Embed Size (px)
DESCRIPTION
Endovascular Treatment of Peripheral Artery Disease in VA Healthcare System. Subhash Banerjee, MD, FACC, FSCAI Chief, Division of Cardiology VA North Texas Health Care System Dallas, TX. SCAI 2014, Las Vegas, AZ. Endovascular Interventions in Veterans Affairs Health Care System. - PowerPoint PPT Presentation
Citation preview

Endovascular Treatment of Peripheral Artery Disease in
VA Healthcare System
Subhash Banerjee, MD, FACC, FSCAIChief, Division of Cardiology
VA North Texas Health Care SystemDallas, TX
SCAI 2014, Las Vegas, AZ

Endovascular Interventions in Veterans Affairs Health Care System
Evolving trends in endovascular interventions: National trends VA trends
Patient outcomes: Medical therapy
Detection of PAD in Veteran population Dual anti-platelet therapy (DAPT)
Interventional therapies: Chronic total occlusions (CTO) Drug-coated balloons (DCB) & drug-coated stents (DCS) VA training programs
PAD research in the VA

Endovascular Interventions in Veterans Affairs Health Care System
Evolving trends in endovascular interventions: National trends VA trends
Patient outcomes: Medical therapy
Detection of PAD in Veteran population Dual anti-platelet therapy (DAPT)
Interventional therapies: Chronic total occlusions (CTO) Drug-coated balloons (DCB) & drug-coated stents (DCS) VA training programs
PAD research in the VA

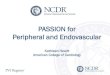
PAD: Endovascular Intervention, Surgery & Amputation Trends: 1996-2006
100
200
300
400
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Num
ber o
f pro
cedu
res /
100,
000
Med
icar
e be
nefic
iarie
s
YearsJ Vascular Surgery 2009; 50:54-60
Total endovascular interventionsRR=3.3; 95% CI 2.9-3.8
Major LE amputationRR=0.71; 95% CI 0.7-0.8
LE bypass surgeryRR=0.58; 95% CI 0.5-0.7
3x growth in endovascular interventions

PAD Endovascular Intervention Trends: 1996-2006
100
200
300
400
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Num
ber o
f pro
cedu
res /
100,
000
Med
icar
e be
nefic
iarie
s
Years
Total endovascular interventionsRR=3.3; 95% CI 2.9-3.8
AngioplastyRR=2.5; 95% CI 2.2-2.8
AtherectomyRR=43.1; 95% CI 34.8-52.0
J Vascular Surgery 2009; 50:54-60PAD: peripheral artery disease

PAD Operator Trends: 1996-2006
100
200
300
400
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Num
ber o
f pro
cedu
res /
100,
000
Med
icar
e be
nefic
iarie
s
YearsJ Vascular Surgery 2009; 50:54-60
CardiologistRR=2.5; 95% CI 2.2-2.8
Vascular surgeonRR=2.5; 95% CI 2.2-2.8
Interventional radiologistRR=2.5; 95% CI 2.2-2.8

Proportion of PAD Endovascular Intervention: 1996-2006
YearsJ Vascular Surgery 2009; 50:54-60
20
40
60
80
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Prop
ortio
n of
all
endo
vasc
ular
pro
cedu
res
100
Radiologists
Cardiologists
Vascular surgeons10%
40%23%
41%67%
19%

U.S. Market Report. Lifesciences Intelligence Inc. May 2014
U.S. PAD Trends: 2004-2013
2004 2008 20130
1
2
3
4
5
PVI (
mill
ion)
2004 2008 20130
0.5
1
1.5
2
2.5
USD
(bill
ion)
Number of Annual Procedures Estimated Annual Cost
3.23.6
4.3
0.91.3
2.0
Endovascular interventions ~1.5x coronary interventional volume Endovascular interventional market annual growth rate >8% Peripheral artery drug-coated stents (DCS): fastest growing sector CTO crossing device: third highest growth after DES and drug-coated balloons
PVI: peripheral vascular interventionsCTO: chronic total occlusionDCS & DES (drug-eluting stent) interchangeable

Complication Rates for Endovascular vs. Open Revascularization: 1998 vs. 2007
Egorova et al. J Vasc Surg. 2010
New York State inpatient and outpatient database1998 2007 pEndovascular revascularizationOperative mortality 2.4% 1.1% <0.05
Cardiac 1.6% 0.8% <0.0001
Stroke 0.2% 0.1% 0.04
Bleeding 9.9% 6.7% <0.0001
Infection 1.7% 1.3% 0.02
Open surgical revascularizationOperative mortality 3.9% 2.7% <0.05
Cardiac 3.0% 2.2% 0.0006
Stroke 0.4% 0.3% 0.03
Bleeding 14.3% 10.8% <0.0001
Infection 3.4% 3.8% 0.10
New York State inpatient and outpatient database

Diabetes Care 34:1157–1163, 2011
PAD Trends in Veterans: 2000-2004
VA inpatient and outpatient database82% increase in patients with established PAD diagnosis
Patie
nts
405,580
2000 20040
200000
400000
600000
800000 739,377
82% increase

Endovascular Interventions in Veterans Affairs Health Care System
Evolving trends in endovascular interventions: National trends VA trends
Patient outcomes: Medical therapy
Detection of PAD in Veteran population Dual anti-platelet therapy (DAPT)
Interventional therapies: Chronic total occlusions (CTO) Drug-coated balloons (DCB) & drug-coated stents (DCS) VA training programs
PAD research in the VA

Predictive Value of ABI in Patients with Established CAD (XLPAD® Registry)
Banerjee et al. Am J Cardiol. 2014 Apr 15;113(8):1280-4
ABI<0.9(58.4%)
ABI=0.9-1.4(38.7%)
ABI>1.4(2.9%)
Prevalence of Abnormal ABI in Patients with Stable CAD
ABI: ankle-brachial index, CAD: coronary artery disease, Normal ABI (>0.9 and <1.4), Abnormal ABI (<0.9 and >1.4)
n=679
www.xlpad.org

Predictive Value of ABI in Patients with Established CAD (XLPAD® Registry)
Banerjee et al. Am J Cardiol. 2014 Apr 15;113(8):1280-4
ABI: ankle-brachial index, CAD: coronary artery disease, Normal ABI (>0.9 and <1.4), Abnormal ABI (<0.9 and >1.4)
Freedom form Major Adverse Cardiovascular Events (MACE)
No DM, Normal ABIDM, Normal ABINo DM, Abnormal ABIDM, Abnormal ABI
No DM, Normal ABI (Reference group)
DM, Normal ABI (HR=1.7, 95% CI: 0.71-4.06, p=0.24)
No DM, Abnormal ABI (HR=2.03, 95% CI: 0.83-4.98, p=0.12)
DM, Abnormal ABI (HR4.85, 95% CI: 2.22-10.61, p=0.0001)

0.0
0.2
0.4
0.6
0.8
1.0
500 1000 1500 2000 2500 3000
Follow-up (days)
Surv
ival
pro
babi
lity
DiabeticsNon-diabeticsLog-rank, p-value <0.001
Kamlesh at al. Clin. Cardiol. 32, 8, 442–446 (2009)
Annual Mortality of Veterans with PAD:DM vs. Non-DM
VA inpatient and outpatient database-199833,629 patients with PAD; 9,474 (29%) with DM*
60-day mortality no different, Mortality significantly increased at 6m for DM
subjects (9.8% vs 8.4%, p<0.001) & continued to 8y
*VA Austin database

Statin Therapy & Limb Outcomes in Patients with PAD: (REACH Registry)
Series10
10
20
30
2221.1
14.7
18.2
3.8
26.225.1
18.2
21.7
5.6
On statin Not on statin
Worsening PAD
New amputationNew limb revascularization
Worsening claudication/ new CLI
Worsening PAD(competing risks)
%
Prior studies have documented improvements in walking distance & coronary revascularization This is the first study to demonstrate the impact of statins on adverse limb outcomes
Kumbhami et al. EHJ 2014
n=5,8614-year follow-up

Endovascular Revascularization & Supervised Exercise For Claudication (ERASE Trial)
Fakhry et al. AHA 2013 Late-breaking trial
1 month 6 month 12 month0
400
800
1200
1600
SETEVR+SET
Max
imum
wal
king
dist
ance
(m)
(n=106)
(n=106)
Endovascular revascularization plus supervised exercise therapy is associated with greater improvement in functional performance in patients with PAD
Multicenter Randomized Clinical Trial

0
25%
50%
75%
100%
50 100 150 200 250 300 350 400 450 500 550
ASA+Clopidogrel (n=426)
ASA+Placebo (n=425)
Overall: HR=0.98; 95% CI: 0.78-1.23)
Primary endpoint was significantly reduced by clopidogrel in prosthetic graft patients (HR=0.65; 95% CI: 0.45-0.95; p=0.025)
No significant difference in severe bleeding: clopidogrel+ASA=2.1% vs. ASA+placebo=1.2%
Prop
ortio
n ev
ent-f
ree
(%)
Belch et al. J Vasc. Surg. October 2010
CASPER Trial: DAPT After Peripheral Arterial Bypass Surgery
DAPT: Dual anti-platelet therapy

Major Adverse Event (MAE)-Free Survival with ≤3m or >3m of DAPT
p=0.0024
≤ 3 months DAPT (n=203)
> 3 months DAPT (n=131)
MAE
-free
Sur
viva
l
Months
≤3 months DAPT>3 months DAPT
0.55
0.68
Das S et al. SCAI Annual Mtng. 2014

Diabetes Care 34:1157–1163, 2011
Lower Extremity Amputation Trends Veterans with PAD: 2000-2004
VA inpatient and outpatient database82% increase in patients with established PAD diagnosis
2000 20040
2
4
6
8
Ampu
tatio
ns/1
000
patie
nts
7.08
4.65
34% decline

Endovascular Interventions in Veterans Affairs Health Care System
Evolving trends in endovascular interventions: National trends VA trends
Patient outcomes: Medical therapy
Detection of PAD in Veteran population Dual anti-platelet therapy (DAPT)
Interventional therapies: Chronic total occlusions (CTO) Drug-coated balloons (DCB) & drug-coated stents (DCS) VA training programs
PAD research in the VA

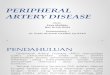
Crossing Peripheral CTO (XLPAD® Registry)
ABI: ankle-brachial index, CAD: coronary artery disease, Normal ABI (>0.9 and <1.4), Abnormal ABI (<0.9 and >1.4)
Proximal cap
Distal capDistal target
vessel
CTO body
Side branch
a b c
Figure: (a) Parts of a typical SFA CTO (b) Inability to direct the wire in a SFA CTO (c) Formation of a wire loop and passage advanced through the sub-intimal space. Arrow head indicates the width of the wire loop and the size of the potential sub-intimal space created
40-50% patients with
symptomatic PAD have a
peripheral artery CTO1
1Norgen et al. J Vasc Surg 2007; 45: S5-67

Peripheral Artery CTO: Surgery vs. PVI
Authors n Lesions Primary endpoint
PVI vs. Surgery Comments
Adam et al.1 452 Infrainguinal Amputation-free survival
71.0% vs. 68.0% (12m); p=ns
5y-multicenter randomized, CLI; no difference at 5y
Wolf et al.2
(VA CSP 199)263 Iliac &
infrainguinalClinicalpatency
64.1% vs. 68.1% (4y); p=ns
4y-multicenter randomized, claudication & CLI; no difference at 6y
McQuade et al.3 100 SFA CTO Clinical patency
72.0% vs. 66.0% (320d); p=ns
2y-single center, prospective, randomized; PTFE stent vs. PTFE bypass graft; no difference at 2y
1. Adam et al. Lancet 2005;366:1925–19342. Wolf et al. JVIR 1993;4:639-6483. McQuade et al. J Vasc Surg 2010;52:584-91
PVI: peripheral vascular intervention

Peripheral Artery CTO: Crossing StudiesFemoropopliteal Wire-catheter vs. Crossing Device Outcomes
Authors n Crossing strategy
Crossing success
Major Complications Comments
‘Wire catheter’
Van der Heijden et al.1 - ‘Wire catheter’ 60% Not reported Retrospective
Charalambous et al.4 76 ‘Wire catheter’ 65.8% Not reported Single arm, prospective
Pigott et al.11 88 ‘Wire catheter’ 4.5% 0% Multicenter, prospective
Banerjee et al.2 45 ‘Wire catheter’ 66% 4% COBRA trial: prospective, rand.
Dedicated CTO device
Banerjee et al.9 13 TruPath™ 77% 0% XLPAD registry
Charalambous et al.4 26 Frontrunner™ 88.1% 3.8% Single arm, prospective
Zeller et al.6 37 Enabler™ 86% 3% Single arm, prospective
Banerjee et al.10 58 VianceTM★ 87.9% 1.7% XLPAD registry
Massop et al.7 16 Frontrunner™ 65% 2.3% Single arm, prospective
Banerjee et al.5 17 CrossBoss™★ 100% 0% Retrospective
Staniloae et al.8 73 Crosser™ 87.7% 0% Single arm, prospective
Galassi et al.3 36 Crosser™ 76.7% 0% Prospective registry
Pigott et al.11 84 WildCat™ 89% 4.8% Multicenter, prospective1. Van der Heijden FH et al. Br J Surg 1993;80:959-63; 2. Banerjee S. et al. J Am Coll Cardiol 2012; 3. Galassi AR et al. J Invasive Cardiol 2011;23:359–362; 4. Charalambous N et al. Cardiovasc Intervent Radiol 2010;33:25-33; 5. Banerjee S et al. JEVT 2014; 6. Zeller T et al. JEVT 2012; 7. Mossop PJ et al. CCI 2006; 8. Staniloae CS et al. JIC 2011; 9. Banerjee et al. JEVT 2014; 10. Banerjee et al. JIC 2014 (accepted); 11. Pigott et al. J Vasc Surg. 2012. ★CrossBossTM is the same device as VianceTM

Peripheral Artery CTO: Stent Studies
Authors n Stent type12m
Primary patency
Mean lesion length Comments
‘Nitinol Self-expanding StentsHong et al.1 150 EverFlexTM 77.0% 226mm Single arm, retrospective
Lagana et al.2 52 Multiple 76.9% Not reported Single arm, retrospective
Lagana et al.3 93 Multiple 69.2% 255mm Single arm, retrospective
Dosluoglu et al.4 45 SmartTM 69.0% Not reported Single arm, retrospective
Banerjee et al.5 45 Multiple 53% 190mm Multicenter randomized
Covered StentsLepantalo et al.6 23 ThrupassTM 48% 160mm Multicenter randomized (terminated)
Farraj et al.6 32 ViabahnTM 86% 154mm Single arm, prospective
Drug-coated stentsBosiers et al.8 135 Zilver PTX 77.6% 226mm Single arm, prospective
1. Hong et al. JEVT 2013;20:782–791 ; 2. Lagana et al. Radiol Med 2011;116:444–453; 3. Lagana et al. Radiol Med 2008; 113:567-577; 4. Dosluoglu et al. J Vasc Surg 2008;48:1166–1174; 5. Banerjee et al. J Am Coll Cardio 2012; 60(15): 1352-1359; 6. Lepantalo et al. Eur J Vasc Endovasc Surg 2009;37:578–584; 7. Farraj et al. J Invasive Cardiol. 2009 Jun;21(6):278-81; 8. Boisiers et al. J Cardiovas Surg 2013;54(1):115-22

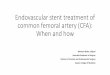
Crossing Peripheral CTO (VA Cooperative Trial; VA CSP 598)
Flowchart of the proposed study design.SFA = superficial femoral artery; CTO = chronic total occlusion; IVUS = intravascular ultrasound; BMS= bare metal Nitinol self-expanding stents; DES= drug-eluting Nitinol self-expanding stents; R = randomization; m = month; FU = follow-up; R1= first randomization based on either use of wire-catheter or dedicated crossing device; R2= second randomization to either drug-coated or bare Nitinol self-expanding stents; ABI= ankle-brachial index
Banerjee et al. VA CSP LOI, 2012

Femoropopliteal Stent: Randomized Trials
1 2 3 40
10
20
30
40
50
60
70
FAST1 Schilinger Angio2 Schilinger DUS2 RESILIENT3
31.7 38.6
p=0.38
24.0 43.0
p=0.05
25.0 45.0
p=0.06
18.7 63.3
p<0.001
Rest
enos
is (%
)
Stent PTA
n=123 n=121 n=51 n=53 n=51 n=53 n=134 n=72
12m 6m 6m 12m
Low –Intermediate complexity patients (~30% DM) & lesions (Mean=69.6 mm)
1. Circulation. 2007 Jul 17;116(3):285-92 2. N Engl J Med 2006; 354:1879-1888 3. Circulation: CV Interventions.2010; 3: 267-276

*Compared to reference group
Cumulative Hazard of Restenosis (CTO vs. Non-CTO SFA Lesions)With Bare-Metal Stent Post-dilation Strategies
Cum
ulat
ive
haza
rd o
f re
sten
osis
Time (in days)
Conventional CTOConventional non-CTOCryoplasty CTOCryoplasty non-CTO
Reference Group
HR=2.65, 95% CI 0.72 – 9.80; p=0.15*
HR=2.69, 95% CI 0.74 – 9.85; p=0.13*
HR=3.61, 95% CI 0.99 –13.18; p=0.05*
Peripheral Artery CTO: Treatment Strategy
Banerjee et al. J Am Coll Cardio 2012; 60(15): 1352-1359

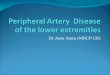
Peripheral Drug Coated StentZilver PTX (Paclitaxel) Trial: Design
Femoro-popliteal lesions (n=508)
PTAn=251
DESn=247
Optimal PTA Failed PTAn=126
DESn=68
BMSn=68
479 patients with Rutherford category ≥ 2 PAD symptomsUp to 2 lesions per SFA
Primary effectiveness end point:primary patency at 12 months. defined by DUS or angio
“As prespecified, acute PTA failure was counted as a loss of patency for the primary effectiveness end point.”
Dake et al. Circ. Interv. Oct. 2011
Lesion length = 64.8 mmCTO = 27.2%
89.9%* 73.0%
32.8% 83.1%*
PTA: balloon angioplasty; DES: drug-eluting stent; BMS: bare metal stent; *p≤0.01

Peripheral Drug Coated Stents
Trial Control Inclusion Criteria
Drug/ Dose (µg/mm2)
Follow-Up (months)
Restenosis* vs. Control
Zilver PTXN=479 PTA & BMS Femoropopliteal
stenosis Paclitaxel/3.0 24 19% vs. 37%
SIROCCOn=93 BMS Femoropopliteal
stenosis Sirolimus/0.9 24 23% vs. 21%
PARADISEn=106 N/A BTK stenosis Paclitaxel/1.4 27 12%
Yukon-BTKn=161 BMS BTK stenosis Sirolimus 24 19% vs. 44%
STRIDESn=104 N/A Femoropopliteal
stenosisEverolimus/
2.25 12 32%
DESTINYn=140 BMS BTK stenosis Everolimus/
2.25 12 21% vs. 47%
Karan Sarode, David Spelber et al. JACCI 2014 (accepted manuscript)

Peripheral Drug Coated Balloons
Trial Study Inclusion Criteria
Balloon/Dose(µg/mm2)
Follow-Up
(months)
Restenosis* vs. Control
THUNDERn=154
DCB vs. PTA vs. PTA + Paclitaxel
in contrast
Femoropopliteal stenosis
Paclitaxel-iopromide/3.0 48 17% vs. 44% vs.
54%
FemPacn=87 DCB vs. PTA Femoropopliteal
stenosisPaclitaxel-
iopromide/3.018 7% vs. 17%
LEVANT In=101 DCB vs. PTA Femoropopliteal
stenosis
Paclitaxel-polysorbate/sorbitol/2.0
6 28% vs. 51%
PACIFIERn=91 DCB vs. PTA Femoropopliteal
stenosis Paclitaxel-urea/3.0 12 7% vs. 35%
LEVANT 2n = 476 DCB vs. PTA Femoropopliteal
stenosis
Paclitaxel-polysorbate/sorbitol/2.0
6
7.7% vs. 17.3%
DEBATE-BTKn=132 DCB vs. PTA Diabetes, BTK
stenosis Paclitaxel-urea/3.0 12 27% vs. 74%
DEBATE SFAn = 110
DCB + BNS vs. PTA + BNS
Femoropopliteal stenosis Paclitaxel-urea/3.0 12 17.0% vs. 47.3%
Karan Sarode, David Spelber et al. JACCI 2014 (accepted manuscript)

Endovascular Interventions in Veterans Affairs Health Care System
Evolving trends in endovascular interventions: National trends VA trends
Patient outcomes: Medical therapy
Detection of PAD in Veteran population Dual anti-platelet therapy (DAPT)
Interventional therapies: Chronic total occlusions (CTO) Drug-coated balloons (DCB) & drug-coated stents (DCS) VA training programs
PAD research in the VA

VA Peripheral Artery Disease Research: 191 studies 2001-2014
VA Trials ClinicalTrials.gov Identifier Year
Center for the Study of Vascular Disease in Hispanic and Native Americans NCT00018590 2001
Does the Reduction of Total Body Iron Storage (TBIS) Alter Mortality in a Population of Patients With Advanced PVD? (FeAST) NCT00032357 2002
Markers and Mechanisms of Vascular Disease in Type II Diabetes NCT00256646 2005
Low-Dose Opiate Therapy for Discomfort in Dementia (L-DOT) NCT00385684 2006
Study Comparing Two Methods of Expanding Stents Placed in Legs of Diabetics With Peripheral Vascular Disease (COBRA) NCT00827853 2009
Remote Ischemic Preconditioning Prior to Vascular Surgery (CRIPES) NCT01558596 2012
Micropuncture vs. Standard Common Femoral Artery Access NCT02026180 2013
www.clinicaltrials.gov

Veteran Affairs Research Programs
VA Research and Quality Improvement ProgramsVA Cooperative Studies Program (CSP): planning and conduct of large multicenter clinical trials and epidemiological studiesResearch on Health Disparities and Minority Health: research addressing the challenges posed by minority health care needs and the disparities that arise in healthcare delivery, access, and qualityMillion Veteran Program (MVP): Data collected from MVP will be stored anonymously for research on diseases like diabetes and cancer, and military-related illnessesResearch Equipment Quick Use Initiative Program (REQUIP): REQUIP is responsible for redistribution of quality, excess, nonexpendable research equipmentVA Technology Transfer Program: The mission of the VA Technology Transfer Program (TTP) is to serve the American public by translating the results of worthy discoveries made by employees of VA into practiceVA Specimen Research and Biobanking Program: The VA Specimen Research and Biobanking Program makes tissue samples available for research on illnesses in Veterans
www.research.va.gov

Endovascular Interventions in Veterans Affairs Health Care System
Period of rapid growth in endovascular interventions: Prospective trials to establish the impact of ABI
screening in asymptomatic individuals & in patients with established CAD
Medical interventions in PAD Statin & DAPT interventions
Endovascular interventions in PAD Refinement of CTO treatment DCB and DCS trials
Growing role of VA sponsored clinical trials & databases

Acknowledgements Emmanouil S. Brilakis, MD,
PhD Clark Gregg, MD John Rumsfeld, MD Joseph Hill, MD, PhD Anand Prasad, MD Nicolas Shammas, MD Osvaldo S. Gigliotti, MD Mazen Abu Fadel, MD Tayo Addo, MD Mirza Shadman Baig, MD Michael Luna, MD Dharam Kumbhani, MD Andrew Klein, MD Jeffry Hastings, MD Gerold Grodin, MD
Bernadette Speiser, RN Shuaib Abdullah, MD Joseph Garcia, MD Knyugen Kytai, PhD Xu Hao, PhD Atif Mohammad MD Preeti Kamath, BDS Michele Lytal, RN Evaster Bennett, LVN Puja Garg, PhD Swagata Das, MBBS Karan Sarode, BS Gene Pershwitz, MD David Spelber, MD Salil Sethi, MD
Pooja Banerjee, MD Bertis Little, PhD Rick Weideman, PharmD Kevin Kelly, PharmD Cheryl Webb-Singh Donald Haagan, RVT Teresa Jeong, RN Susan Droughty, RN Lauren Makke, RVT Dwaine William Omar Hadidi, MD Rahul Thomas, MD OUR PATIENTS