Embed Size (px)
Citation preview

Enhancing Endocrine Therapy for Hormone Receptor Positive
Advanced Breast Cancer
Sung-Bae Kim, MD, PhDProfessor, Dept of Oncology,
Asan Medical CenterUniversity of Ulsan College of Medicine
Seoul, Korea

Outline
• Overview• AI or Fulvestrant• Endocrine resistance - ESR1• mTOR inhibitor/CDK4/6 inhibitors • Cotargeting signaling pathways• Immuno-oncology drug in ER+

Conclusions: Treatment of ER+ MBCFirst Line Rx:
– Can achieve PFS of ~14-16 months with single agent AI or fulvestrant• Likely ‘ceiling’ for endocrine alone approach, but still an important option for many
– Combination approaches with CDK 4/6 inhibitors can achieve 1st PFS of 24+ months:• Do all patients need a combination approach 1st Line ? • What therapy do we use after progression on CDK 4/6 inhibitors ?
Second Line Rx:– Combination approaches standard of care with additional 2nd PFS of 7–9 months
• Wide range of targets still under investigation (ie. PI3K, mTOR/ AKT)
Sequencing and Patient Selection:– Always consider tumor biology, clinical features, and patient factors when selecting
most appropriate therapy

4
Oopho‐rectomy2,3
Abbreviations: AI, aromatase inhibitor; ERDs, estrogen receptor downregulator; HR+; hormone receptor positive; SERMS, selective estrogen receptor modulators. * Marginal improvement over lower dose fulvestrant.1. http://www.advancedbreastcancercommunity.org/treatment/drugs.htm; 2. Beatson CT. Lancet. 1896;2:104‐107; 3. Beatson CT. Lancet. 1896;2:162‐165; 4. Cohen MH, et al. Oncologist. 2001;6:4‐11; 5. Faslodex [package insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2011.
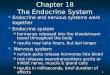
SERMS4• Tamoxifen• Toremifene
AIs4• Anastrozole• Letrozole• Exemestane
ERDs5• Fulvestrant
ERDs5• High‐doseFulvestrant*
1896 1977 1990s 2002 2010
Targeting mechanisms of endocrine resistance: everolimus
2012 Endocrine Therapy
Chemo‐therapy 1990s1980s 2000s
Others1• Capecitabine• Gemcitabine• Ixabepilone • Eribulin• Nab‐paclitaxel
Taxanes1• Paclitaxel• Docetaxel
Anthracyclines1• Doxorubicin• Epirubicin
Evolution of Chemo/Endocrine Treatment in Advanced Breast Cancer
2015
Palbociclib
2017
Ribociclib

1st-line hormonal therapy1st-line hormonal therapy 1st-line chemotherapy1st-line chemotherapy
Determine sites and extent of disease & symptoms; ER status; HER2 status; disease free & treatment-free intervals; performance status
Determine sites and extent of disease & symptoms; ER status; HER2 status; disease free & treatment-free intervals; performance status
No Response
No life-threatening diseaseHormone-responsive
Hormone-unresponsive, orlife-threatening disease
Response No Response
2nd-line hormonal therapy
2nd-line chemotherapy
Progression
Progression
Progression
Progression
3rd-line hormonal therapy
Response
No Response
3rd-line chemotherapy
Supportive care
Management of post-menopausal ER+ MBC
NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. V3.2012
Median PFS 3 moMedian PFS 3–4 mo
Median PFS 9 moMedian PFS 9–13 mo

Criteria to support 1st line choicesin ER+ HER2- advanced disease
Criteria In favor of chemotherapy
Uncertain(grey area)
In favor of endocrine therapy
DFI < 1year 1-2 years > 2yearsVisceral metastases High burden,
impending organ dysfunction (visceral crisis)
Moderate burden Minimal burden or absent
Symptoms Prominent Moderate Minimal or asymptomatic
Hart CD, et al. Nat Rev Clin Oncol 2015

Definition of endocrine resistance

PFS / TTP of AIs as 1st-line endocrine therapytrials in HR+ MBC
Trial Date AI (months) Tamoxifen(months)
AI + fulvestrant 250mg (months) HR
Nabholtz et alAnastrozole vs tamoxifen 2000 11.1 5.6 - 0.81
Bonneterre et al Anastrozole vs tamoxifen 2001 8.2 8.3 - 0.99
Mouridsen et al Letrozole vs tamoxifen 2001 9.4 6.0 - 0.72
Chernozemsky et alExemestane vs tamoxifen 2007 12.0 8.3 - -
Paridaens et alExemestane vs tamoxifen 2008 9.9 5.8 - 0.84
Mehta et al (SWOG0226)Anastrozole vs anastrozole + fulvestrant 250mg
2012 13.5 - 15.0 0.80
Bergh et al (FACT)Anastrozole vs anastrozole + fulvestrant 250mg
2012 10.2 - 10.8 0.99
Range 8–13 6–8 10–15
Plenary Lecture 1. San Antonio Breast Cancer Symposium, Dec 6-10, 2016

ER +ve , HER2 negative Locally advanced (not suitable for surgery) or
metastatic disease Up to 1 line of chemotherapy At least 1 lesion that can be assessed
FALCON: Phase III 1st line study of Fulvestrant 500 vs AI in Endocrine Therapy Naïve MBC / LABC
• Primary endpoint: PFS• Secondary endpoint: OS
– Other secondary endpoints include ORR, CBR, duration of response, duration of clinical benefit, time to deterioration of HRQoL, Safety
Fulvestrant 500mg i.m.
Anastrozole1mg OD
N=450
Note no prior endocrine therapy allowed
Ellis et al, LBA14 ESMO 2016
Plenary Lecture 1. San Antonio Breast Cancer Symposium, Dec 6-10, 2016

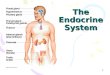
Primary endpoint: PFS
Ellis et al, LBA14 ESMO 2016
HR 0.797 (95% CI 0.637, 0.999) p=0.0486
Median PFSFulvestrant: 16.6 monthsAnastrozole: 13.8 months
Number of patients at risk:
FulvestrantAnastrozole
230232
187194
171162
150139
124120
110102
9684
8160
6345
4431
2422
1110
20
00
Prop
ortio
n of
pat
ient
s al
ive
and
prog
ress
ion
free
Time (months)
0.9
1.0
0.7
0.8
0.5
0.6
0.3
0.4
0.1
0.00 3 6 9 12 15 18 21 24 27 30 3633 39
0.2
Fulvestrant (n=230)Anastrozole (n=232)
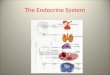
PFS without visceral disease
HR 0.59 (95% CI 0.42, 0.84)
Median PFS Fulvestrant: 22.3 monthsAnastrozole: 13.8 months
Prop
ortio
n of
pat
ient
s al
ive
and
prog
ress
ion-
free
Time (months)
0.9
1.0
0.7
0.8
0.5
0.6
0.3
0.4
0.1
0.0
0.2
0 5 10 15 20 25 30 35 40
Fulvestrant (n=95) Anastrozole (n=113)
PFS with visceral disease
Prop
ortio
n of
pat
ient
s al
ive
and
prog
ress
ion-
free
Time (months)
0.9
1.0
0.7
0.8
0.5
0.6
0.3
0.4
0.1
0.00 5 10 15 20 25 30 35 40
0.2
HR 0.99 (95% CI 0.74, 1.33)
Median PFS Fulvestrant: 13.8 monthsAnastrozole: 15.9 months
Fulvestrant (n=135) Anastrozole (n=119)
FALCON: Phase III 1st line study of Fulvestrant 500 vs AI in Endocrine Therapy Naïve MBC / LABC
Plenary Lecture 1. San Antonio Breast Cancer Symposium, Dec 6-10, 2016

Rationale for the Combination of Fulvestrant plus Aromatase Inhibitors
Brodie A et al, Cancer Res 65:5439-44, 2005
Macedo et al, Cancer Res 68, 3516-22, 2008

EligibilityPostmenopausal
ER+1st line therapy for MBC>1 yr since adjuvant AI
1° EndpointTTP / PFS
Anastrozole
1 mg PO QD
Anastrozole plus Fulvestrant
500 mg d1, 250 mg d14, 28 and every 28 days thereafter
1:1 randomization
SCHEMA for FACT and SWOG 0226 Trials

Bergh J et al. JCO 2012;30:1919-1925
FACT: PFS SWOG 0226: PFS
Mehta RS et al. N Engl J Med 2012;367:435-444
Fulvestrant 250 + AI as 1st-line Rx for ER+ MBC

SWOG 0226: PFS according to subgroups
Mehta RS et al. N Engl J Med 2012;367:435-444

AI blinded
SoFEA Trial Design: Fulvestrant + Anastrozole vs Fulvestrant + Placebo vs Exemestane
ER+ and/or PgR+ postmenopausal patients with locally advanced/ metastatic BC following progression on NSAI
RANDOMIZE
Exemestanen = 250
Fulvestrant 250 mg +placebo
n = 250
Fulvestrant 250 mg +Anastrozole n = 250
Abbreviation: AE, adverse event; AI, aromatase inhibitor; BC, breast cancer; ER+, estrogen-receptor–positive; NSAI, nonsteroidal aromatase inhibitor; PgR+, progesterone-receptor–positive.
Johnston SRD, et al. Lancet Oncol 2013. 15

SoFEA Results: Fulvestrant + Anastrozole vsFulvestrant + Placebo vs Exemestane
FUL + ANA FUL alone EXE aloneMedian PFS 4.4 months 4.8 months 3.4 monthsMedian OS 20.2 months 19.4 months 21.6 monthsORR 7.4% 6.9% 3.6%
Abbreviation: AE, adverse event; ANA, anastrozole; BC, breast cancer; EXE, exemestane; FUL, fulvestrant; ORR, objective response rate; OS, overall survival; PFS, progression-free survival.
Johnston SRD, et al. Lancet Oncol 2013.
• AE profiles were similar across treatment arms except for rates of dyspnea in the FUL alone arm
• 12 deaths not related to BC (4 in each arm) were reported
16

Effects of ER Mutational Status
Disease Progression and LBD Mutation Frequency50
40
30
20
10
0Primary Early
MetastaticDisease
LateMetastaticDisease
0
12
20
Patie
nts W
ithLB
D M
utations, %
LiToy, W. et al. Nat Gen 2013Robinson, D.R. et al. Nat Gen 2013
Jeselsohn, R. et al. Clin Cancer Res 2014

Acquired ESR1 mutation in metastatic ER+ breast cancer
• ESR1 mutation confers constitutiveER activation without ligand binding.
• ER antagonists partially inhibit mutant ER transcription activity whereas higher concentration of fulvestrant fully inhibits growth of ER mutant cell lines.
Toy W, et al. Nature Genetics 2013;45:1439

Toy et al. J Nat Gen 2013
ESR1 mutations activate the estrogen receptor
LBD ESR1 mutationsLigand independent
signaling
Constitutive agonist conformation through the formation of hydrogen bonds between S537 or G538 and N351 in helix 12

Fribbens C, et al. J Clin Onc. 2016;34(25):2961-8
ESR1 wild type
ESR1 wild typeESR1 mutated


22
The Cell Cycle Regulators
M G1
G2 S
CDK4/6Cyclin D1/D2/D3
CDK2Cyclin A
CDK2Cyclin E
CDK1 Cyclin A
CDK1 Cyclin B
• Go:resting phase; G1:prepare for DNA synthesis/ checkpoint
• S:DNA synthesis; G2:pre-division/mitosis, checkpoint, M:mitosis/cell division

23
Regulation of the G1/S Checkpoint
RB
RB
Gene transcriptionG2 S
M
G1
G0
PP P
P
Inactive
Active tumor suppressor
E2F
E2F
CDK4/6Cyclin D
Pl3K/Akt
STATs MAPKs
(ER/PR/AR) Wnt/β-catenin
NF-κB
p16


p16
G1 S phase G2 MG1 S phase G2 M
Cyclin D
Cdk4
E2F/DP1
Rb
E2F/DP1
Rb
E2F/DP1inactive
active
PP
PP
Rb
PP
PP
CDK4Amplification/Mutation:
Sarcomas (18%)Gliomas (18%)Melanoma (5%)
Rb - Inactivation:Retinoblastoma (100%)
SCLC (90%)NSCLC (30%)Gliomas (14%)
Cyclin D1-Amplification:
Head and Neck (43%)Esophageal (34%)
Breast (13%)
P16Deletion/Mutation/
MethylationGlioblastoma (70%)Mesothelioma (55%)
Pancreatic (50%)
Over-Expression:MCL t(11;14) translocation
Myeloma (34%)
Dickson MA, Schwartz GK. Curr Oncol 2009;16:36–43Shapiro GI. J Clin Oncol 2006;24:1770–83
Defects in the RB/CDK4/Cyclin D/p16 Pathway are common

Timeline of CDKs• Early 1970s: Lee Hartwell identifies a number of genes involved in cell
division “CDCs” (cell division cycle) – Using yeast mutation model identified genes involved in the cell cycle
– Developed the concept of “checkpoints”
• Late 1970s/early 1980s: Paul Nurse, again using yeast models, identifies other cdc2 and demonstrates its role in controlling the cell cycle
– Demonstrates the function of CDKs and their conservation
• Early 1980s: Tim Hunt, using sea urchins, identifies proteins that increase before cell division, then abruptly drop off (a cyclical pattern) – Cyclins and their degradation as a control mechanism in the cell cycle
• 2001: Hartwell, Nurse, and Hunt win the Noble Prize in Medicine and Physiology

Objectives of the meeting in Yr 2004

Palbociclib - A Sleeping Beauty

Preferential inhibition of Luminal ER+ and HER2+ breast cancer cell lines by palbociclib
Finn RS, et al. BCR 2009;11(5):R77. Non-luminal/post EMT
Non-luminal
LuminalHER2 amplifiedImmortalized
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint and/or distribute

30
Palbociclib Acts Synergistically with Tamoxifen in ER+ Breast Cancer Cell Lines
Palbociclib Acts Synergistically with Tamoxifen in ER+ Breast Cancer Cell Lines
Tamoxifen 10000 5000 2500 1250 625 312Palbociclib 100 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inhi
bitio
n (%
)
Concentration nM
Tamoxifen 5000 2500 1250 625 312Palbociclib 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inhi
bitio
n (%
)
Concentration nM
Tamoxifen 5000 2500 1250 625 312Palbociclib 50 25 12.5 6.25 3.125
100
80
60
40
20
0
Inhi
bitio
n (%
)
Concentration nM
MCF7CIm = 0.37±0.04
EFM19CIm = 0.45±0.09
T47DCIm = 0.1±0.01
Palbociclib alone Tamoxifen alone Palbociclib/Tamoxifen combination
Finn RS, et al. Breast Cancer Res. 2009;11(5):R77
● Mean combination index (CIm) <1 indicates synergy for the combinations

Abemaciclib Palbociclib Ribociclib
Selective CDK 4/6 inhibitors
O’Leary B, et al. Nat Rev Clin Oncol. 2016;13(7):417–430.

Clinical data for CDK 4/6 inhibitors in HR+/HER2– MBC
• Palbociclib: NCT00721409, NCT01740427, NCT01942135• Abemaciclib: NCT02102490 • Ribociclib: NCT01958021
1L ER+, HER2–mBC
Palbociclib + AI (letrozole)
Recurrent HR+, HER2– mBC
Palbociclib + fulvestrant
PALOMA-3PALOMA-3PALOMA-1PALOMA-1
1L ER+, HER2–mBC
Palbociclib + AI (letrozole)
2015 20162014
PALOMA-2PALOMA-2
1L ER+, HER2–ABC
Ribociclib + letrozole
MONALEESA-2MONALEESA-2
Recurrent ER+, HER2– mBCAbemaciclib
MONARCH-1MONARCH-1
Other trials ongoing
Data read-out dates
www.clinicaltrials.gov

PALOMA-2 & MOLALEESA-2: Design of Phase III Studies
• Primary endpoint: PFS• Secondary endpoints:
– Response, OS, safety, biomarkers, PROs
PALOMA-2
RANDOMISE
Palbociclib (125 mg QD, 3/1
schedule) + letrozole
(2.5 mg QD)
Placebo + letrozole
(2.5 mg QD)
Postmenopausal ER+ HER2– advanced breast cancer with
no prior treatment for advanced disease. AI-resistant patients excluded
N=666
(2:1)
Stratified by the presence/absence of liver and/or lung metastases
Ribociclib (600 mg QD,3/1 schedule)
+letrozole
(2.5 mg QD)
Placebo+ letrozole
(2.5 mg QD)
• Primary endpoint: PFS • Secondary endpoints:
– OS (key), ORR, CBR, safety
Postmenopausal women with HR+/HER2– advanced breast cancer withno prior therapyfor advanced
disease
N=668
MOLALEESA-2
RANDOMISE
(1:1)

Populations in recent Phase III 1st-line ER+ MBC trialsPALOMA-21
(n=666)MONALEESA-22
(n=668)SWOG-02263
(n=707)FALCON4
(n=462)Disease Free Interval
De novo MBC< 12 mo> 12 mo
37%22%40%
34%2%
64%
39%nil
61%(> 10 yr) 28%
MBC 87 %LABC 18 %
Prior TreatmentAdjuvant Endocrine Rx
Adjuvant ChemotherapyChemotherapy for MBC
56%40%nil
52%43%nil
40 %33 %
nil
nil19 %17 %
Site of Disease
VisceralBone only
48%23%
59%21%
54 %22 %
55 %10 %
Median PFS for AI control (95 % CI)
14.5 mo(12.9 - 17.1)
14.7 mo(13.0 – 16.5)
13.5 mo(12.1 – 15.1)
13.8 mo(NR)
1. Finn R, et al. NEJM. 2016;375(20):1925–1936; 2. Hortobagyi G, et al. NEJM. 2016;375(18):1738–1748;
3. Mehta RS et al. N Engl J Med 2012;367:435-44; 4. Ellis et al, LBA14 ESMO 2016

PALOMA-2
Finn R, et al. NEJM. 2016;375(20):1925–1936
mPFS (months)Palbociclib–letrozole: 24.8Placebo–letrozole: 14.5
MONALEESA-2
Hortobagyi G, et al. NEJM. 2016;375(18):1738–1748
mPFS (months)ribociclib–letrozole: NRplacebo–letrozole: 14.7
PALOMA-2 & MONALEESA-2: PFS
mPFS (months)Ribociclib–letrozole: NRPlacebo–letrozole: 14.7

PALOMA-2 & MONALEESA-2: Secondary endpointsPALOMA-2
Measurable diseaseMONALEESA-2
Measurable disease
55.3
84.3
44.4
70.8
0
10
20
30
40
50
60
70
80
90
100
Objective response rate Clinical benefit rate
Palbociclib + letrozole
Placebo + letrozole
53
80.1
37
71.8
0
10
20
30
40
50
60
70
80
90
100
Objective response rate Clinical benefit rate
Ribociclib + letrozole
Placebo + letrozole
OR (95% CI): 1.55 (1.05–2.28)p=0.03
OR (95% CI): 2.23 (1.39–3.56)p<0.001
p=0.00028
p=0.02
Rate
(%
)
Finn R, et al. NEJM. 2016;375(20):1925–1936Finn R, et al. Abstract 507, ASCO 2016
Hortobagyi G, et al. NEJM. 2016;375(18):1738–1748Hortobagyi G, et al. LBA01, ESMO 2016
Rate
(%
)

PALOMA-2 MONALEESA-2
Finn R, et al. NEJM. 2016;375(20):1925–1936 Hortobagyi G, et al. NEJM. 2016;375(18):1738–1748
PALOMA-2 & MONALEESA-2: Toxicity

BOLERO-2 & PALOMA-3: Design of Phase III studies
(2:1)
Palbociclib (125 mg QD; 3 weeks on, 1 week off) + fulvestrant (500
mg IM Q4W)(n=347)
Placebo (3 weeks on, 1 week off) + fulvestrant (500 mg IM Q4
W)(n=174)
HR+, HER2- ABCPre/peri or postmenopausalProgressed on prior ET on or within 12 months of adjuvant therapy and/or on therapy for advanced breast cancer1 or more prior chemotherapy regimen for advanced cancer
• Primary endpoint: PFS• Secondary endpoints:
– OS, ORR, Safety, QoL, CBR
(2:1)
Everolimus 10 mg daily + exemestane 25 mg
daily(n=485)
Placebo + exemestane
25 mg daily(n=239)
Postmenopausal women with estrogen receptor positive locally advanced or metastatic breast cancer who are refractory to letrozole or anastrozole
• Primary endpoint: PFS• Secondary endpoints:
– OS, OR, CBR, Safety, QoL
BOLERO-2 PALOMA-3
RANDOMISE
RANDOMISE

BOLERO-2 & PALOMA-3: PFS
Turner N, et al. N Engl J Med 2015;373:209-19Baselga J, et al. N Engl J Med 2012;366:520-9
BOLERO-2 PALOMA-3

BOLERO-2 & PALOMA-3: SafetyBOLERO-2 PALOMA-3
Turner N, et al. N Engl J Med 2015;373:209-19Baselga J, et al. N Engl J Med 2012;366:520-9

Biomarkers to Predict for Response to Palbociclib• Examination in MBC enrolled on Phase 2 trial assessing the efficacy of
palbociclib in patients with Rb positive metastatic cancer (UPCC 03909)• To predict for response to palbociclib
Rb, p16 or Ki-67 protein expression or CCND1 amplificationBiomarkers and PFS
Clark AS 2013 SABCG
PFS analysis with all biomarkers was not significant

PALOMA2: PFS by Biomarker
HR=hazard ratio; LET=letrozole; PAL=palbociclib; PCB=placebo; PFS=progression-free survival.
n HR (95% CI)
All patients 666 0.58 (0.46–0.72)
ER+ER–
504 62
0.57 (0.44–0.74)0.41 (0.22–0.75)
Rb+Rb–
512 51
0.53 (0.42–0.68)0.68 (0.31–1.48)
Cyclin D1+Cyclin D1–
54915
0.56 (0.44–0.71)1.0 (0.29–3.46)
p16+p16–
46684
0.52 (0.40–0.67)0.73 (0.39–1.36)
Ki-67 ≤20%Ki-67 >20%
318235
0.53 (0.38–0.74)0.57 (0.41–0.79)
HR (95% CI)
Favors PAL+LET Favors PCB+LET
Percentile n HR (95% CI)
All patients 666 0.58 (0.46–0.72)
ER status≤25th
>25th to <75th
≥75th
142282142
0.50 (0.32–0.78)0.53 (0.37–0.74)0.65 (0.41–1.05)
Rb status≤25th
>25th to <75th
≥75th
154249160
0.57 (0.36–0.88)0.46 (0.32–0.67)0.63 (0.42–0.95)
Cyclin D1 status
≤25th
>25th to <75th
≥75th
141247176
0.41 (0.26–0.65)0.69 (0.48–1.00)0.52 (0.34–0.78)
p16 status≤25th
>25th to <75th
≥75th
140258152
0.74 (0.46–1.20)0.62 (0.44–0.89)0.33 (0.21–0.52)
HR (95% CI)
Favors PAL+LET Favors PCB+LET
Qualitative Analysis Quantitative Analysis

Biomarkers for Response to Endocrine Combinations
• Biology of the Primary Tumour:
– ER & PgR expression
– Molecular Profiling (ie. PAM-50 intrinsic subtype)
– Genetics Alterations in key signaling pathways• PIK3CA / PTEN• FGFR 1/2• Cell Cycle (CCND1)
• Real Time Biology in Metastatic Disease:
– ctDNA analysis of acquired mutations (ESR1 and PIK3CA)

Baselga J. Oncologist 2011; 16: Suppl 1: 12Polivka Jr et al. Pharm Thera 2014; 142: 164
The PI3K/AKT/mTOR Pathway in Breast Cancer:Common Molecular Alterations
~40% of HR + breast cancerhave PIK3CA mutations
Frequency of PI3K and PTEN mutationsin 547 human breast cancer samples

PIK3CA mutation status & response to CDK4/6inhibitors in PALOMA-3
PIK3CA mutant PIK3CA WT
PIK3CA mutations do not predict response to CDK4 inhibitors
Cristofanilli M, et al. Lancet Oncol. 2016;17(4):425–439.

PI3K
AKT
PTEN
mTOR
RAS
RAF
MEK
MAPK
ER target gene transcription
P P
EGFRHER2
E
E
ERE
ERE
ERE
TKI
Aromatase InhibitorNonsteroidal AIs
Anastrozole Letrozole
Steroidal AIsExemestane
Aromatase InhibitorNonsteroidal AIs
Anastrozole Letrozole
Steroidal AIsExemestane
Selective Estrogen Receptor ModulatorsTamoxifen Toremifene
Selective Estrogen Receptor ModulatorsTamoxifen Toremifene
ER DownregulatorFulvestrant
ER DownregulatorFulvestrant
Combining Targeted and Antiestrogen Therapies in HR-Positive Breast Cancer
CellCycle
TranscriptionSilencing
mTOR InhibitorsEverolimusSirolimusTemsirolimus
mTOR InhibitorsEverolimusSirolimusTemsirolimus
HDAC InhibitorEntinostatHDAC InhibitorEntinostat
CDK 4/6 InhibitorPalbociclibCDK 4/6 InhibitorPalbociclib
PI3K inhibitorsBMK120BYL790GDC0980
PI3K inhibitorsBMK120BYL790GDC0980

PI3K / TORC / AKT inhibitors in clinical development 2016
AlpelisibTaselisib
Vistusertib
BuparlisibPictilisib
Prob
abilit
y of
Pr
ogre
ssio
n-fre
e Su
rviv
al, %
Time (months)
100
60
0
80
40
20
0 4 8 14 182 6 10 12 16 20 26 3022 24 28
Buparlisib + fulvestrant (n/N=349/576)
Placebo + fulvestrant (n/N=435/571)
BELLE-3
Baselga J et al, SABCS 2015 Oral Abstract S6-01
Krop IE. Lancet Oncol. 2016 Jun;17(6):811-21.
FERGI

Early adaptive resistance to CDK inhibitors
• Resistance develop rapidly, within 72 hrs
Herrera-Abreu MT, et al. Cancer Res 2016;1-13

Combined targeting: CDK4/6 and PI3K
Herrera-Abreu MT, et al. Cancer Res 2016;1-13

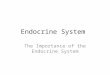
AI + CDK4/6 i24 months
AI alone8–14 months
Fulvestrant+ CDK4/6 i7–9 months
Fulvestrant 50022 months
Optimal sequencing of endocrine therapy in ER+ MBC
AI + everolimus7–9 months
0 5 10 15 20 25 30 35
Fulvestrant 5006.5 months ?
Exemestane3–4 months
Delay Start of Chemotherapy OS
Cumulative Median PFS in months
1st line
AI + CDK4/6 i7–9 months ?
AI + everolimus7–9 months ?
AI + everolimus7–9 months ?
2nd line
A B C
(ie. endo Rx naïve, non-visceral mets, biomarker)
2nd line post Fulvestrant:responsive to 2nd line combinations?
2nd Line post CDK 4/6 inhibitors:still endocrine responsive and
to what therapy?
Plenary Lecture 1. San Antonio Breast Cancer Symposium, Dec 6-10, 2016
A. Conventional ET
B. Optimally selected ET
C. Combination ET

Key Pathways of endocrine resistance
Rugo HS, et al. ASCO education book 2016

1. Klein P, et al. ASCO 2012 Breast Cancer Symposium. Abstract 128. 2. Ordentlich P. Mol Cancer Ther. 2011;10:Abstract PR‐6.
ENCORE 301: Ph II RCT of Exemestane+/-Entinostatin ER+ MBC progessing after NSAI

KEYNOTE-028 Breast Cancer Cohort: Study Design
• Phase Ib multicohort study
• Primary endpoint: ORR• Secondary endpoints: PFS, OS, DoR
Pts with locally advanced or metastatic PD-L1+, ER+/HER2- breast cancer;
failed or ineligible for standard therapy;
ECOG PS 0-1; ≥ 1 measurable lesion;
(N = 25)
Pembrolizumab10 mg/kg IV Q2W
CR, PR, or SD
PD or unacceptable toxicity
Tx to 24 mos orPD or toxicity
Discontinue
Rugo HS, et al. SABCS 2015. Abstract S5-07.

KEYNOTE-028 Breast Cancer Cohort: Antitumor Activity
Pembrolizumab showed ORR of 12% and CBR of 20%• ORR 14%, CBR 23% in 22 evaluable pts
Characteristic, % (95% CI) Pembrolizumab(N = 25)
ORR 12 (2.5-31.2)
CR 0 (0-13.7)
PR* 12 (2.5-31.2)
SD 16 (4.5-36.1)
Clinical benefit rate (CR + PR + SD for ≥ 24 wks) 20 (6.8-40.7)
PD 60 (38.7-78.9)
No assessment† 12 (2.5-31.2)
*All had received ≥ 3 lines of prior therapy in metastatic setting.†Includes pts who discontinued therapy before first post-BL scan.
Rugo HS, et al. SABCS 2015. Abstract S5-07.

Conclusions• Treatment strategies for MBC largely based on disease
pattern, symptoms and pretreatment.
• New insights in tumor biology can help predict endocrine responsiveness and optimal sequencing.
– Acquired mutation in ER‐alpha (ESR1) in response to endocrine deprivation
– Cross talk between ER and growth factor receptor signaling such as HER family members, FGFR pathways, PI3/Akt/mTOR
– Tumor microenvironment and host immune response• Understanding and inhibiting these pathways are being developed to improve efficacy of hormone therapy.