Embed Size (px)
Citation preview

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 1/14
Endocrine ControlMechanismsDaniel E. Peavy, Ph.D.31
C H A P T E R
31■ GENERAL CONCEPTS OF ENDOCRINE CONTROL■ THE NATURE OF HORMONES
■ MECHANISMS OF HORMONE ACTION
C H A P T E R O U T L I N E
1. Hormones are chemical substances, involved in cell-to-cellcommunication, that promote the maintenance of home-ostasis.
2. There are six classes of steroid hormones, based on theirprimary actions.3. Most polypeptide hormones are initially synthesized as
preprohormones.4. Steroid hormones and thyroid hormones are generally
transported in the bloodstream bound to carrier proteins,whereas most peptide and protein hormones are soluble inthe plasma and are carried free in solution.
5. RIA and ELISA have provided major advancements in thefield of endocrinology, but each type of assay has limita-tions.
6. Altered hormone-receptor interactions may lead to en-docrine abnormalities.
K E Y C O N C E P T S
PART IX Endocrine Physiology
567
Endocrinology is the branch of physiology concernedwith the description and characterization of processes
involved in the regulation and integration of cells and or-gan systems by a group of specialized chemical substancescalled hormones. The diagnosis and treatment of a largenumber of endocrine disorders is an important aspect ofany general medical practice. Certain endocrine disease
states, such as diabetes mellitus, thyroid disorders, and re-productive disorders, are fairly common in the general pop-ulation; therefore, it is likely that they will be encounteredrepeatedly in the practice of medicine.
In addition, because hormones either directly or indi-rectly affect virtually every cell or tissue in the body, a num-ber of other prominent diseases not primarily classified asendocrine diseases may have an important endocrine com-ponent. Atherosclerosis, certain forms of cancer, and evencertain psychiatric disorders are examples of conditions inwhich an endocrine disturbance may contribute to the pro-gression or severity of disease.
GENERAL CONCEPTS OF ENDOCRINE CONTROL
Hormones are bloodborne substances involved in regulat-ing a variety of processes. The word “hormone” is derivedfrom the Greek hormaein,which means to “excite” or to “stirup.” The endocrine system forms an important communica-tion system that serves to regulate, integrate, and coordi-nate a variety of different physiological processes. Theprocesses that hormones regulate fall into four areas: (1) thedigestion, utilization, and storage of nutrients; (2) growthand development; (3) ion and water balance; and (4) repro-ductive function.
Hormones Regulate andCoordinate Many Functions
It is difficult to describe hormones in absolute terms. As aworking definition, however, it can be said that hormonesserve as regulators and coordinators of various biological

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 2/14
568 PART IX ENDOCRINE PHYSIOLOGY
functions in the animals in which they are produced. Theyare highly potent, specialized, organic molecules producedby endocrine cells in response to specific stimuli and exerttheir actions on specific target cells. These target cells areequipped with receptors that bind hormones with highaffinity and specificity; when bound, they initiate charac-teristic biological responses by the target cells.
In the past, definitions or descriptions of hormones usu-
ally included a phrase indicating that these substances weresecreted into the bloodstream and carried by the blood toa distant target tissue. Although many hormones travel bythis mechanism, we now realize that there are many hor-mones or hormone-like substances that play importantroles in cell-to-cell communication that are not secreted di-rectly into the bloodstream. Instead, these substances reachtheir target cells by diffusion through the interstitial fluid.Recall the discussion of autocrine and paracrine mecha-nisms in Chapter 1.
Hormone Receptors Determine Whether aCell Will Respond to a Hormone
In the endocrine system, a hormone molecule secretedinto the blood is free to circulate and contact almost anycell in the body. However, only target cells , those cellsthat possess specific receptors for the hormone, will re-spond to that hormone. A hormone receptor is the mo-lecular entity (usually a protein or glycoprotein) eitheroutside or within a cell that recognizes and binds a par-ticular hormone. When a hormone binds to its receptor,biological effects characteristic of that hormone are initi-ated. Therefore, in the endocrine system, the basis forspecificity in cell-to-cell communication rests at the levelof the receptor. Similar concepts apply to autocrine andparacrine mechanisms of communication.
A certain degree of specificity is ensured by the re-stricted distribution of some hormones. For example, sev-eral hormones produced by the hypothalamus regulatehormone secretion by the anterior pituitary. These hor-mones are carried via small blood vessels directly from thehypothalamus to the anterior pituitary, prior to enteringthe general systemic circulation. The anterior pituitary is,therefore, exposed to considerably higher concentrationsof these hypothalamic hormones than the rest of the body;as a result, the actions of these hormones focus on cells ofthe anterior pituitary. Another mechanism that restrictsthe distribution of active hormone is the local transforma-tion of a hormone within its target tissue from a less activeto a more active form. An example is the formation of di-hydrotestosterone from testosterone, occurring in such an-drogen target tissues as the prostate gland. Dihydrotestos-terone is a much more potent androgen than testosterone.Because the enzyme that catalyzes this conversion is foundonly in certain locations, its cell or tissue distributionpartly localizes the actions of the androgens to these sites.Therefore, while receptor distribution is the primary fac-tor in determining the target tissues for a specific hor-mone, other factors may also focus the actions of a hor-mone on a particular tissue.
Feedback Regulation Is an ImportantPart of Endocrine Function
The endocrine system, like many other physiological sys-tems, is regulated by feedback mechanisms. The mecha-nism is usually negative feedback, although a few positivefeedback mechanisms are known. Both types of feedbackcontrol occur because the endocrine cell, in addition tosynthesizing and secreting its own hormone product, hasthe ability to sense the biological consequences of secre-tion of that hormone. This enables the endocrine cell to ad-
just its rate of hormone secretion to produce the desiredlevel of effect, ensuring the maintenance of homeostasis.
Hormone secretion may be regulated via simple first-or-der feedback loops or more complex multilevel second- orthird-order feedback loops. Since negative feedback ismost prevalent in the endocrine system, only examples ofthis type are illustrated here.
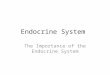
Simple Feedback Loops. First-order feedback regulationis the simplest type and forms the basis for more complexmodes of regulation. Figure 31.1A illustrates a simple first-
order feedback loop. In this example, an endocrine cell se-cretes a hormone that produces a specific biological effectin its target tissue. It also senses the magnitude of the effectproduced by the hormone. As the biological response in-creases, the amount of hormone secreted by the endocrinecell is appropriately decreased.
Complex Feedback Loops. More commonly, feedbackregulation in the endocrine system is complex, involvingsecond- or third-order feedback loops. For example, multi-ple levels of feedback regulation may be involved in regu-lating hormone production by various endocrine glands un-der the control of the anterior pituitary (Fig. 31.1B). Theregulation of target gland hormone secretion, such as adre-nal steroids or thyroid hormones, begins with productionof a releasing hormone by the hypothalamus. The releasinghormone stimulates production of a trophic hormone bythe anterior pituitary, which, in turn, stimulates the pro-duction of the target gland hormone by the target gland. Asindicated by the dashed lines in Figure 31.1B, the targetgland hormone may have negative-feedback effects to in-hibit secretion of both the trophic hormone from the ante-rior pituitary and the releasing hormone from the hypo-thalamus. In addition, the trophic hormone may inhibitreleasing hormone secretion from the hypothalamus, andin some cases, the releasing hormone may inhibit its ownsecretion by the hypothalamus.
The more complex multilevel form of regulation appearsto provide certain advantages compared with the simpler sys-tem. Theoretically, it permits a greater degree of fine-tuningof hormone secretion, and the multiplicity of regulatory stepsminimizes changes in hormone secretion in the event thatone component of the system is not functioning normally.
It is important to bear in mind the normal feedback rela-tionships that control the secretion of each individual hor-mone are discussed in the chapters that follow. Clinical di-agnoses are often made based on the evaluation of

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 3/14
hormone-effector pairs relative to normal feedback rela-tionships. For example, in the case of anterior pituitary hor-mones, measuring both the trophic hormone and the targetgland hormone concentration provides important informa-tion to help determine whether a defect in hormone pro-duction exists at the level of the pituitary or at the level ofthe target gland. Furthermore, most dynamic tests of en-docrine function performed clinically are based on ourknowledge of these feedback relationships. Dynamic tests
involve a prescribed perturbation of the feedback relation-ship(s); the range of response in a normal individual is wellestablished, while a response outside the normal range is in-dicative of abnormal function at some level and greatly en-hances information gained from static measurements ofhormone concentrations (see Clinical Focus Box 31.1).
Signal Amplification Is an ImportantCharacteristic of the Endocrine System
Another important feature of the endocrine system is signalamplification . Blood concentrations of hormones are ex-ceedingly low, generally, 10 Ϫ 9 to 10 Ϫ 12 mol/L. Even at thehigher concentration of 10 Ϫ 9 mol/L, only one hormonemolecule would be present for roughly every 50 billion wa-ter molecules. Therefore, for hormones to be effective reg-ulators of biological processes, amplification must be partof the overall mechanism of hormone action.
Amplification generally results from the activation of a se-ries of enzymatic steps involved in hormone action. At eachstep, many times more signal molecules are generated thanwere present at the prior step, leading to a cascade of ever-increasing numbers of signal molecules. The self-multiplyingnature of the hormone action pathways provides the molec-ular basis for amplification in the endocrine system.
Pleiotropic Hormone Effects and Multiplicityof Regulation Also Characterize theEndocrine System
Most hormones have multiple actions in their target tissuesand are, therefore, said to have pleiotropic effects . For ex-ample, insulin exhibits pleiotropic effects in skeletal mus-cle, where it stimulates glucose uptake, stimulates glycoly-sis, stimulates glycogenesis, inhibits glycogenolysis,
stimulates amino acid uptake, stimulates protein synthesis,and inhibits protein degradation.In addition, some hormones are known to have different
effects in several different target tissues. For example, testos-terone, the male sex steroid, promotes normal sperm forma-tion in the testes, stimulates growth of the accessory sexglands, such as the prostate and seminal vesicles, and pro-motes the development of several secondary sex character-istics, such as beard growth and deepening of the voice.
Multiplicity of regulation is also common in the en-docrine system. The input of information from severalsources allows a highly integrated response to a variety ofstimuli, which is of ultimate benefit to the whole animal.For example, liver glycogen metabolism may be regulatedor influenced by several different hormones, including in-sulin, glucagon, epinephrine, thyroid hormones, and adre-nal glucocorticoids.
Hormones Are Often Secretedin Definable Patterns
The secretion of any particular hormone is either stimu-lated or inhibited by a defined set of chemical substances in
CHAPTER 31 Endocrine Control Mechanisms 569
Targetcell
Endocrinecell
A
B
Hormone
Biological effect
Hypothalamus
Anteriorpituitary
Targetgland
Releasing hormone
Target glandhormone
Biological effect
Trophic hormone
Simple and complex feedback loops in theendocrine system. A, A simple first-order
feedback loop. B, A complex, multilevel feedback loop: the hy-pothalamic-pituitary-target gland axis. Solid lines indicate stim-ulatory effects; dashed lines indicate inhibitory, negative-feed-back effects.
FIGURE 31.1

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 4/14
570 PART IX ENDOCRINE PHYSIOLOGY
the blood or environmental factors. In addition to thesespecific secretagogues , many hormones are secreted in adefined, rhythmic pattern. These rhythms can take severalforms. For example, they may be pulsatile, episodic spikesin secretion lasting just a few minutes, or they may follow adaily, monthly, or seasonal change in overall pattern. Pul-satile secretion may occur in addition to other longer se-cretory patterns.
For these reasons, a single randomly drawn blood sam-ple for determining a certain hormone concentration maybe of little or no diagnostic value. A dynamic test of en-docrine function in which hormone secretion is specificallystimulated by a known agent often provides much moremeaningful information.
THE NATURE OF HORMONES
Hormones can be categorized by a number of criteria.Grouping them by chemical structure is convenient, sincein many cases, hormones with similar structures also usesimilar mechanisms to produce their biological effects. Inaddition, hormones with similar chemical structures areusually produced by tissues with similar embryonic ori-gins. Hormones can generally be classed as one of threechemical types.
The Simplest Hormones, in Terms of Structure,
Consist of One or Two Modified Amino AcidsHormones derived from one or two amino acids are smallin size and often hydrophilic. These hormones are formedby conversion from a commonly occurring amino acid; ep-inephrine and thyroxine, for example, are derived from ty-rosine. Each of these hormones is synthesized by a particu-lar sequence of enzymes that are primarily localized in theendocrine gland involved in its production. The synthesisof amino acid-derived hormones can, therefore, be influ-enced in a relatively specific fashion by a variety of envi-ronmental or pharmacological agents. The steps involved
in the synthesis of these hormones are discussed in detail in
later chapters.
Many Hormones Are Polypeptides
Hormones in the polypeptide group are quite diverse insize and complexity. They may be as small as the tripeptidethyrotropin-releasing hormone (TRH) or as large as humanchorionic gonadotropin (hCG), which is composed of sep-arate alpha and beta subunits, has a molecular weight of ap-proximately 34 kDa, and is a glycoprotein comprised of16% carbohydrate by weight.
Within the polypeptide class of hormones are a numberof families of hormones, some of which are listed inTable 31.1. Hormones can be grouped into these families asa result of considerable homology with regard to amino acidsequence and structure. Presumably, the similarity of struc-
C L I N I C A L F O C U S B O X 3 1 . 1
Growth Hormone and Pulsatile Hormone Secretion
Growth hormone is a 191-amino acid protein hormonethat is synthesized and secreted by somatotrophs of theanterior lobe of the pituitary gland. As described in Chap-ter 32, the hormone plays a role in regulating bone growth
and energy metabolism in skeletal muscle and adipose tis-sue. A deficiency in growth hormone production duringadolescence results in dwarfism and overproduction re-sults in gigantism. Measurements of circulating growthhormone levels are, therefore, desirable in children whosegrowth rate is not appropriate for their age.
Like many other peptide hormones, growth hormonesecretion occurs in a pulsatile fashion. The most consistentpulse occurs just after the onset of deep sleep and lasts forabout 1 hour. There are usually 4 to 6 irregularly timedpulses throughout the remainder of the day. In order to ob-
tain reliable information about growth hormone secretion,endocrinologists employ a dynamic test of growth hor-mone secretory capacity. There are several variations of this test that are used at different hospitals. In one test, abolus of arginine, which is known to stimulate growth hor-
mone secretion, is given and a blood sample is taken ashort time later for the measurement of growth hormoneconcentrations. Another test makes use of the fact that hy-poglycemia is a known stimulus for growth hormone se-cretion. Mild hypoglycemia is induced by an injection of in-sulin, and a blood sample is drawn a short time later.Regardless of which test is used, by perturbing the systemin a well-prescribed fashion, the endocrinologist is able togain important information about growth hormone secre-tion that would not be possible if a random blood samplewere used.
TABLE 31.1 Examples of Peptide Hormone Families
Insulin FamilyInsulinInsulin-like growth factor IInsulin-like growth factor IIRelaxinGlycoprotein FamilyLuteinizing hormone (LH)
Follicle-stimulating hormone (FSH)Thyroid-stimulating hormone (TSH)Human chorionic gonadotropin (hCG)Growth Hormone FamilyGrowth hormone (GH)Prolactin (PRL)Human placental lactogen (hPL)Secretin FamilySecretinVasoactive intestinal peptide (VIP)GlucagonGastric inhibitory peptide (GIP)

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 5/14
ture in these families resulted from the evolution of a singleancestral hormone into each of the separate and distincthormones. In many cases, there is also considerable homol-ogy among receptors for the hormones within a family.
Steroid Hormones Are Derived From Cholesterol
Steroids are lipid-soluble, hydrophobic molecules synthe-
sized from cholesterol. They can be classified into six cate-gories, based on their primary biological activity. An ex-ample of each category is shown in Figure 31.2.
Glucocorticoids , such as cortisol, are primarily pro-duced in cells of the adrenal cortex and regulate processesinvolved in glucose, protein, and lipid homeostasis. Gluco-corticoids generally produce effects that are catabolic innature. Aldosterone, a primary example of a mineralocorti-coid , is produced in cells of the outermost portion of theadrenal cortex. Aldosterone is primarily involved in regu-lating sodium and potassium balance by the kidneys and isthe principal mineralocorticoid in the body.
Androgens , such as testosterone, are primarily producedin the testes, but physiologically significant amounts can besynthesized by the adrenal cortex as well. The primary fe-male sex hormone is estradiol, a member of the estrogenfamily, produced by the ovaries and placenta. Progestins ,such as progesterone, are involved in maintenance of preg-nancy and are produced by the ovaries and placenta.
The calciferols , such as 1,25-dihydroxycholecalciferol,
are involved in the regulation of calcium homeostasis. 1,25-dihydroxycholecalciferol is the hormonally active form of vitamin D and is formed by a sequence of reactions occur-ring in skin, liver, and kidneys.
Polypeptide and Protein Hormones AreSynthesized in Advance of Need andStored in Secretory Vesicles
Steroid hormones are synthesized and secreted on demand,but polypeptide hormones are typically stored prior to se-cretion. Steroid hormone synthesis and secretion are dis-
CHAPTER 31 Endocrine Control Mechanisms 571
Cortisol(a glucocorticoid)
Testosterone(an androgen)
Progesterone(a progestin) 1,25 (OH) 2 Cholecalciferol
(a calciferol)
Estradiol(an estrogen)
(Aldehyde) (Hemiacetal)Aldosterone
(a mineralocorticoid)
Examples of the six types of naturally occurring steroids.FIGURE 31.2

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 6/14
572 PART IX ENDOCRINE PHYSIOLOGY
cussed in Chapter 34; the discussion here is confined to thesynthesis and secretion of polypeptide hormones.
Preprohormones and Prohormones. Like other proteinsdestined for secretion, polypeptide hormones are synthe-sized with a pre-or signalpeptide at their amino terminal endthat directs the growing peptide chain into the cisternae ofthe rough ER. Most, if not all, polypeptide hormones are
synthesized as part of an even larger precursor or prepro-hormone . The prepeptide is cleaved off upon entry of thepreprohormone into the rough ER, to form the prohor-mone . As the prohormone is processed through the Golgiapparatus and packaged into secretory vesicles, it is prote-olytically cleaved at one or more sites to yield active hor-mone. In many cases, preprohormones may contain the se-quences for several different biologically active molecules.These active elements may, in some cases, be separated byinactive spacer segments of peptide.
Examples of prohormones that are the precursors forpolypeptide hormones, which illustrate the multipotent na-ture of these precursors, are shown schematically in Figure31.3. Note, for example, that proopiomelanocortin
(POMC) actually contains the sequences for several bio-logically active signal molecules. Propressophysin serves asthe precursor for the nonapeptide hormone arginine vaso-pressin (AVP). The precursor for TRH contains five repeatsof the TRH tripeptide in one single precursor molecule.
In general, two basic amino acid residues, either lys-argor arg-arg, demarcate the point(s) at which the prohor-mone will be cleaved into its biologically active compo-nents. Presumably, these two basic amino acids serve asspecific recognition sites for the trypsin-like endopepti-dases thought to be responsible for cleavage of the prohor-mones. Although somewhat rare, there are documentedcases of inherited diseases in which a point mutation in-
volving an amino acid residue at the cleavage site results in
an inability to convert the prohormone into active hor-mone, resulting in a state of hormone deficiency. Partially
cleaved precursor molecules having limited biological ac-tivity may be found circulating in the blood in some ofthese cases.
In some disease states, large amounts of intact precursormolecules are found in the circulation. This situation maybe the result of endocrine cell hyperactivity or even un-controlled production of hormone precursor by nonen-docrine tumor cells. Although precursors usually have rela-
tively low biological activity, if they are secreted insufficiently high amounts, they may still produce biologicaleffects. In some cases, these effects may be the first recog-nized sign of neoplasia.
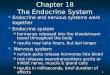
Tissue-specific differences in the processing of prohor-mones are well known. Although the same prohormonegene may be expressed in different tissues, tissue-specificdifferences in the way the molecule is cleaved give rise todifferent final secretory products. For example, within alphacells of the pancreas, proglucagon is cleaved at two posi-tions to yield three peptides, illustrated in Figure 31.4 (left).Glucagon, an important hormone in the regulation of car-bohydrate metabolism, is the best characterized of the threepeptides. In contrast, in other cells of the gastrointestinal
(GI) tract in which proglucagon is also produced, the mole-cule is cleaved at three different positions such that gli-centin, glucagon-like peptide-1 (GLP-1), and glucagon-likepeptide-2 (GLP-2) are produced (Fig. 31.4, right).
Intracellular Movement of Secretory Vesicles and Exocy-tosis. Upon insertion of the preprohormone into the cis-ternae of the ER, the prepeptide or signal peptide is rapidlycleaved from the amino terminal end of the molecule. Theresulting prohormone is translocated to the Golgi appara-
γ -MSH γ -LPH β-Endorphinα-MSH CLIP
ACTH
AVP Neurophysin
Proopiomelanocortin(POMC)
Propressophysin
Prothyrotropin-releasing hormone
T R H T R
H T R
H T R
H T R
H
The structure of three prohormones. Rela-tive sizes of individual peptides are only ap-
proximations. MSH ϭ melanocyte-stimulating hormone; CLIPϭ corticotropin-like intermediate lobe peptide; LPH ϭ
lipotropin; AVP ϭ arginine vasopressin; TRH ϭ thyrotropin-releasing hormone.
FIGURE 31.3
N-peptide Glucagon IP-1 IP-2GLP-1 GLP-2
Proglucagon
Pancreaticalpha cells
Gastrointestinaltract
Glicentin
GlucagonN-peptide IP-1
GLP-1
IP-2
GLP-2
N-peptide
Glucagon
IP-1 GLP-1 GLP-2IP-2
The differential processing of prohor-mones. In alpha cells of the pancreas (left), the
major bioactive product formed from proglucagon is glucagon it-self. It is not currently known whether the other peptides areprocessed to produce biologically active molecules. In intestinalcells (right), proglucagon is cleaved to produce the four peptidesshown. Glicentin is the major glucagon-containing peptide in theintestine. IP-1, intervening peptide 1; IP-2, intervening peptide 2;GLP-1, glucagon-like peptide-1; GLP-2, glucagon-like peptide 2.
FIGURE 31.4

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 7/14
tus, where it is processed and packaged for export. Afterprocessing in the Golgi apparatus, peptide hormones arestored in membrane-enclosed secretory vesicles. Secretionof the peptide hormone occurs by exocytosis; the secretory
vesicle is translocated to the cell surface, its membrane
fuses with the plasma membrane, and its contents are re-leased into the extracellular fluid. Movement of the secre-tory vesicle and membrane fusion are triggered by an in-crease in cytosolic calcium stemming from an influx ofcalcium into the cytoplasm from internal organelles or theextracellular fluid. In some cells, an increase in cAMP andthe subsequent activation of protein kinases is also involvedin the stimulus-secretion coupling process. Elements of themicrotubule-microfilament system play a role in the move-ment of secretory vesicles from their intracellular storagesites toward the cell membrane.
The cleavage of prohormone into active hormone mole-cules typically takes place during transit through the Golgiapparatus or, perhaps, soon after entry into secretory vesi-cles. Secretory vesicles, therefore, contain not only activehormone but also the excised biologically inactive frag-ments. When active hormone is released into the blood, aquantitatively similar amount of inactive fragment is also re-leased. In some instances, this forms the basis for an indirectassessment of hormone secretory activity (see Clinical FocusBox 31.2). Other types of processing of peptide hormonesthat may occur during transit through the Golgi apparatusinclude glycosylation and coupling of subunits.
Many Hormones Reach Their Target Cellsby Transport in the Bloodstream
According to the classical definition, hormones are carriedby the bloodstream from their site of synthesis to their tar-get tissues. However, the manner in which different hor-mones are carried in the blood varies.
Transport of Amino Acid-Derived and Polypeptide Hor-mones. Most amino acid-derived and polypeptide hor-mones dissolve readily in the plasma, and thus no specialmechanisms are required for their transport. Steroid andthyroid hormones are relatively insoluble in plasma. Mech-anisms are present to promote their solubility in the aque-ous phase of the blood and ultimate delivery to a target cell.
Transport of Steroid and Thyroid Hormones. In mostcases, 90% or more of steroid and thyroid hormones in theblood are bound to plasma proteins. Some of the plasma pro-teins that bind hormones are specialized, in that they have aconsiderably higher affinity for one hormone over another,
whereas others, such as serum albumin, bind a variety of hy-drophobic hormones. The extent to which a hormone is pro-tein-bound and the extent to which it binds to specific ver-sus nonspecific transport proteins vary from one hormone toanother. The principal binding proteins involved in specificand nonspecific transport of steroid and thyroid hormonesare listed in Table 31.2. These proteins are synthesized andsecreted by the liver, and their production is influenced bychanges in various nutritional and endocrine factors.
Typically, for hormones that bind to carrier proteins,only 1 to 10% of the total hormone present in the plasmaexists free in solution. However, only this free hormone isbiologically active. Bound hormone cannot directly inter-act with its receptor and, thus, is part of a temporarily inac-
tive pool. However, free hormone and carrier-bound hor-mone are in a dynamic equilibrium with each other(Fig. 31.5). The size of the free hormone pool and, there-fore, the amount available to receptors are influenced notonly by changes in the rate of secretion of the hormone butalso by the amount of carrier protein available for hormonebinding and the rate of degradation or removal of the hor-mone from the plasma.
CHAPTER 31 Endocrine Control Mechanisms 573
C L I N I C A L F O C U S B O X 3 1 . 2
Pancreatic Beta Cell Function and C-Peptide
Beta cells of the human pancreas produce and secrete in-sulin . The product of the insulin gene is a peptide knownas preproinsulin. As with other secretory peptides, theprepeptide or signal peptide is cleaved off early in the
biosynthetic process, yielding proinsulin. Proinsulin is an86-amino acid protein that is subsequently cleaved at twosites to yield insulin and a 31-amino acid peptide known asC-peptide . Insulin and C-peptide are, therefore, localizedwithin the same secretory vesicle and are co-secreted intothe bloodstream.
For these reasons, measurements of circulating C-pep-tide levels can provide a valuable indirect assessment of beta cell insulin secretory capacity. In diabetic patientswho are receiving exogenous insulin injections, the meas-urement of circulating insulin levels would not provide any
useful information about their own pancreatic function be-cause it would primarily be the injected insulin that wouldbe measured. However, an evaluation of C-peptide levelsin such patients would provide an indirect measure of howwell the beta cells were functioning with regard to insulinproduction and secretion.
TABLE 31.2 Circulating Transport Proteins
Principal Hormone(s)Transport Protein Transported
SpecificCorticosteroid-binding globulin Cortisol, aldosterone
(CBG, transcortin)Thyroxine-binding g lobulin Thyroxine, t riiodothyronine
(TBG)Sex hormone-binding globulin Testosterone, estrogen
(SHBG)Nonspecific
Serum albumin Most steroids, thyroxine,triiodothyronine
Transthyretin (prealbumin) Thyroxine, some steroids

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 8/14
574 PART IX ENDOCRINE PHYSIOLOGY
In addition to increasing the total amount of hormonethat can be carried in plasma, transport proteins also pro-
vide a relatively large reservoir of hormone that buffersrapid changes in free hormone concentrations. As unboundhormone leaves the circulation and enters cells, additionalhormone dissociates from transport proteins and replacesfree hormone that is lost from the free pool. Similarly, fol-lowing a rapid increase in hormone secretion or the thera-peutic administration of a large dose of hormone, the ma-
jority of newly appearing hormone is bound to transportproteins, since under most conditions these are present inconsiderable excess.
Protein binding greatly slows the rate of clearance ofhormones from plasma. It not only slows the entry of hor-mones into cells, slowing the rate of hormone degradation,but also prevents loss by filtration in the kidneys.
From a diagnostic standpoint, it is important to recog-nize that most hormone assays are reported in terms of to-tal concentration (i.e., the sum of free and bound hor-mone), not just free hormone concentration. The amountof transport protein and the total plasma hormone contentare known to change under certain physiological or patho-logical conditions, while the free hormone concentrationmay remain relatively normal. For example, increased con-centrations of binding proteins are seen during pregnancyand decreased concentrations are seen with certain forms ofliver or kidney disease. Assays of total hormone contentmight be misleading, since free hormone concentrationsmay be in the normal range. In such cases, it is helpful todetermine the extent of protein binding, so free hormoneconcentrations can be estimated.
The proportion of a hormone that is free, bound to aspecific transport protein, and bound to albumin varies de-pending on its solubility, its relative affinity for the twoclasses of transport proteins, and the relative abundance ofthe transport proteins. For example, the affinity of cortisolfor corticosteroid-binding globulin (CBG) is more than
1,000 times greater than its affinity for albumin, but albu-min is present in much higher concentrations than CBG.Therefore, about 70% of plasma cortisol is bound to CBG,20% is bound to albumin, and the remaining 10% is free insolution. Aldosterone also binds to CBG, but with a muchlower affinity, such that only 17% is bound to CBG, 47%associates with albumin, and 36% is free in solution.
As this example indicates, more than one hormone may
be capable of binding to a specific transport protein. Whenseveral such hormones are present simultaneously, they com-pete for a limited number of binding sites on these transportproteins. For example, cortisol and aldosterone compete forCBG binding sites. Increases in plasma cortisol result in dis-placement of aldosterone from CBG, raising the unbound(active) concentration of aldosterone in the plasma. Simi-larly, prednisone, a widely used synthetic corticosteroid, candisplace about 35% of the cortisol normally bound to CBG.As a result, with prednisone treatment, the free cortisol con-centration is higher than might be predicted from measuredconcentrations of total cortisol and CBG.
Peripheral Transformation, Degradation,and Excretion of Hormones, in Part,Determine Their Activity
As a general rule, hormones are produced by their gland ortissue of origin in an active form. However, for a few no-table exceptions, the peripheral transformation of a hor-mone plays a very important role in its action.
Peripheral Transformation of Hormones. Specific hor-mone transformations may be impaired because of a con-genital enzyme deficiency or drug-induced inhibition ofenzyme activity, resulting in endocrine abnormalities.Well-known transformations are the conversion of testos-terone to dihydrotestosterone (see Chapter 37) and theconversion of thyroxine to triiodothyronine (see Chapter33). Other examples are the formation of the octapeptideangiotensin II from its precursor, angiotensinogen (seeChapter 34), and the formation of 1,25-dihydroxychole-calciferol from cholecalciferol (see Chapter 36).
Mechanisms of Hormone Degradation and Excretion.As in any regulatory control system, it is necessary for thehormonal signal to dissipate or disappear once appropriateinformation has been transferred and the need for furtherstimulus has ceased. As described earlier, steady-stateplasma concentrations of hormone are determined not onlyby the rate of secretion but also by the rate of degradation.Thus, any factor that significantly alters the degradation ofa hormone can potentially alter its circulating concentra-tion. Commonly, however, secretory mechanisms cancompensate for altered degradation such that plasma hor-mone concentrations remain within the normal range.Processes of hormone degradation show little, if any, regu-lation; alterations in the rates of hormone synthesis or se-cretion in most cases provide the primary mechanism for al-tering circulating hormone concentrations.
For most hormones, the liver is quantitatively the mostimportant site of degradation; for a few others, the kidneysplay a significant role as well. Diseases of the liver and kid-
The relationship between hormone secre-tion, carrier protein binding, and hormone
degradation. This relationship determines the amount of freehormone available for receptor binding and the production of bi-ological effects.
FIGURE 31.5

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 9/14
neys may, therefore, indirectly influence endocrine statusas a result of altering the rates at which hormones are re-moved from the circulation. Various drugs also alter normalrates of hormone degradation; thus, the possibility of indi-rect drug-induced endocrine abnormalities also exists. Inaddition to the liver and kidneys, target tissues may take upand degrade quantitatively smaller amounts of hormone. Inthe case of peptide and protein hormones, this occurs via
receptor-mediated endocytosis.The nature of specific structural modification(s) in- volved in hormone inactivation and degradation differsfor each hormone class. As a general rule, however, spe-cific enzyme-catalyzed reactions are involved. Inactiva-tion and degradation may involve complete metabolismof the hormone to entirely different products, or it may belimited to a simpler process involving one or two steps,such as a covalent modification to inactivate the hor-mone. Urine is the primary route of excretion of hormonedegradation products, but small amounts of intact hor-mone may also appear in the urine. In some cases, meas-uring the urinary content of a hormone or hormonemetabolite provides a useful, indirect, noninvasive means
of assessing endocrine function.The degradation of peptide and protein hormones has
been studied only in a limited number of cases. However,it appears that peptide and protein hormones are inacti-
vated in a variety of tissues by proteolytic attack. The firststep appears to involve attack by specific peptidases, re-sulting in the formation of several distinct hormone frag-ments. These fragments are then metabolized by a varietyof nonspecific peptidases to yield the constituent aminoacids, which can be reused.
The metabolism and degradation of steroid hormoneshas been studied in much more detail. The primary organinvolved is the liver, although some metabolism also takesplace in the kidneys. Complete steroid metabolism gener-ally involves a combination of one or more of five generalclasses of reactions: reduction, hydroxylation, side chaincleavage, oxidation, and esterification. Reduction reactionsare the principal reactions involved in the conversion of bi-ologically active steroids to forms that possess little or noactivity. Esterification (or conjugation) reactions are alsoparticularly important. Groups added in esterification reac-tions are primarily glucuronate and sulfate. The addition ofsuch charged moieties enhances the water solubility of themetabolites, facilitating their excretion. Steroid metabo-lites are eliminated from the body primarily via the urine,although smaller amounts also enter the bile and leave thebody in the feces.
At times, quantitative information concerning the rate ofhormone metabolism is clinically useful. One index of therate at which a hormone is removed from the blood is themetabolic clearance rate (MCR). The metabolic clearanceof a hormone is analogous to that of renal clearance (seeChapter 23). The MCR is the volume of plasma cleared ofthe hormone in question per unit time. It is calculated fromthe equation:
MCR ϭ Hormone removed per unit time (mg/min) (1)Plasma concentration (mg/mL)
and is expressed in mL plasma/min.
One approach to measuring MCR involves injecting asmall amount of radioactive hormone into the subject andthen collecting a series of timed blood samples to deter-mine the amount of radioactive hormone remaining. Basedon the rate of disappearance of hormone from the blood, itshalf-life and MCR can be calculated. The MCR and half-life are inversely related—the shorter the half-life, thegreater the MCR. The half-lives of different hormones vary
considerably, from 5 minutes or less for some to severalhours for others. The circulating concentration of hor-mones with short half-lives can vary dramatically over ashort period of time. This is typical of hormones that regu-late processes on an acute minute-to-minute basis, such as anumber of those involved in regulating blood glucose. Hor-mones for which rapid changes in concentration are not re-quired, such as those with seasonal variations and thosethat regulate the menstrual cycle, typically have longerhalf-lives.
The Measurement of Hormone ConcentrationsIs an Important Tool in Endocrinology
The concentration of hormone present in a biological fluidis often measured to make a clinical diagnosis of a suspectedendocrine disease or to study basic endocrine physiology.Substantial advancements have been made in measuringhormone concentrations.
Bioassay. Even before hormones were chemically char-acterized, they were quantitated in terms of biological re-sponses they produced. Thus, early assays for measuringhormones were bioassays that depended on a hormone’sability to produce a characteristic biological response. As aresult, hormones came to be quantitated in terms of units,defined as an amount sufficient to produce a response ofspecified magnitude under a defined set of conditions. Aunit of hormone is, thus, arbitrarily determined. Althoughbioassays are rarely used today for diagnostic purposes,many hormones are still standardized in terms of biologicalactivity units . For example, commercial insulin is still soldand dispensed based on the number of units in a particularpreparation, rather than by the weight or the number ofmoles of insulin.
Bioassays in general suffer from a number of shortcom-ings, including a relative lack of specificity and a lack ofsensitivity. In many cases, they are slow and cumbersometo perform, and often they are expensive, since biological
variability often requires the inclusion of many animals inthe assay.
Radioimmunoassay. Development of the radioim-munoassay (RIA) in the late 1950s and early 1960s was amajor step forward in clinical and research endocrinology.Much of our current knowledge of endocrinology is basedon this method. A RIA or closely related assay is now avail-able for virtually every known hormone. In addition, RIAshave been developed to measure circulating concentrationsof a variety of other biologically relevant proteins, drugs,and vitamins.
The RIA is a prototype for a larger group of assaystermed competitive binding assays . These are modifica-
CHAPTER 31 Endocrine Control Mechanisms 575

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 10/14
576 PART IX ENDOCRINE PHYSIOLOGY
tions and adaptations of the original RIA, relying to a largedegree on the principle of competitive binding on whichthe RIA is based. It is beyond the scope of this text to de-scribe in detail the competitive binding assays currentlyused to measure hormone concentrations, but the princi-ples are the same as those for the RIA.
The two key components of a RIA are a specific anti-body (Ab) that has been raised against the hormone in
question and a radioactively labeled hormone (H*). If thehormone being measured is a peptide or protein, the mole-cule is commonly labeled with a radioactive iodine atom(125 I or 131 I) that can be readily attached to tyrosineresidues of the peptide chain. For substances lacking tyro-sine residues, such as steroids, labeling may be accom-plished by incorporating radioactive carbon ( 14 C) or hy-drogen ( 3 H). In either case, the use of the radioactivehormone permits detection and quantification of very smallamounts of the substance.
The RIA is performed in vitrousing a series of test tubes.Fixed amounts of Ab and of H* are added to all tubes(Fig. 31.6A). Samples (plasma, urine, cerebrospinal fluid,etc.) to be measured are added to individual tubes. Varying
known concentrations of unlabeled hormone (the stan-dards) are added to a series of identical tubes. The principleof the RIA, as indicated in Figure 31.6B, is that labeled andunlabeled hormone compete for a limited number of anti-body binding sites. The amount of each hormone that isbound to antibody is a proportion of that present in solu-tion. In a sample containing a high concentration of hor-mone, less radioactive hormone will be able to bind to theantibody, and less antibody will be able to bind to the ra-dioactive hormone. In each case, the amount of radioactiv-ity present as antibody-bound H* is determined. The re-sponse produced by the standards is used to generate astandard curve (Fig. 31.7). Responses produced by the un-known samples are then compared to the standard curve to
determine the amount of hormone present in the unknowns(see dashed lines in Fig. 31.7).
One major limitation of RIAs is that they measure im-munoreactivity, rather than biological activity. The pres-ence of an immunologically related but different hormoneor of heterogeneous forms of the same hormone can com-plicate the interpretation of the results. For example,POMC, the precursor of ACTH, is often present in highconcentrations in the plasma of patients with bronchogeniccarcinoma. Antibodies for ACTH may cross-react withPOMC. The results of a RIA for ACTH in which such anantibody is used may suggest high concentrations ofACTH, when actually POMC is being detected. BecausePOMC has less than 5% of the biological potency ofACTH, there may be little clinical evidence of significantlyelevated ACTH. If appropriate measures are taken, how-ever, such possible pitfalls can be overcome in most cases,and reliable results from the RIA can be obtained.
One important modification of the RIA is the radiore-ceptor assay , which uses specific hormone receptors ratherthan antibodies as the hormone-binding reagent. In theory,this method measures biologically active hormone, sincereceptor binding rather than antibody recognition is as-sessed. However, the need to purify hormone receptors andthe somewhat more complex nature of this assay limit itsusefulness for routine clinical measurements. It is morelikely to be used in a research setting.
ELISA. The enzyme-linked immunosorbent assay(ELISA) is a solid-phase, enzyme-based assay whose useand application have increased considerably over the pasttwo decades. A typical ELISA is a colorimetric or fluoro-metric assay, and therefore, the ELISA, unlike the RIA, doesnot produce radioactive waste, which is an advantage, con-sidering environmental concerns and the rapidly increasingcost of radioactive waste disposal. In addition, because it is
Antibody(Ab)
Radioactivehormone
(H*)
Hormone-antibodycomplex(Ab-H*)
A
B
The principles of radioimmunoassay (RIA).A, Specific antibodies (Ab) bind with radioactive
hormone (H*) to form hormone-antibody complexes (Ab-H*). B,When unlabeled hormone (open circles) is also introduced into thesystem, less radioactive hormone binds to the antibody. (Modifiedfrom Hedge GA, Colby HD, Goodman RL. Clinical EndocrinePhysiology. Philadelphia: WB Saunders, 1987.)
FIGURE 31.6
0
20
40
60
80
100
R a
d i o a c
t i v e
h o r m o n e - a n
t i b o
d y c o m p
l e x
( p e r c e n
t a g e o
f m a x
i m u m
)
0 1 2 3Unlabeled hormone
(arbitrary units)
4 5 6
A typical RIA standard curve. As indicatedby the dashed lines, the hormone content in
unknown samples can be deduced from the standard curve. (Mod-ified from Hedge GA, Colby HD, Goodman RL. Clinical En-docrine Physiology. Philadelphia: WB Saunders, 1987.)
FIGURE 31.7

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 11/14
a solid-phase assay, the ELISA can be automated to a largedegree, which reduces costs. Figure 31.8 shows a relativelysimple version of an ELISA. More complex assays usingsimilar principles have been developed to overcome a vari-ety of technical problems, but the basic principle remainsthe same. In recent years the RIA has been the primary as-say used clinically; its use has expanded considerably, andit will likely be the predominant assay in the future because
of the advantages listed above.
MECHANISMS OF HORMONE ACTION
As indicated earlier, hormones are one mechanism by whichcells communicate with one another. Fidelity of communi-cation in the endocrine system depends on each hormone’sability to interact with a specific receptor in its target tissues.This interaction results in the activation (or inhibition) of aseries of specific events in cells that results in precise bio-logical responses characteristic of that hormone.
The binding of a hormone to its receptor with subsequentactivation of the receptor is the first step in hormone actionand also the point at which specificity is determined withinthe endocrine system. Abnormal interactions of hormoneswith their receptors are involved in the pathogenesis of anumber of endocrine disease states, and therefore, consider-able attention has been paid to this aspect of hormone action.
The Kinetics of Hormone-Receptor BindingDetermines, in Part, the Biological Response
The probability that a hormone-receptor interaction willoccur is related to both the abundance of cellular receptorsand the receptor’s affinity for the hormone relative to theambient hormone concentration. The more receptors avail-able to interact with a given amount of hormone, thegreater the likelihood of a response. Similarly, the higherthe affinity of a receptor for the hormone, the greater thelikelihood that an interaction will occur. The circulatinghormone concentration is, of course, a function of the rateof hormone secretion relative to hormone degradation.
The association of a hormone with its receptor generallybehaves as if it were a simple, reversible chemical reactionthat can be described by the following kinetic equation:
[H] ϩ [R] [HR] (2)
where [H] is the free hormone concentration, [R] is the un-occupied receptor concentration, and [HR] is the hor-mone-receptor complex (also referred to as bound hor-mone or occupied receptor).
Assuming a simple chemical equilibrium, it follows that
Ka ϭ [HR]/[H] ϫ [R] (3)
where K a is the association constant. If R 0 is defined asthe total receptor number (i.e., [R] ϩ [HR]), then aftersubstituting and rearranging, we obtain the following re-lationship:
[HR]/[H] ϭ Ϫ Ka [HR] ϩ Ka R 0 (4)
Literally translated, this equation states:
Bound hormone ϭ Ϫ Ka ϫ Bound hormone (5)ϩ Ka ϫ Total receptor number
Free hormoneNotice that equations 4 and 5 have the general form of
an equation for a straight line: y ϭ mx ϩ b.To obtain information regarding a particular hormone-
receptor system, a fixed number of cells (and, therefore, afixed number of receptors) is incubated in vitroin a series oftest tubes with increasing amounts of hormone. At eachhigher hormone concentration, the amount of receptor-bound hormone is increased until all receptors are occupiedby hormone. Receptor number and affinity can be obtainedby using the relationships given in equation 5 above andplotting the results as the ratio of receptor-bound hormoneto free hormone ([HR]/[H]) as a function of the amount ofbound hormone ([HR]). This type of analysis is known as aScatchard plot (Fig. 31.9). In theory, a Scatchard plot ofsimple, reversible equilibrium binding is a straight line (Fig.31.9A), with the slope of the line being equal to the nega-tive of the association constant ( Ϫ Ka ) and the x-intercept
CHAPTER 31 Endocrine Control Mechanisms 577
Enz
Ab
Ab
2
1
Ab3
The basic components of an ELISA. A typi-cal ELISA is performed in a 3 ϫ 5-inch plastic
plate containing 96 small wells. Each well is precoated with anantibody (Ab 1 ) that is specific for the hormone (H) being meas-ured. Unknown samples or standards are introduced into thewells, followed by a second hormone-specific antibody (Ab 2 ). Athird antibody (Ab 3 ), which recognizes Ab 2 , is then added. Ab 3 iscoupled to an enzyme that will convert an appropriate substrate(S) into a colored or fluorescent product (P). The amount ofproduct formed can be determined using optical methods. Afterthe addition of each antibody or sample to the wells, the platesare incubated for an appropriate period of time to allow antibod-ies and hormones to bind. Any unbound material is washed out ofthe well before the addition of the next reagent. The amount ofcolored product formed is directly proportional to the amount ofhormone present in the standard or unknown sample. Concentra-tions are determined using a standard curve. For simplicity, onlyone Ab 1 molecule is shown in the bottom of the well, when, infact, there is an excess of Ab 1 relative to the amount of hormoneto be measured.
FIGURE 31.8

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 12/14
578 PART IX ENDOCRINE PHYSIOLOGY
being equal to the total receptor number (R 0 ). Otherequally valid mathematical and graphic methods can beused to analyze hormone-receptor interactions, but theScatchard plot is probably the most widely used.
In practice, Scatchard plots are not always straight linesbut instead can be curvilinear (Fig. 31.9B). Insulin is a clas-sic example of a hormone that gives curved Scatchard plots.One interpretation of this result is that cells contain two
separate and distinct classes of receptors, each with a dif-ferent binding affinity. Typically, one receptor populationhas a higher affinity but is fewer in number compared to thesecond population. Therefore, as indicated in Figure 31.9B,Ka 1 Ͼ Ka 2 , but R0 2 Ͼ R01 . Computer analysis is often re-quired to fit curvilinear Scatchard plots accurately to a two-site model.
Another explanation for curvilinear Scatchard plots isthat occupied receptors influence the affinity of adjacent,unoccupied receptors by negative cooperativity . Accord-ing to this theory, when one hormone molecule binds to itsreceptor, it causes a decrease in the affinity of nearby un-occupied receptors, making it more difficult for additionalhormone molecules to bind. The greater the amount of
hormone bound, the lower the affinity of unoccupied re-ceptors. Therefore, as shown in Figure 31.9B, as bound hor-
mone increases, the affinity (slope) steadily decreases.Whether curvilinear Scatchard plots in fact result fromtwo-site receptor systems or from negative cooperativitybetween receptors is unknown.
Dose-Response Curves Are Useful in DeterminingWhether There Has Been a Change in
Responsiveness or SensitivityHormone effects are generally not all-or-none phenom-ena—that is, they generally do not switch from totally offto totally on, and then back again. Instead, target cells ex-hibit graded responses proportional to the concentration offree hormone present.
The dose-response relationship for a hormone generallyexhibits a sigmoid shape when plotted as the biological re-sponse on the y-axis versus the log of the hormone con-centration on the x-axis (Fig. 31.10). Regardless of the bio-logical pathway or process being considered, cells typicallyexhibit an intrinsic basal level of activity in the absence ofadded hormone, even well after any previous exposure tohormone. As the hormone concentration surrounding thecells increases, a minimal threshold concentration must bepresent before any measurable increase in the cellular re-sponse can be produced. At higher hormone concentra-tions, a maximal response by the target cell is produced,and no greater response can be elicited by increasing thehormone concentration. The concentration of hormone re-quired to produce a response half-way between the maxi-mal and basal responses, the median effective dose orED 50 , is a useful index of the sensitivity of the target cellfor that particular hormone (see Fig. 31.10).
For some peptide hormones, the maximal response mayoccur when only a small percentage (5 to 10%) of the totalreceptor population is occupied by hormone. The remain-ing 90 to 95% of the receptors are called spare receptors
Bound hormone
Bound hormone
Bound hormone
Free hormone
Bound hormone
Free hormone
Slope = -K a
-Ka 1
-Ka 2
X-intercept =receptornumber (R 0)
R01 R02
A
B
Scatchard plots of hormone-receptor bind-ing data. A, A straight-line plot typical of hor-
mone binding to a single class of receptors. B, A curvilinearScatchard plot typical of some hormones. Several models havebeen proposed to account for nonlinearity of Scatchard plots.(See text for details).
FIGURE 31.9 0
50
100
BasalThreshold
Log hormone concentration
ED50
B i o l o g
i c a
l r e s p o n s e
( p e r c e n
t a g e o
f m a x
i m u m
)
Maximal response
A normal dose-response curve of hormoneactivity.
FIGURE 31.10

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 13/14
because on initial inspection they do not appear necessaryto produce a maximal response. This term is unfortunate,because the receptors are not “spare” in the sense of beingunused. While at any one point in time only 5 to 10% of thereceptors may be occupied, hormone-receptor interactionsare an equilibrium process, and hormones continually dis-sociate and reassociate with their receptors. Therefore,from one point in time to the next, different subsets of the
total population of receptors may be occupied, but presum-ably all receptors participate equally in producing the bio-logical response.
Physiological or pathophysiological alterations in targettissue responses to hormones can take one of two generalforms, as indicated by changes in their dose-response curves(Fig. 31.11). Although changes in dose-response curves arenot routinely assessed in the clinical setting, they can serveto distinguish between a receptor abnormality and a postre-ceptor abnormality in hormone action, providing useful in-formation regarding the underlying cause of a particular dis-ease state. A change in responsiveness is indicated by anincrease or decrease in the maximal response of the targettissue and may be the result of one or more factors (Fig.
31.11A). Altered responsiveness can be caused by a changein the number of functional target cells in a tissue, by achange in the number of receptors per cell for the hormonein question or, if receptor function itself is not rate-limitingfor hormone action, by a change in the specific rate-limitingpostreceptor step in the hormone action pathway.
A change in sensitivity is reflected as a right or left shiftin the dose-response curve and, thus, a change in the ED 50 ;a right shift indicates decreased sensitivity and a left shiftindicates increased sensitivity for that hormone (Fig.31.11B). Changes in sensitivity reflect (1) an alteration inreceptor affinity or, if submaximal concentrations of hor-mone are present, (2) a change in receptor number. Dose-response curves may also reflect combinations of changes
in responsiveness and sensitivity in which there is both aright or left shift of the curve (a sensitivity change) and achange in maximal biological response to a lower or higherlevel (a change in responsiveness).
Cells can regulate their receptor number and/or functionin several ways. Exposing cells to an excess of hormone for a
sustained period of time typically results in a decreased num-ber of receptors for that hormone per cell. This phenomenonis referred to as down-regulation . In the case of peptide hor-mones, which have receptors on cell surfaces, a redistribution
of receptors from the cell surface to intracellular sites usuallyoccurs as part of the process of down-regulation. Therefore,there may be fewer total receptors per cell, and a smaller per-centage may be available for hormone binding on the cell sur-face. Although somewhat less prevalent than down-regula-tion, up-regulation may occur when certain conditions ortreatments cause an increase in receptor number compared tonormal. Changes in rates of receptor synthesis may also con-tribute to long-term down- or up-regulation.
In addition to changing receptor number, many targetcells can regulate receptor function. Chronic exposure ofcells to a hormone may cause the cells to become less re-sponsive to subsequent exposure to the hormone by aprocess termed desensitization . If the exposure of cells to
a hormone has a desensitizing effect on further action bythat same hormone, the effect is termed homologous de-sensitization . If the exposure of cells to one hormone hasa desensitizing effect with regard to the action of a dif-ferent hormone, the effect is termed heterologous de-sensitization .
CHAPTER 31 Endocrine Control Mechanisms 579
Log hormone concentration Log hormone concentration
B i o l o g
i c a
l r e s p o n s e
( p e r c e n
t a g e o
f m a x
i m u m
)A B
Altered target tissue responses reflected bydose-response curves. A, Decreased target
tissue responsiveness. B, Decreased target tissue sensitivity.
FIGURE 31.11

7/30/2019 Endocrine System Smch31
http://slidepdf.com/reader/full/endocrine-system-smch31 14/14
580 PART IX ENDOCRINE PHYSIOLOGY
DIRECTIONS: Each of the numbereditems or incomplete statements in thissection is followed by answers or bycompletions of the statement. Select theONE lettered answer or completion that is
BEST in each case.
1. A shift to the right in the biologicalactivity dose-response curve for ahormone with no accompanyingchange in the maximal responseindicates(A) Decreased responsiveness anddecreased sensitivity(B) Increased responsiveness(C) Decreased sensitivity(D) Increased sensitivity and decreasedresponsiveness(E) Increased sensitivity
2. Within the endocrine system,specificity of communication isdetermined by(A) The chemical nature of thehormone(B) The distance between theendocrine cell and its target cell(s)(C) The presence of specific receptorson target cells(D) Anatomical connections betweenthe endocrine and target cells
(E) The affinity of binding between thehormone and its receptor
3. The principal mineralocorticoid in thebody isAldosterone
(A) Testosterone(B) Progesterone(C) Prostaglandin E 2
(D) Cortisol4. An index of the binding affinity of a
hormone for its receptor can beobtained by examining the(A) Y-intercept of a Scatchard plot(B) Slope of a Scatchard plot(C) Maximum point on a biologicaldose-response curve(D) X-intercept of a Scatchard plot(E) The threshold point of a biologicaldose-response curve
5. Most peptide and protein hormones
are synthesized as(A) A secretagogue(B) A pleiotropic hormone(C) Proopiomelanocortin (POMC)(D) A preprohormone(E) Propressophysin
6. The primary form of cortisol in theplasma is that which is(A) Bound to albumin(B) Bound to transthyretin(C) Free in solution
(D) (D Bound to cortisol receptors(E) Bound to corticosteroid-bindingglobulin (CBG)
7. The ability of hormones to be effectiveregulators of biological function
despite circulating at very lowconcentrations results from(A) The multiplicity of their effectsTransport proteins(B) Pleiotropic effects(C) Signal amplification(D) Competitive binding
S U G G E S T E D R E A D I N G
Goodman HM. Basic Medical Endocrinol-ogy. 2nd Ed. New York: Raven, 1994.
Griffin JE, Ojeda SR, eds. Textbook of En-docrine Physiology. 4th Ed. New York:Oxford University Press, 2000.
Hedge GA, Colby HD, Goodman RL.
Clinical Endocrine Physiology.Philadelphia: WB Saunders, 1987.Norman AW, Litwack G. Hormones. 2nd
Ed. San Diego: Academic Press, 1997.Scott JD, Pawson T. Cell communication:
The inside story. Sci Am2000;282(6):72–79.
Wilson JD, Foster DW, Kronenberg HM,Larsen PR, eds. Williams Textbook ofEndocrinology. 9th Ed. Philadelphia:WB Saunders, 1998.
R E V I E W Q U E S T I O N S