Embed Size (px)
Citation preview

oheaspctu
CS
EiAltw
Peer-Review Reports
Endoscopic Aqueductoplasty and Stenting
Michael J. Fritsch and Henry W. S. SchroedertflhTtcb
au(drraosa
itwaticaham
df
ldpbctr
I
MsdwWapcc
T
PPMf
sp
�
INTRODUCTION
Looking at a sagittal magnetic resonance(MR) image with a thin membranous aq-ueductal stenosis (AS), an appealing ideais to simply open the membrane and rees-tablish normal flow through the aqueduct(5, 7, 9-12). However, long-term results
f endoscopic aqueductoplasty (EAP)ave not been as successful as one wouldxpect (6, 8-12). This report discusses an-tomical variations of aqueductal steno-is, the surgical technique of aqueducto-lasty and stenting, long-term results andomplications, and finally concludes onhe correct indication for endoscopic aq-eductoplasty (with stenting).
LASSIFICATION OF AQUEDUCTALTENOSIS
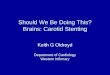
mpirically, we divide aqueductal stenosisnto 3 subtypes (Figure 1). The first type isS caused by a small transverse membrane
eading to a proximal ampullar dilation ofhe prestenotic aqueduct. This is the case
Key words� Endoscopic aqueductoplasty� Isolated fourth ventricle� Stenting
Abbreviations and AcronymsAS: Aqueductal stenosisEAP: Endoscopic aqueductoplastyETV: Endoscopic third ventriculostomyMR: Magnetic resonance
Department of Neurosurgery, Ernst MoritzArndt Universität Greifswald,
Greifswald, Germany
To whom correspondence should be addressed:Michael J. Fritsch, M.D., Ph.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2013) 79, 2S:S20.e15-S20.e18.http://dx.doi.org/10.1016/j.wneu.2012.02.013
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter © 2013 Elsevier Inc.All rights reserved.
hen it is appealing to simply open the c
WORLD NEUROSURGERY 79 [2S]: S20.e1
ransverse membrane to reestablish CSFow. However, in our experience, patientsave a reclosure rate of up to 40% (6).herefore, endoscopic third ventriculos-
omy (ETV), with a higher long-term suc-ess rate and less risk for the patient, woulde the better alternative.
The second subtype of AS is tumor or cystssociated. Tumors or cysts obstruct the aq-educt either by secondary compressione.g., tumor from the pineal region) or byirect obstruction (e.g., tectal glioma). Weealize that all of the aqueductoplasties willeclose within a short time postoperatively,nd the placement of a stent is too danger-us (risk of via falsa). Therefore, we con-ider tumor biopsy (if possible) and ETV asbetter choice for treatment.The third type of aqueductal stenosis
s the isolated fourth ventricle. Here we findhe radiographic picture of an AS combinedith occlusion of the foramina of Luschkae
nd Magendi leading to a cystic dilation ofhe isolated fourth ventricle. The brainstems compressed against the clivus and theerebellum against the tentorium. Patientsll share the same medical history: post-emorrhagic or postmeningitic hydroceph-lus within the first year of life, early place-ent of a ventriculoperitoneal shunt, and
� OBJECTIVE: This paper discusses iscopic aqueductoplasty with stenting.
� METHODS: We review and summacopic aqueductoplasty gained overatients.
RESULTS: Endoscopic aqueductopladure. In well selected patients, it proAqueductoplasty alone has a high rec
� CONCLUSIONS: Aqueductoplasty wthe treatment of isolated fourth veaqueductal stenosis should be treated
linical and radiographic signs of over- T
5-S20.e18, FEBRUARY 2013 www.WOR
rainage. Subsequently, AS and isolatedourth ventricle will develop.
In our experience, patients with an iso-ated fourth ventricle are the best candi-ates for EAP and stenting. Aqueducto-lasty is establishing a communicationetween the formerly isolated ventricularompartments, and the stent is mandatoryo keep the communication open and avoideclosure (1-3).
NDICATION
embranous AS and tumor-associated AShould be treated by ETV. The best candi-ates for EAP with stenting are patientsith symptomatic isolated fourth ventricle.e also must mention that aqueductoplasty
nd stenting are not surgical techniquesrimarily to treat hydrocephalus but toommunicate formerly isolated ventricularompartments with each other.
ECHNIQUE
reoperative Evaluation and SurgicallanningR imaging is the most important first step
or evaluating a patient (7). In addition to
ations for and the technique of endo-
the clinical experience with endo-last 15 years on pediatric and adult
with stenting presents a safe proce-s a long-term, stable clinical course.re rate and should be avoided.
tenting is the procedure of choice forle. Membranous and tumor-relatedendoscopic third ventriculostomy.
ndic
rizethe
styvidelosu
ith sntricby
2-weighted axial images, we recommend
LDNEUROSURGERY.org S20.e15

AteicdsiCisH
ntpt
tatamvt
STpnhscca1oifvoitw
ctemptrv3
stswst
stltflAsttft
h isol
PEER-REVIEW REPORTS
MICHAEL J. FRITSCH AND HENRY W. S SCHROEDER ENDOSCOPIC AQUEDUCTOPLASTY AND STENTING
sagittal T2-weighted images, which on oneside display anatomical structures, includ-ing membranes, very precisely (e.g., 3-dimensional constructive interference insteady-state) and on the other side displayflow through the aqueduct and within theventricular system (e.g., inversion recoveryturbo spin echo). Additionally, it is helpfulto obtain a coronal image to allow betterevaluation of the foramina of Monro andthe trajectory for the endoscopic approach.
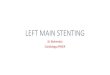
For the endoscopic procedures, we usethe LOTTA ventriculoscope (4) manufac-tured by Karl Storz G.m.b.H. & Co. KG,Tuttlingen, Germany (Figure 2). For orien-tation in the ventricles and for positioningof the trocar, the 6° working optic is used.
Figure 1. Sagittal T2-weighted magnetic resonancstenosis. (A) First type, distal membranous aqueassociated AS. (C) Third type, AS associated wit
Figure 2. LOTTA endoscopy system an
S20.e16 www.SCIENCEDIRECT.com
dditionally, 30° or 45° optics can be usedo visualize surrounding structures or thentry of the aqueduct. Additionally, the flex-ble scope, following the “two in one” con-ept, can be used to go through the aque-uct and explore the fourth ventricle. For allurgeries, we use a pneumatic self-retain-ng holding device (Pointsetter, Mitakaorp., Tokyo, Japan), HD camera and mon-
tor (Karl Storz G.m.b.H. & Co. KG), and inelected cases neuronavigation (BrainLAB,eimstetten, Germany).Aside from individual approach plan-
ing, one can generalize that the approacho the aqueduct is different from the ap-roach for an ETV. The burr hole must be 3
o 5 cm anterior to the coronal suture, and
ge showing 3 different types of aqueductall stenosis (AS). (B) Second type, tumor-ated fourth ventricle.
od set-up in the operating room.
WORLD NEUROSURGERY, http://d
herefore usually just behind the hairline. Itlso is slightly more medial than a conven-ional burr hole in order to allow a straightxis from the burr hole through the fora-en of Monro to the median posterior third
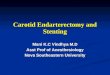
entricle. Navigation is helpful to plan thisrajectory (Figure 3).
urgical Techniquehe patient is placed supine. The head isositioned in a horseshoe head rest unlessavigation is used. With navigation, theead is fixed in a 3-pin head clamp. A smalltraight or curved skin incision is made ac-ording to the planning of the trajectory. Theurved incision has the advantage of coveringburr hole reservoir. The burr hole should be
0 mm in size to allow tilting and movementf the endoscope. It is helpful to remove the
nner table of the cranial bone to have morereedom for tilting. After dura opening, theentricular system is approached using a Scottr Cushing cannula. The endoscopic sheath is
ntroduced into the ventricular system withhe trocar. After removal of the trocar, theorking scope is introduced.After orientation within the ventricle and
areful passage of the foramen of Monro,he posterior aspect of the third ventricle isxplored. The typical anatomical land-arks are the entry into the aqueduct, the
osterior commissure, the pineal recess,he habenular commissure, the suprapinealecess, and the posterior roof of the thirdentricle (the latter usually seen only with a0° or 45° scope).
The positioning of the endoscopic sheathhould bring the opening of the aqueduct intohe center of the endoscopic field. If neces-ary, a 30° optic can be used. After fixationith the aid of the holding device, the endo-
copic sheath is not moved until the aqueduc-oplasty has been completed.
The obstructed aqueduct is carefully in-pected. The stenosis can be opened by gen-le passage of a noninflated 3-F Fogarty bal-oon catheter. Once the catheter has passedhe short aqueductal stenosis, it can be in-ated (much less compared with an ETV).fter removal of the balloon catheter, in-pection of the aqueduct and the fourth ven-ricle should be performed to ensure that arue communication between third andourth ventricles has been achieved. If therajectory is straight and the aqueduct is
e imaducta
pen wide enough, a rigid 0° or 30° scope
x.doi.org/10.1016/j.wneu.2012.02.013

toaL
hp
wdfnldt
tmwtcvhgvaithwstodo
proach
PEER-REVIEW REPORTS
MICHAEL J. FRITSCH AND HENRY W. S SCHROEDER ENDOSCOPIC AQUEDUCTOPLASTY AND STENTING
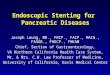
can be used. Alternatively, a flexible scopecan be used (Figure 4).
The anatomical landmarks within thefourth ventricle are anteriorly the floor of
Figure 3. Navigation for planning of the ap
Figure 4. Example of aqueductal stenting in a15-month-old boy with progressivelyenlarging isolated fourth ventricle. (A)Constructive interference in steady-state(left) and inversion recovery turbo spin echo(right) sagittal magnetic resonance imageshowing the enlarged and isolated fourthventricle. Endoscopic views. (B) Opening ofthe aqueduct using a balloon catheter. (C)Inspection of the dilated fourth ventriclethrough the aqueduct. (D) Final inspection ofthe positioned stent, which is coming fromthe aqueduct through the foramen of Monrointo the lateral ventricle. (E) Inversionrecovery turbo spin echo sagittal magnetic
resonance image obtained 2 weeks after surgery shWORLD NEUROSURGERY 79 [2S]: S20.e1
he ventricle (the rhomboid fossa), inferi-rly and medially the foramen of Magendi,nd laterally on both sides the foramina ofuschkae. The cerebellum, the cerebellar
as well as for intraoperative orientation.
owing a decrease in the size of the fourth ventricle a
5-S20.e18, FEBRUARY 2013 www.WOR
emispheres, and the vermis can be seenosteriorly.
After communication is confirmed, theorking endoscope is reintroduced and un-er direct vision the stent is inserted into theourth ventricle through the working chan-el. As stent we use a conventional 15-cm-
ong ventricular catheter, which is intro-uced with the aid of a grasping forceps or
he small Decq forceps.It is of utmost importance that the cathe-
er has additional side holes allowing com-unication between the proximal part,hich will be positioned in the fourth ven-
ricle, and the distal part, which will be lo-ated in the third ventricle and the lateralentricles. We make these additional sideoles with small scissors or a small ron-eur. The catheter is placed under directision into the fourth ventricle through thequeduct for a length of 2 to 4 cm depend-ng on the anatomy of the patient. Withinhe aqueduct, there should be no additionalole. After proper placement, the forcepsill be removed and the positioning of the
tent can be reevaluated with the aid of ei-her a flexible scope or a small 0° inspectionptic. The stent should lead from the aque-uct via the third ventricle and the foramenf Monro to the lateral ventricle. The stent is
nd the correct position of the stent.
LDNEUROSURGERY.org S20.e17

faMtE
1
1
1
Cc
R
Ch
J
A
1
PEER-REVIEW REPORTS
MICHAEL J. FRITSCH AND HENRY W. S SCHROEDER ENDOSCOPIC AQUEDUCTOPLASTY AND STENTING
fixated on a burr hole reservoir to preventstent migration. The reservoir allows pres-sure measurement, removal of CSF for di-agnostic and therapeutic purposes, andconnection to a conventional shunt systemusing the stent as proximal ventricularcatheter.
COMPLICATIONS AND RESULTS
Possible complications of aqueductoplastyand stenting include infection, ventriculi-tis, subdural hygroma, dysconjugate gaze,oculomotor and trochlear palsy, as well asstent migration. The overall revision ratewithout stenting is higher than 50% due toreclosure of the aqueduct. After experienc-ing migration of 4- and 5-cm stents, wehave established the technique of utilizing along stent measuring 12 to 14 cm and con-nected to a burr hole reservoir. In well-se-lected patients, aqueductoplasty with sub-sequent stenting provides a long-termstable clinical course and good communi-cation between the formerly isolated fourthventricle and the remaining ventricular sys-tem, with a success rate of 80% to 85%.
CONCLUSIONS
Aqueductoplasty with stenting is the proce-
dure of choice for the treatment of isolatedS20.e18 www.SCIENCEDIRECT.com
ourth ventricle. Aqueductoplasty alone hashigh reclosure rate and should be avoided.embranous and tumor-related aqueduc-
al stenosis should be primarily treated byTV.
REFERENCES
1. Fritsch MJ, Manwaring KH: Endoscopic stenting inaqueductal stenosis. In Hellwig D, Bauer BL, eds.Minimally invasive techniques for neurosurgery—current status and future perspectives. Springer,1997:87-92.
2. Fritsch MJ, Kienke S, Mehdorn HM: Endoscopic aq-ueductoplasty: stent or not to stent? Childs NervSystem 20:137-142, 2004.
3. Fritsch MJ, Manwaring KH, Kienke S, MehdornHM: Endoscopic treatment of isolated fourth ventri-cle in children. Neurosurgery 55:372-379, 2004.
4. Schroeder HWS: A new multipurpose ventriculo-scope. Neurosurgery 62:489-492, 2008.
5. Schroeder HWS, Gaab MR: Endoscopic aqueducto-plasty—technique and results. Neurosurgery 45:508-518, 1999.
6. Schroeder HWS, Oertel JMK, Gaab MR: Endoscopicaqueductoplasty in the treatment of aqueductal ste-nosis. Childs Nerv Syst 20:821-827, 2004.
7. Schroeder HWS, Oertel J, Gaab MR: Endoscopictreatment of cerebrospinal fluid pathway obstruc-
tions. Neurosurgery 60(suppl 1):ONS-44-ONS-52,2007. AWORLD NEUROSURGERY, http://d
8. Schroeder HWS, Schweim C, Schweim KH, GaabMR: Analysis of aqueductal cerebrospinal fluid flowafter endoscopic aqueductoplasty using cine phase-contrast magnetic resonance imaging. J Neurosurg93:237-244, 2000.
9. Da Silva LR, Cavalheiro S, Zymberg ST: Endoscopicaqueductoplasty in the treatment of aqueductal ste-nosis. Childs Nerv Syst 23:1263-1268, 2007.
0. Sagan LM, Kojder I, Poncyljusz W: Endoscopic aq-ueductal stent placement for the treatment of atrapped fourth ventricle. J Neurosurg 105:275-280,2006.
1. Ersahin Y: Endoscopic aqueductoplasty. Childs NervSyst 23:143-150, 2007.
2. CinalliG, Spennato P, Savarese L, Ruggiero C, Alib-erti F, Cuomo L, Cianciulli E, Maggi G: Endoscopicaqueductoplasty and placement of a stent in the ce-rebral aqueduct in the management of isolatedfourth ventricle in children. J Neurosurg 104:21-27,2006.
onflict of interest statement: Henry W. S. Schroeder is aonsultant to Karl Storz GmbH, Tuttlingen, Germany.
eceived 18 August 2011; accepted 02 February 2012
itation: World Neurosurg. (2013) 79, 2S:S20.e15-S20.e18.ttp://dx.doi.org/10.1016/j.wneu.2012.02.013
ournal homepage: www.WORLDNEUROSURGERY.org
vailable online: www.sciencedirect.com
878-8750/$ - see front matter © 2013 Elsevier Inc.
ll rights reserved.x.doi.org/10.1016/j.wneu.2012.02.013
![Annals of Clinical Case Reports Case Report · followed by the management of complications [3,4]. We report the efficacy of endoscopic stenting for the anastomotic stricture of hepaticojejunostomy](https://img.pdfslide.us/doc/110x75/5e676878f8cb0a5976739dfb/annals-of-clinical-case-reports-case-followed-by-the-management-of-complications.jpg)


![The Current Role of Endoscopic Stenting in Upper ...cdn.intechopen.com/pdfs/43563/InTech-The_current_role_of...possibility.[10] In patient with advanced esophageal cancer with very](https://img.pdfslide.us/doc/110x75/5e48447b3f02b349e235ab3a/the-current-role-of-endoscopic-stenting-in-upper-cdn-possibility10-in.jpg)















![Bifurcation and Left Main Stenting[1]](https://img.pdfslide.us/doc/110x75/5466ba34b4af9ffd748b4bcf/bifurcation-and-left-main-stenting1.jpg)