Embed Size (px)
Citation preview
Endovascular Treatment of Splenomesenteric–Portal Vein Thromboses during OrthotopicLiver TransplantationMilagros Marini, MD, Manuel Gomez-Gutierrez, MD, Ignacio Cao, MD, Carlos Selles, MD,
Javier Aguirrezabalaga, MD, Alejandra Otero, MD, and Rafaela Soler, MD
Extensive splanchnic venous thrombosis in patients undergoing orthotopic liver transplantation (OLT) continues tohave a substantial impact on surgical complexity and perioperative morbidity and mortality rates. This report presentsan experience in eight patients with splanchnic venous thrombosis treated by means of splanchnic vessel recanali-zation, primary stent placement, and closure of spontaneous competitive shunts during OLT. In all cases, portalperfusion in the allograft was adequate, portal hypertension was solved, and no complications were observed. Noneof the patients died during surgery or follow-up. The results reported here need to be confirmed in future studies.
J Vasc Interv Radiol 2005; 16:1135–1142
Abbreviations: ETVE � eversion thromboendovenectomy, IMV � inferior mesenteric vein, OLT � orthotopic liver transplantation, PV � portal vein,SMV � superior mesenteric vein, SV � splenic vein, UV � umbilical vein
EXTENSIVE splanchnic venousthrombosis has always made ortho-topic liver transplantation (OLT) moredifficult. Portal vein (PV) thrombosisincidence in OLT usually ranges from2% to 19% but may reach 39% in cer-tain patient populations (1–7). Indeed,in early OLT experience, PV thrombo-sis was regarded to be sufficient causeto rule out OLT, in the belief that thegraft could not be provided a satisfac-tory portal inflow. The introduction ofinnovative surgical techniques such asthrombectomy, venous jump grafts, andthe use of PV tributaries has sur-mounted many obstacles, but PVthrombosis still has a substantial impact
on surgical complexity and periopera-tive morbidity and mortality rates (1–5).
Endovascular techniques providesafe and effective treatment for earlyand late vascular complications afterOLT, with excellent medium- andlong-term results (8–13). However,operating theater cooperation betweensurgeons and interventional radiolo-gists during OLT to treat these cases ofextensive PV thrombosis is fairly infre-quent.
The aim of the present study is todetermine the efficacy of endovasculartechniques to assist intraoperativemanagement of splenomesenteric–PVthrombosis and competitive shuntsduring OLT.
MATERIALS AND METHODS
We performed 467 OLTs in 436adults between May 1994 and July2004. Seventy-three patients presentedPV thrombosis or portal sclerosis atthe time of OLT.
Study Group
Eight patients treated from Novem-ber 1999 to January 2004 who had in-
traoperatively confirmed PV thrombo-sis in a cirrhotic liver are the subject ofour present analysis. This study wasapproved by our institutional reviewboard and a waiver was granted forinformed consent. In all cases, endo-vascular procedures were conductedduring OLT. In six patients, the cirrho-sis was of alcoholic origin; in one case,the disease was caused by Hepatitis Bvirus; and in another, it was a result ofde novo Hepatitis C virus plus infec-tion in a replaced graft. Five patientswith alcoholic cirrhosis also had hep-atocellular carcinoma. All patients hada chronic, nontumoral thrombus in thePV or a sclerotic PV (ie, PV reduced toa fibrotic vessel remnant). The diagno-sis was made intraoperatively in thefirst two cases and preoperatively inthe rest. The Table shows the charac-teristics of patients, their surgical andendovascular treatment, and follow-up. On the basis of the intraoperativethrombosis extension, PV thrombosiswas classified according to the criteriaof Stieber et al (1): grade I, minimallyor partially thrombosed PV with athrombus no more than 50% of thevessel lumen; grade II, more than 50%and less than 100% occlusion of the
From the Department of Radiology (M.M., I.C., R.S.)and Liver Transplant Unit (M.G.G., C.S., J.A., A.O.),Complejo Hospitalario Universitario Juan Canalejo,84 La Coruna 15006, Spain. Received December 11,2004; revision requested February 12, 2005; final re-vision received March 20; accepted March 25. Fromthe 2004 SIR Annual Meeting. Address correspon-dence toM.M.; E-mail: [email protected]
None of the authors have identified a conflict ofinterest.
© SIR, 2005
DOI: 10.1097/01.RVI.0000167851.00221.B0
1135
PV; grade III, complete thrombosis ofthe PV and proximal superior mesen-teric vein (SMV); grade IV, completethrombosis of the PV and proximaland distal SMV.
The surgical technique for PVthrombosis was eversion thromboen-dovenectomy (ETVE) (3) with end-to-end PV anastomosis. When the portalflow was insufficient despite surgery,a vascular interventional radiologistwas called into the operating theater toperform intraoperative portography.
Endovascular Technique
The Seldinger technique (Fig 1) wasused to catheterize the graft umbilicalvein (UV) or one of the recipient’s in-ferior mesenteric vein or SMV tribu-taries with a 7–10-F sheath (Terumo,Tokyo, Japan). When the approachwas through the umbilical vein, a 5-FCobra 2 glide catheter (Terumo) with a0.035-inch angled hydrophilic guidewire (Terumo) was inserted throughthe PV anastomosis, placing the cath-eter beyond the SMV or splenic vein(SV) junction. When the approach wasthrough a SMV or IMV tributary, theportogram was obtained through theside port of the sheath before measur-ing the pressure in the main PVbeyond the anastomosis with a 5-Fvertebral glide catheter (Terumo) at-tached to a 0.035-inch angled hydro-philic guide wire.
If the cause of sluggish flow was anobstructive thrombus or stenosis re-
sulting from incomplete thrombus re-moval from the splenomesenteric con-fluence, and the gradient was 5 mmHg or higher, portal venoplasty wasperformed using a 12-mm-diameter,4-cm-long angioplasty balloon, fol-lowed by primary placement of self-expanding, 14-mm-wide, 30-mm-longEasy Wallstents (Boston Scientific,Natick, MA) in four cases and 14-mm-wide, 40-mm-long Wallstent Unistents (Boston Scientific) in three cases.The PV pressure was remeasured im-mediately after these procedures and,in cases in which the gradient re-mained persistently higher than 5 mmHg, a second venoplasty was per-formed with a 14-mm-diameter, 4-cm-long angioplasty balloon. Portographywas subsequently conducted to assessthe results of the procedures and em-bolize any competitive portosystemicshunts that had not disappeared. Em-bolization was effected with multiple10-mm, 12-mm, and 15-mm-diameterstainless-steel coils to obtain betterportal hepatopetal flow, improve graftperfusion, and prevent steal at the ex-pense of portal flow.
Shunts were surgically ligated orembolized with stainless-steel coilsprovided there was no evidence of re-sidual thrombus after ETEV, no gradi-ent was found in the retropancreaticarea of the PV, and the sole cause ofthe insufficient portal flow was a stealphenomenon resulting from nativeportosystemic shunts.
A further portographic analysis
was then conducted and pressuremeasurements were taken. After suit-able results were obtained, bringingthe interventional radiology team’sparticipation to a close, the surgicalteam completed the OLT. Patients didnot undergo anticoagulation duringthe endovascular procedure or in thepostoperative period, nor were anti-platelet agents used routinely duringfollow-up.
Follow-up included Doppler ultra-sound (US) assessment of PV patencyat 24, 48, and 72 hours, 1 week, and 1month after surgery, and then every 3months for 1 year and annually there-after. PV patency was established onDoppler US by the detection of contin-uous flow with variations in velocityinduced by respiration. Angiographywas performed only in patients inwhom Doppler US findings were notconclusive.
Study Endpoints
We studied the grade of PV throm-bosis by direct portography in theoperating theater, the success of theendovascular procedures, and the fol-low-up until 2004.
Immediate technical success onportography images was defined by agood demonstration of the intrahe-patic portal radicles, disappearance ofhepatofugal collateral veins, no fillingof the closed competitive portosys-temic shunts, and accurate stent place-ment in the occluded venous system,
Summary of Patients’ Clinical Characteristics and Surgical Outcomes
Pt. No./Sex/Age (y)
Indication for OLT Grade of PVThrombosis
Thrombosis Extension SurgicalTechniques
EndovascularProcedure
1/M/58 Alcoholic HCC IV PV, SMV, SV ETVE Stent/shunts,embolization
2/M/55 Alcoholic HCC IV PV, SMV, SV ETVE Stent/shunts,embolization
3/M/61 Alcoholic HCC III PV, minimum extensionof SMV, SV
ETVE Shunts, embolizations
4/M/61 Alcoholic HCC III Sclerosed PV PV confluenceanastomosis
Stent/shunts,embolization
5/M/59 Alcoholic HCC III Sclerosed PV PV confluenceanastomosis
Stent/shunts,embolization
6/M/66 Alcoholic HCC III PV calcification ETVE Stent7/M/48 Regraft for HCV, de novo IV PV, SMV, SV ETVE Stent8/F/43 HBV modified Sugiura
procedureIV PV, SMV, SV ETVE Stent
Note.—All patients were alive at follow-up July 31, 2004. HCC � hepatocellular carcinoma; HBV � Hepatitis B virus; HCV �Hepatitis C virus. See text for details of PV thrombosis grading.
1136 • Splenomesenteric–Portal Vein Thromboses Treatment during OLT August 2005 JVIR
which was recanalized with a pressuregradient of less than 5 mm Hg. Imme-diate clinical success was defined bythe absence of complications dur-ing OLT, no postoperative mortalitywithin 30 days, no PV rethrombosis,and no signs of portal hypertension,variceal hemorrhage, or ascites.
Technical and clinical success at fol-low-up was defined by stent and sple-nomesenteric PV patency by means of
Doppler US or arteriography. If Dopp-ler US assessment was not conclusive;technical and clinical success was de-fined by no signs of portal hyperten-sion, normal function of the graft, andliver test results in normal ranges.
RESULTS
Our series comprised four cases ofgrade IV PV thrombosis and four cases
of grade III PV thrombosis. Portal re-canalization, primary stent placement,and closure of native shunts were suc-cessful in all patients. Portal perfusionin the graft was adequate and portalhypertension was solved in all pa-tients. No complications were ob-served during endovascular proce-dures. None of the patients diedduring surgery or in the postoperativeor follow-up periods. At this writing,
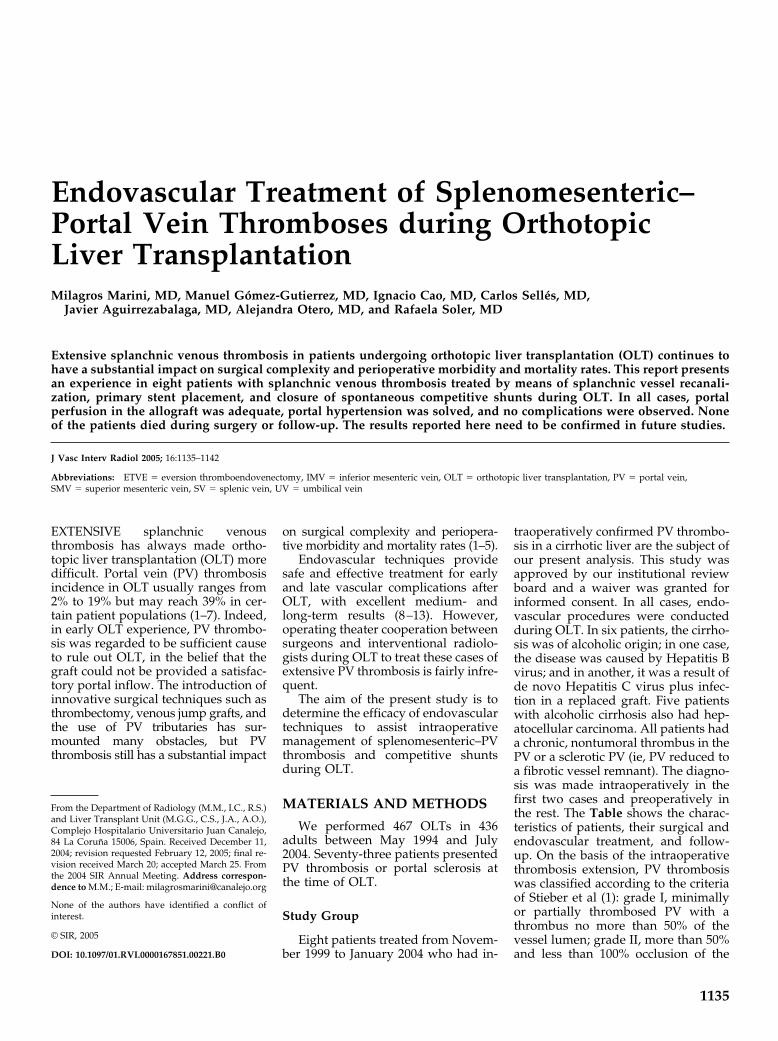
Figure 1. A pigtail catheter is advanced via umbilical donor vein to reach access to the splanchnic vessel system. Stenosis andobstructions resulting from incomplete surgical thrombus removal in the SMV and SV (arrowheads). (a) Enlarged coronary vein(arrows) and (c) preexisting spontaneous splenorenal shunts (arrows) are indicative of the steal phenomena generally associated withthis type of PV thrombosis (the arrows show the direction of the steal flow). (b,d) Stent (arrows) placed at the splenoportal union andcompetitive shunts closed with coils (arrowhead).
Marini et al • 1137Volume 16 Number 8
all stents and PVs remain patent andhave required no further surgery (Ta-ble). The duration of the endovascularprocedures was 45–90 minutes.
Four patients (patients 1, 2, 7, and8) had a grade IV PV thrombosis. Theyall presented incomplete thrombus re-moval in the recipient PV that ex-tended beyond the SMV and/or SVjunction. In two of these patients(cases 1 and 2), the occluded and par-tially recanalized areas were identifiedand the recipient splanchnic veinswere stent-implanted for connectionto the donor PV. A UV approach wasused, the proximal segment of the SVwas recanalized, and venoplasty wasperformed. Subsequently a 14-mm-wide, 30-mm-long Easy Wallstent(Boston Scientific) was placed betweenthe recipient SV and the recipient PVslightly downstream of the anastomo-sis. All competitive portosystemicshunts were identified and embolizedwith multiple coils (Fig 2). In one pa-tient (case 7), the SMV and the SV upto the IMV were found to be com-pletely thrombosed. The catheter wasinserted through an IMV tributary.The recipient SV and PV were recana-lized and a 14-mm-wide, 40-mm-longWallstent Uni was set in place aftervenoplasty. Patient 8 underwent mod-ified Sugiura surgery. A portogramobtained through an SMV tributary
showed a residual thrombus in the PV,as well as in the SV at the union be-tween the two veins and along a sub-stantial segment of the SMV, withhepatofugal flow in the left gastricvein. After venoplasty, a 14-mm-wide,40-mm-long Wallstent Uni (BostonScientific) was successfully placed be-tween the thrombosed segment of theSMV and the portal anastomosis. Graftperfusion improved considerably andsubsequent portographic analysisshowed that the enlarged left gastricvein collateral had disappeared (Fig3).
Four patients (patients 3–6) had agrade III PV thrombosis. In one patient(case 3), portography confirmed com-plete surgical removal of the thrombusin the recipient splanchnic veins, al-though previously formed competi-tive portosystemic shunts were alsoidentified and embolized with multi-ple 10–15-mm-diameter coils.
Patients 4 and 5 had sclerotic PVs.Their PVs were directly anastomosedto the SMV/SV confluence and had anative splenorenal shunt. The shuntswere embolized to improve portalflow and prevent steal at its expense.Because the control portogramsshowed moderate stenosis around theanastomosis and a residual gradient ofmore than 5 mm Hg, a 14-mm-wide,30-mm-long Easy Wallstent was in-
serted. No residual gradient was ob-served across the stent-implanted por-tal anastomosis in these patients (Fig4).
Preoperative CT revealed calcifica-tions in one patient (case 6) near theSMV/SV confluence. After ETEV, thethrombus was partially removed andan intimal dissection was seen in thesplenomesenteric vein junction. It wasclosed by means of two 14-mm-wide,40-mm-long Wallstent Uni stentsthrough the graft UV to the recipient’sSMV and PV.
DISCUSSION
The restoration of normal portalflow is essential to good liver graftfunction (1–5). In the beginning of thissurgical technique, OLT was dis-missed when the PV and/or any of itstributaries were found to havethrombi. Because the incidence of PVthrombosis may be as high as 39% (1–7), a number of different alternativesurgical procedures have been pro-posed to circumvent this difficulty.The first method developed consists ofvenous thrombectomy with a Fogartycatheter. One of the variations on thistechnique, ETEV, is still the mostcommonly used method in partial PVthrombosis. Alternative approachesinclude direct anastomosis from thedonor PV to the SV/SMV confluenceof the recipient or the use of an inter-positional graft involving the donoriliac vein when the SMV and SV arepatent (1). Currently, there is no con-sensus about the most suitable surgi-cal approach to treat PV thrombosisduring OLT. Despite these alterna-tives, the operative mortality rates re-main high (9.1%–42%) (1–7). The ma-jor risk is the recurrence of PVthrombosis after OLT as a result of theinvolvement of the splanchnic veinwalls and the reduction of the PV flowcaused by the extensive collateral cir-culation developing in the wake of PVthrombosis (1–5). Prognosis is poor inthe event of recurrent thrombosis ofthe PV, particularly in the early post-transplantation period. This condition,a risk to the graft and to patient sur-vival, may appear in as many as 28.5%of cases (2). Thrombectomy and re-transplantation have been the pre-ferred treatment in early posttrans-plantation PV thrombosis. However,both alternatives are associated with
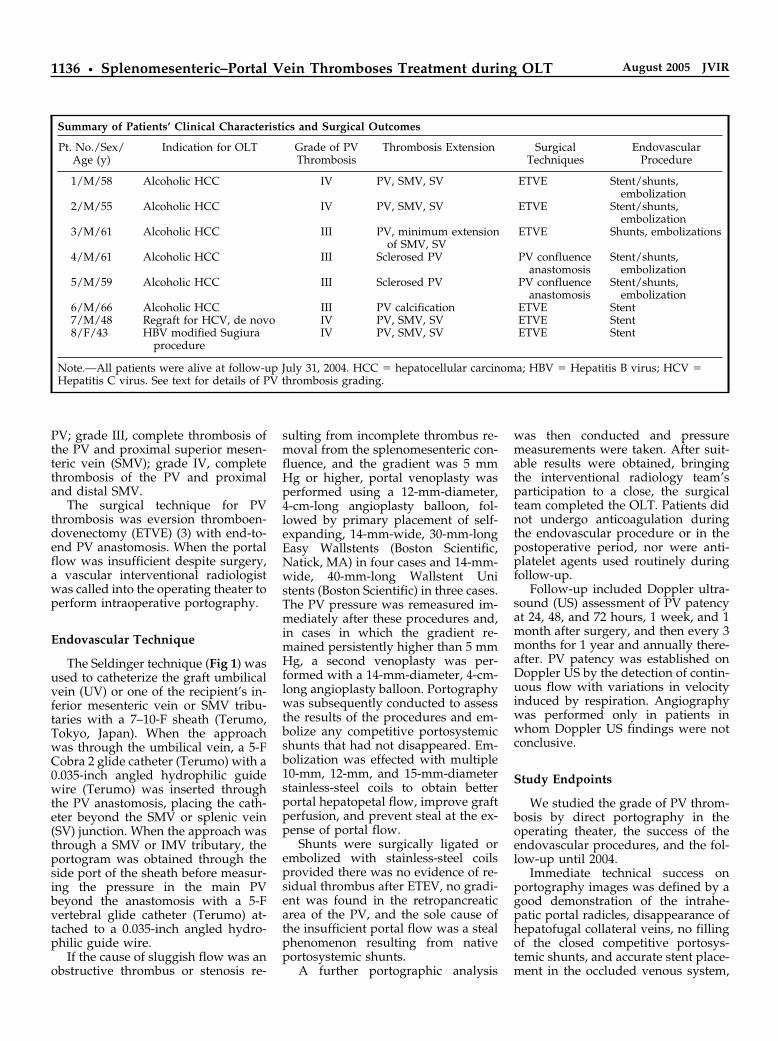
Figure 2. Image from patient 1, in whom chronic thrombosis in the splenomesentericjunction was treated with a 14-mm-wide, 30-mm-long Easy Wallstent (arrows) and coilclosure of competitive shunts (arrowheads) during OLT. PV phase of the celiac trunkarteriogram obtained 3 months later shows splenic and PV patency and complete occlu-sion of the splenorenal collaterals.
1138 • Splenomesenteric–Portal Vein Thromboses Treatment during OLT August 2005 JVIR
high rates of surgical morbidity andmortality (1–5). Patients at high riskwho are not considered for surgery areprecisely the group that benefits mostfrom the minimally invasive treat-ments developed in the past few years.They play a leading role in solvingsome PV complications in postopera-tive period and follow-up, thereby re-ducing morbidity and mortality. Thesetreatments include venoplasty, stent
placement, thrombolytic therapy, andembolization of portosystemic shunts(8–13).
Although experience with these ap-proaches is still limited, some authorshave reported effectiveness at medi-um- and long-term follow-up. Our ex-perience in treating postoperative vas-cular complications of OLT has beensimilarly promising. In light of thisand previous cooperation with the he-
patic surgery team in the operatingtheater, we decided to apply endovas-cular techniques during OLT.
For some authors, intraoperativeportography is a test performed rou-tinely in extensive splanchnic veinthrombosis to find a vessel to revascu-larize the liver graft, particularly if PVthrombosis is suspected before OLT ordiscovered during OLT. In such cases,portography is needed to evaluate the
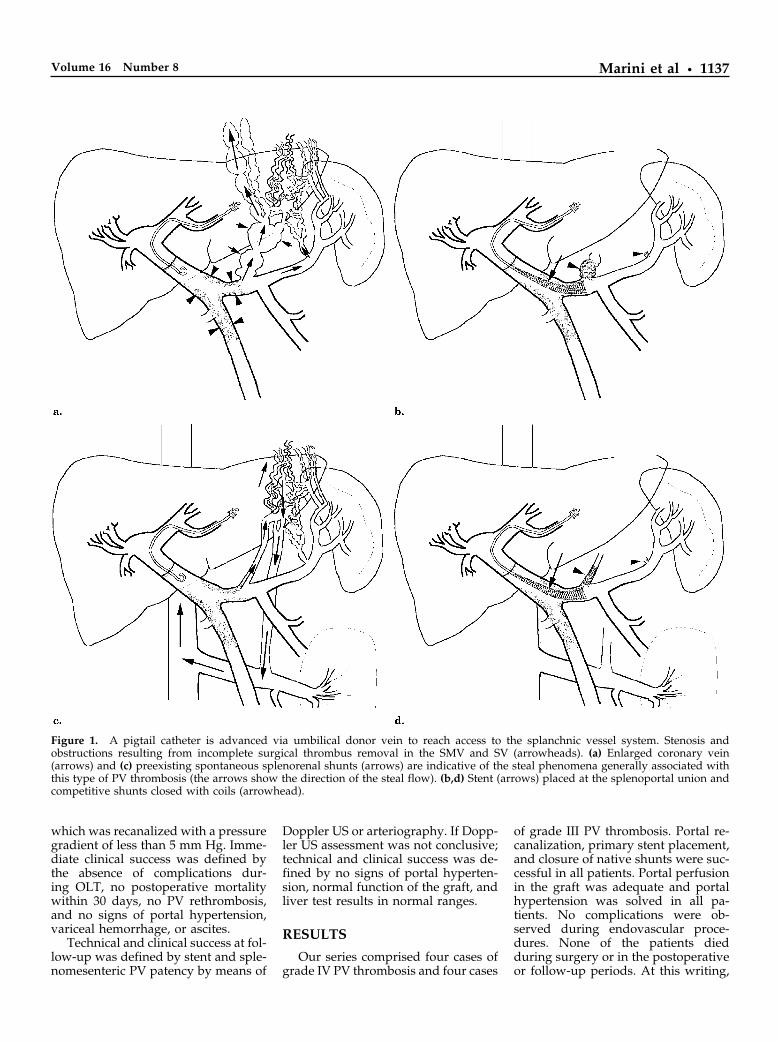
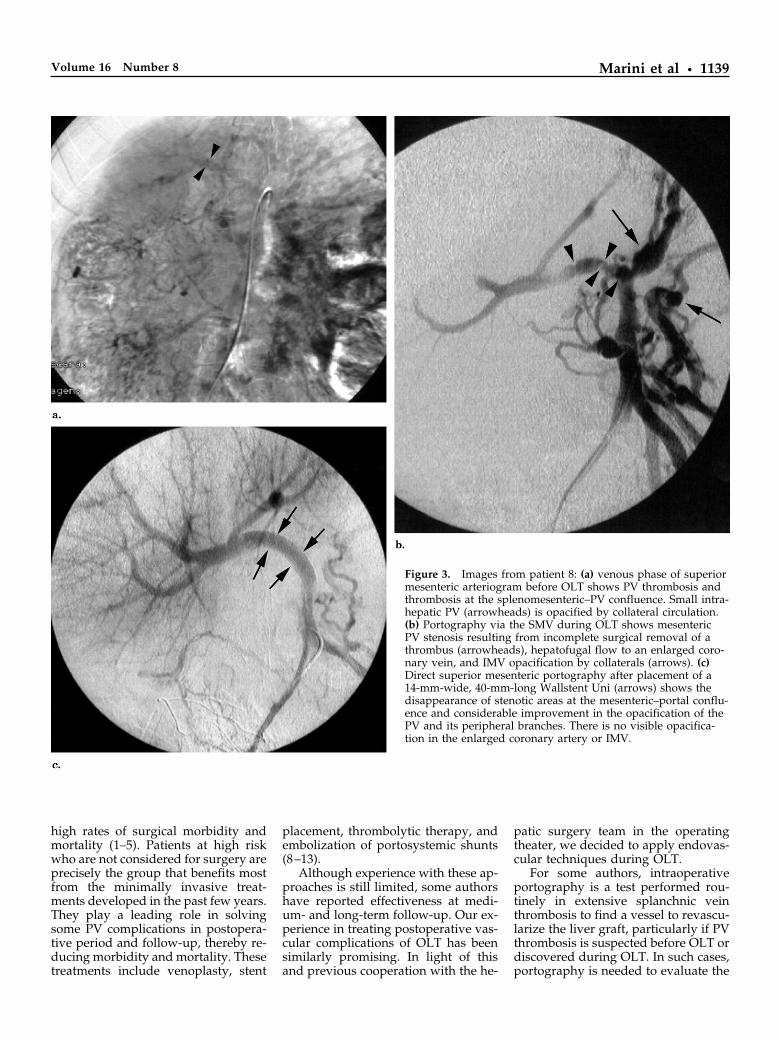
Figure 3. Images from patient 8: (a) venous phase of superiormesenteric arteriogram before OLT shows PV thrombosis andthrombosis at the splenomesenteric–PV confluence. Small intra-hepatic PV (arrowheads) is opacified by collateral circulation.(b) Portography via the SMV during OLT shows mesentericPV stenosis resulting from incomplete surgical removal of athrombus (arrowheads), hepatofugal flow to an enlarged coro-nary vein, and IMV opacification by collaterals (arrows). (c)Direct superior mesenteric portography after placement of a14-mm-wide, 40-mm-long Wallstent Uni (arrows) shows thedisappearance of stenotic areas at the mesenteric–portal conflu-ence and considerable improvement in the opacification of thePV and its peripheral branches. There is no visible opacifica-tion in the enlarged coronary artery or IMV.
Marini et al • 1139Volume 16 Number 8
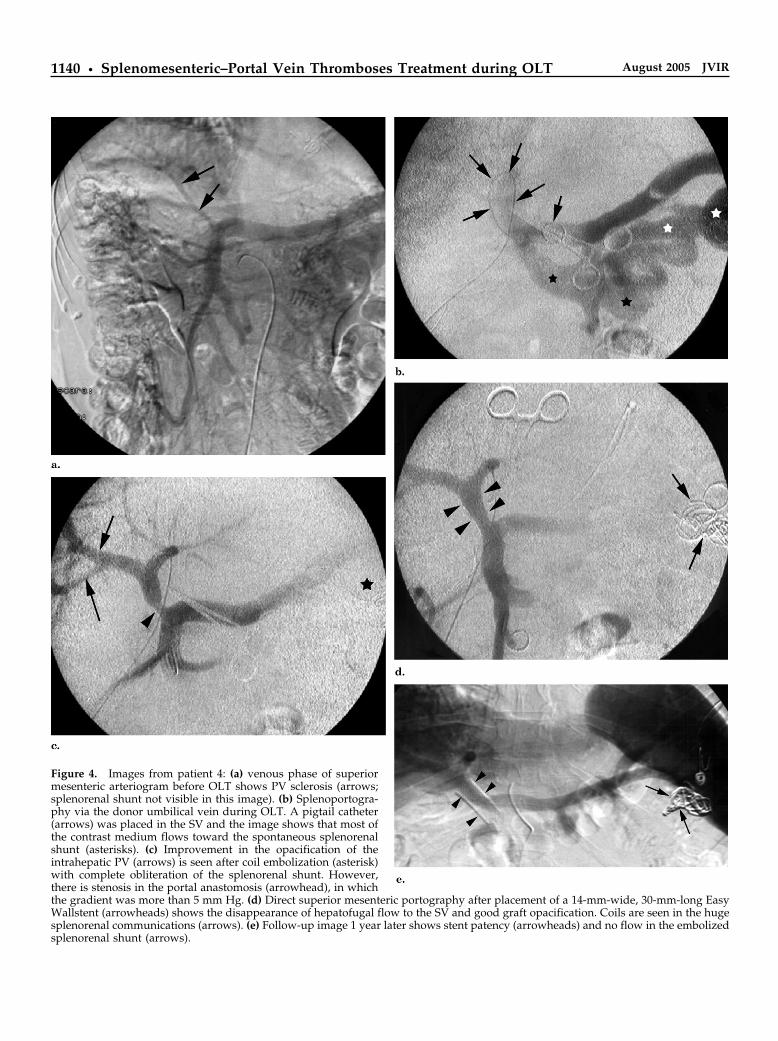
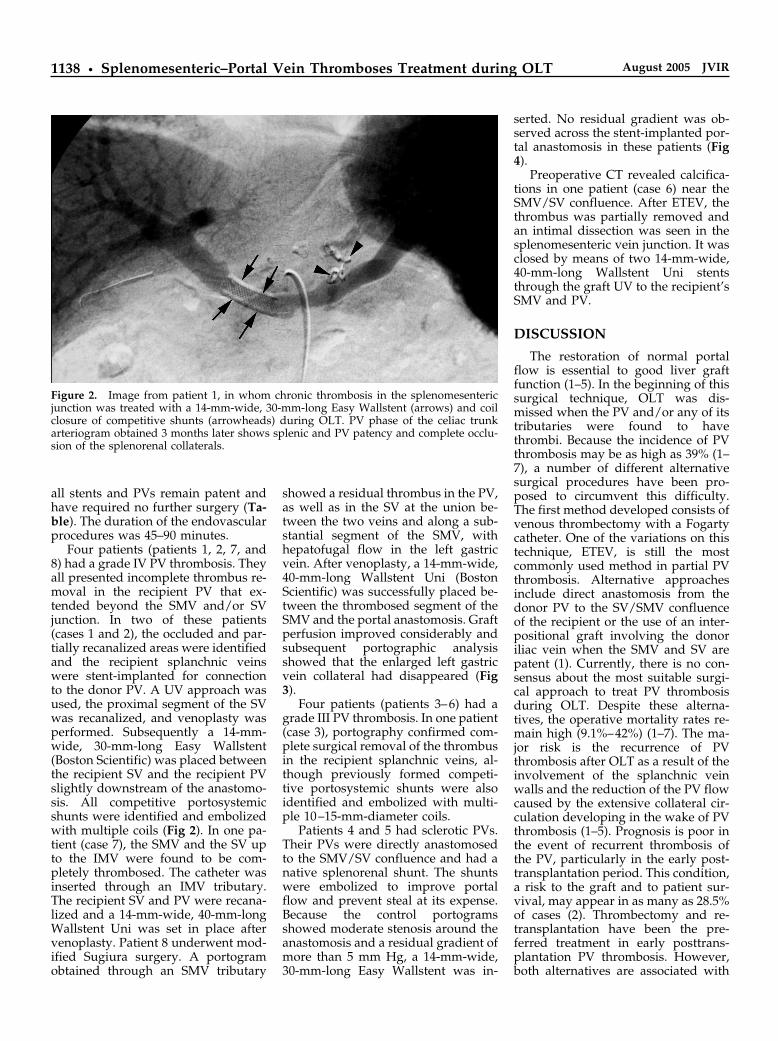
Figure 4. Images from patient 4: (a) venous phase of superiormesenteric arteriogram before OLT shows PV sclerosis (arrows;splenorenal shunt not visible in this image). (b) Splenoportogra-phy via the donor umbilical vein during OLT. A pigtail catheter(arrows) was placed in the SV and the image shows that most ofthe contrast medium flows toward the spontaneous splenorenalshunt (asterisks). (c) Improvement in the opacification of theintrahepatic PV (arrows) is seen after coil embolization (asterisk)with complete obliteration of the splenorenal shunt. However,there is stenosis in the portal anastomosis (arrowhead), in whichthe gradient was more than 5 mm Hg. (d) Direct superior mesenteric portography after placement of a 14-mm-wide, 30-mm-long EasyWallstent (arrowheads) shows the disappearance of hepatofugal flow to the SV and good graft opacification. Coils are seen in the hugesplenorenal communications (arrows). (e) Follow-up image 1 year later shows stent patency (arrowheads) and no flow in the embolizedsplenorenal shunt (arrows).
1140 • Splenomesenteric–Portal Vein Thromboses Treatment during OLT August 2005 JVIR

extent of the thrombosis and to moni-tor the results of thrombectomy aftervascular reconstruction. When a sig-nificant hepatofugal shunt is detected,the most prominent collateral vesselsmust be ligated to increase portal flow(1–5,14–16). Our portography proce-dures were performed by graft UVwhen possible because surgical re-opening of the UV is feasible in mostadult patients. Other reasons for thisapproach are that competitive porto-systemic shunts are easily embolizedand that, in the UV, the stent can beplaced under the anastomosis. This isparticularly advantageous when usingWallstents because the considerabledistal/proximal shortening to whichthese devices are subject is minimizedat this particular point. However, inpatients 7 and 8, the Wallstent wasfitted near the SMV or at the SV/IMVconfluence.
In all our cases, portographyproved to be very useful in helpingidentify PV thrombosis that had notbeen suspected preoperatively (pa-tients 1 and 2; Table). It should berecalled in this regard that PV throm-bosis may occur during the pretrans-plant waiting period after normal im-aging is conducted, and therefore itmay appear as an unexpected opera-tive finding. Intraoperative portogra-phy afforded precise identification ofoccluded and partially removedthrombi in the recipient portal system(patients 1, 2, 6–8), anastomotic dys-function (patients 4 and 5), and stealphenomena resulting from native por-tosystemic communications detectedbefore surgery (patients 1–5); finally,this technique was also very valuablein recognizing spontaneous competi-tive shunts, which are well-known po-tential causes of PV thrombosis andrecurrent thrombosis in the postoper-ative period.
Portal recanalization and recon-struction with endovascular stents arean effective radiologic procedure forthe treatment of symptomatic PV ab-normalities. In fact, portal stent im-plantation plays an important role inmaintaining PV patency when portalvenoplasty fails to correct PV obstruc-tion or stenosis subsequent to OLT (8–12). or living donor liver transplants(13,17). Primary and long-term fol-low-up patency in this series is opti-mal.
Metallic stents were used to re-
model a venous surface with throm-bus remaining. This might be one ofthe most controversial procedures inour methodology. Although predila-tion was performed in all patients andall responded to angioplasty, dilationtook place across chronically occludedvenous vessels and some of the pa-tients (patients 1, 2, 6–8) had alreadyundergone incomplete ETVE. To someauthors, this is a technique with a highrisk of recurrent thrombosis becauseETVE leaves a pathologic venous wall.In the event of significant PV throm-bosis, they recommend a venovenousbypass (4,16).
We prefer to use self-expandingWallstents in cases such as this. Theycover a vessel diameter range of 11–14mm, can be passively oversized, adaptvery well to vessel curvature and vari-able geometry, and have been exten-sively used in venous applications(18).
Another problem is that the long-term durability of metallic stents hasnot been clearly established. Few arti-cles have reported 4-year primary pa-tency (11,13). Two determining factorsin PV stent occlusion are liver disease(Child-Pugh class C) and/or obstruc-tion of the splanchnic veins (19,20). Allthe patients studied received a newliver graft; splanchnic vein obstructionand low flow were remedied andblood flow was improved by placingstents in the occluded venous seg-ments and embolizing any vessels in-volved in steal phenomena. This maybe the reason that a 100% primary pa-tency rate was attained after follow-up(mean, 25.6 months; range, 8–54months). Of all the patients discussed,patient 7 may be the one with theworst prognosis. This patient requireda repeat transplantation after a graftfailure as a result of an earlier PVthrombosis secondary to the recur-rence of Hepatitis C virus despite an-tiviral therapy. Therefore, the possibil-ity of a Hepatitis C virus relapsecannot be ruled out.
Finally, all competitive spontane-ous systemic shunts were embolizedbecause, for example, in patient 3, theonly cause of liver graft malfunctionand low portal flow was a competitivesplenorenal shunt, which stole all thePV flow from the liver graft. The sametechnique was applied to improveportal flow in patients 1, 2, 4, and 5.Most authors believe that spontaneous
competitive portosystemic shuntsshould be ligated during OLT to main-tain adequate portal flow, chieflywhen ETEV is performed (3,14,16,21).Competitive portosystemic shuntshave been reported as a cause of PVthrombosis or recurrent thrombosis inthe early postoperative period afterOLT (21–23). These patients were suc-cessfully treated with thrombolytictherapy and closure of competitiveshunts with coils.
In conclusion, stent placement insplenomesenteric–PV stenoses andclosure of competitive portosystemicshunts via endovascular techniquesduring OLT comprise an effective pro-cedure to resolve liver graft perfusionand portal hypertension caused bysplanchnic vein thrombosis and thesteal phenomenon. In complexsplanchnic vein thromboses, operatingtheater cooperation between surgeonsand interventional radiologists duringOLT introduces new lines of researchand enhances patients’ therapeutic op-tions. Although the primary durabilityof stents at medium- and long-termfollow-up has been very good, the re-sults reported here need to be con-firmed in future studies.
References1. Stieber AC, Zetti G, Todo S, et al. The
spectrum of portal vein thrombosis inliver transplantation. Ann Surg 1990;213:199–206.
2. Gonzalez EM, Garcia IG, Sanz RG, etal. Liver transplantation in patientswith thrombosis of the portal, splenicor superior mesenteric vein. Br J Surg1993; 80:81–85.
3. Lerut JP, Mazza D, Leeuw VV, et al.Adult liver transplantation and abnor-malities of splanchnic veins: experi-ence in 53 patients. Transpl Int 1997;10:125–132.
4. Yerdel MA, Gunson B, Mirza D, et al.Portal vein thrombosis in adults under-going liver transplantation: risk fac-tors, screening, management, and out-come. Transplantation 2000; 69:1873–1881.
5. Molmenti EP, Roodhouse TW, Mol-menti H, et al. Thrombendvenectomyfor organized portal vein thrombosis atthe time of liver transplantation. AnnSurg 2002; 235:292–296.
6. Okuda K, Ohnishi K, Kimura K, et al.Incidence of portal vein thrombosis inliver cirrhosis. an angiographic studyin 708 patients. Gastroenterology 1985;89:279–286.
7. Nonami T, Yokoyama I, Iwatsuki S, etal. The incidence of portal vein
Marini et al • 1141Volume 16 Number 8

thrombosis at liver transplantation.Hepatology 1992; 16:1195–1198.
8. Olcott EW, Ring EJ, Roberts JP, et al.Percutaneous transhepatic portal veinangioplasty and stent placement afterliver transplantation: early experience.J Vasc Interv Radiol 1990; 1:17–22.
9. Zajko AB, Sheng R, Bron K, Reyes J,Nour B, Tzakis A. Percutaneoustransluminal angioplasty of venousanastomotic stenoses complicatingliver transplantation: intermediate-term results. J Vasc Interv Radiol 1994;5:121–126.
10. McDaniel HM, Johnson M, PescovitzMD, et al. Intraoperative placementof a Wallstent for portal vein stenosisand thrombosis after liver transplanta-tion. Transplantation 1997; 63:607–608.
11. Cherukuri R, Haskal ZJ, Naji A, et al.Percutaneous thrombolysis and stentplacement for the treatment of portalvein thrombosis after liver transplanta-tion: long-term follow-up. Transplan-tation 1998; 65:1124–1126.
12. Bhattacharjya T, Olliff SP, Bhattachar-jya SH, et al. Percutaneous portalvein thrombosis and endovascularstent for management of posttrans-
plant portal venous conduit throm-bosis. Transplantation 2000; 69:2195–2198.
13. Funaki B, Jordan D, Rosenblum JD, etal. Percutaneous treatment of portalvenous stenosis in children an adoles-cents with segmental hepatic trans-plants: long-term results. Radiology2000; 215:147–151.
14. Manzanet G, Sanjuan F, Orbis P, et al.Liver transplantation in patients withportal vein thrombosis. Liver Transpl2001; 7:125–131.
15. Langnas AN, Marujo WC, Stratta RJ, etal. A selective approach to preexist-ing portal vein thrombosis in patientsundergoing liver transplantation. AmJ Surg 1992; 163:132–136.
16. Figueras J, Torras J, Rafeacas J, et al.Extra-anatomic venous graft for portalvein thrombosis in liver transplanta-tion. Transpl Int 1997; 10:407–408.
17. Lee SY, Koo GY, Gwon DY, et al. Liv-ing donor liver transplantation: com-plications in donors and interventionalmanagement. Radiology 2004; 230(2):443–449.
18. Sharafuddin MJ, Sun S, Hoballah JJ, etal. Endovascular management of ve-
nous thrombotic and occlusive dis-eases of the lower extremities. J VascInterv Radiol 2003; 14:405–423.
19. Stein Moni, Link Daniel P. Symptom-atic spleno-mesenteric-portal venousthrombosis: Recanalization and recon-struction with endovascular stents. JVasc Interv Radiol 1999; 10:363–371.
20. Koichiro Yamakado, Atsuhiro Nakat-suka, Naoshi Tanaka, et al. Malignantportal venous obstructions treated bystent placement: significant factors af-fecting patency. J Vasc Interv Radiol2001; 12:1407–1415.
21. Lyas S, Eid A, Jurim O. Coronaryvein “steal” and portal vein thrombosisafter orthotopic liver transplantation.Transplant Proc 2000; 32:702–703.
22. Durham JD, LaBerge JM, Altman S, etal. Portal vein thrombolysis and clo-sure of competitive shunts followingliver transplantation. J Vasc Interv Ra-diol 1994; 5:611–615.
23. Bilbao JI, Arias M, Herrero JI, et al.Percutaneous transhepatic treatment ofa posttransplant portal vein thrombo-sis and a preexisting spontaneous sple-norenal shunt. Cardiovasc InterventRadiol 1995; 18:323–326.
1142 • Splenomesenteric–Portal Vein Thromboses Treatment during OLT August 2005 JVIR





























