Embed Size (px)
Citation preview

Endod Dent Traumatol 1993: 9: 238-242Printed in Denmark . All rights reserved
Copyright (Ci Munksgaard I993
Endodontics &Dental Traumatolo^
/5.S'A' 0109-2502
Partial pulpotomy in young permanent teethwith deep carious lesionsMejare I, Cvek M. Partial pulpotomy in young permanent teethwith deep carious lesions. Endod Dent Traumatol 1993;9: 238-242. © Munksgaard, 1993.
Abstract - The material comprised 37 young posterior teeth withdeep carious lesions and exposed pulps, treated with partialpulpotomy and dressed with calcium hydroxide. The teeth weredivided into tw"o groups. Group 1 consisted of 31 teeth with noclinical or radiographic symptoms before treatment. Group 2 of6 teeth with temporary pain, widened periodontal space peri.,apically and/or productive osteitis, i.e. increased density of thesurrounding alveolar bone. After an observation time of 24 to140 months (x = 56 months), healing had occurred in 29 of 31teeth in Group 1 (93.5%) and in 4 of 6 teeth in Group 2. It wasconcluded that the present, as well as pre\'iously reported resultsindicate that partial pulpotomy may be an adequate treatmentlor young permanent molars with a carious exposure, althoughmore studies are needed before the treatment can be recommendedlor routine clinical use.
I, Mejare, M, CvekDepartment ot Pedodontics, Eastman DentalInstitute, Stockholm, Sweden,
Key words: denial caries: pulp capping: partialpulpotomy,
Ingegerd Meiare, Department of Pedodontics,
Eastmaninstitutet, Dalagatan 11,
S-113 24 Stockholm, Sweden
Accepted June 28, 1993
In mature teeth, a pulp exposed by caries is ustiallyremoved and the root canals are filled. In immatureteeth the usual procedure in\olves treating exposedvital pulps with capping or pulpotomy and dressingwith calciutn hydroxide. However, neither of thelatter two methods has given satisfactory results.Capping is considered to be so unpredictable thatit should be avoided and pulpotomy, i.e. removalof the whole coronal pulp, is regarded as an inter-mediate treatment that should be followed by pul-pectomy, when root development has been com-pleted (1-4). Treatment of a pulp exposed by cariesis clearly a problem in paediatric dentistry and new-methods are needed to improve the prospects ofpulpal healing, particularly in immature teeth. Anytreatment of a pulp exposed by caries or acciden-tally, should aim to preser\'e it, vital and free ofinflammation. To a very high degree this has beenachieved by partial pulpotomy, i.e. removal of onlya superficial layer of damaged and/or inflamedti,ssue in traumatieally exposed pulps (5, 6), Partialpulpotomy has also been reported to be successfulin treatment of pulps exposed by caries, in tempor-ary and permanent molars, although the number
238
of treated permanent leeth is rather limited (7-9),Ihe aim of the present study was, therefore, furtherto evaltiate the outcoine of partial pulpotomy ofpulps exposed by excavation in posterior permanentteeth with deep cariotis lesion.
Material and methods
Forty-four permanent teeth with pulps exposed dur-ing excavation of deep caries were treated with par-tial pulpotomy and dressed with ealcium hydroxide.The treatments took place at the Department ofPedodontics, Eastmaninstitutet, Stockholm, be-tween 1978 and 1990 and were performed by 16dentists, who were specialists or post-graduate stu-dents. The minimum follow-up time was to be twoyears. Seven teeth did not meet this requirement,leaving 37 teeth, 2 premolars and 35 molars, forevaluation, in patients aged 6 to 15 years (x = 9years).
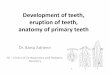
The treatment included application of a rubberdam and excavation of all carious dentin, foUowrdby ample Hushing of the cavity and exposed pulpwith sterile saline. The exposed pulp tissue and
surrounding dentin were then removed with a dia-mond instrument and a high-speed air-turbine toa depth of about 1.0-1.5 mm, during continuousflushing with a water spray from the turbine. There-after, the pulp wound was flushed with sterile salineuntil bleeding had ceased. When haemostasis hadbeen achieved, the pulpal wound was dressed withcalcium hydroxide (Calasept'-, Scania Dental,Knivsta, Sweden), which was adapted and driedwith sterile cotton pellets. Care was taken to avoida blood clot between the wound surface and thedressing material. After the whole cavity floor hadbeen covered with calcium hydroxide, the cavitywas sealed with zinc oxide-eugenol cement. Perma-nent restoration with anialgam or composite wasperformed at a later appointment. After 3—6months, the formation of a hard tissue barrier wasilinically explored in 17 teeth, (Fig. 1,2). The teethwere controlled after 3 and 6 months and thereafterannually. The observation period varied from 24 to140 months (x = 56 months).
The files of the patients were examined for the
Partial pulpotomv in carious teeth
presence of clinical symptoms, such as spontaneousor provoked pain and sensitivity to percussion.Radiograhs, taken at the time of treatment, wereexamined separately by both authors with respect toroot maturity and periapical conditions. Thereafter,the teeth were divided into two groups:
Group /, consisting of 31 teeth which prior totreatment exhibited no clinical or radiographicsymptoms. In 17 teeth pulpotomy was performedat the first appointment, after complete removalof carious dentin and exposure of the pulp. Theremaining 14 teeth were primarily treated by step-wise excavation, i.e. the carious dentin was gradu-ally excavated and covered with calcium hydroxidebefore the pulp was exposed (10-12). The stepwiseexcavation was done during 2—3 consecutive ap-pointments at inter\ als of 2—3 weeks.
Group 2, consisting oi^ 6 teeth which at the timeof treatment showed clinical and/or radiographicsymptoms. Three teeth exhibited a periapically wid-ened and diffusely outlined periodontal space.Spontaneous pain was recorded for 2 of these teeth.
mm^tmmmaill^^^mmmi^^^t^mmil^^t^ma^mB''it^^m^ t^^^mm^immmm^fmmm^^^mmmmiim^^imm^ami^i^i^ammmm ma^aBmmm^^^mmmmmm^^mmmmmm^^^^^mmm^^m
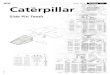
Fig. I. A; 36; Two sm;iil pulp cxposurrs lifter cxrawilion of a der-p carious lesion siiowin^ haemostasis in the mesial, firsi preparedamputation ravity (arrow) and ceased bleeding in the distal cavity. B, The pulp wounds dressed with calcium hydroxide. C:Appearance of hard tissue barriers three months after treatment. D: Radiograph taken before treatment showing; a deep carious lesionand normal periapical conditions. E: Three months after treatment, before the clinical control of hard tissue barriers. F; Eight yearsafter partial pulpotomy, showing normal periapical conditions and completed root development.
239

Mejare & Cvek
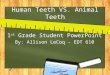
Fig. 2. A: 36; pulp exposed by caries (arrow). B. Haemostasis after complete removal of carious dentin and partial pulpotomy. C
Appearance of hard tissue barrier 3 months later (arrow). D: Radiograph taken before treatment, showing a temporary filling in the
occlusal cavity, normal pcriapical conditions, E and F: Two and four years after partial pulpotomy.
The other 3 teeth exhibited a productive periapicalosteitis, i.e. a widened periodontal space with in-creased density of the surrounding alveolar bone,but with no other clinical symptoms. Stepwise exca-vations was performed in one of these teeth.
At the end of the observation period, healingwas recorded if there were no clinical symptoms ordemonstrable radiographic changes other than acompleted root development in immature teeth.
Table 1. Distribution of posterior permanent teeth, treated with partial pulp-otomy after pulp exposure due to carles, with respect to the observationperiod, maturity of roots and occurrence of a failure: (') denotes one separatecase of failure. Group 1: teeth without clinical or radiographic symptoms andGroup 2: teeth with such symptoms before treatment.
Group 1: no ol teethimmaturemature
Group 2: no ot teettiimmaturemature
24
3114170
6
1 05 0
Observation period (months)
25-36
291415
4
4
37-48
239
140
4
4
49-60
1578
1
1
61-140
725
The tooth should also be sensible to electric stimula-tion. The distribution of the teeth within the twogroups, with respect to root maturity and length ofthe observation time, is shown in Table 1.
Results
The results are presented in Table 1.In Group I, healing was found in 29 of 31 teeth,
i.e. in 93.5%, (Figs. 1, 2). Failure occurred in twoteeth; in one, pulpitis developed after 10 days; inthe other, the occlusal filling was missing and aperiapical radiolucency was observed 48 monthsafter treatment.
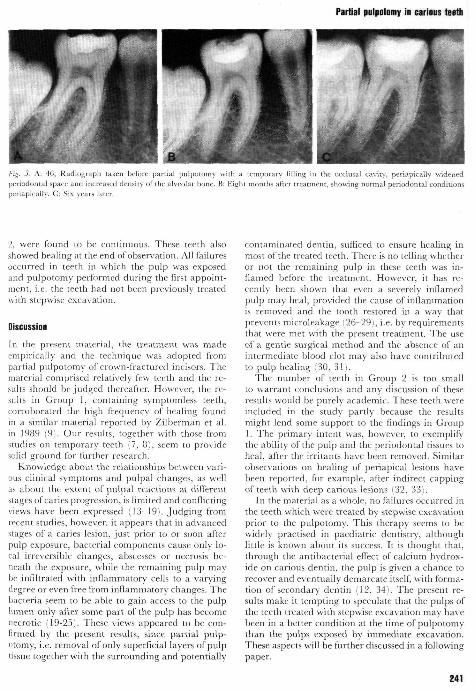
In Group 2, clinical symptoms ceased after treat-ment and at the end of the observation period theradiographs showed periapically a normal peri-odontal space bordered by lamina dura in 4 teeth,ineluding 3 which before treatment had shown aproductive periapical osteitis (Fig. 3). In the re-maining 2 teeth, the widened and diffusely outlini--dperiapical space developed into a periapical radio-lucency, 10 or 24 months after treatment.
In the material as a whole, all clinically inspectt'dhard tissue barriers, 15 in Groups 1 and 2 in Group
240
Partial pulpotomy in carious teeth
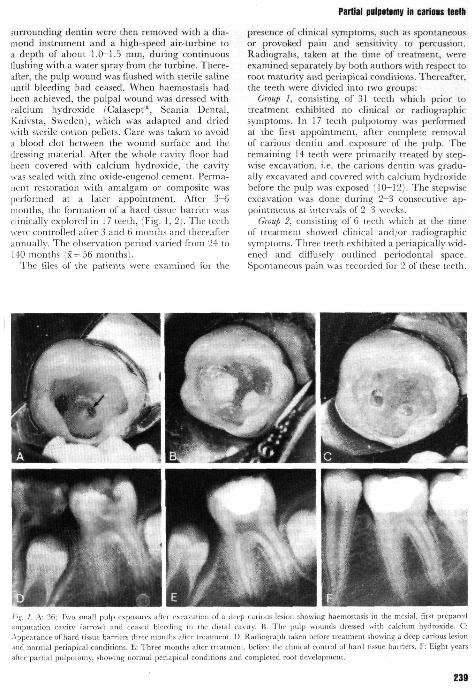
Fig. 3. A: 46; Radiograph taken before partial pulpotomy with a temporary filling in. the occlusal ca\'ity, periapicalSy widenedperjodontai space and increased den.sity of the alveolar bone. B: Eight months after treatment, showing normal periodontal condition.speriapically. C: Six years later.
2, were found to be continuous. These teeth alsoshowed healing at the end of observation. All failuresoccurred in teeth in which the pulp was exposedand pulpotomy performed during the first appoint-ment, i.e. the teeth had not been previously treatedwith stepwise excavation.
Discussion
In the present material, the treatment was madeempirically and the technique was adopted frompartial pulpotomy of crown-fractured incisors. Thematerial comprised relati\'ely few teeth and the re-sults should be judged thereafter. However, the re-sults in Group 1, containing symptomless teeth,corroborated the high frequency of healing foundin a similar material reported by Zilberman et al.in 1989 (9). Our results, together with those fromstudies on temporary teeth (7. 8), seem to providesolid ground for further research.
Knowledge about the relationships between vari-ous clinical symptoms and pulpal changes, as wellas about the extent of pulpa! reactions at differentstages of caries progression, is limited and conflictingviews have been expressed (13-19). Judging fromrecent studies, however, it appears that in advancedstages of a caries lesion, just prior to or soon afterpulp exposure, bacterial components cause only lo-cal irreversible changes, abscesses or necrosis be-neath the exposure, while the remaining pulp maybe infiltrated with inflammatory cells to a varyingdegree or even free from inflammatory changes. Thebacteria seem to be able to gain access to the pulplumen only after some part of the pulp has becomenecrotic (19-25). These views appeared to be con-firmed by the present results, since partial pulp-otomy, i.e. removal of only superficial layers of pulptissue together with the surrounding and potentially
contaminated dentin, sufficed to ensure healing inmost of the treated teeth. There is no telling whetheror not the remaining pulp in these teeth was in-flamed before the treatment. However, it has re-cently been shown that even a severely inflamedpulp may heal, provided the cause of inflammationis removed and the tooth restored in a way thatprevents microleakage (26-29), i.e. by requirementsthat were met with the present treatment. The useof a gentle surgical method and the absence of anintermediate blood clot may also have contributedlo pulp healing (30, 31).
The number of teeth in Group 2 is too smallto warrant conclusions and any discussion of theseresults would be purely academic. These teeth wereincluded in the study partly because the resultsmight lend some support to the findings in Group1. The primary intent was, however, to exemplifythe ability of the pulp and the periodontal tissues toheal, after the irritants have been removed. Similarobservations on healing of periapical lesions havebeen reported, for example, after indirect cappingof teeth with deep carious lesions (32, 33).
In the material as a whole, no failures occurred inthe teeth which were treated by stepwise excavationprior to the pulpotomy. This therapy seems to bewidely practised in paediatric dentistry, althoughlittle is known about its success. It is thought that,through the antibacterial effect of calcium hydrox-ide on carious dentin, the pulp is given a chance torecover and e\'entually demarcate itself, with forma-tion of secondary dentin (12, 34). The present re-sults make it tempting to speculate that the pulps ofthe teeth treated with stepwise excavation may havebeen in a better condition at the time of pulpotomythan the pulps exposed by immediate excavation.These aspects will be further discussed in a followingpaper.
241

Mejare & Cvek
Conclusions
The results indicated a high frequency of pulpalhealing in young posterior teeth when superficiallayers of the pulp beneath a carious exposure wererwnoved, provided that all surrounding carious den-tin was removed, the pulp wound was dressed withcalcium hydroxide, and the coronal cavity wassealed with zinc oxide-eugenol cement. However,more comprehensive studies are needed before thistreatment can be recommended for routine clinicaluse. -- :. ^r-. ••"'...
Acknowledgement — The authors wish to express theirsincere gratitude to Mrs Catrine Rohdin, SeniorDental Assistant, for invaluable help with collectingand compiling the material for this study.
References
1. SELTZF.R R , BENDER IB. The dental pulp. Philadelphia: Lip-pincott 1984; Ch 14.
2. ToBiN DF. Pulpotomy in primary and young permanentteeth. J Dent Child 1954; 21: 252-4.
3. HAH.ET G E , PORTEOUS JR. Fractured incisors treated byvital pulpotomy. A report on 100 consecutive cases. Br DentJ 1963; 115: 414-26.
4. LANGELAND K , DOWDEN WE, TRONSTAD L, LANGEI.AND L K .
Human pulp changes of iatrogenic origin. Oral Surg Oral.Med Oral Fathol \971; 32: 943-80.
5. CVEK M . A clinical report on partial pulpotomy and cappingwith calcium hydroxide in permanent incisors with compli-cated crown fracture. J Endod 1978; 4: 232-7.
6. FuKS A, CHOXSAK A, EIDELMAN E. Partial pulpotomy as analternative treatment for exposed pulps in crown-fracturedpermanent incisors. Endod Dent Traumatol 1987; 3: 100-2.
7. JEPPESEN K . Direct pulp capping on primary teeth - a long'term investigation. J Int Assoc Dent Child 1971; 12: 10-9.
8. SCHRODER U , SZPRINGER-NODZAK M , JANICHAJ, WACINSKA
M, BuDNY J, LosEK K. A one-year follow-up of partialpulpotomy and calcium hydroxide capping in primary mo-lars. Fndod Dent Traumatol 1987; 3: 304-6.
9. Ztt,BERMAN U, ELIYAHU M , SARNAT H . Partial pulpotomyin carious permanent molars. Am J Dent 1989; 2: 147-50.
10. LAW DB, LEWIS T M . The effect of calcium hydroxide ondeep carious lesions. Oral Surg Oral Med Oral Pathol 1961;14: 1130-7.
11. SowDEN JR. A preliminary report on the recalcification oi'carious dentin. ASDC J Dent Child 1956; 23: 187-8.
12. MAGNUSSON B O , SUNDELL SO. Stepwise excavation of deepcarious lesions in primary molars. .7 ^^'^ Assoc Dent Child 1977;8: 36-40.
13. SBI-TZER S, BENDER IB, ZIONZ M . The dynamics of pulp
inflammation: correlations between diagnostic data and ac-
tual histologic fmdings in the pulp. Oral Surg Oral Med OralFathol 1963; 16: 846-7 L
14. KOCH G , NYBORG H . Correlation between cHnica! and histo-logical indications for pulpotomy of deciduous teeth. J ImAssoc Dent Child 1970; 1: 3-10.
15. SCHRODER U , Agreement between clinical and histologicfindings in chronic coronal pulpitis in primary teeth. ScandJ Dent Res 1977; 85: 583-7.
16. BRANNSTROM M , LIND PO. Pulpal response to early dentalcaries. J Dent Res 1965; 44: 1045-50.
17. BAUME L J . Dental pulp conditions in relation to cariomlesions. Int Dent J 1970; 20: 309-37.
18. LANGELAND K , LANGELAND LK. Indirect capping and the
treatment of deep carious lesions. Int Dent J 1968; 18: 326-80.19. REEVES R , STANLEY H R . The relationship of bacterial pene-
tration and pulpal pathosis in carious teeth. Oral Surg OralMed Oral Pathol 1966; 22: 59-71.
20. LANGELAND K. Management of the inflamed pulp associatedwith deep carious lesion. J Fndod 1981; 7; 169-81.
21. TRowBRtDGE HO. 2. Pathogenesis of pulpitis resulting fromdental caries. J Endod 1981; /.- 52-60.
22. LIN L, LANGELAND K . Light and electron microscopic studyof teeth with carious pulp exposures. Oral Surg Oral Med OralPathol 1981; 51: 292-316.
23. ToRNECK CD. I. A report of studies into change.s in the finestructure of the dental pulp in human caries pulpitis. J Endod1981; 7: 8-16.
24. LANGELAND K. Tissue response to dental caries, Endod DentTraumatol 1987; 3: 149-71.
25. EIDELMAN E, ULMANSKY M , MICHAELI Y, Histopathology of
the pulp in primary' incisors with deep dentinal caries. PediatrDent 1992; 14: 372-5,
26. MjOR IA, TRONSTAD L . Healing of experimentally inducedpulpitis. Oral Surg Oral Med Oral Pathol 1974; 38: ! 15-21,
27. Cox CF, BERGENHOLTZ G, HEYS DR, SYED SA, FITZGERALD
M, HEYS RJ, Pulp capping of dental pulp mechanicallyexposed to oral microflora: a 1-2 year observation of woundhealing in the monkey. J Oral Pathol 1985; 14: 156-68,
28. WARFINOE J, BERGENHOLTZ G, Healing capacity of humanand monkey dental pulps following experimentally-inducedpulpitis. Endod Dent Traumatol 1986; 2: 256-62,
29. BERGENHOLTZ G, COX CF, LOESCHE W J , SYED SA, Bacterial
leakage around dental restorations: its effect on the dentalpulp, J Oral Pathol 1982; 11: 439-50.
30. GRANATH L - E , HAGMAN G. Experimental pulpotomy in hu-
man bicuspids with reference to tutting technique. ArtaOdontol Scand 1971; 29: 155-63.
31. SCHRODER U . Effect of extra-pulpal blood clot on healingfollowing experimental pulpotomy and capping with cal-cium hydroxide. Odont Reiy 1973; 24: 257-68.
32. JORDAN RE, SUZUKI M , SKINNER DH. Indirect pulp-capping
of carious teeth with periapical lesions. J Am Dent A.-i.so''1978; 97; 37-43.
33. COTTON W, LANGELAND K, BURMEISTER J A , FARELL PE,
Evaluation of carious teeth with apical radiolucencies forindirect pulp capping. J Dent Re.^ Abstr 1983; 62: 216, abstr424,
34. FISHER FJ, The effect of a calcium hydroxide/water paste onmicro-organisms in carious dentine. Br Dent J 1972: l-'^-'^'19-21,
242