Embed Size (px)
Citation preview

Endovascular Embolization of Varicoceles:Resorption of Tungsten Coils in the SpermaticVeinJames Barrett, Irving Wells, Richard Riordan, Carl Roobottom
Department of Radiology, Derriford Hospital, Plymouth, Devon PL6 8DH, UK
AbstractPurpose:To investigate whether resorption of tungsten coilsoccurs in patients with varicoceles treated by endovascularembolization of the spermatic vein.Methods:Patients who had previously had varicocele embo-lization were requested by letter to attend the radiologydepartment. Blood levels of tungsten were compared with agroup of controls. Fluoroscopic images of the coils weretaken and compared with those obtained during the originalprocedures.Results:Nineteen patients attended, whose procedure hadbeen done 19–57 months previously (mean 40 months).Blood levels of tungsten were raised in 18 patients comparedwith the controls. Radiographic evidence of loss of substanceof the coils was seen in four patients.Conclusion:Tungsten coil resorption occurs in varicoceleembolization. In view of the unknown long-term effects ofraised blood tungsten levels and the availability of alterna-tive embolization agents, we feel that it is unwise to persistin the use of tungsten coils in this application.
Key words: Varicocele—Vein, spermatic—Therapeuticblockage—Interventional procedure, complication—Tung-sten
Percutaneous embolization of the spermatic vein offers acost-effective and minimally invasive method of treatmentfor varicocele. The outcome of embolization has been shownto compare favorably with both traditional surgical methodsand newer laparoscopic surgery, but with a lower incidenceof complications [1]. In our department we have used coilembolization as the first line of treatment for varicocele forthe last 15 years, and during the last 5 years have usedtungsten coils (Spirale tungsten coil, Balt, Montmorency,France). A recent report has highlighted resorption of tung-
sten coils associated with loss of function and elevation ofblood tungsten levels in the context of intracerebral aneu-rysm and dural fistula embolization [2]. As a result of thisconcern we performed a study to determine whether resorp-tion of the coil occurred in the spermatic vein and whether ornot there was any associated elevation of serum tungstenlevels.
Materials and MethodsEthics approval for the study was obtained. The radiology computerwas used to identify those patients who had undergone endovascu-lar embolization of the spermatic vein with tungsten coils. Thesecoils were first used in December 1994. Thirty-one patients wereidentified who had had technically successful spermatic vein em-bolization with tungsten coils in the period up to February 1998. Ofthese, one patient had subsequently died, one patient had previouslyhad Gianturco coil embolization (and was excluded in view ofpotential interaction) and four patients were from outside the re-gion. Therefore, 25 patients were selected.
An abdominal fluoroscopic image was acquired using a PhilipsIntegris C2000 image intensifier (Philips, Eindhoven, The Nether-lands) (the same as was used to perform the embolization, with thesame kV and automatic exposure parameters). The present fluoro-scopic images were compared with representative images of thecoils obtained during the procedures by two readers independently(I.W., C.R.), and a qualitative assessment of morphologic changewas made.
A whole blood sample was collected in lithium heparin vacu-tainers and analyzed for tungsten levels using an inductively cou-pled mass spectrometer. This was performed at the EnvironmentalSciences department of Plymouth University. The lower limit ofdetection was 0.2 ng/ml. Accuracy was determined using a spiking/recovery method (a known quantity of tungsten mixed with blood),which produced a recovery of greater than 95% at a tungstenconcentration of 1 ng/ml. The blood levels of tungsten in thepatients were compared with those in a normal population ofvolunteers.
The patients were asked to comment on the outcome of theembolization.Correspondence to:J.A. Barrett, BSc, MBBS, MRCP
CardioVascularand InterventionalRadiology
© Springer-Verlag New York, Inc. 2000 Cardiovasc Intervent Radiol (2000) 23:457–459DOI: 10.1007/s002700010104

ResultsTwenty-five patients were sent letters and 19 patients at-tended. The embolization had been performed between 57and 19 months previously (mean 40 months). The averageage of the patients who attended was 37.7 years; the averageage of the initial cohort was 35.6 years.
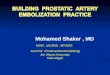
The readers concurred that there was a significant de-crease in substance of the coils, as determined by a decreasein width of the tungsten wire, in four patients (Fig. 1). In afurther patient, one reader felt there was equivocal changeand the other no change. This reduction in substance wasonly seen in patients who had had their procedure performedat least 43 months previously (n 5 9).
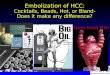
The blood results revealed an increase in the tungstenlevels in 18 patients compared with a population of controls(13 volunteers) (Fig. 2). Statistical analysis was performedon the means of the log data using the nonparametric Mann–Whitney test for medians, which revealed a significant dif-ference (p , 0.0001). Nocorrelation was obtained betweenthe length of time the coils had been in situ and the tungstenlevels in the blood (Fig. 3).
On questioning the patients, there were 15 whose symp-toms responded to the treatment. There were no cases of latefailure.
DiscussionThis study supports the previous report [2], in that there wasresorption of the tungsten coils and elevation of blood tung-sten levels. However, the clinical significance of this has to
be evaluated in terms of recurrence of the varicocele andtoxicity of the tungsten.
A finding of note on repeated imaging of the coils wastheir retraction (decrease in lateral volume of the loops: Fig.1). Histologic examination of tungsten coils in animal mod-els has shown a combination of thrombus organization and
Fig. 2. Blood tungsten levels in patients and controls.
Fig. 1. A Image obtained during the embolization procedure. B Image of the same patient 57 months later. Two observationswere made. Firstly, there has been a reduction in substance of the coil as shown by the decrease in width of the tungsten wire.Secondly, there has been retraction of the coil as shown by the decrease in the lateral volume of the loops.
458 J. Barrett et al.: Tungsten Coil Resorption in Varicocele Embolization

fibrous tissue reaction around the coil [3]. If this is the casein the spermatic vein, as evidenced by the coil retraction,then the loss of coil substance will not necessarily lead torecanalization. The absence of late failure in our groupwould support this. This contrasts with the treatment ofneurovascular disease, where resorption is associated withrecanalization [2].
The mechanism of resorption of the tungsten coils isincompletely understood. It is suggested that it may be due tothe mechanical percussion by the systolic-diastolic flow onthe spirals (especially in the high-flow setting of intracranialvascular malformations). This is not possible with the ab-sence of flow in the thrombosed spermatic vein. Resorptionof the coils has also occurred in the venous drainage of atreated dural fistula [2] and research in rabbits has shown thatthe metal could be found in the adventitia of the vessel walland in phagocytic cells, fibroblasts, and spindle cells wellremoved from the coil [4]. Resorption is therefore likely tooccur in any vessel, independent of flow characteristics. Thefact that radiographically detectable resorption occurs laterin the spermatic vein than the cerebral arteries may relate tothe absence of flow.
Tungsten is found in trace amounts in the human body.However, its biological effects are incompletely understoodand it has not been shown to be an essential element in plantsor animals [5]. No normal range or toxic levels in blood arereadily available. Previous studies have used either a pool of“regular” patients [4] or unexposed individuals [6]. Modelsof acute exposure in the human, extrapolated from animal
studies, suggest that the majority of the tungsten is excretedrapidly in urine and feces [7]. There is only one case reportof acute tungsten toxicity from oral ingestion causing comaand acute renal failure [8]. The blood concentrations werevery high in this case (5 mg/ml).
Animal models suggest that chronic exposure to tungstenwould result in accumulation in the skeleton, liver, kidneys,and spleen [7]. Hypersensitivity pneumonitis, lung fibrosis,and dermatitis have been shown to occur in hard metalworkers chronically exposed to tungsten carbide and cobalt,but it is felt that the presence of cobalt is necessary for thisinjury to occur [9]. Tungsten has been found in the urine,toenails, and hair of workers exposed to the metal [10], butno complications due to long-term exposure are described.There has been no report of toxicity resulting from endovas-cular intervention as yet, but the long-term effects are un-known.
We have demonstrated that resorption of tungsten coilsoccurs in varicocele embolization. This has not been asso-ciated with clinical recurrence. Although there is no evi-dence of toxicity and no loss of efficacy in this study, we feelthat it is unwise to persist in the use of tungsten coils in thisapplication as the long-term effects are unknown and goodalternative embolization agents exist.
Acknowledgment.The authors wish to thank Dr. Andy Fisher at PlymouthUniversity for measuring the blood tungsten levels.
References1. Wells IP (1995) Embolization of varicoceles. Curr Opin Urol 5:82–842. Weill A, Ducross V, Cognard C, Piotin M, Moret J (1998) “Corrosion”
of tungsten spirals: A disturbing finding. Interv Neuroradiol 4:337–3403. Reul J, Weis J, Spretzger U, Konert T, Thron A (1997) Long-term
angiographic and histopathic findings in experimental aneurysms of thecarotid bifurcation embolized with platinum and tungsten coils. Am JNeuroradiol 18:35–42
4. Ruel J (1998) “Corrosion of tungsten spirals” by Weill et al. IntervNeuroradiol 4:341–342
5. Kazantzis G (1986) Tungsten. In: Freiberg F, Nordberg GP, Vouk V(eds) Handbook of Toxicology of Metals, 2nd edn. Elsevier Science,Amsterdam, pp 610–622
6. Wester PO (1973) Trace elements in serum and urine from hypertensivepatients before and during treatment with chlorthalidone. Acta MedScand 194:505–512
7. Leggett RW (1997) A model of the distribution and retention oftungsten in the human body. Sci Tot Environ 206:147–165
8. Marquet P, Franc¸ois B, Vignon P, Lachaˆtre G (1996) A soldier who hadseizures after drinking a quarter of a litre of wine. Lancet 348:1070–1071
9. Cugell D (1992) The hard metal diseases. Clin Chest Med 13:269–27910. Nicolaou G, Pietra R, Sabbioni E, Mosconi G, Cassina G, Seghizzi P
(1987) Multielement determination of metals in biological specimens ofhard metal workers: A study carried out by neutron activation analysis.J Trace Elem Electrolyte Health Dis 1:73–77
Fig. 3. Blood tungsten levels against time elapsed sinceembolization.
J. Barrett et al.: Tungsten Coil Resorption in Varicocele Embolization 459







![Metastatic Spermatic Cord Tumor From Colorectal Cancer...A spermatic cord tumor is unusual, and, in particular, a metastatic tumor of the spermatic cord is very rare [1, 2]. The primary](https://img.pdfslide.us/doc/110x75/60f81a86b8201957b46aac37/metastatic-spermatic-cord-tumor-from-colorectal-cancer-a-spermatic-cord-tumor.jpg)