Embed Size (px)
Citation preview

147
ALAT of the patient
200 - A m A P -
Michael Winkler Burckhardt Ringe Karin Schneider Axel Maibucher Lothar Farber Hubertus Wietholtz Michael Manns Rudolf Pichlmayr
2000
Enhanced bioavailability of cyclosporinyusing a new oral formulation (Sandimmun optoral) in a liver-grafted patient with severe cholestasis
Received: 19 August 1993 Accepted: 2 September 1993
Sir: Cyclosporin-NOF (CyA-NOF) is a new oral formulation of cyclospo- rin A (CyA) based on the concept of microemulsion; its rate of resorption and its bioavailability are higher and more reliable than those of CyA [4]. We report here on a liver-grafted pa- tient suffering from severe cholesta- sis with CyA malabsorption who was converted from CyA to CyA-NOF. Following conversion to CyA-NOF, adequate CyA blood levels were maintained using only 20 % of the previous CyA dose, thereby avoiding prolonged intravenous CyA.
grafted for cholangiocellular carcino- ma in August 1991. Following trans- plantation (RWTH, Aachen, Ger- many) the patient was treated with CyA and steroids; the postoperative course was uneventful. In March 1992 the patient developed choles- tasis; several graft biopsies were per- formed but were inconclusive. On cholangiography a stenosis of the he- patic duct was found and effectively treated by endoscopic insertion of a stent prosthesis. A control cholangio- graphy performed in September 1992 showed sufficient bile flow without mechanical obstruction following
A 60-year-old male was liver
stent implantation; however, only a transient improvement in liver func- tion was observed.
In March 1993 the patient was ad- mitted to the Hannover Medical School for diagnostic work-up. On endoscopic cholangiography no sign of extrahepatic mechanical obstruc- tion was observed, and Doppler ultra- sound demonstrated vascular paten- cy of the graft. A biopsy showed late- stage chronic graft rejection with pro-
gressive loss of bile ducts. Since the patient presented with advanced stage liver dysfunction (bilirubin 700 pmol/l, AP 2000 U/I), antirejection treatment such as OKT3 therapy or conversion to FK 506 was not at- tempted.
Continuation of oral CyA treat- ment, however, was complicated by impaired CyA resorption, resulting in subtherapeutic CyA blood levels; only intravenous CyA therapy was
0 0 5 10 15 20 25 30
0 5 10 15 20 25 30
30 I
- m
H CYA CyA NOF
0 5 10 15 20 25 30
Days

148
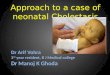
able to maintain the desired blood level range of 60-100 ng/ml. As un- limited continuation of intravenous CyA was not acceptable, the patient was placed on very high-dose oral CyA again (Fig. 1). However, neither stable nor adequate CyA blood lev- els could be achieved. Therefore, the decision was made to switch the patient to CyA-NOF for mainte- nance immunosuppression.
the resulting blood levels are shown in Fig. 1. Following the switch to CyA-NOF, adequate blood levels were maintained using only 20 % of the previous oral dose. After conver- sion to CyA-NOF, the patient was dis- charged from the hospital and is cur- rently scheduled for retransplanta- tion.
After oral application, resorption of CyA is highly dependent on bile q ~ w [l]. While in kidney-graftedpa- tients oral CyA treatment can be ini- tiated immediately post-transplanta- tion, in liver transplant patients a pro- longed initial intravenous treatment phase is necessary to ensure suffi- cient blood levels. In these patients oral CyA resorption is impaired by the initial bile diversionvia Tgube drainage [2,3] and/or initial liver dysfunction.
CyA therapy is safe and does not cause major problems, cholestatic liver dysfunction (e. g., due to me- chanical bile duct obstruction or graft rejection) may occur in some pa- tients, necessitating intravenous treatment or even conversion to other baseline immunosuppressants such asFK 506 [5].
The newly developed, advanced galenic form of cyclosporin (CyA- NOF) should ensure continuation of
The course of the CyA dosing and
While in the long-term course oral
oral CyA therapy in some of these pa- tients, e. g., in patients with nonimmu- nological cholestasis or with advanc- ed forms of chronic graft rejection that usually do not respond to immu- nosuppressive therapy with OKT3 or FK 506 [5]. This is clearly demon- strated by the clinical course of our patient. In this patient a switch from CyA to FK 506 for CyA malabsorp- tion was considered because unlimit- ed continuation of i. v. CyA was not feasible and oral CyA treatment re- sulted in insufficient blood levels bearing the risk of acute rejection. However, by administering CyA- NOF, the conversion to FK 506 was not necessary.
The good and constant resorp- tion of CyA-NOF that was ob- served in our patient and in other patients [4], despite low bile produc- tion of the liver due to cholestasis, implies that CyA-NOF therapy might also be indicated in patients with external bile diversion, e. g., in patients during the early phase after liver transplantation. It should be possible to administer early oral treatment with CyA-NOF to these patients and maintain reliable im- munosuppressive blood levels. Thus, prolonged intravenous treat- ment could be avoided, resulting in a reduction in the incidence and se- verity of the typical complications of i. v. CyA treatment, such as acute toxicity or anaphylactic reactions.
In conclusion, the reported case clearly demonstrates that CyA mal- absorption due to cholestasis and probably other causes can be over- come by the administration of CyA- NOF. Since CyA-based immunosup- pression is continued, conversion to other baseline immunosuppressants is not necessary in these patients.
References
1. Lemaire M,Fahr A, Maurer G (1990) Pharmacokinetics of cyclosporine: inter- and intra-individual variations and meta- bolicpathways. Transplant Proc22: 1110- 1112
2. Meta MU, Venkataramanan R, Bur- chardt GJ, Ptachcinski RJ, Delamos B, Stachak S,Thiel DHvan, Iwatsuki S, Starzl TE (1988) Effect of bile on cyclo- sporine absorption in liver transplant pa- tients. Br J Clin Pharmacol25: 579-584
3. NaournovNV, Tredger JM,Steward CM, O’GradyJG, Grevel J,Niven A, Whiting B, Williams R (1 989) Cyclosporine A pharmacokinetics in liver transplant reci- pients in relation to biliary T-tube clam- ping and liver dysfunction. Gut 30: 391- 396
4. Trull AK,Tan KKC, Uttridge J,BauerT, Alexander GJM, Jamieson NV (1 993) Cyclosporine absorption from microe- mulsion formulation in a liver transplant recipient. Lancet 341: 433
RodeckB,BuhrT, Brinkmann C, Pichlmayr R (1993) Conversion from cy- closporin to FK 506 after liver transplan- tation. Transpl Int 6: 319-324
5. Winkler M, Ringe B, Jost U, Melter M,
M. Winkler (E l ) . B. Ringe R. Pichlmayr Klinik fur Abdominal- und Transplantationschirurgie, Medizinische Hochschule Hannover, Konstanty Gutschowstrasse 8, D-30623 Hannover, Germany
K. Schneider M. Manns Abteilung fur Gastroenterologie und Hepatologie, Zentrum Innere Medizin, Medizinische Hochschule Hannover, Konstanty Gutschowstrasse 8, D-30623 Hannover, Germany
A. Maibiicher L. Farber Clinical Research Deparjment, Sandoz AG, Deutschherrnstrasse 15, D-90429 Npnberg, Germany
H. Wietholtz Medizinische Klinik 111, RWTH Aachen, Medizinische Fakultat, Pauwelsstrasse 30, D-52074Aachen, Germany