Embed Size (px)
Citation preview

Enrollment Checklist
The address must first be verified to establish district and school attendance boundaries. After the address is verified,
please use the following checklist to assist you in gathering the necessary documents needed to successfully enroll your
student(s). Contact the District Office Welcome Center at 952.232.2048 for further assistance with enrollment.
Verify Address District and Attendance Areas (https://sis.isd194.org/enroll)
Lakeville Area Public Schools Student Enrollment Form
Proof of Address (examples include Home Purchase Agreement, Lease, or Current Utility Bill)
Proof of Student Legal Name and Birthdate (examples include Birth Certificate, Passport, Hospital Record)
Student Immunization Form (a current record of immunizations is required to start school)
Student Health Inventory
Consent to Release Educational Data (allows ISD194 to retrieve education records from other schools)
Minnesota Language Survey
Application for Educational Benefits (School Meals, State & Federal Programs (optional for parents to complete))
Consent to Share Information for Benefits for Other Programs (optional for parents to complete)
After Enrolling Your Student Contact Schmitty & Sons for Bus Information (952.985.7517)
Contact the School to schedule a Tour and Register for Classes
KINDERGARTEN STUDENTS: Early Childhood Screening is required before starting Kindergarten.
If not yet completed, schedule an appointment at 952.232.3000 (option 3).
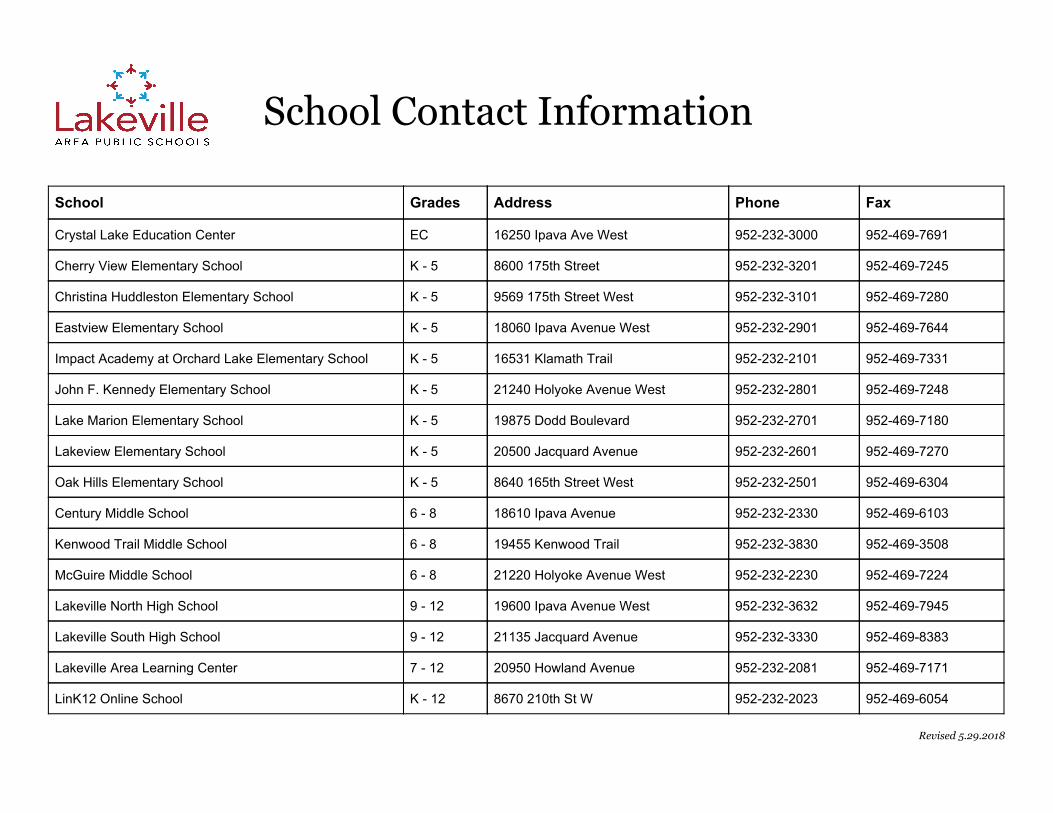
School Contact Information
School Grades Address Phone Fax
Crystal Lake Education Center EC 16250 Ipava Ave West 952-232-3000 952-469-7691
Cherry View Elementary School K - 5 8600 175th Street 952-232-3201 952-469-7245
Christina Huddleston Elementary School K - 5 9569 175th Street West 952-232-3101 952-469-7280
Eastview Elementary School K - 5 18060 Ipava Avenue West 952-232-2901 952-469-7644
Impact Academy at Orchard Lake Elementary School K - 5 16531 Klamath Trail 952-232-2101 952-469-7331
John F. Kennedy Elementary School K - 5 21240 Holyoke Avenue West 952-232-2801 952-469-7248
Lake Marion Elementary School K - 5 19875 Dodd Boulevard 952-232-2701 952-469-7180
Lakeview Elementary School K - 5 20500 Jacquard Avenue 952-232-2601 952-469-7270
Oak Hills Elementary School K - 5 8640 165th Street West 952-232-2501 952-469-6304
Century Middle School 6 - 8 18610 Ipava Avenue 952-232-2330 952-469-6103
Kenwood Trail Middle School 6 - 8 19455 Kenwood Trail 952-232-3830 952-469-3508
McGuire Middle School 6 - 8 21220 Holyoke Avenue West 952-232-2230 952-469-7224
Lakeville North High School 9 - 12 19600 Ipava Avenue West 952-232-3632 952-469-7945
Lakeville South High School 9 - 12 21135 Jacquard Avenue 952-232-3330 952-469-8383
Lakeville Area Learning Center 7 - 12 20950 Howland Avenue 952-232-2081 952-469-7171
LinK12 Online School K - 12 8670 210th St W 952-232-2023 952-469-6054
Revised 5.29.2018

Lakeville Area Public Schools ISD #194
Enrollment Form - Family Information
Primary Household Parent/Guardian Information (*If other than father or mother, please provide guardianship documents)
*Parent/Guardian Last Name First Name Middle Name Sex Birth Date Relationship (to Student)
Cell Phone Work Phone Email Address
M F
M F
Primary Household Address City, State and Zip Code Home Phone Date Moved In
Do you currently reside with another family, person or other temporary housing facility? Yes: ❏ No: ❏ Primary Phone to Call: H:❏ C:❏ W:❏
Please list in order of birth all children and other adults living in the Primary Household (Please use legal name as listed on birth record)
Last Name First Name Middle Name Sex Birth Date Grade Level Relationship to Student
M F
M F
M F
M F
M F
M F
Additional Household Parent/Guardian information (*If applicable due to separation, divorce or other circumstances)
*Parent/Guardian Last Name First Name Middle Name Sex Birth Date Relationship (to Student)
Cell Phone Work Phone Email Address
M F
M F
Additional Household Address City, State and Zip Code Home Phone Date Moved In
Explanation of private information requested on this form: In accordance with the Federal Data Privacy Act of 1974 and the State of Minnesota Privacy Law,
you are not required to provide the information noted with an asterisk (*). There will be no adverse effect on you or your student if you do not choose to provide it.
However, your cooperation in providing this information will ensure its accuracy and help to facilitate equitable educational opportunities for all students.
Be assured that we will use the information in a manner that respects the privacy of our students and families.
Revised 2.13.2018
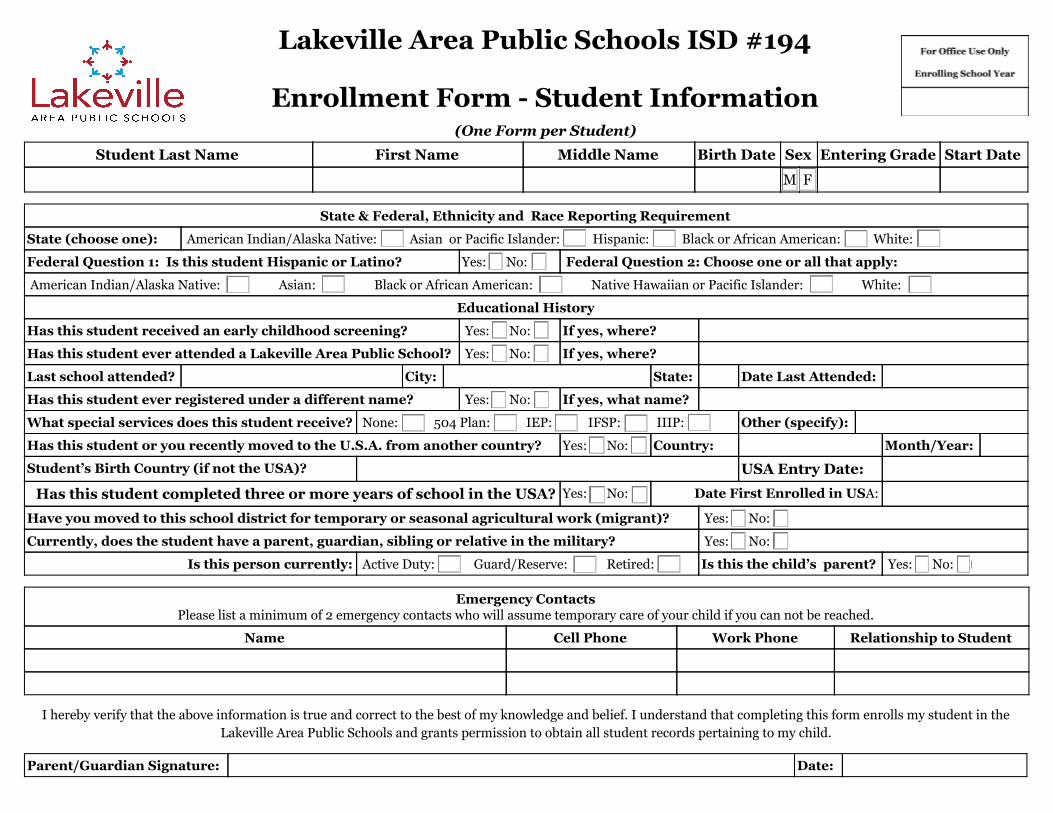
Lakeville Area Public Schools ISD #194
Enrollment Form - Student Information
(One Form per Student)
Student Last Name First Name Middle Name Birth Date Sex Entering Grade Start Date
M F
State & Federal, Ethnicity and Race Reporting Requirement
State (choose one): American Indian/Alaska Native: ❏ Asian or Pacific Islander: ❏ Hispanic: ❏ Black or African American: ❏ White: ❏
Federal Question 1: Is this student Hispanic or Latino? Yes: ❏ No: ❏ Federal Question 2: Choose one or all that apply:
American Indian/Alaska Native: ❏ Asian: ❏ Black or African American: ❏ Native Hawaiian or Pacific Islander: ❏ White: ❏
Educational History
Has this student received an early childhood screening? Yes: ❏ No: ❏ If yes, where?
Has this student ever attended a Lakeville Area Public School? Yes: ❏ No: ❏ If yes, where?
Last school attended? City: State: Date Last Attended:
Has this student ever registered under a different name? Yes: ❏ No: ❏ If yes, what name?
What special services does this student receive? None: ❏ 504 Plan: ❏ IEP: ❏ IFSP: ❏ IIIP: ❏ Other (specify):
Has this student or you recently moved to the U.S.A. from another country? Yes: ❏ No: ❏ Country: Month/Year:
Student’s Birth Country (if not the USA)? USA Entry Date:
Has this student completed three or more years of school in the USA? Yes: ❏ No: ❏ Date First Enrolled in USA:
Have you moved to this school district for temporary or seasonal agricultural work (migrant)? Yes: ❏ No: ❏
Currently, does the student have a parent, guardian, sibling or relative in the military? Yes: ❏ No: ❏
Is this person currently: Active Duty: ❏ Guard/Reserve: ❏ Retired: ❏ Is this the child’s parent? Yes: ❏ No: ❏
Emergency Contacts
Please list a minimum of 2 emergency contacts who will assume temporary care of your child if you can not be reached.
Name Cell Phone Work Phone Relationship to Student
I hereby verify that the above information is true and correct to the best of my knowledge and belief. I understand that completing this form enrolls my student in the
Lakeville Area Public Schools and grants permission to obtain all student records pertaining to my child.
Parent/Guardian Signature: Date:
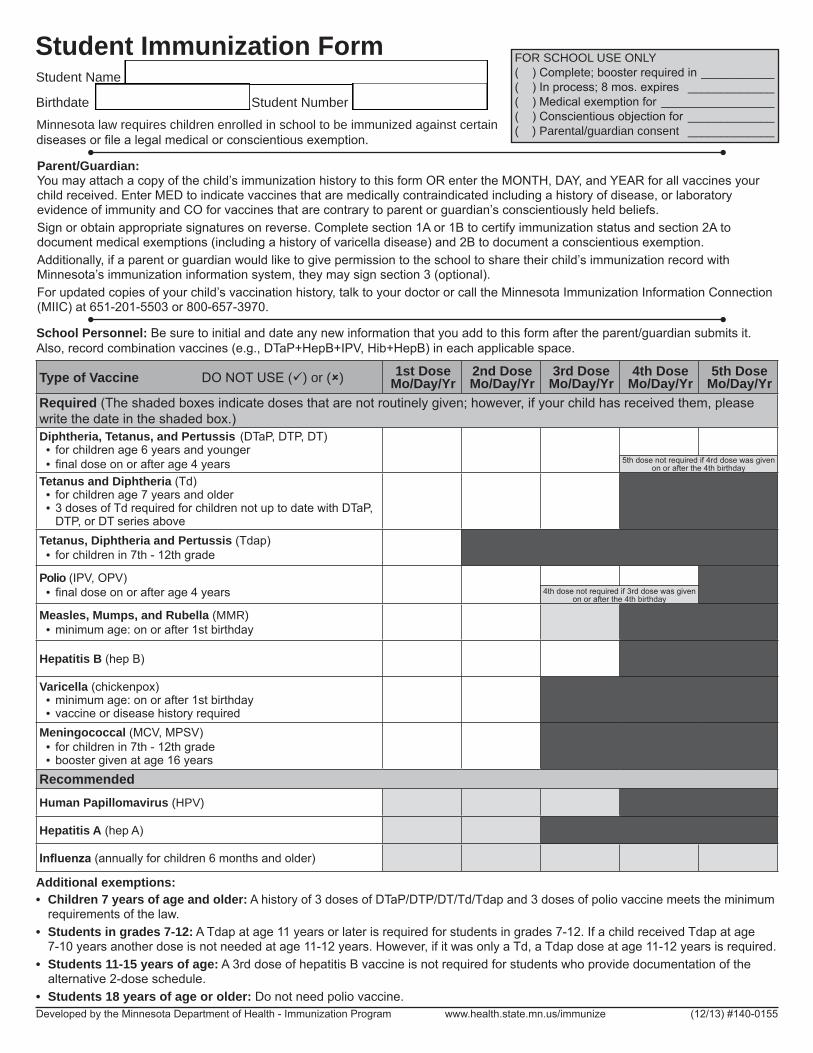
Minnesota law requires children enrolled in school to be immunized against certain diseases or file a legal medical or conscientious exemption.
Student Immunization Form FOR SCHOOL USE ONLY( ) Complete; booster required in ___________( ) In process; 8 mos. expires _____________( ) Medical exemption for _________________( ) Conscientious objection for _____________( ) Parental/guardian consent _____________
Developed by the Minnesota Department of Health - Immunization Program www.health.state.mn.us/immunize (12/13) #140-0155
Student Name _________________________________________________
Birthdate _____________________Student Number __________________
Additional exemptions: • Children 7 years of age and older: A history of 3 doses of DTaP/DTP/DT/Td/Tdap and 3 doses of polio vaccine meets the minimum
requirements of the law.• Students in grades 7-12: A Tdap at age 11 years or later is required for students in grades 7-12. If a child received Tdap at age
7-10 years another dose is not needed at age 11-12 years. However, if it was only a Td, a Tdap dose at age 11-12 years is required. • Students 11-15 years of age: A 3rd dose of hepatitis B vaccine is not required for students who provide documentation of the
alternative 2-dose schedule.• Students 18 years of age or older: Do not need polio vaccine.
Type of Vaccine DO NOT USE () or () 1st DoseMo/Day/Yr
2nd DoseMo/Day/Yr
3rd DoseMo/Day/Yr
4th DoseMo/Day/Yr
5th DoseMo/Day/Yr
Required (The shaded boxes indicate doses that are not routinely given; however, if your child has received them, please write the date in the shaded box.) Diphtheria, Tetanus, and Pertussis (DTaP, DTP, DT)• for children age 6 years and younger• final dose on or after age 4 years
Tetanus and Diphtheria (Td) • for children age 7 years and older• 3 doses of Td required for children not up to date with DTaP,
DTP, or DT series aboveTetanus, Diphtheria and Pertussis (Tdap)
• for children in 7th - 12th grade
Polio (IPV, OPV)• final dose on or after age 4 years
Measles, Mumps, and Rubella (MMR)• minimum age: on or after 1st birthday
Hepatitis B (hep B)
Varicella (chickenpox)• minimum age: on or after 1st birthday • vaccine or disease history required
Meningococcal (MCV, MPSV) • for children in 7th - 12th grade• booster given at age 16 years
RecommendedHuman Papillomavirus (HPV)
Hepatitis A (hep A)
Influenza (annually for children 6 months and older)
5th dose not required if 4rd dose was given on or after the 4th birthday
4th dose not required if 3rd dose was given on or after the 4th birthday
School Personnel: Be sure to initial and date any new information that you add to this form after the parent/guardian submits it. Also, record combination vaccines (e.g., DTaP+HepB+IPV, Hib+HepB) in each applicable space.
Parent/Guardian:You may attach a copy of the child’s immunization history to this form OR enter the MONTH, DAY, and YEAR for all vaccines your child received. Enter MED to indicate vaccines that are medically contraindicated including a history of disease, or laboratory evidence of immunity and CO for vaccines that are contrary to parent or guardian’s conscientiously held beliefs. Sign or obtain appropriate signatures on reverse. Complete section 1A or 1B to certify immunization status and section 2A to document medical exemptions (including a history of varicella disease) and 2B to document a conscientious exemption. Additionally, if a parent or guardian would like to give permission to the school to share their child’s immunization record with Minnesota’s immunization information system, they may sign section 3 (optional).For updated copies of your child’s vaccination history, talk to your doctor or call the Minnesota Immunization Information Connection (MIIC) at 651-201-5503 or 800-657-3970.
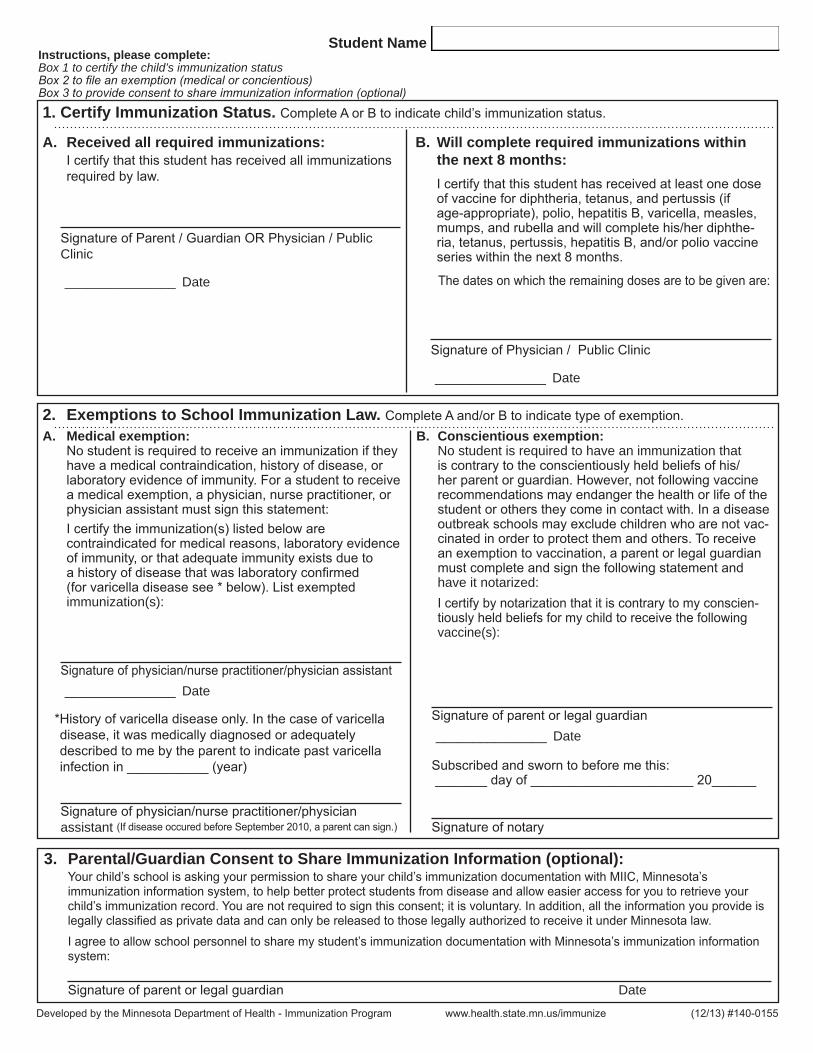
Developed by the Minnesota Department of Health - Immunization Program www.health.state.mn.us/immunize (12/13) #140-0155
Student Name _______________________________________________Instructions, please complete:Box 1 to certify the child’s immunization status Box 2 to file an exemption (medical or concientious) Box 3 to provide consent to share immunization information (optional)
3. Parental/Guardian Consent to Share Immunization Information (optional): Your child’s school is asking your permission to share your child’s immunization documentation with MIIC, Minnesota’s
immunization information system, to help better protect students from disease and allow easier access for you to retrieve your child’s immunization record. You are not required to sign this consent; it is voluntary. In addition, all the information you provide is legally classified as private data and can only be released to those legally authorized to receive it under Minnesota law.
I agree to allow school personnel to share my student’s immunization documentation with Minnesota’s immunization information system:
Signature of parent or legal guardian Date
A. Received all required immunizations: I certify that this student has received all immunizations
required by law.
Signature of Parent / Guardian OR Physician / Public Clinic
_______________ Date
B. Will complete required immunizations within the next 8 months:
I certify that this student has received at least one dose of vaccine for diphtheria, tetanus, and pertussis (if age-appropriate), polio, hepatitis B, varicella, measles, mumps, and rubella and will complete his/her diphthe-ria, tetanus, pertussis, hepatitis B, and/or polio vaccine series within the next 8 months.
The dates on which the remaining doses are to be given are:
Signature of Physician / Public Clinic
_______________ Date
1. Certify Immunization Status. Complete A or B to indicate child’s immunization status.
A. Medical exemption: No student is required to receive an immunization if they have a medical contraindication, history of disease, or laboratory evidence of immunity. For a student to receive a medical exemption, a physician, nurse practitioner, or physician assistant must sign this statement:I certify the immunization(s) listed below are contraindicated for medical reasons, laboratory evidence of immunity, or that adequate immunity exists due to a history of disease that was laboratory confirmed (for varicella disease see * below). List exempted immunization(s):
Signature of physician/nurse practitioner/physician assistant _______________ Date
*History of varicella disease only. In the case of varicella disease, it was medically diagnosed or adequately described to me by the parent to indicate past varicella infection in ___________ (year)
Signature of physician/nurse practitioner/physician assistant (If disease occured before September 2010, a parent can sign.)
B. Conscientious exemption: No student is required to have an immunization that is contrary to the conscientiously held beliefs of his/her parent or guardian. However, not following vaccine recommendations may endanger the health or life of the student or others they come in contact with. In a disease outbreak schools may exclude children who are not vac-cinated in order to protect them and others. To receive an exemption to vaccination, a parent or legal guardian must complete and sign the following statement and have it notarized:I certify by notarization that it is contrary to my conscien-tiously held beliefs for my child to receive the following vaccine(s):
Signature of parent or legal guardian _______________ Date
Subscribed and sworn to before me this: _______ day of ______________________ 20______
Signature of notary
2. Exemptions to School Immunization Law. Complete A and/or B to indicate type of exemption.

STUDENT HEALTH INVENTORY
Student Name (Last, First, Middle) Sex Birth Date School Grade
M F
This information is needed to keep your child healthy and safe at school. If your child has a life threatening health condition; it is the parent/guardian’s responsibility to notify the school nurse prior to
school attendance so that an appropriate plan of care is developed.
HAS YOUR CHILD BEEN DIAGNOSED BY A
LICENSED HEALTHCARE PROVIDER WITH ANY OF THE
FOLLOWING:
YES NO EXPLAIN ALL “YES” ANSWERS
ADD/ADHD medication? dose?
Allergies: drugs, foods, insects, latex?
Arthritis or joint pain
Asthma, mild moderate severe meds?
Autism
Birth defects
Bladder concerns
Bleeding disorder: type?
Brain injury/ concussion ?
Cancer: type? Remission?
Cerebral palsy: identify type/limbs
Cystic Fibrosis
Depression: medication/counseling?
Developmental delays
Diabetes: age at diagnosis?
Dietary restrictions
Down’s Syndrome
Ear or hearing concerns
Eating disorder: over/ underweight
Emotional or psychological concern
Eye or vision concerns
Heart condition: restrictions?
Intestinal/bowel concerns: soiling?
Kidney disease
Migraines or severe headaches
Prematurity: weeks? Apgars?
Seizures: type, meds, last seizure?
Skin concerns
Speech/communication concerns
Spina bifida
OVER CONFIDENTIAL
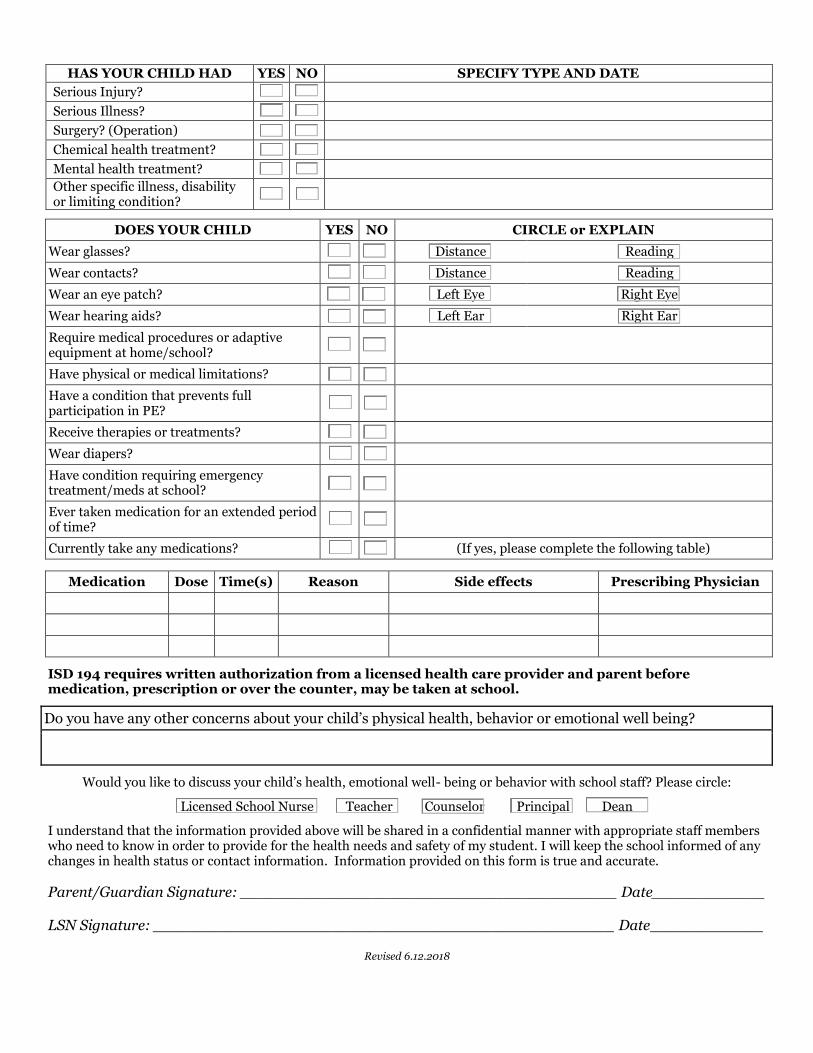
HAS YOUR CHILD HAD YES NO SPECIFY TYPE AND DATE
Serious Injury?
Serious Illness?
Surgery? (Operation)
Chemical health treatment?
Mental health treatment?
Other specific illness, disability or limiting condition?
DOES YOUR CHILD YES NO CIRCLE or EXPLAIN
Wear glasses? Distance Reading
Wear contacts? Distance Reading
Wear an eye patch? Left Eye Right Eye
Wear hearing aids? Left Ear Right Ear
Require medical procedures or adaptive equipment at home/school?
Have physical or medical limitations?
Have a condition that prevents full participation in PE?
Receive therapies or treatments?
Wear diapers?
Have condition requiring emergency treatment/meds at school?
Ever taken medication for an extended period of time?
Currently take any medications? (If yes, please complete the following table)
Medication Dose Time(s) Reason Side effects Prescribing Physician
ISD 194 requires written authorization from a licensed health care provider and parent before medication, prescription or over the counter, may be taken at school.
Do you have any other concerns about your child’s physical health, behavior or emotional well being?
Would you like to discuss your child’s health, emotional well- being or behavior with school staff? Please circle:
Licensed School Nurse Teacher Counselor Principal Dean
I understand that the information provided above will be shared in a confidential manner with appropriate staff members who need to know in order to provide for the health needs and safety of my student. I will keep the school informed of any changes in health status or contact information. Information provided on this form is true and accurate.
Parent/Guardian Signature: ________________________________________ Date____________ LSN Signature: _________________________________________________ Date____________
Revised 6.12.2018

Consent to Release Educational Data to Lakeville ISD #0194
This form allows information about your student to be forwarded from a previous school.
I authorize Lakeville Area Public Schools ISD #0194 to obtain educational information from:
Previous School District Name: District #: Phone: Fax:
Address: City: State: Zip:
Student Last Name: First: Middle:
Previous School Name: Birth Date: Grade: Sex: M F
Parent/Guardian Signature: _______________________________________________________________________ Date: ___________________
Previous School District: Please provide the following information* (as applicable):
School Records & Transcripts Special Education Records & Related Services**
Withdrawal Grades if transfer is during school term EL (Language) Records
Health & Immunization Records 504 Plan
Preschool Screening Records Psychological Reports
Standardized Test Results Discipline/Violent behavior records per MN Statute 120A.22 subd 7(e)
Teacher, Counselor, Staff Observations IEP/IIIP**
Attendance Records Other (specify):
*Please DO NOT mail a student’s Cumulative File
** Schools using SpEd Forms: Please have current case manager Share/Transfer the student record to First name: New Last name: Case Manager
Please fax requested records to the number listed for the following school the student has enrolled at:
Cherry View Elementary, Fax: 952-469-7245 Century Middle, Fax: 952-469-6103
Christina Huddleston Elementary, Fax: 952-469-7280 Kenwood Trail Middle, Fax: 952-469-3508
Eastview Elementary, Fax: 952-469-7644 McGuire Middle, Fax: 952-469-7224
Impact Academy at Orchard Lake Elementary, Fax: 952-469-7331 Lakeville North High, Fax: 952-469-7945
John F. Kennedy Elementary, Fax: 952-469-7248 Lakeville South High, Fax: 952-469-8383
Lake Marion Elementary, Fax: 952-469-7180 Area Learning Center, Fax: 952-469-7171
Lakeview Elementary, Fax: 952-469-7270 LinK12 Lakeville (Online Learning), Fax: 952-469-6054
Oak Hills Elementary, Fax: 952-469-6304 Crystal Lake Education Center, Fax: 952-469-7691
Revised 6.29.2018

Consent to Release Educational Data to Lakeville ISD #0194 Page 2 - Blank
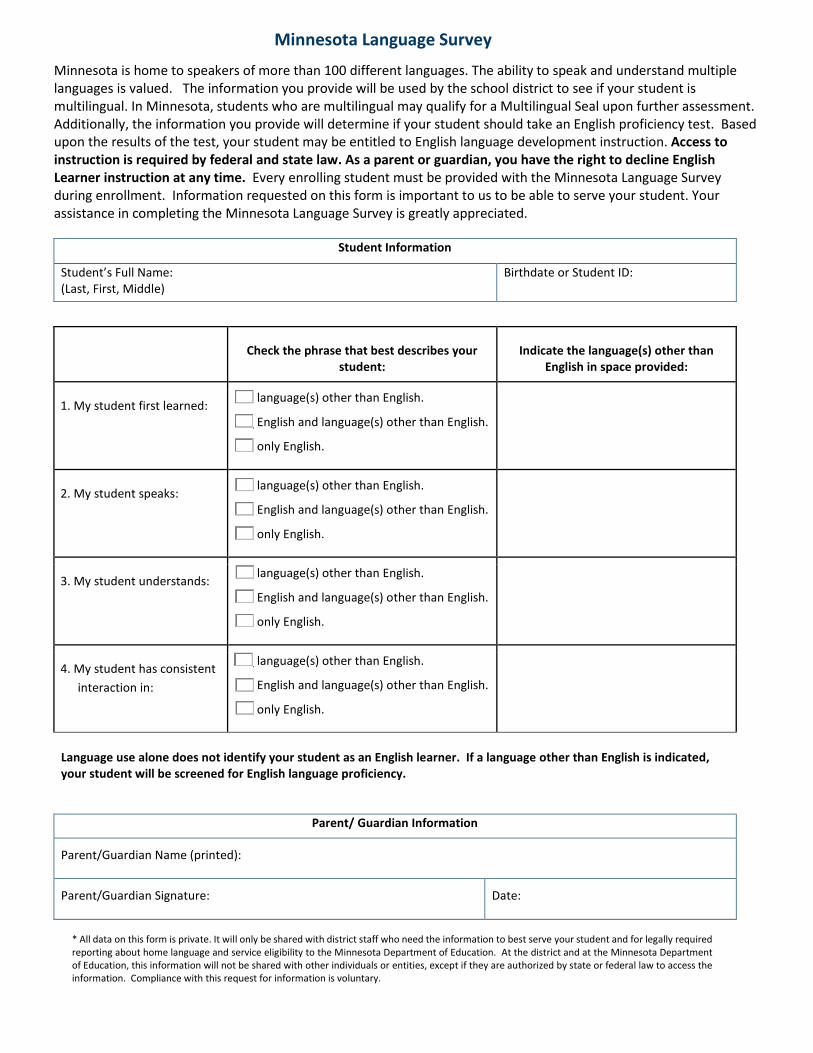
Minnesota Language Survey
Minnesota is home to speakers of more than 100 different languages. The ability to speak and understand multiple languages is valued. The information you provide will be used by the school district to see if your student is multilingual. In Minnesota, students who are multilingual may qualify for a Multilingual Seal upon further assessment. Additionally, the information you provide will determine if your student should take an English proficiency test. Based upon the results of the test, your student may be entitled to English language development instruction. Access to instruction is required by federal and state law. As a parent or guardian, you have the right to decline English Learner instruction at any time. Every enrolling student must be provided with the Minnesota Language Survey during enrollment. Information requested on this form is important to us to be able to serve your student. Your assistance in completing the Minnesota Language Survey is greatly appreciated.
Student Information
Student’s Full Name: (Last, First, Middle)
Birthdate or Student ID:
Check the phrase that best describes your student:
Indicate the language(s) other than English in space provided:
1. My student first learned: ___ language(s) other than English.
___ English and language(s) other than English.
___ only English.
2. My student speaks: ___ language(s) other than English.
___ English and language(s) other than English.
___ only English.
3. My student understands: ___ language(s) other than English.
___ English and language(s) other than English.
___ only English.
4. My student has consistent interaction in:
___ language(s) other than English.
___ English and language(s) other than English.
___ only English.
Language use alone does not identify your student as an English learner. If a language other than English is indicated, your student will be screened for English language proficiency.
Parent/ Guardian Information
Parent/Guardian Name (printed):
Parent/Guardian Signature: Date:
* All data on this form is private. It will only be shared with district staff who need the information to best serve your student and for legally required reporting about home language and service eligibility to the Minnesota Department of Education. At the district and at the Minnesota Department of Education, this information will not be shared with other individuals or entities, except if they are authorized by state or federal law to access the information. Compliance with this request for information is voluntary.

Minnesota Language Survey Page 2 - Blank

Office of Student Nutrition 17685 Juniper Path #300 Lakeville, MN 55044
Dear Parent/Guardian:
Our school provides healthy meals each day. Breakfast costs: Kindergarten – Free, Elementary (gr. 1-5) $1.30, Secondary $1.65, Adult $2.15; lunch costs: Elementary (all) $2.50, Middle School $2.60 (reg) $3.45 (Big Cat), High School $2.65 (reg) $3.45 (Big Cat), Adult (reg) $3.85 (Big Cat) $4.65.
Your children may qualify for free or reduced-price school meals. To apply, complete the enclosed Application for Educational Benefits following the instructions. A new application must be submitted each year. At public schools, your application also helps the school qualify for education funds and discounts.
State funds help to pay for reduced-price school meals, so all students who are approved for either free or reduced-price school meals will receive school meals at no charge. State funds also help to pay for breakfasts for kindergarten students, so all participating kindergarten students receive breakfasts at no charge.
Return your completed Application for Educational Benefits to:
ISD 194, Student Nutrition, 17685 Juniper Path #300, Lakeville, MN 55044
Who can get free school meals? Children in households participating in the Supplemental Nutrition Assistance Program (SNAP), Minnesota Family Investment Program (MFIP) or Food Distribution Program on Indian Reservations (FDPIR), and foster, homeless, migrant and runaway children can get free school meals without reporting household income. Or children can get free school meals if their household income is within the maximum income shown for their household size on the instructions.
I get WIC or Medical Assistance. Can my children get free school meals? Children in households participating in WIC or Medical Assistance may be eligible for free school meals. Please fill out an application.
Who should I include as household members? Include yourself and all other people living in the household, related or not (such as grandparents, other relatives, or friends).
May I apply if someone in my household is not a U.S. citizen? Yes. You or your children do not have to be U.S. citizens for your children to qualify for free or reduced-price school meals.
What if my income is not always the same? List the amount that you normally get. If you normally get overtime, include it, but not if you get overtime only sometimes. For seasonal work, write in the total annual income.
Will the information I give be checked? Yes, and we may also ask you to send written proof.
How will the information be kept? Information you provide on the form, and your child’s approval for school meal benefits, will be protected as private data. For more information see the back page of the Application for Educational Benefits.
If I don’t qualify now, may I apply later? Yes. Please complete an application at any time if your income goes down, your household size goes up, or you start getting SNAP, MFIP or FDPIR benefits.
Please provide the information requested about children’s racial identity and ethnicity, which helps to make sure we are fully serving our community. This information is not required for approval of school meal benefits.
If you have other questions or need help, call me at 952-232-2061, or email me at [email protected].
Sincerely,
Julie Wharton Student Nutrition Support Specialist
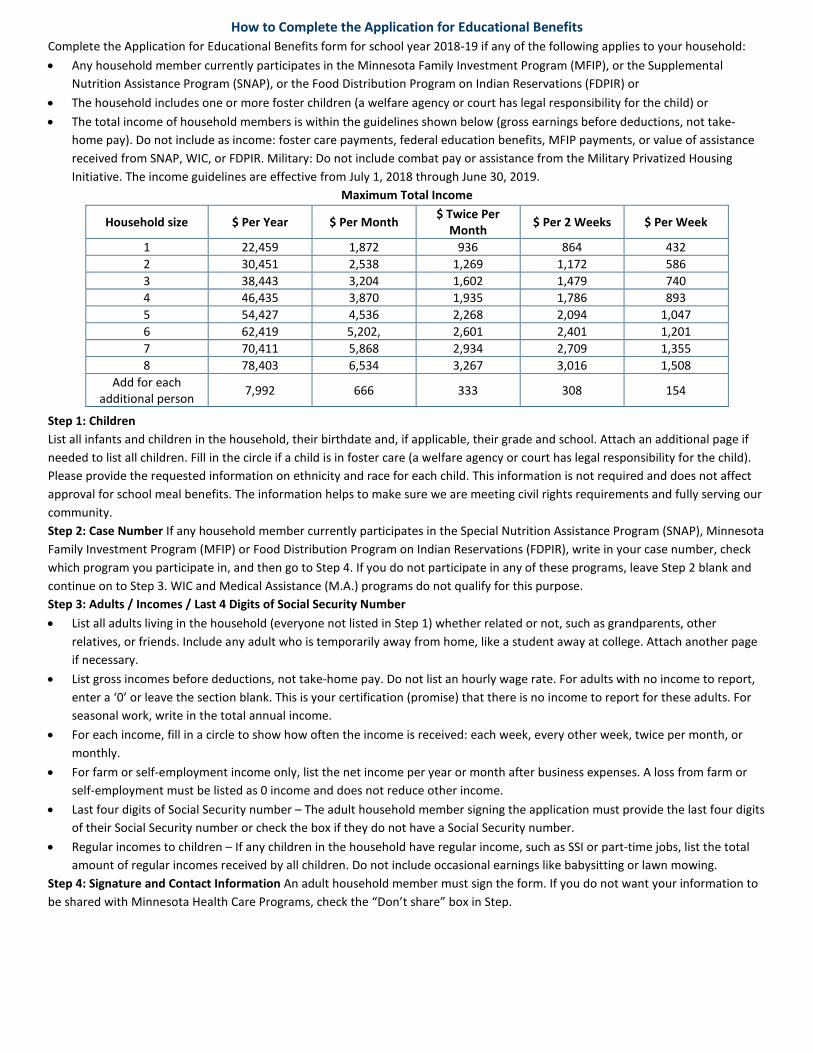
How to Complete the Application for Educational Benefits Complete the Application for Educational Benefits form for school year 2018-19 if any of the following applies to your household: • Any household member currently participates in the Minnesota Family Investment Program (MFIP), or the Supplemental
Nutrition Assistance Program (SNAP), or the Food Distribution Program on Indian Reservations (FDPIR) or • The household includes one or more foster children (a welfare agency or court has legal responsibility for the child) or • The total income of household members is within the guidelines shown below (gross earnings before deductions, not take-
home pay). Do not include as income: foster care payments, federal education benefits, MFIP payments, or value of assistance received from SNAP, WIC, or FDPIR. Military: Do not include combat pay or assistance from the Military Privatized Housing Initiative. The income guidelines are effective from July 1, 2018 through June 30, 2019.
Maximum Total Income
Household size $ Per Year $ Per Month $ Twice Per Month $ Per 2 Weeks $ Per Week
1 22,459 1,872 936 864 432 2 30,451 2,538 1,269 1,172 586 3 38,443 3,204 1,602 1,479 740 4 46,435 3,870 1,935 1,786 893 5 54,427 4,536 2,268 2,094 1,047 6 62,419 5,202, 2,601 2,401 1,201 7 70,411 5,868 2,934 2,709 1,355 8 78,403 6,534 3,267 3,016 1,508
Add for each additional person 7,992 666 333 308 154
Step 1: Children List all infants and children in the household, their birthdate and, if applicable, their grade and school. Attach an additional page if needed to list all children. Fill in the circle if a child is in foster care (a welfare agency or court has legal responsibility for the child). Please provide the requested information on ethnicity and race for each child. This information is not required and does not affect approval for school meal benefits. The information helps to make sure we are meeting civil rights requirements and fully serving our community. Step 2: Case Number If any household member currently participates in the Special Nutrition Assistance Program (SNAP), Minnesota Family Investment Program (MFIP) or Food Distribution Program on Indian Reservations (FDPIR), write in your case number, check which program you participate in, and then go to Step 4. If you do not participate in any of these programs, leave Step 2 blank and continue on to Step 3. WIC and Medical Assistance (M.A.) programs do not qualify for this purpose. Step 3: Adults / Incomes / Last 4 Digits of Social Security Number • List all adults living in the household (everyone not listed in Step 1) whether related or not, such as grandparents, other
relatives, or friends. Include any adult who is temporarily away from home, like a student away at college. Attach another page if necessary.
• List gross incomes before deductions, not take-home pay. Do not list an hourly wage rate. For adults with no income to report, enter a ‘0’ or leave the section blank. This is your certification (promise) that there is no income to report for these adults. For seasonal work, write in the total annual income.
• For each income, fill in a circle to show how often the income is received: each week, every other week, twice per month, or monthly.
• For farm or self-employment income only, list the net income per year or month after business expenses. A loss from farm or self-employment must be listed as 0 income and does not reduce other income.
• Last four digits of Social Security number – The adult household member signing the application must provide the last four digits of their Social Security number or check the box if they do not have a Social Security number.
• Regular incomes to children – If any children in the household have regular income, such as SSI or part-time jobs, list the total amount of regular incomes received by all children. Do not include occasional earnings like babysitting or lawn mowing.
Step 4: Signature and Contact Information An adult household member must sign the form. If you do not want your information to be shared with Minnesota Health Care Programs, check the “Don’t share” box in Step.
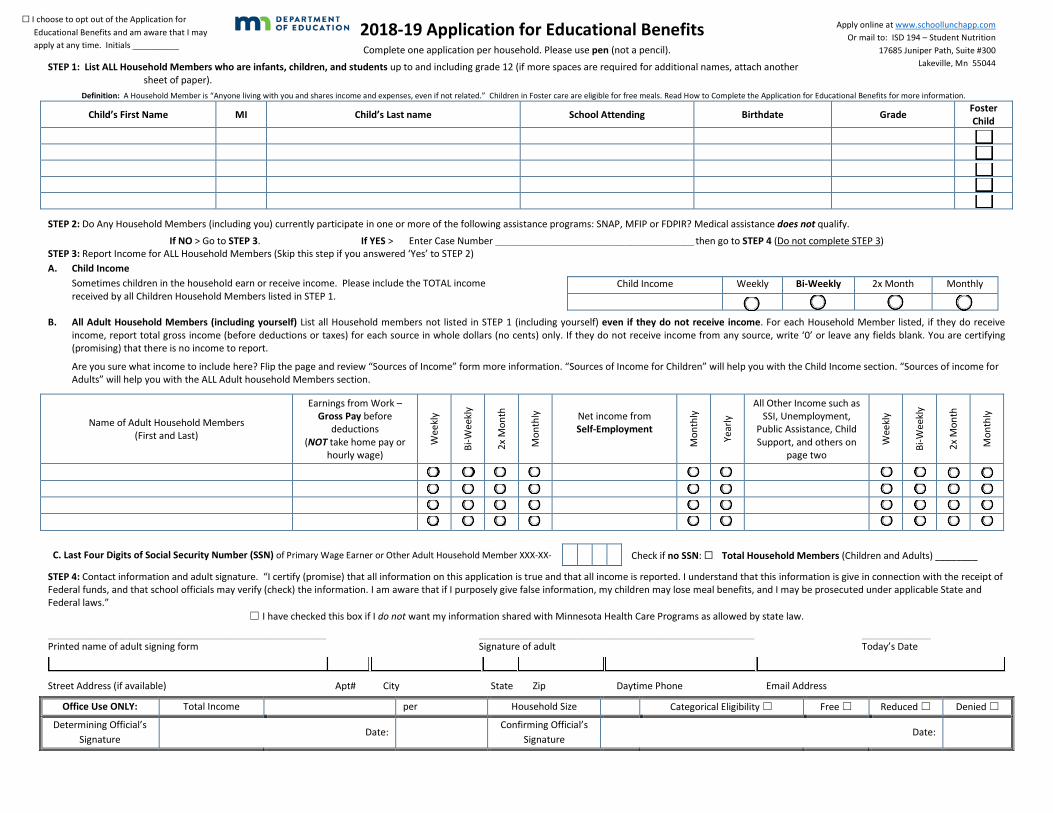
2018-19 Application for Educational Benefits Complete one application per household. Please use pen (not a pencil).
STEP 1: List ALL Household Members who are infants, children, and students up to and including grade 12 (if more spaces are required for additional names, attach another sheet of paper).
Definition: A Household Member is “Anyone living with you and shares income and expenses, even if not related.” Children in Foster care are eligible for free meals. Read How to Complete the Application for Educational Benefits for more information.
Child’s First Name MI Child’s Last name School Attending Birthdate Grade Foster Child
☐ ☐ ☐ ☐ ☐
STEP 2: Do Any Household Members (including you) currently participate in one or more of the following assistance programs: SNAP, MFIP or FDPIR? Medical assistance does not qualify.
If NO > Go to STEP 3. If YES > Enter Case Number ____________________________________________________________ then go to STEP 4 (Do not complete STEP 3) STEP 3: Report Income for ALL Household Members (Skip this step if you answered ‘Yes’ to STEP 2) A. Child Income
Sometimes children in the household earn or receive income. Please include the TOTAL income received by all Children Household Members listed in STEP 1.
Child Income Weekly Bi-Weekly 2x Month Monthly ☐ ☐ ☐ ☐
B. All Adult Household Members (including yourself) List all Household members not listed in STEP 1 (including yourself) even if they do not receive income. For each Household Member listed, if they do receive income, report total gross income (before deductions or taxes) for each source in whole dollars (no cents) only. If they do not receive income from any source, write ‘0’ or leave any fields blank. You are certifying (promising) that there is no income to report.
Are you sure what income to include here? Flip the page and review “Sources of Income” form more information. “Sources of Income for Children” will help you with the Child Income section. “Sources of income for Adults” will help you with the ALL Adult household Members section.
Name of Adult Household Members (First and Last)
Earnings from Work – Gross Pay before
deductions (NOT take home pay or
hourly wage)
Wee
kly
Bi-W
eekl
y
2x M
onth
Mon
thly
Net income from Self-Employment
Mon
thly
Year
ly
All Other Income such as SSI, Unemployment,
Public Assistance, Child Support, and others on
page two
Wee
kly
Bi-W
eekl
y
2x M
onth
Mon
thly
☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐
C. Last Four Digits of Social Security Number (SSN) of Primary Wage Earner or Other Adult Household Member XXX-XX- Check if no SSN: ☐ Total Household Members (Children and Adults) ________
STEP 4: Contact information and adult signature. “I certify (promise) that all information on this application is true and that all income is reported. I understand that this information is give in connection with the receipt of Federal funds, and that school officials may verify (check) the information. I am aware that if I purposely give false information, my children may lose meal benefits, and I may be prosecuted under applicable State and Federal laws.”
☐ I have checked this box if I do not want my information shared with Minnesota Health Care Programs as allowed by state law.
_________________________________________________________________________________________________________ ________________________________________________________________________________________________________ __________________________
Printed name of adult signing form Signature of adult Today’s Date
Street Address (if available) Apt# City State Zip Daytime Phone Email Address
Office Use ONLY: Total Income per Household Size Categorical Eligibility ☐ Free ☐ Reduced ☐ Denied ☐
Determining Official’s Signature
Date: Confirming Official’s
Signature Date:
Apply online at www.schoollunchapp.com Or mail to: ISD 194 – Student Nutrition
17685 Juniper Path, Suite #300 Lakeville, Mn 55044
☐ I choose to opt out of the Application for Educational Benefits and am aware that I may apply at any time. Initials __________

INSTRUCTIONS: Sources of Income
Sources of Income for Children Sources of Income for Adults
Sources of Child Income Examples NA Earnings from Work Public Assistance / Alimony
/ Child Support All Other Income
• Earnings from work • Social Security
o Disability Payments o Survivor’s Benefits
• Income from person outside the household
• Income from any other source
• A child has a regular full or part-time job where they earn a salary or wages
• A child is blind or disabled and receives Social Security
• A Parent is disabled, retired, or deceased, and their child receives Social Security benefits
• A friend or extended family member regularly gives a child spending money
• A child receives regular income from a private pension fund, annuity, or trust
• Salary, wages, cash bonuses (before deductions or taxes)
• Net income from self-employment (farm or business)
• If you are in the U.S. Military: o Basic pay and cash bonuses (do
NOT include combat pay, FSSA or privatized housing allowances)
o Allowances for off-base housing, food and clothing
• Cash Assistance from State or local government
• Supplemental Security Income • Unemployment benefits • Worker’s compensation • Alimony payments • Child support payments • Veteran’s benefits • Strike benefits
• Social Security • Disability benefits • Regular income from
trusts or estates • Annuities • Investment income • Rental income • Regular cash payments
from outside household
OPTIONAL: Children’s Racial and Ethnic Identities We are required to ask for information about your children’s race and ethnicity. This information is important and helps to make sure we are fully serving our community. Responding to this section is optional and does not affect your children’s eligibility for free or reduced price meals. Ethnicity (check one): ☐ Hispanic or Latino ☐ Not Hispanic or Latino Race (check one or more): ☐ American Indian or Alaskan Native ☐ Asian ☐ Black or African American ☐ Native Hawaiian or Other Pacific Islander ☐ White
The Richard B. Russell National School Lunch Act requires the information on this application. You do not have to give the information, but if you do not, we cannot approve your child for free or reduced price meals. You must include the last four digits of the social security number of the adult household member who signs the application. The last four digits of the social security number is not required when you apply on behalf of a foster child or you list a Supplemental Nutrition Assistance Program (SNAP), Temporary Assistance for Needy Families (TANF) Program or Food Distribution Program on Indian Reservations (FDPIR) case number or other FDPIR identifier for your child or when you indicate that the adult household member signing the application does not have a social security number. We will use your information to determine if your child is eligible for free or reduced price meals, and for administration and enforcement of the lunch and breakfast programs. We MAY share your eligibility information with education, health, and nutrition programs to help them evaluate, fund, or determine benefits for their programs, auditors for program reviews, and law enforcement officials to help them look into violations of program rules. At public school districts, each student’s school meal status also is recorded on a statewide computer system used to report student data to MDE as required by state law. MDE uses this information to: (1) Administer state and federal programs, (2) Calculate compensatory revenue for public schools, and (3) Judge the quality of the state’s educational program.
In accordance with Federal civil rights law and U.S. Department of Agriculture (USDA) civil rights regulations and policies, the USDA, its Agencies, offices, and employees, and institutions participating in or administering
USDA programs are prohibited from discriminating based on race, color, national origin, sex, disability, age, or reprisal or retaliation for prior civil rights activity in any program or activity conducted or funded by USDA. Persons with disabilities who require alternative means of communication for program information (e.g. Braille, large print, audiotape, American Sign Language, etc.), should contact the Agency (State or local) where they applied for benefits. Individuals who are deaf, hard of hearing or have speech disabilities may contact USDA through the Federal Relay Service at (800) 877-8339. Additionally, program information may be made available in languages other than English. To file a program complaint of discrimination, complete the USDA Program Discrimination Complaint form, (AD-3027) online at: https://www.ascr.usda.gov/filing-program-discrimination-complaint-usda-customer, and at any USDA office, or write a letter addressed to USDA and provide in the letter all of the information requested in the form. To request a copy of the complaint form, call (866) 632-9992. Submit your completed form or letter to USDA by: mail: U.S. Department of Agriculture
Office of the Assistant Secretary for Civil Rights 1400 Independence Avenue, SW Washington, D.C. 20250-9410 fax: (202) 690-7442; or email: [email protected].
This institution is an equal opportunity provider.
Do not fill out: For School Use Only
Annual Income Conversion: Weekly x 52, Every 2 Weeks x 26, Twice a Month x 24, Monthly x 12
Total Income Weekly Bi-Weekly 2x Month Monthly Household Size Categorical Eligibility Free Reduced Denied ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐
_______________________________________________________________________________________ _____________________________________________________________________________________ Determining Official’s Signature Date Confirming Official’s Signature Date ☐ Selected for Verification – attach Verification Tracker

Lakeville Area Public Schools
Student Information Services
Consent to Share Information for Benefits for Other Programs
Children who are eligible to receive federal and state educational benefits such as free or reduced-price meals may also receive additional benefits such as reduced athletic fees, reduced transportation fees, or additional academic support.
If you agree to share this information, your children’s eligibility status will be shared with other school staff on a need-to-know basis for the purposes described in this form and will not be shared with anyone else.
Please complete your children’s information and check (√) the appropriate boxes. Your agreement to share this information is completely voluntary. Declining to share your children’s eligibility with other ISD194 programs will not affect their eligibility for free or reduced-price meals.
Student Name Grade School Name Please check (√) the box or boxes that apply:
□ YES. I want my children’s eligibility to be shared with the programs I have checked (√) below. I understand not all benefits and programs will be available to students at every school and every grade level.
□ Student Fees □ Academic Support □ Community Education □ Transportation □ Athletics / Activities □ Class Fees
□ NO. I DO NOT want to share my children’s eligibility for educational benefits such as free or
reduced-price meals with other programs. Signature of Parent/Guardian:
Date:
Printed Name:
Please return this form with your application or send to:
Lakeville Area Public Schools, Student Information Support, 8670 210th St West, Lakeville, MN 55044
OR fax to 952-469-7660
Lakeville Area Public Schools ISD #194 • Student Information Services • Revised 1.2.2018
![˘ ˇ - Forum chauffageˇ˛ ˘# # ’ ˘ ˘ ,# ˚+ ˘ * $ , C D##(9 - & D#ˇ DDE(!" & ˘# # ’ ˘ ˘ ,# ˚+ ˘]] 0 ; S 9 S T#DQ˛T=] ] ] ] 0 ; S 9 S T#DQ˛T=](https://img.pdfslide.us/doc/110x75/61223cb4ca6f6a43714a9bd3/-forum-a-c-d9-d-dde.jpg)