Embed Size (px)
Citation preview
Endoscopic Repair of Endoscopic Repair of Bilateral Congenital Bilateral Congenital
Choanal Atresia: 15 Years Choanal Atresia: 15 Years ExperienceExperience
Yasser W. Khafagy, MDYasser W. Khafagy, MD
Professor of Otolaryngology Professor of Otolaryngology Mansoura UniversityMansoura University
IntroductionIntroduction
• It is a condition that describes narrowing or obliteration of the posterior nasal aperature
• It occurs in 1:7,000 to 8,000 births, of those 45% are bilateral
• Much more commonly in females
• Mostly bony or mixed, rarely purely membranous
IntroductionIntroduction
• High resolution CT scan is the definitive radiological study of choice.
• The useful parameters are vomer width, choanal air space, medial pterygoid plate projection into the choana
Ideal ProcedureIdeal Procedure
• Restore normal nasal passage
• Avoid damage to any growing structures
• Be safe
• Short surgery time and hospitalization stay
• Minimal morbidity and mortality– Endoscopic repair is more commonly used
than other approaches ( transnasal, transpalatal, transseptal)
ObjectiveObjective
• Early experience with 9 cases was published in the Laryngoscope; (112:316-319, 2002)
• This study aims to present 15 years experience with treatment of bilateral congenital choanal atresia, report technique, results, pitfalls, complications
Patients and MethodsPatients and Methods
• A prospective study including 80 cases of bilateral congenital choanal atresia, treated at Mansoura University Hospital endoscopically in the period from March 1997 to March 2011 are reported.
• All cases were diagnosed clinically and referred by the attending pediatrician
Patients and MethodsPatients and Methods
• All cases had careful history, axial CT scanning
• CT scan is examined to confirm the diagnosis, assess the choanal area, vomer width, medial pterygoid projection, bone thickness, septum and lateral nasal wall.
• Complete preoperative work up including bleeding profile, pediatric and anesthetic consult. Preoperative counseling is important and very helpful (nature of the condition, treatment, postop care, expectation, 2nd look)
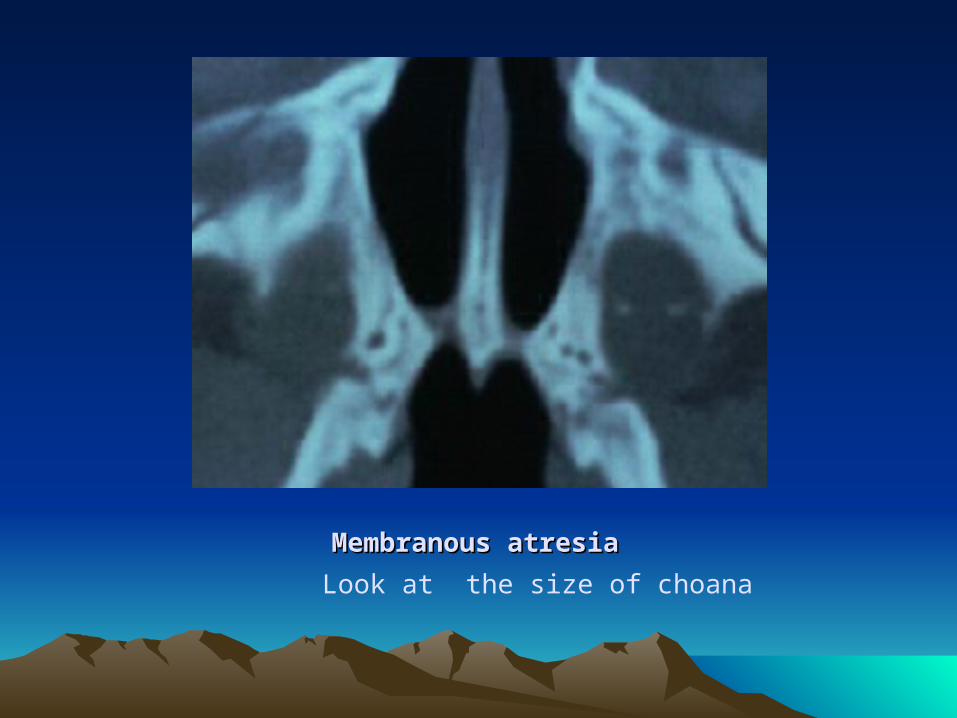
Membranous atresiaMembranous atresia
Look at the size of choana
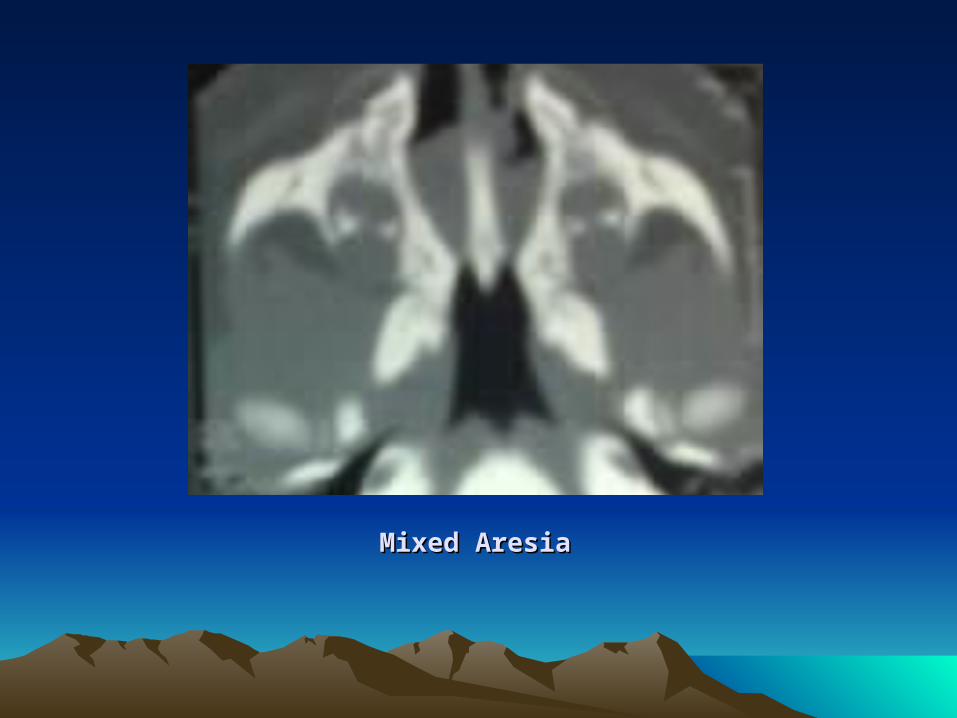
Mixed AresiaMixed Aresia
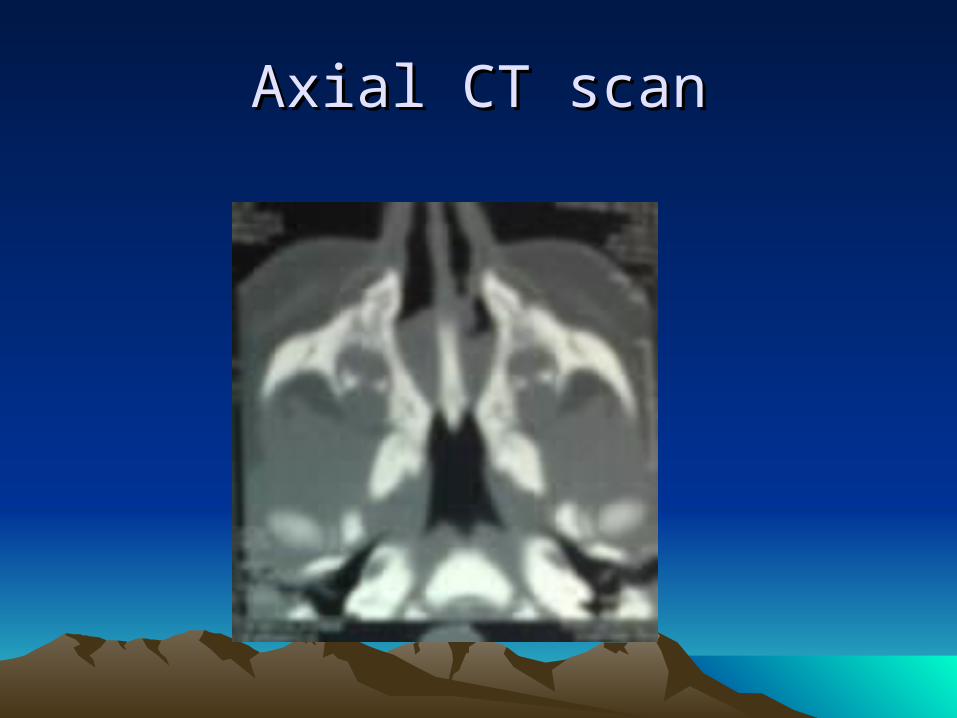
Axial CT scanAxial CT scan
Surgical TechniqueSurgical Technique
• GA with endotracheal tube, moist cotton in the oropharynx, be careful not to put bulky gauze in the oral cavity this will narrow the nasopharynx especially over the soft palate.
• Supine position, Afrin nose drops, 4 mm, 0 degree nasal endoscope, few instruments are usually needed, Some otologic instruments will be helpful.
Surgical TechniqueSurgical Technique
• Although the technique remains the same, some modifications were made as directed by the follow up for cases through the years.
• Incision is made in the posterior septum close to the atretic plate, using sickle knife radiofrequency needle, coblation needle
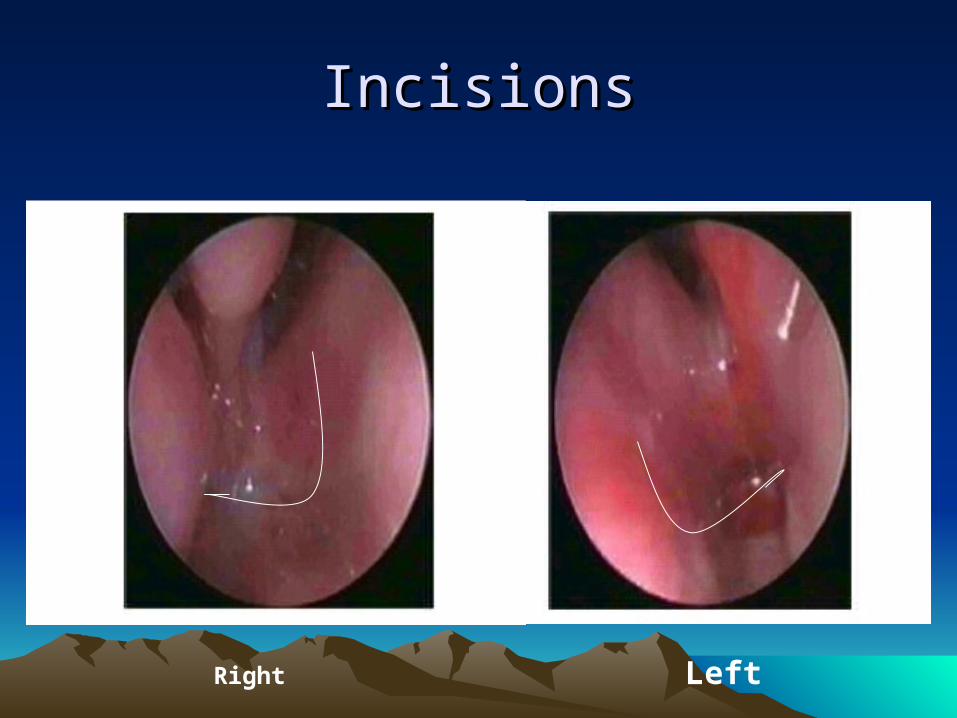
IncisionsIncisions
Right Left
Surgical TechniqueSurgical Technique
• The incision extended to the atretic plate• The mucosa over the atretic plate is
removed, In cases with mixed atresia, the atretic plate is perforated with suction tip inferiorly and medially,
• Removal of the vomer is the most important step, Extralong burs, ear curettes, dissectors are used to create the neochoana
Surgical techniqueSurgical technique
• Extreme care to keep the cartilagenous septum intact, also extreme caution not to injure the alar cartilage by drill heat.
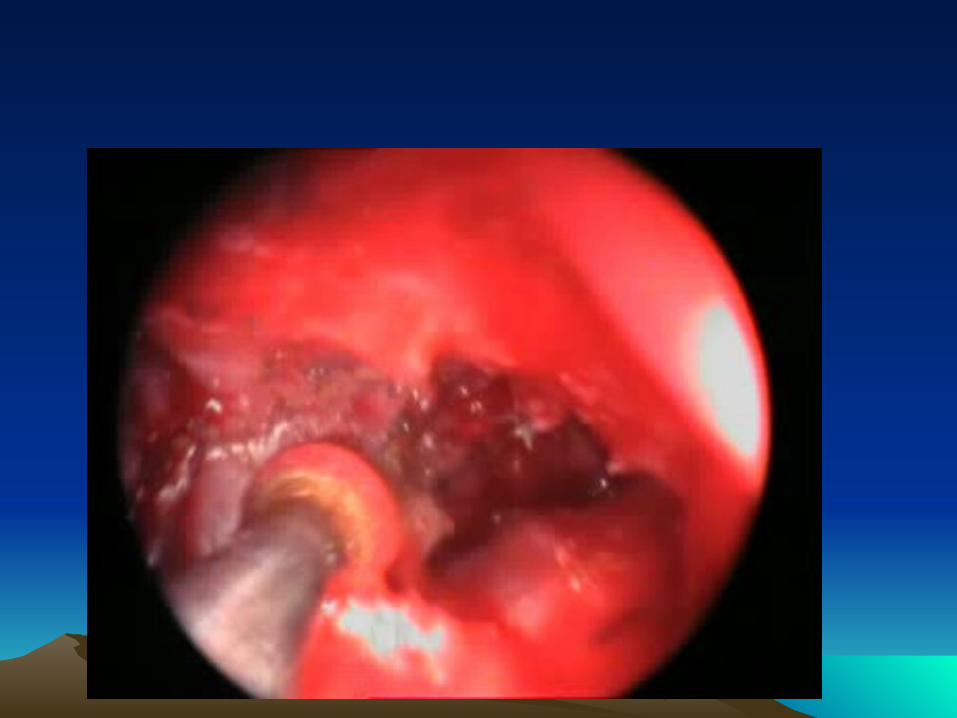
• Attention is then directed to the lateral boundary of the neochoana, in most cases drilling is required to obtain a good sized neochoana keeping in mind the continuous healing attempts of all tissues in the area of surgery!
Surgical TechniqueSurgical Technique
• Stenting was always used, Portex endotracheal tube size 3-3.5 ( mm ID)
• The length is measured by suction tube, it is fixed through the floor of the nose sublabially
• Stenting was kept for about 6 weeks.
Post-operative carePost-operative care
• Early feeding is helpful for the baby and the mother!
• Patient discharge is determined after ped consult
• Parents are educated to use suction of the tubes
• Regular weekly examination
Second Look procedureSecond Look procedure
• Now it is done for the majority of infants 2 months after surgery
• Under GA, examination, and evaluation of the neochoana, re-widening, removal of new bone formation or soft tissue re-closure.
ResultsResults• 80 infants (71 females, 9 males)• Age at operation average 1 week, (1 day
to 28 days)• Weight average, 2.8 kg• All except 3 were diagnosed at birth, 9
infants had assisted ventilation due to respiratory distress, in these cases extubation was done first before surgery.
ResultsResults
• 62 cases were mixed atresia, 16 cases were bony atresia, only two cases were membranous.
• In all cases atretic bone removal was done, the vomer was removed in all cases, lateral wall drilling was used in 55 cases.
• Average follow up was 6 years (6months to 13 years)
Complications and re-stenosisComplications and re-stenosis
• The most common is Re-stenosis (soft, bony or both).
• one cases had alar cartilage necrosis.• One case had collumelar necrosis by the stent• One case had septal perforation with
depressed nose at age of 8.• One patient had pin point palate perforation
that heals spontaneously.• Only one case died shortly after the procedure,
she had profuse bleeding during removal od soft tissue over the atretic plate (hemorrhagic disease of the newborn was suspected).
• All are among the first 15 cases.
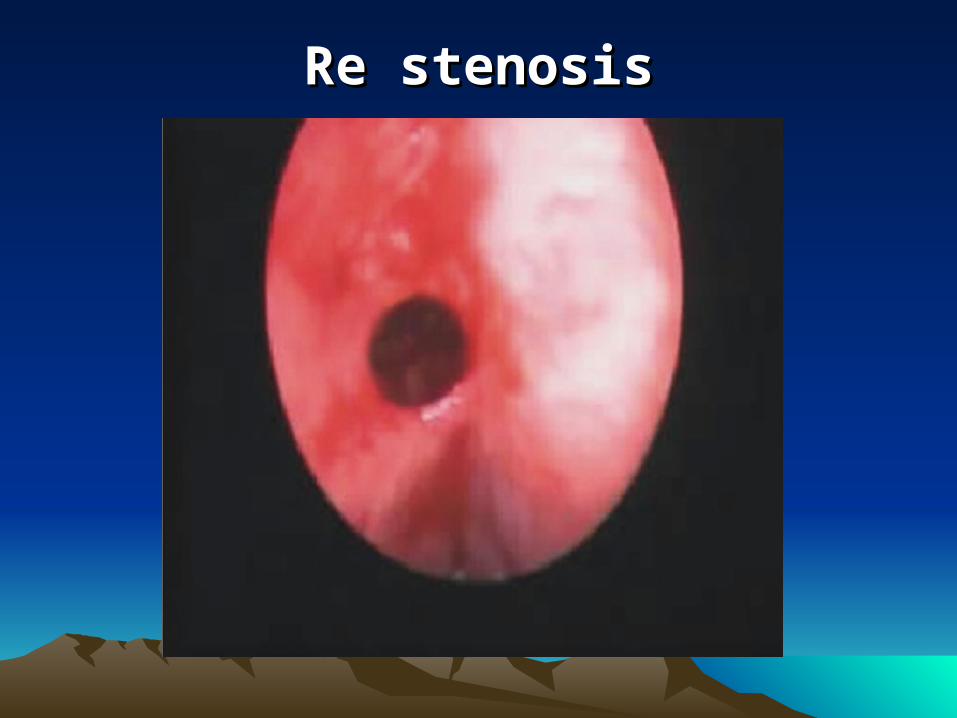
Re stenosisRe stenosis
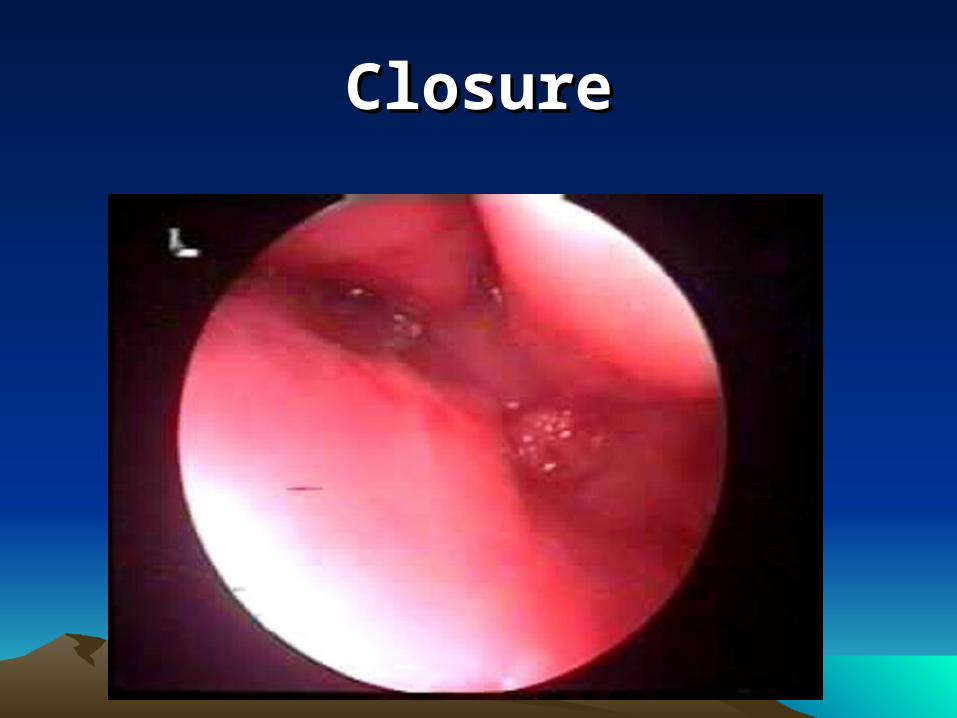
ClosureClosure
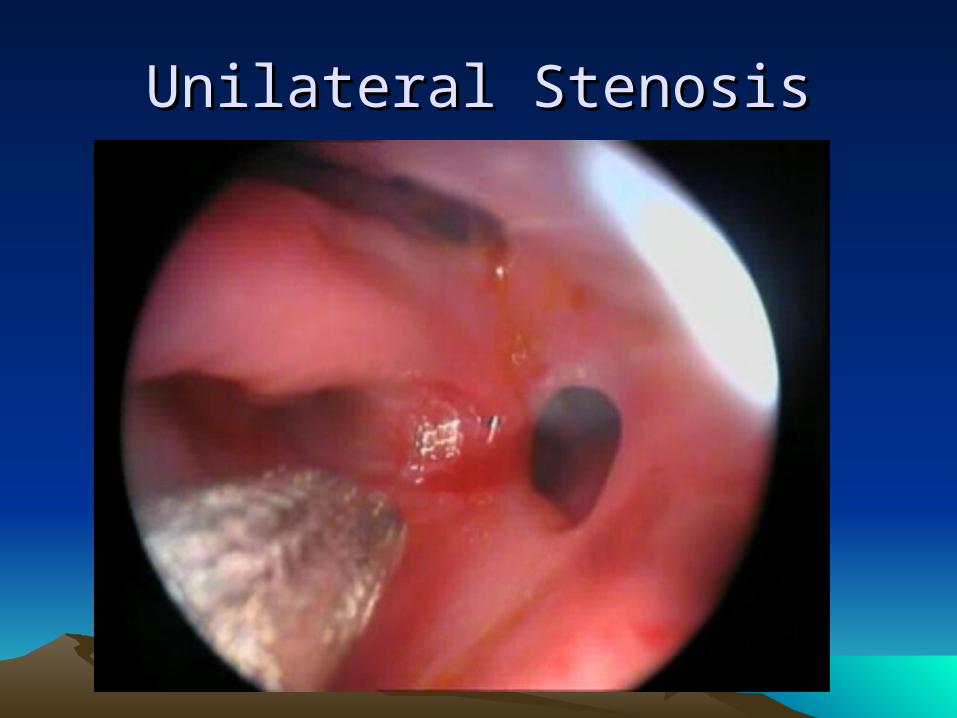
Unilateral StenosisUnilateral Stenosis

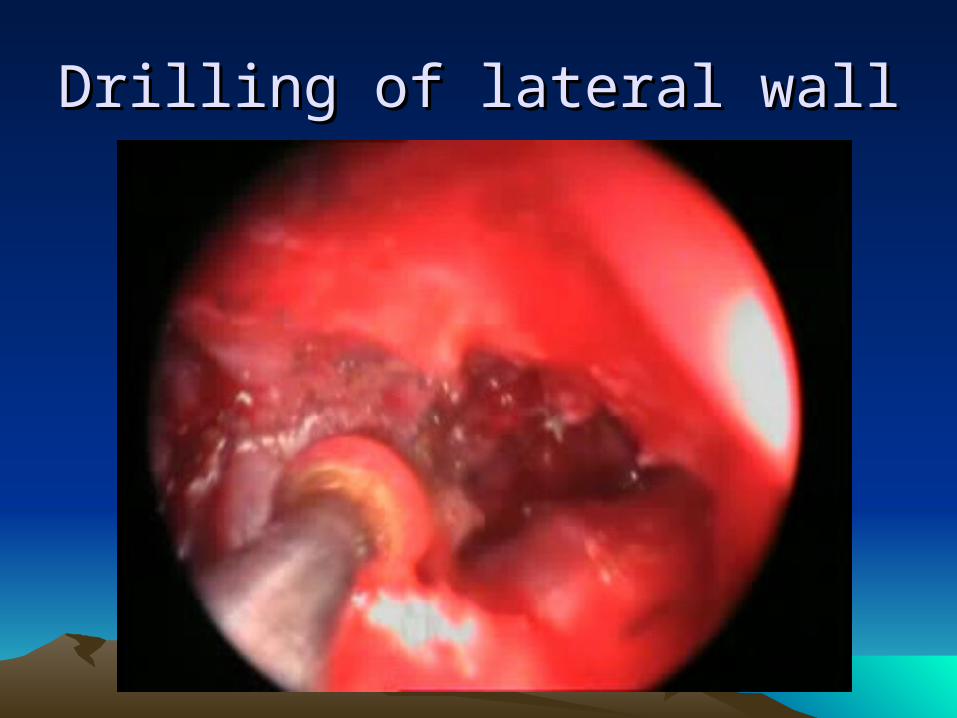
Drilling of lateral wallDrilling of lateral wall
DiscussionDiscussion
• “Choanal Obliteration” is more descriptive term than choanal atresia because the abnormally thick vomer and the medial pterygoid plates are more contributing to the problem than the atretic plate itself.
• In many cases, the closure of the choana is made by meeting of the medial and lateral walls with or without soft tissue or small bony plate
DiscussionDiscussion
• Removal of the atretic plate only or perforation of the central part of the choana on both sides will result eventually in re-closure
• Removal of the vomer or and drilling out of the medial pterygoid plates are crucial in management of these cases.
DiscussionDiscussion
• Careful review of the CT scan is important.
• Evaluation of the thickness of the obliterating components of the posterior choana and the width and height of nasopharynx for accurate surgical planning
• Infants tolerate only minimal blood loss, hence ; shortening of the procedure and avoiding working laterally is important
DiscussionDiscussion: : Stent or notStent or not
• Stenting was used empirically in our series,• The importance of stenting is debatable,
even in our team.• I have found that stenting would help to keep
better breathing in the early postoperative period thus helping the child growth
• It is unknown if it helps in reducing the narrowing and keeping the mucosa in place after surgery however, solid evidence based studies are lacking.
DiscussionDiscussion
• Second look procedure is important in bilateral atresia, because of the small size of choanal space at this age in addition to the good rapid healing as well as active rapid growth in this age also predisopse to re-narrowing.
• Sometimes , polyps are formed at the edge of the choana, restenosis with bone is not also uncommon ( growth, healing)
DiscussionDiscussion• Parent counseling is essential for assurence,
postoperative care, explanation for the problem of re-stenosis
• Teissier et al. [2008] noted that gastroesophageal reflux disease (GERD), age younger than 10 days at the time of surgery (bilateral atresia) and insufficient postoperative endoscopic revision are predictive factors for restenosis.
ConclusionsConclusions• Endoscopic repair of bilateral choanal
atresia meet the goals for efficacy, safety, and minimal effects on growth
• Second look procedure is recommended for better outcome
• Working in the infant nose is not difficult in the majority of cases
• Careful dealing with the septum, alar cartilages is important.