Enhanced Recovery After Surgery The ERAS protocol Prof. Ioana
Grigora Anesthesia and Intensive Care Department University of
Medicine and Pharmacy, Gr.T.Popa Regional Institute of Oncology
Iasi, Romania Slide 2 Enhancing Recovery after GI surgery Factors
influencing patient recovery Pre-op information Optimised organ
function No nutritional defects No alcohol pre-op Stop smoking
pre-op Neuraxial blockade Minimally invasive surgery Normothermia
Nausea prevention Ileus prevention Early feeding Good oxygenation
Good sleep Opioid sparing Evidence-based post-op care Anxiety, fear
Pre-op organ dysfunction Surgical stress response Hypothermia
Nausea, vomiting Ileus Semi-starvation Hypoxaemia Poor sleep Drains
& tubes Catheters Accelerated recovery Delayed recovery Slide 3
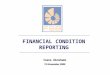
What is ERAS ? Standardized protocol for perioperative care
Function al capacity Days Weeks Traditional Care Enhanced Recovery
Henrik Kehlet, Br J Anaesth 1997; 78 : 606 Multi-modal intervention
Reduce operative stress Support organ function Reduced morbidity
Accelerate convalescence Slide 4 What is ERAS ? Standardized
protocol for perioperative care Henrik Kehlet, Br J Anaesth 1997;
78 : 606 preop information stress attenuation pain relief
exerciseenteral nutrition
nursessurgeonsanesthesistsdieticiankinesitherapist Multi-modal
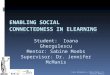
intervention Multi-disciplinary approach Slide 5 ERAS
EpiduralAnaesthesia Prevention of ileus/ prokinetics CHO-loading/
no fasting Early mobilisation Peri-op fluid management DVT
prophylaxis Pre-op councelling Remifentanyl No premed No bowel prep
Perioperative nutrition Bairhugger Oral analgesics/ NSAIDs
Incisions No NG tubes Early removal of catheters/drains Lassen et
al, Arch Surg, 2009 Slide 6 Slide 7 Outline Anesthetist approach
Surgeon approach Protocolization Slide 8 Outline Anesthetist
approach Surgeon approach Protocolization Slide 9 Enhanced Recovery
in practice Referral from Primary Care Pre- Operative Admission
Operative Post- Operative Follow-up Fluid management Postoperativ
glycaemic control Postoperative nutrition Early mobilisation Rapid
hydration / nourishment Appropriate iv therapy Catheters removed
early Regular oral analgesia Avoid opiates Antimicrobial
prophylaxis Multimodal analgesia PONV Optimal fluid therapy
Hypotermia prophylaxis Optimised medical conditions Nutrition
Fasting time Carbohidrate drinking Pre-anesthestic medication Anti-
thrombotic prophylaxis Slide 10 Preoperative ERAS components
Patient information Health/medical optimisation Nutrition Fasting
time Carbohidrate drinking Pre-anesthestic medication
Anti-thrombotic prophylaxis U.O. Gustafsson et al. Clin Nutr 2012;
31: 783-800 Slide 11 Preoperative ERAS components Patient
information Health/medical optimisation Nutrition Fasting time
Carbohidrate drinking Pre-anesthestic medication Anti-thrombotic
prophylaxis U.O. Gustafsson et al. Clin Nutr 2012; 31: 783-800
Slide 12 Patient information Preadmission education and counselling
Decrease fear and anxiety Improve wound healing perioperative
feeding postoperative mobilisation pain control Reduce the
prevalence of complications U.O. Gustafsson et al. Clin Nutr 2012;
31: 783-800 Enhance Postoperative Recovery and Discharge Slide 13
Preoperative ERAS components Patient information Health/medical
optimisation Nutrition Fasting time Carbohidrate drinking
Pre-anesthestic medication Anti-thrombotic prophylaxis U.O.
Gustafsson et al. Clin Nutr 2012; 31: 783-800 Slide 14 Prehab
Preoperative improvement of physiological function Increasing
exercise preoperatively WALK Training programs Slide 15 Prehab
Preoperative improvement of physiological function Increasing
exercise preoperatively WALK Increasing distance Increasing
duration Increasing frequency Easier to implement Psychological
preparation Motivation adherence to exercise Less efficient Slide
16 Prehab Preoperative improvement of physiological function
Increasing exercise preoperatively Training programs Slide 17
Prehab Hulzebos EH, JAMA. 2006;296(15):1851-1857 Slide 18 Prehab
Hulzebos EH et al. JAMA. 2006;296(15):1851-1857 RCT, n=279 high
risk pts single centre, 2002-2005 prehospitalization period before
CABG surgery may be used to improve a patients pulmonary condition
Slide 19 Prehab Hulzebos EH, JAMA. 2006;296(15):1851-1857
postoperative pulmonary complication time of postoperative
hospitalization Slide 20 Preoperative alcohol consumption Increase
(x 3) in postoperative morbidity Cardiopulmonary complications
Bleeding Wound infections Tnnesen et al. Br J Surg 1999;86:869-74
Slide 21 Preoperative alcohol consumption Abstinence from alcohol
for 1 month before surgery reduces postoperative morbidity after
colorectal surgery U.O. Gustafsson et al. Clin Nutr 2012; 31:
783-800 Does it any difference???!!??? Slide 22 Preoperative
alcohol consumption Tnnesen et al. BMJ 1999; 318:13116
Postoperative ECG and pulse oxymetry Mean HR Ischemia % Arrhythmias
SpO2 Hypoxemic episodes Slide 23 Preoperative alcohol consumption
Tnnesen et al. BMJ 1999; 318:13116 Responses to surgical stress
Mean BP Mean HR Serum cortisol Plasma glucose Plasma noradrenaline
Plasma adrenaline Plasma IL-6 Slide 24 Preoperative alcohol
consumption Alcohol consumption should be stopped 4 weeks before
surgery U.O. Gustafsson et al. Clin Nutr 2012; 31: 783-800 Slide 25
Preoperative smoking Increased postoperative morbidity
Cardiopulmonary complications Wound infections Lindstrm D. et al.
Ann Surg 2008, 248:739-45. Anaesthesia, 2009 Slide 26 Preoperative
smoking RCT n = 117 (Blinded outcome assessment) Hernia,
Cholecystectomy, Hip/knee replacement Smoking cessation 4 weeks
before surgery Postoperative complications 41% vs. 21% Smoking
abstinent after 1 yr 33% vs. 15% Lindstrm D. et al. Ann Surg 2008,
248:739-45. Anaesthesia, 2009 Slide 27 Preoperative smoking Meta
analysis, 11 RCTs, 1194 pts T. Thomsen et al. Br J Surg 2009; 96:
451461 Slide 28 Preoperative smoking Any complication T. Thomsen et
al. Interventions for preoperative smoking cessation Cochrane
Database of Systematic, 2010, 7. CD002294 Slide 29 Preoperative
smoking Wound complications T. Thomsen et al. Interventions for
preoperative smoking cessation Cochrane Database of Systematic,
2010, 7. CD002294 Slide 30 Preoperative smoking Smoking should be
stopped 4 weeks before surgery U.O. Gustafsson et al. Clin Nutr
2012; 31: 783-800 Slide 31 Preoperative ERAS components Patient
information Health/medical optimisation Nutrition Fasting time
Carbohidrate drinking Pre-anesthestic medication Anti-thrombotic
prophylaxis U.O. Gustafsson et al. Clin Nutr 2012; 31: 783-800
Slide 32 Bozzetti, Nutrition, 2002, 18:953 Slide 33 Norman,
Clinical Nutrition, 2008,27, 5/15 Slide 34 Questions regarding
perioperative nutrition: TNP vs EN ? Pre- vs post- vs pre- and
postoperative ? Standard vs immunonutrition ? Slide 35 All
malnourished patients All cancer patients Scheduled for upper
gastro-intestinal surgery No matter the nutritional status ESPEN
RECOMMENDATIONS Preoperative Preoperative enteral (immuno)nutrition
for 1014 days RECOMMENDATION GRADE A Slide 36 Only
moderately/severely malnourished patients scheduled for elective
surgery Imposibility of meeting nutritional needs > 7-14 days
ASPEN RECOMMENDATIONS Perioperative Early postoperative enteral
(delayed PN) nutrition Slide 37 Rationale for PREOPERATIVE
NUTRITIONAL SUPPORT PRO Malnourished pts at risk of postoperative
complications Reduced nutrient intake frequent in cancer pts and
correlates with nutrition status and complications Although
malnutrition usually develops over weeks/months a short course of
nutrition support can improve physiologic functions Preoperative
nutrition support better tolerance for postoperative nutrition
Preoperative glucose reduced postoperative insulin resistance Slide
38 Rationale for PREOPERATIVE NUTRITIONAL SUPPORT CON The
nutritional status of cancer patients correlates with disease stage
and cancer control If nutritional depletion is the result of
metabolic use of nutrients the benefit ?? Short-term refeeding
reversal of long-term malnutrition?? Preoperative nutrition
increases the length of preoperative stay and increases the costs
Slide 39 Who should receive preoperative nutrition support? The
patient should be moderately/severely malnutrished The procedure
should be one in which nutrition support has been shown to improve
outcome thoraco-abdominal surgery Surgery should be elective and
safe to delay for 7- 10days The enteral route is always prefered
(when possible) Combination with postoperative nutrition
Immune-enhancing formulas Slide 40 Preoperative nutrition
Malnourished patients should receive nutritional support oral
supplements enteral nutrition Immunonutrition 5 -7 days
preoperatively reduce the prevalence of infectious complications in
patients undergoing major open abdominal surgery K. Lassen et al.
Clin Nutr 2012, 31: 817- 830 Slide 41 Preoperative ERAS components
Patient information Health/medical optimisation Nutrition Fasting
time Carbohidrate drinking Pre-anesthestic medication
Anti-thrombotic prophylaxis U.O. Gustafsson et al. Clin Nutr 2012;
31: 783-800 Slide 42 Preoperative fasting While it is desirable
that there should be no solid matter in the stomach when chloroform
is administered, it will be found very salutary to give a cup of
tea about 2 h previously. Joseph Lister. On anaesthetics, Holmes'
system of surgery. Vol 3, 3rd ed. London: Longmans Green and
Company, 1883 Slide 43 Preoperative fasting Standard practice
fasting from midnight reduce the volume and acidity of stomach
contents decrease the risk of pulmonary aspiration But Ljungqvist
& Sreide, Br J Surg, 2003; 90: 400-406 Slide 44 Preoperative
fasting Standard practice fasting from midnight reduce the volume
and acidity of stomach contents decrease the risk of pulmonary
aspiration But Cochrane review of 22 RCTs fasting from midnight no
reduction in gastric content no rise in pH of gastric fluid clear
fluids until 2h before anesthesia Brady M, et al. Cochrane Database
Syst Rev 2003;(4). CD004423. Thirst, headaches, hunger Slide 45 Why
challange fasting by midnight? Normal physiology Is no guarantee of
an empty stomach The same gastric volume with/without clear fluids
Improved well being Slide 46 Preoperative fasting Standard practice
Fasting from midnight Reduce the volume and acidity of stomach
contents Decrease the risk of pulmonary aspiration Modern fasting
guidelines Clear fluids 2 h before anaesthesia Exclusions Emergency
surgery Slide 47 Eur J Anaesthesiology 2011;28:556-569 Slide 48
What are the effects of the preoperative fasting ? Slide 49
Preoperative fasting and perioperative fluids If fasted risk of
dehydration Dehydration and anesthesia -> hypotension
Hypotension -> more fluids infused Overload of fluids Preop
clear fluids -> less iv fluids -> improved outcomes
Gustafsson et al Arch Surg, 2011 Slide 50 Metabolic effects of
overnight fasting DayNight HormonesInsulin +Insulin Glucagon
Cortizol SubstratesStorageBreakdown UtilizationCHO > FatFat >
CHO Ljungqvist O.et al. Scand J Nutr 2004; 48 (2): 77-82 Slide 51
Surgical stress Insulin resistance Slide 52 Insulin sensitivity
falls with the magnitude of surgery Percentage (%) Thorell A et al,
Curr Opin Clin Nutr Metab Care 1999; 2: 69 More Insulin Resistance
Slide 53 Insulin resistance cause complications Elective cardiac
surgery, n= 273 Diabetics and non diabetics Complications increase
with insulin resistance: 50% reduction in insulin sensitivity: 5-6
fold increase risk of complications 10 fold risk for infections
Sato et al, JCEM 2010, 95; 4338-44 Slide 54 Can we change the
metabolism ? Slide 55 Preoperative ERAS components Patient
information Health/medical optimisation Nutrition Fasting time
Carbohidrate drinking Pre-anesthestic medication Anti-thrombotic
prophylaxis U.O. Gustafsson et al. Clin Nutr 2012; 31: 783-800
Slide 56 Carbohydrate treatment 20% glucose iv 12.5% carbohydrate
drink 400 ml 2h before anesthesia + 800 ml evening before Induce
insulin release Slide 57 What is the effect of the carbohydrate
drink ? Slide 58 Setting before surgery FastedCHO fed Hyperglycemia
- + Insulin sensitivity - + 50% Glucose production+ - - -
Peripheral glucose uptake - + + + Ljungqvist et al, Clin Nutr 2001,
Svanfeldt et al Clin Nutr 2005 Slide 59 Carbohydrate treatment 20%
glucose iv 12.5% carbohydrate drink 400 ml 2h before anesthesia +
800 ml evening before Safety ??? Slide 60 Carbohydrate treatment
Nygren et al, Ann Surg, 1995 Minutes after intake Isotope activity
in the stomach (%) 120906030 0 0 20 40 60 80 100 120 * * * * * CHO,
n=6 Water, n=6 Gastric emptying is complete in 90 min for CHO /
water Slide 61 Oral intake of CHO does not increase gastric volumes
Gastric volume (ml) Acidity (pH) Overnight fast (n=89) 6-411.6-4.0
Placebo (n=86) 12-351.6-2.5 CHO 12.5 % (n=80) 7-411.6-2.7 Hausel et
al, Anesth Analg 2001 Slide 62 Carbohydrate treatment 20% glucose
iv 12.5% carbohydrate drink 400 ml 2h before anesthesia + 800 ml
evening before Safe fast gastric emptying Slide 63 Preop CHO
reduces postoperative insulin resistance Per cent change from preop
**** *P < 0.05 Nygren et al: Curr Opin Clin Nutr Metab Care 2001
CHO Control More resistance Slide 64 Preop CHO activates muscle
insulin signalling pathways p=0.02 Wang et al, BJS 2010 Slide 65
Preop CHO maintains postoperative muscle anabolic pathways P
Preoperative carbohydrates, fluids and outcomes Main factors for
better outcomes: Preop carbohydrates & fluid balance Preop
carbohydrates -> Less fluid overload (450 ml) For every litre
extra*: 32% increased risk of complications (cardiovascular) *
Limit: Day of surgery: Colonic 3,000 ml, Rectal 3,500 ml Gustafsson
et al, Arch Surg 2011 Slide 96 Fluid requirements are different
Open laparatomy Increase fluid shifts Bowel handling SIRS
Laparoscopy CO reduction Head-down position Pneumoperitoneum Slide
97 Fluid shifts should be minimised Avoid bowel preparation
Maintain hydration till 2 hours before surgery Minimise bowel
handling Avoid blood loss Slide 98 Goal Directed Therapy The use of
cardiac output / surrogate to guide iv fluid alone or in
combination with inotropics during the perioperative period. Slide
99 Goal directed intra-operative fluid therapy Noblett et al. BJS
2009 Slide 100 Varadhan K, Proc Nutr Soc, 2010 2.75 liters/24h Meta
analysis based on amount of fluid given Slide 101 Rahbari NN, BJS
2009: 96: 331 Fluids recent meta analysis Slide 102 Types of fluids
cristaloids and coloids Slide 103 Varadhan K, Proc Nutr Soc, 2010
59% reduced risk for complications 3.4 days reduction in hospital
stay Slide 104 Perioperative fluid management The types of fluids
cristaloids and coloids Vasopressors are indicated in hypotensive
normovolemic patients Iv fluids should be discontinued as soon as
practicable Fluid therapy is vital for outcome Fluid requirements
are different Fluid shifts should be minimised Fluid administration
must be goal directed Slide 105 Intraoperative ERAS components
Antimicrobial prophylaxis Anesthesia protocol Multimodal analgesia
PONV Fluid management Hypotermia prophylaxis Slide 106 Hypothermia
prophylaxis Hypothermia central temperature < 36 C Risk factor
for wound infections, prolonged cicatrisation cardiac events
shivering increase O2 consumption bleeding coagulation disorders
trombocites dysfunction postoperative ileus increase pain prolonge
emergence time Slide 107 Hypothermia prophylaxis Hypothermia
central temperature < 36 C Methods warming devices (forced air
warming blankets) warmed iv fluids warm gases in laparoscopic
surgery Slide 108 Postoperative ERAS components Postoperative
analgesia Fluid management Postoperative glycaemic control
Postoperative nutrition Early mobilisation Slide 109 Postoperative
analgesia Optimale analgesic regimen Good pain relief Reduction of
cardiovascular, cognitive, endocrino metabolic complications in at
risk patients Decrease the risk of chronic pain Allow early
mobilisation Allow early return of gut function and feeding Slide
110 Postoperative analgesia Principles of Multimodal Analgesia
Avoidance of iv opioids Regional anesthesia techniques Thoracic
epidural analgesia (TEA) Spinal analgesia Local anesthetic
techniques Transversus abdominis plane (TAP) block The analgesic
regimen is specific to the type of surgery/incision Slide 111
Postoperative analgesia in open surgery Thoracic epidural
anesthesia (TEA) Middle thoracic (T7-T10) Superior analgesia in the
first 72 h Earlier return of gut function Slide 112 Postoperative
analgesia in open surgery Thoracic epidural anesthesia (TEA) Low
dose concentration of local anesthetic Short acting opiate
Maintained for 48 -72 h postoperative Slide 113 Efficacy of
Postoperative Epidural Analgesia: A Meta-analysis Block BM et al,
JAMA. 2003;290(18):2455-2463 Slide 114 Slide 115 Slide 116 Epidural
analgesia vs opiates GI function EDA results in less GI paralysis
(vs iv opiates) Jorgensen Cochr Database Syst Rev 2004 Slide 117
Postoperative analgesia in laparoscopic surgery Spinal analgesia
Low dose long acting opioid- morphine Slide 118 Modification of
ERAS in lap surgery ? RCT EDA vs Spinal vs PCA, n=91 Lap colorectal
surgery LOS EDA (3.7 d) longer than PCA and Spinal (2,8 and 2,7 d)
Spinal Faster return of bowel function (vs EDA and PCA) Earlier
tolerance of food (vs EDA) Levy, BJS, 2011 Slide 119 ERAS and Lap
colorectal resection One center (North Bristol, UK), n=606,
2004-2009 Primary anastomosis ERAS formally after 2008 Transversus
abdominis plane (TAP) or rectus sheath block No EDA or PCA KAD
withdrawn in theatre 46% discharged within 3 days (Median LOS 4
days) 2 same day, 70 within 24 hrs, 116 within 48 hrs, 91 within 72
hrs Readmission rates 4 %, Gash KJ, Colorectal Dis, 2012 Slide 120
Early removal of KAD during EDA ? During thoracic epidural
anesthesia Removal of KAD in the morning after surgery Or after
removal of EDA RCT, N=205 No increased need for recatheterization
Transient increase in post-void residual volume (UL Scanning)
Zaouter, Acta Anasth Scand, 2012 Slide 121 Postoperative ERAS
components Postoperative analgesia Fluid management Postoperative
glycaemic control Postoperative nutrition Early mobilisation Slide
122 Varadhan K, Proc Nutr Soc, 2010 59% reduced risk for
complications 3.4 days reduction in hospital stay Slide 123
Postoperative ERAS components Postoperative analgesia Fluid
management Postoperative glycaemic control Postoperative nutrition
Early mobilisation Slide 124 Postoperative glycaemic control Slide
125 Hyperglycemia in surgical stress Insulin resistance is the key
Traditional belief Hyperglycemia in the acutely stressed patient is
not dangerous Glucose levels treated > 200 mg/dl Slide 126
Elective major surgery opportunity to prevent /attenuate metabolic
responses to surgery rather than having to treat them with insulin.
Several stress-reducing interventions in ERAS attenuate insulin
resistance as single interventions: preoperative oral carbohydrate
treatment epidural blockade minimally invasive surgery If
interventions are combined in ERAS protocol, hyperglycaemia can be
avoided even during full enteral feeding starting immediately after
major colorectal surgery. Slide 127 Postoperative ERAS components
Postoperative analgesia Fluid management Postoperative glycaemic
control Postoperative nutrition Early mobilisation Slide 128
Postoperative nutrition Fluids immediately after recovery from
anesthesia Normal hospital food on day 1 traditional care
enhanced-recovery protocol Nygren Clin Nutr 2003 Slide 129
Postoperative early enteral nutrition Lewis et al BMJ
2001;323(7316):773-6 Slide 130 Postoperative ERAS components
Postoperative analgesia Fluid management Postoperative glycaemic
control Postoperative nutrition Early mobilisation Slide 131 Early
mobilisation EFFECTS Early return of bowel function Improved
digestive tolerance Enhanced anabolism Decreased risk of
venousthromboembolism Deacreased risk of pulmonary complications
Enhanced recovery !!! CONDITIONS Good analgesia No ventilatory
support No postoperative somnolence Psycological support Slide 132
Outline Anesthetist approach Surgeon approach Protocolization Slide
133 It is ironic that the American Society of Anesthesiologists,
whose members are critical observers of surgical procedures,
evolved the best index of operative risk. Arthur S. Keats,
Anesthesiology 1978 Slide 134 Perhaps the American Surgical
Association, whose members are critical observers of anesthetic
procedures, will provide us with a meaningful index of anesthetic
risk. Arthur S. Keats, Anesthesiology 1978 Slide 135 Surgeon: No
bowel prep Food after surgery No drains or KAD No iv fluids, no
lines Early discharge All evidence based! Anesthetist:
Carbohydrates No fasting No premedication Epidural Anesthesia
Balanced fluids Vasopressors No or short acting opioids Slide 136
SURGEONS!! TRADITION EVIDENCE BASED MEDICINE Slide 137 BOWEL
PREPARATION PRO Avoids massive contamination !?! Minor
inconvenience to the patient !?! Looks better inside !?! CON
Preoperative dehydration !!! Modification of enteral flora !!!
Delayed gut motility !!! Slide 138 Arch Surg.Arch Surg. 2004
Dec;139(12):1359-64; discussion 1365. Mechanical bowel preparation
for elective colorectal surgery: a meta-analysis. Bucher PBucher P,
Mermillod B, Gervaz P, Morel P.Mermillod BGervaz PMorel P
CONCLUSIONS: 7 trialuri 1300 pt There is no evidence to support the
use of MBP in patients undergoing elective colorectal surgery.
Available data tend to suggest that MBP could be harmful with
respect to the incidence of anastomotic leak and does not reduce
the incidence of septic complications. Slide 139 Rectal cancer TME
(total mesorectum excision) Standardised Enhanced Recovery
Programme for the EnROL Trial Day before surgery avoidance of oral
bowel preparation except in patients undergoing total mesorectal
excision (TME) and reconstruction. Kennedy et al. BMC Cancer 2012,
12:181 Slide 140 Reduce surgical injury Minimally invasive surgery
FAST TRACK Surgery Early postoperative recovery Decreased stress
response Decreased inflammatory response Decreased pain Early bowel
movement Slide 141 FAST TRACK Early rehabilitation Minimally
invasive surgery NOT MANDATORY for FAST TRACK surgery but shortens
hospitalization Slide 142 NO routine nasogastric tube 28
multicenter trials >4000 pts Decreased duration of postoperative
ileus Decreased risk of postoperative pulmonary complications
Increased patient QOL No increase in anastomotic leak Nelson, R. at
all Systematic review of prophylactic nasogastric decompression
after abdominal operations. Br. J. Surg., 2005, 92, 673680. Slide
143 No drains Rationale of drains: A surgical tradition Difficult
to be abandoned For how long? 24h / 48h / 7days ??? In majority of
cases serous drained fluid (physiological reabsorption) When in
doubt, drain Lawson Tait, english surgeon The drain= the surgeon
eye in the patients abdomen Slide 144 No drains RCTs: Unreliable
indication of anastomotic leak Underestimates the significance of
anastomotic leak Underestimates the postoperative bleeding Does not
influence the rate of anastomotic leak Increases the contamination
risk Prolongs the duration of postoperative ileus Prolongs the
hospital lenght of stay Petrowsky, H. at all: Evidence-based value
of prophylactic drainage in gastrointestinal surgery: A systematic
review and meta-analyses. Ann. Surg., 2004, 240, 10741085. Slide
145 Day of surgery postoperative period IV fluids, if clinically
indicated pressors for epidural hypotension regular pre-emptive
antiemetics (ondansetron as first line) Early mobilization (patient
sits up) Starts drinking protein drinks COLONIC SURGERY Slide 146
Day 1 Urinnary catheter removed in the morning 8 hrs of enforced
mobilisation Resumes normal diet Pre-emptive oral analgesia is
started Paracetamol and NSAIDs Avoid Opioids Day 2 Epidural
infusion is stopped in the morning Epidural Catheter is removed at
14.00 if pain controlled and timed with anticoagulant dose COLONIC
SURGERY Slide 147 Day 3/4 - discharge criteria: Return of GI
function Able to eat and drink without discomfort Passing flatus
Pain controlled with oral analgesia Adequate home support Discharge
date is an important target for patients and staff but flexibility
is vital COLONIC SURGERY Slide 148 THE SURGEON the cornerstone of
FAST TRACK and ERAS programs Slide 149 Outline Anesthetist approach
Surgeon approach Protocolization Slide 150 Preventing hypotermia
Postoperative nutrition Preoperative Fasting Carbohydrates
Treatment Properative prophylaxys Early mobilisation PONV Analgesia
Preoperative optimisation Analgesia Fluid management Preoperative
nutrition Fluid management Slide 151 Results? Randomised trials
Meta analysis 1. ERAS Slide 152 Slide 153 ERAS compliance &
outcomes 953 consecutive colorectal surgery patients Multi variate
analysis ERAS factors Carbohydrate treatment 44% reduced risk of
symptoms delaying discharge (PONV, pain, GI sympoms, dizziness )
16% reduced risk of wound dehiscence Fluid balance: For each extra
Liter 16% increased risk of symptoms delaying discharge 32%
increased risk of complications Gustafsson et al Arch Surg, in
press 2011 Slide 154 ERAS - clinical outcome Complications K K.
Varadhan et al. Clin Nutr, 2010: 29 ;434440 Review of 6 RCTs
(n=452) Reduce complications by 50% Slide 155 ERAS - clinical
outcome Mortality K K. Varadhan et al. Clin Nutr, 2010: 29 ;434440
Review of 6 RCTs (n=452) Slide 156 ERAS - clinical outcome Length
of stay K K. Varadhan et al. Clin Nutr, 2010 : 29 ;434440 Review of
6 RCTs (n=452) Shorter length of stay by 2.5 days Slide 157
Readmissions (days) Experimental group= Enhanced Recovery After
Surgery (ERAS) Control = Traditional Care (TC) Slide 158 JAMA
Surgery 2011 Slide 159 Slide 160 Ciaran OHare Fast-track
rehabilitation after colonic surgery in elderly patientsis it
feasible? International Journal of Colorectal Disease Volume 22,
Number 12 / December, 2007 M. Scharfenberg1, W. Raue1, T. Junghans1
and W. Schwenk1 Conclusion Using the fast-track rehabilitation
programme on elderly patient is not only feasible but may also
lower the number of general complications and the duration of the
hospital stay. Slide 161 Slide 162 Slide 163 Slide 164 Slide 165
Slide 166 Slide 167 World J Surg.World J Surg. 2011 Sep 1.
Fast-Track Concepts in Major Open Upper Abdominal and
Thoracoabdominal Surgery: A Review. Fagevik Olsn MFagevik Olsn M,
Wennberg E.Wennberg E 15 articles: gastric (n = 2), pancreatic (n =
5), hepatic (n = 2), esophageal (n = 3), aortic surgery (n = 3).
Slide 168 Slide 169 Slide 170 Sipos P, HMJ, 2007 Vol.1, Number
2,165174 Slide 171 Anesth Analg 2007;104:1380-1396 2007
International Anesthesia Research Society doi:
10.1213/01.ane.0000263034.96885.e1 International Anesthesia
Research Society AMBULATORY ANESTHESIA The Role of the
Anesthesiologist in Fast-Track Surgery: From Multimodal Analgesia
to Perioperative Medical Care Paul F. White, PhD, MD *, Henrik
Kehlet, MD, PhD, and the Fast-Track Surgery Study Group CONCLUSION:
The decisions of the anesthesiologist as a key perioperative
physician are of critical importance to the surgical care team in
developing a successful fast-track surgery program. Slide 172 Slide
173 Slide 174 ORIGINAL ARTICLE Current perioperative practice in
rectal surgery in Austria and Germany Till HasenbergTill Hasenberg,
Friedrich Lngle, Bianca Reibenwein, Karin Schindler, Friedrich
LngleBianca ReibenweinKarin Schindler Stefan PostStefan Post,
Claudia Spies,Wolfgang Schwenk and Edward ShangClaudia
SpiesWolfgang SchwenkEdward Shang INTERNATIONAL JOURNAL OF
COLORECTAL DISEASEINTERNATIONAL JOURNAL OF COLORECTAL DISEASE 2010
Volume 25, Number 7Volume 25, Number 7, 855-863, DOI:
10.1007/s00384-010-0900-2 Results The response rate - 63% A (76
centers) + 30% G (385 centers). Mechanical bowel preparation -
abandoned by 2% G and 7% A surgeons. Nasogastric decompression
tubes - rarely used; 4/5 of the questioned surgeons - use
intra-abdominal drains. Half of the surgical centers - intake of
clear fluids on the day of surgery. Mobilization - in half of the
centers on the day of surgery. Epidural analgesia - three-fourths
of the institutions. Institutions which have implemented fast track
rehabilitation discharge earlier. Slide 175 Surgery and
peri-operative care remains heavily based in tradition Practice
varies substantially internationally survey of UK general surgeons:
there is inadequate multidisciplinary and community support to
initiate ERAS never heard of it. survey regarding practice across
European countries: nil by mouth almost abandoned in others This is
the biggest challenge facing the wide implementation and acceptance
of ERAS programs. Hill, Andrew (2008, December 10). Enhanced
Recovery after Surgery. SciTopics.
http://www.scitopics.com/Enhanced_Recovery_after_Surgery.html Slide
176 Slide 177 Current evidence supports the potential role of
multi-modal care programmes in the promotion of early recovery from
major surgical trauma. To achieve the desired outcome targets, all
elements of the protocol must function, a committed,
multidisciplinary approach is essential and a simple, but effective
implementation and reinforcement strategies are necessary.
Implementation in Practice (C.H.C. Dejong, Netherlands)
http://www.jspen.jp/doc6/sec7.html Slide 178 Implementation of the
ERAS protocol select a target invite participation to create a team
explain what you are trying to achieve select an expert group
create change concept and priorities implement strategy regular
review to measure and evaluate change review strategy
Implementation in Practice (C.H.C. Dejong, Netherlands)
http://www.jspen.jp/doc6/sec7.html Slide 179 There is nothing new
under the sun but there are lots of old things we dont know.
Ambrose Bierce.