-
7/30/2019 Endocrine Disorders in Children
1/92
NURSINGTHERAPEUTICSFORCHILDRENANDADOLESCENT
II
Prepared by: Sarah Jane L. Racal RN,MAN
Christian University of Thailand
-
7/30/2019 Endocrine Disorders in Children
2/92
Love your callingwith passion; it is the
meaning of yourlife- Sir Pagsi
-
7/30/2019 Endocrine Disorders in Children
3/92
THE ENDOCRINE SYSTEM
Controls orregulatesmetabolic processes,
governing energyproduction, growth, fluid
and electrolyte balance,response to stress, and
sexual reproduction.
-
7/30/2019 Endocrine Disorders in Children
4/92
THE ENDOCRINESYSTEM
Hormones
Cells
Target organ
Environment ( blood, lymph,
extracellular fluids
http://localhost/var/www/apps/conversion/tmp/scratch_1/The%20Endocrine%20System.mp4
-
7/30/2019 Endocrine Disorders in Children
5/92
GLANDSOFTHEENDOCRINESYSTEM
-
7/30/2019 Endocrine Disorders in Children
6/92
-
7/30/2019 Endocrine Disorders in Children
7/92
-
7/30/2019 Endocrine Disorders in Children
8/92
-
7/30/2019 Endocrine Disorders in Children
9/92
DISORDERSOF PITUITARYFUNCTION
Hypopituitarism
Pituitary Hyperfunction
Precocious PubertyDiabetes Insipidus
Syndrome of InappropriateAntidiuretic Hormone
( SIADH)
-
7/30/2019 Endocrine Disorders in Children
10/92
HYPOPITUITARISM
Is diminished or deficient secretion of pituitaryhormones.
Growth hormone (GH)Short stature
Delayed epiphyseal closure
Retarded bone age
Premature aging
Increased insulin sensitivity
Thyroid Stimulating Hormone ( TSH )Short stature with infantile
proportions
Dry, coarse skin, yellow discoloration, pallorCold
Intolerance
Constipation
Somnolence
Bradycardia
Dyspnea on exertionDelayed dentition, loss of teeth
-
7/30/2019 Endocrine Disorders in Children
11/92
HYPOPITUITARISM : MANIFESTATIONS
Gonadotropins
Absence of sexualmaturation/loss of secondarysex
characteristics
Atrophy of genitalia, prostate
gland, breastsAmenorrhea withoutmenopausal symptoms
Decreased spermatogenesis
Adrenocorticotropic Hormone( ACTH)
Severe anorexia, weight lossHypoglycemia
Hypotension
Hyponatremia, Hypokalemia
Anidiuretic Hormone( ADH )Polyuria
Polydipsia
Dehydration
Melanocyte-Stimulating Hormone
( MSH )Decreased
pigmentation
-
7/30/2019 Endocrine Disorders in Children
12/92
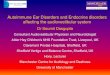
HYPOPITUITARISM : CAUSES
Media file 1: The left photograph shows an untreated
21-month-old girl with congenital hypopituitarism. The right panel
depicts thesame child aged 29 months, following 8 months of
growth
hormone therapy.
Aplasia or HypoplasiaIdiopathicTraumaSurgeryAnorexia
NervosaAutoimmuneHypophysisIrradiation
-
7/30/2019 Endocrine Disorders in Children
13/92
HYPOPITUITARISM: MANAGEMENT
Hormone replacement and Surgical Intervention
Medications:
Somatropin
LevothyroxineHydrocortisoneVasopressinDesmopressin
Androgen
-
7/30/2019 Endocrine Disorders in Children
14/92
PITUITARY HYPERFUNCTION
Gigantism ( Before epiphyseal closure)
Acromegaly ( After epiphyseal closure)
Facial features (overgrowthhead, lips, nose,tongue,
jaw,increased facialhair), increasedtendency towardDM
Elevated growthhormone
Causes:Congenital Adrenal
HyperplasiaAdenoma/Carcinoma
Glucocorticoid resistance
Idiopathic
Trauma
Post- Inflammation
-
7/30/2019 Endocrine Disorders in Children
15/92
TREATMENT
Treatment is directed toward the specific causeof the
disorder.
Injection of a specific analog of
Luteinizing Hormone ( regulates
Pituitary secretion)
Leuprolide acetate given 0.2-0.3mg/kg
Psychological Management
-
7/30/2019 Endocrine Disorders in Children
16/92
DIABETES INSIPIDUS ( POSTERIOR PITUITARY
HYPOFUNCTION )
also known as Neurogenic Diabetes Insipidus
Familial
IdiopathicTraumaInfectionAlcoholPhenytoin
DecreasedADH/Vasopressin/Pitressin
UncontrolledDiuresis
PolyuiriaPolydipsia
First sign :Enuresis
-
7/30/2019 Endocrine Disorders in Children
17/92
DIABETES INSIPIDUS
Infants IrritabilityFeeding withWater and NotMilk
ALERT! For dehydration, electrolyteimbalance, elevated
temperature,azotemia, potential circulatorycollapse
ALERT! Encourage patient to drink more liquids toprevent
electrolyte imbalance ( special precaution tothose with
trauma/under anesthesia)
-
7/30/2019 Endocrine Disorders in Children
18/92
TREATMENT
Hormone replacement
Overdosage effect: SIADH symptoms
IM/SC vasopressin Tannate ( 48-72 hours
)Nasal Spray of aqueous lysinevasopressin ( every 8-12
hours)
-
7/30/2019 Endocrine Disorders in Children
19/92
NURSING CARE MANAGEMENT
Assess
Body weightSerumElectrolyteBlood
UreaNitrogenHematocritUrineSpecific
GravityIntake andOutput
Health Education
Wear medical alertbracelet
-
7/30/2019 Endocrine Disorders in Children
20/92
SIADH ( SYNDROMEOFINAPPROPRIATE
ANTIDIURETICHORMONE )
Increased ADH Fluid retentionHypotoniciy
Low serumOsmolalityHigh urineosmolality
Anorexia,Nausea,
Stomach cramps
Irritability
Personality
changes
StuporConvulsions
Immediate Management:
RESTRICT FLUIDS ( -1/2 maintenance)
-
7/30/2019 Endocrine Disorders in Children
21/92
NURSING CARE MANAGEMENT
Monitor Intake and Output
Seizure precautions
Long term ADH antagonizingmedication
Observe for signs and symptoms offluid overload
Weight
Health education
-
7/30/2019 Endocrine Disorders in Children
22/92
THYROID DISORDERS
ThyroidHormone
T4 (Throxine)
T3 ( Triiodothyronine )
Calcitonin Regulates calcium levelsby decreasing
itsconcentration PTH
Controls Basal MetabolicRate
-
7/30/2019 Endocrine Disorders in Children
23/92
-
7/30/2019 Endocrine Disorders in Children
24/92
JUVENILE HYPOTHYROIDISM
CongenitalHypoplastic
Thyroid Radiotherapy
Infection
Low dietary
intake of iodine
Decreasedcirculatorythyroidhormones
Poor growthConstipationSleepiness
Mental declineMyxedematousskin ( dry skin,puffiness, sparse
hair)
-
7/30/2019 Endocrine Disorders in Children
25/92
HYPOTHYROIDISM
-
7/30/2019 Endocrine Disorders in Children
26/92
TREATMENT
Thyroid Hormone Replacement
Increasing amounts of Levothyroxine ( 4-8weeks )
Nursing Care Management
Early recognition of disorderHealth EducationEncourage
compliance to therapy
-
7/30/2019 Endocrine Disorders in Children
27/92
GOITER Enlargement or Hypertrophy of the
Thyroid gland
Can occur in deficient, excessive and normalTH secretion
DecreasecirculatingTH
Increasedsecretion ofPituitaryTSH
Enlargementof Thyroid
Low dietaryintake ofIodine
ALERT! If an infant is bornwith goiter, prepare foremergency
ventilation.Hyperextension of neckcan improve ventilation.
-
7/30/2019 Endocrine Disorders in Children
28/92
LYMPHOCYTIC THYROIDITIS
Hashimoto disease/ Juvenile Autoimmune
Thyroiditis
- Most common cause of thyroid disease inchildren. Accounts for
the largest percentage in
juvenile hypothyroidism
- After age 6
Strong geneticpredisposition
Lymphocyticinfiltration of thegland
Symmetricallyenlarged gland
-
7/30/2019 Endocrine Disorders in Children
29/92
TREATMENT
Oral Replacement of Thyroid Hormone
Surgery is NOT RECOMMENDED
Nursing Care Management
Reasure the child that the condition is
temporary
Compliance to thyroid therapyHealth education
-
7/30/2019 Endocrine Disorders in Children
30/92
HYPERTHYROIDISMGraves Disease
Autoimmune response
to TSH receptors; no
specific etiologyidentified
Clinical Manifestations:
irritability, hyperactivity, short attention span,tremors,
insomnia and emotional lability, warm, flushedand moist skin; hair
is fine and unable to hold a wave;exophthalmos; increased blinking;
absence of wrinklesin the forehead;visual disturbances.
-
7/30/2019 Endocrine Disorders in Children
31/92
TREATMENT
DRUG THERAPY
(PTU: propylthiouracil and Methimazole)
THYROIDECTOMY
(subtotal thyroidectomy)
RADIATION THERAPY
(ablation with radioiodine)
-
7/30/2019 Endocrine Disorders in Children
32/92
TREATMENT
Drug therapy:
Most serious side-effect:
Agranulocytosis ( severe leukopenia )
Thyroidectomy complications:
- Possible incidence of hypothyroidism
- Laryngeal nerve palsy
- Permanent hypothyroidism
-
7/30/2019 Endocrine Disorders in Children
33/92
THYROTOXICOSIS
Occur from sudden release of
hormones-LIFE
THREATENING!
THYROID STORM:
Clinical Manifestations:
severe irritability,hyperthermia,hypertension,
severe tachycardia, prostration
-
7/30/2019 Endocrine Disorders in Children
34/92
NURSING CARE MANAGEMENT
Early Identification
Children: Need quiet, unstimulating
environment conducive to rest.
ALERT : children taking propylthiouracil ormethimazole must be
monitored for side-
effects: Sore throat + Fever ( leukopenia)=
early detection is important. See a doctor
immediately.
-
7/30/2019 Endocrine Disorders in Children
35/92
SURGICAL CARE
Iodine ( given few weeks before
surgery)=unpalatable.
Mix with a strong tasting fruit juice (grape/punch
flavors) Use straw
Compliance is essential to avoid thyroid crisis.
Psychological preparation
Health education
Assess for bleeding ( damage to laryngeal
nerves: severe stridor, hoarseness )
-
7/30/2019 Endocrine Disorders in Children
36/92
LARYNGOSPASM
Can occur and is life-threatening.
Characterized by stridor, hoarseness and feeling of
tightness in the throat.
Tracheostomy set
Observe for signs of hypothyroidism and
hypocalcemia especially in the immediate post
operation period.
-
7/30/2019 Endocrine Disorders in Children
37/92
PARATHYROID DISORDERS
Function: Homeostasis inserum calcium
Parathyroid gland ParathyroidHormone +
Vitamin D +Calcium
PTH
Increases serumcalciumBone
demineralization
CalcitoninDecreases serumcalciumBone formation
-
7/30/2019 Endocrine Disorders in Children
38/92
HYPOPARATHYROIDISM: DEFICIENT PTH
Deficient in the
synthesis or cellular
processing of PTH
Aplasia/Hypoplasia of
the gland
CongenitalHypothyroidism
Postthyroidectomy Hypoparathyroidism
Decreased Calcium
Clinical Manifestations: Numbness, tingling inhands and feet, +
Chvostekssign,+trousseaus sign, larygospasm.Convulsion may
occur.
-
7/30/2019 Endocrine Disorders in Children
39/92
HYPOPARATHYROIDISM
Treatment goal:
Maintain normal serum calcium and phosphoruslevels with minimal
complications.
Acute/sever tetany: IV/PO Calcium gluconate
Vitamin D- prolonged onset; long half life
Long term management- massive doses ofvitamin D; Oral calcium
supplementation
-
7/30/2019 Endocrine Disorders in Children
40/92
NURSINGCAREMANAGEMENT
Recognition of Hypocalcemia
convulsions, irritability, GI symptoms,
seizures
Establish seizure and safety
precautions and reduce environmental
stimuli.
Observe for signs of larygospasm
Always prepare calcium gluconate for
emergency.
-
7/30/2019 Endocrine Disorders in Children
41/92
HYPERPARATHYROIDISM
A rare condition in children
Primary:
Glandadenoma
Hyperparathyroidism
Nausea, vomiting,abdominal
discomfort, vaguebone pain, polyuria,polydipsia
Secondary:Chronic renal disease; Renal osteodystrophy;
congenital anomalies of urinary tract;
hypercalcemia
-
7/30/2019 Endocrine Disorders in Children
42/92
TREATMENT: DEPENDINGONTHECAUSE
Primary :
Surgical removal of tumors or
hyperplasic tissue
Secondary:Calcium and Vitamin D
-
7/30/2019 Endocrine Disorders in Children
43/92
NURSING CARE MANAGEMENT
1. Early recognition of the disorder
2. Assess complications : Bone pain/fracture
3. Assess for unexplained GI symptoms and
cardiac irregularities4. Hydration to minimize renal calculi
formation
5. Take fruit juices to decrease urinary PH (cranberry or apple
juice
-
7/30/2019 Endocrine Disorders in Children
44/92
NURSING CARE MANAGEMENT
6. Strain urine
7. Keep side rails in place and assist inambulation.
8. Take vital signs and pulse for one full minute
( report bradycardia and cardiac arrest ) 9. Health education re
diet ( Calcium and
Vitamin D )
10. Surgery may lead to hypocalcemia ( observe
for signs of tetany, instituting seizureprecautions.
Have calcium gluconate ready for emergency
-
7/30/2019 Endocrine Disorders in Children
45/92
ADRENAL GLAND
Adrenal Medulla :
catecholamines ( Epinephrine and
Norepinephrine
Adrenal Cortex :Steroids
Glucocorticoid ( cortisol, corrtisone)
Mineralocorticoid ( aldosterone )Sex steroids ( androgen,
estorgen,and progestine )
-
7/30/2019 Endocrine Disorders in Children
46/92
MINERALOCORTICOID
Aldos
teron
e Sodium and water retention
and Potassium excretion
Renin-angiotensionAldosterone system
-
7/30/2019 Endocrine Disorders in Children
47/92
RENIN-ANGIOTENSIN-ALDOSTERONE
SYSTEM
C
-
7/30/2019 Endocrine Disorders in Children
48/92
ADRENALMEDULLA
Catecholam
ines
ActivityVasoconstriction
RespirationBronchialdilation
Heightened
sensory awarenessPupillary dilation
Metabolic rate
-
7/30/2019 Endocrine Disorders in Children
49/92
ACUTEADRENOCORTICALINSUFFICIENCY
AD
RENALC
RISIS
Hemorrhage intothe gland fromtrauma( prolonged difficult
labor, fulminatinginfectionsmeningococcemia
,abrupt
withdrawal of
cortisone)
AAIIncreasedIrritabilityHeadache
Diffuseabdominalweakness,nausea,
vomiting,diarrhea
-
7/30/2019 Endocrine Disorders in Children
50/92
TREATMENT
Cortical Replacement
Replace body fluids
Administer glucose solution
Antibiotic if with infection
-
7/30/2019 Endocrine Disorders in Children
51/92
NURSINGCAREMANAGEMENT
Prompt recognition is essential
VS and BP every 15 minutes ( hyperpyrexia;shocklike state)
MIOMonitor response to treatment
Rapid administration of fluids : heart failure
High dosage of cortisol: sudden fall in blood
pressure and temperature.
Increased sodium and cortisol tx: decreasedpotassium---flaccif
paralysis
-
7/30/2019 Endocrine Disorders in Children
52/92
ALERT!
Monitor electrolyte level especially a
decrease or increase in potassium (
weakness, poor muscle control,
paralysis,cardiac dysrhythmias, apnea
Intravenous or oral Potassium- mixed with fruit
juice
-
7/30/2019 Endocrine Disorders in Children
53/92
CHRONIC ADRENOCORTICAL
INSUFFICIENCY ADDISONS DISEASE
Rare in children
Generalized TB
Destructivelesion inAdrenal glandNeoplasm
Idiopathic
Adrenal Gland
Destruction
-
7/30/2019 Endocrine Disorders in Children
54/92
TREATMENT
Glucocorticoid replacement
1. mineralocorticoid=== liberal salt intake
BUT:
Fever, infection, emotional upset, surgery= triple
dose ( if not, may lead to ACUTE CRISIS
Monthly injections of desoxycorticosterone
Implantation of desoxycorticosterone acetatepellets SC every 12
months.
-
7/30/2019 Endocrine Disorders in Children
55/92
NURSINGCAREMANAGEMENT
Health education- continued need for
cortisol replacement
Drug side-effect:
Gastric Irritation ( ingest food or use
antacid )
Increased excitability and sleeplessness
May require dietary management toprevent obesity.
-
7/30/2019 Endocrine Disorders in Children
56/92
ALERT!
Taste different preparations of
cortisone. Smaller volume of liquid to
ingest is also the most bitter.
Side Effects of Mineralocorticoidgeneralized edema ( eyes,
headache.
Cardiac arrhythmias, signs andsymptoms of decreased
potassium)
-
7/30/2019 Endocrine Disorders in Children
57/92
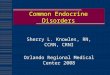
CUSHING SYNDROME
Excessivec
irculatingfreecortiso
l
AdrenalHyperplasiaAdrenocorticalneoplasmExtra
pituitaryneoplasmsAdministration oflarge amounts
ofexogenouscorticosterone
Glucocorticoid/cortisol
Poor wound healingExcessive hair growthMoon faceBuffalo hump
Pundulum abdomenEcchymosisRed abdominal StriaeBruisesWeight
gain
-
7/30/2019 Endocrine Disorders in Children
58/92
CUSHING SYNDROME
-
7/30/2019 Endocrine Disorders in Children
59/92
TREATMENT
Depending on the case
Surgery:
Bilateral Adrenalectomy (post-op replacement of cortical
hormones)
-
7/30/2019 Endocrine Disorders in Children
60/92
NURSING CARE MANAGEMENT
Depending on the cause
To decrease cushingoid features = give
during early am to maintain normal
diurnal pattern of cortisol secretion.
= at night: decrease level of cortisol (
more pronounced effect if withincreased supply of
medication)
-
7/30/2019 Endocrine Disorders in Children
61/92
ALERT!
Post operation complications ofadrenalectomy
( sudden withdrawal of cortisol)
Observe for shock-like
symptoms ( hypotension,
hyperglycemia )
-
7/30/2019 Endocrine Disorders in Children
62/92
CONGENITALADRENALHYPERPLASIA
Family of disorders caused by a decreased
enzyme activity required for cortisol
production in the adrenal cortex.
21-hydroxylase deficiency :most common defect ( 90% of all
cases of CAH)
1/12000-15000 births
Causes over production of the adrenal
androgen = virilization of female fetus
-
7/30/2019 Endocrine Disorders in Children
63/92
CONGENITAL ADRENAL HYPERPLASIA
Interference in thebiosynthesis of cortisolduring fetal life
Increased production of ACTH
Hyperplasia of
adrenal gland
-
7/30/2019 Endocrine Disorders in Children
64/92
SIGNSANDSYMPTOMS
Girls will usually have normal female reproductiveorgans
(ovaries, uterus, and fallopian tubes).They may also have the
following changes:
Abnormal menstrual periods
Deep voiceEarly appearance of pubic and armpit hair
Excessive hair growth and facial hair
Failure to menstruate
Genitals that look both male and female(ambiguous genitalia),
often appearing moremale than femal
http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003263&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003148&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003149&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003149&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003148&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=003263&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1
-
7/30/2019 Endocrine Disorders in Children
65/92
SIGNSAND SYMPTOMS
Boys won't have any obvious problems at birth.However, they may
appear to enter puberty as early
as 2 - 3 years of age. Changes may include:
Deep voice
Early appearance of pubic and armpit hair
Early development of male characteristics
Enlarged penis
Small testes Well-developed muscles
http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=002334&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=002334&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1
-
7/30/2019 Endocrine Disorders in Children
66/92
SIGNS AND SYMPTOMS
Both boys and girls will be tall as children but much
shorter than normal as adults.
Some forms of congenital adrenal hyperplasia are
more severe and cause adrenal crisis in thenewborn due to a loss
of salt. Newborns with these
forms develop severe symptoms shortly after birth,
including:
Cardiac arrhythmias
Dehydration
Electrolyte changes
Vomiting
http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=000357&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=001101&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=000982&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=002350&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=002350&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=000982&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=001101&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1http://www.whcenter.org/BOdy.CFM?xyzpdqabc=0&id=555586&action=detail&AEArticleID=000357&AEProductID=Adam2004_117&AEProjectTypeIDURL=APT_1
-
7/30/2019 Endocrine Disorders in Children
67/92
TREATMENT
Protecting normal growth
Androgen blockade (sprinolactone)
Inhibition of estrogen synthesis ( testosterone )
GH therapy Lupon therapy
Cortisol replacement choices
Dexamethasone day at low dosage
Laboratory assessments of control
Androstenedione emphasis in adolescent females
-
7/30/2019 Endocrine Disorders in Children
68/92
-
7/30/2019 Endocrine Disorders in Children
69/92
PHEOCHROMOCYTOMA
Pheochromocytomas are a type oftumorof the adrenal glands
that
can release high levels of
epinephrine and norepinephrine
W
http://www.medicinenet.com/script/main/art.asp?articlekey=118966http://www.medicinenet.com/script/main/art.asp?articlekey=3286http://www.medicinenet.com/script/main/art.asp?articlekey=3286http://www.medicinenet.com/script/main/art.asp?articlekey=118966
-
7/30/2019 Endocrine Disorders in Children
70/92
WHATARESYMPTOMSOF
PHEOCHROMOCYTOMA?
Classic symptoms
SweatingPalpitations
Headache
O
-
7/30/2019 Endocrine Disorders in Children
71/92
OTHERCONDITIONSTHATMAYACCOMPANY
THECLASSICSYMPTOMSARE:
Anxiety
Nausea
TremorsWeakness
Abdominal
painWeight loss
-
7/30/2019 Endocrine Disorders in Children
72/92
TREATMENT
Surgery is the definitive treatment until
the tumor is removed.
Top Priority!!!! Control BloodPressure
In rare cases, rediationtherapy or
chemotherapy may berequired after surgery
-
7/30/2019 Endocrine Disorders in Children
73/92
DIABETES MELLITUS
Diabetes is an autoimmune disorder that occursin children that
have a certain geneticpredisposition. It is not yet known what
triggersor causes the autoimmune reaction to occur in
these kids
At about 6-7 years old:Type I Insulin Dependent DiabetesMellitus
( more common in children )
-
7/30/2019 Endocrine Disorders in Children
74/92
MAIN SYMPTOMS
Polyuria
Polydipsia
Polyphagia
Weight loss
-
7/30/2019 Endocrine Disorders in Children
75/92
TYPE IAND TYPE II DIABETES MELLITUS
Completely unable to
produce insulin
Autoimmune disease ofinsulin-producing beta
cells of the pancreas.
Almost 10% of diabeticchildren
More common in adults Usually overweight
May have acanthosisnigricans
Produce insulin butcells dont respond toit.
Type I IDDM Type II NIDDM
POPULATION AT RISK OF DEVELOPING TYPE II
-
7/30/2019 Endocrine Disorders in Children
76/92
POPULATIONATRISKOFDEVELOPING TYPE II
DIABETES MELLITUS
people who are overweight or obese (more than 20 percentabove
their ideal body weight)
people who have a parent or sibling with type 2 diabetes
thosewho belong to a high-risk ethnic population
(African-American,Native American, Asian-American, Hispanic, or
PacificIslander)
people who live a sedentary lifestyle (i.e., exercise less
thanthree times a week) women who have been diagnosed
withgestational diabetes or have delivered a baby weighing morethan
9 lbs (4 kg)
people with high blood pressure (140/90 mmHg or above)
people with high density lipoprotein cholesterol (HDL, or
"good"cholesterol) level less than or equal to 35 mg/dl and/or
atriglyceride level greater than or equal to 250 mg/dl
-
7/30/2019 Endocrine Disorders in Children
77/92
MANAGEMENT
When to call a doctor?
Any child displaying
symptoms of diabetesshould be taken to a doctoror emergency care
facilityfor evaluation immediately.
-
7/30/2019 Endocrine Disorders in Children
78/92
MANAGEMENT
Diagnosis
Suspected based on symptoms
and confirmed by blood tests
that measure the level of
glucose in blood plasma
-
7/30/2019 Endocrine Disorders in Children
79/92
BLOOD TESTS
Fasting Plasma Glucose Test
Random Plasma Glucose Test
Oral Glucose Tolerance Test
-
7/30/2019 Endocrine Disorders in Children
80/92
FASTINGPLASMAGLUCOSETEST
Blood is drawn from a vein in the child's armfollowing an
eight-hour fast (i.e., no food ordrink), usually in the morning
beforebreakfast. The red blood cells are separated
from the sample and the amount of glucoseis measured in the
remaining plasma. Afasting plasma glucose level of 126 mg/dl(7.0
mmol/l) or higher indicates diabetes
(with a confirming retest on a subsequentday).
-
7/30/2019 Endocrine Disorders in Children
81/92
RANDOMPLASMAGLUCOSETEST
Blood is drawn at any time ofday, regardless of whether
thepatient has eaten. A random
plasma glucose concentrationof 200 mg/dl (11.1 mmol/l) orhigher
in the presence of
symptoms indicates diabetes.
-
7/30/2019 Endocrine Disorders in Children
82/92
ORALGLUCOSETOLERANCETEST
Blood samples are taken both beforeand several times after a
patient drinks75 grams of a glucose-based
beverage. If plasma glucose levelstaken two hours after the
glucosedrink is consumed are 200 mg/dl (11.1
mmol/L) or higher, the test isdiagnostic of diabetes (and should
beconfirmed on a subsequent day ifpossible).
-
7/30/2019 Endocrine Disorders in Children
83/92
MANAGEMENTOFDIABETESMELLITUS
Medication
D
iet
Exercise
-
7/30/2019 Endocrine Disorders in Children
84/92
TREATMENT
Type I Diabetes insulin injections orinfusions
operate a home blood
glucose monitor
Insulin height, weight, age, food intake, and activitylevel
given subcutaneously
upper arm, abdomen, or upperthigh.
-
7/30/2019 Endocrine Disorders in Children
85/92
INSULIN
Insulin Onset ofaction
Peak ofaction/Duration
Regular Insulin 15 to 30minutes
Two hours ( 4-6hrs)
Intermediate Acting Insulin( NPH and Lente)
1 to 3 hours 18 to 26 hours
Ultra-lente 4 to 8 hours 28 to 36 hours
Basal action insulin (peakless insulin)glargine orLantus
15 minutes Duration : 18-26hours
-
7/30/2019 Endocrine Disorders in Children
86/92
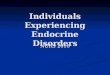
INSULININJECTIONSITE
-
7/30/2019 Endocrine Disorders in Children
87/92
ADMINISTRATIONOFINSULIN
-
7/30/2019 Endocrine Disorders in Children
88/92
INSULINANDINSULINSYRINGE
-
7/30/2019 Endocrine Disorders in Children
89/92
NUTRITIONAL CONCERNS
10 to 20 % ofcalories from
protein
50 to 60 % ofcalories fromcarbohydrates
Less than 30% ofcalories from fats
-
7/30/2019 Endocrine Disorders in Children
90/92
ORAL MEDICATIONS
Metformin (Glucophage)
Only medication approved by
the U.S. FDA for use inchildren over age ten
Works by reducing the amount ofglucose the liver produces and
theamount of circulating insulin in thebody.
-
7/30/2019 Endocrine Disorders in Children
91/92
METFORMIN
-
7/30/2019 Endocrine Disorders in Children
92/92
"WHATEVERTHEMINDOFMANCANCONCEIVEANDBELIEVE,
ITCANACHIEVE."NAPOLEON
HILL
Have a healthy dayahead of all of you!
http://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htmhttp://www.famous-inspirational-quotes.com/famous_people_quotes/napoleon_hill_quotes.htm