Embed Size (px)
Citation preview

New Zealand Endodontic Journal Vol 25 November 1999
EndodonticJournalVol 25 November 1999 ISSN 0114-7722
New
Zea
land
Contents21 The use of tissue regenerative techniques in Lara Ralph healing alveolar bone loss of endodontic origin Robert Love
32 Ledermix or Calcium Hydroxide for the Treatment of Endodontic Pathology Fiona Manson
36 Endodontic Publications 37 International Literature
39 Society News
New Zealand Societyof Endodontics (Inc)
PresidentHarish Lala3 Ely AvenueRemueraAuckland
SecretaryPeter Cathro120 Remuera RoadRemueraAuckland
TreasurerRichard Ellis6/128 Hurstmere RoadTakapunaAuckland
Journal EditorRobert LoveUniversity of OtagoSchool of DentistryPO Box 647Dunedin
Front Cover: Guided tissue regeneration using a non-resorbable membrane as an adjunct in strip perforation repair. (Reproduced with permission from G. K. Silver/R. M. Love)
GUNZ ADVERT

Editorial Notices
The New Zealand Endodontic Journal is published twice yearly and sent free to members of the New Zealand Society of Endodontics (Inc). The subscription rates for membership of the Society are $28.15 per annum in New Zealand or $30 plus postage for overseas members. Graduates of the University of Otago School of Dentistry enjoy complimentary membership for the first year after graduation. Subscription inquiries should be sent to the Honorary Secretary, Dr Peter Cathro, 120 Remuera Road, Auckland. Contributions for inclusion in the Journal should be sent to the Editor, Dr Robert Love, PO Box 647, Dunedin. Deadline for inclusion in the May or November issue is the first day of the preceding month. All expressions of opinion and statements of fact are published on the authority of the writer under whose name they appear and are not necessarily those of the New Zealand Society of Endodontics, the Editor or any of the Scientific Advisers.
Information for AuthorsThe Editor welcomes original articles, review articles, case reports, views and comments, correspondence, announcements and news items. The Editor reserves the right to edit contributions to ensure conciseness, clarity and consistency to the style of the Journal. Contributions will normally be subjected to peer review. It is the wish of the Editor to encourage prac-titioners and others to submit material for publication. Assistance with world processing and photographic and graphic art production will be available to authors.
Arrangement
Articles should be typewritten on one side of A4 paper with double spacing and 3cm margins. The author’s name should appear under the title and name and postal address at the end of the article. If possible, the manu-script should also be submitted on computer disc, either Macintosh or PC compatible.
References
References cited in the text should be placed in parenthesis stating the authors’ names and date, eg (Sundqvist & Reuterving 1980). At the end of the article references should be listed alphabetically giving surnames and initials of all authors, the year, the full title of the article, name of periodical, volume number and page numbers.
The form of reference to a journal article is:Sundqvist G, Reuterving C-O (1980) Isolation of
Actinomyces israelii from periapical lesion. Journal of Endodontics 6, 602-6
The form of reference to a book is:Trowbridge HO, Emling RC (1993) Inflammation,
4th edn, pp 51-7. Chicago, USA: Quintessence Publishing Company Inc.
Illustrations
Illustrations should be submitted as clear drawings, black & white or colour photographs and be preferably of column width. Radiographs are acceptable. However a black & white photograph is preferred. Illustrations must be numbered to match the text and bear the author’s name and an indication of the top edge on the back. Legends are required for all illustrations and should be typewritten on a separate page.
New Zealand Endodontic Journal Vol 25 November 1999

New Zealand Endodontic Journal Vol 25 November 1999 Page 21
The use of tissue regenerative techniques in healing alveolar bone loss of endodontic origin
Lara Ralph and Robert M Love
IntroductionAlveolar bone loss of endodontic origin is a result of infection gaining access to the root canal system via the crown or periodontium, or by iatrogenic damage to the supporting tissues (eg canal per-foration during the course of conventional root canal treatment. The regeneration of bone following destruction by pathological processes has an important clinical significance for tooth retention and function within the dentition. Much of the research on regeneration techniques comes from the periodontal literature where the ultimate goal of treatment has been restoration of alveolar bone, periodontal ligament and cementum. Such tech-niques have the potential to be applied to the field of endodontics where the aim of healing is by re-generation of periapical structures. In order to evaluate these techniques a sound knowledge of periapical tissue healing is required.
Healing following endodontic treatmentIntracanal infection is implicated as the primary etiologic factor in apical periodontitis (Kakehashi et al., 1965; Sundqvist, 1976; Möller et al., 1981). Root canal treatment aims at eliminating infection from the root canal system by means of chemo-mechanical debridement and preparation. This is followed by obturation of the root canal to limit growth of residual bacteria and impede invasion of bacteria into the root canal by coronal micro-leakage. When root canal treatment is employed according to accepted clinical principles and under aseptic conditions the success rate is high. Most follow-up studies on endodontic therapy report overall success rates of around 85-90% (Strindberg 1956; Kerekes & Tronstad, 1979, Sjögren et al., 1990). Successful healing of a periapical lesion usually occurs by regeneration of periapical bone and periodontium. This is characterized by a gradual reduction and resolution of the periapical radiolucency on subsequent follow-up radiographs
(Strindberg, 1956; Sjögren et al., 1990; Sjögren et al., 1997). Regeneration of tissue is defined as a reproduction or reconstitution of a lost or injured part in such a way that the architecture and function of the lost or injured tissue are completely restored (Glossary of Periodontal Terms 1992). Thus, regen-eration of the periodontal supporting apparatus (periodontium) includes reformation of cementum, periodontal ligament and alveolar bone.
Strindberg (1956) provided strict radiographic criteria for successful healing which has been adopted and used in later studies. In this classical study, Strindberg (1956) radiographically followed up teeth that he had completed endodontic therapy on for up to 10 years after treatment. Treatment was classified successful when: 1) the width and structure of the apical lamina dura was within normal limits; or 2) the periodontal contours were widened only around an excess of filling material. Cases in which these criteria were not met were judged unsuccessful. Strindberg’s work provided fundamental data on healing patterns and the minimum length of observation period required to evaluate the outcome of endodontic treatment. He suggested that healing is a sign that the balance between the irritants and the host defence is tipped positively in favour of the latter. However, he also said that a reduction in the radiographic size of the apical lesion is no guarantee for eventual complete healing. Most lesions resolved within 4-5 years after therapy, although some cases took as long as ten years to heal. The size of the preoperative lesion had no influence on the outcome of treatment ex-cept if it was a retreatment, where larger lesions had a lower rate of healing.
Endodontic treatment failure after several years cannot be discounted. Studies with observation periods less than four years may include cases which have not attained a stable periapical condition, and so the results may be erroneous. Later studies by Bryström et al. (1987), Sjögren et al. (1990), and Ørstavik (1996) support the 4-5 year observation period for healing. Furthermore, Ørstavik (1996) went on to suggest that the process of healing could be diagnosed earlier. Five hundred and ninety nine

Page 22 New Zealand Endodontic Journal Vol 25 November 1999
The use of tissue regenerative techniques
roots with and without preoperative chronic apical periodontitis were root canal treated and followed up for 4 years. He reported that 88% of roots with preoperative chronic apical perio-dontitis (CAP) showed signs of healing after endodontic treatment. In some instances complete healing of CAP required 4 years for completion however, radiographic signs of initiated, but incomplete healing, were visible in at least 89% of all healing roots after 1 year.
The host response to bacterial infection of the dental pulp is inflammation. The inflammatory process and bacterial products result in tissue damage. Porphyromonas gingivalis and Porphyro-monas endodontalis are very efficient at causing tissue destruction via the liberation of bacterial products (eg endotoxins, lipopolysaccharides) and activation inflammatory mediators (eg Interleukin-1, Tumour Necrosis Factor, Prostaglandin-E2). Although referred to as a lesion, periapical pathoses actually represent a protective host response. The periapical lesion is more than an accumulation of inflammatory cells. In chronic inflammation where there is concomitant destruction and repair, inflam-matory cells as well as fibroblasts and endodothelial cells are present walling off the area and preventing widespread infection. This functions to limit the infection to the root canal system. The periapical inflammatory process is initiated by the periodontal ligament cells and enlarges at the expense of alveolar bone supporting the tooth (Stashenko 1990).
After intracanal infection is removed resolution of periradicular lesions results with specific changes in the inflammatory cells. The destructive phase decreases with an increase in T suppressor cells, and decrease in T helper cells (Torabinejad & Kettering, 1985). At the same time the healing phase increases with activity of tissue forming cells (fibroblasts and endothelial cells). Tissue organ-isation and maturation ensue. Bone that has been resorbed is replaced by new bone; resorbed cemen-tum and dentine are repaired by cellular cementum. The periodontal ligament, which is the first tissue affected, is the last to be restored to normal archi-tecture (Fouad et al., 1993).
Complete regeneration of periapical structures does not always occur. Repair by dense fibrous connective tissue, may occur under certain con-ditions. Nair et al. (1999) suggested that healing after conventional root canal treatment might result in a periapical scar, rather than regeneration, which may be indistinguishable from a periapical radio-lucency seen in failed endodontic treatment.
In this study, six teeth that had conventional root canal treatment or retreatment that demonstrated non-resolving periapical radiolucencies underwent periapical surgery. Biopsies were obtained and ana-lysed descriptively by correlative light and trans-mission electron microscopy for general features and microbial findings. In 2 biopsies, the histologic features were in accordance with a periapical scar. The radiolucent areas were composed of dense collagenous fibre bundles with no signs of inflam-mation. These histological findings of fibrous repair were consistent with another histopathologic study in which periapical scars were diagnosed at apices of conventionally root filled teeth (Bhaskar 1966).
Scar healing is characteristically observed after periapical surgery (Rud et al., 1972a) and especially related to through-and-through lesions involving the destruction of both cortical plates eg. following periapical surgery on upper lateral incisors where there has been perforation of the palatal cortical plate (Hjörting-Hansen & Andreasen, 1971). Radiographically, scar healing following periapical surgery and through-and-through lesions presents as a decreasing rarefaction with an irregular outline extending angularly into the periodontal space. The rarefaction may be located asymmetrically in relation to the root apex with or without visible internal bone structures. Further healing may include the forming of a lamina dura around the apex, separating the rarefaction from the tooth (Rud et al., 1972b). Molvern et al. (1996) followed 24 cases treated by periapical surgery, which at 2-6 years after surgery were classified as incompletely healed (scar tissue). After 8-12 years observation 22 cases were still recorded in the same healing group. These findings suggested that cases clearly showing features of incomplete healing (scar tissue) at 1 year follow-up after surgery can be regarded as successes.
Periapical surgery is required when conventional orthograde endodontics is not successful or not likely to be successful. Teeth with clinical and radiographic signs of periapical inflammation, despite endodontic procedures which have been thoroughly undertaken to eliminate bacteria, can be regarded as having a persistent infection. Factors that have been identified as contributing to chronic endodontic failure include the following: intra-radicular infection persisting in the apical root canals of root filled teeth (Nair et al., 1990a); extra-radicular infection, generally in the form of peri-apical actinomycosis (Sjögren et al., 1988); extruded root canal filling or other materials that cause foreign body reactions (Nair et al., 1990b;

The use of tissue regenerative techniques
New Zealand Endodontic Journal Vol 25 November 1999 Page 23
Koppang et al., 1989); and true cysts (Nair et al., 1993). Of these, only intraradicular infection can be resolved with conventional retreatment. The other factors are located outside the root canal in the periapical tissues and necessitate periapical surgery to optimize healing.
Periapical surgery requires reflection of a mucoperiosteoal flap to gain access to the periapical tissues, exposure of the root end by removal of bone, curettage of infected and inflammatory tissue surrounding the root and alveolar bone. Most commonly this is followed by apical root resection, root-end preparation and retrograde obturation of the root canal. Successful postsurgical excisional wound healing following periapical surgery entails dentoalveolar healing (i.e. re-establishment of an apical attachment apparatus) and alveolar healing (i.e. osseous repair of trabecular and cortical bone). Efforts should be made to maintain root-attached connective tissue at the time of flap elevation in order to enhance connective tissue reattachment. Early connective tissue reattachment is the most predictable means of preventing excessive apical migration of the epithelium (Harrison & Jurosky 1991).
After closure if the surgical wound the bone cavity becomes filled with a coagulum, although the coagulum does not promote bone healing, as in the healing of the flap, it does provide a framework for healing to occur. Granulation tissue emanating from the severed periodontal ligament (PDL) and endosteum proliferate into the coagulum and are responsible for repair of the excisional wound. The PDL-derived tissue is primarily re-sponsible for dentoalveolar healing and endosteal-derived tissue is primarily responsible for osseous healing. Proliferation of granulation tissue from the severed PDL is observed at 4 days and by 8 days it completely encapsulates the root ends. This initiates reformation of the apical dentoalveolar apparatus. At 3-4 days, outgrowths of endosteal tissues from the surfaces of the bone cavity begin proliferating into the coagulum and within a short time surround the granulation tissue at the root end. The pluripotential, undifferentiated ectomesenchy-mal cells, young fibroblasts, and fibroblast-like cells are derived from both the periodontal ligament and the endosteum. These cells differentiate into functional fibroblasts, which synthesize ground substance and collagen, and cementoblasts and osteoblasts, which initiate new cementum and bone formation respectively (Craig & Harrison, 1993). Formation of cementum begins at the root periphery and proceeds centrally towards the root
canal and the new apical periodontal ligament fibers become functionally orientated between cementum and bone (Andreasen & Rud, 1972b).
Formation of new bone within the excisional wound begins internally and progresses externally towards the former cortical plate. As the more external woven bone trabeculae are formed in contact with the endosteal tissue of the cortical plate, the latter tissue becomes a functioning peri-osteum. Craig & Harrison (1993) suggested that endosteal-derived new bone may be necessary to induce a functioning periosteum and to induce the encapsulating tissue to initiate the osteogenic activity of a functioning PDL.
Craig & Harrison (1993) evaluated the effect of demineralisation of resected root ends with 50% citric acid on wound healing following periapical surgery. Microscopic evaluation at post-surgical intervals ranging from 4-45 days revealed that the demineralised root ends were associated with more rapid and complete healing than the non-demineralised root ends. They proposed that de-mineralisation enhances cementogenesis, the key to dentoalveolar healing, by removing the smear layer barrier and exposing the organic component (collagen fibrils) of resected cementum and dentine. In contrast, alveolar healing was not totally depen-dent on cementogenesis with osseous repair pro-gressing in both experimental and control groups.
The histological events in periapical healing in humans after endodontic surgery studied by Andreasen and Rud (1972a) from 70 biopsy speci-mens. They reported three different types of re-sponses: 1) healing with reformation of the perio-dontal membrane; 2) healing with scar tissue and varying degrees of inflammation; 3) moderate or severe inflammation without scar tissue. The third type of tissue response is considered endodontic failure with an absence of healing due to either presence of infection or foreign body. The size of the lesion may be a critical factor, because the dis-tance between soft and hard tissues will determine which kind of tissue is formed. If fibrous tissue is formed first, it will probably act as a barrier to prevent further bone formation. This is especially true in lesions that have perforated both cortical plates ie. through-and-through lesions (Pecora et al., 1995).
Through-and-Through LesionsApical surgery may enhance the success of restor-ing function to certain endodontically treated teeth but when there has been complete loss of buccal cortical plate or through-and-through lesions

Page 24 New Zealand Endodontic Journal Vol 25 November 1999
The use of tissue regenerative techniques
where both cortical plates have been destroyed healing by regeneration is unlikely. Boyne et al. (1961) reported that when a bony lesion perforated the palatal or lingual cortical plate the success rate of healing by regeneration was lower than 25%. Fibrous scar tissue is often formed because the connective tissue outpaces the slower bone regeneration from the osseous part of the cavity.
Furcation or Root PerforationsFurcation or root perforations occur as a result of internal or external root resorption, carious lesions in or adjacent to the floor of the pulp chamber, or they can also be produced iatro-genically during endodontic instrumentation and post space prepara-tion. Furcal perforation during endodontic treat-ment predisposes the periapical structures to in-flammation, breakdown and eventual loss of periodontal attachment. This is often irreparable and frequently leads to tooth loss. The aim of treatment is to maintain healthy tissues against the perforation without continuing inflammation or loss of periodontal attachment.
It has been shown that a favourable prognosis is possible when a small perforation occurs at a dis-tance away from the gingival sulcus of the furcation area and when it is repaired immediately via an intracoronal approach (Nicholls 1962; Pitt Ford et al., 1995). Prognosis is largely determined by the crucial role of infection. Surgical treatment of perforations can often lead to loss of periodontal attachment, chronic inflammation, and furcal pocket formation (Oswald 1979).
Repair materials must be biocompatible and have a good ability to seal against bacterial leakage. Cavit, zinc oxide-eugenol, SuperEBA, calcium hydroxide, amalgam, gutta-percha, glass ionomer, tricalcium phosphate and hydroxyapatite have been used. Re-establishment of tissue attachment has not proved possible with these current materials. More recently mineral trioxide aggregate (MTA) used as a repair material in endodontic surgery has shown histologic evidence of bone, cementum, and periodontal ligament regeneration (Torabinejad et al., 1993).
Endodontics & PeriodontologyThe fact that the periodontium is anatomically interrelated with the dental pulp by virtue of apical foramina and lateral canals creates pathways for exchange of noxious agents between the two tissue compartments when either or both of the tissues
are diseased. Pathologic changes of pulpal origin are not
always confined to the apical tissues but may mimic a periodontal problem, as such, accurate diagnosis of the origin of the lesion is crucial to treatment outcomes. Lesions may be of primary endodontic origin, primary periodontic origin or a true com-bined lesion. A combined lesion represents two separate processes, endodontic and periodontal lesions that have developed independently.
Endodontic-Periodontal LesionsIrritants from a necrotic pulp can induce pathologic alterations in the periodontium. As a result of an endodontic lesion, the periodontium is replaced by inflammatory connective tissue however, following successful root canal treatment, these pathological changes generally disappear with the periodontium regenerating to normal. There may not be perma-nent loss of the connective tissue attachment to the root surface. This is in contrast to periodontal detachment and loss during periodontal diseases. However, longstanding endoperio pockets may not heal due to the fact that periodontal bacteria may have colonised the root surface and pocket, and initiated a periodontal lesion.
Endodontic infection has been shown to augment periodontal attachment loss on periodontally prone individuals. Jansson et al. (1995) investigated the magnitude and rate of proximal attachment loss in relation to endodontic infection in periodontally involved teeth over a 3-year observation period. Teeth in periodontitis-prone patients with pro-gressive periapical pathology indicating root canal infection were found to lose comparatively more radiographic attachment (3-fold amplification) than teeth with no signs of periapical pathology or teeth with extensive periapical destruction, which had subsided during the observation period. This finding was consistent with earlier studies which found that periodontally involved teeth were found to exhibit significantly deeper periodontal pockets, more advanced attachment loss and a higher frequency of angular defects in the presence of endodontic infection compared to their perio-dontally intact counterparts (Jansson et al., 1993). Furthermore, periapical pathology was significantly correlated with an impaired marginal healing following periodontal therapy (Ehnevid et al., 1993).
Periodontal-Endodontic LesionsThe formation of bacterial plaque on detached

The use of tissue regenerative techniques
New Zealand Endodontic Journal Vol 25 November 1999 Page 25
root surfaces following periodontal disease has the potential to induce pathologic changes in the pulp the same way as endodontic infection can affect the periodontium in the opposite direction. How-ever, studies have failed to confirm a direct cor-relation between periodontal disease and pulp tissue changes. Bergenholtz & Lindhe (1978) observed the frequency and nature of tissue changes in the pulp of teeth following an experimentally induced breakdown of the attachment apparatus. They found that 70% of root specimens exhibited no pathological pulp changes despite having lost 30-40% of periodontal attachment. Breakdown of the pulp presumably does not occur until the perio-dontal disease process involves the main apical foramen. As long as the blood supply through the apical foramen remains intact, the pulp is capable of mounting a defence response. Treatment is directed towards periodontal therapy.
Combined Endodontic-Periodontal LesionsOccasionally distinct endodontic and periodontal lesions may effect the same tooth. Radiographic-ally and clinically they may appear as one lesion. Treatment of combined endodontic and periodontal lesions is the same as if they were to occur separ-ately. Endodontic treatment should be instituted first. The part of the lesion sustained by the root canal infection can usually be expected to resolve after proper debridement and disinfection of the root canal. The second phase of treatment includes observation to determine the extent of periodontal healing resulting from endodontic treatment. Later periodontal treatment including deep scaling with or without periodontal surgery will also contribute to healing. Little or no regeneration of the attach-ment apparatus can be expected without the aid of regenerative techniques.
Materials and TechniquesVarious types of regenerative techniques have been proposed for the treatment of alveolar bone lesions of endodontic origin in conjunction with conven-tional root canal treatment, with or without peri-apical surgery. Barrier matrices, barrier mem-branes, bone grafts or bone substitutes, root conditioning, and proteins have all been suggested for use separately or in combination to enhance bone healing of these lesions.
Mineral Trioxide AggregateSubsequent to periapical surgery, regeneration of the periodontal tissues occurs over the resected root end with a reasonable degree of certainty (Craig & Harrison, 1993). Achieving predictable regenera-tion over the root-end filling material is more difficult.
Recently studies on dogs and monkeys have suggested the potential use of mineral trioxide aggregate (MTA) as a root end filling material (Torabinejad et al., 1995a; 1997), pulp capping material (Pitt Ford et al., 1996), and for the repair of furcal perforations (Pitt Ford et al., 1995). The composition of MTA has not been published, how-ever mineral oxides are reported to be responsible for the chemical and physical properties of the material (Torabinejad et al., 1995b). The sealing ability of MTA has been shown by dye and bacterial leakage studies to be superior to that of amalgam, IRM, or SuperEBA (Torabinejad et al., 1994) and it is biocompatible with host tissues (Torabinejad et al., 1995a; 1997; Pitt Ford et al., 1995).
Use of MTA as a Root-End Filling MaterialHistological findings by Torabinejad et al. (1995a) showed that the application of MTA as a root-end filling material does not prevent re-generation of dental and osseous tissues, and may induce cementoblasts to produce matrix for cementum formation over MTA. This activation of cementoblasts may be caused by its sealing ability (Torabinejad et al., 1993), its high pH (Torabinejad et al., 1995c), or the release of substances that activate cementoblasts to lay down a matrix for cementogenesis.
Torabinejad et al. (1997) investigated the response of periradicular tissues in monkeys to MTA and amalgam when used as root-end filling materials in teeth that had undergone apicectomy and were free of bacterial contamination of the root canals. The tissue response to MTA was more favourable than to amalgam, and was characterised by a lack of periapical inflammation. A thick layer of cementum was observed over five of six MTA root-end fillings and associated root end dentine. Some of the cementum surface was characterised by fiber insertion, mimicking Sharpey’s fibers, and new cementum was attached to the original cementum at the sides of the root. In contrast, all root ends filled with amalgam showed periradicular inflammation and cementum had not formed over the root-end filling material, although it was present over the cut root end.

Page 26 New Zealand Endodontic Journal Vol 25 November 1999
The use of tissue regenerative techniques
Root-End DemineralisationIt has been suggested that citric acid applied to root ends at the time of periapical surgery enhances early cementogenesis (Craig & Harrison, 1993). How-ever, Torabinejad et al. (1995a) showed the presence of cementum over > 80% of root ends filled with MTA at 10-18 weeks post-surgery, this indicates that cementogenesis occurs without demineralisation. The periodontal literature shows no clinical advantage in demineralisation of the root surface with respect to attachment (Kersten et al., 1992) and the technique may be useful but clearly not necessary for regeneration.
Use of MTA for Furcation RepairWhen treating perforations the aim is to maintain healthy tissues against the perforation without inflammation or loss of periodontal attachment. Pitt Ford et al. (1995) histologically examined the tissue response to amalgam or MTA when used to repair experimentally induced furcal perforations in dog mandibular premolar teeth. In half of the 30 teeth, the perforations were repaired immediately; the remaining perforations were exposed to salivary contamination for 6 weeks before repair. Four months after perforation repair, histological examination revealed that five of six specimens repaired immediately with MTA had cementum in continuance with the root cementum and also over the repair material. This occurred even when the material had extruded into the furcal defect, an indication of the materials biocompatability. In the specimens where repair was delayed, three of seven filled with MTA were free of inflammation, but four were inflamed. In contrast, all of the amalgam specimens were associated with inflammation both in the immediate and delayed repair groups, with an absence of cementum around the repair material. Because MTA sets in the presence of moisture, blood does not affect its sealing ability. For this reason it is not necessary to dry the perforation site or place a barrier.
BarriersThe major technical difficulty in the non-surgical repair of perforation defects is the extrusion of material into the periradicular tissues. Lemon (1992) developed the internal matrix concept in which a layer of material is placed into the defect site to create a barrier prior to placement of the repair material. Hydroxyapatite, decalcified freeze-dried bone, calcium hydroxide, plaster of Paris and sterile bovine collagen have all been advocated as matrix materials for perforation
repair. These materials are favourable because as well as provid-ing a suitable barrier to pack repair materials against, they are biocompatible and are able to be completely degraded during the repair process allowing regeneration to occur.
Plaster of Paris has been used as a bone substitute for filling defects. It acts as a space filler and its natural rate of resorption compares closely with the rate of new bone growing into the defect (Bahn, 1966). It has been used as a successful barrier for packing repair materials against and in preventing extrusion of material into defect sites (Alhadainy & Himel, 1994; Jantarat et al., 1999).
Although not published in the literature, barrier materials may have potential as an adjunct to periapical surgery in the treatment of large peri-apical lesions where there has been bicortical destruction ie. through-and-through lesions. The placement of a plaster of Paris plug in one of the cortical defects with a membrane barrier over the other would enhance both clot stabilisation and concentration of growth factors thus encouraging regeneration.
Guided Tissue RegenerationThe concept of periodontal regeneration includes the restoration of alveolar bone, periodontal ligament and cementum. The cell-type which populates the root surface first will determine whether regeneration or repair occurs. Studies in animals and humans have demonstrated that placing a barrier membrane over a periodontal bone defect allowed the selective repopulation of the root surface by periodontal ligament progenitor cells which have the potential for regeneration (Nyman et al., 1980; 1982a; 1982b; Karring et al., 1980). This is the concept of guided tissue regeneration (GTR). It uses a microporous membrane positioned to permit desirable osteogenic cells to invade the clot. The membrane acts as a physical barrier to prevent epithelial downgrowth and the formation of a long junctional epithelium or the ingrowth of connective tissue from the flap. Instead a space is created into which regenerative cells can migrate to regenerate a new attachment apparatus. In the absence of bacterial contamination this may result in new cementum, PDL and alveolar bone (Nyman et al., 1987).
In order for a barrier material to function it must meet certain design criteria. It must be biocom-patible, act as a barrier to exclude undesirable cells from entering the space and allow for tissue integration. In addition, it should provide stability to underlying blood clot and the overlying flap

New Zealand Endodontic Journal Vol 25 November 1999 Page 27
during healing (Karring et al., 1997).Barrier membranes are of two types; non-
resorbable and bioabsorbable. The use of bio-absorbable membranes are attractive because they are biocompatible with the host and do not require a second surgical procedure for their removal. Studies have compared absorbable materials to non-absorbable expanded polytetrafluoroethylene (ePTFE) in the treatment of intrabony periodontal defects. It appears that there are similar clinical results with both types of barrier (Eickholz et al., 1997). The absorbable materials which have been introduced fall into two categories based on their composition: 1) those made of collagen and 2) those composed of polylactic and polyglycolic acid polymers. Mattson et al. (1999) evaluated the regenerative potential of both types of bio-absorbable barrier membranes used in the treatment of periodontal intrabony defects and found both to be equally effective. The materials resulted in a reduction in probing depths, gain of relative attach-ment, and regeneration of bone within the osseous defect.
GTR use for Large Periapical LesionsStudies indicate the potential for the use of barrier membranes in management of large periapical lesions with or without periodontal involvement and for the treatment of recent root canal perfor-ations. Pecora et al. (1995) demonstrated the use of the GTR principle for the treatment of large periapical lesions. Periapical surgery was per-formed on twenty patients with large endodontic lesions, which had failed to respond to conventional endodontic treatment. In 10 test sites PTFE mem-branes (Gortex) were placed to cover the lesions, while at the control sites the lesions were not covered before resuturing. Baseline radiographs and colour transparencies were taken pre- and post-operatively and followed up every three month for one year. Radiographic analysis at six months showed an average 52% reduction in size of the periapical radiolucencies in the control group com-pared to 70% size reduction in those with the membranes. These results showed that the mem-brane barrier technique promoted more rapid healing of periapical lesions. Conversely, the con-trol defect areas without membrane demonstrated slow and sometimes incomplete healing. The time-frame to assess successful healing in this study was short and a longer observation period of 4-5 years may give a more accurate assessment of healing in the control group (Sjögren et al., 1990; Ørstavik 1996). Rankow & Krasner (1996) suggested that
the use of GTR may greatly enhance healing in large through-and-through periapical lesions where incomplete healing is frequently observed.
Pompa (1997) presented similar tissue re-generation results in a clinical retrospective study. GTR employing a Gortex membrane with and without the use of allograft demineralised bone was used for the repair of complete buccal dehiscences associated with periapical defects. GTR alone provided an effective treatment for osseous regener-ation. In addition this technique incorporated the opening of marrow spaces during periapical surgery by creating multiple perforations with the use of a surgical bur which penetrated the cortical wall or inner wall of the defect. Despite no supporting evidence, Pompa (1997) suggested that these perforations allow a rich supply of osteoprogenitor cells to the area, thus ensuring an adequate blood supply for healing and enhancing regeneration.
Although not published in the literature, the use of membranes in these large lesions of endodontic origin may enhance regeneration by enabling clot stabilisation for osteogenesis and providing a confined area for the concentration of growth factors. Dahlin et al. (1988) found that there is a clinically significant increase in the amount of growth factors (insulin growth factor and platelet-derived growth factor) that occupy the periodontal surgical defect when a membrane is overlying the area.
GTR use in Perforation RepairThe use of GTR as an adjunct to perforation repair has been proposed. Dean et al. (1997) in a study with dogs evaluated a technique that included zinc oxide-eugenol retrofill to repair molar root canal perforations and guided tissue regeneration to restore the periodontium that was removed from the furcation area for access to the sites. Some sites had the inclusion of a demineralised freeze dried bone allograft (DFDBA). The results indi-cated that membranes enhanced the bony closure of the surgical access openings after root canal perforations had been filled. The addition of a bone graft did not seem to enhance healing and failure to repair the perforation site was always associated with failure.
Salman et al. (1999) employed the use of a membrane as an adjunct to intracoronal repair. This group evaluated a bioresorbable membrane (Atrisorb) as a matrix under resin-modified glass ionomer sealants in the intra-coronal repair of furcal perforations in vivo. The membrane was placed
The use of tissue regenerative techniques

Page 28 New Zealand Endodontic Journal Vol 25 November 1999
flush with the pulp chamber floor. Histological parameters were used to evaluate the tissue re-sponse in dogs. The placement of a resorbable barrier at the pulp chamber aspect of the furcation perforation did not result in superior healing, com-pared with the use of resin-modified glass ionomer alone. Because this was an intra-coronal repair it may be that the interaction between the membrane and vital tissues was less direct than in the case of periodontal regeneration procedures.
GraftsThe periodontal literature questions the induction potential of commercially processed bone allo-grafts. The osteoinductive potential of demineral-ised freeze dried bone allograft (DFDBA) appears to be dependent on the age and health of the donor and methods of procurement (Schwartz et al., 1998). It has been reported that most commercially available DFDBA has little or no bone morphogenic protein (BMP) activity and that the graft material may act primarily by oseoconduction.
Human studies have shown that synthetic bone grafts, (alloplasts) composed of hydroxyapatite or tricalcium phosphate, placed in osseous periodontal defects resulted in no histological evidence of periodontal regeneration suggesting that the materials only function as space fillers (Froum et al., 1982; Baldock et al., 1985). Their application in endodontics is limited to use as a matrix barrier to pack gutta-percha or perforation repair materials against.
Allograft bone materials obtained from human tissue banks, specifically DFDBA and freeze-dried bone allograft (FDBA) have been evaluated clinically and histologically for their use as an ad-junct to endodontic surgery. Tseng et al. (1995) illustrated the potential of endodontic treatment, combined with GTR, and bone grafting in the treatment of a large bony lesion with an associated soft tissue fenestration. Conventional endodontic treatment was followed by apicectomy and amal-gam retrofilling. DFDBA mixed with tetracycline powder was placed in the bony cavity and a nonresorbable (GTAM, WL Gore) membrane placed to cover the graft material. The clinical course of healing was reported to be uneventful and the membrane was removed at six months. The authors reported the presence of bone regeneration with complete closure of the soft tissue fenestration. This case report illustrates the potential of com-bined endodontic therapy, GTR, and bone grafting in the treatment of large bony and soft tissue defects, however, a controlled clinical
study is required to assess whether this treatment is better in terms of healing than standard endodontic therapy. Rankow & Krasner (1996) used GTR with bone allograft (DFDBA or FDBA) as an adjunct to endodontic surgery. They found no advantage in the use of bone grafts to repair periapical defects. The authors suggest that bone allografts, although functioning as a space filler, may also serve as a physical barrier that blocks osteoblastic activity within the defect below the membrane. Pompa (1997) supported the view that a bone allograft combined with membrane is no more beneficial to healing than a membrane alone.
Bovine bone mineral is a naturally porous material that is structurally similar to human can-cellous bone but is free from organic matter and cellular components. Its osseoconductive proper-ties have been shown by McAllister et al. (1998) who used bovine bone mineral as a sinus graft for augmentation. He demonstrated new bone forma-tion with integration with host bone when bovine bone mineral was used. In a study comparing the bone regenerative capacity of porous bone mineral to biologically active glass in a large bone defect model, Schmitt et al. (1997) found significantly greater amount of newly regenerated bone in bone mineral treated sites. Nevins et al. (1998) evaluated the clinical, radiographic and histological responses to porous bovine bone mineral (Bio-Oss) when used alone or in combination with a resorbable collagen membrane (Bio-Gide) in treating perio-dontal defects in humans. The results showed that osseous defect fill, new cementum and inserting collagen fibers was possible with the use of bovine bone mineral alone. The results were enhanced when bovine bone mineral was used in combination with a collagen membrane. In sites treated with bovine bone and resorbable collagen membrane which had 11mm of attachment loss and 7mm intrabony lesions there was 7mm of new cementum and 5.3mm increase in bone height on histological evaluation of block sections. Hutchens (1999) eval-uated the use of Bio-Oss alone and in combination with a resorbable synthetic membrane (Guidor). Thirty-two periodontal intrabony defects of various sizes and morphology were surgically treated and evaluated at 6 months. There was improvement of the bony defects with gain in attachment levels. No significant difference between the use of bone mineral alone or in combination with a barrier membrane was observed. This may be related to the use of a synthetic membrane. The slow resorp-tion of collagen membranes may allow more time for the new periodontium to form in a protected
The use of tissue regenerative techniques

The use of tissue regenerative techniques
New Zealand Endodontic Journal Vol 25 November 1999 Page 29
environment (Hutchens, 1999).The favourable use of bovine bone mineral for
treatment of intrabony defects may suggest the potential for use as an adjunct to endodontic surgery where a large bony cavity exists or in the case of a true combined perio-endo lesion.
Growth FactorsGrowth factors are naturally occurring poly-peptides that exert their influences by binding to high-affinity cell membrane receptors that trans-duce signals to the cell nucleus via complex signal pathways (Regan et al., 1999). These factors stimulate a wide variety of activities, including cell proliferation, differentiation, chemotaxis, migration and formation of extracellular matrix proteins. The application of specific growth factors has been shown to promote periodontal regeneration. Key factors that have been identified include bone morphogenic proteins (BMP’s), insulin-like growth factors (IGF’s), fibroblast growth factors (FGF’s) and platelet-derived growth factors (PDGF’s) (Howell et al., 1997).
Growth factors influence cell metabolism in different ways depending on whether they act as competence factors or progression factors. Com-petence factors (eg. PDGF and FGF) stimulate cells to move from the resting phase into the mitotic phase of the cell cycle. Progression factors eg. IGF stimulate DNA synthesis and allow competent cells to progress to completion of the cell cycle (Pardee, 1989). Combinations of competence and progres-sion growth factors are known to work syner-gistically to promote periodontal regeneration.
The use of these growth factors as an adjunct to periapical surgery may have the potential to enhance regeneration. The incorporation of the growth factors in a suitable carrier medium would ensure accurate delivery to the area and prolong their presence at the surgical site. Material sug-gested for the carrying of growth factors include collagen impregnated with the osseoconductive material tetracalcium phosphate; gels (methylcello-lose, hyaluronate); and polylactic acid resorbable membranes. These materials have potential as carriers because of their lack of toxicity and their biodegradability however early results suggest that clinical success is not yet achievable (Regan et al., 1999).
Regan et al. (1999) evaluated the healing of the periradicular tissues in dogs when exogenous growth factors were delivered to the surgical area as part of endodontic surgery. Periapical surgery was performed following conventional endodontic
treatment and it included root-end resection (api-cectomy) and root-end cavity preparation. Insulin-like growth factor in combination with platelet-derived growth factor, or fibroblast growth factor alone were immobilised on a polylactic acid carrier (Atrisorb) and then placed in the root-end prepara-tions. Using strict criteria the healing was evaluated at 60 days with regard to the presence of an inflammatory response, bone regeneration, perio-dontal ligament formation, and cementum forma-tion. The healing response was compared with controls that were filled with a conventional root-end filling material (Diaket). The use of specific growth factors did not initiate the desired peri-radicular tissue response as regeneration was significantly reduced compared to the control groups over this time frame. With regard to growth factors there remains a disparity between their effects seen in in vitro experiments compared to results in vivo, possibly because of the lack of appropriate carrier systems. It may be that the carriers are incompletely resorbed and so create a barrier to complete bone healing.
Enamel Matrix ProteinsEnamel matrix proteins secreted by Hertwig’s epithelial sheath play an important role in cemen-togenesis and also in the development of the periodontal attachment apparatus. An example of an enamel matrix protein Enamel Matrix Derivative (EMD, Emdogain), which is harvested from de-veloping pigs teeth. Emdogain consists of purified freeze-dried EMD of which the major protein is amelogenin. Heijl et al. (1997) demonstrated in a clinical trial that topical application of Emdogain onto diseased periodontal roots associated with intrabony defects during periodontal surgery pro-moted regeneration. This may suggest that adjunctive use of Enamel Matrix Derivative at the time of periapical surgery could provide an alter-native technique in the future with the potential for periapical regeneration in large periapical lesions or combine perioendo lesions. However, further carefully controlled studies are required before the technique can be adopted.
SummaryIt is desirable from both a biological and clinical standpoint to have periodontal lesions of endo-dontic origin heal by regeneration of bone, cemen-tum and periodontal ligament rather than dense connective tissue. MTA has been shown to stimulate cemental regeneration and shows promise
Page 30 New Zealand Endodontic Journal Vol 25 November 1999
The use of tissue regenerative techniques
as a regenerative repair material for furcation de-fects as well as a root-end filling material. Guided tissue regeneration principles have the potential for future development of techniques for the clinical management of large bony lesions with extensive cortical bone destruction, particularly when they encroach on the periodontium. An optimal carrier system for delivery of BMP’s and growth factors may further enhance clinical regeneration.
ReferencesAlhadainy HA, Himel VT (1994). An in vitro evaluation of
plaster of Paris barriers used under amalgam and glass ionomer to repair furcation perforations. Journal of Endodontics 20:449-452.
Andreasen JO, Rud J (1972a). Modes of healing histologically after endodontic surgery in 70 cases. International Journal of Oral Surgery 1:148-160.
Andreasen JO, Rud J (1972b). Correlation between histology and radiography in the assessment of healing after endodontic surgery. International Journal of Oral Surgery 1:161-173.
Bahn SL (1966). Plaster: a bone substitute. Oral Surgery, Oral Medicine, Oral Pathology 21:672-681.
Baldock WT, Hutchens LH, McFall WT (1985). An evaluation of tricalcium phosphate implants in human periodontal osseous defects of two patients. Journal of Periodontology 56:1-7.
Bergenholtz G, Lindhe J (1978). Effect of experimentally induced marginal periodontitis and periodontal scaling on the dental pulp. Journal of Clinical Periodontology 5:59-73.
Bhaskar SN (1966). Periapical lesion: types, incidence, and clinical features. Oral Surgery, Oral Medicine, Oral Pathology 21:657-671.
Boyne PJ, Lyon HW, Miller CW (1961). The effects of osseous implant materials on regeneration of alveolar cortex. Oral Surgery, Oral Medicine, Oral Pathology 14:369-378.
Bryström A, Happonen RP, Sjögren U, Sundqvist G (1987). Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endodontics and Dental Traumatology 3:58-63.
Craig KR, Harrison JW (1993). Wound healing following demineralization of resected root ends in periradicular surgery. Journal of Endodontics 19:339-347.
Dahlin C, Lindhe A, Gottlow J, Nyman S (1988). Healing of bone defects by guided tissue regeneration. Plastic Reconstructive Surgery 81:672-676.
Dean JW, Lenox RA, Lucas FL, Culley WL, Himel VT (1997). Evaluation of combined surgical repair and guided tissue regeneration to treat recent root canal perforations. Journal of Endodontics 23:525-532.
Ehnevid H, Jansson L, Lindskog S, Blomlöf L (1993). Periodontal healing in teeth with periapical lesions. A clinical retrospective study. Journal of Clinical Periodontology 20;254-258.
Eickholz P, Kim T-S, Holle F (1997). Guided tissue regeneration with non-resorbable and biodegradeable barriers: 6 month results. Journal of Clinical Perio-dontology 24:92-101.
Fouad AF, Walton RE, Rittman BR (1993). Healing of induced periapical lesions in ferret canines. Journal of Endodontics 19:123
Froum SJ, Kushner L, Scopp W (1982). Human clinical and histologic response to durapatite implants in intraosseous lesions. Journal of Periodontology 53:719-725.
Glossary of Periodontal Terms (1992). Third Edition. Chicago:
The American Academy of Periodontology.Harrison JW, Jurosky KA (1991). Wound healing in the tissues
of the periodontium following periradicular surgery. II. The incisional wound. Journal of Endodontics 17:425-436.
Heijl L, Heden G, Svardström G, Ostgren A (1997). Enamel matrix derivative (EMDOGAIN) in the treatment of intrabony periodontal defects. Journal of Clinical Periodontology 24:705-714.
Hjörting-Hansen E, Andreasen JO (1971). Incomplete bone healing of experimental cavities in dog mandibles. British Journal of Oral Surgery 9:33-40.
Howell TH, Fiorellini JP, Paquette DW, Offenbacher S, Giannobile WV, Lynch SE (1997). A phase I/II clinical trial to evaluate a combination of recombinant human platelet-derived growth factor-BB and recombinant human insulin-like growth factor-1 in patients with periodontal disease. Journal of Periodontology 68;1186-1193.
Hutchens LH (1999). The use of a bovine bone mineral in periodontal osseous defects: Case reports. Compendium 20:365-376.
Janarat J, Dashper SG, Messer HH (1999). Effect of matrix placement on furcation perforation repair. Journal of Endodontics 25:192-196.
Jansson L, Ehnevid H, Lindskog S, Blomlöf L (1993). Relationship between periapical and periodontal status. A clinical retrospective study. Journal of Clinical Periodontology 20:117-123.
Jansson L, Ehnevid H, Lindskog S, Blomlöf L (1995). The influence of endodontic infection on progression of marginal bone loss in periodontitis. Journal of Clinical Periodontology 22:729-734.
Kakehashi S, Stanley HR, Fitzgerald RJ (1965). The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surgery, Oral Medicine, Oral Pathology 20:340-349.
Karring Y, Nyman S, Lindhe J (1980). Healing following implantation of periodontitis affected roots into bone tissue. Journal of Clinical Periodontology 7:96-105.
Karring T, Lindhe J, Cortellini P (1997). Regenerative periodontal therapy. In Clinical Periodontology and Implant Dentistry. Third Edition. Munksgaard, Copen-hagen. Pages 597-646.
Kerekes K, Tronstad L (1979). Long-term results of endodontic treatment performed with a standardized tech-nique. Journal of Endodontics 5:83-90.
Kersten B, Chamberlain A, Khorsandl S, Wikesjü U, Selvig K, Nilveus R (1992). Healing of the intrabony periodontal lesion following root conditioning with citric acid and wound closure including an expanded PTFE membrane. Journal of Periodontology 63:876-882.
Koppang HS, Koppang R, Solheim T, Aarnes H, Stölen SO (1989). Cellulose fibers from endodontic paper points as an etiologic factor in postendodontic periapical granulomas and cysts. Journal of Endodontics 15:369-372.
Lemon R (1992). Non-surgical repair of perforation defects. Dental Clinics of North America 36:439-457.
Mattson JS, Gallagher SJ, Mansoor HJ (1999). The use of 2 bioabsorbable barrier membranes in the treatment of interproximal intrabony periodontal defects. Journal of Periodontolog y 90:510-517.
McAllister BS, Margolin MD, Cogan AG (1998). Residual lateral wall defects following sinus grafting with recombinant osteogenic protein-1 or Bio-Oss in the chimpanzee. International Journal of Periodontics and Restorative Dentistry 18:227-239.
Möller ARJ, Fabricius L, Dahlen G, Ohman AE, Heyden G (1981). Influence on the periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scandinavian Journal of Dental Research 89:475-484.
Molven O, Halse A, Grung B (1996). Incomplete healing (scar tissue) after periapical surgery- Radiographic findings 8-12
The use of tissue regenerative techniques
New Zealand Endodontic Journal Vol 25 November 1999 Page 31
years after treatment. Journal of Endodontics 22:264-268.Nair PNR, Sjögren U, Kahnberg KE, Krey G, Sundqvist G
(1990a). Intraradicular bacteria and fungi in root-filled asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. Journal of Endodontics 16:580-588.
Nair PNR, Sjögren U, Krey G, Sundqvist G (1990b). Therapy-resistant foreign-body giant cell granuloma at the periapex of a root-filled human tooth. Journal of Endodontics 16:589-595.
Nair PNR, Sjögren U, Schumacher E, Sundqvist G (1993). Radicular cyst affecting a root-filled human tooth: A long-term post-treatment follow-up. International Endodontic Journal 26:225-233.
Nair PNR, SjögrenU, Figdor D, Sundqvist G (1999). Persistent periapical radiolucencies of root-filled human teeth, failed endodontic treatments, and periapical scars. Oral Surgery, Oral Medicine, Oral Pathology 87:617-627.
Nevins M, Camelo M, Nevins M (1998). Clinical, radiographic and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. International Journal of Periodontics and Restorative Dentistry 18:3-13.
Nicholls E (1962). Treatment of traumatic perforations of the pulp cavity. Oral Surgery, Oral Medicine, Oral Pathology 15:603-612.
Nyman S, Karring T, Lindhe J, Platen S (1980). Healing following implantation of periodontics affected roots into gingival connective tissue. Journal of Clinical Periodontology 7:394-401.
Nyman S, Gottlow J, Karring T, Lindhe J (1982a). The regenerative potential of the periodontal ligament: an experimental study in the monkey. Journal of Clinical Periodontology 9:257-265.
Nyman S, Lindhe J, Karring T, Rylander H (1982b). New attachment following surgical treatment of human periodontal disease. Journal of Periodontology 9:290-296.
Nyman S, Gottlow J, Lindhe J, Karring T, Wennstrom J (1987). New attachment formation by guided tissue regeneration. Journal of Periodontal Research 22:252-254.
Ørstavik D (1996). Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. International Endodontic Journal 29: 150-155.
Oswald R (1979). Procedural accidents and their repair. Dental Clinics of North America 23:593-616.
Pardee AB (1989). G1 events and regulation of cell pro-liferation. Science 246:603-608.
Pecora G, Kim S, Celletti R, Davarpanah M (1995). The guided tissue regeneration principle in endodontic surgery: one-year postoperative results of large periapical lesions. International Endodontic Journal 28:41-46.
Pitt Ford TR, Torabinejad M, McKendry DJ, Hong C-U, Stalin P (1995). Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surgery, Oral Medicine, Oral Pathology 79:756-762.
Pitt Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP (1996). Using mineral trioxide aggregate as a pulp-capping material. Journal of the American Dental Association 127:1491-1496.
Pompa DG (1997). Guided tissue repair of complete buccal dehiscences associated with periapical defects: A clinical retrospective study. Journal of the American Dental Association 128:989-997.
Rankow H, Krasner P (1996). Endodontic applications of guided tissue regeneration in endodontic surgery. Journal of Endodontics 22:34-43.
Regan JD, Gutmann JL, Lacopino AM, Diekwisch T (1999). Response of periradicular tissues to growth factors intro-duced into the surgical site in the root-end filling material. International Endodontic Journal 32:171-182.
Rud J, Andreasen JO, Möller ARJ, Jensen JE (1972a). A
follow-up study of 1000 cases treated by endodontic surgery. International Journal of Oral Surgery 1:215-228.
Rud J, Andreasen JO, Möller ARJ, Jensen JE (1972b). Radiographic criteria for the assessment of healing after endodontic surgery. International Journal of Oral Surgery 1:195-214.
Salman MA, Quinn F, Dermody J, Hussey D, Claffey N (1999). Histological evaluation of repair using a bioresorbable membrane beneath a resin-modified glass ionomer after mechanical furcation perforation in dogs teeth. Journal of Endodontics 25:181-186.
Schmitt JM, Buck DC, Seong-Pil J (1997). Comparison of porous bone mineral and biologically active glass in critical sized defects. Journal of Periodontology 68:1043-1053.
Schwartz Z, Somers A, Mellonig JT (1998). Ability of com-mercially demineralized freeze-dried bone allograft to induce bone formation is dependent on donor age but not gender. Journal of Periodontology 69:470-478.
Sjögren U, Happonen RP, Kahnberg K-E, Sundqvist G (1988). Survivial of Arachnia propionica in periapical tissue. International Endodontic Journal 24:119-125.
Sjögren U, Hägglund B, Sundqvist G, Wing K (1990). Factors affecting the long-term results of endodontic treatment. Journal of Endodontics 16:498-504.
Sjögren U, Figdor D, Persson S, Sundqvist G (1997). Influence of infection at the time of root filling on the outcome of teeth with apical periodontitis. International Endodontic Journal 30:297-306.
Stashenko P (1990). The role of immune cytokines in pathogenesis of periapical lesions. Endodontics and Dental Traumatology 6:89-95.
Strindberg LZ (1956). The dependence of the results of pulp therapy on certain factors: An analytic study based on radiographic and clinical follow-up examinations. Acta Odontologica Scandinavica 14(Suppl 21): 1-175.
Sundqvist G (1976). Bacteriological studies of necrotic dental pulps. Umeâ: Umeâ University Publications No. 7.
Torabinejad M, Kettering JD (1985). Identification and relative concentration of B and T lymphocytes in chronic periapical lesions. Journal of Endodontics 11:122-125.
Torabinejad M, Higa RK, McKendry JD, Pitt Ford TR (1994). Dye leakage of four root-end filling materials: effects of blood contamination. Journal of Endodontics 20:109-112.
Torabinejad M, Hong CU, Lee SJ, Monsef M, Pitt Ford T (1995a). Investigation of mineral trioxide aggregate for root-end filling in dogs. Journal of Endodontics 21:603-608.
Torabinejad M, Hong CU, McDonald F, Pitt Ford TR (1995b). Physical and chemical properties of a mew root-filling material. Journal of Endodontics 21:349-353.
Torabinejad M, Falah Rastegar A, Kettering JD, Pitt Ford TR (1995c). Bacterial leakage of mineral trioxide aggregate as a root end filling material. Journal of Endodontics 21:109-112.
Torabinejad M, Pitt Ford T, McKendry DJ, Abedi HR, Miller DA, Kariyawasam SP (1997). Histologic assessment of mineral trioxide aggregate as a root-end filling in monkeys. Journal of Endodontics 23:225-228.
Tseng C-C, Chen Y-H, Huang C-C, Bowers GM (1995). Correction of a large periradicular lesion and mucosal defect using combined endodontic and periodontal therapy: a case report. The International Journal of Periodontics and Restorative Dentistry 15:377-383.
Lara Ralph and Robert M LoveUniversity of Otago School of DentistryPO Box 647, Dunedin

Page 32 New Zealand Endodontic Journal Vol 25 November 1999
Ms Manson is a final year dental student and this paper was completed as a final year exercise-editor.
IntroductionMicroorganisms play a most important role in the aetiology of pulpitis and apical periodontitis. Endodontic treatment aims to eliminate these bac-teria and their toxic products from the root canal. Complete debridement and bacterial decontamina-tion of the root is thought to be a precondition for successful repair of the apical tissues (Taylor et al. 1989).
In most instances, because of the complexity of root canal anatomy, bacteria can be detected in the root canal system even after thorough chemo-mechanical root canal instrumentation (Bystrom et al. 1983). The bacteria are mainly within dentinal tubules and canal ramifications (Abbott et al. 1988). During the period between appointments, in the absence of a root canal medicament, bacteria surviving instrumentation and irrigation have been shown to increase rapidly in number (Chong, 1992). Because of this it is one of the principles of endo-dontic therapy of nonvital teeth to use an anti-microbial medicament between appointments before placing the definitive filling material (Tepel, 1994).
Intracanal medications have also been advocated for many other reasons besides the elimination of any remaining bacteria from the root canal system (Chong et al. 1992). An intracanal medication can be used to (i) reduce inflammation of periapical tissues and pulp remnants; (ii) treat external in-flammatory root resorption; (iii) render canal con-tents inert and neutralise tissue debris; (iv) help dry persistently wet canals.
It is the aim of this paper to discuss two such intracanal dressings – calcium hydroxide and Ledermix – in terms of the advocated uses of root canal medicaments and to determine the most suitable situations in which to use them.
Calcium hydroxide is a simple, biologically acceptable chemical substance with a wide variety of uses. It is considered by many to be the best
Ledermix or Calcium Hydroxide for the Treatment of Endodontic Pathology
Fiona Mansonif not only, inter-appointment, intracanal dressing (Marais, 1996). As an intracanal medicament calcium hydroxide is used in the non-setting paste form.
Ledermix is a non-setting paste containing the tetracycline antibiotic Demethylchlortetracycline (3.2%) and the corticosteroid Triamcinolone (1%).
Antibacterial actionIn order to be effective as an antibacterial agent,
the diffusion of the intracanal dressing through the dentinal tubules is important. This is because, as mentioned above, after chemomechanical debride-ment of the root canal bacteria still remain in the dentinal tubules. Tronstad et al. (1981) demon-strated that hydroxyl ions from an intracanal calcium hydroxide dressing were able to penetrate through dentine and elevate the pH to antimicrobial levels. Similarly, Ledermix also has the ability to diffuse through dentine. This was demonstrated by Abbott et al. (1988) using corticosteroid and antibiotic tracer molecules and spectral analysis.
There is some variation in the reports of the effectiveness of calcium hydroxide as an anti-microbial agent. Chong and Pitt Ford (1992) stated that the antibacterial action of calcium hydroxide is of short duration and it is not equally effective against all bacteria found in root canals. However, other research has shown that root canals treated with calcium hydroxide become totally sterile after seven days (Sjögren, 1991). The general consensus seems to be that calcium hydroxide has good antimicrobial properties and its effects are best achieved if the calcium hydroxide remains in the root canal for at least one week after initial chemo-mechanical debridement of the canal.
The antibacterial effects of calcium hydroxide have been mainly attributed to its high pH of 12.5 (Miserindino, 1994). This high pH is reported to hydrolyse the lipid moiety of bacterial lipopoly-saccharides, rendering it incapable of producing biological effects such as toxicity, pyrogenicity, macrophage activation, and complement activation (Safavi, 1994). Researchers have suggested a

New Zealand Endodontic Journal Vol 25 November 1999 Page 33
number of alternative ways in which calcium hydroxide exerts its antimicrobial effect. These include (i) absorption of carbon dioxide resulting in nutritional starvation of various anaerobic bac-teria which require carbon dioxide for their survival (Kontakiotis, 1995) and (ii) obliteration of the root canal space which minimises the ingress of tissue exudate, a potential source of nourishment for the remaining bacteria (Ørstavik, 1990).
The antibacterial action of Ledermix is due to tetracycline, a broad spectrum antibiotic which is effective against both Gram positive and Gram negative microorganisms. Evidence suggests that at lower concentrations, tetracycline antibiotics are more effective against Gram positive than Gram negative organisms. In light of this, the effective-ness of Ledermix as an antibacterial agent has been questioned as Gram negative bacteria are the main organism in established endodontic infections. Additionally, bacteria remaining within a root canal after chemomechanical preparation are dispersed within the dentinal tubules and anatomical irregu-larities are not in direct contact with the root canal medicament, hence the concentration of the anti-biotic may not be high enough to be inhibitory to these Gram negative bacteria. Studies by Goldman and Pearson (1962) have also found that 23% of organisms isolated from root canals were resistant to tetracycline antibiotics. Another example of the apparent ineffectiveness of the tetracycline in Ledermix was demonstrated by Barker and Lockett (1971) who showed that, despite high sensitivity of S. viridans to the tetracycline component of Leder-mix, streptococci persisted in the apices of experi-mentally infected dog teeth when Ledermix paste was used as a root canal dressing even after prolonged us of the drug. They stated that “in view of this frequent ineffectiveness against sensitive organisms, and the fact that various organisms infecting human root canals are in any event insen-sitive to the tetracycline, it is apparent that Leder-mix paste is not a panacea for treatment of, and cannot be relied upon to eradicate bacteria from, infected root canals”.
Anti-inflammatory effectsand the relief of postoperative pain
Pain is primarily due to the release of chemical mediators and to a local build up in pressure due to the production of inflammatory exudate, hence the
reduction of inflammation is aimed at alleviation of pain and any acute exacerbation.
Ledermix contains a corticosteroid and is there-fore specifically used as a topical anti-inflammatory agent in root canal therapy. Corticosteroids appar-ently alter the inflammatory or vascular response sufficiently to affect pain (Walton & Rivera, 1996). The clinical usefulness of Ledermix in alleviating acute symptoms of apical periodontitis appears to be well documented by clinicians, however accord-ing to Barker and Lockett (1971) this does not necessarily denote subsidence of periapical inflam-mation. Also clinical trials of intracanal cortico-steroids by Chance et al. (1987) have found that they were only effective against post operative pain in teeth with vital pulps, but were ineffective when the pulp was infected or necrotic. It is also apparent from clinical trials by Trope (1990) that Ledermix does not reduce the incidence of endodontic flare ups (severe pain) between appointments. There-fore, in endodontic applications, the action of Ledermix seems to be minor and affects only milder degrees of pain.
According to a histological study by Tepel et al. (1994) the combination of a corticosteroid and an antibiotic, as in Ledermix, rather than promoting healing by its anti-microbial and anti-inflammatory effects in fact causes a severe reaction in the peri-apical tissues of the tooth. This study was carried out on the mesial roots of lower rat molars and supports earlier findings that Ledermix is in fact extremely toxic to fibroblasts (Taylor et al. 1989). This helps to explain why, in Tepel et al.’s study, healing did not occur and in fact the periapical lesions treated with Ledermix were notably larger than the untreated ones. This also supports studies by Barker and Lockett (1971) which showed that apical inflammation was not always counteracted by the paste.
In contrast, the same study by Tepel et al. (1994), showed that after the use of calcium hydroxide, virtually no periapical inflammation was evident and new bone had formed leading to healing of the periapical tissues. According to Fava (1992) this anti-inflammatory action of calcium hydroxide is due to three different mechanisms (i) hygroscopic action- the inflammatory exudate is absorbed by the calcium hydroxide; (ii) the formation of calcium bridges with proteins around endothelial cells- this prevents exit of exudate from the blood vessels to the tissues; (iii) phospholipase inhibition which decreases cellular lysis and hence release of prostaglandin, a mediator of inflammation.
Despite its anti-inflammatory and anti-microbial
Ledermix or Calcium Hydroxide for the Treatment of Endodontic Pathology

Page 34 New Zealand Endodontic Journal Vol 25 November 1934
Ledermix or Calcium Hydroxide for the Treatment of Endodontic Pathology
activities, clinical trials have demonstrated that, like Ledermix, calcium hydroxide appears to have no effect on the incidence of inter-appointment flare ups (Trope, 1990) and in fact Walton and Rivera (1996) stated that the routine use of calcium hydroxide as an intracanal medication has no effect on the prevention or control of pain.
Treatment of external inflammatory root resorption
The aetiology of external inflammatory root resorption is root canal infection and resorption is particularly severe when there is an associated compromised periodontal ligament commonly seen with some traumatic injuries. External inflam-matory root resorption is most commonly treated by chemomechanical debridement of the root canal system and placing a calcium hydroxide dressing. In most cases this results in arrest of the resorption and repair of the defect by cementum deposition and reconstitution of the periodontal ligament (Marais, 1996).
Proposed additional modes of action of calcium hydroxide in the treatment of external inflammatory root resorption include neutralisation of acid products causing the dissolution, activation of the complement system in the immunological reaction by the calcium ion, activation of a calcium depen-dent ATPase which may be associated with hard tissue formation, or the antibacterial and denaturing effects of calcium hydroxide which may decrease the concentration of toxic products which have been associated with root resorption (Tronstad et al. 1991). However, it is generally accepted that its anti-microbial action within the root canal and dentinal tubules is the primary function that causes the arrest of the resorption.
Ledermix may also be effective in the treatment of external inflammatory root resorption. It has been proposed that Ledermix paste is able to bio-logically inactivate the osteoclastic cells involved in the resorption. This is probably due to the Triamcinolone in the Ledermix paste (Heithersay, 1994).
Studies by Pierce and Lindskog (1987) involving replanted monkey incisors dressed with Ledermix also demonstrated the usefulness of this paste in treating external inflammatory root resorption.
Additional benefits of calcium hydroxideNeutralisation of tissue debris
Calcium hydroxide also has some tissue altering and dissolving effects. It is able to denature proteins in the necrotic pulp tissue which then allows sodium hypochlorite to dissolve the remaining tissue more easily (Miserindino, 1994), ie calcium hydroxide aids in the debridement of the root canal system.
Hard tissue repair and apexificationCalcium hydroxide is recommended by a
number of investigators to aid hard tissue repair and apexification (see Silver, 1997 for review). The formation of a proper apex in young teeth with incompletely formed roots which need to be root canal treated can be induced by repeated treatments with calcium hydroxide (Marais, 1996). On the other hand Ledermix is not the dressing of choice for the stimulation of hard tissue repair and apexi-fication as it may have a negative effect on these processes. This is supported by investigations by Uitto et al. (1975).
Treatment of persistent weeping orwet canals
Seepage of apical fluids into the root canal results in a persistently weeping or wet canal. This con-tinuous exudate is commonly and effectively con-trolled using calcium hydroxide as an intracanal medicament (Chong and Pitt Ford, 1992). However the exact mechanism of action of calcium hydrox-ide in the treatment of a wet canal is unknown. It is likely to be due to its antibacterial properties as discussed above; but may also be due to the release of hydroxyl ions and the pH shift of calcium hydroxide providing an environment that favours repair and calcification (Tronstad, et al. 1981); contraction of capillaries; the formation of a fibrous barrier; or the formation of an apical plug by calcium hydroxide (Chong and Pitt Ford, 1992).
ConclusionIt would appear that Ledermix paste may be of
value in treating the symptoms of apical perio-dontitis, but the compound cannot be relied upon to eradicate bacteria from infected canals or rou-tinely stimulate repair. Therefore the only situation in which Ledermix should be used as an intra-canal

Ledermix or Calcium Hydroxide for the Treatment of Endodontic Pathology
New Zealand Endodontic Journal Vol 25 November 1999 Page 35
medicament is when the clinician has failed to remove all the remaining vital pulp tissue from the canal system, either due to time pressures or to an inability to anaesthetise the tooth because of acute inflammatory pain.
In all other cases, because of its more proven and potent anti-bacterial and anti-inflammatory effects, calcium hydroxide is the dressing of choice.
Calcium hydroxide also has other advantages over Ledermix. It can be successfully used in the treatment of persistently weeping canals, to stimulate hard tissue repair and apexification, or to aid in the debridement of the root canal system.
ReferencesAbbott P, Heithersay G, Hume W (1988). Release and diffusion
through human tooth roots in vitro of corticosteroid and tetracycline trace molecules from Ledermix paste. Endodontics & Dental Traumatology 4:55-62.
Barker BCW, & Lockett BC (1971). Experiments using a glucocorticosteroid/ antibiotic paste in infected dog root canals. Journal of the British Endodontic Society 5:60-68.
Barker BCW, & Lockett BC (1972). Reaction of dog pulp and periapical tissues to two glucocorticosrteroid preparations. Oral Surgery, Oral Medicine and Oral Pathology 33:249-262.
Bystrom A, Sundqvist G (1983). Bacteriological evaluation of the effect of 0.5 percent sodium hyporchlorite in endodontic therapy. Oral Surgery, Oral Medicine and Oral Pathology 55:307-12.
Chance K, Lin L, Shovlin FE, Skribner J (1987). Clinical trial of intracanal corticosteroid in root canal therapy. Journal of Endodontics 13:466-468.
Chong BS, Pitt Ford TR (1992). The role of intracanal medication in root canal treatment. International Endodontic Journal 25:97-106.
Miserindino LJ (1994). Instruments, materials, and devices. In Pathways of the Pulp 7th edition, Cohen S & Burns R eds pp 377-413. St Louis, USA: Mosby Inc 1998.
Fava LRG (1992). Human pulpectomy: Incidence of postoperative pain. International Endodontic Journal 25:257-260.
Kontakiotis E, Nakou M, Georgopoulou M (1995). In vitro study of the indirect action of calcium hydroxide on the anaerobic flora of the root canal system. International Endodontic Journal 28:285.
Marais JT (1996). The use of calcium hydroxide as a dressing in root canal treatment. Journal of the Dental Association of South Africa 51:593-599.
Ørstavik D, Haapasalo M (1990). Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endodontics & Dental Traumatology 6:27.
Pierce AM & Lindskog S (1987). The effects of an antibiotic/corticosteroid paste on inflammatory root resorption in vivo. Oral Surgery, Oral Medicine and Oral Pathology 64:216-220.
Reit C. & Dahlen G (1988). Decision making analysis of endodontic treatment strategies in teeth with apical periodontitis. International Endodontic Journal 21:291-299.
Safavi KE, Nichols FC (1994). Alteration of biological properties of bacterial lipopolysaccharide by calcium hydroxide treatment. Journal of Endodontics 20:127.
Silver G (1997). Calcium hydroxide or Ledermix as the root canal medicament? New Zealand Endodontic Journal 23:35-45.
Sjogren U, Figdor D, Spanberg L, Sundqvist G (1991). The antimicrobial effect of calcium hydroxide as a short term intracanal dressing. International Endodontic Journal 24:119.
Taylor M, Hume W, Heithersay G (1989). Some effects of Ledermix paste and Pulpdent pasts on mouse fibroblasts and on bacteria in vitro. Endodontics & Dental Traumatology 5:266-273.
Tepel J, Darwisch el Sawaf M, Hoppe W (1994). Reaction of inflamed periapical tissue to intracanal medicaments and root canal sealers. Endodontics & Dental Traumatology 10:233-238.
Tronstad L, Andreason J, Hasselgren G, Kristerson L, and Rus I (1981). pH changes in the dental tissues after root canal filling with calcium hydroxide. Journal of Endodontics 7:17-21.
Trope M (1990). Relationship of intracanal medicaments to endodontic flare ups. Endodontics & Dental Traumatology 6:226.
Uitto VJ, Antila R, Ranta R (1975). Effects of topical glucocorticosteroid medication on collagen biosynthesis in the dental pulp. Acta Odontoogial Scandanavia 33:287-298.
Walton RE, Rivera EM (1996). Cleaning and shaping. In Principles and practice of endodontics 2nd edition, Walton RE & Torabinejad Meds, pp 228-229. Philadelphia, USA: WB Saunders Company 1996.
Fiona MansonUniversity of Otago School of DentistryPO Box 647Dunedin
Page 36 New Zealand Endodontic Journal Vol 25 November 1999
1997
New Zealand Dental Journal 93:14-16.Love, R.M., McMillan, M.D. and Jenkinson, H. Invasion of dentinal tubules by oral streptococci is
associated with collagen recognition medicated by antigen I/II family polypeptides. Infection and Immunity 65:5157-5164.
Love, R.M. Effects of dental trauma on the pulp. Practical Periodontics and Aesthetic Dentistry 9:427-436.
Chandler, N.P. and Fyfe, D.M. Root canals of buried teeth: radiographic changes due to crystal growth. International Journal of Osteo-archaeology 7:11-17.
Purton, D.G. and Chandler, N.P. Sclerotic bone lesions: report of three cases.
1998
Love, R.M., Carman, N., Carmichael, S. and MacFadyen, E. Sport related dental injury claims 1993-1996: analysis of the ten most common sports excluding rugby union. New Zealand Dental Journal 94:146-149.
Heling, I and Chandler N.P. Antimicrobial effect of irrigant combinations within dentinal tubules. International Endodontic Journal 31:8-14.
Fuge K., Stuck A. and Love R.M. Digitally scanned radiograph versus conventional radiograph for the detection of a small file in working length determination. International Endodontic Journal 31:123-126.
Purton, D.G., Chandler, N.P. and Love R.M. Rigidity and retention of root canal posts. British Dental Journal 184:294-296.
Warren, C.J. and Chandler, N.P. Influence of file handle attachments on tactile discrimination: an evaluation by dental students. International Endodontic Journal 31:100-102.
Love, R.M. and Purton, D.G. Retention of posts with resin, glass ionomer and hybrid cements. Journal of Dentistry 26:599-602.
1999
Kelsen, A., Love, R.M., Kieser, J., and Herbison, P. Root canal anatomy of anterior and premolar teeth in Down’s Syndrome. International Endodontic Journal 32:211-216.
Chandler, N.P., Love, R.M. and Sundqvist G. Laser Doppler flowmetry. An aid in differential diagnosis of apical radiolucencies. Oral Surgery, Oral Medicine, Oral Pathology 87:613-616.
Silver, G.K., Love, R.M. and Purton, D.G. Comparison of two root canal obturation techniques: vertical condensation and System B. International Endodontic Journal 32:287-295.
Odor, T.M., Chandler, N.P., Watson, T.F., Pitt Ford, T.R. and McDonald F. Laser light transmission in teeth: a study of the patterns in different species. International Endodontic Journal 32:296-302.
Endodontic publications from theUniversity of Otago School of Dentistry
Readers can obtain copies of the papers by contacting the Librarian, University of OtagoSchool of Dentistry, PO Box 647, Dunedin – Editor.

New Zealand Endodontic Journal Vol 25 November 1999 Page 37
AbstractsMicrobiological Status of Root-Filled Teeth
with Apical PeriodontitisMolander A, Reit C, Dahlen G and Kvist T
International Endodontic Journal 1998; 31:1-7
This study examined the microbiological status of 100 root-filled teeth with radiographically verified apical periodontitis, and of 20 root filled teeth that required retreatment but did not have signs of periapical pathology. In the group with apical periodontitis 117 strains of bacteria were recovered in 68 teeth. In most of the cases one or two strains were found. Facultative anaerobic species predominated among these isolates with enterococci being the most frequently isolated genera. In 11 teeth with no evidence of periapical pathology no bacteria were recovered, whilst the remaining nine yielded 13 microbial strains. The authors concluded that the microflora of the obturated canal differs from that found in the untreated necrotic dental pulp. This work reinforces the concept that retreatment of failed cases by conventional endodontic therapy to remove intracanal bacteria should be considered before surgical intervention.
Retention of Posts with Resin, Glass Ionomerand Hybrid CementsLove RM and Purton DG
Journal of Dentistry 1998; 26:599-602
The objective of this study was to measure and compare the retention of serrated root canal posts cemented with either glass ionomer, resin, or resin-modified glass ionomer (hybrid) cements. Post holes were prepared in fifty single-rooted decoronated human teeth and divided into five equal-sized groups. Serrated stainless steel posts were cemented using either a glass ionomer cement, one of two resin cements or one of two resin-modified glass ionomer luting cements. The tensile force required to dislodge the cemented posts in a testing machine was recorded. Statistical analysis revealed that posts cemented with Scotchbond (3M Dental Products) resin cement were significantly better retained (340.06 N+/-23.13 N) than those cemented with Panavia 21 (Kuraray Co, Ltd) resin cement (212.56 N+/-67.62 N), or either of the two resin-modified glass ionomer cements (Vitremer (3M Dental Products) 53.90 N+/-28.42 N, Fuji DUET (GC Corp) 25.97 N+/-14.70 N), but not statistically better than posts cemented with Ketac-Cem (ESPE) glass ionomer cement (286.16 N+/-38.71 N). The retention of posts cemented with either Panavia 21 or Ketac-Cem cement was significantly better than with either hybrid cement. There was no significant difference in retention between the hybrid cements. The authors concluded that the performance of the resin-modified glass ionomer cements was significantly below that of alternative cements in this study. Possible explanations for this finding were discussed and it was suggested that dentists should be cautious in adopting this new cementing regime.
Inte
rnat
iona
l Lite
ratu
re

Page 38 New Zealand Endodontic Journal Vol 25 November 1999
Inte
rnat
iona
l Lite
ratu
rePersistent Periapical Radiolucencies of Root-Filled
Human Teeth, Failed Endodontic Treatmentsand Periapical Scars
Nair P, Sjogren U, Figdor D, and Sundqvist GOral Surgery, Oral Medicine, Oral Pathology, Oral Radiology,
& Endodontics 1999; 87:617-27
This paper describes the light and transmission electron microscopy and microbial findings of periapical lesions from 6 cases that demonstrated persistent periapical radiolucent lesions after conventional root canal treatment. The authors reported that two periapical lesions were due to persisting infection in the apical root canal system , one case was a cyst, and two cases had the histological features of periapical healing by scar tissue formation, the remaining sample was a granulamotous lesion with no obvious cause being identified. The authors concluded that the results confirmed previous observations that associated factors in the failure of endodontic treatment include persistent intraradicular infection and periapical cysts. In addition, unresolved periapical radiolucencies may occasionally be due to healing by scar tissue, which may be mistaken as a sign of failed endodontic treatment.
Effect of Systemic Tetracycline and Amoxicillinon Inflammatory Root Resorption of
Replanted Dogs’ TeethSae-Lim V, Wang CY, and Trope M
Endodontics & Dental Traumatology 1998; 14:216-20
The use of systemic penicillin after an avulsion injury has been recommended as a way to decrease the occurrence of resorption complications. Previous work by this group has shown systemic tetracycline to possess anti-resorptive properties independent of potential anti-bacterial actions. The purpose of this study was to compare histologically the effectiveness of tetracycline and amoxicillin in limiting inflammatory root resorption (IR) secondary to pulpal infection in replanted dogs’ teeth. Thirty root canals in five dogs were infected with plaque. The roots were extracted and handled so as to ensure damage to the cementum and immediately replanted. The dogs were given either tetracycline hydrochloride or amoxicillin, administered orally, on the day of extraction and replantation and for the following 6 days. The control group consisted of other teeth in these animals which were treated in the same manner but no antibiotics were given. After approximately 6 months the teeth were recovered and prepared for histologic evaluation. The amount of root surface affected by inflammatory resorption was similar for either antibiotic group, while the healing response of the tetracycline group was superior to the control group. Since tetracycline has been shown to have anti-resorptive properties in addition to anti-bacterial properties, the authors concluded that tetracycline could be considered as an alternative to amoxicillin after avulsion injuries.
New Zealand Endodontic Journal Vol 25 November 1999 Page 39
THE NEW ZEALAND SOCIETY OF ENDODONTICS INCORPORATEDFINANCIAL STATEMENTSFOR THE YEAR ENDED 31ST MARCH 1998
ACCOUNTANTS’ STATEMENTFOR THE YEAR ENDED 31st MARCH 1998
DISCLAIMER OF LIABILITY
We have compiled the financial statements of THE NEW ZEALAND SOCIETY OF ENDODONTICS INCORPORATED for the year ended 31st March 1998, based on generally accepted accounting principles.
A compilation is limited primarily to the collection, classification, and summarisation of financial information supplied by our client. A compilation does not involve the verification of that information.
We have not carried out an audit or a review assignment on the financial statements and therefore neither we nor any of our employees accept any responsibility for the accuracy of the materials from which the financial statements have been prepared.
Further, the financial statements have been prepared at the request of and for the purpose of our client only and neither we nor any of our employees accept any responsibility on any ground whatever, including liability in negligence, to any other person.
SPICER & OPPENHEIMChartered AccountantsAuckland20th May 1999
COURSES AND CONFERENCES STATEMENTFOR THE YEAR ENDED 31ST MARCH 1998
Notes 1998 1997 $ $COURSE INCOMECourse Fees Received 31,213 15,543
LESS EXPENDITURECost of Courses 26,018 21,318Total Expenditure 26,018 21,318GROSS PROFIT/(LOSS) FROM COURSES 5,195 (5,775)
This statement has not been audited and should be read with the Accountants’ Statement and Notes to the Accounts.THE NEW ZEALAND SOCIETY OF ENDODONTICS INCORPORATED
Society News
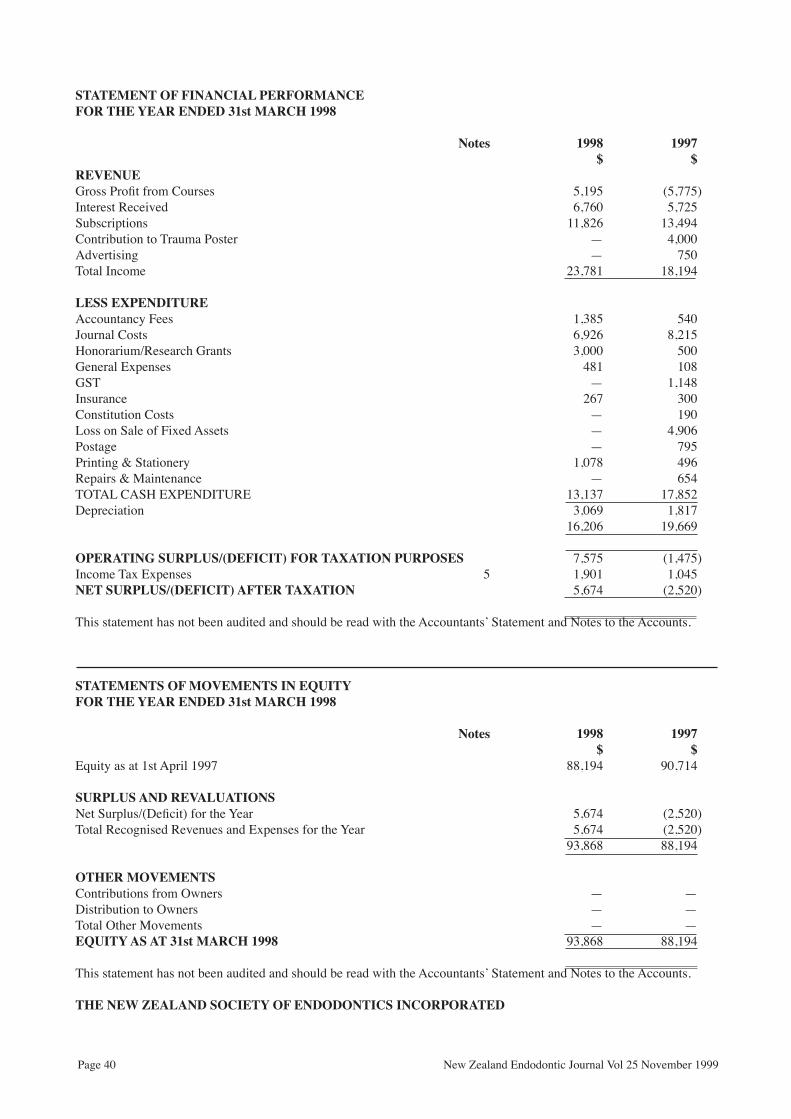
Page 40 New Zealand Endodontic Journal Vol 25 November 1999
STATEMENT OF FINANCIAL PERFORMANCEFOR THE YEAR ENDED 31st MARCH 1998
Notes 1998 1997 $ $REVENUEGross Profit from Courses 5,195 (5,775)Interest Received 6,760 5,725Subscriptions 11,826 13,494Contribution to Trauma Poster — 4,000Advertising — 750Total Income 23,781 18,194
LESS EXPENDITUREAccountancy Fees 1,385 540Journal Costs 6,926 8,215Honorarium/Research Grants 3,000 500General Expenses 481 108GST — 1,148Insurance 267 300Constitution Costs — 190Loss on Sale of Fixed Assets — 4,906Postage — 795Printing & Stationery 1,078 496Repairs & Maintenance — 654TOTAL CASH EXPENDITURE 13,137 17,852Depreciation 3,069 1,817 16,206 19,669
OPERATING SURPLUS/(DEFICIT) FOR TAXATION PURPOSES 7,575 (1,475)Income Tax Expenses 5 1,901 1,045NET SURPLUS/(DEFICIT) AFTER TAXATION 5,674 (2,520)
This statement has not been audited and should be read with the Accountants’ Statement and Notes to the Accounts.
STATEMENTS OF MOVEMENTS IN EQUITYFOR THE YEAR ENDED 31st MARCH 1998
Notes 1998 1997 $ $Equity as at 1st April 1997 88,194 90,714
SURPLUS AND REVALUATIONSNet Surplus/(Deficit) for the Year 5,674 (2,520)Total Recognised Revenues and Expenses for the Year 5,674 (2,520) 93,868 88,194
OTHER MOVEMENTSContributions from Owners — —Distribution to Owners — —Total Other Movements — —EQUITY AS AT 31st MARCH 1998 93,868 88,194
This statement has not been audited and should be read with the Accountants’ Statement and Notes to the Accounts.
THE NEW ZEALAND SOCIETY OF ENDODONTICS INCORPORATED
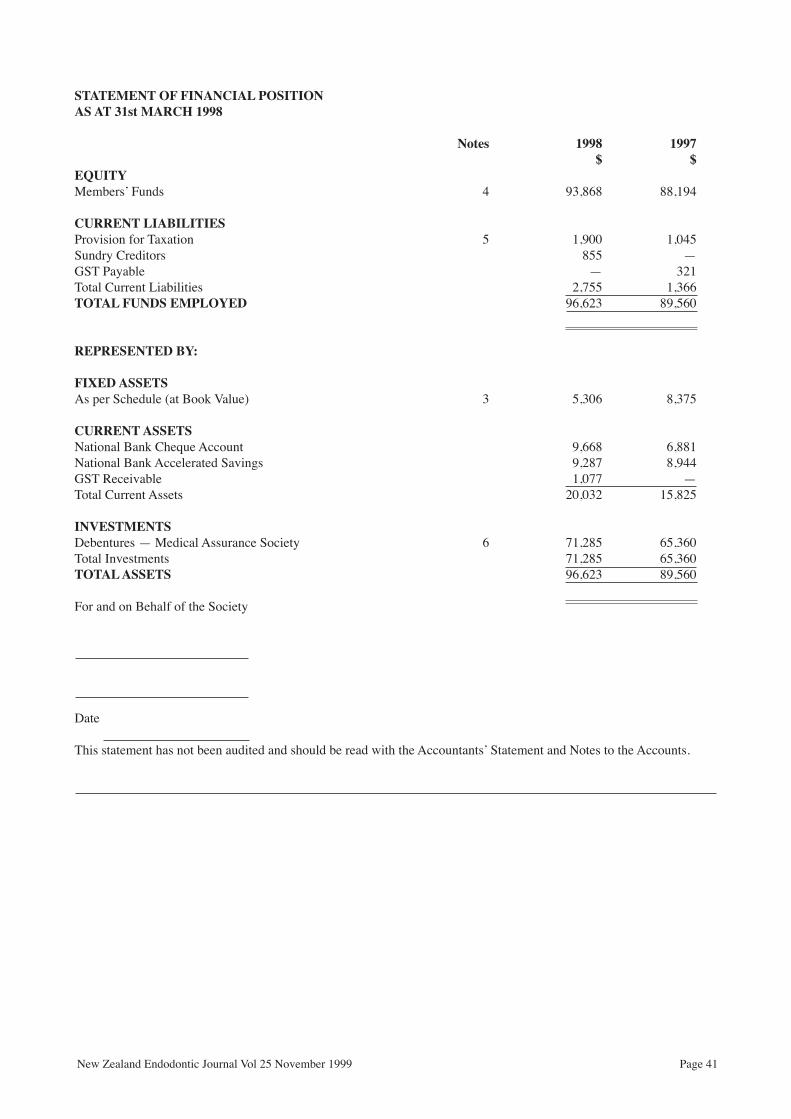
New Zealand Endodontic Journal Vol 25 November 1999 Page 41
STATEMENT OF FINANCIAL POSITIONAS AT 31st MARCH 1998
Notes 1998 1997 $ $EQUITYMembers’ Funds 4 93,868 88,194
CURRENT LIABILITIESProvision for Taxation 5 1,900 1,045Sundry Creditors 855 —GST Payable — 321Total Current Liabilities 2,755 1,366TOTAL FUNDS EMPLOYED 96,623 89,560
REPRESENTED BY:
FIXED ASSETS As per Schedule (at Book Value) 3 5,306 8,375
CURRENT ASSETSNational Bank Cheque Account 9,668 6,881National Bank Accelerated Savings 9,287 8,944GST Receivable 1,077 —Total Current Assets 20,032 15,825
INVESTMENTSDebentures — Medical Assurance Society 6 71,285 65,360Total Investments 71,285 65,360TOTAL ASSETS 96,623 89,560
For and on Behalf of the Society
Date
This statement has not been audited and should be read with the Accountants’ Statement and Notes to the Accounts.
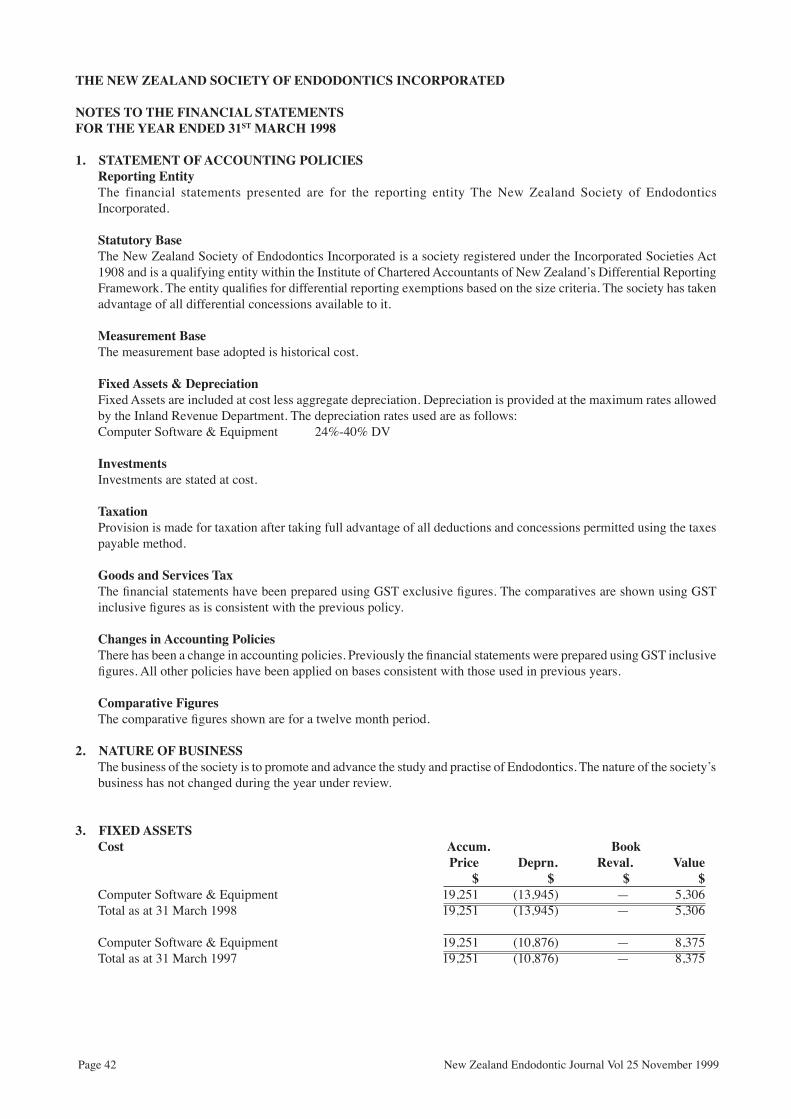
Page 42 New Zealand Endodontic Journal Vol 25 November 1999
THE NEW ZEALAND SOCIETY OF ENDODONTICS INCORPORATED
NOTES TO THE FINANCIAL STATEMENTSFOR THE YEAR ENDED 31ST MARCH 1998
1. STATEMENT OF ACCOUNTING POLICIESReporting EntityThe financial statements presented are for the reporting entity The New Zealand Society of Endodontics Incorporated.
Statutory BaseThe New Zealand Society of Endodontics Incorporated is a society registered under the Incorporated Societies Act 1908 and is a qualifying entity within the Institute of Chartered Accountants of New Zealand’s Differential Reporting Framework. The entity qualifies for differential reporting exemptions based on the size criteria. The society has taken advantage of all differential concessions available to it.
Measurement BaseThe measurement base adopted is historical cost.
Fixed Assets & DepreciationFixed Assets are included at cost less aggregate depreciation. Depreciation is provided at the maximum rates allowed by the Inland Revenue Department. The depreciation rates used are as follows:Computer Software & Equipment 24%-40% DV
InvestmentsInvestments are stated at cost.
TaxationProvision is made for taxation after taking full advantage of all deductions and concessions permitted using the taxes payable method.
Goods and Services TaxThe financial statements have been prepared using GST exclusive figures. The comparatives are shown using GST inclusive figures as is consistent with the previous policy.
Changes in Accounting PoliciesThere has been a change in accounting policies. Previously the financial statements were prepared using GST inclusive figures. All other policies have been applied on bases consistent with those used in previous years.
Comparative FiguresThe comparative figures shown are for a twelve month period.
2. NATURE OF BUSINESSThe business of the society is to promote and advance the study and practise of Endodontics. The nature of the society’s business has not changed during the year under review.
3. FIXED ASSETSCost Accum. Book Price Deprn. Reval. Value $ $ $ $Computer Software & Equipment 19,251 (13,945) — 5,306Total as at 31 March 1998 19,251 (13,945) — 5,306
Computer Software & Equipment 19,251 (10,876) — 8,375Total as at 31 March 1997 19,251 (10,876) — 8,375

GUNZ/BELMONT AD
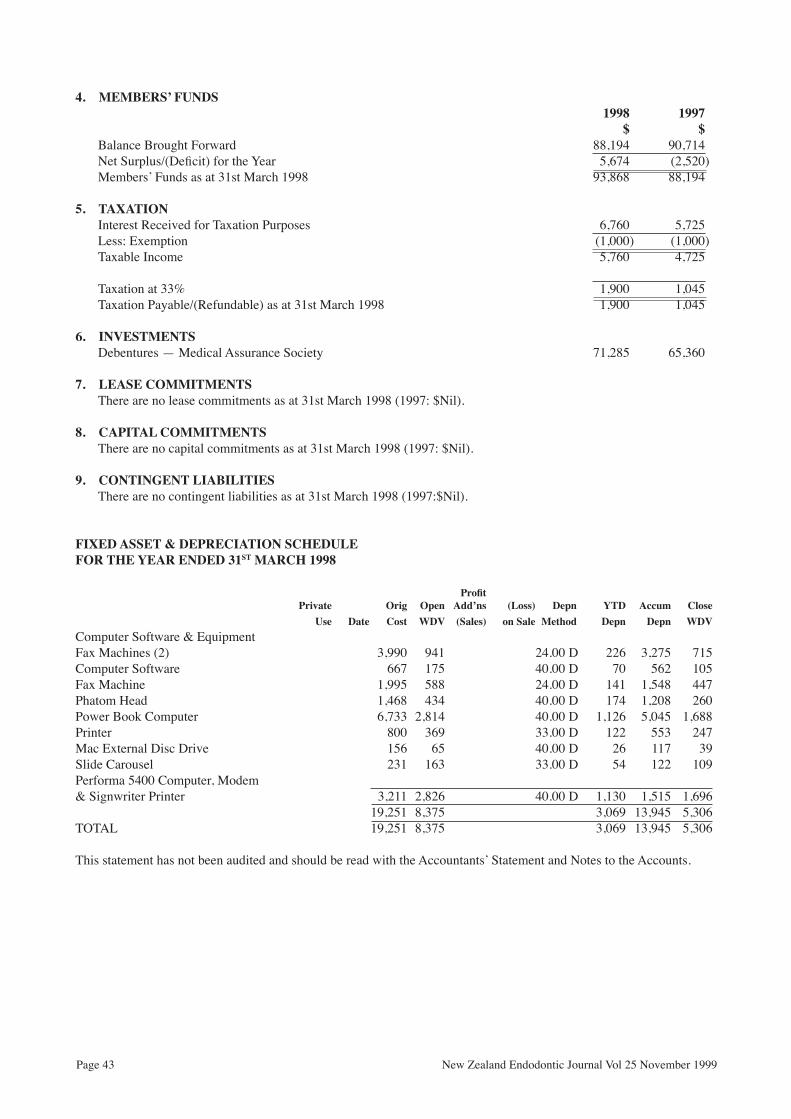
Page 43 New Zealand Endodontic Journal Vol 25 November 1999
4. MEMBERS’ FUNDS 1998 1997 $ $
Balance Brought Forward 88,194 90,714Net Surplus/(Deficit) for the Year 5,674 (2,520)Members’ Funds as at 31st March 1998 93,868 88,194
5. TAXATIONInterest Received for Taxation Purposes 6,760 5,725Less: Exemption (1,000) (1,000)Taxable Income 5,760 4,725
Taxation at 33% 1,900 1,045Taxation Payable/(Refundable) as at 31st March 1998 1,900 1,045
6. INVESTMENTSDebentures — Medical Assurance Society 71,285 65,360
7. LEASE COMMITMENTSThere are no lease commitments as at 31st March 1998 (1997: $Nil).
8. CAPITAL COMMITMENTSThere are no capital commitments as at 31st March 1998 (1997: $Nil).
9. CONTINGENT LIABILITIESThere are no contingent liabilities as at 31st March 1998 (1997:$Nil).
FIXED ASSET & DEPRECIATION SCHEDULEFOR THE YEAR ENDED 31ST MARCH 1998
Profit Private Orig Open Add’ns (Loss) Depn YTD Accum Close Use Date Cost WDV (Sales) on Sale Method Depn Depn WDVComputer Software & EquipmentFax Machines (2) 3,990 941 24.00 D 226 3,275 715Computer Software 667 175 40.00 D 70 562 105Fax Machine 1,995 588 24.00 D 141 1,548 447Phatom Head 1,468 434 40.00 D 174 1,208 260Power Book Computer 6,733 2,814 40.00 D 1,126 5,045 1,688Printer 800 369 33.00 D 122 553 247Mac External Disc Drive 156 65 40.00 D 26 117 39Slide Carousel 231 163 33.00 D 54 122 109Performa 5400 Computer, Modem& Signwriter Printer 3,211 2,826 40.00 D 1,130 1,515 1,696 19,251 8,375 3,069 13,945 5,306TOTAL 19,251 8,375 3,069 13,945 5,306
This statement has not been audited and should be read with the Accountants’ Statement and Notes to the Accounts.