signature DateGroup submitting this application. Coverage, eligibility, pre-existing condition limitations, the effect of misrepresentations, and termination provisions were discussed.
Producer Information (if applicable)
*If more than one Producer, provide the second Producer's information on an additional sheet of paper.
Page 4 of 4
Dental indemnity benefits are provided through UnitedHealthcare Insurance Company and Dental HMO (DHMO) benefits are offered throughNational Pacific Dental, Inc. In order to receive benefits from the DHMO plan, an enrollee must utilize only network providers, except foremergency dental care, and pay the copayments specified in the evidence of coverage. To receive benefits under the dental indemnity plan, theenrollee may utilize any provider but prior to receiving reimbursement, the enrollee must meet the required deductible and is responsible forthe coinsurance amount specified in the policy or certificate.
Texas Mandatory Disclosure Statement:
Sales Representative or Account Executive (First & Last Name)UHC Sales Representative/Account Executive
General Agent Phone # Franchise Code
Street Address City State Zip Code
General Agent Information (if applicable)
1250 Capital of Texas Hwy SouthBuilding One, Ste. 250Austin, TX 78746
2000 W. Loop SouthSuite 900Houston, TX 77027
5800 Granite ParkwaySte. 900Plano, TX 75024
6200 Northwest ParkwaySan Antonio,TX 78249
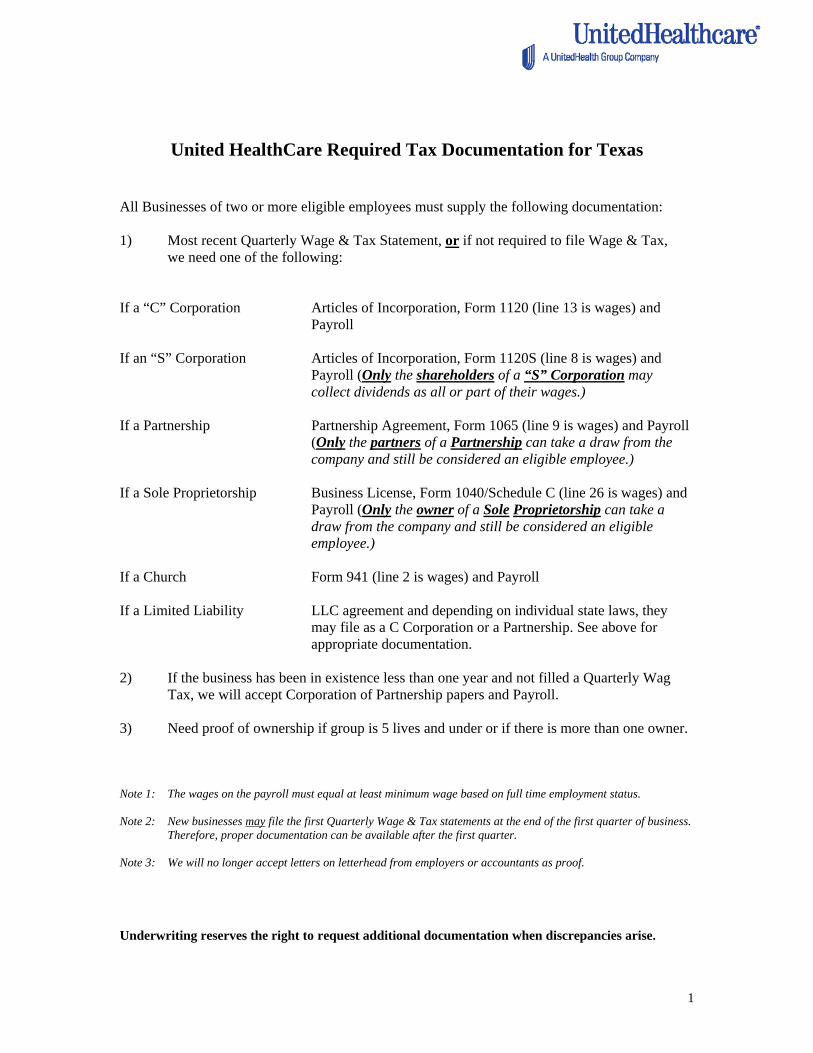
United HealthCare Required Tax Documentation for Texas
All Businesses of two or more eligible employees must supply the following documentation: 1) Most recent Quarterly Wage & Tax Statement, or if not required to file Wage & Tax,
we need one of the following: If a “C” Corporation Articles of Incorporation, Form 1120 (line 13 is wages) and
Payroll If an “S” Corporation Articles of Incorporation, Form 1120S (line 8 is wages) and
Payroll (Only the shareholders of a “S” Corporation may collect dividends as all or part of their wages.)
If a Partnership Partnership Agreement, Form 1065 (line 9 is wages) and Payroll
(Only the partners of a Partnership can take a draw from the company and still be considered an eligible employee.)
If a Sole Proprietorship Business License, Form 1040/Schedule C (line 26 is wages) and
Payroll (Only the owner of a Sole Proprietorship can take a draw from the company and still be considered an eligible employee.)
If a Church Form 941 (line 2 is wages) and Payroll If a Limited Liability LLC agreement and depending on individual state laws, they
may file as a C Corporation or a Partnership. See above for appropriate documentation.
2) If the business has been in existence less than one year and not filled a Quarterly Wag
Tax, we will accept Corporation of Partnership papers and Payroll. 3) Need proof of ownership if group is 5 lives and under or if there is more than one owner. Note 1: The wages on the payroll must equal at least minimum wage based on full time employment status. Note 2: New businesses may file the first Quarterly Wage & Tax statements at the end of the first quarter of business.
Therefore, proper documentation can be available after the first quarter. Note 3: We will no longer accept letters on letterhead from employers or accountants as proof. Underwriting reserves the right to request additional documentation when discrepancies arise.
1
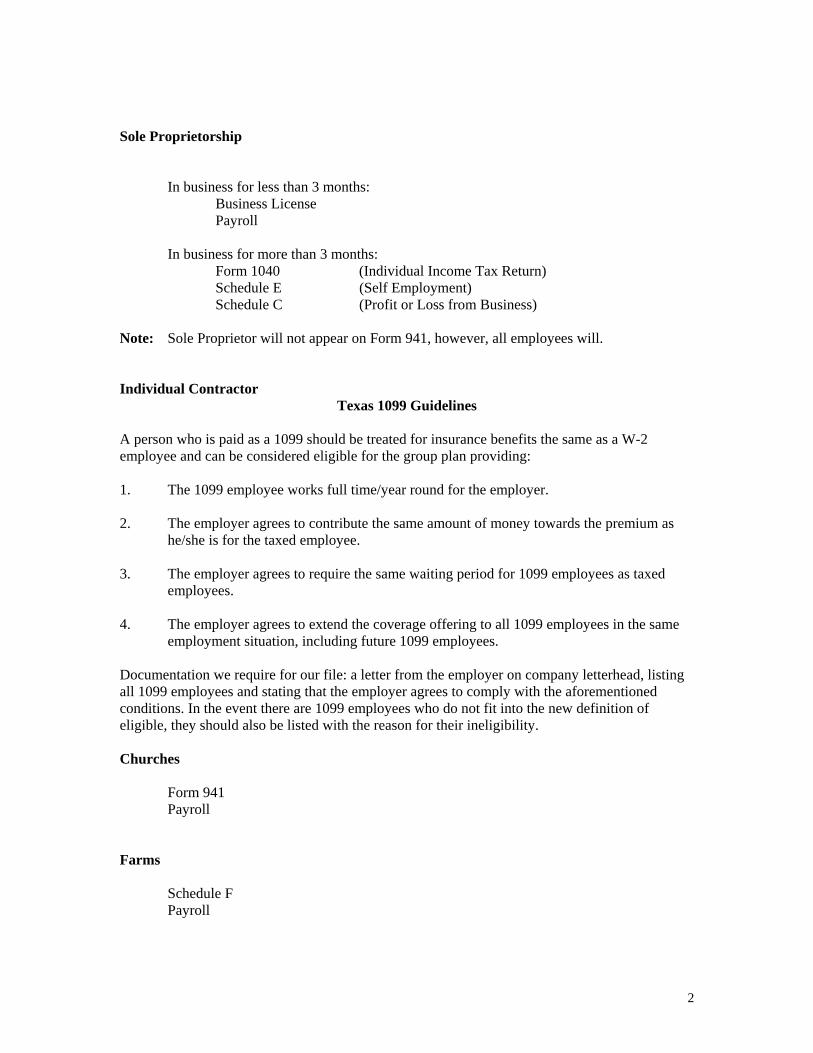
Sole Proprietorship In business for less than 3 months: Business License Payroll In business for more than 3 months: Form 1040 (Individual Income Tax Return) Schedule E (Self Employment) Schedule C (Profit or Loss from Business) Note: Sole Proprietor will not appear on Form 941, however, all employees will. Individual Contractor
Texas 1099 Guidelines A person who is paid as a 1099 should be treated for insurance benefits the same as a W-2 employee and can be considered eligible for the group plan providing: 1. The 1099 employee works full time/year round for the employer. 2. The employer agrees to contribute the same amount of money towards the premium as
he/she is for the taxed employee. 3. The employer agrees to require the same waiting period for 1099 employees as taxed
employees. 4. The employer agrees to extend the coverage offering to all 1099 employees in the same
employment situation, including future 1099 employees. Documentation we require for our file: a letter from the employer on company letterhead, listing all 1099 employees and stating that the employer agrees to comply with the aforementioned conditions. In the event there are 1099 employees who do not fit into the new definition of eligible, they should also be listed with the reason for their ineligibility. Churches Form 941 Payroll Farms Schedule F Payroll
2
CHEAT SHEET FOR TEXAS TAX DOCUMENTS
The following is a list of available tax documents filed for various organizational types: “C” Corporation In business for less than 3 months: Articles of Incorporation Payroll In business for more than 3 months: Form 1120 Line 13 = wages (Corporation Income Tax Return) Form 941 Line 2 = wages (Quarterly Federal Tax Return) “S” Corporation In business for less than 3 months: Articles of Incorporation Payroll In business for more than 3 months: Form 1120S (Tax Return for an S Corporation) Schedule K1 (Shareholders Share of Income) Form 941 (If employees besides the shareholders) Partnership In business for less than 3 months: Partnership Agreement Payroll In business for more than 3 months: Form 1065 (Partnership Return of Income) Schedule K1 (Partner’s Share of Income) Schedule SE (Self Employment Tax) Note: General Partners will not have Form 941. Income information will be founded on Schedule K1 – Line 15A. Limited Liability Company (LLC) Depending on individual state laws, they may file as a C Corporation or a Partnership. See above for appropriate documentation.
3
1/14/2013
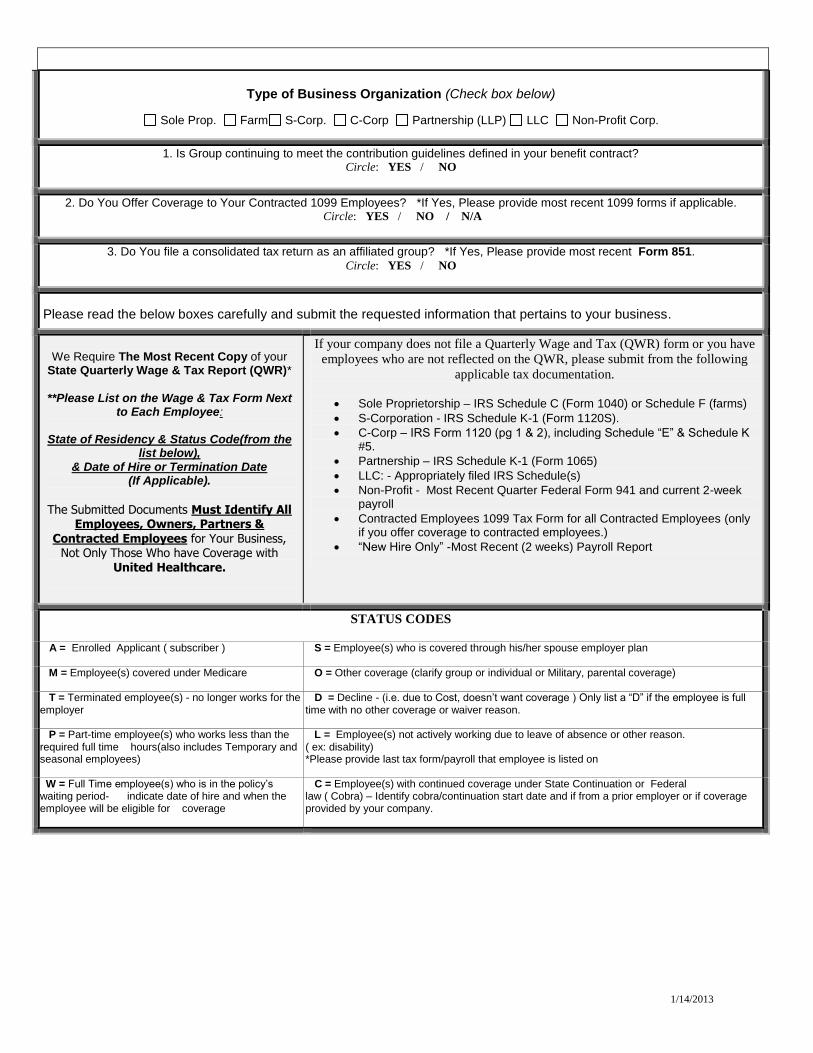
Type of Business Organization (Check box below)
Sole Prop. Farm S-Corp. C-Corp Partnership (LLP) LLC Non-Profit Corp.
1. Is Group continuing to meet the contribution guidelines defined in your benefit contract? Circle: YES / NO
2. Do You Offer Coverage to Your Contracted 1099 Employees? *If Yes, Please provide most recent 1099 forms if applicable. Circle: YES / NO / N/A
3. Do You file a consolidated tax return as an affiliated group? *If Yes, Please provide most recent Form 851. Circle: YES / NO
Please read the below boxes carefully and submit the requested information that pertains to your business.
We Require The Most Recent Copy of your
State Quarterly Wage & Tax Report (QWR)*
**Please List on the Wage & Tax Form Next
to Each Employee:
State of Residency & Status Code(from the list below),
& Date of Hire or Termination Date (If Applicable).
The Submitted Documents Must Identify All
Employees, Owners, Partners & Contracted Employees for Your Business,
Not Only Those Who have Coverage with United Healthcare.
If your company does not file a Quarterly Wage and Tax (QWR) form or you have
employees who are not reflected on the QWR, please submit from the following
applicable tax documentation.
Sole Proprietorship – IRS Schedule C (Form 1040) or Schedule F (farms)
S-Corporation - IRS Schedule K-1 (Form 1120S).
C-Corp – IRS Form 1120 (pg 1 & 2), including Schedule “E” & Schedule K #5.
Partnership – IRS Schedule K-1 (Form 1065)
LLC: - Appropriately filed IRS Schedule(s)
Non-Profit - Most Recent Quarter Federal Form 941 and current 2-week payroll
Contracted Employees 1099 Tax Form for all Contracted Employees (only if you offer coverage to contracted employees.)
“New Hire Only” -Most Recent (2 weeks) Payroll Report
STATUS CODES
A = Enrolled Applicant ( subscriber ) S = Employee(s) who is covered through his/her spouse employer plan
M = Employee(s) covered under Medicare
O = Other coverage (clarify group or individual or Military, parental coverage)
T = Terminated employee(s) - no longer works for the employer
D = Decline - (i.e. due to Cost, doesn’t want coverage ) Only list a “D” if the employee is full time with no other coverage or waiver reason.
P = Part-time employee(s) who works less than the required full time hours(also includes Temporary and seasonal employees)
L = Employee(s) not actively working due to leave of absence or other reason. ( ex: disability) *Please provide last tax form/payroll that employee is listed on
W = Full Time employee(s) who is in the policy’s waiting period- indicate date of hire and when the employee will be eligible for coverage
C = Employee(s) with continued coverage under State Continuation or Federal law ( Cobra) – Identify cobra/continuation start date and if from a prior employer or if coverage provided by your company.
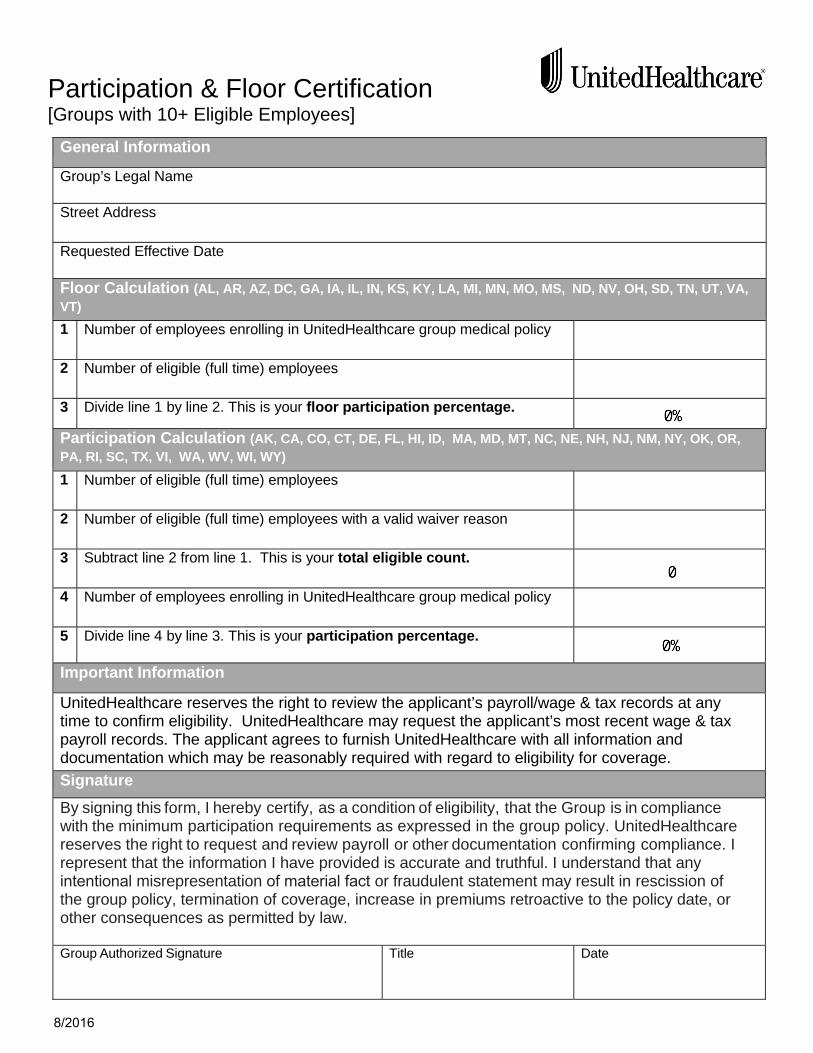
Participation & Floor Certification [Groups with 10+ Eligible Employees]
General Information
Group’s Legal Name
Street Address
Requested Effective Date
Floor Calculation (AL, AR, AZ, DC, GA, IA, IL, IN, KS, KY, LA, MI, MN, MO, MS, ND, NV, OH, SD, TN, UT, VA,
VT)
1 Number of employees enrolling in UnitedHealthcare group medical policy
2 Number of eligible (full time) employees
3 Divide line 1 by line 2. This is your floor participation percentage.
Participation Calculation (AK, CA, CO, CT, DE, FL, HI, ID, MA, MD, MT, NC, NE, NH, NJ, NM, NY, OK, OR,
PA, RI, SC, TX, VI, WA, WV, WI, WY)
1 Number of eligible (full time) employees
2 Number of eligible (full time) employees with a valid waiver reason
3 Subtract line 2 from line 1. This is your total eligible count.
4 Number of employees enrolling in UnitedHealthcare group medical policy
5 Divide line 4 by line 3. This is your participation percentage.
Important Information
UnitedHealthcare reserves the right to review the applicant’s payroll/wage & tax records at any time to confirm eligibility. UnitedHealthcare may request the applicant’s most recent wage & tax payroll records. The applicant agrees to furnish UnitedHealthcare with all information and documentation which may be reasonably required with regard to eligibility for coverage.
Signature
By signing this form, I hereby certify, as a condition of eligibility, that the Group is in compliance with the minimum participation requirements as expressed in the group policy. UnitedHealthcare reserves the right to request and review payroll or other documentation confirming compliance. I represent that the information I have provided is accurate and truthful. I understand that any intentional misrepresentation of material fact or fraudulent statement may result in rescission of the group policy, termination of coverage, increase in premiums retroactive to the policy date, or other consequences as permitted by law.
Group Authorized Signature Title Date
8/2016
Sign up for UnitedHealthcare’s Scheduled Direct Debit and have your
premium payments automatically deducted from your bank account.
If you’re looking for new and better ways to help organize, streamline and generally make your job easier, there’s no better place to start than with UnitedHealthcare’s Scheduled Direct Debit.
That’s because Scheduled Direct Debit is a safe, convenient and automatic way to pay your monthly insurance premiums.
All you do is sign up, then every month we automatically deduct your premium from your company’s bank account.
Even better, Scheduled Direct Debit helps you better organize your payment records, streamlines your monthly invoice payment process and frees you up to get on with the business of your business.
Enroll today in UnitedHealthcare’s Scheduled Direct Debit program. Just fill
in the simple form on the reverse side and return it to us. Do it today. And
give yourself one less thing to worry about.
Employer eServices Scheduled Direct Debit
Get organized.
Get streamlined.
Get UnitedHealthcare’s
Scheduled Direct Debit.
Scheduled Direct Debit:} Lets you pay your premium at the same time each month.
} Provides predictable cash outflow.
} Gives you a consistent process for your premium payment.
} Provides an accurate record of your payment listed right on your bank statement.
} Means you’ll never have to worry about missing an invoice or a deadline again. Everything’s taken care of. Automatically.
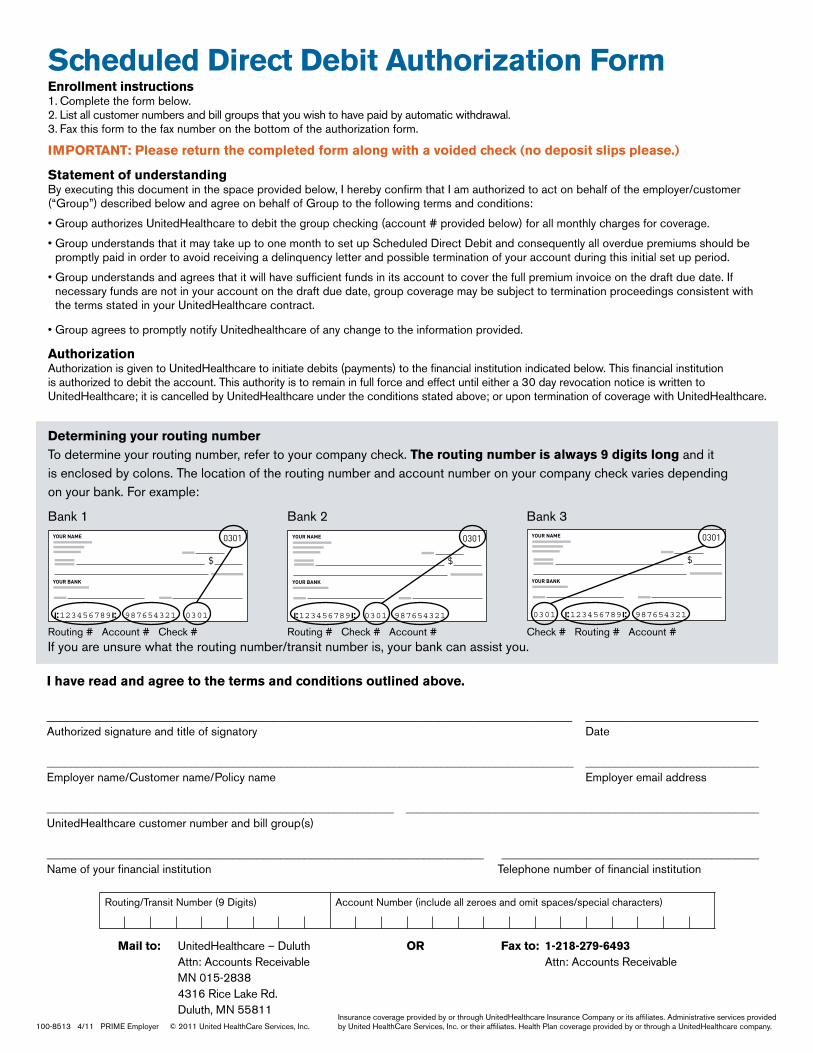
Enrollment instructions1. Complete the form below.2. List all customer numbers and bill groups that you wish to have paid by automatic withdrawal.3. Fax this form to the fax number on the bottom of the authorization form.
IMPORTANT: Please return the completed form along with a voided check (no deposit slips please.)
Statement of understandingBy executing this document in the space provided below, I hereby confirm that I am authorized to act on behalf of the employer/customer (“Group”) described below and agree on behalf of Group to the following terms and conditions:
• Group authorizes UnitedHealthcare to debit the group checking (account # provided below) for all monthly charges for coverage.
• Group understands that it may take up to one month to set up Scheduled Direct Debit and consequently all overdue premiums should be promptly paid in order to avoid receiving a delinquency letter and possible termination of your account during this initial set up period.
• Group understands and agrees that it will have sufficient funds in its account to cover the full premium invoice on the draft due date. If necessary funds are not in your account on the draft due date, group coverage may be subject to termination proceedings consistent with the terms stated in your UnitedHealthcare contract.
• Group agrees to promptly notify Unitedhealthcare of any change to the information provided.
Authorization Authorization is given to UnitedHealthcare to initiate debits (payments) to the financial institution indicated below. This financial institution is authorized to debit the account. This authority is to remain in full force and effect until either a 30 day revocation notice is written to UnitedHealthcare; it is cancelled by UnitedHealthcare under the conditions stated above; or upon termination of coverage with UnitedHealthcare.
Scheduled Direct Debit Authorization Form
I have read and agree to the terms and conditions outlined above.
_______________________________________________________________________________ __________________________Authorized signature and title of signatory Date
________________________________________________________________________________________ _____________________________Employer name/Customer name/Policy name Employer email address
__________________________________________________________ ___________________________________________________________UnitedHealthcare customer number and bill group(s)
_________________________________________________________________________ ___________________________________________Name of your financial institution Telephone number of financial institution
100-8513 4/11 PRIME Employer © 2011 United HealthCare Services, Inc.
Routing/Transit Number (9 Digits) Account Number (include all zeroes and omit spaces/special characters)
Determining your routing number To determine your routing number, refer to your company check. The routing number is always 9 digits long and it is enclosed by colons. The location of the routing number and account number on your company check varies depending on your bank. For example:
Bank 1 Bank 2 Bank 3
If you are unsure what the routing number/transit number is, your bank can assist you.Routing # Account # Check # Routing # Check # Account # Check # Routing # Account #
Mail to: UnitedHealthcare – Duluth OR Fax to: 1-218-279-6493 Attn: Accounts Receivable Attn: Accounts Receivable MN 015-2838 4316 Rice Lake Rd. Duluth, MN 55811
Insurance coverage provided by or through UnitedHealthcare Insurance Company or its affiliates. Administrative services provided by United HealthCare Services, Inc. or their affiliates. Health Plan coverage provided by or through a UnitedHealthcare company.
Employer eServices
Becoming a UnitedHealthcare customer has its privileges! As a UnitedHealthcare customer, the group contact listed on the Employer Group Application will automatically be enrolled in Employer eServices and emailed a User ID and Password. The Employer eServices Web site provides easy access to benefit administration, with 24 hour convenience to make benefit management simpler, easier and better!
With Employer eServices, you have real-time administration to:
Verify eligibility Review enrollment information Add employees and dependents Change eligibility Reinstate employees Terminate employees Request employee ID cards Select or Change Primary Care Physician (as required by plan) Delegate benefits administration work to additional staff
Once you receive your User ID and Password, simply go to www.employereservices.com.
We believe in putting the power of information into the hands of our customers!
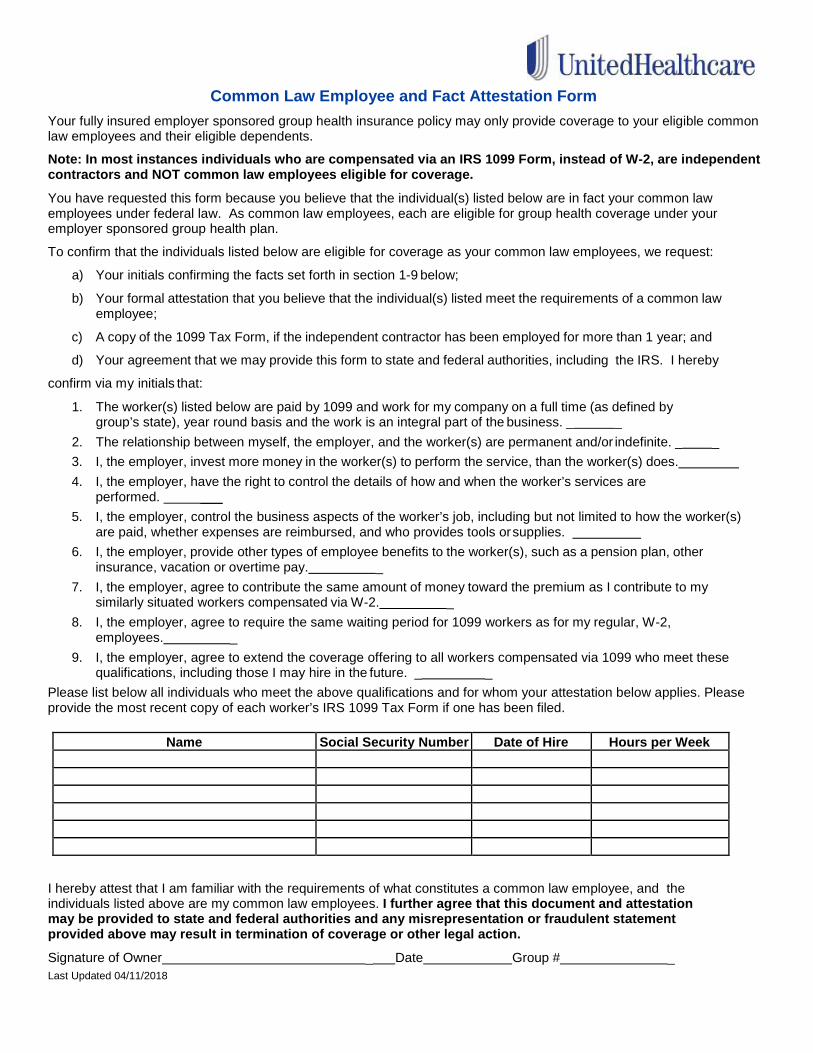
Common Law Employee and Fact Attestation Form
Your fully insured employer sponsored group health insurance policy may only provide coverage to your eligible common law employees and their eligible dependents.
Note: In most instances individuals who are compensated via an IRS 1099 Form, instead of W-2, are independent contractors and NOT common law employees eligible for coverage.
You have requested this form because you believe that the individual(s) listed below are in fact your common law employees under federal law. As common law employees, each are eligible for group health coverage under your employer sponsored group health plan.
To confirm that the individuals listed below are eligible for coverage as your common law employees, we request:
a) Your initials confirming the facts set forth in section 1-9 below;
b) Your formal attestation that you believe that the individual(s) listed meet the requirements of a common law employee;
c) A copy of the 1099 Tax Form, if the independent contractor has been employed for more than 1 year; and
d) Your agreement that we may provide this form to state and federal authorities, including the IRS. I hereby
confirm via my initials that:
1. The worker(s) listed below are paid by 1099 and work for my company on a full time (as defined by group’s state), year round basis and the work is an integral part of the business. _ _
2. The relationship between myself, the employer, and the worker(s) are permanent and/or indefinite. _ _ 3. I, the employer, invest more money in the worker(s) to perform the service, than the worker(s) does. 4. I, the employer, have the right to control the details of how and when the worker’s services are
performed. ___ 5. I, the employer, control the business aspects of the worker’s job, including but not limited to how the worker(s)
are paid, whether expenses are reimbursed, and who provides tools or supplies. 6. I, the employer, provide other types of employee benefits to the worker(s), such as a pension plan, other
insurance, vacation or overtime pay. _ 7. I, the employer, agree to contribute the same amount of money toward the premium as I contribute to my
similarly situated workers compensated via W-2. _ 8. I, the employer, agree to require the same waiting period for 1099 workers as for my regular, W-2,
employees. _ 9. I, the employer, agree to extend the coverage offering to all workers compensated via 1099 who meet these
qualifications, including those I may hire in the future. _ _ Please list below all individuals who meet the above qualifications and for whom your attestation below applies. Please provide the most recent copy of each worker’s IRS 1099 Tax Form if one has been filed.
Name Social Security Number Date of Hire Hours per Week
I hereby attest that I am familiar with the requirements of what constitutes a common law employee, and the individuals listed above are my common law employees. I further agree that this document and attestation may be provided to state and federal authorities and any misrepresentation or fraudulent statement provided above may result in termination of coverage or other legal action.
Signature of Owner _ Date Group # _ Last Updated 04/11/2018
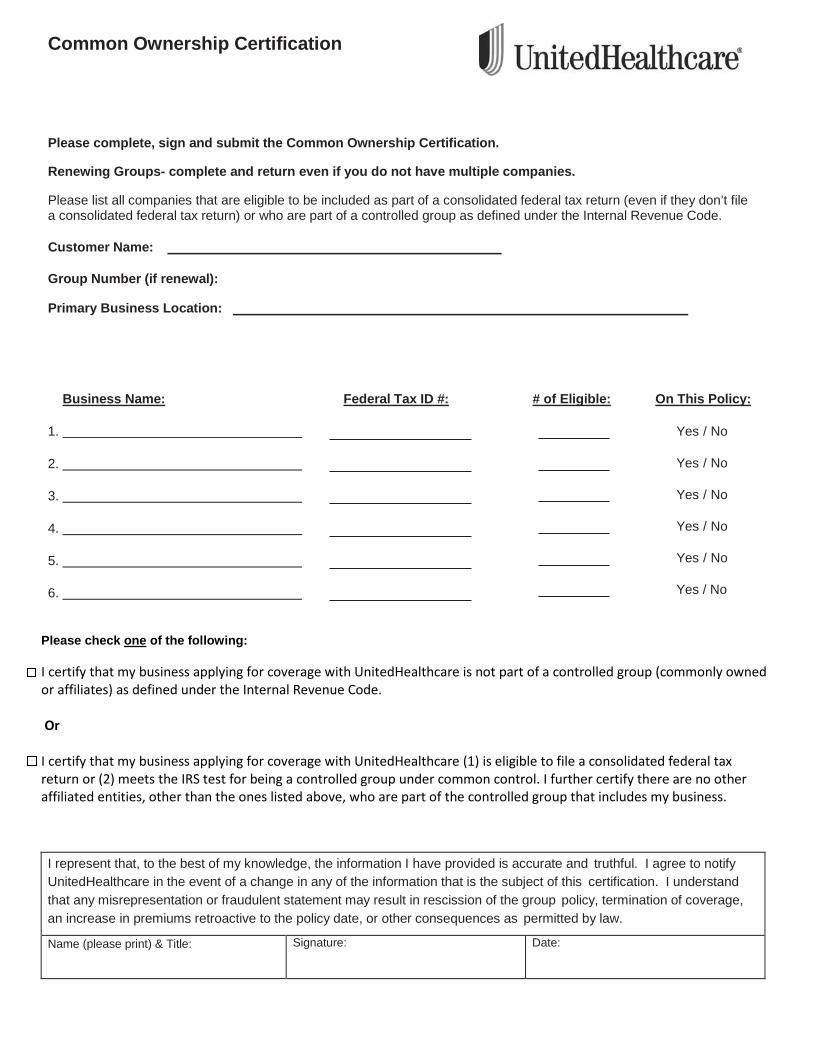
Common Ownership Certification Please complete, sign and submit the Common Ownership Certification.
Renewing Groups- complete and return even if you do not have multiple companies.
Please list all companies that are eligible to be included as part of a consolidated federal tax return (even if they don’t file a consolidated federal tax return) or who are part of a controlled group as defined under the Internal Revenue Code.
Customer Name:
Group Number (if renewal):
Primary Business Location:
Business Name: Federal Tax ID #: # of Eligible: On This Policy:
1.
2.
3.
4.
5.
6.
Please check one of the following:
Yes / No
Yes / No
Yes / No
Yes / No
Yes / No
Yes / No
I certify that my business applying for coverage with UnitedHealthcare is not part of a controlled group (commonly owned or affiliates) as defined under the Internal Revenue Code. Or I certify that my business applying for coverage with UnitedHealthcare (1) is eligible to file a consolidated federal tax return or (2) meets the IRS test for being a controlled group under common control. I further certify there are no other affiliated entities, other than the ones listed above, who are part of the controlled group that includes my business. I represent that, to the best of my knowledge, the information I have provided is accurate and truthful. I agree to notify UnitedHealthcare in the event of a change in any of the information that is the subject of this certification. I understand that any misrepresentation or fraudulent statement may result in rescission of the group policy, termination of coverage, an increase in premiums retroactive to the policy date, or other consequences as permitted by law.
Name (please print) & Title: Signature: Date:

Updated 10.31.2014
PEO/ELC Employer Questionnaire
An officer of the employer (not the Professional Employer Organization (PEO) or Employee Leasing
Company (ELC)) must complete and sign the application for coverage. Some employers/plan sponsors
may find it helpful to consult with legal counsel for completion, comprehension and agreement with the
statements on this form.
The total number of eligible employees (leased and non-leased) will be used to determine if the group
qualifies as a small employer under federal and state law.
Company/Client Name
PEO Name
1. The Employer/Client and their co-employees are eligible to file a Wage and Tax /Payroll document
specific to their Group.
Yes No
2. As the employer, I have the sole authority to control the working hours, hiring, training and
discharging of these individuals.
Yes No
3. All leased employees will be considered eligible for coverage on the same basis as non-leased
employees.
Yes No
4. UnitedHealthcare will be the sole provider of health insurance for all eligible employees (leased and
non-leased).
Yes No No Leased Employees
5. Are the Employer/Client and their co-employees eligible for health benefits under the PEO or ELC?
Yes No
6. If applicable, is the PEO or ELC the policyholder?
Yes No
7. Does your contract with the PEO or ELC permit you to obtain coverage for your co-employees outside
of the PEO or ELC?
Yes No
Employer Certification
I represent that the information I have provided is accurate and truthful. I understand that any
misrepresentation or fraudulent statement may result in rescission of the group policy, termination of
coverage, an increase in premiums retroactive to the policy date, or other consequences as permitted by
law.
Employer Name (Print) Title/Position
Employer signature Date
275-3281 4/07 ©2007 United HealthCare Services, Inc.
Your rights and
responsibilities
CONFIDENTIALITY
Make sure your employer has completed the “To be completed by the employer” section ofthe enrollment form before you begin tocomplete your portion of the form. If you do notwish to disclose personal medical informationthrough this form to anyone other thanUnitedHealthcare and its affiliates andrepresentatives for underwriting and otherpurposes permitted by law, you may complete allinformation on the enrollment form, then insertand seal the form in an envelope before returningit to your employer or broker.
Health Coverage Provided by United HealthCare InsuranceCompany/UnitedHealthcare of Texas, Inc.
Important information
In order to make choices about your coverage andtreatment, we believe that it is important for you tounderstand how your plan operates and how it mayaffect you. In an ever-changing environment, theinformation can never be complete and we urge youto contact us if the information in your SummaryPlan Description, Certificate of Coverage or othermaterials does not answer your questions. Furtherinformation is available at myuhc.com®.
1. We do not provide medical services or maketreatment decisions. We help finance and/oradminister the health benefit plan in which youare enrolled. That means:
• We make decisions about whether the healthbenefit plan you chose will reimburse you forcare that you may receive.
• We do not decide what care you need or willreceive. You and your physician make thosedecisions.
2. We may enter into arrangements where anotherentity carries out some of our duties, but thoseentities must operate consistently with ourcommitment to your plan.
3. We contract with networks of physicians andother providers. Our credentialing processconfirms public information about the providers’licenses and other credentials, but does notassure the quality of the services provided.
4. Physicians and other providers in our networksare independent contractors and are not ouremployees or agents. We do not control nor do
we have a right to control your physician’streatment or plan.
5. We may enter into agreements with yourphysician or other provider to share in the costsavings that our approach may generate. Weencourage providers in our network to disclosethe nature of those arrangements to you. If theydo not, we encourage you to talk to yourphysician about these arrangements.
6. We encourage physicians to talk with you aboutmedical care you or your physician think mightbe valuable.
In determining whether there has been a break incoverage of 63 days or more, plans may notinclude a waiting period you or your dependentsmay have had to satisfy. To receive credit forcoverage under prior health plans, you must showproof of prior coverage. You have the right torequest a Certificate of Prior Creditable coveragefrom your prior employer or insurer. If necessary,UnitedHealthcare will help you obtain thisinformation.
Statement of affirmation and
authorization to obtain and disclose
information in connection with
eligibility for medical coverage
I understand that I am completing a healthapplication and that the response must becomplete and accurate.
I (we) request the indicated group medicalcoverage for myself and, if the plan provides, formy dependents.
I authorize any required premium contributions tobe deducted from earnings.
By completing this application:
I (we) authorize all providers of health services orsupplies and any of their representatives to givethe following to the health plans: any availableinformation about the medical history, condition ortreatment of any person named in this request. I(we) authorize the health plans to use thisinformation to determine eligibility for medicalcoverage and eligibility for benefits under an existing policy.
I (we) also authorize the health plans to give thisinformation to its (their) representatives or to anyother organization for the reason notified above. I(we) agree that this authorization is valid for 30months from the date of this application. I (we)know that I (we) have the right to ask for andreceive a copy of this authorization.
I understand that the Certificate of Coverage or Summary Plan Description and other documents, notices and communicationsregarding my coverage may be transmittedelectronically.
I (we) have not given the agent or any otherpersons any health information not included on theapplication. I (we) understand that the health plansis not bound by any statements I (we) have madeto any agent or to any other persons, if thosestatements are not written or printed on theapplication and any attachments.
Page 1 of 5SG.EE.16.TX 4/15 275-8893 12/15
To speed the enrollment process, please be thorough and fill out all sections that apply.
Group Name Requested Effective Date of Coverage/Date of Change / /Group Name Policy Number
Date of Hire / /Position/Title
Hours Worked per week
Salary $_____________ Required only if Life, STD,or LTD Plan based on salary
If you are waiving all coverage, please complete sections A and B.
Last Name First Name MI Social Security Number
Address Apt # City State Zip Code Home/Cell Phone
Date of Birth Gender Marital Status �� Single �� Married �� Divorced �� Widowed Work Phone
/ / �� M �� F Language Preference, if not English
Email Address
Do you have a disability affecting your ability to communicate or read? �� Yes �� No
Primary Care Physician2, Obstetrician or Gynecologist Primary Care Dentist3
Physician First & Last Name _________________________________ Dentist First & Last Name _________________________________
Address _________________________________________________ ID# __________________________________________________
ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ – ___ ___ ___ ___ Existing Patient? �� Yes �� No
Existing Patient? �� Yes �� No
HMO female enrollees are not required to select an obstetrician or gynecologist. Obstetrical or gynecological care can be received from herprimary care physician, primary care provider or an obstetrician or gynecologist.
To Be Completed by Employer
Reason for Application�� New Group Plan �� New Hire�� Life Event/Date_______ �� Annual �� Status Change_______ Open �� Dependent Add/Delete Enrollment�� Change Name/Address �� Late�� Part time to Full time Enrollee�� Waiving Coverage �� Termination�� Other_________________________
Employee Type(Check all that apply)�� Active �� COBRA �� State Continuation
Start dt ____/____/____ End dt____/____/____
�� Hourly*�� Salary*�� Union* �� Non-Union* �� Retired�� Other ____________________________*Does not apply to health benefits
A. Employee Information
Employee Enrollment Form – Texas(DO NOT STAPLE)
Do you use tobacco?1 �� Yes �� NoIf yes, are you currently participating in a tobacco cessationprogram or do you intend to join one? �� Yes �� No
B. Waiver of CoverageI decline all coverage for:�� Myself �� Spouse�� Dependent Children�� Myself and all dependents
Declining coverage due to existence of other coverage:�� Spouse’s Employer’s Plan �� Individual Plan�� Covered by Medicare �� Medicaid�� COBRA from Prior Employer �� VA Eligibility�� Tri-Care�� I (we) have no other coverage at this time�� Other ____________________________________
I understand that by waiving coverage at this time, Iwill not be allowed to participate unless I qualify at aspecial enrollment period or as a late enrollee, ifapplicable, or at the next open enrollment period.
Date Employee Signature if waiving all coverage
UnitedHealthcare Insurance CompanyUnitedHealthcare of Texas, Inc.
National Pacific Dental, Inc.
Notice for Small Employers:You have the option to choose this Consumer Choice of Benefits HealthMaintenance Organization health care plan that, either in whole or in part,does not provide state-mandated health benefits normally required inevidences of coverage in Texas. This standard health benefit plan may providea more affordable health plan for you although, at the same time, it mayprovide you with fewer health plan benefits than those normally included asstate-mandated health benefits in Texas. If you choose this standard healthbenefit plan, please consult with your insurance agent to discover which state-mandated health benefits are excluded in this evidence of coverage.
List All Enrolling (Attach sheet if necessary)
Relationship4 Last Name First Name MI Sex Date of Birth�� M �� F / /
Social Security Number
Primary Care Physician2, Obstetrician or Gynecologist Primary Care Dentist3
Physician First & Last Name _________________________________ Dentist First & Last Name __________________________________
Address _________________________________________________ ID# ___________________________________________________
ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ – ___ ___ ___ ___ Existing Patient? �� Yes �� No
Existing Patient? �� Yes �� No Permanently disabled and age 26 or older5 �� Yes �� No
Relationship4 Last Name First Name MI Sex Date of Birth�� M �� F / /
Dependent Social Security Number
Primary Care Physician2, Obstetrician or Gynecologist Primary Care Dentist3
Physician First & Last Name _________________________________ Dentist First & Last Name __________________________________
Address _________________________________________________ ID# ___________________________________________________
ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ – ___ ___ ___ ___ Existing Patient? �� Yes �� No
Existing Patient? �� Yes �� No Permanently disabled and age 26 or older5 �� Yes �� No
Relationship4 Last Name First Name MI Sex Date of Birth�� M �� F / /
Dependent Social Security Number
Primary Care Physician2, Obstetrician or Gynecologist Primary Care Dentist3
Physician First & Last Name _________________________________ Dentist First & Last Name __________________________________
Address _________________________________________________ ID# ___________________________________________________
ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ – ___ ___ ___ ___ Existing Patient? �� Yes �� No
Existing Patient? �� Yes �� No Permanently disabled and age 26 or older5 �� Yes �� No
Relationship4 Last Name First Name MI Sex Date of Birth�� M �� F / /
Dependent Social Security Number
Primary Care Physician2, Obstetrician or Gynecologist Primary Care Dentist3
Physician First & Last Name _________________________________ Dentist First & Last Name __________________________________
Address _________________________________________________ ID# ___________________________________________________
ID# ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ ___ – ___ ___ ___ ___ Existing Patient? �� Yes �� No
Existing Patient? �� Yes �� No Permanently disabled and age 26 or older5 �� Yes �� No
C. Family Information
Do you use tobacco?1 �� Yes �� No If yes, are you currently participating in a tobacco cessation program or do you intend to join one? �� Yes �� No
Do you use tobacco?1 �� Yes �� No If yes, are you currently participating in a tobacco cessation program or do you intend to join one? �� Yes �� No
Do you use tobacco?1 �� Yes �� No If yes, are you currently participating in a tobacco cessation program or do you intend to join one? �� Yes �� No
Do you use tobacco?1 �� Yes �� No If yes, are you currently participating in a tobacco cessation program or do you intend to join one? �� Yes �� No
Page 2 of 5
Employee Name __________________________________________________________________________________________________________
Spouse/DomesticPartner
(1) Tobacco means all tobacco products, including, but not limited to, cigarettes, cigars, and chewing tobacco. You should only check the “yes” box above iftobacco was used four or more times per week on average (excluding religious or ceremonial use) within the past 6 months by someone of legal age topurchase tobacco in the state of residence. (2) For UnitedHealthcare Health Maintenance Organization (HMO) products, including Compass, Navigate, Select,Select Plus, and other products requiring you to choose a Primary Care Physician (PCP), you must use the UnitedHealthcare directory of providers to choosea PCP for yourself and each of your covered dependents. (3) Please see employer representative as some HMO dental plans require a Primary Care Dentist(PCD) selection. (4) For court ordered dependent, legal documentation must be attached. If a dependent does not reside with eligible employee, pleaseprovide address on a separate sheet. (5) If you answered “Yes” for Disabled and the dependent child is 26 years of age or older, unmarried, chiefly dependentupon subscriber for support and is not able to be self-supporting because of a physically or mentally disabling injury, illness or condition, please attach amedical certification of disability.
Within the last 12 months, have you, your spouse, or your dependents had any other medical coverage? �� NO �� YES (if yes, please complete this section.)Prior medical carrier name ____________________________________________________ Effective date ___/___/___ End date ___/___/___
Prior coverage type: �� Employee �� Spouse �� Child(ren) �� Family
E. Prior Medical Insurance Information
Medicare – Employee Information: If enrolled in Medicare, please attach a copy of your Medicare ID card.�� Enrolled in Part A: Effective Date _____________ �� Ineligible for Part A* �� Not Enrolled in Part A (chose not to enroll)**�� Enrolled in Part B: Effective Date _____________ �� Ineligible for Part B* �� Not Enrolled in Part B (chose not to enroll)**�� Enrolled in Part D: Effective Date _____________ �� Ineligible for Part D* �� Not Enrolled in Part D (chose not to enroll)**Reason for Medicare eligibility: �� Over 65 �� Kidney Disease �� Disabled �� Disabled but actively at workAre you receiving Social Security Disability Insurance (SSDI)? �� YES �� NO Start Date ___ /___ /___
Medicare – Spouse/Dependent Name: ____________________________________________�� Enrolled in Part A: Effective Date _____________ �� Ineligible for Part A* �� Not Enrolled in Part A (chose not to enroll)**�� Enrolled in Part B: Effective Date _____________ �� Ineligible for Part B* �� Not Enrolled in Part B (chose not to enroll)**�� Enrolled in Part D: Effective Date _____________ �� Ineligible for Part D* �� Not Enrolled in Part D (chose not to enroll)**Reason for Medicare eligibility: �� Over 65 �� Kidney Disease �� Disabled �� Disabled but actively at work*Only check “Ineligible” if you have received documentation from your Social Security benefits that indicate that you are not eligible for Medicare.** If you are eligible for Medicare on a primary basis (Medicare pays before benefits under the group policy), you should enroll in and maintaincoverage under Medicare Part A, Part B, and/or Part D as applicable.
On the day this coverage begins, will you, your spouse or any of your dependents be covered under any other medical health plan or policy,including another UnitedHealthcare plan or Medicare? �� YES (continue completing this section) �� NO (skip the rest of this section)
Name of other carrier ______________________________________________________
Other Group Medical Coverage Information Type Effective Date End Date Name and date of birth of policyholder (only list those covered by other plan) (B/S/F)* MM/DD/YY MM/DD/YY for other coverage
Employee:
Spouse Name:
Dependent Name:
Dependent Name:
Dependent Name:
*B.Enter ‘B’ when this dependent is covered under both you and your spouse’s insurance plan (married)S.Enter ‘S’ if you are the parent awarded custody of this dependent and no other individual is required to pay for this dependent’s medical expenses.F. Enter ‘F’ if this dependent is covered by another individual (not a member of your household) required to pay for this dependent’s medical expenses.
F. Other Medical Coverage Information This section must be completed. (Attach sheet if necessary.)
Page 3 of 5
Employee Name __________________________________________________________________________________________________________
Please check the box for each coverage in which you or your dependents are enrolling. If your employer offers a choice of plans, indicate which plan you are selecting. Indicate the dollar amountselected for the Life and Accidental Death & Dismemberment (AD&D), Supplemental Life, Short-Term Disability(STD), and Long-Term Disability (LTD) plans. Benefit offerings are dependent upon employer selection.
Person Medical Dental Vision Basic Life/AD&D Supp Life/AD&D
Employee �� _____________ �� _____________ �� �� $_____________ �� $_____________ Spouse [Domestic Partner] �� _____________ �� _____________ �� �� $_____________ �� $_____________Dependent �� _____________ �� _____________ �� �� $_____________ �� $_____________
Person STD LTD
Employee �� ��
Life Insurance Beneficiary Full Name and Address (if applying for Life Insurance with UnitedHealthcare) Relationship
Primary
Secondary
D. Product Selection
Date Employee Signature for all applying Spouse Signature (if applying for coverage)
Page 4 of 5
G. Signature
Your enrollment in the plan is expressly conditioned upon your acceptance of all terms and conditions contained in this enrollment application.If you do not agree to the following terms and conditions, you may not complete your enrollment.
TERMS AND CONDITIONSAs a condition of my and/or my dependents’ participation in the plan, and in consideration for the privileges that come from participation inthe plan, I hereby agree for myself and/or for my dependents as follows: I recognize and understand that the plan contracts with physicians and other providers that make up the plan network. I recognize that allphysicians and other providers that participate in the plan network are subject to credentialing under applicable State regulations and pursuantto the plan’s network credentialing process. I understand that such credentialing includes a review of provider education, training andlicensure. However, by participating in the plan I hereby acknowledge and accept that the plan is not a provider of medical services, and I amaware that obtaining or not obtaining medical care involves significant risks such as serious injury and even death. I acknowledge that thecredentialing of physicians and other providers does not in any way reduce this risk. I agree to assume all risks and responsibility for, andhold the plan harmless from, any and all claims for damages, including personal injury or death, medical expenses, disability, lost wages, andloss of earning capacity which may be incurred or associated with medical treatment obtained through a participating physician or otherprovider. I recognize that all physicians and other providers that participate in the plan network are independent contractors and not the plan’semployees or agents and are solely responsible for any malpractice, adverse outcomes, or any other claims arising from medical treatmentrendered to me and my dependents. I HEREBY AGREE THAT THE PLAN IS NOT RESPONSIBLE NOR LIABLE FOR ANY ADVICE, COURSE OFTREATMENT, DIAGNOSIS OR ANY OTHER INFORMATION, SERVICES OR PRODUCTS THAT I OR MY DEPENDENTS OBTAIN THROUGH APARTICIPATING NETWORK PHYSICIAN OR OTHER PROVIDER.I recognize and understand that the plan does not recommend, endorse or make any representation about the appropriateness or suitability ofany specific tests, products, procedures, treatments, services, or opinions. I recognize that the plan, plan documents, and any health andwellness information provided by the plan, are not intended or implied to be a substitute for professional medical advice, diagnosis ortreatment. I agree to confirm any medical information obtained from or through the plan with other sources, and will review all informationregarding any medical condition or treatment with my physician. I HEREBY AGREE TO NEVER DISREGARD PROFESSIONAL MEDICAL ADVICEOR DELAY SEEKING MEDICAL TREATMENT BECAUSE OF SOMETHING I HAVE READ OR ACCESSED THROUGH THE PLAN.I authorize UnitedHealthcare Insurance Company and its affiliates (collectively, "UnitedHealthcare") to obtain, use and disclose my medical,claim or benefit records, including any individually identifiable health information contained in these records. I understand these records maycontain information created by other persons or entities (including health care providers) as well as information regarding the use of drug,alcohol, HIV/AIDS, mental health (other than psychotherapy notes), sexually transmitted disease and reproductive health services. I authorizeany health care provider, pharmacy benefit manager, other insurer or reinsurer, hospital, clinic or other medical facility, health careclearinghouse, and any of their affiliates, representatives or business associates, to disclose my information to UnitedHealthcare and Affiliates.I understand that the purpose of the disclosure and use of my information is to allow UnitedHealthcare to facilitate the appropriatemanagement of treatment, services, payment and benefits. I further understand that the information disclosed will not be used for purposesof eligibility, enrollment, underwriting and premium risk rating. I understand this authorization is voluntary and I may refuse to sign theauthorization. I understand I may revoke this authorization at any time by notifying my UnitedHealthcare representative in writing, except tothe extent that action has already been taken in reliance on this authorization. As required by HIPAA, UnitedHealthcare also requires that Iacknowledge the following, which I do: I understand that information I authorize a person or entity to obtain and use may be re-disclosed andno longer protected by federal privacy regulations. This authorization, unless revoked earlier, expires 30 months after the date it is signed.
I understand that I am completing a joint life and health application and that each response must be complete and accurate. I (we) request theindicated group medical coverage. I authorize any required premium contributions to be deducted from my earnings. I (we) have not given theagent or any other persons any required information not included on the application. I (we) understand that UnitedHealthcare is not bound byany statements I (we) have made to any agent or to any other persons, if those statements are not written or printed on this application andany attachments.
Please note that if you knowingly or intentionally leave out information or make a misrepresentation of a material fact on this form we may beallowed by law to take one or more of the following actions: terminate or non-renew your coverage or change your premium retroactively tothe date your policy became effective.
Please maintain a copy of this authorization for your records.
Employee Name __________________________________________________________________________________________________________
Coverage Provided by “UnitedHealthcare and Affiliates”: Medical coverage provided by UnitedHealthcare Insurance Company (PPO, indemnity) or UnitedHealthcare of Texas, Inc. (HMO)Dental coverage provided by UnitedHealthcare Insurance Company (indemnity) or National Pacific Dental, Inc. (HMO)Life, Short-Term Disability (STD), Long-Term Disability (LTD) Insurance coverage provided by UnitedHealthcare Insurance Company Vision coverage provided by UnitedHealthcare Insurance Company
1. Race, check all that apply: �� White �� Black, African-American �� American Indian/Alaska Native �� Asian�� Native Hawaiian/Pacific Islander �� Other Race, please specify_______________________
2. Are you of Hispanic or Latino origin? �� Yes �� No
NOTE: Responding to this question is optional and is not required. Data collected in this section will be used only to help communicate withenrollees and inform them of specific programs to enhance their well-being. This information will not be used in the eligibility process.
H. Census Information (optional)
Page 5 of 5
Employee Name __________________________________________________________________________________________________________
Texas Mandatory Disclosure Statement:
Dental indemnity benefits are provided through UnitedHealthcare Insurance Company and Dental HMO (DHMO) benefits are offered throughNational Pacific Dental, Inc. In order to receive benefits from the DHMO plan, an enrollee must utilize only network providers, except foremergency dental care, and pay the copayments specified in the evidence of coverage. To receive benefits under the dental indemnity plan, theenrollee may utilize any provider but prior to receiving reimbursement, the enrollee must meet the required deductible and is responsible forthe coinsurance amount specified in the policy or certificate.





























