Embed Size (px)
Citation preview

Eur J Vasc Endovasc Surg 19, 489–495 (2000)
doi:10.1053/ejvs.1999.1050, available online at http://www.idealibrary.com on
Endovascular Treatment of Penetrating Thoracic Outlet Arterial Injuries
D. F. du Toit∗1, D. C. Strauss1, M. Blaszczyk2, R. de Villiers2 and B. L. Warren1
Departments of 1Surgery and 2Diagnostic Radiology, Tygerberg Hospital and the University of Stellenbosch,Tygerberg, South Africa
Objectives: to establish the feasibility of stent-graft treatment of penetrating thoracic outlet arterial injuries.Design: prospective study.Materials and methods: forty-one patients with penetrating injuries to the carotid, subclavian and proximal axillaryarteries admitted between August 1998 and May 1999 were studied. Patients requiring urgent surgical exploration foractive bleeding (n=26) were excluded. Remaining patients underwent arteriography to assess suitability for stent-graftplacement. After successful stent-graft treatment clinical and sonographic follow-up were done at 1 month and thereafter3-monthly.Results: of the 15 patients considered, 10 patients qualified for stentgraft treatment (seven male, three female, mean age27 years). The vessels involved were subclavian artery (seven), carotid artery (two) and axillary artery (one). Seven hadarteriovenous fistulae and three, pseudoaneurysms. Stent-graft treatment was successful in all 10 patients with noprocedure-related complications. On mean follow-up of 7 months no complications were encountered.Conclusion: endovascular treatment shows promise as a treatment modality for thoracic outlet arterial injuries. Long-term follow-up is required for comparison to the results of standard surgical repair.
Key Words: Thoracic outlet; Penetrating arterial injury; Endovascular; Stent graft.
Introduction humans.7 Since then, rapid improvement of endo-
vascular techniques and graft technology have led to
Injuries to arteries of the thoracic outlet constitute wide application of this treatment method. Several
investigators have reported applications in vascular5–10% of arterial trauma.1 Due to inaccessibility and
extensive dissection to achieve control, attempts to trauma.8–11
The inaccessibility of arteries of the thoracic outlettreat these lesions often end in exsanguination and
death. Reported morbidity and mortality rates range makes stent-graft treatment of injuries to these vessels
particularly attractive. The stable patient with afrom 5–30%.2 Surgical exposures that are used to
achieve control include supra- and infraclavicular dis- pseudoaneurysm or an arteriovenous fistula seems to
be the ideal candidate to treat in this way. This reportsection, clavicular transection, thoracotomy and me-
dian sternotomy.3 This major dissection contributes describes the experience of a single trauma unit with
stent-graft treatment of arterial pseudoaneurysms andsignificantly to the high morbidity when treating these
injuries. Concomitant injuries might render these arteriovenous fistulae of the thoracic outlet.
patients a high risk for general anesthetic and open
surgery.
In 1964, Charles Dotter described the first an-Patients and Methods
gioplasty4 and in 1969 reported the first stent graft used
in a canine popliteal artery.5 These reports initiated theDuring a 10-month period from August 1998 to May
era of modern endovascular therapy. The use of stents1999, all patients with injuries of the carotid, subclavian
in humans was first reported in 1987.6 In 1990 Juanand proximal axillary artery were considered for endo-
Parodi and colleagues were the first to use stent graftsvascular management. Patients requiring urgent sur-
for the treatment of abdominal aortic aneurysms ingical exploration for active bleeding or acute occlusion
were excluded. Remaining patients underwent ar-∗ Please address all correspondence to: D. F. du Toit, Department
teriography to assess their suitability for stent-graftof Surgery, University of Stellenbosch, PO Box 19063, Tygerberg7505, South Africa. placement.
1078–5884/00/040489+07 $35.00/0 2000 Harcourt Publishers Ltd.

D. F. du Toit et al.490
This was performed in the operating suite with both ation criteria were graft patency, limb loss, thea vascular surgeon and interventional radiologist in presence or absence of other complications, andattendance. Facilities were available for immediate death.conversion to open repair if necessary. Routine pre-
procedural heparin (50 units/kg) and prophylactic
cefazolin were given and continued for 24 hours.ResultsTransfemoral arterial access was gained under local
anaesthetic. Anatomical location of lesions and prox-
imal and distal vessel diameter were determined with During the study period a total of 41 patients with
routine angiography. A final decision regarding stent- thoracic outlet arterial injury were seen. Twenty-sixgraft treatment was then taken with inability to tra- required urgent open surgery for active bleeding orverse the lesion by guidewire and large proximal/ acute occlusion. The remaining 15 patients were evalu-distal lumen discrepancy representing exclusion cri- ated for stent-graft treatment. All were haemo-teria for stent-graft placement. dynamically stable and underwent angiography. Five
The stent graft used was the Hemobahn endo- were excluded due to inability to traverse the lesionvascular prosthesis (W. L. Gore). It consists of a self- with a guidewire (n=4) or too large a proximal/distalexpanding nitinol stent with a thin expanded poly- lumen discrepancy (n=1).tetrafluoroethylene (ePTFE) inner lining. It was avail- Ten patients (seven male, three female) with a meanable in different lengths and sizes (6–10 mm diameter) age of 27 years (range 18–40 years) were consideredwith an introducer sheath 1 French bigger than the suitable for stent-graft placement (Table 1). Ninedeployed stent diameter in millimetres. The delivery injuries were the result of stab wounds and one wascatheter length (110 cm) makes it possible to reach the a gunshot wound. Three lesions were arteriovenouscervicothoracic vessels via a femoral puncture. fistulae, three were false aneurysms and four patients
Exact proximal and distal lumen diameter meas- had both a false aneurysm and an arteriovenousurements were used to choose the right size stent. fistula. The vessels involved were subclavian arteryMeasurements were made on precalibrated computer- (seven), carotid artery (two) and axillary artery (one).generated digital subtraction angiography images. Subclavian artery sidebranches that were embolisedThe proximal diameter was oversized 1–1.5 mm and
were thyrocervical trunks (three), internal mammarythe lesion overlapped with at least 1 cm at both
arteries (three) and vertebral arteries (four). Fourends. To prevent endoleak formation, all arterial
patients had associated pathology with two haemo-branches that could participate in complex lesions,
thoraces and two brachial plexus injuries. Durationespecially arteriovenous fistulae of the subclavian
between injury and presentation varied from 24 h tovessels, were embolised liberally before stent de-
more than 2 years. The mean duration of the pro-ployment. To avoid neurological complications, ver-
cedure was 123 min (range: 77 min–179 min) (Tabletebral artery cross-flow was checked angiographically
1).before embolisation.
Stent-graft treatment was ultimately successful inWith the guidewire traversing the lesion, the stent
all 10 patients. Success was defined as complete ex-graft was introduced through a femoral introducer
clusion of the lesion with no endoleaks, as confirmedsheath and advanced under fluoroscopic guidance toby completion angiography. No deaths, limb loss oroverlap the injury. Initially, image masking (road-procedure-related complications were encounteredmapping) and bony landmarks were used to positionand no conversion to open repair was necessary. Twothe stent graft, but later replaced by localisation underpatients required a second stent to exclude endoleaksangiographic control using a contralateral trans-caused by incorrect positioning of the first stent notfemoral catheter. The stent graft was then deployed,overlapping the lesion.seated by balloon dilatation, and a routine completion
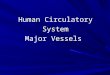
Careful perioperative neurological observationsangiogram was obtained.were done in patients with carotid artery lesions andAngiographic examples of the above procedures forall patients who needed vertebral artery embolisation.a right common carotid arteriovenous fistula, a leftNone of these patients experienced any neurologicalsubclavian arteriovenous fistula and a left subclaviansigns or symptoms. All patients were dischargedpseudoaneurysm can be seen in Figures 1–3.within 24 h after the procedure.All data were collected prospectively from time
On mean follow-up of 7 months (range 6–10of admission. Immediate postoperative evaluationmonths), no evaluable patient had clinical or sono-was followed up by clinical and sonographic evalu-
ation after 1 month and thereafter 3-monthly. Evalu- graphic evidence of graft stenoses or occlusion. No
Eur J Vasc Endovasc Surg Vol 19, May 2000

Endovascular Treatment of Thoracic Outlet Injuries 491
(a)(b)
(c)
Fig. 1. Treatment of an arteriovenous fistula between the right common carotid artery and the brachiocephalic vein. (a) Initial aortogramvia the transfemoral catheter; (b) selective common carotid arteriogram demonstrating the fistula; (c) completion arteriogram showingexclusion of the arteriovenous fistula.
Eur J Vasc Endovasc Surg Vol 19, May 2000

D. F. du Toit et al.492
(b)(a)
(c)
tality for axillary/subclavian artery injury ranges from
3% to 33%.1 The average mortality associated with
carotid artery injury is 17%, ranging from 6.6% to
33%.12,13 Even in the elective setting, achievement of
surgical exposure may require a sternotomy, thora-
cotomy or clavicular transection with substantial sur-
gical morbidity and blood loss.1 This is the group of
trauma patients thought most likely to benefit from
stent-graft treatment.
(d)
Fig. 2. Treatment of an arteriovenous fistula between the artery and vein. (a) Selective left subclavian arteriogram demonstrating thefistula; (b) coil embolisation of subclavian artery branches; (c) stent graft before deployment; (d) complete exclusion of lesion afterdeployment.
neurological or upper-limb symptoms due to em-
bolisation or progressive ischaemia were encountered.
Two patients were lost to follow-up.
Discussion
Arterial injuries of the thoracic outlet present a chal-
lenge even to the experienced surgeon. Reported mor-
Eur J Vasc Endovasc Surg Vol 19, May 2000

Endovascular Treatment of Thoracic Outlet Injuries 493
(b)(a)
Fig. 3. Treatment of a pseudoaneurysm of the left subclavian artery. (a) Selective left subclavian artery arteriogram demonstrating thepseudoaneurysm; (b) complete exclusion of the lesion after stent-graft deployment.
Table 1. Patients, pathology and procedure duration.
Sex/ Mechanism Pathology Vessel/s Associated Duration injury to Duration ofage of injury involved injuries procedure (days) procedure
(minutes)
M 20 GSW AVF L SCA/L BCV Left haemothorax 3 119M 30 STAB AVF R CCA/R BCV None 1 77M 30 STAB AVF L CCA/L IJV None 4 91F 21 STAB PA+AVF R SCA/R BCV None 17 130M 35 STAB PA+AVF L SCA/L SCV None 25 179F 28 STAB PA L SCA Brachial plexus injury 730 85F 18 STAB PA+AVF L SCA/L SCV None 2 145M 40 STAB PA+AVF L AXA/L AXV Brachial plexus injury 28 153M 19 STAB PA L SCA None 4 135M 21 STAB PA L SCA Left haemothorax 4 115
PA=pseudoaneurysm; AVF=arteriovenous fistula; SCA=subclavian artery; AXA=axillary artery; CCA=common carotid artery; BCV=brachiocephalic vein; IJV=int. jugular vein; SCV=subclavian vein; AXV=axillary vein.
All the patients treated in this series presented with routine angiography. Completing the patient’s treat-
ment during angiography makes excellent economicestablished false aneurysms or arteriovenous fistule.
If left untreated, these lesions can enlarge and present and medical sense. Not only is extensive surgery
avoided, but also prolonged hospital stay. If long-termwith numerous complications, such as pressure effects,
erosion of adjacent organs and rupture in the pleural results of stent-graft treatment can be demonstrated
to be comparable to the standard surgical approach,cavity or extravasation into soft tissue. Thrombosis or
distal embolisation can lead to upper limb or cerebro- it might replace open repair as method of choice for
treating these selected lesions.vascular ischaemic incidents. In the case of arterio-
venous fistulae, additional problems of venous The success of stent-graft treatment for traumatic
lesions depends to a great extent on patient selection.hypertension, ulceration and high-output cardiac
failure can add to the long-term morbidity and Patients have to be haemodynamically stable and it
must be possible to traverse the lesion by guidewire.mortality.
Stent-graft treatment of arterial injuries has been To avoid endoleaks with this technique, the proximal–
distal lumen discrepancy must not be too large. Thisreported since 19918 with good short- and medium-
term results.10,11 Patients treated in these series were becomes a problem with time as the distal vessel
becomes small and atrophic. Attempted stent place-mostly haemodynamically stable and able to undergo
Eur J Vasc Endovasc Surg Vol 19, May 2000

D. F. du Toit et al.494
ment in this situation can lead to either a proximal goal is easier with arterial stent-graft treatment than
with standard surgical repair as no periarterial dis-endoleak or distal oversizing to the extent of vessel
rupture. These lesions are probably best excluded from section is required. Postoperative arm-swelling was
minimised and all involved veins were patent onstent-graft treatment. If the lumen discrepancy is not
a problem, the stent should still be oversized by 1 follow-up Doppler studies.
The need for covered stents in the treatment ofmillimetre (relative to proximal vessel diameter) to
achieve a tight seal. pseudoaneurysms has been questioned by reports of
successful treatment with non-covered stents16,17 andAnother reason for endoleaks is side-branch in-
volvement. In false aneurysms, as in abdominal aortic the adjunct use of endovascular coil placement.18 Even
arteriovenous fistulae have been treated with non-aneurysm repair, most might seal off, but in arterio-
venous fistulae even small branches might maintain covered stents in the experimental setting with reason-
able results.19 Despite these reports a well-designedthe lesion and eventually return it to its original size.
This is particularly true of the subclavian artery, where covered stent seems to be the logical choice for
endovascular treatment of these lesions.numerous sizeable branches might be involved in the
injury and participate in the lesion. To avoid endoleaks Potential disadvantages of stent-graft repair are
early thromboembolic events, late stenosis and oc-in this location, we believe that all side-branches which
potentially participate must be embolised before stent- clusion caused by neointimal hyperplasia.16 These are
well-known complications of uncovered stenting foring.
Contralateral vertebral artery patency and flow occlusive disease, with late re-stenosis rates of 4.3 to
6.5% for iliac20 and 15 to 30% for coronary arteryshould be confirmed before embolisation. Endoleaks
can also develop when the lesion is not overlapped at stents.21 The results of carotid artery stents for stenotic
disease have been promising, with preliminary re-both ends by at least 1 cm. To achieve this accurate
deployment we now favour fluoroscopic guidance stenosis rates of less than 5%.22 Other authors have
been less enthusiastic, reporting total stroke and deathwith a second contralateral femoral catheter. We be-
lieve that by adhering to these principles endoleaks, rates ten times higher in carotid stenting than with
endarterectomy.23 These neurological complicationsas reported by Reber et al.,14 can be prevented.
One advantage of stent-graft use in trauma is the were the result of perioperative embolic events and
the results of potential long-term re-stenosis were notoption of approaching the lesion from an anatomical
site unaffected by injury. The graft used in our series taken into account. In trauma cases, predominantly
young patients with healthy vessels are treated, andmade it possible to deliver the stent via a femoral
puncture under local anaesthetic. With the low-profile with short-term follow-up no symptomatic stenosis
or occlusions have been reported due to neointimalintroducer sheath (only 1-F bigger than the diameter
in millimetres of the deployed stent) percutaneous hyperplasia.10,11 Parodi et al.28 reported one stenosis
and three occlusions with long-term follow-up. Nonepuncture without cutdown was possible. The small
introducer sheath and larger artery minimises the risk of these were symptomatic and they included one
internal carotid stent graft. Our early results are alsoof arterial injury at the delivery site, as reported by
others.10 promising, but long-term follow-up is necessary to
resolve this issue. If stenosis occurs it should be rel-ePTFE-covered stents in trauma raise the old con-
troversy of potential septic complications. The extent atively easy to treat with redilatation or deployment
of another stent. Identifying a failing stent graft in theof most of the lesions treated would, however, have
generally required surgical grafting rather than prim- trauma patient might not be that easy, as compliance
with respect to follow-up is generally poor (two of 10ary repair. In this location, availability and size will
lead in most cases to the use of ePTFE grafts, which patients in this study were lost to follow-up). This
could lead to late presentation with irreversiblehave proved their reliability in the trauma setting.15
Graft kinking or fracture, especially in the subclavian cerebral or upper-limb ischaemia.
The potential occurrence of thromboembolism dur-artery, where shoulder movement causes compression
between the first rib and the clavicle, has been re- ing or after stent deployment, especially in the carotid
artery, is also a cause of concern. Some pseudo-ported11 and remains a potential long-term com-
plication. aneurysms and arteriovenous fistulae can contain lu-
minal clot that might embolise, but no cases have beenWhen repairing arteriovenous fistulae it is advisable
to try to preserve patency of the involved veins rather recorded in numerous reports, although individually
small in patient numbers.16,24,25than resorting to ligation. This restricts long-term com-
plications of venous hypertension.26,27 Achieving this In summary, early results of endovascular treatment
Eur J Vasc Endovasc Surg Vol 19, May 2000

Endovascular Treatment of Thoracic Outlet Injuries 495
13 Ramadan F, Ruthledge R, Oller D et al. Carotid artery trauma:of selected patients with traumatic thoracic outlet ar-A review of contemporary trauma center experiences. J Vasc
terial injuries suggest it to be an effective, minimally Surg 1995; 21: 46–56.14 Reber PU, Patel AG, Do DD, Kniemyeyer HW. Surgical im-invasive and safe method of treatment. Although this
plications of failed endovascular therapy for post traumaticearly experience is encouraging, long-term follow-upfemoral arteriovenous fistula repair. J Trauma 1999; 46: 352–354.
of larger numbers is required for comparison to the 15 Feliciano DV, Mattox KI, Graham JM, Bitondo CG. Five-year experience with PTFE grafts in vascular wounds. J Traumaresults of standard surgical repair.1985; 25: 71–83.
16 Mase M, Banno T, Yamada K, Katano H. Endovascular stentplacement for multiple aneurysms of the extracranial internalcarotid artery: technical case report. Neurosurgery 1995; 37: 832–835.References
17 Duke B, Ryu R, Coldwell D, Brega KE. Treatment of bluntinjury to the carotid artery by using endovascular stents: an
1 Hyre CE, Cikrit DF, Lalka SG, Sawchuk AP, Dalsing MC. early experience. J Neurosurg 1997; 87: 825–829.Aggressive management of vascular injuries of the thoracic 18 Babatasi G, Massetti M, Le Page O, Theron J, Khayat A.outlet. J Vasc Surg 1998; 27: 880–885. Endovascular treatment of a traumatic subclavian artery an-
2 Flint LM, Snyder WH, Perry MO, Shires GT. Management of eurysm. J Trauma 1998; 44: 545–547.major vascular injuries in the base of the neck. Arch Surg 1973; 19 Geremia G, Bakon M, Brennecke L, Haklin M. Experimental106: 407–413. arteriovenous fistulas: treatment with porous metallic stents. Am
3 Henry AK. Extensile Exposure, 2nd edition. Edinburgh: Churchill J Neuroradiol 1995; 16: 1965–1973.Livingstone, 1973: 44–58. 20 Vorwerk D, Gunther RW. Stent placement in iliac arterial
4 Dotter CT, Judkins MP. Transluminal treatment of arterio- lesions. Three years of clinical experience with the wallstent.sclerotic obstruction. Description of a new technique and a Cardiovasc Intervent Radiol 1992; 15: 285–290.preliminary report of its application. Circulation 1964; 30: 654–670. 21 Serruys PW, Strauss BH, Beat KJ et al. Angiographic follow-
5 Dotter CT. Transluminally-placed coilspring endarterial tube up after placement of a self-expanding coronary artery stent. Ngrafts: long-term patency in canine popliteal artery. Invest Radiol Engl J Med 1991; 324: 13–17.1969; 4: 329–332. 22 Roubin GS, Yadav S, Iyer SS, Vitek J. Carotid stent supported
6 Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. angioplasty: neurovascular intervention to prevent stroke. Am JIntravascular stents to prevent occlusion and re-stenosis after Cardiol 1996; 78: 8–12.transluminal angioplasty. N Engl J Med 1987; 316: 701–706. 23 Jordan WD, Voellinger DC, Fisher WS, Redden D, McDowell
7 Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal HA. A comparison of carotid angioplasty with stenting versusgraft implantation for abdominal aortic aneurysms. Ann Vasc endarterectomy with regional anesthesia. J Vasc Surg 1998; 28:Surg 1991; 5: 491–499. 397–403.
8 Volodos NL, Karpovich IP, Troyan VI et al. Clinical experience 24 Shames MI, Davis JW, Evans AJ. Endoluminal stent placementof the use of self-fixing synthetic prosthesis for remote endo- for the treatment of traumatic carotid artery pseudoaneurysm:prosthetic of the thoracic and the abdominal aorta and iliac case report and review of the literature. J Trauma 1999; 46:arteries through the femoral artery and as intra operative endo- 724–726.prosthesis for aorta reconstruction. Vasa Suppl 1991; 33: 93–95. 25 Ruebben A, Merlo M, Verri A et al. Exclusion of an internal
9 May J, White G, Waugh R, Weiyun YU, Harris JE. Transluminal carotid aneurysm by a covered stent. J Cardiovasc Surg 1997; 38:placement of a prosthetic graft-stent device for treatment of 301–303.subclavian artery aneurysm. J Vasc Surg 1993; 18: 1056–1059. 26 Hughes CW, Jahnke EJ Jr. The surgery of traumatic arterio-
venous fistulas and aneurysms, a five-year followup study of10 Marin ML, Veith FJ, Panetta TF et al. Transluminally placed215 lesions. Ann Surg 1958; 148: 790–797.endovascular stented graft repair for arterial trauma. J Vasc Surg
27 Rich NM, Hughes CW, Baugh JH. Management of venous1994; 20: 466–473.injuries. Ann Surg 1970; 171: 724–730.11 Patel AV, Marin ML, Veith FJ, Kerr A, Sanchez LA. Endo-
28 Parodi JC, Schonholz C, Ferreira LM, Bergan J. Endovascularvascular graft repair of penetrating subclavian artery injuries. Jstent-graft treatment of traumatic arterial lesions. Ann Vasc SurgEndovasc Surg 1996; 3: 382–388.1999; 13: 121–129.12 Asensio JA, Valenciano CP, Falcone RE, Grosh JD. Man-
agement of penetrating neck injuries. The controversy sur-rounding Zone II injuries. Surg Clin North Am 1991; 71: 267–296. Accepted 14 December 1999
Eur J Vasc Endovasc Surg Vol 19, May 2000