Embed Size (px)
Citation preview

Endovascular Electrocoagulation: Concept, Technique, andExperimental Results
Cheng Ji, Guido Guglielmi, and Hank Chen
PURPOSE: To evaluate the safety and efficacy of an embolotherapeutic technique that useselectrolytically detachable platinum coils and radio frequency (RF) energy to achieve rapid anddistal occlusion of targeted vessels. METHODS: In swine, branches of the ascending cervical arteryand the hepatic artery measuring 1.5 mm or less were subjected to endovascular electrocoagula-tion. RF energy was delivered through modified Guglielmi detachable platinum coils that wereplaced in the targeted arteries. Ohmic heating generated by RF caused vessel occlusion. After thevessel occlusions were confirmed angiographically, the platinum microcoils were electrolyticallydetached from the delivery wire and left in the vessels as implants. RESULTS: All vessels wererapidly and superselectively occluded by endovascular electrocoagulation. Following use of theappropriate methods derived from this research, we did not observe rupture of the artery, dissectionof the artery, unintended occlusion, or migration of the platinum microcoil. Histologic examinationof treated vessels at 6 and 12 weeks revealed obliteration of the vessel lumen by the platinummicrocoil surrounded by granulation tissue. CONCLUSION: Endovascular electrocoagulation is arapid method of achieving vessel occlusion. It may be a useful and controllable embolotherapeutictechnique when expeditious occlusion of small vessels and distal superselectivity are desired.
Index terms: Animal studies; Arteries, therapeutic blockade; Interventional instuments, coils
AJNR Am J Neuroradiol 18:1669–1678, October 1997
In the past few decades, embolotherapy hasbecome an indispensable tool of interventionalneuroradiology. Many different materials areused to occlude vascular lesions via the endo-vascular route, including polyvinyl alcohol,steel and platinum coils, cyanoacrylate, and de-tachable balloons. However, reflux or migrationof these embolic materials cannot always beavoided, and none of these embolic agents hasproved to be ideal when distal, controlled, su-perselective, or rapid occlusion of small vesselsis desired.
In search of a rapid and effective method ofembolization, a few investigators turned to the
Received November 21, 1996; accepted after revision April 24, 1997.Supported by NIH grant 5 R01 HL46286–04.From the Leo G. Rigler Center for Radiological Research, University of
California at Los Angeles Medical School.Address reprint requests to Cheng Ji, MD, Leo G. Rigler Center for
Radiological Research, Department of Radiological Sciences, University ofCalifornia Medical Center, Los Angeles, CA 90095.
AJNR 18:1669–1678, Oct 1997 0195-6108/97/1809–1669
© American Society of Neuroradiology
166
phenomenon of electrocoagulation (1–6). Elec-trocoagulation was discovered at the turn of thecentury by researchers who observed that whensufficient electricity was passed through biolog-ical tissue, heat was produced (7). When thisheat reached a critical temperature, proteinsdenatured and formed a material called coagu-lum. The phenomenon of coagulum formationcaused by electrical energy was termed electro-coagulation. It was also observed that alternat-ing current of greater than 10 000 cycles persecond (10 kHz) at moderate levels did notproduce significant pain or generalized musclecontraction in the human body (1, 7). Currentabove this cycling rate was known as radio fre-quency (RF). By applying RF energy to an areajust proximal to the aperture of a bleeding ves-sel, surgeons have long been using electroco-agulation to achieve hemostasis and vessel oc-clusion quickly, safely, and effectively. Heatenergy generated from RF causes vessel occlu-sion by the following mechanisms: desiccationof the vessel wall leading to shrinkage and re-traction of the vessel; coagulation of blood pro-
9

1670 JI AJNR: 18, October 1997
teins resulting in the formation of an occlusivecoagulum; and induction of thrombosis follow-ing vessel wall injuries (8).
It was the rapidity and the efficacy of surgicalelectrocoagulation that prompted the investiga-tors to explore its use for achieving vessel oc-clusion via the endovascular route (1–6). Viacatheters, a guidewire serving as an electrodewas positioned in the targeted vessel and RFenergy was delivered through the guidewire.The results were disappointing; many investiga-tors reported vessel rupture and/or unsatisfac-tory occlusion rates (1, 2, 5). It is believed thatthese failures were due to either application ofexcess energy or removal of the adherentguidewire after electrocoagulation. During elec-trocoagulation, thermal energy causes vesselwalls and blood proteins to become adherent tothe guidewire. At this point, the blood vessel isoccluded by the shrinkage of the vessel wall, thecoagulum, and the physical presence of theguidewire. Continued application of RF energyto the targeted vessel beyond this point willoverheat the vessel wall and cause it to rupture.Even if application of excess energy is avoided,the subsequent withdrawal of the adherentguidewire removes the occlusive coagulum,which leads to recanalization or to tearing of thevessel wall, which leads to rupture. Unlike withsurgical electrocoagulation, in which the sur-geon can see the vessel, these investigatorscould not know when the vessel was occludedand when to turn off the power.
In the early 1990s, the platinum Guglielmidetachable coil (GDC) system became avail-able for clinical use. The GDC can be detachedat will from the delivery wire, by electrolysis,and left in place as an implant. GDCs, which areformed by many centimeters of looped plati-num coil, are used primarily for brain aneu-rysms (9). A shorter (0.4 to 1 cm), crescent-shaped version of the GDC can be used for theendovascular occlusion of small feeders of ar-teriovenous malformations, fistulas, and hyper-vascular tumors (G. Guglielmi, “Controlled Dis-tal Occlusion of Anterior Choroidal and AnteriorSpinal Artery Feeders of AVMs Using Detach-able Coils,” presented at the annual meeting ofthe American Society of Neuroradiology, Wash-ington, DC, June 1991). This coil is controllablebeyond the tip of the microcatheter and can besteered and then detached into the targeted ves-sel. Complete occlusion of each vessel, how-ever, requires dense mechanical filling of the
vascular lumen, often with multiple parallelcoils, and can be time-consuming to such anextent as to become impractical. As a result,chances of incomplete occlusion or recanaliza-tion may become significant.
To enhance the efficacy and rapidity of thetechnique of distal, selective, and controllableocclusion of small vessels, it was decided tocombine the technique of electrocoagulationwith GDC technology. The aim was to achievefrom the inside of the vessel what in surgery isdone from the outside of the vessel: instanta-neous occlusion of blood vessels by electroco-agulation.
This study was undertaken to evaluate thisconcept, which was conceived in our laboratoryto overcome the problems of the adherent elec-trode and the delivery of excess energy encoun-tered by earlier investigators. It was also ourobjective to demonstrate that this technique ofendovascular electrocoagulation is capable ofproviding distal vessel occlusion in a safe, rapid,controllable, and superselective manner.
Materials and MethodsTo develop the technique of endovascular electrocoag-
ulation, an experimental study was performed in swinewith the material and methods described below.
RF
Two different systems of RF generation were tested,constant voltage and constant power. A constant voltagesystem maintains the same voltage throughout its activa-tion. Changes in the resistance of the circuit are counteredby opposite changes in the current according to Ohm’s law(voltage 5 current 3 resistance); voltage is not affected bychanges in resistance. On the other hand, a constantpower system maintains the same power throughout itsactivation. Since power 5 voltage 3 current 5 voltage2/resistance, any change in the resistance of the circuit ismet by a corresponding change in voltage.
Figure 1 is a diagrammatic representation of the com-ponents used in a constant voltage system. A signal gen-erator (CFG 280, Tektronix, Wilsonville, Ore) is set at afrequency of 500 kHz with a continuous sine wave output.The signal is sent to an RF amplifier (75A220, AmplifierResearch, Souderton, Pa), where it is amplified. A powermeter capable of measuring both forward power and re-flected power (Thruline Wattmeter, Bird Electronics,Cleveland, Ohio) is connected to the amplifier. The powermeter has two output alligator grabbers for delivering RFalternating current. One grabber is connected to the dis-persive electrode or ground pad (E7506, Valleylab, Boul-der, Colo) placed on the abdomen of the animal. The othergrabber is connected to the proximal end of the detachable
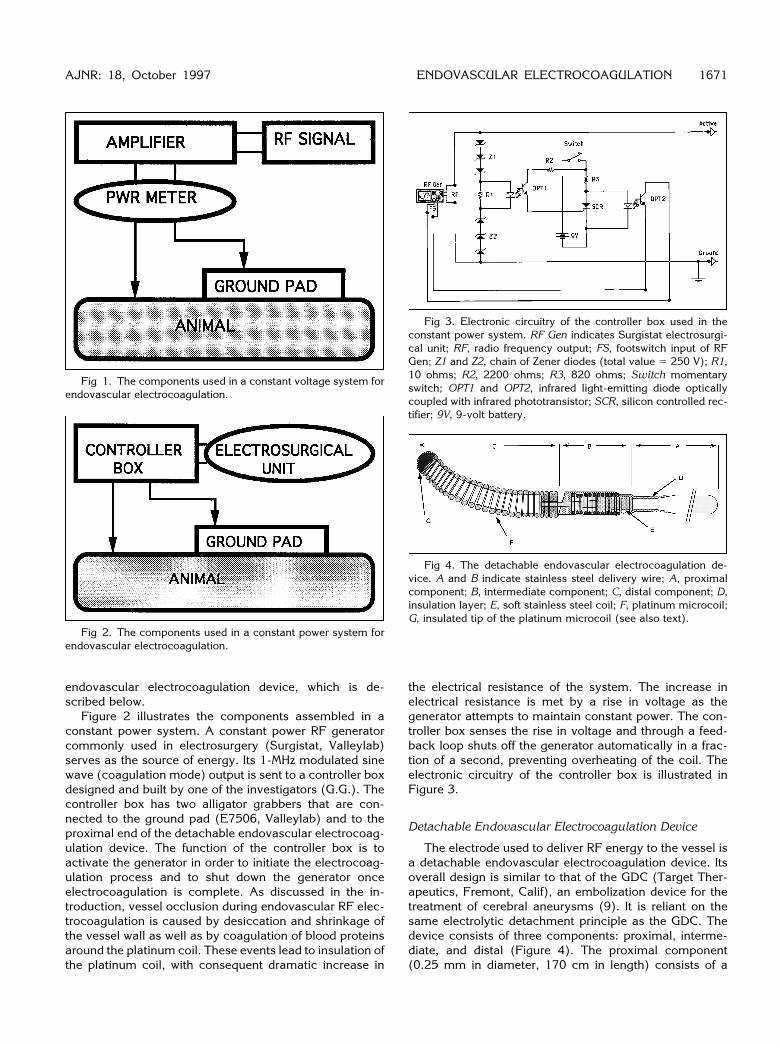
endovascular electrocoagulation device, which is de-scribed below.
Figure 2 illustrates the components assembled in aconstant power system. A constant power RF generatorcommonly used in electrosurgery (Surgistat, Valleylab)serves as the source of energy. Its 1-MHz modulated sinewave (coagulation mode) output is sent to a controller boxdesigned and built by one of the investigators (G.G.). Thecontroller box has two alligator grabbers that are con-nected to the ground pad (E7506, Valleylab) and to theproximal end of the detachable endovascular electrocoag-ulation device. The function of the controller box is toactivate the generator in order to initiate the electrocoag-ulation process and to shut down the generator onceelectrocoagulation is complete. As discussed in the in-troduction, vessel occlusion during endovascular RF elec-trocoagulation is caused by desiccation and shrinkage ofthe vessel wall as well as by coagulation of blood proteinsaround the platinum coil. These events lead to insulation ofthe platinum coil, with consequent dramatic increase in
Fig 1. The components used in a constant voltage system forendovascular electrocoagulation.
Fig 2. The components used in a constant power system forendovascular electrocoagulation.
AJNR: 18, October 1997
the electrical resistance of the system. The increase inelectrical resistance is met by a rise in voltage as thegenerator attempts to maintain constant power. The con-troller box senses the rise in voltage and through a feed-back loop shuts off the generator automatically in a frac-tion of a second, preventing overheating of the coil. Theelectronic circuitry of the controller box is illustrated inFigure 3.
Detachable Endovascular Electrocoagulation Device
The electrode used to deliver RF energy to the vessel isa detachable endovascular electrocoagulation device. Itsoverall design is similar to that of the GDC (Target Ther-apeutics, Fremont, Calif), an embolization device for thetreatment of cerebral aneurysms (9). It is reliant on thesame electrolytic detachment principle as the GDC. Thedevice consists of three components: proximal, interme-diate, and distal (Figure 4). The proximal component(0.25 mm in diameter, 170 cm in length) consists of a
Fig 3. Electronic circuitry of the controller box used in theconstant power system. RF Gen indicates Surgistat electrosurgi-cal unit; RF, radio frequency output; FS, footswitch input of RFGen; Z1 and Z2, chain of Zener diodes (total value 5 250 V); R1,10 ohms; R2, 2200 ohms; R3, 820 ohms; Switch momentaryswitch; OPT1 and OPT2, infrared light-emitting diode opticallycoupled with infrared phototransistor; SCR, silicon controlled rec-tifier; 9V, 9-volt battery.
Fig 4. The detachable endovascular electrocoagulation de-vice. A and B indicate stainless steel delivery wire; A, proximalcomponent; B, intermediate component; C, distal component; D,insulation layer; E, soft stainless steel coil; F, platinum microcoil;G, insulated tip of the platinum microcoil (see also text).
ENDOVASCULAR ELECTROCOAGULATION 1671

stainless steel core wire, which is laminated with an insu-lation layer except at its most proximal portion. This un-insulated portion is connected to the RF energy source.The intermediate component (0.25 mm in diameter, 3 cmin length) is made of a very soft, electrically insulatedtapering stainless steel wire. At the distal portion of theintermediate component, the tapering stainless steel wireis uninsulated; this is the site of electrolytic detachment.Together, the proximal and the intermediate componentsare known as the delivery wire. The distal component ismade of a crescent-shaped platinum microcoil (it isshaped with a curve to allow for vessel selectivity). Theplatinum microcoil comes in two diameter sizes: 0.010inches (0.25 mm) and 0.015 inches (0.375 mm), knownas #10 and #15, respectively. Both versions are 6 mm inlength. Except at its most distal 1 mm, the platinum mi-crocoil is uninsulated. This is where RF energy exits thedevice and where electrocoagulation occurs. The platinummicrocoil is also the component that is left in the vessel asan implant following electrolytic detachment. Figure 5 is aphotograph of the detachable endovascular electrocoagu-lation device.
Direct Current Generator
After the vessel is occluded, a direct current generator(GDC Power Supply, Target Therapeutics) with a 1.0-mAoutput is used to electrolytically detach the platinum mi-crocoil, which is left in the vessel as an implant.
Endovascular Electrocoagulation Protocol
Since June 1993, 112 arteries (branches of the ascend-ing cervical artery and the hepatic artery) of Red Duroc
Fig 5. The distal end of the detachable endovascular electro-coagulation device shows stainless steel delivery wire (doublearrows); uninsulated steel junction (long black arrow); crescent-shaped 6-mm long platinum coil (short arrow). The distal, 1-mm,portion of the platinum coil is insulated (white arrow) to avoidpossible convergence of the RF energy in a too-small area of thevessel.
1672 JI
swine have been subjected to the endovascular electroco-agulation protocol approved by the Animal ResearchCommittee of our institution. Branches of the ascendingcervical artery were chosen because they are superficialand easy to expose and retrieve. Branches of the hepaticartery were used because they allow the assessment ofpossible periarterial parenchymal damage. Also, occlu-sion of these arteries does not impair the survival of theswine. All arteries were 1.5 mm or less in inner diameter asassessed angiographically. Arteries 1.0 mm or less in di-ameter were treated with both the #10 and the #15 devicesand those between 1.0 and 1.5 mm diameter were treatedwith the #15 device only. Sixty-four of the arteries weretreated with the constant voltage system and 48 weretreated with the constant power system. With the swineunder general anesthesia a ground pad was placed on theanimal’s abdomen (RF return electrode). Then, under sys-temic heparinization, a 6F nontapered transfemoral angio-graphic catheter (Fasguide, Target Therapeutics) was po-sitioned in either the hepatic or ascending cervical artery.Preocclusion angiography delineated the location and thesize of the arteries to be occluded. A 2.0F or 2.7F micro-catheter (Tracker 10 or Tracker 18, respectively, TargetTherapeutics) was introduced through the guiding cathe-ter. Both the guiding catheter and the microcatheter werecontinuously flushed with pressurized saline by means ofside-arm adapters. The detachable endovascular electro-coagulation device was then passed through the micro-catheter and the platinum microcoil positioned beyond themicrocatheter tip in the targeted arterial segment underdigital roadmapping. In many instances, the targeted ar-teries were too small in diameter and/or too tortuous to bereached by the microcatheters. Placement of the platinumcoil simply involved pushing and steering it into the de-sired vessel by maneuvering the delivery wire, as onewould do with a microguidewire. This was possible be-cause the coil was pushable, torquable, steerable, andradiopaque.
Figure 6 is a diagrammatic representation of the endo-vascular electrocoagulation technique. The platinum distalportion of the device was positioned in the targeted arterialsegment through a microcatheter under fluoroscopy androadmapping. Note that the platinum microcoil can beextended far beyond the tip of the microcatheter and it canbe repositioned again and again until the location is satis-factory. Application of RF energy induces desiccation andretraction of the vessel wall, formation of the protein co-agulum and thrombus, and adhesion of the platinum mi-crocoil to the arterial segment.
In the constant voltage system, RF energy is slowlyincreased from zero at the start of the procedure until theabove events occur, which dramatically increases theelectrical resistance of the circuit. This great increase inresistance reduces the actual power delivered to the vesselto close to zero, since power 5 voltage2/resistance. Mostof the power is reflected back to the generator, and this isseen as a surge in reflected power in the power meter. Thissurge is taken as the end point of the electrocoagulationprocess and it typically occurs within seconds of RF en-
AJNR: 18, October 1997

ergy application. Once this surge in reflected power is seenon the meter, the energy is turned off manually. Thisprocedure is done three times to ensure complete electro-coagulation of the artery. An angiogram at this time canconfirm that the artery is occluded. After occlusion hasbeen confirmed, the RF generator is disconnected and thedelivery wire is connected to the DC generator. Applicationof the positive, 1-mA direct electric current induces elec-trolysis of the uninsulated steel junction and separates theadherent platinum coil from the delivery wire. Detachmenttypically occurs within 2 minutes of direct current appli-cation. Following detachment, the delivery wire is with-drawn and a repeat angiogram confirms occlusion of theartery and the position of the platinum microcoil that hasbeen left behind as an implant.
In the constant power system, the Surgistat electrosur-gical unit is set at level 5 (12 watts) in the coagulationmode. Pushing a switch on the controller box (Fig 3)activates the electrocoagulation process. As in the con-stant voltage system, an increase in electrical resistance ofthe circuit signals occlusion of the vessel. Because it is aconstant power generator, the Surgistat will raise its outputvoltage when the resistance of the system increases in aneffort to maintain constant power (power 5 voltage2/resistance). This rise in voltage is detected by the control-ler box, which in turn automatically shuts off the Surgistatin a matter of fractions of a second, thus preventing deliv-
Fig 6. The endovascular electrocoagulation technique.A, Platinum microcoil is positioned in the targeted vessel seg-
ment through a microcatheter. Note that there is still control of themicrocoil beyond the microcatheter tip.
B, Application of RF energy induces retraction and desiccationof the targeted vessel segment, local formation of coagulum andthrombus, and adhesion-straightening of the platinum microcoilto the vessel wall.
C, Application of positive direct current causes the uninsulatedsteel junction to undergo electrolysis. The platinum microcoil isseparated from the steel delivery wire.
D, The delivery wire and the microcatheter are removed. Theplatinum microcoil remains as an implant.
AJNR: 18, October 1997
ery of excess energy. As it is in the constant voltagesystem, the application of RF alternating current is donethree times to ensure complete electrocoagulation of thevessel. The coil is then detached electrolytically.
Results
All arteries were occluded within 15 seconds,typically, within 3 to 6 seconds, by endovascu-lar RF electrocoagulation, whether via theconstant voltage system or the constant powersystem. In all cases, an immediate postelectro-coagulation angiogram showed the occlusion ofthe targeted artery, the preservation of the par-ent artery, and the position of the platinum mi-crocoil (Fig 7). Following use of the appropriatemethods described above, we did not observerupture of the artery, dissection of the artery,unintended occlusion, or migration of the plati-num microcoil; nor did the platinum microcoilever fail to electrolytically detach from the restof the device. Follow-up angiograms obtained 1week to 12 weeks after the procedure confirmedin all cases persistent and complete occlusionof the targeted arteries and patency of the par-ent vessels. Migration of the platinum microcoil,pseudoaneurysm formation, and dilatation ofthe vessel segment proximal to the platinummicrocoil were never observed throughout theexperimental period (Fig 7).
Histologic examination of vessels treated viathe constant voltage system showed that at 1week the vessel lumen was occluded by theplatinum coil, denatured fibrin, and red bloodcells (eg, occlusive coagulum). Loss of the en-dothelium and some minor damage to the in-ternal elastic lamina were also observed, to-gether with mild periadventitial acute infiltrate.At 6 weeks, the vessel lumen was obliterated bygranulation tissue within and surrounding theplatinum coil. The endothelium was not presentand a thickened fibrous adventitia surrounded athinner muscularis. The periadventitial soft tis-sue showed a thin ring of fibroblastic prolifera-tion (Fig 8). Histologic findings at 12 weekswere similar to those seen at 6 weeks, except fora thinner muscularis and adventitia.
No adverse reactions were observed in theexperimental animals either during or after en-dovascular electrocoagulation. All animals wereexamined daily by the veterinary staff, and allanimals were determined to be healthy duringthe experimental period.
ENDOVASCULAR ELECTROCOAGULATION 1673

Fig 7. A, Arteriogram of the right as-cending cervical artery of a swine, antero-posterior view. Arrows point at the threetarget locations to be occluded.
B, A Tracker catheter was placed in theproximal portion of the ascending cervicalartery (arrowhead). From that location,two platinum coils (double arrows) weredelivered through the Tracker to two of thetargeted locations, and vessel occlusionwas achieved by RF and electrolytic de-tachment. Through the Tracker, still posi-tioned in the original location, a third coilwas steered into a distal and tortuous lo-cation (single arrow): before RF applica-tion there was still flow of blood around thecoil.
C, Angiogram shows that after RF ap-plication and electrolytic detachment, thethird distal vessel was also completely oc-cluded (arrow).
D, Control angiogram at 4 weeks showspersistent occlusion with patency of thesurrounding vascular tree.
1674 JI AJNR: 18, October 1997
Discussion
Biophysics of Electrocoagulation
Over the past century, the biophysics of elec-trocoagulation has become well understood. Atypical electrosurgical system consists of an ac-tive electrode in the form of a needle or a blade,a dispersive electrode (also known as a groundelectrode) in the form of a conductive pad witha large surface area, and an RF current gener-ator to which the two electrodes are connected.An electrical circuit is completed when the dis-persive electrode is applied to the skin and theactive electrode touches the body. During itsapplication, RF energy travels through the in-tervening biological tissue between the twoelectrodes and generates electromagnetic heat-ing called resistive or ohmic heating (10). It isthrough this heating effect that hemostasis isachieved. The heat generated is proportional to
the square of the current intensity, which is in-versely proportional to the surface area of theelectrode (11, 12). Thus, heat is greatest at theactive electrode, owing to its small surface areaand high current intensity. Because resistiveheating decreases with distance from the activeelectrode to the fourth power (1/r4), significantresistive heating only occurs within a narrow(,1 mm) rim of tissue in direct contact with theactive electrode (10, 11). Although heat is alsoproduced underneath the dispersive electrode,it does not reach a high enough level to causetissue damage. This is because heat is diffusedover the large area of the dispersive electrodeand is dissipated rapidly (7, 12).
Heat energy generated from RF alternatingcurrent causes surgical hemostasis by the fol-lowing mechanisms: desiccation of the vesselwall leading to shrinkage and retraction of thevessel, coagulation of blood proteins and con-

nective tissues resulting in the formation of anocclusive coagulum, and induction of thrombo-sis consequent to vessel wall injuries (8). Bleed-ing is usually stopped with a few seconds ofenergy application. If, however, more energy isapplied beyond this point, denatured proteinalong with glucose deriving from the pyrolysisof the collagen will appear, causing the elec-trode to stick to the vessel (10, 13). Experi-enced surgeons can usually prevent the adher-ence of the electrode by shutting off the energywhen they see the vessel shrink.
With any electrical medical device, possibleinterference with the cardiac conduction path-ways is a concern. However, as was known inthe late 1890s, high-frequency current above10 000 cycles per second (10 kHz) at moderatelevels does not produce muscle contraction (7).Today, most electrosurgical units operate be-tween 300 kHz and 3 MHz, which is high enoughto prevent rapid myocardial depolarization and,therefore, the induction of ventricular fibrillation(10). In fact, high-frequency alternating currentis applied directly to the myocardium for abla-tion of arrhythmogenic pathways without induc-ing ventricular fibrillation (14, 15). Over thepast century, surgical hemostasis by electroco-agulation has proved to be a safe and effectivetechnique.
Fig 8. Low-power photomicrograph of an axial section of ahepatic artery of a swine, obtained 6 weeks after coil positioning,RF application, and electrolytic coil detachment. The 0.25-mmplatinum coil (between arrowheads) is near the center of theartery. Granulation tissue is within and surrounding the coil. Noendothelium is discernible. The internal elastic lamina is visible(long arrows). A thickened fibrous adventitia (double arrows)surrounds a thinned muscularis. A periadventitial thin ring of mildfibroblastic proliferation is observable (hematoxylin-eosin, origi-nal magnification 32.5).
AJNR: 18, October 1997
Development of EndovascularElectrocoagulation
The success of surgical hemostasis by elec-trocoagulation prompted investigators to studyits potential for achieving vascular occlusion viathe endovascular route. Electrocoagulation,when applied successfully from within the bloodvessel, certainly appeared to be advantageousrelative to existing embolotherapeutic tech-niques; it could be precise, effective, easy touse, and unaffected by reflux, migration, coagu-lopathy, or blood flow velocity. In 1970, Tarenand Gabrielsen (4) reported on endovascularRF thrombosis of the feeding arteries of arterio-venous malformations of the jaw in two pa-tients, with good clinical outcome. These re-searchers used a 0.5-mm wire and a 100-mAalternating current for 5 to 15 seconds to oc-clude branches of the external carotid artery.Both patients were awake during the treatment,under local anesthesia supplemented by intra-venous ketamine hydrochloride. In 1973, Phil-lips (5) evaluated endovascular occlusion byRF energy. In that study, a regular guidewireprotruding 2 to 3 mm beyond the catheter tipwas placed in canine abdominal vessels. Cur-rent was passed through the guidewire (servingas an active electrode) from a constant powerelectrosurgical unit set on coagulation mode.Phillips found that a few seconds of RF energywould cause either vessel occlusion or vesselrupture; the amount of energy necessary tocause occlusion differed only slightly from theamount that would cause rupture. Moreover, helacked a mechanism that could detect vesselocclusion and thus signal when to stop the RFenergy. Delivering more energy to an alreadyoccluded and desiccated vessel led to the de-struction of the vessel wall and its eventual rup-ture. Phillips also observed that the guidewiretip became adherent to the vessel wall duringelectrocoagulation and that tearing of the vesselwall sometimes occurred with removal of theguidewire.
In 1975, Gold et al (3) described a clinicalcase in which a vessel was occluded via high-frequency alternating current. These investiga-tors successfully occluded several arterialbranches to a pseudoaneurysm in the head ofthe pancreas by using a regular guidewire and aconstant power electrocoagulation unit. The ap-plied electric current was increased in a stepwisefashion until vessel occlusion was observed an-
ENDOVASCULAR ELECTROCOAGULATION 1675

giographically. This method presumably avoidedoverheating and consequent rupture. Adhesionof the guidewire tip to the vessel wall was notreported.
To prevent the guidewire/electrode tip fromadhering to the vessel wall during electrocoag-ulation, Cragg et al (1) in 1982 withdrew theguidewire while applying RF energy to the ce-phalic and lateral saphenous veins of dogs.Nevertheless, failure to withdraw the guidewirequickly led to one case of guidewire tip adhe-sion. Subsequent extraction of this guidewireresulted in a vascular tear. Using this withdrawalmethod, these investigators observed only oneimmediate and 13 permanent occlusions (as-sessed at 4 weeks after treatment) in a sampleof 20 vessels in dogs. The poor occlusion ratecould be attributed to the fact that the coagulumformed during electrocoagulation was removedwith the withdrawal of the guidewire. Vessel oc-clusion was caused solely by thrombus forma-tion resulting from heat injury of the vessel wall.However, thrombus induction did not alwaysoccur, as it was affected by a variety of factors:speed of blood flow within the vessel, status ofthe subject’s blood clotting system, and extentof vessel wall injury.
In 1983, Brunelle et al (2) improved thesafety of endovascular electrocoagulation byusing a constant voltage power supply andmonitoring the current level during the proce-dure. By progressively increasing the voltageevery 30 seconds until a current drop was ob-served, rupture of the canine anterior tibial ar-teries during electrocoagulation was prevented.A decrease in current was used as the end pointof the electrocoagulation process, and was ex-plained by Brunelle et al as the local desiccationof tissues surrounding the guidewire as a con-sequence of heat, resulting in an opening of theelectrical circuit. The main factor is that hightemperature causes the adhesion of proteinsand connective tissues to the guidewire, leadingto a dramatic increase in electrical resistance(16). In a constant voltage system, an increasein resistance is balanced by a decrease in cur-rent (Ohm’s law: voltage 5 current 3 resis-tance), which translates into a proportional de-crease in power (power 5 voltage 3 current 5voltage2/resistance). In such a system, heatingis a self-limited phenomenon; the decrease inpower (and thus decrease in heating) makes itunlikely for vessel rupture to occur by overheat-ing. This is in contradistinction to constant
1676 JI
power systems used by previous investigators,in which a rise in resistance was compensatedby a rise in voltage, thus maintaining the samepower output. Despite the improvement insafety, Brunelle et al were not able to achieve asatisfactory occlusion rate, as vessel closurewas still dependent on thrombus formation afterremoval of the guidewire. Only six of 11 anteriortibial arteries in dogs were permanently oc-cluded. Tanigawa et al (6) reported on the clin-ical use of endovascular RF electrocoagulationin a case of a fibrous histiocytoma of the rightthigh. They did not use a definite safety methodto automatically control the RF energy delivery.
Such unsatisfactory occlusion rates and/orthe danger of extracting an adherent guidewiretip eventually led investigators to abandon theendovascular electrocoagulation technique.
Development of Electrolytic Detachment
Electrolysis is defined as the nonspontaneouschemical reaction driven by direct electric cur-rent (17). It is seen when two electrodes con-nected to a source of direct electric current aredipped into a solution. Under these conditions,the immersed end of the positive electrode dis-solves while the negative electrode recruits themigrating ions from the anode to the cathode.Certain metals such as iron and silver are sus-ceptible to electrolysis while noble metals suchas platinum are not (18). In 1991, Guglielmi etal described the phenomenon of electrolysis todetach embolic coils into cerebral aneurysms(9, 19) and feeders to arteriovenous malforma-tions (Guglielmi, “Controlled...”).
Using a device that consisted of a platinumcoil joined to an insulated steel delivery wire byan uninsulated steel junction, these researcherswere able to position and reposition the plati-num coil inside the cerebral aneurysm until thelocation of the platinum coil was satisfactory.This repeated positioning was possible becausethe platinum coil remained attached to the de-livery wire. Once the coil was properly placedinside the aneurysm, a direct current passedalong the device electrolytically dissolved theuninsulated steel junction, thus separating theplatinum coil from the delivery wire. This de-vice, the GDC described earlier, is used in thetreatment of high-risk intracranial aneurysmsand has been approved for clinical use by theFood and Drug Administration. The GDC rep-resented a significant improvement over exist-
AJNR: 18, October 1997

ing embolic coil technology, such as pushablecoils, because it gave users a great degree ofcontrol over the placement of the coil. A modi-fied version of the GDC was used in the presentstudy.
Development of the Present EndovascularElectrocoagulation Technique
It is clear that the failure of endovascular elec-trocoagulation reported by previous investigatorsstemmed from two problems: the extraction of theadherent electrode (typically a guidewire) afterendovascular electrocoagulation, with conse-quent tearing or recanalization of the vessel, andthe inability to know when vessel occlusion hasoccurred, which resulted in vessel rupture due tothe application of excess energy.
The first problem was solved in our laboratoryby employing the concept of electrolysis to de-tach the adherent electrode. To solve the sec-ond problem, a method was needed to detectprecisely when a vessel has been occluded byendovascular electrocoagulation during energyapplication. In our early experience, using astandard constant power electrosurgical unit(Surgistat, Valleylab) without a controller shut-off mechanism, we successfully occluded manyvessels by combining electrocoagulation withdetachment of the adherent portion of the elec-trode. RF energy was applied through the elec-trode in intervals of a few seconds, and angio-grams were obtained between the intervals.When an angiogram revealed occlusion of thetargeted vessel, the adherent portion of theelectrode was electrolytically separated fromthe rest of the electrode by applying a smallpositive direct current to it. However, in theseearly experiences, there were instances in whichthe vessel ruptured after the RF energy wasapplied. Because it was not known when thevessel was occluded, the continued and exces-sive application of energy to the vessel some-times caused it to rupture. As described above,previous work has shown that when a vessel hasbeen occluded by electrocoagulation, the elec-trical resistance of the circuit increases dramat-ically. By monitoring the electrical resistance ofthe circuit during RF application, it became pos-sible to determine when the vessel was oc-cluded and to shut off the energy in fractions ofa second. Therefore, a controller unit was built(Figs 2 and 3) that could monitor the electricalresistance and shut off the electrosurgical unit
AJNR: 18, October 1997
once the electrical resistance had risen. Thetime of response of the controller unit can bevaried. To avoid tissue damage beyond the ad-ventitia, a very short response time was needed.Also, in a constant voltage system, vessel rup-ture due to excess energy application is un-likely, because resistive heating is a self-limitedphenomenon (see “Development of Endovas-cular Electrocoagulation” section). Althoughresistance monitoring in a constant voltage sys-tem was not needed to prevent excess powerdelivery, it did signal when the vessel was oc-cluded. Therefore, on the basis of this experi-ence, we determined that both the constantvoltage and the constant power generators areefficacious in achieving rapid vessel occlusion.However, the constant voltage generator seemsto have intrinsic safety properties. With the con-stant power generator, safety is achieved byadding the controller shut-off unit.
Although this report describes our experiencewith the occlusion of vessels 1.5 mm or smaller,larger vessels may be occluded using platinumcoils with larger diameters (thereby matchingthe increased size of the vessel), or by usingmultiple parallel coils. In fact, we believe thatboth electrocoagulation and mechanical occlu-sion are necessary for the long-term efficacy ofthe technique.
Acute, 6-week, and 12-week histologic stud-ies of the occluded arteries showed persistentocclusion and only a thin ring of mild fibroblas-tic periadventitial proliferation. However, longerterm histologic and angiographic studies, aswell as a more accurate analysis of the extent ofpossible tissue damage beyond the arterial wall,are needed. These will allow a more thoroughassessment of the long-term efficacy and of thesafety of the technique.
Conclusions
Endovascular electrocoagulation has beenattempted in the past by many investigators toachieve vessel occlusion, without much suc-cess. Some of these failures were due to theapplication of excess RF energy that resulted invessel rupture. By monitoring the rise in electri-cal resistance, we were able to determine whena vessel has been occluded and to prevent over-heating. We think that other failures resultedfrom the extraction of the adherent electrode/guidewire after electrocoagulation; that is, with-drawal of the adherent electrode/guidewire re-
ENDOVASCULAR ELECTROCOAGULATION 1677

moved the occlusive coagulum and/or tore thevessel wall. By using the GDC crescent-shapedplatinum coil, we were able to electrocoagulatethe vessel and then leave the electrode/coil inthe vessel as an implant/embolic material. Thiswas accomplished by applying the RF energyfirst, followed by electrolytic direct current de-tachment of the coil. Using this approach, wewere able to occlude small arteries of swinepermanently in a rapid, controlled, and super-selective manner. No substantial differenceswere noticed between the constant power (withautomatic shut-off mechanism) and the con-stant voltage generators. The former are easierto find in commerce; the latter, being self-limit-ing, have intrinsic safety properties. Unlike withembolic materials, such as pushable coils, poly-vinyl alcohol, and cyanoacrylate, placement ofthe detachable endovascular electrocoagula-tion device in the targeted vessel is not depen-dent on the position of the microcatheter; thedevice can enter those small and tortuous ves-sels distal to and unreachable by the microcath-eter in much the same manner as that of amicroguidewire. The preliminary experimentaldata observed in this work make this techniquesuitable for the preoperative or definitive embo-lization of a variety of vascular disorders, in-cluding arteriovenous malformations, arterio-venous fistulas, and hypervascular tumors.
AcknowledgmentsWe thank John Robert and Christopher Carangi at the
Leo G. Rigler Center for Radiological Research, Universityof California at Los Angeles, and Target Therapeutics,Fremont, Calif, for their valuable collaboration. We alsothank Hiroshi Tenjin and Maria Alzona for their coopera-tion in obtaining the histologic studies.
References1. Cragg AH, Galliani CA, Rysavy JA, et al. Endovascular diathermic
vessel occlusion. Radiology 1982;144:303–308
1678 JI
2. Brunelle F, Kunstlinger F, Quillard J. Endovascular electrocoag-ulation with a bipolar electrode and alternating current: a fol-low-up study in dogs. Radiology 1983;148:413–415
3. Gold RE, Blair DC, Finlay JB, et al. Transarterial electrocoagula-tion therapy of a pseudoaneurysm in the head of the pancreas.AJR Am J Roentgenol 1975;125:422–426
4. Taren JE, Gabrielsen TO. Radio-frequency thrombosis of vascularmalformations with a transvascular magnetic catheter. Science1970;168:138–141
5. Phillips JF. Transcatheter electrocoagulation of blood vessels.Invest Radiol 1973;8:295–304
6. Tanigawa N, Sawada S, Morioka N. Intraarterial occlusion byradiofrequency (technical note). Acta Radiol 1994;35:626–628
7. Memon MA. Surgical diathermy. Br J Hosp Med 1994;52:403–408
8. Sigel B, Dunn MR. The mechanism of blood vessel closure by highfrequency electrocoagulation. Surg Gynecol Obstet 1965;35:823–831
9. Guglielmi G, Vinuela F, Sepetka I, et al. Electrothrombosis ofsaccular aneurysms via endovascular approach, 1: electrochem-ical basis, technique, and experimental results. J Neurosurg 1991;75:1–7
10. Nath S, Haines DE. Biophysics and pathology of catheter energydelivery system. Prog Cardiovasc Dis 1995;38:185–204
11. Burton CV. RF lesion generation. Appl Neurophysiol 1976/1977;39:77–79
12. Organ LW. Electrophysiologic principles of radiofrequency lesionmaking. Appl Neurophysiol 1976/1977;39:69–76
13. Haag R, Cuschieri A. Recent advances in high-frequency electro-surgery: development of automated systems. J R Coll Surg Edinb1993;38:354–364
14. Jayaeri MR, Hempe SL, Sra JS. Selective transcatheter ablation ofthe fast and slow pathways using radiofrequency energy in pa-tients with atrioventricular nodal reentrant tachycardia. Circula-tion 1992;85:1318–1328
15. Kay GN, Chong F, Epstein AE. Radiofrequency ablation for treat-ment of primary atrial tachycardias. J Am Coll Cardiol 1993;21:901–909
16. Haines DE, Verhow AF. Observations on electrode-tissue inter-face temperature and effect on electrical impedance during radio-frequency ablation of ventricular myocardium. Circulation 1990;82:1034–1038
17. Ebbing DD, Wrighton MS. General Chemistry. Boston, Mass:Houghton Mifflin; 1984:683–715
18. Potter EC. Electrochemistry, Principles and Applications. London,England: Cleaver-Hume; 1956:1–19, 124–154
19. Guglielmi G, Vinuela F, Dion J, et al. Electrothrombosis of sac-cular aneurysms via endovascular approach, 2: preliminary clin-ical experience. J Neurosurg 1991;75:8–14
AJNR: 18, October 1997





























