Embed Size (px)
Citation preview
ACUTEABDOMEN
1emss17.sats-kbh.dk
EMSS17:AcuteAbdomencoursematerialIntroductionDuringtheacuteabdomenworkshopattheEmergencyMedicineSummerSchool2017(EMSS17)youwilllearnhowtoassessandtreatpatientspresentingwithacuteabdomen(abdominalpain).There'saninexhaustiblenumberofreasonswhypatientspresentwithacuteabdomen.In35%ofthecaseswewillneverfindthereasonforthesymptoms.Becauseofthegreatamountofdiagnoses,wewillgiveyousometoolstodiagnosethepatientwithacuteabdomen.Anoverviewofthemostcommonandmostdangerousreasonsforacuteabdomenisgivenintheendofthisdocument.Mostdiagnosescausingacuteabdomencanleadtolife-threateningdiseasesifleftuntreated.Perforationswillleadtocontaminationoftheabdomencausingsepsis,multi-organfailureanddeath.Severeabdominalbleedingcanlikewiseleadtodeathinashorttime.
AssessmentofthepatientwithacuteabdomenPatientspresentingwithacuteabdomenshouldbeinitiallyassessedusingtheABCDEassessmentapproach.InthismaterialwewillnotgointodetailswiththeABCDEassessment,butrefertothecoursematerial'ABCDEWorkshop'thatyou'llfindonhttp://emss17.sats-kbh.dk/course-materials.Howyouexaminetheabdomenisdescribedinthevideothatyou'llfindintheonlinecoursematerialsforthe'AcuteAbdomenWorkshop'.Inwomenwithacuteabdomenremembertoconsidergynaecologicconditions.Ingeneral,whenawomanpresentswithacuteabdomenaurineorplasmahCGshouldbemeasured(toassessifthepatientispregnant)andagynaecologicalexaminationshouldbeconsidered.
ACUTEABDOMEN
2emss17.sats-kbh.dk
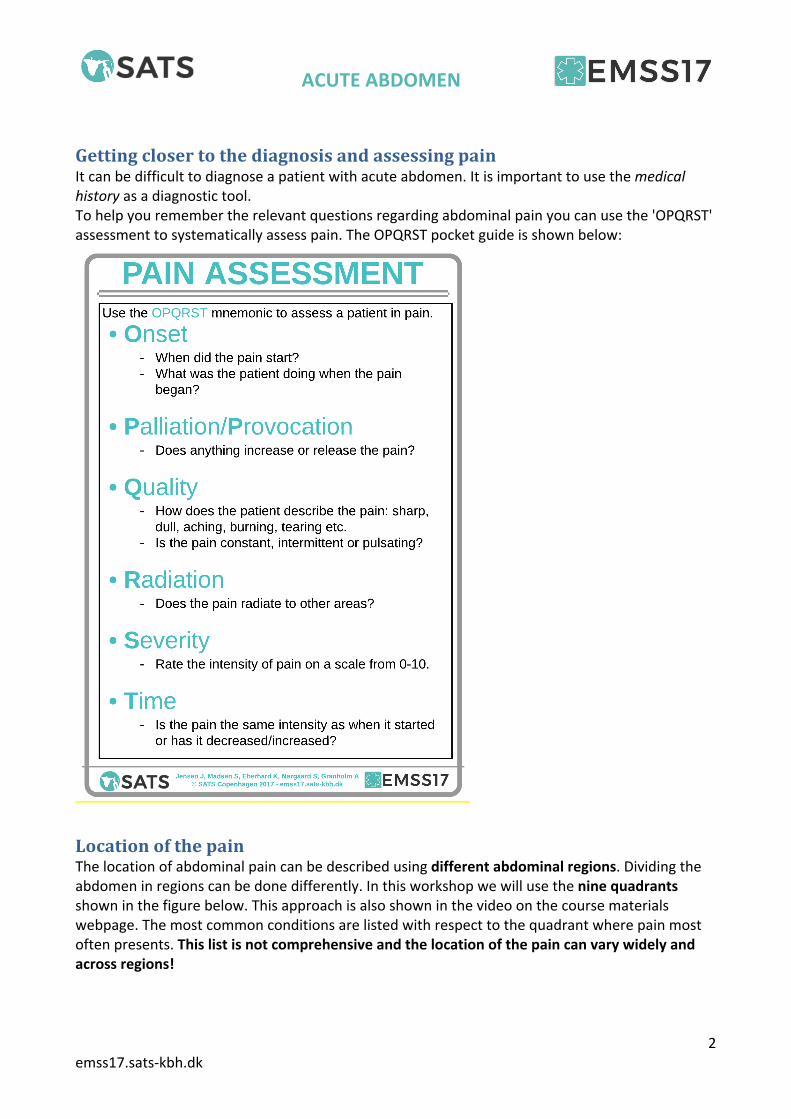
GettingclosertothediagnosisandassessingpainItcanbedifficulttodiagnoseapatientwithacuteabdomen.Itisimportanttousethemedicalhistoryasadiagnostictool.Tohelpyouremembertherelevantquestionsregardingabdominalpainyoucanusethe'OPQRST'assessmenttosystematicallyassesspain.TheOPQRSTpocketguideisshownbelow:
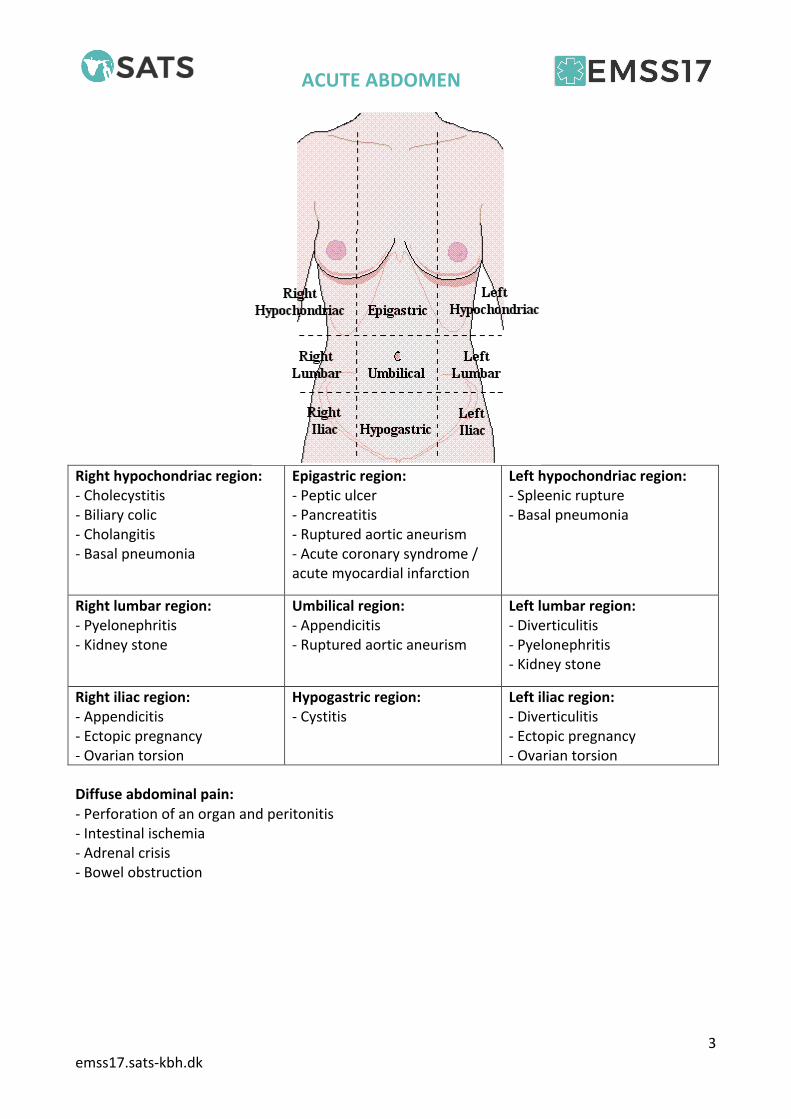
LocationofthepainThelocationofabdominalpaincanbedescribedusingdifferentabdominalregions.Dividingtheabdomeninregionscanbedonedifferently.Inthisworkshopwewillusetheninequadrantsshowninthefigurebelow.Thisapproachisalsoshowninthevideoonthecoursematerialswebpage.Themostcommonconditionsarelistedwithrespecttothequadrantwherepainmostoftenpresents.Thislistisnotcomprehensiveandthelocationofthepaincanvarywidelyandacrossregions!
ACUTEABDOMEN
3emss17.sats-kbh.dk
Righthypochondriacregion:-Cholecystitis-Biliarycolic-Cholangitis-Basalpneumonia
Epigastricregion:-Pepticulcer-Pancreatitis-Rupturedaorticaneurism-Acutecoronarysyndrome/acutemyocardialinfarction
Lefthypochondriacregion:-Spleenicrupture-Basalpneumonia
Rightlumbarregion:-Pyelonephritis-Kidneystone
Umbilicalregion:-Appendicitis-Rupturedaorticaneurism
Leftlumbarregion:-Diverticulitis-Pyelonephritis-Kidneystone
Rightiliacregion:-Appendicitis-Ectopicpregnancy-Ovariantorsion
Hypogastricregion:-Cystitis
Leftiliacregion:-Diverticulitis-Ectopicpregnancy-Ovariantorsion
Diffuseabdominalpain:-Perforationofanorganandperitonitis-Intestinalischemia-Adrenalcrisis-Bowelobstruction
ACUTEABDOMEN
4emss17.sats-kbh.dk
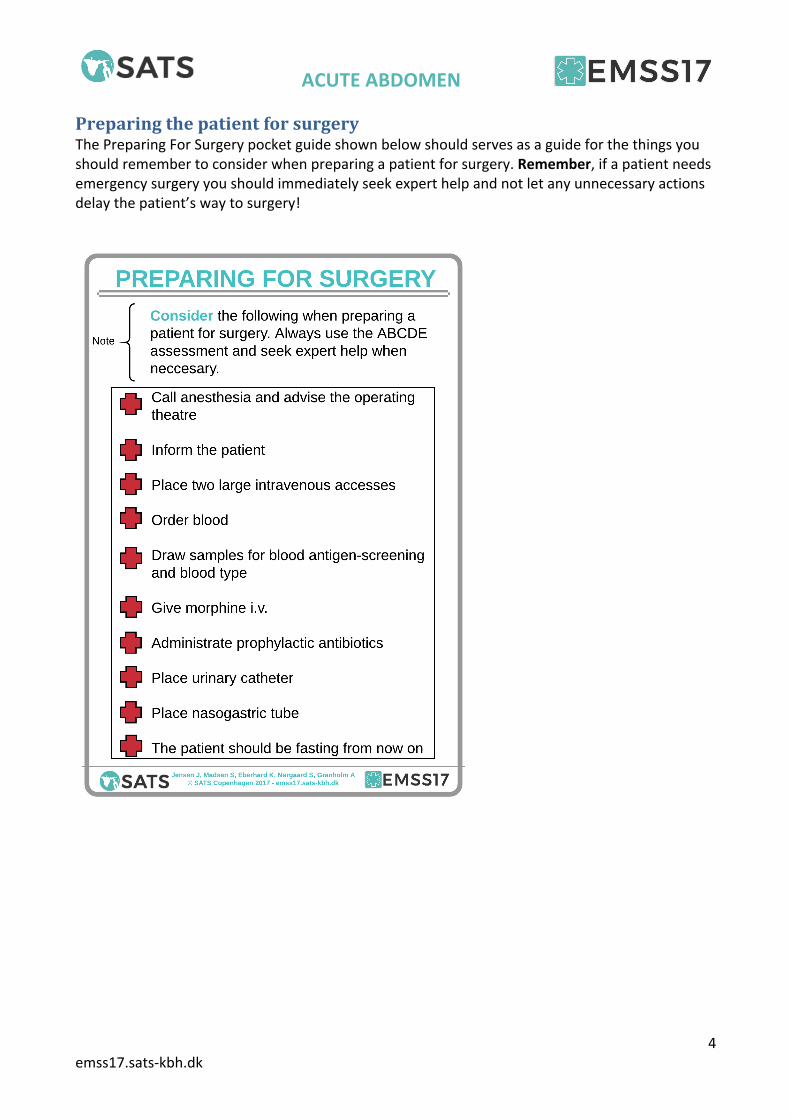
PreparingthepatientforsurgeryThePreparingForSurgerypocketguideshownbelowshouldservesasaguideforthethingsyoushouldremembertoconsiderwhenpreparingapatientforsurgery.Remember,ifapatientneedsemergencysurgeryyoushouldimmediatelyseekexperthelpandnotletanyunnecessaryactionsdelaythepatient’swaytosurgery!
ACUTEABDOMEN
5emss17.sats-kbh.dk
Acuteabdomen:diagnosesWewillnowgothroughsomeofthemostfrequentorlife-threateningcausesofacuteabdomen:
- Appendicitis- Perforatedulcer- Acutebiliarydiseases:
o Gallstoneattacko Cholecystitiso Cholangitis
- Bowelobstruction- Acutepancreatitis- Urinarytractstones- Rupturedabdominalaorticaneurism- Gynecologiccausesoftheacuteabdomen
ACUTEABDOMEN
6emss17.sats-kbh.dk
AppendicitisThemostfrequentreasonforacuteabdomen.Itisseeninallages,butismorefrequentamong10-30yearolds.Theconditioniscausedbyaninflammationintheappendix.Theconditioncanvaryfromamildlocalinflammationtoaperforatedappendixwithdiffuseperitonitisandsepsis,whichisalife-threateningcondition.
SymptomsOPQRST:Increasingabdominalpaindevelopingin12-24hours,mostoftenlocatedtotherightiliacregion.Paincanbeworsenedbymovement.In50%ofthecasesthepainstartsasdullandachingintheumbilicalregionandprogressestomoresevereandconstantpainintherightiliacregion.Nauseaisoftenpresentandvomitingandfevercanbeseen.
ClinicalpresentationThepatientpresentswithpainandliesstillinbed.Palpationshowssorenessintherightiliacregion.Peritonealreactionorabdominalguarding(“défensemusculaire”)canbeseen.Vitalsigns:temperatureof37.5-38.5°C,tachycardia(highpulse).
FurtherinvestigationBloodtests:↑C-reactiveprotein(CRP)and↑leucocytescanbeseen.Considerultrasound.
DiagnosisAppendicitisisaclinicaldiagnosis.AbdominalCTorultrasoundcanverifythediagnosiswithasensitivityof90%.Normallythediagnosisisfinallyverifiedduringsurgery.
TreatmentStrongsuspicionofappendicitis:Preparethepatientforsurgery.Diagnosticlaparoscopyandremovaloftheappendix.Ifperforatedappendix:IVantibioticsaccordingtolocalguidelines.Littlesuspicionofappendicitis:admissiontosurgicaldepartmentfollowedbyclinicalexaminationagainafter6-8hours.
ACUTEABDOMEN
7emss17.sats-kbh.dk
PerforatedulcerAperforatedulcercanbelocalizedinthestomachortheduodenum.Theconditionismostcommonlycausedbyacid,medications(e.g.NSAIDs)and/orthebacteriaHelicobacterpylori.Itismostcommonlyseeninpatients>50yearsold.Oftenagastricorduodenalulcerdoesnotcauseseveresymptomspriortoperforation.Nightlyburningordullpainintheepigastricregioncanbeexperiencedaswellasanorexia,vomitingandweightloss.
SymptomsOPQRST:suddenonsetofseverepainintheepigastricregionthatincreaseswithmovement.Nauseaandvomitingismostoftenseen.Thepatientisoftenknownwithpepticulcers.
ClinicalpresentationAcutelyaffectedpatient,paleandlyingstillinbed.Severepainwhenpalpatingtheabdomen,mostoftenabdominalguarding.Vitalparameters:superficialrespirationduetopain.Tachycardia(highpulse).Hypotension(lowbloodpressure)ifseptic.
FurtherinvestigationsBloodtests:↑CRPand↑leucocytesABGCToftheabdomen(unlessabdominalguarding,thenCTmustnotdelaysurgery)orabdominalX-rayECG
DiagnosisMedicalhistory,clinicalpresentationandCTwithfreeintraabdominalairconfirmsthediagnosis.Thediagnosisisfinallyconfirmedduringsurgery.
TreatmentPreparethepatientforsurgery.Laparoscopicsuturingoftheperforation.Aftersurgery:eradicationofHelicobactorpyloriandprotonpumpinhibitors(medicationtodecreaseacidproductioninthestomach)untiltheulcerhashealed.
ACUTEABDOMEN
8emss17.sats-kbh.dk
AcutebiliarydiseasesTherearethreecommonconditionsofthebiliarysystemthatcauseacuteabdomen:gallstoneattack,cholecystitisandcholangitis.GallstoneattackAsimplegallstoneattackcanbeseenintheemergencydepartment,butismostlytreatedoutsidethehospital.Normallyagallstoneattacklasts<24hoursandisnotaccompaniedbyfever.Thepatientissusceptibleforcholecystitisorcholangitisiffebrileorinpain>24hoursandshouldbeadmittedtothehospital.CholecystitisAninflammationofthegallbladder,mostoftencausedbyagallstoneobstructingtheoutletofthegallbladdersoitcan'tbeemptied.Thiscausesedema,inflammationandischemiaofthegallbladder.
SymptomsOPQRST:theonsetisoftensimilartoaregulargallstoneattack,butthepainispersistent.Thepainisdescribedasachingandconstant.Thepainisincreasedbymovementanddeepinspiration.Thepainisaccompaniedwithvomitingandfever.
ClinicalpresentationPatientacutelyaffectedbypain.Temperature37.5-38.5°C.Strongsorenesswhenpalpatingtherighthypochondriacregion.Sometimesthetensegallbladdercanbepalpatedduringinspiration;thisiscalledMurphy'ssign.Jaundicecanbeseen.
FurtherinvestigationsBloodsamples:↑CRPand↑leucocytes,↑bilirubincanbeseen,↑livermarkers(ALAT,ASAT,alkalinephosphatase)Ultrasoundofliverandbileducts.
DiagnosisMedicalhistory,clinicalfindingsandaprevioushistoryofgallstoneattacksshouldleadtosuspicionofcholecystitis.Ultrasoundconfirmsthediagnosis.Ifthepatientisseptic,suspectperforatedgallbladder!
TreatmentDuration<5days:preparethepatientforsurgery:laparoscopicremovalofthegallbladderthenextday.Duration≥5days:conservativetreatmentwithanalgesics,antibioticsandregularbloodsamplestomeasurethetreatmenteffect.Electiveremovalofthegallbladdercanbedoneafter3months.Ifthepatientisseverelyaffected,ultrasoundguidedgallbladderdrainageshouldbeconsidered.
ACUTEABDOMEN
9emss17.sats-kbh.dk
CholangitisCausedbyagallstoneortumorobstructingthecommonbileduct(ductuscholedochus;thebileductleadingthebiletotheduodenum).
SymptomsOPQRST:acuteonsetofpainintherighthypochondriacregion.Thepainissevereandconstantandaccompaniedbynausea.Oftenhighlyfebrilewithtemperature>39°C.Thepatientcanbeseptic.Oftenthepatientisknowntohavegallstonesoracancerinthebileduct.
ClinicalpresentationThepatientisacutelyaffected.Mostlikelywithjaundice.Strongpainwhenpalpatingtherighthypochondriacandepigastricregion,canbewithperitonealreaction.Vitalsigns:temperature39-40°C,tachycardia,lowbloodpressure(ifseptic).Cerebralinvolvementwithconfusioncanbeseen.
FurtherinvestigationsBloodsamples:↑CRPand↑leucocytes,↑↑↑bilirubin,↑livermarkers(ALAT,ASAT,alkalinephosphatase)UltrasoundoftheliverandbileductsMagneticresonancecholangiopancreatography(MRCP)
DiagnosisThemedicalhistory,clinicalfindingsandaprevioushistoryofgallstoneattacksshouldraisesuspicionofcholangitis.Findingssupportingthediagnosisareincreasedalkalinephosphataseandbilirubinaswellasotherlivermarkers.Dilatedcommonbileduct(>10mm)onMRCPorultrasonographyconfirmsthediagnosis.MRCPhasahighersensitivitythanultrasound.
TreatmentPreparethepatientforsurgery!Thetreatmentisendoscopicretrogradecholangio-pancreaticography(ERCP)andshouldbeperformedwithin24hours.ERCPisanendoscopicprocedurethatisusedtovisualizethebileductandextractthegallstonecausingtheobstruction.Astentcanbeplacedafterthestonehasbeenextracted.
ACUTEABDOMEN
10emss17.sats-kbh.dk
BowelobstructionAconditionwithpassagethroughtheintestineblockedbyanobstruction.Themostcommoncausesforbowelobstructionsarepreviousabdominalsurgery(causingadhesionsbetweentheintestinesandtheperitoneum),herniasandcancer.
SymptomsOPQRST:intermittentpainevolvingtoconstantpain.Paincanvaryfrommildtosevere.Symptomsvarydependingonthelocationoftheobstruction.Moreproximalobstructionswillquickerleadtovomitingthanmoredistalobstructions.Noflatulenceorexcretionoffecesfordays.
ClinicalpresentationDistendedabdomen,clinicaldehydration.Moredistalobstructionswillleadtomoredistension.High-pitchedbowelsoundscanbeheardwhenauscultatingthepatient.Ifperitonealreactionisfound,perforationshouldbeexpected.Rectalexplorationfortumorsshouldbeperformed.
FurtherinvestigationsBloodsamples:↑CRPand↑leucocytescanbeseen.Electrolytederangementcanbeseenaswell.ABGCT(ifpossiblewithcontrast)orX-rayoftheabdomen
DiagnosisCTorX-rayshowsdilatedintestinesandair-fluidlevels,confirmingthediagnosis.
TreatmentPreparethepatientforsurgery!Treatmentdependsofthecauseoftheobstructionandcanincludeexplorativelaparotomyorendoscopy.Thetreatmentshouldrelievethepatientoftheobstruction.
ACUTEABDOMEN
11emss17.sats-kbh.dk
AcutepancreatitisAnacuteinflammationofthepancreas.Theunderlyingcausesaremostoftenobstructionsofthebileductoralcohol,butmanyothercausescanbeseen.
SymptomsOPQRST:severeabdominalpainintheepigastricorlefthypochondriacregionradiatingtotheback.Nausea,vomiting,feverandperitonealreactioncausedbyileus(paralysisoftheintestines)canbeseen.Thepatientcanbeincirculatoryshockbecauseofhypovolemiaorsepsis.
ClinicalpresentationAcutelyaffectedpatientwithseverepain.Soreabdomen,possiblywithabdominalguarding.Vitalsigns:tachycardiaandhypotensioncanbeseen.Fever.
FurtherinvestigationsBloodsamples:↑↑↑amylase,↑CRP,↑leucocytesABGECGAbdominalX-rayorCT:toruleoutotherdiagnosesAbdominalultrasoundorCT:toseeifpancreasisenlargedoredematousorifanycystsortumorsarepresentChestX-ray
DiagnosisAbloodamylase3timeshigherthantheupperlimitofthereferenceintervalconfirmsthediagnosis.
TreatmentThetreatmentaimstoeliminatethecauseandtreatsymptomsandcomplications.Treatmentandsupportcaninclude:-Fluidsandelectrolytes(derangementsshouldbecorrected)-ERCPifthebileductisobstructed-Morphine-Nutritionaldiet-Protonpumpinhibitors-Considerantibiotics
ACUTEABDOMEN
12emss17.sats-kbh.dk
Urinarytractstones'Stones'areformedintherenalpelvis.Whenthestonespass,theycangetstuckintheureters,thebladderortheurethraandcausepainfulsymptoms.
SymptomsOPQRST:oftenwithoutsymptoms,butwhenobstructingtheuretertheycauseseverepainintheleftorrightlumbarregionwithsuddenonset.Thepainoftenradiatestothebackandgroinandtheintensitycanvary.Apatientwithurinarytractstoneswilloftenberestless.Symptomslastfrom30minutestoseveralhours.Nauseaandvomitingcanbeseen.
ClinicalpresentationAcutelyaffectedbypain,restless.Typicallysoreinthelumbarregion,butnotintherestoftheabdomen.Vitalsigns:nofever.Pain-inducedhypertensionandtachycardiacanbeseen.
FurtherinvestigationsBloodsamplestoruleoutotherconditions(resultsaretypicallynormal)UrinedipsticktestCT-urography
DiagnosisMedicalhistoryandclinicalfindingswithseverepain,butotherwisenotacutelyaffectedpatientgivesshouldraisethesuspicion..CT-urographyisdiagnosticwhenthestonecanbeseenintheurinarytract.
TreatmentRectalpainkillers.Anattacknormallydoesn'tlastformorethan6-8hoursifthestoneis<5mm,asthestonepassestheureterspontaneously.Hydronephrosis(enlargedrenalpelvis)shouldberuledoutandthepatientcanbedischargedwithpainkillers.Ifthestoneis>5mmortheobstructionhascausedhydronephrosis,thepatientshouldbeadmittedtoanurologicaldepartment.
ACUTEABDOMEN
13emss17.sats-kbh.dk
RupturedabdominalaorticaneurismAnaneurismisanabnormaldilatationofanartery.Theabdominalaneurismismorefrequentthanthethoracic.Theprevalenceofaneurismsincreaseswithage.Ananeurismisatriskofrupturing,whichcausesbleeding-thebiggertheaneurism,thebiggertheriskofrupture.Arupturedaorticaneurismisaconditionwithhighmortality.
SymptomsOPQRST:suddenonsetofseverepain,mostoftenintheumbilicalregion,radiatingtothebackandthighs.
ClinicalpresentationClinicalfindingsdependontheamountofbleeding.Thepatientpresentswithsignsofcirculatoryshock:paleandclammywithhypotensionandtachycardia.Apulsatingandsoreabdominalmasscanattimesbepalpatedbetweentheumbilicusandthexiphoidprocessofthesternum.
FurtherinvestigationsBloodsamplesincludingbloodtypeandbloodantigenscreening-testABGBedsideultrasoundcanshowaneurismandbleeding
DiagnosisTheclinicalpresentationofapatientincirculatoryshockshouldraisesuspicion.Inpatientsknownwithanabdominalaorticaneurism(previouslydiagnosedonultrasoundorCT),thediagnosisshouldbesuspected.
TreatmentPreparethepatientforimmediateemergencysurgery!Seekseniorandexperthelpimmediately.Orderblood(massivetransfusionpackaged–redbloodcells,freshfrozenplasmaandplatelets)andadminister.Plantransfertoavascularsurgicaldepartment.Surgerywithavascularprosthesisoranendovascularstenthastobeperformedasfastaspossible.
ACUTEABDOMEN
14emss17.sats-kbh.dk
GynecologiccausesoftheacuteabdomenInawomanpresentingwithacuteabdomen,alwaysconsidergynecologicalcauses.Onlyabriefoverviewofthemostimportantgynecologiccausestoconsiderisprovidedhere.Themostfrequentgynecologiccausesofacuteabdomenareectopicpregnancy,spontaneousabortionandovariancyststhatcanburstortorque.Allconditionscancausepaininthelowerabdomen.Ifthewomanisinthefertileage,alwaystakeapregnancytest(urineorplasmahCG)toruleoutectopicpregnancyorspontaneousabortion.Agynecologicexaminationshouldbeperformedtoruleouttumorsinthelowerpartoftheabdomenthatcouldbeanectopicpregnancyorovariancyst.Alwayspalpateforsoreness.Ifthepatientisnotacutelyaffected,atransvaginalultrasoundcanvisuallyinvestigateectopicpregnancy,cystsandbloodorfreefluidintheabdomen.Ifthepatientisacutelyaffected,surgerymaybeindicated.Gynecologiccausesofacuteabdomencancausebleedingintotheabdomen.Thiscanbealife-threateningconditionthatrequiressurgery.Torquedovariancystsshouldalsobetreatedwithemergencysurgerytopreventnecrosis.Aburstedovariancystisacommonandgenerallyharmlesscondition.Itcancausearelativelymildpainintheiliacregions,butwillnotacutelyaffectthepatient.Thepaintypicallydecreaseswithinacoupleofdays.FinalwordsAswritteninthebeginning,thisisapresentationofsomeofthepossiblecausesofacuteabdomenandisonlymeanttoprovideyouwithabriefoverview.Thedocumentisnotexhaustive,andyoushouldnotmemorizeeverything.Remember:Ifyouareindoubt,alwaysseekexperthelp–callaseniorcolleagueoraspecialist!





