Embed Size (px)
Citation preview

EMS Agenda for the Future: Where We Are . . .
Where We Want to Be
EMS Agenda for the FutureSteering Committee:
Theodore R Delbridge, MD, MPH*
Bob Bailey‡
John L Chew Jr, MS§
Alasdair KT Conn, MDII
Jack J Krakeel, MBA**
Dan Manz‡‡
David R Miller§§IIII
Patricia J O’Malley, MD¶#
Susan D Ryan¶¶
Daniel W Spaite, MD##
Ronald D Stewart, OC, MD, DSC***
Robert E Suter, DO, MHA‡‡‡
E Marie Wilson, RN, MPA§§§
During the past 30 years, emergency medical services (EMS) in theUnited States have experienced explosive growth. The Americanhealth care system is now transforming, providing an opportunetime to examine what we have learned over the past three decadesin order to create a vision for the future of EMS. Over the courseof several months, a multidisciplinary steering committee collab-orated with hundreds of EMS-interested individuals, organiza-tions, and agencies to develop the “EMS Agenda for the Future.”Fourteen EMS attributes were identified as requiring continueddevelopment in order to realize the vision established within theAgenda. They are Integration of Health Services, EMS Research,Legislation and Regulation, System Finance, Human Resources,Medical Direction, Education Systems, Public Education, Prevention,Public Access, Communication Systems, Clinical Care, InformationSystems, and Evaluation. Discussion of these attributes providesimportant guidance for achieving a vision for the future of EMSthat emphasizes its critical role in American health care.
[Delbridge TR, Bailey B, Chew JL Jr, Conn AKT, Krakeel JJ, Manz D,Miller DR, O’Malley PJ, Ryan SD, Spaite DW, Stewart RD, SuterRE, Wilson EM: EMS agenda for the future: Where we are . . .where we want to be. Ann Emerg Med February 1998;31:251-263.]
I N T R O D U C T I O N
The 1966 paper “Accidental Death and Disability: TheNeglected Disease of Modern Society” provided 29 recom-mendations to improve the American emergency health caresystem.1 Eleven related directly to out-of-hospital emergencymedical services (EMS). Subsequent federal initiatives, inthe forms of the Highway Safety Act of 1966 and the Emer-gency Medical Services Systems Act of 1973, and otherpublic and private support spawned rapidly evolving EMSsystems across the country. EMS expanded in the beliefthat better response would improve patient outcomes. Yetinitial EMS growth began with a lack of knowledge of themost efficient processes for delivering optimal resources tothe spectrum of situations addressed by today’s EMS systems.
From the Department of EmergencyMedicine, University of Pittsburgh,Pittsburgh, PA*; the North CarolinaOffice of Emergency Medical Services,Raleigh, NC‡; EMSSTAR Group,Annapolis, MD§; Emergency ServicesII
and Pediatric Emergency Services,¶
Massachusetts General Hospital, andEmergency Medical Services for Chil-dren, Massachusetts Department ofPublic Health,# Boston, MA; FayetteCounty Fire and Emergency Services,Fayetteville, GA**; Vermont EmergencyMedical Services Division, Burlington,VT‡‡; HealthSpan TransportationServices§§ and Allina Health System,II II
St Paul, MN; National Highway TrafficSafety Administration, WashingtonDC¶¶; Arizona Emergency MedicineResearch Center, University ofArizona, Tucson, AZ##; Ministry ofHealth, Halifax, Nova Scotia***;Department of Emergency Services,Providence Hospital and MedicalCenters, Southfield, MI‡‡‡; and theConnecticut Office of EmergencyMedical Services, Hartford, CT.§§§
This article is being copublished inPrehospital Emergency Care.
Received for publication August 21, 1997. Revision receivedDecember 11, 1997. Accepted forpublication December 15, 1997.
Supported by grant DT4N22-G-05188 from the National HighwayTraffic Safety Administration.
Copyright © 1998 by the AmericanCollege of Emergency Physicians.
S P E C I A L C O N T R I B U T I O N
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 5 1
E M S A G E N D ADelbridge et al
2 5 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8
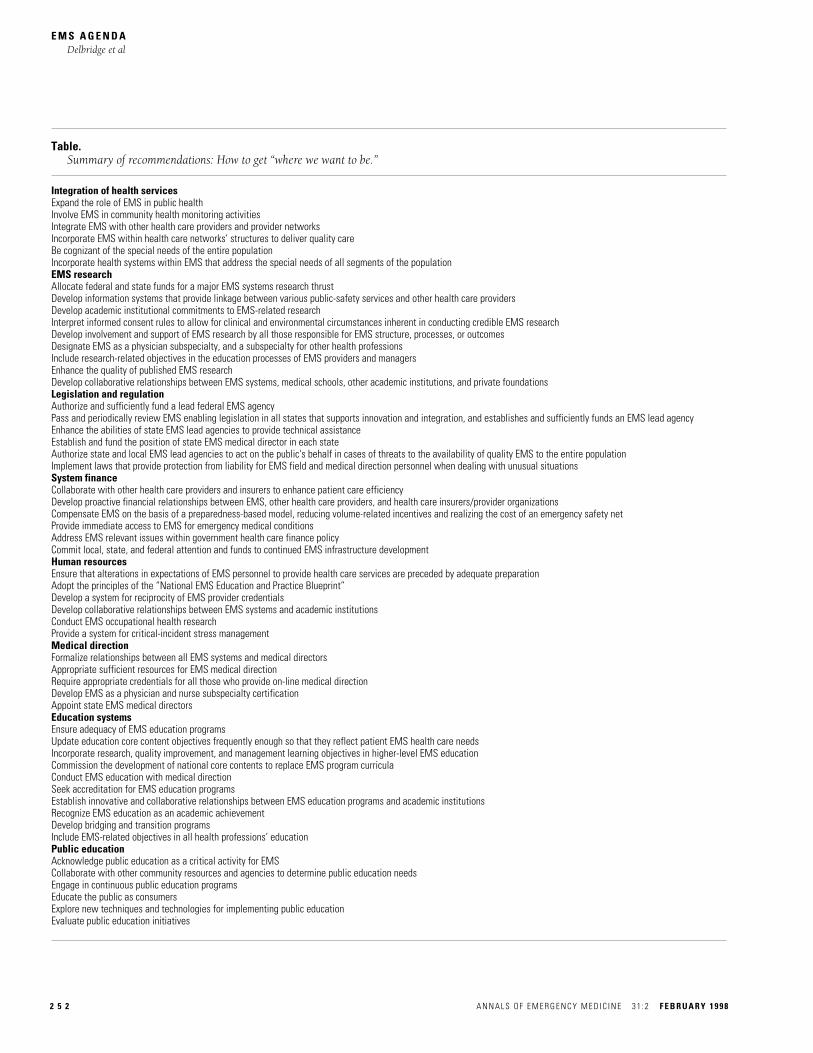
Table. Summary of recommendations: How to get “where we want to be.”
Integration of health servicesExpand the role of EMS in public healthInvolve EMS in community health monitoring activitiesIntegrate EMS with other health care providers and provider networksIncorporate EMS within health care networks’ structures to deliver quality careBe cognizant of the special needs of the entire populationIncorporate health systems within EMS that address the special needs of all segments of the populationEMS researchAllocate federal and state funds for a major EMS systems research thrustDevelop information systems that provide linkage between various public-safety services and other health care providers Develop academic institutional commitments to EMS-related researchInterpret informed consent rules to allow for clinical and environmental circumstances inherent in conducting credible EMS researchDevelop involvement and support of EMS research by all those responsible for EMS structure, processes, or outcomesDesignate EMS as a physician subspecialty, and a subspecialty for other health professionsInclude research-related objectives in the education processes of EMS providers and managersEnhance the quality of published EMS researchDevelop collaborative relationships between EMS systems, medical schools, other academic institutions, and private foundationsLegislation and regulationAuthorize and sufficiently fund a lead federal EMS agencyPass and periodically review EMS enabling legislation in all states that supports innovation and integration, and establishes and sufficiently funds an EMS lead agencyEnhance the abilities of state EMS lead agencies to provide technical assistanceEstablish and fund the position of state EMS medical director in each stateAuthorize state and local EMS lead agencies to act on the public's behalf in cases of threats to the availability of quality EMS to the entire populationImplement laws that provide protection from liability for EMS field and medical direction personnel when dealing with unusual situationsSystem financeCollaborate with other health care providers and insurers to enhance patient care efficiencyDevelop proactive financial relationships between EMS, other health care providers, and health care insurers/provider organizationsCompensate EMS on the basis of a preparedness-based model, reducing volume-related incentives and realizing the cost of an emergency safety netProvide immediate access to EMS for emergency medical conditionsAddress EMS relevant issues within government health care finance policyCommit local, state, and federal attention and funds to continued EMS infrastructure developmentHuman resourcesEnsure that alterations in expectations of EMS personnel to provide health care services are preceded by adequate preparationAdopt the principles of the “National EMS Education and Practice Blueprint”Develop a system for reciprocity of EMS provider credentialsDevelop collaborative relationships between EMS systems and academic institutionsConduct EMS occupational health researchProvide a system for critical-incident stress managementMedical directionFormalize relationships between all EMS systems and medical directorsAppropriate sufficient resources for EMS medical direction Require appropriate credentials for all those who provide on-line medical directionDevelop EMS as a physician and nurse subspecialty certificationAppoint state EMS medical directorsEducation systemsEnsure adequacy of EMS education programsUpdate education core content objectives frequently enough so that they reflect patient EMS health care needsIncorporate research, quality improvement, and management learning objectives in higher-level EMS educationCommission the development of national core contents to replace EMS program curriculaConduct EMS education with medical directionSeek accreditation for EMS education programsEstablish innovative and collaborative relationships between EMS education programs and academic institutionsRecognize EMS education as an academic achievementDevelop bridging and transition programsInclude EMS-related objectives in all health professions’ educationPublic educationAcknowledge public education as a critical activity for EMSCollaborate with other community resources and agencies to determine public education needsEngage in continuous public education programsEducate the public as consumersExplore new techniques and technologies for implementing public educationEvaluate public education initiatives
Because the health care system is undergoing transfor-mation, this is an opportune time to examine what has beenlearned during the past three decades in order to create avision for the future of EMS. In June 1995, the NationalHighway Traffic Safety Administration (NHTSA), in partner-ship with the Health Resources and Services Administration(HRSA), Maternal and Child Health Bureau (MCHB), real-ized the need for agencies, organizations, and individualsinvolved in EMS to evaluate their roles and chart a coursefor the future. They commissioned the development of the“EMS Agenda for the Future” to help meet that need.
The purpose of creating the “EMS Agenda for the Future”was to determine the most important directions for futureEMS development, incorporating input from a broad groupof EMS stakeholders. This would provide guiding principlesfor the continued evolution of EMS, focusing on out-of-hospital aspects of the system.
P R O C E S S
The process used to develop the “EMS Agenda for the Future”was a modification of the National Institutes of Health (NIH)Technology Assessment and Practice Guidelines Forum.2
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 5 3
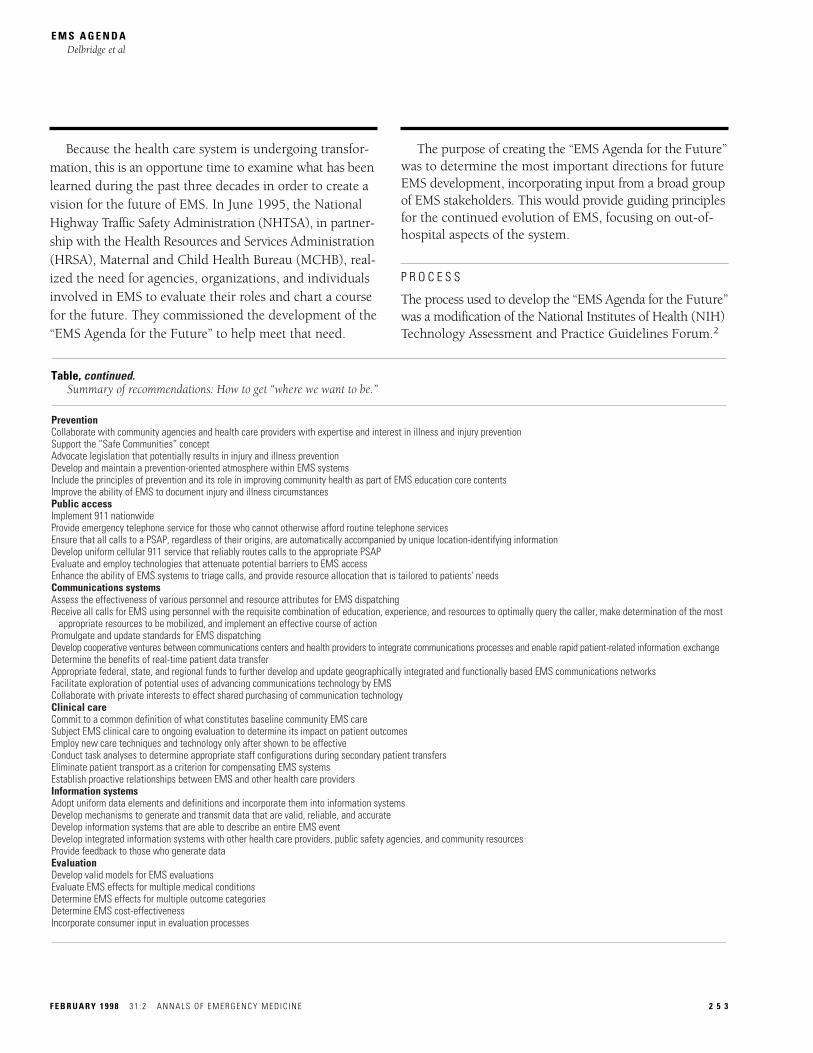
Table, continued. Summary of recommendations: How to get “where we want to be.”
PreventionCollaborate with community agencies and health care providers with expertise and interest in illness and injury preventionSupport the “Safe Communities” conceptAdvocate legislation that potentially results in injury and illness preventionDevelop and maintain a prevention-oriented atmosphere within EMS systemsInclude the principles of prevention and its role in improving community health as part of EMS education core contentsImprove the ability of EMS to document injury and illness circumstancesPublic accessImplement 911 nationwideProvide emergency telephone service for those who cannot otherwise afford routine telephone servicesEnsure that all calls to a PSAP, regardless of their origins, are automatically accompanied by unique location-identifying informationDevelop uniform cellular 911 service that reliably routes calls to the appropriate PSAPEvaluate and employ technologies that attenuate potential barriers to EMS accessEnhance the ability of EMS systems to triage calls, and provide resource allocation that is tailored to patients' needsCommunications systemsAssess the effectiveness of various personnel and resource attributes for EMS dispatchingReceive all calls for EMS using personnel with the requisite combination of education, experience, and resources to optimally query the caller, make determination of the most
appropriate resources to be mobilized, and implement an effective course of actionPromulgate and update standards for EMS dispatchingDevelop cooperative ventures between communications centers and health providers to integrate communications processes and enable rapid patient-related information exchangeDetermine the benefits of real-time patient data transferAppropriate federal, state, and regional funds to further develop and update geographically integrated and functionally based EMS communications networksFacilitate exploration of potential uses of advancing communications technology by EMSCollaborate with private interests to effect shared purchasing of communication technologyClinical careCommit to a common definition of what constitutes baseline community EMS careSubject EMS clinical care to ongoing evaluation to determine its impact on patient outcomesEmploy new care techniques and technology only after shown to be effectiveConduct task analyses to determine appropriate staff configurations during secondary patient transfersEliminate patient transport as a criterion for compensating EMS systemsEstablish proactive relationships between EMS and other health care providersInformation systemsAdopt uniform data elements and definitions and incorporate them into information systemsDevelop mechanisms to generate and transmit data that are valid, reliable, and accurateDevelop information systems that are able to describe an entire EMS eventDevelop integrated information systems with other health care providers, public safety agencies, and community resourcesProvide feedback to those who generate dataEvaluationDevelop valid models for EMS evaluationsEvaluate EMS effects for multiple medical conditionsDetermine EMS effects for multiple outcome categories Determine EMS cost-effectivenessIncorporate consumer input in evaluation processes
A multidiscipline steering committee prepared initial draftsof the document. The committee distributed its second draftto 500 EMS-interested organizations and individuals for peerreview. Of these, 178 (28%) furnished comments. Thesteering committee analyzed these comments and revisedthe document accordingly.
The “EMS Agenda for the Future” Blue Ribbon Confer-ence convened in McLean, VA, on December 1-3, 1995. Onehundred thirty-three individuals, including physicians, EMSproviders, nurses, educators, and administrators, partici-pated. Each participant attended several of 32 breakoutsessions to comment on critical aspects of the future of EMSand to critique the steering committee’s updated draft. Later,the steering committee sent its subsequent revision to con-ference participants for their final comments. The steering
committee met again in March 1996, at which time finalcomments were reviewed and appropriately incorporated.The following discussion summarizes the conclusions andrecommendations of the “EMS Agenda for the Future.”
E M S : V I S I O N F O R T H E F U T U R E
The health system of today, with its emphasis on advancedtechnology and costly acute interventions to achieve societalhealth, is transforming to focus on the early identificationand modification of risk factors before illness or injurystrikes. EMS will mirror and, in some cases, may lead thistransition.
EMS of the future will be community-based health man-agement that is fully integrated with the overall health care
E M S A G E N D ADelbridge et al
2 5 4 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8
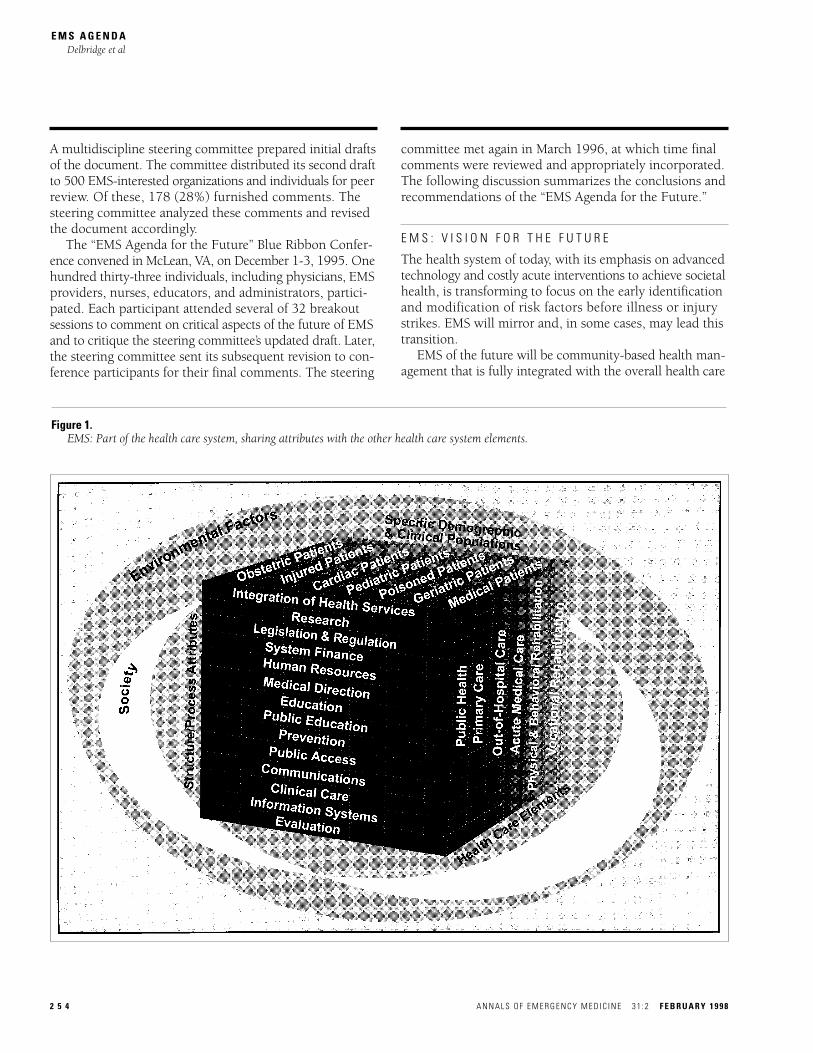
Figure 1.EMS: Part of the health care system, sharing attributes with the other health care system elements.

system. It will have the ability to identify and modify ill-ness and injury risks, provide acute illness and injury careand follow-up, and contribute to treatment of chronic con-ditions and community health monitoring. EMS will beintegrated with other health care providers and public healthand public safety agencies. It will improve communityhealth and result in more appropriate use of acute healthcare resources. EMS will remain the public’s emergencymedical safety net.
The vision for the future emphasizes a continued criticalrole for EMS in caring for the health of Americans. FourteenEMS attributes, described below, require ongoing attentionand development if such a vision is to be realized. Specificrecommendations with regard to each attribute are sum-marized in the Table.
I N T E G R A T I O N O F H E A L T H S E R V I C E S
Where we are Contemporary EMS systems were created to meet the
immediate needs of the acutely ill and injured. EMS, ingeneral, meets these objectives in relative isolation fromother health care and community resources. EMS systemsare disconnected from other community resources and donot routinely ensure appropriate follow-up by other healthcare providers or agencies. They are unable to integrate theircare with sources for patients’ continuing health care. Thus,potential positive effects of EMS, in terms of improvedhealth for individual patients and the community, remainunrealized.
Researchers have published reports regarding publichealth surveillance and referral to social-service agenciesby EMS personnel.3-5 Others have described a model forincorporating EMS and health monitoring referral systems.6
Some EMS systems are determining the benefits of collabo-ration and routine communication with patients’ primaryhealth care providers.
Where we want to be EMS is an integral component of the health care system,
and it shares the same attributes as the other elements thatcollectively represent the continuum of health care (Figure 1).EMS provides care that is integrated with other health careproviders and community health resources, ensuring thatEMS treatment is part of a complete health care program.Liaisons with other community resources enable EMS to beproactive in affecting people’s long-term health, relayinginformation regarding potentially unhealthy situations toagencies with a vested interest in maintaining the health oftheir clients. With medical direction, EMS facilitates accessfor its patients to appropriate sources for continued medical
care, supporting efforts to implement cost-effective com-munity health care while ensuring that the special needs ofspecific patients are addressed.
E M S R E S E A R C H
Where we are EMS has evolved rapidly over the past 30 years despite
slow progress in developing EMS-related research. The “chainof survival” concept provides the best evidence of meaning-ful systems research.7,8 Most published EMS research focuseson a single intervention or health problem and rarely ad-dresses the inherent complexities of EMS systems.9 In manycases our poor understanding of systems research has ledto the development of wrong assumptions with regard toEMS care.9,10
Currently there are major impediments to the develop-ment of high quality EMS research. They include inadequatefunding, lack of integrated information systems that providefor meaningful linkage with patient outcomes, paucity ofacademic research institutions with long-term commitmentsto EMS systems research, overly restrictive informed consentinterpretations, and lack of education and appreciation byEMS personnel regarding the importance of EMS research.
Where we want to be A national EMS research agenda provides guidance so
that a sufficient volume of quality research is undertaken todetermine the effectiveness of EMS system design and spe-cific interventions. EMS evolves with a scientific basis.Adequate investigations of EMS interventions and systemdesigns occur before they are advocated as standards. Asmuch as possible, EMS research employs systems analysismodels, using multidisciplinary approaches to answer com-plex questions. Federal agencies responsible for fundinghealth care research are committed to EMS-related studies.Additionally, integrated information systems facilitate datacollection to determine EMS effectiveness. EMS personnelof all levels appreciate the role of research in terms of creat-ing a scientific basis for EMS care.
L E G I S L A T I O N A N D R E G U L A T I O N
Where we are All states have legislation that provides a statutory basis
for EMS activities and programs. However, during 35 stateevaluations by NHTSA technical assessment teams, only40% of states reported having comprehensive enabling legis-lation for development of a statewide EMS system.11 Only20% of states had an identified lead agency that providedcentral coordination of EMS system activities.11 In some
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 5 5

cases, local governments have passed ordinances to delineateEMS standards for their communities. Authorities respon-sible for implementing regulations are, in general, exten-sively involved in personnel licensing, training programcertification, EMS vehicle licensing, and record keeping.
Where we want to be A federal lead EMS agency is sufficiently funded to pro-
vide coordination among federal programs and agenciesaffecting EMS, serve as an information clearinghouse, andfacilitate nationwide EMS development. All states have asingle EMS lead agency responsible for developing and over-seeing a statewide EMS system. It ensures that EMS of accept-able quality is available to the entire population and providestechnical assistance to local EMS systems. Furthermore,state legislation provides a template that allows local medi-cal directors to determine the specific parameters of practicefor their EMS systems, helping them meet the health careneeds of their communities.
S Y S T E M F I N A N C E
Where we are Providing the nation with EMS is a multi–billion-dollar
effort each year. In Hawaii, where the entire EMS system isstate-funded, the cost is approximately $27 per capita peryear.12 Extrapolating that cost to the entire US populationyields an estimate of $6.75 billion per year for EMS. Thisdoes not include the costs of human efforts, including thoseby volunteers.
EMS systems are funded by a combination of public andprivate funds. Those EMS systems relying on third-partypayers for significant revenue must, in general, providepatient transportation in order to be reimbursed for theirservices. The primary determinants of EMS cost relate tosystem preparedness. On the other hand, the primary deter-minant of payment for services is patient transport. Thusthe driving forces of cost and payment are not aligned.
Some health care insurers or providers may stipulate totheir subscriber patients that authorization must precedeutilization of EMS. Refusal to pay EMS for services providedmay be based on lack of preauthorization or retrospectivedetermination that the patient condition did not representan emergency.
Where we want to be As a component of the health care delivery system, EMS
is consistently funded by mechanisms that fund other aspectsof the system. These mechanisms recognize the value oftreatment that is provided without transport. Payment forEMS is preparedness-based, accounting for the cost of main-
taining a state of suitable readiness. It considers such factorsas service area size and complexity, utilization, and prede-termined quality standards. Finances are linked to value, asdetermined by community consumers, and cost and pay-ment drivers are aligned. The maintenance of EMS systempreparedness and continued development of its infrastruc-ture is also facilitated by local, state, and federal governments.
H U M A N R E S O U R C E S
Where we are Across the country, more than 40 different levels of emer-
gency medical technician (EMT) certification exist. However,the “National EMS Education and Practice Blueprint” hasestablished standard knowledge and practice expectationsfor four levels of EMS providers: first responder, EMT-basic,EMT-intermediate, and EMT-paramedic.13 Many other healthcare workers also collaborate to effect the patient care pro-vided by EMS. They include physicians, nurses, nursepractitioners, physician assistants, respiratory therapists, andothers. Volunteers serve more than 25% of the nation’s pop-ulation, but the number of EMS volunteer organizations isdecreasing.14,15
Perennial issues for EMS workers include unique occu-pational risks, limited mobility, and inadequate compensa-tion. Emergency personnel are at least twice as likely as thegeneral population to suffer from posttraumatic stress dis-orders.16,17 Exposure to bloodborne pathogens may be an-other significant risk. Between 6 and 19 per 1,000 advancedlife support (ALS) EMS responses involve a contaminatedneedlestick to EMS personnel.18,19 The average hepatitis Bvirus seroprevalence among EMS workers has been reportedto be 14%, three to five times higher than the general pop-ulation.20 EMS workers frequently confront dangeroussituations, and assault, lifting, falling, and motor vehiclecrashes contribute to injuries.21-24
Where we want to be People attracted to EMS service reflect the cultural diver-
sity of our communities. The value of supporting the well-being of the work force is widely recognized, and there isimproved understanding of the occupational issues uniqueto EMS workers. All EMS workers receive available immu-nizations against worrisome communicable diseases, appro-priate protective equipment, and pertinent education.
Reciprocity agreements between states eliminate un-necessary barriers to mobility for credentialed EMS profes-sionals. Career ladders exist to facilitate transitions for EMSworkers to parallel fields. EMS personnel are recognized asmembers of the health care delivery team. Optimal prepa-
E M S A G E N D ADelbridge et al
2 5 6 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8

ration helps ensure that they deliver quality care that meetsan acceptable community standard.
M E D I C A L D I R E C T I O N
Where we are Administrative and medical direction management com-
ponents, working in concert, are theoretically required toensure quality state-of-the-art EMS. In most states, medicaldirection of EMS systems that provide advanced care is man-dated by law. The form of such direction varies dramati-cally from close supervision to infrequent consultation. Agrowing number of basic level EMS systems are also beingrequired to establish a formal relationship with a medicaldirector, and the “Emergency Medical Technician: Basic(EMT-B), National Standard Curriculum” emphasizes therole of medical direction during EMT-B education andpractice.11,25
EMS medical directors come from several specialties.However, most on-line medical direction, contemporaneousmedical supervision of EMS personnel caring for patientsin the field, is provided by emergency physicians.11 A modelcurriculum for EMS education within emergency medicineresidency programs has been published.26 Although on-linemedical direction may be important for selected patients, itssystematic application for all EMS patients remains contro-versial.27-33 Medical direction activities in addition to con-temporaneous oversight of in-field personnel are also criticalfor ensuring optimal EMS. The medical director’s role is toprovide medical leadership for EMS, involving the partici-pation of medical direction staffs, oversight agencies andboards, community physicians, administrative staffs, andothers. Ultimately, this collaborative effort is responsiblefor ensuring the appropriateness and quality of EMS care.
Where we want to be All EMS providers and activities have the benefit of effec-
tive medical direction. Each state has a qualified EMS medi-cal director responsible for overseeing the state’s EMS system.EMS medical directors, in consultation with other healthprofessionals, are responsible for determining EMS systems’practice parameters to ensure that the needs of individualpatients and communities are being met.
Medical direction is provided by qualified physiciansand staffs with special competency in EMS. The resourcesavailable to medical directors are commensurate with respon-sibilities and the size and complexity of the populationserved. EMS medical directors are in a position to positivelyinfluence systems and the care they deliver through theirknowledge of the complexity of EMS, optimal care for thespectrum of EMS patients, issues related to population-based
care, occupational health concerns of EMS personnel, andprinciples of clinical research.
E D U C A T I O N S Y S T E M S
Where we are Curricula developed on behalf of the US Department of
Transportation (DOT) provide the bases for education offirst responders, EMT-Bs, EMT-intermediates, and EMT-paramedics. Settings for EMS education include hospitals,community colleges, universities, technical centers, privateinstitutions, and fire departments.34 Increasing numbersof colleges offer bachelor’s degrees in EMS.35 Most reportsof EMS education issues discuss the requirements to developspecific skill proficiency.36-44 However, meaningful analyseslinking the suitability of EMS education to the spectrum ofservices provided have not been published.
Where we want to be EMS education employs sound principles and facilitates
lifelong learning for EMS professionals. It provides the toolsnecessary for EMS providers to serve identified health careneeds of the population. Thus educational objectives arecongruent with the services provided. Education programsare based on nationally standardized core contents for pro-viders of various levels. Core-content standardization facili-tates recognition by credentialing agencies while providingprogram infrastructure and opportunity for local customiza-tion. Higher-level EMS education programs are affiliatedwith academic institutions. Colleges and universities recog-nize EMS education as achievement worthy of academiccredit. Interdiscipline and bridging programs provide avenuesfor EMS professionals to enhance their credentials or transi-tion to other health care roles.
P U B L I C E D U C A T I O N
Where we are EMS has not yet developed its full potential to educate
the lay public. Most of what the public knows about EMSis derived from television programs intended for entertain-ment and not for education. Isolated examples of EMS pub-lic education initiatives exist. In some areas EMS for Children(EMS-C) funds have facilitated development of programsrelated to childhood illness and injury.45 The “Make theRight Call” campaign and other efforts have focused on timelyaccess and appropriate utilization of EMS.46,47 Additionally,some EMS systems participate in disseminating CPR andbystander care education. However, planned and evaluatedEMS public education initiatives remain sporadic. In general,EMS is not optimally engaged in providing education that
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 5 7

improves community health through prevention, earlyidentification, and treatment.
Where we want to be Public education is acknowledged as an essential ongoing
activity of EMS. EMS contributes to improving communityhealth by disseminating valuable information regardingprevention of illnesses and injuries, appropriate access andutilization of EMS and other health care services, and by-stander care. EMS public education programs address theneeds of all members of the community, including school-age children, senior citizens, and those with special needs.The public’s knowledge of EMS-related issues, includingfunding, level of care provided, and system expectationsand standards, is enhanced. Furthermore, purchasers ofhealth care services are well-informed about EMS issues,including evaluating and ensuring optimal EMS.
P R E V E N T I O N
Where we are The health care system is evolving from an emphasis on
providing highly technologic, curative care to improvinghealth through prevention and wellness. In this era, injuryprevention has taken on a new dimension for both improv-ing the nation’s health and truly controlling health carecosts.48 Addition of injury prevention modules to the“National EMS Education and Practice Blueprint” has beenstrongly advocated.49
EMS is not commonly linked to the public’s preventionconsciousness. However, the potential role of EMS in pre-vention has been recognized.49,50 In some regions EMS per-sonnel currently are taught principles of injury prevention.51
EMS-initiated prevention programs have been successfulin reducing drowning in Pinellas County, FL, and in Tucson,AZ, and falls from height in New York.45,52,53 The “SafeCommunities” and “Safe America” concepts involve system-atic approaches to address all injuries and emphasize theneed for integration of public and private partners and efforts,including acute care.54,55
Where we want to be EMS providers receive education regarding prevention
principles. EMS systems and providers are actively engagedin injury and illness prevention programs. These are basedon local needs, addressing identified injury and illness prob-lems. EMS systems also maintain prevention-oriented atmo-spheres that emphasize safety and well-being for their ownworkers. They enhance their ability to document the circum-stances contributing to illness and injuries. Such information
is shared with other community resources to help attenuateinjury and illness risk factors.
P U B L I C A C C E S S
Where we are For nearly 30 years, 911 has been the designated national
emergency telephone number. Currently, approximately 25%of the US geography is covered by 911, making it availableto 78% of the population.56,57 Seventy-nine percent of thelargest US cities use 911E, which automatically providesemergency call-takers with callers’ telephone numbers andlocations.58 When 911 is the emergency telephone number,85% of the public knows it, compared with 36% to 47%when the emergency telephone number is seven digits.59
Cellular telephones provide one alternative for accessingemergency help. However, in many areas cellular-telephoneusers cannot be assured of reaching the appropriate publicsafety answering point (PSAP) for their locations. The mostimportant piece of information provided during an emer-gency call is the location of the person(s) requiring help.Yet adequate address systems are lacking in many areas.
Financial barriers also affect access to appropriate emer-gency care by way of 911. These include inability to pay fortelephone services, requirements of health care networksfor their patients to obtain authorization before using 911,requirements to access emergency care through an alterna-tive telephone number, and others.
Many EMS systems prioritize calls to appropriately delayresponse to less acute situations. This theoretically enhancesthe system response to critical emergencies. However, EMSis generally unsophisticated in terms of its ability to ensurethat the eventual response is commensurate with the servicesthat are actually needed.
Where we want to be Implementation of 911 is nationwide. From any telephone
in the United States, a caller can dial 911 or push an emer-gency icon in order to contact the appropriate PSAP. In caseswhere routine telephone services are not provided becauseof an inability to pay for them, limited service that enables911 access is made available. Every call for emergency ser-vices is automatically accompanied by location identifyinginformation, including an address or other geographic data.Cellular telephones and other personal communicationsystems provide a reliable means of accessing EMS by wayof 911. Position-identifying technology ensures that allemergency calls are routed to the appropriate PSAP.
No financial, legal, social, or age-related barriers to access-ing appropriate care by way of 911 exist for those who per-ceive an emergency. Systems for accessing EMS and other
E M S A G E N D ADelbridge et al
2 5 8 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8
emergency services also employ communications technol-ogy that reduce barriers imposed by geography, caller age,specific disabilities, and language spoken. EMS access resultsin allocation of system resources that best fulfill the need.Calls are triaged so that the EMS response, given the avail-able options, is the most appropriate (Figure 2).
C O M M U N I C A T I O N S Y S T E M S
Where we are Effective communication networks provide access to the
EMS system, dispatch of EMS and other public safety agen-cies, coordination among EMS and other public safety agen-cies, access to medical direction, communications to andbetween emergency health care facilities, communicationbetween EMS and other health care providers, and outletsfor disseminating information to the public. Emergencymedical dispatchers (EMDs) have been advocated as essen-tial personnel at all EMS dispatching centers, and a national
standard curriculum is available.60-64 They are able to effi-ciently query callers and provide dispatch life support viapre-arrival instructions.65,66 Such instructions are thoughtto be a cost-effective mechanism for improving survivalfrom out-of-hospital cardiac arrest.67
From a communications perspective, EMS personnel are,for the most part, isolated from the rest of the health caredelivery system. They rarely have access to medical historyinformation that might improve decision making. Limita-tions of communication systems may even hinder the abilityto obtain on-line medical direction. The spectrum of com-munications equipment currently in use is broad and includesantiquated radios, cellular telephones, and mobile data ter-minals. Only 14 states have a comprehensive EMS commu-nications plan in place.11
Where we want to be Each call for emergency medical care is received by per-
sonnel with the requisite combination of education, expe-rience, and resources necessary to enable them to determine
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 5 9
Figure 2.Public access to an appropriate EMS response.

the most effective course of action. All callers to EMS receiveappropriate medically directed dispatch life support. EMScommunication networks incorporate other health careproviders and community services. These networks allowEMS workers to receive and share data with others who haveimportant information about their patients and clients.Additionally, EMS communication systems ensure reliableavailability of on-line medical direction and enable trans-mission of relevant real-time patient data. Networks are geo-graphically integrated and based on functional need to enablereliable communications among EMS, fire, law enforcement,and other public safety agencies. Issues related to disasterpreparedness are addressed, and each state maintains anup-to-date communications plan.
C L I N I C A L C A R E
Where we are The clinical care delivered by EMS has evolved signifi-
cantly over the past 30 years. To some extent it has capital-ized on the availability of new pharmacologic agents andtechnology, developed the means to deliver life-saving carefaster, and begun to systematically address the particularneeds of specific groups of patients. However, EMS systemsvary dramatically with regard to the sophistication of carethey provide. There is no standard baseline of care that isprovided by all systems, and the scope of EMS care differsamong states and often between localities. The interventionsEMTs can perform, the equipment available to them, andthe medications they carry varies greatly.68,69 In some areas,EMS clinical care variations may be the result of adaptingto meet the health care needs of communities. A project atRed River, NM, is an example of such adaptation in a ruralcommunity.70 However, the effectiveness of EMS care hasbeen established for few clinical problems.
Regardless of its sophistication, EMS care is usually in-tended to get patients to a hospital. Transportation of patientsto nonemergency facilities or between facilities may beaccomplished by EMS providers or ambulance services oper-ating outside the EMS system.
Where we want to be EMS provides a defined baseline of care and services in
all communities. Expansion of services occurs in responseto identified community health care needs. Out-of-hospitalEMS care is optimal for patients’ circumstances, so that itpositively influences outcomes. The effects of EMS are prop-erly and continually evaluated. Technologic and pharmaceuti-cal advances are evaluated in terms of their appropriatenessand effectiveness before their widespread deployment inEMS systems.
Patient transport activities are integrated with the over-all health care system. EMS is capable of facilitating accessto hospital emergency departments and other health careresources designated by medical direction. Staffing patternsfor interfacility or secondary transports match the potentialcare required for specific types of patients. The responsibilityand authority for medical direction during these transportsis clear.
I N F O R M A T I O N S Y S T E M S
Where we are Several initiatives have focused on the need for develop-
ment of improved techniques for collecting EMS-relateddata. The Trauma Care Systems and Planning Act of 1990emphasized the need for collection of data for the evaluationof emergency care for serious injuries.71 The 1993 Instituteof Medicine report “Emergency Medical Services for Chil-dren” recommended that states collect and analyze uniformEMS data needed for planning, evaluation, and research ofEMS for children.72 During the 1993 Uniform Pre-HospitalEmergency Medical Services Data Conference, confereesdiscussed potential data elements and determined them tobe essential or desirable.73,74
The data required to completely describe an EMS eventexist in separate disparate locations. These include EMSagencies, hospital records, public safety agencies, and vitalstatistics offices. In most cases, meaningful linkages betweensuch sites are nonexistent. The lack of organized informa-tion systems that provide data which are valid, reliable, andaccurate is a significant barrier to conducting EMS systemevaluation, including outcomes analysis.10,75 Lack of infor-mation systems that are integrated with EMS and otherhealth care providers and community resources limits theability to share useful data. Research efforts are also hindered.For example, integrated information systems may serve asmultisource databases, which have been advocated as usefultools for conducting EMS cardiac arrest research.76
Where we want to be EMS shares integrated information systems with other
health care providers, public safety agencies, and commu-nity resources. They provide mechanisms for EMS to trans-mit and receive useful information. The data necessary todescribe entire EMS events are available within informationsystems that link multiple source databases. These informa-tion systems incorporate uniform data elements, facilitatingcontinuous EMS evaluation, even across multiple EMS sys-tems, and supporting EMS-related research.
E M S A G E N D ADelbridge et al
2 6 0 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8
E V A L U A T I O N
Where we are Evaluation is the process of assessing the quality and
effects of EMS, so that strategies for continuous improve-ment can be designed and implemented. EMS systems areevaluated using structural (input), process, and outcomemeasures. Because long-term patient outcomes may be in-sensitive to variation in EMS care, intermediate outcomesthat have a closer temporal relationship to EMS care oftenare utilized.77 Cardiac arrest and trauma are widely used as“tracer” conditions to determine the overall effects of EMSsystems.78-80 For other conditions, there is a paucity ofliterature evaluating the effects of EMS. Estimates of EMScosts for saving the life of a cardiac arrest victim are similarto those for other life saving treatments.81,82 However, suchestimates are locality specific and do not necessarily apply
to all EMS systems. Models for determining EMS effective-ness and cost-effectiveness are lacking.
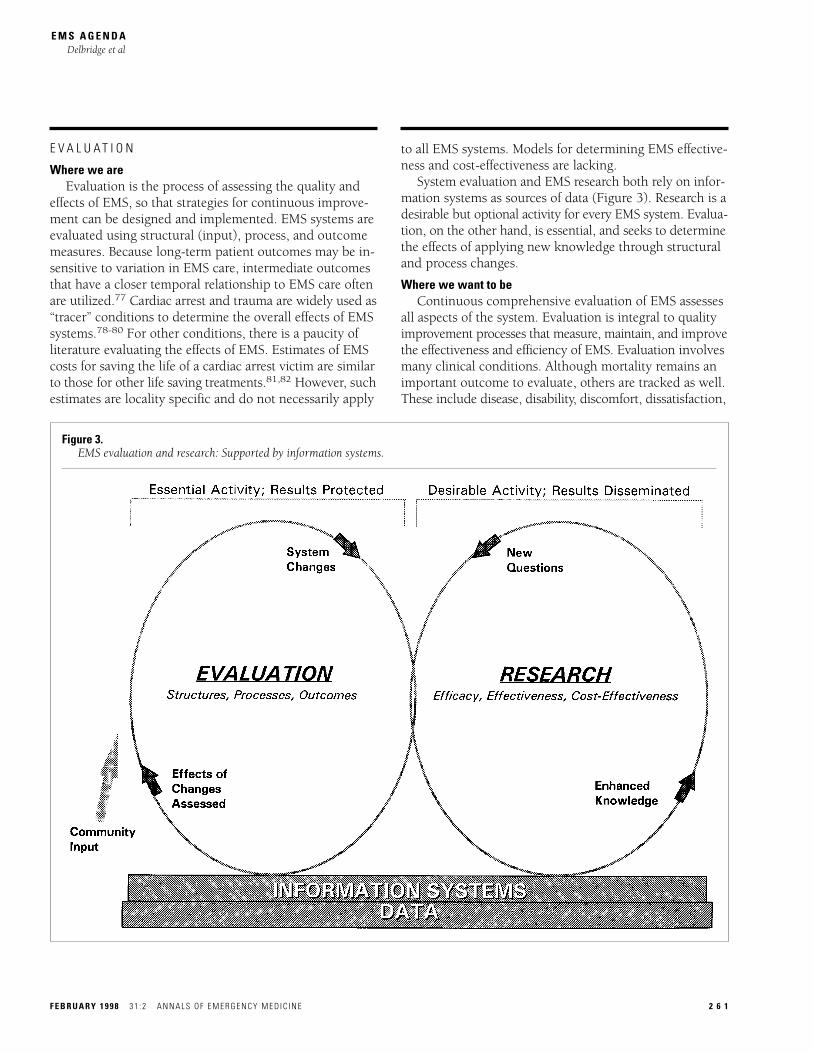
System evaluation and EMS research both rely on infor-mation systems as sources of data (Figure 3). Research is adesirable but optional activity for every EMS system. Evalua-tion, on the other hand, is essential, and seeks to determinethe effects of applying new knowledge through structuraland process changes.
Where we want to be Continuous comprehensive evaluation of EMS assesses
all aspects of the system. Evaluation is integral to qualityimprovement processes that measure, maintain, and improvethe effectiveness and efficiency of EMS. Evaluation involvesmany clinical conditions. Although mortality remains animportant outcome to evaluate, others are tracked as well.These include disease, disability, discomfort, dissatisfaction,
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 6 1
Figure 3.EMS evaluation and research: Supported by information systems.

and destitution.83 Public satisfaction and consumer inputis a focus of EMS evaluation efforts. The cost-effectivenessof EMS is also evaluated. This includes the cost-effectivenessof system preparedness and relates to various injury andillness conditions.
I M P L I C A T I O N S F O R T H E F U T U R E
The “EMS Agenda for the Future” project sought and re-ceived input from a large group of individuals and organiza-tions with interests in EMS. Despite the group’s heterogeneity,common themes pervaded the process. This facilitated iden-tification of areas appropriate for future EMS development.
Our collective EMS experience over the last 30 years pro-vides a foundation on which to create the future. As we lookforward, it is clear that EMS must be integrated with otherservices intended to maintain and improve communityhealth and ensure its safety. The special needs of membersof our diverse society must be recognized and addressed.We must also focus on aspects of EMS that improve itsscience, strengthen its infrastructure, and broaden its involve-ment in enhancing the health of our communities. Addition-ally, the value of EMS as the public’s emergency medicalsafety net cannot be neglected. Most importantly, the abilityto achieve the vision for the future of EMS will depend onthe development of new partnerships within the health caresystem and commitments to improve the emergency healthcare system.
The “EMS Agenda for the Future” represents an effort tolook toward the future from a specific point in time. Ameri-can society and the health care system are dynamic. Thusfrequent evaluation of where we are and where we want tobe is essential to ensure that EMS fulfills its critical role inoptimally caring for the health of Americans.
R E F E R E N C E S1. National Academy of Sciences, National Research Council: Accidental Death and Disability:The Neglected Disease of Modern Society. Washington DC: National Academy Press, 1966.
2. Perry S, Wilkinson SL: The technology assessment practice guidelines forum: A modified groupjudgement method. Int J Tech Assess in Health Care 1992;8:289-300.
3. Gerson LW, Hoover R, McCoy S, et al: Linking the elderly to community services. JEMS 1991;16:45-48.
4. Gerson LW, Schelble DT, Wilson JE: Using paramedics to identify at-risk elderly. Ann EmergMed 1992;21:688-691.
5. Krumperman KM: Filling the gap: EMS social service referrals. JEMS 1993;18:25-29.
6. Hsiao AK, Hedges JR: Role of the emergency medical services system in region wide healthmonitoring and referral. Ann Emerg Med 1993;22:1696-1702.
7. Cummins RO, Ornato JP, Thies WH, et al: Improving survival from sudden cardiac arrest: Thechain of survival concept: A statement for health professionals from the Advanced Cardiac LifeSupport Subcommittee and the Emergency Cardiac Care Committee, American Heart Association.Circulation 1991;83:1832-1847.
8. Newman MM: Chain of survival takes hold. JEMS 1989;14:11-13.
9. Spaite DW, Criss EA, Valenzuela TD, et al: Emergency medical service systems research:Problems of the past, challenges of the future. Ann Emerg Med 1995;26:146-152.
10. Spaite DW, Valenzuela TD, Meislin HW: Barriers to EMS system evaluation: Problems associ-ated with field data collection. Prehosp Disaster Med 1993;8(suppl):S35-S40.
11. Snyder JA, Baren JM, Ryan SD, et al: Emergency medical service system development: Resultsof the statewide emergency medical service technical assessment program. Ann Emerg Med1995;25:768-775.
12. Maiava D, director, Hawaii Emergency Medical Services: Personal communication, February1996.
13. National Emergency Medical Services Education and Practice Blueprint. Columbus, OH:National Registry of Emergency Medical Technicians, 1993.
14. McNally VP: A history of the volunteers. Fire House 1986;11:49-53.
15. Fitch JJ: Volunteers. In Kuehl AE (ed): Prehospital Systems and Medical Oversight, ed 2. StLouis: Mosby–Year Book, 1994:316-320.
16. Mitchell JT: Critical incident stress management. In Kuehl AE (ed): Prehospital Systems andMedical Oversight, ed 2. St Louis: Mosby–Year Book, 1994:339-344.
17. Mitchell J, Bray G: Emergency Services Stress: Guidelines for Preserving the Health andCareers of Emergency Personnel. Englewood Cliffs, NJ: Brady Publishing-Prentice Hall, 1990.
18. Hockreiter MC, Barton LL: Epidemiology of needlestick injury in emergency medical servicepersonnel. J Emerg Med 1988;6:9-12.
19. Reed E, Daya MR, Jui J, et al: Occupational infectious disease exposures in EMS personnel.J Emerg Med 1993;11:9-16.
20. Menegazzi JJ: A meta-analysis of hepatitis B serologic marking prevalence in EMS personnel.Prehosp Disaster Med 1991;6:299-302.
21. Garza M: Paramedics report many on-duty assaults. EMS Insider 1993;20:7.
22. Gershon RRM, Vlahov D, Kelen G, et al: Review of accidents/injuries among emergency medi-cal services workers in Baltimore, Maryland. Prehosp Disaster Med 1995;10:14-18.
23. Hogya PT, Ellis L: Evaluation of the profile of personnel in a busy urban EMS system. Am JEmerg Med 1990;8:308-311.
24. Schwartz RJ, Benson L, Jacobs LM: The prevalence of occupational injuries in EMTs in NewEngland. Prehosp Disaster Med 1993;8:45-50.
25. Emergency Medical Technician: Basic, National Standard Curriculum. Washington DC: USDepartment of Transportation, National Highway Traffic Safety Administration, 1994.
26. Swor RA, Chisolm C, Krohmer J: Model curriculum in emergency medical services for emer-gency medicine residencies. Ann Emerg Med 1989;18:418-421.
27. Erder MH, Davidson SJ, Chaney RA: On-line medical command in theory and practice. AnnEmerg Med 1989;18:261-288.
28. Gratton MC, Bethkey RA, Watson WA, et al: Effect of standing orders on paramedic scenetime for trauma patients. Ann Emerg Med 1991;20:52-55.
29. Hunt RC, Bass RR, Graham RG, et al: Standing orders vs. voice control. JEMS 1982;7:26-31.
30. Pointer JE, Osur MA: Effect of standing orders on field times. Ann Emerg Med 1989;18:1119-1121.
31. Hoffman JR, Luo J, Schriger DL, et al: Does paramedic base hospital contact result in beneficialdeviations from standard prehospital protocols? West J Med 1989;153:283-287.
32. Thompson SJ, Schriber JA: A survey of prehospital care paramedic/physician communicationfrom Multnomah County (Portland), Oregon. J Emerg Med 1984;1:421-428.
33. Wuerz RC, Swope GE, Holliman CJ, et al: On-line medical direction: A prospective study.Prehosp Disaster Med 1995;10:174-177.
34. The Future of EMS Education: A National Perspective. Washington DC: Joint Review-Committee on Educational Programs for the EMT Paramedic, 1994.
35. Polk DA, Langford SJ: EMS degree programs. JEMS 1992;17:69-75.
36. Anderson TE, Arthur K, Kleinman M, et al: Intraosseous infusion: Success of a standardizedregional training program for prehospital advanced life support providers. Ann Emerg Med 1994;23:52-55.
37. Cayten CG, Staroccik R, Walker K, et al: Impact of prehospital cardiac algorithms on ventricu-lar fibrillation survival rates. Ann Emerg Med 1981;10:432-436.
38. Fuchs S, LaCovey D, Paris P: A prehospital model of intraossesous infusion. Ann Emerg Med1991;20:371-374.
E M S A G E N D ADelbridge et al
2 6 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 3 1 : 2 F E B R U A R Y 1 9 9 8

39. Landis SS, Benson NH, Whitley TW: A comparison of four methods of testing emergencymedical technician triage skills. Am J Emerg Med 1989;7:1-4.
40. Losek JD, Szewczuga D, Glaeser PW: Improved prehospital pediatric ALS care after an EMT-Paramedic clinical training course. Am J Emerg Med 1994;12:429-432.
41. Powell JP: Training for EMT/Paramedics in perinatal care and transport. J Tenn Med Assoc1982;75:133-134.
42. Trooskin SZ, Rubinowicz S, Eldridge C, et al: Teaching endotracheal intubation with animalsand cadavers. Prehosp Disaster Med 1992;7:179-184.
43. Walters G, D'Auria D, Glucksman E: Automatic external defibrillators: Implications for train-ing qualified ambulance staff. Ann Emerg Med 1992;21:692-697.
44. Werman HA, Keseg DR, Glimcher M: Retention of Basic life support skills. Prehosp DisasterMed 1990;5:137-144.
45. Feely HB, Athey JL: Emergency Medical Services for Children: Ten-Year Report. Arlington,VA: National Center for Education in Maternal and Child Health, 1995.
46. Ho MT, Eisenberg MS, Litwin PE, et al: Delay between onset of chest pain and seeking medi-cal care: The effect of public education. Ann Emerg Med 1989;18:727-731.
47. Moses HW, Engelking N, Taylor GJ, et al: Effect of a two year public education campaign onreducing response time of patients with symptoms of acute myocardial infarction. Am J Cardiol1991;68:249-251.
48. Martinez R: Injury prevention: A new perspective. JAMA 1994;19:1541-1542.
49. Garrison HG, Foltin G, Becker L, et al: The role of emergency medical services in primary injuryprevention. Prehospital Emergency Care 1997;1:156-162.
50. MacLean CB: The future role of emergency medical services systems in prevention. AnnEmerg Med 1993;22:1743-1746.
51. Sklar D, Sapien R, Olson L, Monahan C: EMTs and Injury Prevention, Advocates for Children.Albuquerque: New Mexico EMS-C Project, 1995.
52. Harrawood D, Gunderson MR, Fravel S, et al: Drowning prevention: A case study in EMS epi-demiology. JEMS 1995;19:34-41.
53. Ogden JR, Criss EA, Spaite DW, et al: The impact of an EMS-initiated, community-baseddrowning prevention coalition on submersion deaths in a southwestern metropolitan area. AcadEmerg Med 1994;1:304.
54. Safe communities: An approach to reduce traffic injuries [discussion paper]. Washington DC:National Highway Traffic Safety Administration, September 24, 1995.
55. Rosenberg M: Program briefing to Dr. David Satcher, director, Centers for Disease Controland Prevention. Atlanta, GA: Centers for Disease Control and Prevention, March 13, 1996.
56. Lumpe D: Calling 911: Who will answer? Emerg Med News 1993;April:10-13.
57. National Heart Attack Alert Program Coordinating Committee Access to Care Subcommittee:9-1-1: Rapid identification and treatment of acute myocardial infarction. Am J Emerg Med 1995;13:188-195.
58. Cady G, Scott T: EMS in the United States 1995 Survey of providers in the 200 most populouscities. JEMS 1995;20:76-82.
59. Eisenberg M, Hallstrom A, Becker L: Community awareness of emergency phone numbers.Am J Publ Health 1981;71:1058-1060.
60. ASTM Committee F-30 on Emergency Medical Services: ASTM Standards on EmergencyMedical Services. Philadelphia, PA: ASTM, 1994.
61. Clawson JJ: Emergency medical dispatch. In Kuehl AE (ed): Prehospital Systems and MedicalOversight, ed 2. St Louis: Mosby–Year Book, 1994:125-152.
62. Clawson JJ: Emergency medical dispatch. In Roush WR (ed): Principles of EMS Systems.Dallas, TX: ACEP, 1994:263-289.
63. Emergency Medical Dispatch National Standard Curriculum: Instructor’s Guide. WashingtonDC: National Highway Traffic Safety Administration, 1996.
64. National Association of EMS Physicians: Emergency medical dispatching. Prehosp DisasterMed 1989;4:163-166.
65. Stratton SJ: Triage by emergency medical dispatchers. Prehosp Disaster Med 1992;7:263-268.
66. Clark JJ, Culley L, Eisenberg M, et al: Accuracy of determining cardiac arrest by emergencymedical dispatchers. Ann Emerg Med 1994;23:1022-1026.
67. Valenzuela T, Spaite D, Clark D, et al: Estimated cost-effectiveness of dispatcher CPR instruc-tion via telephone to bystanders during out-of-hospital ventricular fibrillation. Prehosp DisasterMed 1992;7:229-234.
68. Delbridge TR, Verdile VP, Platt TE: Variability of state-approved emergency medical servicesdrug formularies. Prehosp Disaster Med 1994;9(suppl 2):S55.
69. Garrison HG, Benson NH, Whitley TW, et al: Paramedic skills and medications: Practiceoptions utilized by local advanced life support medical directors. Prehosp Disaster Med 1991;6:29-33.
70. Senate Joint Memorial #44: Expanded-EMS Study. Albuquerque, NM: New Mexico Departmentof Health, Emergency Medical Services Bureau, 1995.
71. Trauma Care Systems Training and Development Act of 1990: Public Law 101-590. WashingtonDC: 1990.
72. Durch JS, Lohr KN (eds): Emergency Medical Services for Children. Washington DC: NationalAcademy Press, 1993.
73. Uniform Pre-hospital Emergency Medical Services (EMS) Data Conference: Final Report.Washington DC: National Highway Traffic Safety Administration, 1994.
74. Spaite D, Benoit R, Brown W, et al: Uniform prehospital data elements and definitions: Areport from the uniform prehospital emergency medical services data conference. Ann EmergMed 1995;25:525-534.
75. EMS Outcomes Evaluation: Key Issues and Future Directions. Proceedings from the NHTSAWorkshop on Methodologies for Measuring Morbidity Outcomes in EMS. Washington DC: NationalHighway Traffic Safety Administration, April 11-12, 1994.
76. Hedges JR: Beyond Utstein: Implementation of a multisource uniform database for prehospitalcardiac arrest research. Ann Emerg Med 1993;22:41-46.
77. Cayten CG: Evaluation. In Kuehl AE (ed): Prehospital Systems and Medical Oversight, ed 2. StLouis: Mosby–Year Book, 1994:158-167.
78. Eisenberg MS, Horwood BT, Cummins RO: Cardiac arrest and resuscitation: A tale of 29 cities.Ann Emerg Med 1990;19:179-186.
79. American College of Surgeons Committee on Trauma: Quality assessment and assurance intrauma care. Bull Am Coll Surg 1986;71:4-23.
80. Shackford SR, Mackersie RC, Hoyt DB, et al: Impact of a trauma system on outcome ofseverely injured patients. Arch Surg 1987;122:523-527.
81. Urban N, Bergner L, Eisenberg MS: The costs of the suburban paramedic program in reducingdeaths due to cardiac arrest. Med Care 1981;19:379-392.
82. Valenzuela TD, Criss EA, Spaite D, et al: Cost-effectiveness analysis of paramedic emergencymedical services in the treatment of prehospital cardiopulmonary arrest. Ann Emerg Med 1990;19:1407-1411.
83. Fletcher RH, Fletcher SW, Wagner EH: Clinical Epidemiology: The Essentials. Baltimore, MD:Williams & Wilkins, 1988.
We gratefully acknowledge the support and guidance of Dr Ricardo Martinez and DrJean Athey, the research assistance of Dr Thomas Auble, the direction by KathleenStage-Kern, the administrative skills of Gina Baker, and the assistance of all thosewho participated during the process of creating the “EMS Agenda for the Future.”
Reprint no. 47/1/88099Reprints not available from the authors.
E M S A G E N D ADelbridge et al
F E B R U A R Y 1 9 9 8 3 1 : 2 A N N A L S O F E M E R G E N C Y M E D I C I N E 2 6 3
![EmS: PS-10 · information from EMS providers nationwide. As one EMS leader pointed out: “There is an illusion that EMS is so safe now - [we] have forgotten how inherently dangerous](https://img.pdfslide.us/doc/110x75/5f0c9c0f7e708231d43641ad/ems-ps-10-information-from-ems-providers-nationwide-as-one-ems-leader-pointed.jpg)




























