-
8/4/2019 Endocrine Lymphatic and Immune Disorders
1/74
Disorders -
Endocrine/Lymphatic/Immune
Systems
Compiled by Sen.T/Sr. Navuta
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
2/74
Disorders of the Endocrine System
May be related to either anexcess or a deficiency of aspecific
hormone
May be related to a defect at itsreceptor site
Onset of an Endocrine Disordercan be either slow and insidiousor
abrupt and life-threatening
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
3/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
4/74
Laboratory Testing for Endocrine
Functioning
Radioimmunoassay: competitive bindingassay test in which
radioactively labeledamounts of hormones compete with
unlabeled hormones from plasma orserum for antibody binding
sites.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
5/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
6/74
Urine Testing: measures hormone levelsand metabolites of
specific hormones in
urine Usually done in a 24 hour urine collection
to better reflect the functioning of a gland
such as adrenal gland Certain hormones may require addition
of
additives to the collection container
No unnecessary medications should beused by client during
collection process
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
7/74
24 Hour Urine Collection
Test starts when client first arises andurinates
The first specimen is discarded but time is
noted - (first specimen is not collectedbecause it is hard to
tell how long it has beenin bladder)
Client adds all urine voided after that first
discarded specimen during next 24 hours Some hospital labs may
have it put on ice
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
8/74
Glucose Testing
Can be done via finger stick or
venous puncture
Glycosylated hemoglobin (HbA1c)value reveals the average
bloodglucose level over a period of 2-3
months
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
9/74
Radiographic Examinations Anterior, posterior and lateral skull
x-ray
studies may be used to visualize sellaturcica (an indentation of
sphenoid bonewhich houses the pituitary gland)
Erosion of this structure indicates invasionof the wall from an
abnormal growth
CT and MRI scans can show extent of
growth or location of a tumor buried withinpituitary
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
10/74
Radiographic Examinations
Size and shape of other glands andnearby structures may be
visualizedby use of a contrast media
Angiography and Venography mayreveal structural abnormalities
inblood vessels and ultrasonography of
thyroid gland can indicate whethernodules or masses are solid or
cystic
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
11/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
12/74
Pituitary Hypofunction
Caused by a deficiency of one or
more anterior pituitary hormones
Results in metabolic abnormalitiesand sexual dysfunction
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
13/74
Pituitary Hypofunction
Interventions focus on replacement ofdeficient hormones to treat
delayed
puberty
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
14/74
Testosterone therapy is initiated withhigh-dose testosterone
derivativesand continued until virilization isachieved (deepened
voice, increased
chest, facial, pubic and axillary hairgrowth)
Dose is then decreased, but therapy
continues throughout lifetime
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
15/74
Androgen therapy is avoided in men with
prostate cancer
Male fertility may be decreased and/ordepleted due to
testosterone therapy
Side effects include: gynecomastia (male breasts)
baldness
prostatic hypertrophy
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
16/74
Women may be treated with a combination of
estrogen & progesterone administered attheir menstrual
cycle
The risk for hypertension or thrombosis is
increased with estrogen therapy especiallyif the woman
smokes
Female fertility may be decreased andmedications are needed to
induce ovulation
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
17/74
Growth Hormone Deficiency changes tissue growth
patterns indirectly In children, GH deficiency leads to short
stature &
other manifestations of growth retardation
GH deficiency in adults produces no obvious
anatomic changes - does increase rate of bonedestructive
activity leading to thinner, more fragilebones
Adult clients may be treated with injections of GH,
although this treatment is rare
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
18/74
Pituitary Hyperfunction
A condition of hormone oversecretion that occurswhen client has
pituitary tumors or hyperplasias
Tumors usually arise from:
somatotropic cells (growth hormone) lactotropic cells
(prolactin)
corticotropic cells (adrenocorticotrophic hormone)
Can also be caused by hypothalmic dysfunction
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
19/74
Adenomas can develop in clients without afamily history or as
part of a syndrome knownas multiple endocrine neoplasia
Multiple endocrine neoplasia is a familialdisorder inherited as
an autosomal dominanttrait may include parathyroid and
pancreatic
tumors
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
20/74
Benign epithelial tumor, which is classified bysize, degree of
invasiveness and hormonesecreted
As it grows, it compresses brain tissue
causing neurologic symptoms, as well asendrocrine symptoms (i.e.
visual changes,headache and increased ICP)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
21/74
Prolactin secreting tumors are most commonof the Pituitary
Adenomas
Produces excessiveprolactin inhibitingsecretion of gonadal
steroids and
gonadotropins in men Men (gynecomastia due to low levels of
testosterone & muscle weakness)
Women (no production of breast milk, nomenses)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
22/74
Overproduction of Growth Hormone
Results in gigantism or acromegaly
Onset may be gradual, slow progression, andchanges may remain
unnoticed for years
before diagnosis
Early detection and treatment is essential toprevent irreverible
changes in the soft
tissues, such as those of the face, hands,feet and skin
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
23/74
Enlarged hands and feet in an adult are anindicator of growth
hormone excess
Although some changes are reversible after
treatment for overproduction of growthhormone, skeletal changes
are permanent
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
24/74
Gigantism
Onset of Growth Hormone Hypersecretionoccurs before puberty
causing rapidproportional growth in the length of all bones
Back pain and arthralgias (joint pain) may besymptoms in
response to bone changes
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
25/74
Gigantism
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
26/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
27/74
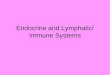
Acromegaly
Occurs after puberty and produces increasedskeletal thickness,
hypertrophy of the skinand enlargement of many visceral organs
such as liver and heart.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
28/74
Acromegaly
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
29/74
Acromegaly
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
30/74
Cushings Disease
Caused by hypersecretion of Adrenocorticotrophichormone
(ACTH)
Results in overstimulationof Adrenal Cortex
producing excessive amounts of glucocorticoids,mineralcorticoids
and androgens
Clients have alterations of nitrogen, carbohydrateand mineral
metabolism
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
31/74
Cushings Disease
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
32/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
33/74
Posterior Pituitary
Disorders of posterior pituitary are directlyrelated to a
deficiency or excess of hormoneVasopressin (antidiuretic hormone -
ADH)
Two disorders associated with ADHdeficiency or ADH excess are:
Diabetes Insipidus
Syndrome of Inappropriate Antidiuretic Hormone
(SIADH)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
34/74
Diabetes Insipidus
Two clinical manifestations/signs that alertyou to possible
endocrine disorder would be:
increased thirst
increased urination
Diabetes Insipidus is a disorder of watermetabolism caused by a
deficiencyof ADH
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
35/74
Diabetes Insipidus
Source of ADH insufficiency is caused eitherby: decrease in ADH
synthesis
inability of kidneys to respond appropriately toADH
ADH deficiency results in excretion of largevolumes of dilute
urine called polyuria
Hypernatremia is a potential problem
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
36/74
Diabetes Insipidus
Dehydration caused by massivediuresiscaused by polyuria results
in an increase inplasma osmolality causing thirst
However, if thirst mechanism is inadequate orabsent, or if
person is unable to obtain water,dehydration becomes moresevere
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
37/74
Types of Diabetes Insipidus
Nephrogenic diabetes insipidus is an inheriteddisorder where the
renal tubules do not respond tothe action of ADH.
This results in inadequatewater reabsorption by
kidney Urine output is then increased and specific gravity
is
decreased.
With effective treatment, urine output is effectively
decreased and specific gravity is increased
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
38/74
Primary Diabetes Insipidus: caused by a
defect in Hypothalmus or Pituitary Glandresulting in a lackof
ADH production orrelease
Secondary Diabetes Insipidus: resultsfrom tumors within/adjacent
to hypothalmusor pituitary gland, head trauma, infectiousprocesses,
surgical procedures or metastatic
tumors.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
39/74
Drug-related Diabetes Insipidus : causedby administration of
lithium carbonate ordemeclocycline as these drugs can
interfere with kidneys response to ADH.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
40/74
Clinical Manifestations of Diabetes
Insipidus
Loss of free water produces expectedchanges in blood and urine
tests
Initial step in diagnosis is to measure a 24
hour fluid I&O. Urine output during thisperiod must be more
than 4 liters fordiagnosis. However, it may vary from 4-30
liters in a day
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
41/74
Insipidus vs. Mellitus
Diabetes Mellitusis endocrine problemcaused by a decreased
sensitivity of insulinreceptors to presence of insulin
Diabetes Insipidusis endocrine problemcaused by an insufficiency
of AntidiureticHormone (ADH)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
42/74
Drug Therapy for Diabetes Insipidus
Client with permanent Diabetes Insipidus requireslife-long
vasopressin therapy
Client is instructed to recognize poluria and
polydipsia signals for another dose of medication All clients
taking vasopressin need to record daily
weights to identify weight gains
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
43/74
Syndrome of Inappropriate Antidiuretic
Hormone (SIADH)
Occurs when vasopressin (ADH) is secretedwhen plasma osmolarity
is low or normal
Decrease in plasma osmolarity normally
inhibits ADH production and secretion In SIADH, the feedback
mechanisms that
regulate ADH do not function properly ADHcontinues to be
released even when plasma
is hyposmolar
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
44/74
As a result of ADH secretion, water is
retained, resulting in: dilutional hyponatremia
expansion of the extracellular fluid volume
Pulmonary disorders (including Emphysema &other chronic lung
diseases) can cause SIADHeither by causing increased secretion of
ADHor ectopic synthesis of ADH.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
45/74
Adrenal Gland Hypofunction
Addisons Disease is caused by an insufficiency of
adrenocortical steroids causing problems throughloss of
mineralocorticoid (aldosterone) andglucocorticoid (cortisol)
action
Reducedaldosterone secretion causes potassium,sodium and water
imbalances:
Hyperkalemia
Hyponatremia Hypovolemia
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
46/74
Lower adrenal andogen levels result in
decreased/loss of body/axillary/pubic hair(esp. in women)
because adrenals producemost of androgrens in females
Excessive production of melanocyte-stimulating hormone increases
pigmentationof skin and causes darkening of skin
It can cause vitiligopatchy areas ofdepigmentation of skin
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
47/74
Acute Adrenal Insufficiency
Called Addisonian crisis a life-threateningevent in which
physiologic need forglucocorticoid and mineralocorticoid
hormones is greater than the available supply Usually occurs in
response to a stressful
event (surgery, trauma, severe infection)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
48/74
Hormone Replacement
Glucocorticoid and mineralocorticoiddeficiencies are completely
corrected byreplacement therapy
Drug regimen is divided into thirds 2/3given in morning and 1/3
given in lateafternoon to mimic normal adrenal hormone
secretion rhythm
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
49/74
Additional mineralocorticoid hormone may beneeded (such as
Florinef) to maintain correctelectrolyte balance (esp. Na and
Kcl)
Adjustments may be needed in hot weather
to compensate for sodium loss due toexcessive perspiration
Salt restriction or diuretic therapy should not
be started withoutconsidering whether itmight precipitate an
adrenal crisis
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
50/74
Endocrine Disorders: Thyroid,
Parathyroid and Pancreas
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
51/74
Graves Disease
(Hyperthyroidism)
Also known as Toxic Diffuse Goiter
Autoimmune disorder antibodies orimmunoglobulins are made and
attach to
thyroid stimulating hormone (TSH) receptorsites on thyroid
tissue
Thyroid gland increases in size and
overproduces thyroid hormones
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
52/74
Presentation:
Goiter (enlargement of the thyroid gland)
Exophthalmos (abnormal protrusion of the eyes
giving a wide-eyed startled look) Pretibial myxedema (dry, waxy
swelling of the
front surfaces of the lower legs)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
53/74
Graves Disease
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
54/74
Clients may have excessive tearing,
bloodshot eye appearance or have sensitivityto light.
Fine, soft, silky hair and smooth, moist skin
are common with hyperthyroidism. Emotional lability (mood
instability) is often
experienced. Client may also appear
extremely restless, irritable and fatigued.
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
55/74
Extremity muscle weakness, hyperactivedeep tendon reflexes or
tremors
Not all clients with goiter have
hyperthyroidism A hallmark assessment finding: heat
intolerance
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
56/74
Hypothyroidism
Decreased metabolism from low levels ofthyroid hormones
Can occur at any time throughout life span;
however most often occurs in womenbetween ages 30-60. Women are
affected 7-10 times more than men
Link between diabetes mellitus and
development of hypothyroidism has beenestablished
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
57/74
Most tissues and organs are affected by lowmetabolic rate
Cellular energy production is decreased and
many metabolites build up (compounds ofprotein and sugars)
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
58/74
Cellular energy is decreased and metabolites buildup inside of
cells, which increases mucous andwater, thus forming cellular edema
and changesorgan texture.
Cellular edema is called myxedema because it isNOT formed from
water alone. Nonpitting edemaforms everywhere
Myxedema coma is rare serious complication
M d
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
59/74
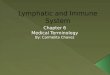
Myxedema
H h idi
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
60/74
Hypothyroidism
Client reports more time sleeping (14 -16 hrsper day)
Generalized weakness, anorexia, muscle
aches and paresthesias Constipation is common, as is cold
intolerance
Women have difficulty getting pregnant or
changes in menses; Men have problems withimpotence and
fertility
H h idi
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
61/74
Hyperparathyroidism
Primary hyperparathyroidism results when 1or more parathyroid
glands does not respondto normal feedback of serum calcium
In 80-85% of cases, cause is benign tumor in1 parathyroid
gland
H h idi
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
62/74
Hyperparathyroidism
Client may develop renal calculi (kidney stones) anddeposits of
calcium in soft tissue of kidney
Pathologic fractures, bone cysts and osteoporosis iscaused due
to increased rate of bone destruction(osteoclastia)
Anorexia, nausea, vomiting, epigastric pain,constipation and
weight loss are common when
serum calcium levels are high
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
63/74
Peptic ulcer disease can result from elevatedserum gastrin
levels (hypergastrinemia)caused by hypercalcemia.
Fatigue and lethargy may be present and willbecome more severe
as calcium levels rise
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
64/74
Disorders of the Lymphatic System
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
65/74
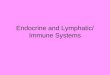
El h ti i
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
66/74
Elephantiasis
Immune System Disorders
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
67/74
Immune System Disorders
Hypersensitivity
Autoimmune Disease
Immunodeficiency Diseases
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
68/74
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
69/74
Type II (antibody-dependant cytotoxic)- as intransfusion
reaction.
Type III (immune complex)- large antibody-antigen complexes that
get trapped under the tunic
interna of blood vessels and cause inflammation. Type IV
(delayed)- occur 12 to 72 hours after
exposure. Delay commonly associated with traveltime to lymph
nodes. Cosmetics and poison ivy
hapten commonly do this.
Autoimmune Diseases
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
70/74
Autoimmune Diseases
Failure of the immune system to distinguish self fromforeign
antigens.
Immune systems produces antibodies against bodies
own tissues.
Causes:
- Cross reactivity fight against a foreign antigenleds to
antibodies that attack self.
- Abnormal exposure to self-antigens in the blood
- Changes in the structure of self-antigens
Immunodeficiency Diseases
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
71/74
Immunodeficiency Diseases
SCID Severe combined immunodeficiency disease
- congenital deficiency of both T and B cells.
- susceptible to opportunistic infections.
- Bubble babies
AIDS Acquired
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
72/74
AIDS AcquiredImmunodeficiency diseases
Acquired after birth, likeHIV.
HIV targets helper T cells Without these cells, all 3
immune responses arehampered.
Most patients with AIDS
die of opportunisiticinfections.
HIV virus
T torial Q estions
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
73/74
Tutorial Questions
Discuss the following conditions
- Diabetes Mellitus
- Goiter
- Cushings Syndrome
- Pancreatitis
- HIV/AIDS
- Systemic Lupus Erythmatosus
-
8/4/2019 Endocrine Lymphatic and Immune Disorders
74/74
The End