Embed Size (px)
Citation preview

CLINICAL ARTICLE
In recent years, enhanced recovery after surgery (ERAS) protocols have emerged as multimodal ap-proaches designed to improve clinical outcomes in
surgical patients. ERAS engages all healthcare providers in a longitudinal fashion, with an underlying theme of reduction of the dramatic stress response due to surgery.
Coordination among multiple teams (outpatient staff, an-esthesia team, surgical team, in-house ward staff, etc.) and dedicated interventional education as well as engagement of patients is critical to ensure a unified approach to the patient’s surgical journey in order to deliver a higher qual-ity of care.14
ABBREVIATIONS BMI = body mass index; EQ-5D = EuroQol–5 Dimensions Scale; ERAS = enhanced recovery after surgery; LOS = hospital length of stay; NDI = Neck Disability Index; ODI = Oswestry Disability Index; PCA = patient-controlled analgesia; POD = postoperative day; PRO = patient-reported outcome. SUBMITTED May 30, 2018. ACCEPTED September 10, 2018.INCLUDE WHEN CITING Published online January 25, 2019; DOI: 10.3171/2018.9.SPINE18681.
Enhanced recovery after elective spinal and peripheral nerve surgery: pilot study from a single institutionZarina S. Ali, MD,1 Tracy M. Flanders, MD,1 Ali K. Ozturk, MD,1 Neil R. Malhotra, MD,1 Lena Leszinsky,1 Brendan J. McShane, BA,1 Diana Gardiner, CRNP,1 Kristin Rupich, CRNP,1 H. Isaac Chen, MD,1 James Schuster, MD, PhD,1 Paul J. Marcotte, MD,1 Michael J. Kallan, MS,2 M. Sean Grady, MD,1 Lee A. Fleisher, MD,3 and William C. Welch, MD1
1Department of Neurosurgery, 2Center for Clinical Epidemiology and Biostatistics, and 3Department of Anesthesia, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania
OBJECTIVE Enhanced recovery after surgery (ERAS) protocols address pre-, peri-, and postoperative factors of a patient’s surgical journey. The authors sought to assess the effects of a novel ERAS protocol on clinical outcomes for patients undergoing elective spine or peripheral nerve surgery.METHODS The authors conducted a prospective cohort analysis comparing clinical outcomes of patients undergoing elective spine or peripheral nerve surgery after implementation of the ERAS protocol compared to a historical control co-hort in a tertiary care academic medical center. Patients in the historical cohort (September–December 2016) underwent traditional surgical care. Patients in the intervention group (April–June 2017) were enrolled in a unique ERAS protocol created by the Department of Neurosurgery at the University of Pennsylvania. Primary objectives were as follows: opioid and nonopioid pain medication consumption, need for opioid use at 1 month postoperatively, and patient-reported pain scores. Secondary objectives were as follows: mobilization and ambulation status, Foley catheter use, need for straight catheterization, length of stay, need for ICU admission, discharge status, and readmission within 30 days.RESULTS A total of 201 patients underwent surgical care via an ERAS protocol and were compared to a total of 74 patients undergoing traditional perioperative care (control group). The 2 groups were similar in baseline demograph-ics. Intravenous opioid medications postoperatively via patient-controlled analgesia was nearly eliminated in the ERAS group (0.5% vs 54.1%, p < 0.001). This change was not associated with an increase in the average or daily pain scores in the ERAS group. At 1 month following surgery, a smaller proportion of patients in the ERAS group were using opioids (38.8% vs 52.7%, p = 0.041). The ERAS group demonstrated greater mobilization on postoperative day 0 (53.4% vs 17.1%, p < 0.001) and postoperative day 1 (84.1% vs 45.7%, p < 0.001) compared to the control group. Postoperative Foley use was decreased in the ERAS group (20.4% vs 47.3%, p < 0.001) without an increase in the rate of straight cath-eterization (8.1% vs 11.9%, p = 0.51).CONCLUSIONS Implementation of this novel ERAS pathway safely reduces patients’ postoperative opioid require-ments during hospitalization and 1 month postoperatively. ERAS results in improved postoperative mobilization and ambulation.https://thejns.org/doi/abs/10.3171/2018.9.SPINE18681KEYWORDS enhanced recovery after surgery; ERAS; opioid epidemic; clinical outcomes; spine surgery; multimodal
J Neurosurg Spine January 25, 2019 1©AANS 2019, except where prohibited by US copyright law

Ali et al.
J Neurosurg Spine January 25, 20192
Since the inception of ERAS,16 multiple surgical fields such as colorectal,5 urology,21 and orthopedic joint sur-gery6 have applied their respective protocols with varying levels of success. Because the national opioid epidemic is a growing concern in the medical community, and in par-ticular in surgical populations, we hypothesized that the patient-centered approach inherent to ERAS has the po-tential to decrease overall opioid use both in the short and long term.7,18,24 Indeed, the United States makes up less than 5% of the world’s population but is responsible for 80% of the world’s prescription opioids.19 Directly addressing opi-oid use with patients as well as the active introduction of a multimodal, opioid-sparing ERAS pain regimen aims to combat this growing public health concern.
In today’s aging population of patients with spinal dis-orders and multiple comorbid conditions, a comprehensive care pathway like ERAS serves to reduce overall surgical morbidity.9 A neurosurgical ERAS pathway aims to opti-mize the pre-, peri-, and postoperative care of patients in order to result in a more efficient recovery.8 Despite the success of ERAS in other fields of surgery, development and application of such a pathway has been limited in neu-rosurgery. There have been some early investigations of its application to lumbar fusion surgery via a minimally invasive surgical procedure,30,31 but no reports have been published on a comprehensive ERAS pathway in elective spine and peripheral nerve surgery. We present our institu-tion’s initial experience with implementation of ERAS in elective spine and peripheral nerve surgery and assess its impact on perioperative and postoperative opioid use.
MethodsStudy Design
This is a prospective cohort analysis to evaluate the impact of a novel ERAS protocol for patients undergo-ing elective spine or peripheral nerve surgery by the same attending neurosurgeons (Z.A., A.O., W.W.) who operate at a single hospital (Pennsylvania Hospital) within the University of Pennsylvania Health System. The 2 cohorts underwent treatment at a single institution before ERAS implementation (September–December 2016) and after ERAS implementation (April–June 2017). Clinical out-comes before and after ERAS implementation were as-sessed. This study was approved as quality improvement by the institutional review board at the University of Penn-sylvania.
Patient Inclusion and Exclusion CriteriaInclusion criteria consisted of the following: clinical
history and diagnostic imaging supporting the need for elective spine or peripheral nerve surgery, age older than 18 years, and the ability to understand and actively partici-pate in the program as deemed by the attending neurosur-geon. Exclusion criteria included the following: contrain-dications to elective spine or peripheral nerve surgery as deemed by the attending neurosurgeon, diagnosis of liver disease, and pregnancy.
Control GroupThe control group was a historical cohort of 74 patients
who underwent elective spine and peripheral nerve sur-gery at Pennsylvania Hospital between September and December 2016. These patients included all individu-als who had at least 1-month follow-up data in historical medical records and who underwent traditional surgical care at the discretion of the attending neurosurgeon in a nonstandardized fashion. This care included routine Foley catheter placement peri- or postoperatively, and routine postoperative pain management with patient-controlled analgesia (PCA) postoperatively (i.e., postoperative day [POD] 0–1), among other routine parameters. Patients fasted the night before surgery, beginning at midnight.
ERAS GroupThe ERAS group comprised 201 consecutive eligible
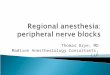
patients who underwent surgery between April and June 2017 at the same institution. Once an attending neurosur-geon determined that a patient was a candidate for elective spine or peripheral nerve surgery, the patient was prospec-tively asked for consent and enrolled into a unique ERAS protocol, which is outlined here (Fig. 1) and has previously been published in full.1
Patients underwent extensive preoperative education with the surgeon and advanced care provider in the neuro-surgery clinic about the ERAS standardized approach to their pre-, peri-, and postoperative care. In the preopera-tive setting, patients received surgical site care education. Patients who met the criteria were requested to obtain ad-ditional consultations in the preoperative time period with the following specialists: pain management for patients on significant preoperative opioid medications (requiring a > 30 morphine equivalent dose [MED] for > 4 weeks); sleep medicine if the patient had a score of > 2 on the STOP-BANG sleep apnea screening questionnaire; primary care for smoking cessation initiation if applicable; endocrine for diabetic patients with serum glucose > 200 g/dl or HbA1c > 8%. All patients were provided with written educational materials detailing their ERAS surgical journey, as well as being given written educational materials provided by a nutritionist about preoperative protein intake optimization and smoking cessation education if applicable. Patients in the ERAS group completed the Risk Assessment and Pre-diction Tool (RAPT) preoperatively as a means of educat-ing patients and their families about their discharge dis-position. Preoperative nutrition screening for patients with body mass index (BMI) < 18.5 or > 25 kg/m2 with serum albumin levels was performed; patients were referred for nutrition consultation if albumin was < 3.5 g/dl. Patients were also asked to consent to receive mobile text message reminders prior to and following their surgery; this ap-plication was facilitated through a pilot program called “Engaged Recovery at Penn” through the Penn Innovation Center. No additional resources were required other than establishing open lines of communication with consulting services to facilitate appointments.
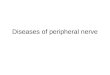
In the perioperative setting, patients were instructed to take a carbohydrate load (20 oz Gatorade or Powerade) the day prior to and on the day of surgery, 2 hours before their scheduled arrival to the hospital. Perioperative pain con-trol was performed via an opioid-sparing multimodality regimen (Fig. 2), which was adapted from the ERAS path-

J Neurosurg Spine January 25, 2019 3
Ali et al.
way created by McEvoy et al.20 The Penn Neurosurgery ERAS Pain Management Protocol includes preoperative administration of gabapentin, elimination of the routine use of postoperative intravenous opioids via PCA pumps, and use of acetaminophen. Additionally, local infiltration of bupivacaine at the time of closure was also adminis-tered. Other intraoperative analgesia was provided as per the anesthesiologist. Patients were also provided with 1 packet of chewing gum and asked to comply with chewing 1 piece of gum 3 times daily postoperatively to reduce the risk of postoperative ileus.23,26
Surgery was performed using a Safe Spinal Surgery Checklist, which was designed to engage all operating room staff just prior to closure of the wound to ensure completion of all elements of the desired procedure, in-cluding use of drains, local anesthetic, and other compo-nents of surgery as deemed necessary by the attending neurosurgeon. Postoperative nursing instructions in the ERAS pathway included the instruction to assist the pa-tients in getting out of bed within 6 hours of surgery. Ad-ditionally, nurses were instructed to ambulate patients 3–5 times daily beginning on POD 1 unless bed rest restric-tions were applied as deemed by the attending surgeon. Mobilization was defined as any active movement from the bed. Nursing was also encouraged to assist all patients in having meals out of the bed and in a chair. Foley cath-eter use was limited to those patients with intraoperative durotomies or greater than 3 levels of thoracolumbosacral fusion procedures. A standard wound care regimen was established in which all patients received a chlorhexidine
bath daily beginning on POD 1 while in the hospital. After the in-patient hospitalization, in addition to routine follow-up with the surgeon, patients are instructed to follow up routinely with their primary care provider within 2 weeks to maintain continuity of medical care. Patients were also provided with a Web link via text message with resources on nutrition, exercise, and mindfulness after surgery. A postacute care resource triage pathway was developed to provide guidance to nursing home and rehabilitation cen-ters for managing acute neurosurgical patient issues.
Study ParametersPrimary outcomes included the following: opioid and
nonopioid consumption on POD 1, need for opioid use at 1 month postoperatively, and patient-reported pain scores. Secondary outcomes included mobilization and ambula-tion status on POD 0–1, Foley catheter use (intraoperative and postoperative), need for straight catheterization, hos-pital length of stay (LOS; days), need for ICU admission, discharge status, and readmission within 30 days. Com-plications were defined as infection, reoperation, deep venous thrombosis or pulmonary embolism, durotomy, cardiac arrest, death, or any adverse event that could be at-tributed to the surgery and verified via the electronic med-ical record. Patient-reported outcomes (PROs) were mea-sured using the EuroQol–5 Dimensions Scale (EQ-5D), Oswestry Disability Index (ODI) for patients undergoing lumbar surgery, and the Neck Disability Index (NDI) for patients undergoing cervical surgery. Patients were asked to complete each appropriate questionnaire at their preop-
FIG. 1. Illustration showing the pre-, peri-, and postoperative components of the Penn Neurosurgery ERAS protocol. Figure is available in color online only.

Ali et al.
J Neurosurg Spine January 25, 20194
erative and 1-month postoperative visit. The mean change in score was calculated for patients with complete pre- and postoperative scores.
Statistical AnalysisComparisons among various patient characteristics and
measurements for the 2 patient groups (control vs ERAS) were performed with independent 2-sample t-tests for continuous variables and Fisher’s exact test for categori-cal variables. All data for the study were collected and analyzed by independent observers in collaboration with a biostatistician (M.J.K.). SAS software version 9.4 (SAS Institute) was used for all analyses.
ResultsTable 1 summarizes the patient demographics for each
group. The control group consisted of 74 patients, and the ERAS group was composed of 201 patients. The 2 groups were similar in age, BMI, sex, history of prior spine sur-gery, preoperative narcotic use, and smoking status. The groups were also similar in preoperative overall health index measured using the EQ-5D and the preoperative disability index measured by the ODI and NDI. Medical comorbidities (such as obstructive sleep apnea, diabetes, chronic obstructive pulmonary disease) in each group were not significantly different. The distribution of surgi-cal procedures between groups was also similar, with the majority of surgeries consisting of laminectomies, discec-tomies, and foraminotomies (Table 1). Less than 10% of surgeries in both groups consisted of other surgeries; in the control group there were 4 peripheral nerve surger-
ies, 2 hardware revision/removal surgeries, and 1 repair of durotomy. In the ERAS group there were 4 deep muscle biopsies, 4 peripheral nerve cases, 3 hardware removals, 2 tumor resections, 1 spinal cord detethering, and 1 arach-noid cyst fenestration. The majority of surgeries were per-formed under general anesthesia. Less than 10% of cases in both groups consisted of outpatient surgery.
Table 2 outlines opioid and nonopioid consumption in the control group as compared to the ERAS group. A greater proportion of ERAS patients received a combina-tion of at least 3 (72.6% vs 41.9%, p < 0.001) or 4 (44.8% vs 18.9%, p < 0.001) nonopioid agents compared to control patients. PCA use was almost completely eliminated in the ERAS group (0.5%), whereas more than half (54.1%) of patients used PCAs in the control group (p < 0.001). Similarly, the proportion of ERAS patients using opioids at 1 month postoperatively was significantly reduced as compared to the non-ERAS group, half of whom were still using narcotics (38.8% vs 52.7%, p = 0.041). Ketoro-lac (23.9% vs 10.8%, p = 0.018) and gabapentin (80.6% vs 21.6%, p < 0.001) were more frequently administered to the ERAS patients compared to the control group. Aceta-minophen and cyclobenzaprine were used in both popula-tions, with a tendency to be used more frequently in the ERAS group. A similar number of patients in both groups used dexamethasone and diazepam as adjuncts to pain control. Maximum pain scores on POD 0–3 in patients remaining in the hospital were not significantly different between ERAS and control groups (Table 2).
Mobilization and ambulation data were limited in both groups due to lack of nursing data entry. However, based on the available data, the ERAS group demonstrated greater
FIG. 2. Illustration highlighting the various components of the pain management protocol within ERAS. IV = intravenous; PACU = postanesthesia care unit. Figure is available in color online only.

J Neurosurg Spine January 25, 2019 5
Ali et al.
mobilization on POD 0 (53.4% vs 17.1%, p < 0.001) and on POD 1 (84.1% vs 45.7%, p < 0.001) as compared to the control group. Ambulation was also found to be greater in the ERAS group on POD 0 (46.9% vs 17.1%, p = 0.001) and POD 1 (64.2% vs 28.6%, p < 0.001) compared to the control group. Postoperative Foley use was significantly decreased in the ERAS group (20.4% vs 47.3%, p < 0.001) without a significant increase in straight catheterization (11.9% vs 8.1%, p = 0.51).
With regard to resource utilization (Table 3), imple-mentation of ERAS did not significantly increase overall LOS (3.6 vs 4.0 days, p = 0.37) or ICU admission (11.9% vs 14.9%, p = 0.54). The readmission rate at 30 days was also not found to be significantly different between the ERAS patients and the control group (3.0% vs 5.4%, p = 0.47). There was no significant difference in change in PROs (Table 4) at 1 month postoperatively measured with the EQ-5D (-0.5 vs -0.8, p = 0.38), ODI (-4.3 vs -11.8, p = 0.12), or NDI (11.1 vs 11.1, p = 1.00).
DiscussionWainwright et al. first proposed the application of
ERAS in major spine surgery.29 Since then, ERAS has made initial forays into the population undergoing elective minimally invasive spine surgery.30,31 We report the clini-cal outcomes of the first prospective cohort study in which a novel ERAS protocol was used in a heterogeneous popu-lation that underwent elective spine and peripheral nerve surgery.
The current opioid epidemic is a public health emer-gency in the United States.18 Three-quarters of our insti-tution’s spinal and peripheral nerve surgical population represent opioid-naïve patients. There is an increasing amount of data supporting the finding that between 3% and 7% of opioid-naïve patients undergoing surgery con-tinued to take opioids 1 year after surgery.27 Decreasing opioid use after spine surgery is a daunting task, but our multidimensional ERAS protocol addresses this issue, in part, by using a multimodal, opioid-sparing approach to spine surgery pain management. PCA use with intra-venous opioids was nearly completely eliminated in the ERAS group (0.5% vs 54.1%, p < 0.001). This was accom-plished without an increase in pain scores in the ERAS population, suggesting that routine PCA use is not nec-essary in this population. We believe that the addition of multiple nonopioid agents, such as acetaminophen and preoperative gabapentin, among other agents, helps to mitigate the need for routine PCA use and overall opioid use in patients following spine surgery. Most notably, our results show that the adoption of an opioid-sparing multi-modal pain regimen following spine surgery via an ERAS pathway resulted in reduced opioid use at 1 month post-operatively. This has profound implications in helping to limit the chronic opioid dependency in patients following spine surgery, but further studies will need to assess the durability of this change.
The cognitive-behavioral phenomenon of fear avoid-ance further perpetuates pain in the patient undergoing spine surgery.13,17 Postoperative fear of movement has strong associations with pain, disability, and physical
TABLE 1. Baseline demographic data in patients with elective spine and peripheral nerve surgery
CharacteristicControl, n = 74
ERAS, n = 201
p Value
Age, yrs μ = 62.9 (σ = 11.3) μ = 60.5 (σ = 14.5) 0.14‡BMI μ = 30.2 (σ = 5.6) μ = 29.7 (σ = 5.4) 0.56†Males 42 (56.8%) 106 (52.7%) 0.59*Prior spinal surgery 28 (37.8%) 68 (33.8%) 0.57*Preop narcotic use 19 (25.7%) 47 (23.4%) 0.75*Obstructive sleep
apnea13 (17.6%) 31 (15.4%) 0.71*
Smoking status 0.41* Current 11 (14.9%) 20 (10.0%) Former 30 (40.5%) 78 (38.8%) Never 33 (44.6%) 103 (51.2%)Diabetes 16 (21.6%) 32 (15.9%) 0.29*Chronic obstructive
pulmonary disease4 (5.4%) 9 (4.5%) 0.75*
Procedures 1: laminectomy/
discectomy/foraminotomy
31 (41.9%) 95 (47.3%) 0.46*
2: thoracolumbo-sacral fusion
<4 levels 12 (16.2%) 47 (23.4%) ≥4 levels 3 (4.1%) 4 (2.0%) 3: cervicothoracic
laminectomy w/ or w/o fusion
<4 levels 5 (6.8%) 17 (8.5%) ≥4 levels 11 (14.9%) 10 (5.0%) 4: anterior cervical
discectomy & fusion
Total 5 (6.8%) 13 (6.5%) 1 level 2 (2.7%) 9 (4.5%) 2 levels 3 (4.1%) 4 (2.0%) 3 levels 0 (0.0%) 0 (0.0%) 5: other 7 (9.5%) 15 (7.5%)Patient status Inpatient 67 (90.5%) 182 (90.5%) 0.61* Outpatient 7 (9.5%) 15 (7.5%) Observational 0 (0.0%) 4 (2.0%)Anesthetic type General 64 (86.5%) 180 (89.6%) 0.40* Spinal 10 (13.5%) 18 (9.0%) MAC 0 (0.0%) 3 (1.5%)
MAC = monitored anesthesia care; μ = average; σ = standard deviation. Unless otherwise stated, there were 74 patients in the control group and 201 in the ERAS group.* Compares association between the 2 groups using Fisher’s exact test.† Compares mean differences, pooled method (assuming equal variances across the groups).‡ Compares mean differences, Satterthwaite method (assuming unequal vari-ances across the groups).

Ali et al.
J Neurosurg Spine January 25, 20196
health in patients who undergo spine surgery.2 To com-bat this, strict parameters for early ambulation were pre-scribed in the ERAS protocol, and indeed, the ERAS group exhibited greater mobilization and ambulation on POD 0–1 than the control group. We believe that address-ing the fear of movement immediately in the postoperative period by encouraging timely postoperative mobility and ambulation reduces immobility and enhances recovery. Early and aggressive mobility in the ERAS cohort did not result in increased pain, and no changes in LOS were ob-served in our pilot program. This may be due to a modest sample size.
Foley catheters are associated with acute25 and chron-ic12 urinary tract infections, urethral trauma,15 kidney and bladder damage,11 bladder stones,10 and pseudopolyps.22 Conscious limitation of the use of Foley catheters in the patient undergoing spine surgery has the potential to avoid or minimize numerous adverse effects as well as allow for ease in patient mobility and ambulation. The ERAS group demonstrated significantly less postoperative Foley use compared to the pre-ERAS group. This factor was not found to result in an increase in straight catheterization. Because postoperative urinary retention (POUR) can in-crease the LOS and impact surgical morbidity,3 avoiding the use of Foley catheters is a major goal during the inpa-tient period for patients who do not require bed restric-tions. Our findings suggest that such avoidance may be associated with improved inpatient mobility and ambula-tion.
ERAS implementation did not result in increased over-all LOS or ICU admission. Patients in the ERAS group
demonstrated a trend toward reduced LOS, which perhaps may be more apparent with a larger cohort analysis. The readmission and complications rates at 30 days were not found to be significantly different, although these conclu-sions may also be limited due to the small sample size.
The major goals of the ERAS pathway are to optimize the surgical experience for patients and improve their clinical outcomes. The patient population undergoing spine and peripheral nerve surgery is indeed heteroge-neous. This care paradigm relies on the multidisciplinary and collaborative care of all individuals involved in the patient’s surgical journey to engage in the patient’s care in a relatively standardized fashion. We believe that the incremental benefits of the various elements of the ERAS pathway translate into improved overall care in the form of a reduction in opioid use.
Future directions aim to include cost-effectiveness of the ERAS protocol as well as PRO measures with well-validated questionnaires such as the Patient-Reported Out-comes Measurement Information System (PROMIS), ODI, NDI, and EQ-5D. PROs have become the gold standard to measure clinical efficacy after a surgical intervention,4,28 and such questionnaires in the pre- and postoperative time points provide both the patient and the neurosurgeon with insight into the patient’s overall clinical function and im-provement. We also hope to study the effects of the ERAS protocol on overall health, such as long-term improve-ments in BMI and A1C.
Limitations of the StudyThere are several limitations to this study. This is a
TABLE 2. Opioid and nonopioid pain medication use in patients with elective spine and peripheral nerve surgery
Variable* Control, n = 74 ERAS, n = 201 p Value
Opioid medications PCA use 40 (54.1%) 1 (0.5%) <0.001† No. of patients using any opioid on POD 1 [66/183] 63 (95.5%) 164 (89.6%) 0.21†Maximum overall pain score μ = 8.1 (σ = 1.9) μ = 8.0 (σ = 2.2) 0.76‡ POD 0 [73/199] n = 73/74; μ = 6.4 (σ = 2.7) n = 199/201; μ = 6.6 (σ = 2.9) 0.56‡ POD 1 [65/181] n = 65/66; μ = 7.6 (σ = 2.4) n = 181/183; μ = 7.5 (σ = 2.3) 0.69‡ POD 2 [52/139] n = 52/54; μ = 7.6 (σ = 1.9) n = 139/139; μ = 7.1 (σ = 2.4) 0.14‡ POD 3 [34/78] n = 34/35; μ = 6.5 (σ = 2.6) n = 78/81; μ = 6.9 (σ = 2.4) 0.43‡Narcotic use postop (1 mo) 39 (52.7%) 78 (38.8%) 0.041†Nonopioid medications Acetaminophen 62 (83.8%) 182 (90.5%) 0.13† Dexamethasone 12 (16.2%) 27 (13.4%) 0.56† Ketorolac 8 (10.8%) 48 (23.9%) 0.018† Valium 45 (60.8%) 119 (59.2%) 0.89† Cyclobenzaprine 33 (44.6%) 105 (52.2%) 0.28† Gabapentin 16 (21.6%) 162 (80.6%) <0.001† ≥3 multimodal nonopioid agents 31 (41.9%) 146 (72.6%) <0.001† ≥4 multimodal nonopioid agents 14 (18.9%) 90 (44.8%) <0.001†
Boldface type indicates statistical significance.* Numbers in brackets represent patients from the control group/ERAS group.† Compares association between the 2 groups using Fisher’s exact test.‡ Compares mean differences, pooled method (assuming equal variances across the groups).

J Neurosurg Spine January 25, 2019 7
Ali et al.
prospective cohort analysis limited by a moderate sample size. The control group is a historical one, and the data were reviewed retrospectively. Randomization and blind-ing were not performed. Data collection is limited to the information provided in medical records. Minor protocol deviations from this multimodal pathway were not well documented and are difficult to assess. Baseline activity level and cognitive function can lead to bias within the ERAS or control groups. Differences in these factors were not fully explored but could introduce selection bias. We hope that a future randomized controlled design can help eliminate any forms of selection bias. Although we monitored medical comorbidities and assessed for overall trends, we have not yet studied the compliance of patients in performing all recommended preoperative consulta-tions. However, we believe that the value of a formalized ERAS pathway allows for better surgical education for pa-tients preoperatively. Because expectations drive patients’ outcomes, we believe that ERAS aids in aligning expecta-tions and personalizing surgical education.
Despite these limitations, this study demonstrates the safety and efficacy of our Penn Neurosurgery ERAS protocol. We continue to refine the pathway and monitor outcomes. An ERAS pathway similar to this one can be safely incorporated in other centers performing spine and peripheral nerve surgery and, based on these data, has the potential to result in improved outcomes.
ConclusionsERAS engages each aspect of the patient’s surgical
journey in order to improve outcomes in a multidisci-plinary, multimodal approach. In the patient undergoing elective spine and peripheral nerve surgery, ERAS is fea-
TABLE 3. Mobilization and/or ambulation, urinary retention, and disposition in patients with elective spine and peripheral nerve surgery
Variable* Control, n = 74 ERAS, n = 201 p Value
Mobilization POD 0 [35/178] n = 35/74; 6 (17.1%) n = 178/201; 95 (53.4%) <0.001† POD 1 [35/164] n = 35/66; 16 (45.7%) n = 164/183; 138 (84.1%) <0.001†Ambulation POD 0 [35/177] n = 35/74; 6 (17.1%) n = 177/201; 83 (46.9%) 0.001† POD 1 [35/162] n = 35/66; 10 (28.6%) n = 162/183; 104 (64.2%) <0.001†Urinary retention No Foley 30 (40.5%) 88 (43.8%) <0.001† Intraop Foley only 9 (12.2%) 72 (35.8%) Postop Foley 35 (47.3%) 41 (20.4%) Straight catheterization 6 (8.1%) 24 (11.9%) 0.51†Disposition Overall LOS (days) μ = 4.0 (σ = 3.2) μ = 3.6 (σ = 2.4) 0.37‡ ICU admission 11 (14.9%) 24 (11.9%) 0.54† Complications 12 (16.2%) 22 (10.9%) 0.30† Readmission w/in 30 days 4 (5.4%) 6 (3.0%) 0.47†
Boldface type indicates statistical significance. * Numbers in brackets represent patients from the control group/ERAS group.† Compares association between the 2 groups using Fisher’s exact test.‡ Compares mean differences, Satterthwaite method (assuming unequal variances across the groups).
TABLE 4. PROs in patients with elective spine and peripheral nerve surgery
Outcome* Control, n = 74 ERAS, n = 201p
Value†
Preop PRO score EQ-5D [74/180] μ = 8.8 (σ = 1.7) μ = 9.1 (σ = 1.6) 0.29 ODI [37/145] μ = 40.5 (σ = 17.4) μ = 43.3 (σ = 18.1) 0.41 NDI [13/32] μ = 38.0 (σ = 20.6) μ = 40.4 (σ = 20.0) 0.72 Overall health
rating [74/183]μ = 62.5 (σ = 22.4) μ = 66.6 (σ = 19.4) 0.14
Postop PRO score (1 mo)
EQ-5D [61/95] μ = 8.0 (σ = 2.0) μ = 8.4 (σ = 1.8) 0.20 ODI [21/78] μ = 25.4 (σ = 16.5) μ = 37.8 (σ = 19.9) 0.010 NDI [9/18] μ = 43.1 (σ = 18.8) μ = 40.8 (σ = 13.6) 0.71 Overall health
rating [61/100]
μ = 71.8 (σ = 21.3) μ = 73.0 (σ = 19.1) 0.70
∆ in PRO scores ∆EQ-5D [61/91] μ = −0.8 (σ = 2.0) μ = −0.5 (σ = 2.0) 0.38 ∆ODI [18/72] μ = −11.8 (σ = 12.9) μ = −4.3 (σ = 19.1) 0.12 ∆NDI [7/14] μ = 11.1 (σ = 22.6) μ = 11.1 (σ = 16.5) 1.00 ∆Overall health
rating [61/97]μ = 8.3 (σ = 25.9) μ = 4.5 (σ = 22.6) 0.33
∆ = change. Boldface type indicates statistical significance. * Numbers in brackets represent patients from the control group/ERAS group. † Compares mean differences, pooled method (assuming equal variances across the groups).

Ali et al.
J Neurosurg Spine January 25, 20198
sible and necessary to optimize the value of neurosurgical care. The present study has shown that our ERAS protocol greatly improves postoperative mobilization and ambula-tion and, most importantly, has the potential to safely re-duce opioid use both in the perioperative period and at 1 month after surgery, with important potential for relief of chronic opioid dependence.
AcknowledgmentsWe thank the personnel in the Neurosurgery Clinical Research
Division, who contributed to data acquisition in this manuscript. Some data capture was made possible by the Neurosurgery Qual-ity Improvement Initiative (NQII) EpiLog project. We also thank the Penn Innovation Center for allowing us to participate in Engaged Recovery at Penn.
References 1. Ali ZS, Ma TS, Ozturk AK, Malhotra NR, Schuster JM,
Marcotte PJ, et al: Pre-optimization of spinal surgery pa-tients: development of a neurosurgical enhanced recovery after surgery (ERAS) protocol. Clin Neurol Neurosurg 164:142–153, 2018
2. Archer KR, Wegener ST, Seebach C, Song Y, Skolasky RL, Thornton C, et al: The effect of fear of movement beliefs on pain and disability after surgery for lumbar and cervical de-generative conditions. Spine (Phila Pa 1976) 36:1554–1562, 2011
3. Baldini G, Bagry H, Aprikian A, Carli F: Postoperative uri-nary retention: anesthetic and perioperative considerations. Anesthesiology 110:1139–1157, 2009
4. Black N: Patient reported outcome measures could help transform healthcare. BMJ 346:f167, 2013
5. Brescia A, Tomassini F, Berardi G, Sebastiani C, Pezzatini M, Dall’Oglio A, et al: Development of an enhanced recovery after surgery (ERAS) protocol in laparoscopic colorectal surgery: results of the first 120 consecutive cases from a uni-versity hospital. Updates Surg 69:359–365, 2017
6. Christelis N, Wallace S, Sage CE, Babitu U, Liew S, Dugal J, et al: An enhanced recovery after surgery program for hip and knee arthroplasty. Med J Aust 202:363–368, 2015
7. Clarke H, Soneji N, Ko DT, Yun L, Wijeysundera DN: Rates and risk factors for prolonged opioid use after major surgery: population based cohort study. BMJ 348:g1251, 2014
8. Dangayach NS, Caridi J, Bederson J, Mayer SA: Enhanced Recovery After Neurosurgery: paradigm shift and call to arms. World Neurosurg 100:683–685, 2017
9. Fehlings MG, Tetreault L, Nater A, Choma T, Harrop J, Mroz T, et al: The aging of the global population: the changing epidemiology of disease and spinal disorders. Neurosurgery 77 (Suppl 4):S1–S5, 2015
10. Feneley R, Painter D, Evans A, Stickler D: Bladder catheteri-sation. Br J Gen Pract 52:500, 2002
11. Feneley RC, Hopley IB, Wells PN: Urinary catheters: history, current status, adverse events and research agenda. J Med Eng Technol 39:459–470, 2015
12. Garcia MM, Gulati S, Liepmann D, Stackhouse GB, Greene K, Stoller ML: Traditional Foley drainage systems—do they drain the bladder? J Urol 177:203–207, 2007
13. Grotle M, Vøllestad NK, Brox JI: Clinical course and impact of fear-avoidance beliefs in low back pain: prospective cohort study of acute and chronic low back pain: II. Spine (Phila Pa 1976) 31:1038–1046, 2006
14. Kahokehr A, Sammour T, Zargar-Shoshtari K, Thompson L, Hill AG: Implementation of ERAS and how to overcome the barriers. Int J Surg 7:16–19, 2009
15. Kashefi C, Messer K, Barden R, Sexton C, Parsons JK: Inci-
dence and prevention of iatrogenic urethral injuries. J Urol 179:2254–2258, 2008
16. Kehlet H: Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 78:606–617, 1997
17. Landers MR, Creger RV, Baker CV, Stutelberg KS: The use of fear-avoidance beliefs and nonorganic signs in predicting prolonged disability in patients with neck pain. Man Ther 13:239–248, 2008
18. Manchikanti L, Helm S II, Fellows B, Janata JW, Pampati V, Grider JS, et al: Opioid epidemic in the United States. Pain Physician 15 (3 Suppl):ES9–ES38, 2012
19. Manchikanti L, Singh A: Therapeutic opioids: a ten-year perspective on the complexities and complications of the escalating use, abuse, and nonmedical use of opioids. Pain Physician 11 (2 Suppl):S63–S88, 2008
20. McEvoy MD, Scott MJ, Gordon DB, Grant SA, Thacker JKM, Wu CL, et al: American Society for Enhanced Recov-ery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on optimal analgesia within an en-hanced recovery pathway for colorectal surgery: part 1—from the preoperative period to PACU. Perioper Med (Lond) 6:8, 2017
21. Melnyk M, Casey RG, Black P, Koupparis AJ: Enhanced re-covery after surgery (ERAS) protocols: time to change prac-tice? Can Urol Assoc J 5:342–348, 2011
22. Milles G: Catheter-induced hemorrhagic pseudopolyps of the urinary bladder. JAMA 193:968–969, 1965
23. Pereira Gomes Morais E, Riera R, Porfírio GJ, Macedo CR, Sarmento Vasconcelos V, de Souza Pedrosa A, et al: Chewing gum for enhancing early recovery of bowel func-tion after caesarean section. Cochrane Database Syst Rev 10:CD011562, 2016
24. Rajpal S, Gordon DB, Pellino TA, Strayer AL, Brost D, Trost GR, et al: Comparison of perioperative oral multimodal anal-gesia versus IV PCA for spine surgery. J Spinal Disord Tech 23:139–145, 2010
25. Saint S, Kowalski CP, Kaufman SR, Hofer TP, Kauffman CA, Olmsted RN, et al: Preventing hospital-acquired urinary tract infection in the United States: a national study. Clin Infect Dis 46:243–250, 2008
26. Short V, Herbert G, Perry R, Atkinson C, Ness AR, Pen-fold C, et al: Chewing gum for postoperative recovery of gastrointestinal function. Cochrane Database Syst Rev (2):CD006506, 2015
27. Sun EC, Darnall BD, Baker LC, Mackey S: Incidence of and risk factors for chronic opioid use among opioid-naive patients in the postoperative period. JAMA Intern Med 176:1286–1293, 2016
28. Valderas JM, Kotzeva A, Espallargues M, Guyatt G, Ferrans CE, Halyard MY, et al: The impact of measuring patient-reported outcomes in clinical practice: a systematic review of the literature. Qual Life Res 17:179–193, 2008
29. Wainwright TW, Immins T, Middleton RG: Enhanced recov-ery after surgery (ERAS) and its applicability for major spine surgery. Best Pract Res Clin Anaesthesiol 30:91–102, 2016
30. Wang MY, Chang HK, Grossman J: Reduced acute care costs with the ERAS® minimally invasive transforaminal lumbar interbody fusion compared with conventional minimally invasive transforaminal lumbar interbody fusion. Neurosur-gery 83:827–834, 2018
31. Wang MY, Chang PY, Grossman J: Development of an En-hanced Recovery After Surgery (ERAS) approach for lumbar spinal fusion. J Neurosurg Spine 26:411–418, 2017
DisclosuresDr. Welch reports ownership of Transcendental Spine.

J Neurosurg Spine January 25, 2019 9
Ali et al.
Author ContributionsConception and design: Ali, Kallan. Acquisition of data: Leszin-sky, McShane. Analysis and interpretation of data: Ali, Kallan. Drafting the article: Ali, Flanders. Critically revising the article: Ali, Flanders, Ozturk, Malhotra, McShane, Chen, Schuster, Grady, Welch. Reviewed submitted version of manuscript: Ali, Flanders, Ozturk, Malhotra, Leszinsky, Gardiner, Rupich, Chen, Schuster, Marcotte, Grady, Fleisher, Welch. Approved the final version of the manuscript on behalf of all authors: Ali. Statistical analysis: Kallan. Administrative/technical/material support: Ali, Flanders, Leszinsky, McShane, Gardiner, Rupich, Marcotte, Grady, Fleisher, Welch. Study supervision: Ali, Gardiner, Rupich, Grady, Fleisher, Welch.
Supplemental InformationPrevious PresentationsPart of this work was presented at the AANS annual meeting plenary session: “Enhanced Recovery After Surgery (ERAS) decreases post-operative opioid use in elective spine and periph-
eral nerve surgery.” AANS annual meeting, Plenary I; New Orleans, LA, April 30, 2018. A portion of this work was also pre-sented at the AANS Spine section meeting: “Enhanced Recovery After Surgery (ERAS) protocol in spinal and peripheral nerve surgery improves postoperative mobility and ambulation.” DSPN (Disorders of the Spine and Peripheral Nerves) meeting; Orlando, FL, March 16, 2018.
CorrespondenceZarina S. Ali: University of Pennsylvania, Philadelphia, PA. [email protected].