-
ENFOQUE MULTIDIMENSIONAL DE LA FALLA
CARDIACA EN EL ADULTO
MAYOR DIANA CAROLINA MORALES BENAVIDES
MEDICA INTERNISTA Y GERIATRA UNIVERSIDAD
DE CALDAS
GRUPO DE GERIATRIA Y CUIDADO
PALIATIVO GERIATRICO FUNDACION SANTA
FE DE BOGOTA
2016
JUEVES 19 DE MAYO DE 2016
07:00 – 18:00 INSCRIPCIONES
SALÓN SANTA FE 1
CURSO 1 Metodología de investigación. Bases de datos
longitudinales en el campo delenvejecimiento.
Coordinador: Rafael Samper, BogotáHorario: 09:00 - 13:00
Presentación del cursoRafael Samper, BogotáMetodología de
investigación. Bases de datos longitudinales en el campo
delenvejecimientoRebeca Wong, USAAlejandra Michaels,
BogotáResultados de investigación con los estudios ELPS y
ELCARafael Santos, Bogotá
SALÓN SANTA FE 2
CURSO 2 Papel del gerontólogo en la humanización y en los
servicios de cuidado socio-sanitario en la vejez
Coordinador: Fabián Ricardo Villacis, BogotáHorario: 09:00 -
13:00
Presentación del cursoFabián Ricardo Villacis, BogotáPapel del
gerontólogo en la humanización y los sistemas de cuidados en la
vejezDerechos y participación de las personas adultas
mayoresRoberto Angarita, BogotáModelo participativo de salud mental
comunitaria en personas adultas mayores.Elizabeth Machado,
SincelejoHogar san Vicente de Paul, un lugar de apropiación y
vínculos.Diana Fernanda Bermúdez, ArmeniaCalidad y humanización en
la atención socio sanitaria a las personas adultas mayoresClaudia
Janeth Ladino, Armenia
SALÓN SANTA FE 3 (AB)
CURSO 3 Enfermedad terminal: un desafío y una oportunidad
integralExpositora: Nidia Aristizabal, BogotáHorario: 09:00 -
13:00
Enfermedad terminal: un desafío y una oportunidad integral
-
CONTENIDO
• Contexto epidemiológico: prevalencia de
falla cardíaca en el adulto
mayor
• Cambios fisiológicos con el
envejecimiento • Enfoque
mul>dimensional • Falla cardíaca
y grandes síndromes geriátricos:
fragilidad, mul>morbilidad, deterioro
cogni>vo
• Conclusiones
-
Falla cardíaca: prevalencia • Causal
de 59 000 muertes
en 2005 en US • Causas primarias.
CORONARIA-‐HIPERTENSIVA • Prevalencia: 5-‐10%
entre
65-‐69 años • 18% en mayores de
85 años • IMPACTO NEGATIVO para
lograr envejecimiento exitoso
-
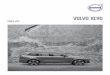
ENVEJECIMIENTO Y SISTEMA CARDIOVASCULAR
European Journal of Heart Failure
(2013) 15, 717–723 Heart failure
in elderly paJents: disJncJve
features and unresolved issues
Reducción en número y función de
miocitos (apoptosis)
ARTERIOESCLEROSIS: aumento de la
poscarga
Alteración en la regulación del
calcio Cambios en las
proteínas contrác>les Menor
eficacia en la u>lización de
ATP
PREDOMINIO DE FALLA CARDIACA DE
FRACCION DE EYECCION CONSERVADA
ACORTAMIENTO TELOMERICO: presbicardia: aumento
del contenido colágeno en
inters>cio: FIBROSIS
Precipitado por: hiperac>vación del
eje RAA, ROS, INFLAMAGING
TENDENCIA A LA HIPERTROFIA DEL VI
Trastorno de relajación
-
European Journal of Heart Failure
(2013) 15, 717–723 Heart failure
in elderly paJents: disJncJve
features and unresolved issues
overall survival after HF onset has substantially improved with
con-temporary therapies,9 this benefit is less evident in older
agegroups.15,16 Advanced age remains a strong predictor for poor
out-comes in patients with chronic17 or acute HF,11 and it is
included inseveral prognostic models for mortality after
hospitalization.18
Pathophysiology of the ageingheartSeveral specific changes in
cardiac structure and function are asso-ciated with cardiac ageing,
and they may explain a number ofpathophysiological and phenotypic
features typical of the elderly.Among these, particularly important
is the greater predispositionof the elderly to develop HF,
particularly HF with preserved ejec-tion fraction (HFpEF)4,12,19
(Figure 1).
With age, there is a decrease both in number and in function
ofmyocytes, which occurs even in subjects without evidence of
car-diovascular disease.20 The underlying mechanisms of such
changesinclude enhanced necrosis and apoptosis,21 and a reduced
regen-erative capacity of cardiac progenitor cells. This prevents
adequatereparation for myocyte loss either caused by ageing, or
secondaryto myocardial injury and ischaemia.21 The loss of
functioning
cardiomyocytes is compensated by the hypertrophy of the
remain-ing cells.20
Alterations in the function of myocytes associated with
ageinclude impaired calcium metabolism and regulation, which
reflectsan alteration of processes of contraction and relaxation.22
In add-ition, contractile proteins change with age similarly to the
altera-tions seen in hypertrophic hearts.23 Finally, ATP
utilization is lessefficient in the ageing heart. These
abnormalities may providethe substrate for worsening cardiac
function in the setting of ex-acerbating conditions, even in
otherwise healthy hearts.22
Another potential mechanism associated with the higher risk of
de-velopment of HF in advancing age is the shortening of
telomeres,which has been suggested as a marker of biological and
cellularageing and associated with development of HF.21,24
Simultaneously with the reduced number, function, and
com-pensatory hypertrophy of myocytes, the senescent myocardiumis
affected by an imbalance of extracellular matrix metabolism,with a
subsequent detrimental increase in myocardial collagencontent and
development of fibrosis.25 Myocardial fibrosis is pro-moted by
several mechanisms26 known to be up-regulated in HF atany age, and
which are constitutively activated in the elderly. Theyinclude the
up-regulation of the renin–angiotensin–aldosteronesystem,25
enhanced inflammatory activity,27 and oxidative stress.25
Figure 1 Suggested pathophysiological mechanisms predisposing to
the development of diastolic dysfunction and heart failure in
otherwisehealthy ageing hearts.
V. Lazzarini et al.718
-
Impacto en calidad de vida:
FUNCIONALIDAD
Impacto en cuidadores: AGOBIO
Adherencia al tratamiento Riesgo
de hospitalización
Interacción con la mulJmorbilidad
Costos para el sistema
DIMENSION DE LA FALLA CARDIACA EN
EL ADULTO MAYOR
-
DIMENSION DE LA FALLA CARDIACA EN
EL ADULTO MAYOR
85% marcapasos 61% CDI 53% CABG
51% ICP 60% cambio valvular 75%
endarterectomías
COSTOS. En los mayores de
65 años se realizan:
-
ABORDAJE MULTIDIMENSIONAL DE LA FALLA
CARDIACA EN EL ADULTO MAYOR
Condición índice: FALLA
CARDIACA
-
FRAGILIDAD Y FALLA CARDIACA
• Falla cardíaca en el adulto
mayor: más allá del modelo
orientado en la enfermedad
• Enfoque desde la FRAGILIDAD •
Ayuda a es>mar:
CliniCal MediCine insights: Cardiology
2014:8(s1) The Biologic Syndrome of
Frailty in Heart Failure
Riesgo de mortalidad , toma de
decisiones
Potencial riesgo de eventos adversos
Riesgo de hospitalizaciones
-
COMO MEDIR LA FRAGILIDAD? ÍNDICE
DE FRAGILIDAD
-
EDAD BIOLÓGICA/ EDAD CRONOLÓGICA:
Canadian Study of Health and
Aging “Es>mar el acúmulo de
déficit se relaciona con la
edad biológica”
-
COMO MEDIR LA FRAGILIDAD? CUESTIONARIO
FRAIL
• CUESTIONARIO FRAIL • Evaluación
subje>va de 5 puntos. • Ha
demostrado correlación con riesgo de
discapacidad, baja velocidad de
marcha, mortalidad y menor desempeño
en SPPB
• FRAGIL 3 A 5 PUNTOS • PRE
FRAGIL 1 A 2 PUNTOS •
NO FRAGIL 0 PUNTOS.
•
A SIMPLE FRAILTY QUESTIONNAIRE (FRAIL)
PREDICTS OUTCOMES IN MIDDLE AGED
AFRICAN AMERICANS
J Nutr Health Aging. 2012 July
; 16(7): 601–608.
FATIGA. En las úlJmas 4 semanas
qué tanto se ha senJdo cansado
o faJgado? Respuestas 1 y
2: 1 punto. Demás 0
puntos
1. Todo el Jempo 2. La
mayoría del Jempo 3. Algunas
veces 4. Muy pocas veces 5.
Nunca
RESISTENCIA. Presenta alguna dificultad
para caminar 10 pasos sin
descansar sin ayuda de disposi>vos
ni de otra persona?
1. Si 2. No
DEAMBULACION. Sin uso de ayudas,
>ene alguna dificultad para
caminar mas de 100 metros?
1. Si 2. No
Número de enfermedades 0 a
4: 0 puntos 5 a 11:
1 punto
PESO. Cuál es su peso
actual y cuál era su peso
hace 1 año?
Porcentaje de cambio > 5% 1
punto Porcentaje de cambio
< 5% 0 puntos.
-
Estrategia clínica de falla cardíaca
Fundación Santa Fe
1. Paciente adulto mayor llega a
consulta o interconsulta hospitalaria
a clínica de falla cardíaca
2. Aplicación de cues>onario FRAIL
por el servicio de cardiología
3. Cumple criterios para fragilidad o
además presenta:
• Polifarmacia • Comorbilidad
MÉDICOS
• Demencia • Depresión moderada/severa
PSÍQUICOS • Discapacidad moderada-‐severa
FUNCIONALES
• InsJtucionalización • Agobio del cuidador
SOCIALES
-‐ Valoración Geriátrica mulJdimensional
-
728 F. Cacciatore et al.
© 2005 Blackwell Publishing Ltd, European Journal of Clinical
Investigation, 35, 723–730
mobility with a tendency to fall, polipharmacy, comorbidity,low
social status, cognitive impairment and nutritionalimpairment
[30–32]. Several attempts have been made tograde frailty [30,31],
which was recently resolved accordingto the results of two tests of
physical ability involving rapidwalking and standing from a sitting
position: subjects ableto perform one of these tests were
considered moderatelyfrail and those unable to perform either were
consideredseverely frail [33]. However, that method considers
onlythe physical domain. This study considers that its
gradingmethod is more consistent with the complexity of
frailty,which utilizes a short approach focused on selected tests
ofvision, hearing, arm and leg function, urinary
incontinence,mental status, instrumental and basic activities of
dailyliving, environmental hazards and social support systems
[13].
Relationship between frailty and CHF in the elderly
Newman et al. in the Cardiovascular Health Study deter-mined
that persons with a history of CHF were more likelyto be frail
[17]. In a prospective study of 178 patientsdependent in at least
one basic activity of daily living andhospitalized with
cardiovascular disease, primarily CHFand acute coronary syndromes,
there was an increased riskof further functional decline after 1
year [34]. Chronic heartfailure is associated with increased health
service care [35]and institutionalization [36], both of which are
products offrailty. Patients with functional decline are at
increased riskof hospitalization for CHF [37].
These data demonstrate that frailty is more predictive
ofmortality in elderly subjects with CHF than in those withoutCHF.
None of the CHF subjects, in this study, with advancedfrailty
survived after 9 years’ follow up, whereas those inNYHA class IV
are still alive. Why does frailty influence themortality of elderly
patients with CHF in such a way? Thereare several possible reasons
for this intriguing phenomenon.In this sample the high grade of
frailty, when compared withNYHA class IV, represents the highest
value of comorbidity
(5·4 vs. 5·2), of drugs used (5·1 vs. 4·9), and the lowest
scoreof MMSE (18·7 vs. 22·6). More importantly, disability inADL
affects 83% of frail subjects but only 25% of NYHAclass IV
subjects. The use of vasodilators, such as nitrates,known to
influence the prognosis of CHF, progressivelydecreases with frailty
(from 42% to 11%). These findingsare particularly significant in
understanding how to managethe care of frail CHF elderly
patients.
Considered singularly, each of the characteristics of frailtyis
highly prevalent and is a predictor of poor prognosis inelderly
patients with CHF. The Charlson comorbidity indexscore closely
correlates with early hospital readmission ordeath in patients with
CHF [38,39]. Rich et al. have dem-onstrated that iatrogenic CHF,
i.e. CHF precipitated bymedications or excessive fluid
administration, characterizesthe poor prognosis of debilitated
older patients showing lesssevere premorbid cardiac disease, but
more marked non-cardiac disease and longer hospital stays [40]. In
this regard,the declining use of nitrates, observed in our study,
mightreflect a greater risk of side-effects (hypotension leading
tofalls) in the frail elderly. However, it could not be
excludedthat the reduced use of nitrates could reflect the
lowprevalence of ‘typical’ CHF symptoms compared with‘atypical’
presentations in the frail elderly (assuming nitrateswere primarily
prescribed to treat typical CHF symptoms)[9]. The prevalence of CHF
in cognitively impaired subjectsis high and the risk of developing
cognitive impairmentwas 1·96-fold greater in subjects with CHF
[11], and it isassociated with a fivefold increase in mortality
after adjust-ing for several potential confounders [12]. A recent
studyon cardiovascular diseases as determinants of disabilityshowed
that the prevalence of disability was 22·6% in menand 37·3% in
women with CHF. After the cerebrovasculardiseases, CHF was the most
powerful predictor of disabilityin men [41]. Poor social support
has also been described asa marker for patients with CHF [38]. In
292 elderly subjectswith CHF, after adjustment for demographic
factors,clinical severity, comorbidity and functional status,
socialties and instrumental support, the absence of
emotionalsupport remained associated with a significantly higher
risk
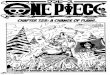
Figure 1 Cox regression adjusted survival curve in subjects with
(a) CHF (n = 120) and without (b) CHF (n = 1139) chronic renal
failure (CHF) stratified by frailty.
European Journal of Clinical Inves9ga9on
(2005) 35, 723–730 Frailty predicts
long-‐term mortality in elderly
subjects with chronic heart failure
OBJETIVO: rol predic>vo de la
fragilidad en mortalidad en pacientes
con ICC N: 1139 >65 años
en comunidad. 129 con ICC.
Seguimiento a 12 años
Campania, Italia. FRAGILIDAD: perfil
de Linda Fried MORTALIDAD:
ICC + FRAGILIDAD= 94.4% ICC
sin FRAGILIDAD= 70%
-
• 90% de los pacientes con falla
cardíaca >enen más de 2
comorbilidades
• La ERC y EPOC son predictores
de riesgo de hospitalización y
reingresos en falla cardíaca
• 2010. Medicare. 27% de pacientes
con falla cardíaca tenían deterioro
cogni>vo
MulJmorbidity in Older Adults with
Heart Failure
Clin Geriatr Med 32 (2016) 277–289
FALLA CARDIACA Y MULTIMORBILIDAD
-
EL PROBLEMA… contexto clínico
MulJmorbidity in Older Adults with
Heart Failure
Clin Geriatr Med 32 (2016) 277–289
exist, one can simply start by asking patients if they
can do what is asked of them, andif so, at what cost?70 Their
responses should be used to prioritize the conditions
worthaddressing and the specific strategies used. Reducing
polypharmacy is one relativelyeasy way to decrease treatment burden
and may improve quality of life without otheradverse effects.72
Enhance Care-Coordination
Care coordination and multidisciplinary team-based care has been
shown to improveoutcomes in older multimorbid patients at high risk
for hospitalization. For example,Medicare demonstration projects
successful in lowering preventable hospitalizationsthrough improved
care coordination had the following common features: (1)
frequentin-person meetings between care coordinators and patients;
(2) in-person meetingsbetween care coordinators and health
providers; (3) supplemental educational ses-sions for patients and
caregivers; (4) medication management services; and (5) timelyand
comprehensive transitional care after hospitalization.73 Similarly,
reductions inreadmission after hospitalization for HF have been
achieved through use of multi-pronged strategies delivered by
multidisciplinary teams of physicians, nurses, socialworkers,
pharmacists, physical therapists, and care managers both during and
afterhospitalization.74–76 The most successful hospitals have used
a large number of stra-tegies designed to integrate hospital and
postacute care77 and have successfullyreduced readmissions from the
full range of medical conditions to which older patientswith HF are
vulnerable after hospital discharge.78
SUMMARY
Multimorbidity is a common feature of HF that impacts diagnosis,
management,and outcomes. It is therefore critical that providers
caring for older patients withHF adopt broad patient-centered
perspectives rather than focus exclusively on car-diovascular
conditions. Treatment strategies should be closely aligned to
patients’specific health goals and well-calibrated to the workload
they wish to expend. Withthis perspective, benefits of treatment
can be maximized while minimizing poten-tially harmful
consequences.
REFERENCES
1. Chamberlain AM, St Sauver JL, Gerber Y, et al. Multimorbidity
in heart failure: acommunity perspective. Am J Med
2015;128:38–45.
Box 1Typical burden of an older person with heart failure and
multimorbidity
! Has 4 other chronic conditions in addition to heart
failure1
! Takes 10 or more medications a day47
! Spends about 2 hours per day on health-related
activities80
! Attends 15 or more outpatient appointments with physicians
each year81
! Needs assistance with at least one activity of daily
living5,82
! Experiences hospitalizations for multiple conditions7,8
All are best estimates based on the available published
literature, but burden is likely to varywidely across individual
patients.
Data from Refs.1,5,7,8,47,80–82
Dharmarajan & Dunlay284
-
• 90% de los estudios excluyen
pacientes con mul>morbilidad
• 1/3 de los estudios fase 3:
excluyen pacientes con discapacidad,
deterioro cogni>vo, ins>tucionalizados
o comorbilidad crónica
• Ejemplos: CHARM y PRESERVE excluyeron
pacientes con expecta>va de vida
menor de 3 años.
• Desenlaces primarios en geriatría:
mareo, inestabilidad, caídas, calidad
de vida, descompensación de
comorbilidad (?)
EL PROBLEMA… nivel de evidencia
MulJmorbidity in Older Adults with
Heart Failure
Clin Geriatr Med 32 (2016) 277–289
-
patients’ lives by advances in heart failure management.
Analysis
of trends in comorbidities and drug use from 1988 to 2008
shows
an increase in the proportion of octogenarians with heart
failure
(from 13.3% to 22.4%) along with an increase in the number
of
patients with five or more comorbidities (from 42% to 58%)
and
number of daily prescription medications from 4.1 to 6.4
drugs
[5]. Comorbidities unrelated to heart failure (e.g., dementia
and
hip fracture) are more prevalent in above 86 age group [6].
Comorbidities affect the quality of life and survival in heart
failure
patients—the more the comorbidities, the more the
hospitaliza-tion and mortality. Noncardiac comorbidities are found
to be more
prevalent in patients with heart failure with preserved
ejection
fraction compared to those with heart failure with reduced
ejec-
tion fraction, leading to higher non-HF hospitalization rate.
The
impact of these comorbidities in both groups is, however,
the
same [7].
Previous data on the presence and effect of comorbidities on
CHF were derived from geographically limited studies of
relatively
small numbers of patients such as the Framingham cohort [8].
More recent studies have utilized databases to examine the
impact
of comorbidity in larger groups of elderly patients with
CHF.
Utilizing data from 27,477 Scottish morbidity records listing
CHF,
Brown and Cleland [9] reported 11.8% of CHF admissions were
associated with chronic airway obstruction, 8.3% with chronic
or
acute renal failure, and 5.3% with cerebrovascular accident.
The
National Heart Failure project, from the Centres for Medicare
and
Medicaid Services in the USA, previously reported
comorbidities
among 34,587 Medicare patients aged >65 years who were
hospi-talized with a principal diagnosis of CHF [10]. About a third
had
chronic obstructive pulmonary disease (COPD), 18% had a his-
tory of stroke, and 9.2% had dementia. A retrospective
cohort
study of 1,363,977 elderly Medicare beneficiaries
hospitalized
with heart failure from 2001 to 2004 described comorbid
condi-
tions including diabetes mellitus (36.8%), renal failure
(18.5%),
and dementia or major psychiatric disorders (13.5%) [11].
Braunstein et al. identified 122,630 individuals aged >65
yearswith CHF through a 5% random sample of all US Medicare
ben-
eficiaries. Nearly 40% of patients with CHF had >5
noncardiaccomorbidities, and this group accounted for 81% of the
total
inpatient hospital days experienced by patients with CHF.
The
risk of hospitalization and potentially preventable
hospitalizations strongly increased with the number of
chronic
Figure 1 Interaction of noncardiac comorbidities in chronic
heart failure (CHF). Solid lines toward centre: Comorbidities
contributing to CHF; Solid lines
away from centre: Sequelae of CHF; Blue boxes: Direct
contributors to worsening CHF; Yellow boxes: Indirect contributors
to worsening CHF; Curved
arrows: Interaction between comorbidities.
ª 2015 John Wiley & Sons Ltd Cardiovascular Therapeutics 33
(2015) 300–315 301
V. H. Chong et al. Management of Comorbidities in Heart
Failure
Management of Noncardiac ComorbidiJes in
Chronic Heart Failure Cardiovascular
Therapeu>cs 33 (2015) 300–315
-
• UK. Clínica de falla cardíaca:
74% de los pacientes con clase
funcional NYHA II-‐ IV tenían
puntajes de MOCA test entre
17-‐25 puntos
• SOLVD-‐ WHAS I: hallazgos similares
FALLA CARDIACA Y DETERIORO COGNITIVO
CogniJve impairment in heart failure
paJents Journal of Geriatric
Cardiology (2014) 11: 316−328
Atención Velocidad de procesamiento
Síndrome disejecuJvo Memoria de trabajo
Recomendación de American Geriatric
Society: aplicar tamizaje cogniJvo
ANUAL a pacientes con ICC
-
RECOMENDACIONES PARA TENER EN CUENTA
MulJmorbidity in Older Adults with
Heart Failure
Clin Geriatr Med 32 (2016) 277–289
1. ENFOQUESE EN LOS DESENLACES
GLOBALES EN SALUD
IdenJfique síntomas: dolor, disnea,
faJga Evalúe calidad de vida
Determine el estado funcional MEBE-‐
AVD Procure reducir CUALQUIER CAUSA
de hospitalización no solo por
falla cardíaca Discuta pronósJco
2. EVALUE FORMALMENTE COGNICION Y
AFECTO
MOCA-‐ MMT-‐ Mini Cog-‐ Yesavage-‐
PHQ2
3. APLIQUE TRATAMIENTOS NO
FARMACOLOGICOS
Ac>vidad usica-‐ rehabilitación cardíaca
Medidas generales para
ortosta>smo
4. MINIMIZE EL AGOBIO POR
LA ENFERMEDAD
Pregúntele al paciente cuál es le
principal síntoma que lo agobia
Des-‐prescripción Disminuya el
número de citas médicas
5. COMUNIQUESE CON LOS OTROS
ESPECIALISTAS QUE TRATAN AL PACIENTE
Plan interdisciplinario INTEGRADO
-
CONCLUSIONES • La transición
demográfica lleva a mayor carga
de enfermedad
cardiovascular en el mundo • Es
más frecuente la ICC de
fracción de eyección preservada en
el
adulto mayor • Existe alta
prevalencia de fragilidad en adultos
mayores con ICC • La fragilidad
es un predictor de desenlaces
adversos • La presencia de
comorbilidad genera un impacto
nega>vo en
índices de pronós>co y calidad
de vida en el adulto mayor
con ICC • Existe una relación
directamente proporcional entre la
severidad
de ICC y la presencia de
deterioro cogni>vo • Es necesario
realizar tamizajes de deterioro
cogni>vo en
pacientes con ICC