Embed Size (px)
Citation preview

EMPOWERING MINORITY POPULATIONS TO BETTER HEALTH
BY: BRICIA SANTOYO SENIOR UCF SPORTS AND EXERCISE SCIENCE STUDENT MINOR IN EDUCATION


What is Diversity? Diversity: Refers to the variety of backgrounds and characteristics found among humankind; thus it embraces all aspects of human similarities and differences.
WE ARE ALL UNIQUE
Age
Religion
Ethnicity (Race?)
National Origin (language)
Gender
Education
Educational Status
Mobility (including handicaps)
Source: (diversity.ucf.edu/diversity_definition).

Limited English Proficiency (LEP): Person who is unable to communicate effectively in English, their primary language is not English and they have not developed fluency in the English language.
Culture: Includes values, beliefs, standards, language, thinking patterns, behavioral norms, communications styles, etc.
Cultural Competence: A set of congruent behaviors, practices, attitudes and policies that come together in a system or agency or among professionals, enabling effective work to be done in cross-cultural situations.
Meaningful Access: The ability to use services and benefits comparable to those enjoyed by members of the mainstream cultures. It is achieved by eliminating communication barriers and ensuring that the client or potential client can communicate effectively.
Cultural Sensitivity: Is a set of skills that enables you to learn about and get to know people who are different from you, thereby coming to understand how to serve them better within their own communities.
Terminology

The growth of cultural diversity in the United States is creating more Language Barriers.
How do language barriers affect health care, Access, Quality of Care, Cost.
What is the government doing to help, Laws and Policies.
What are the resources we use to help, Interpreters, and Translated Documentation.
How can Cultural Competence aid professionals, more Awareness, and Knowledge .
Issues involving language barriers and cultural diversity

THE UNITED STATES: ONE OF THE MOST DIVERSE COUNTRIES
▪ “Plurality Nation”: Referring to a group of candidates where none has an absolute majority over the others (Nancee Hunter, National Geographic Society writer).
▪ A multitude of anything.
▪ “We’re on our way to becoming the first country in history that is literally made up of every part of the world.” - Kenneth Prewitt

How many languages are spoken in the United States?
2006–2008 US Census Bureau and Census Bureau American Community Survey
(ACS) listed over 300 languages spoken in the United States (Migration Policy Institute
[MIP]).
Even more if we consider dialects

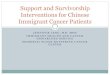
Top Ten Languages Spoken In the United States Language Population
English 230,947,071
Spanish 37,579,787
Chinese 2,882,497
Tagalog 1,594,413
Vietnamese 1,419,539
French 1,301,443
Korean 1,141,277
German 1,083,637
Arabic 951,699
Russian 905,843
Source: U.S. Census Bureau (census.gov)

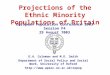
ENGLISH-SPEAKING ABILITY

Top Six States with the Highest LEP Populations
Source: http://www.migrationpolicy.org/

http://www.youtube.com/watch?v=R2NcwrPZBLMEXAMPLE SENARIO

TRANSLATION SERVICES COST MONEY & THERE ARE INADEQUATE LEVELS OF FUNDING
▪ Lack of Awareness on Funding Availability
▪ Tight Budgets (State/ County)
▪ Population Dependent (All based on needs)
Health Care Facilities should have access to the following:
▪ Interpreting Staff
▪ Telephone services that interpret callers
▪ Contract Interpreters
▪ Translated documentation/ Paperwork
Source:(www.gih.org)

LITTLE PUBLIC SUPPORT FOR THE AFFECTED MINORITIES
▪ Some people can feel uncomfortable with the growth of Diversity
▪ Some people can feel uncomfortable around people who do not speak English
▪ Lack of knowledge/ don’t know what steps to take to help
▪ New Issue (1990-now)
Health Care Facilities should have access to the following:
▪ Trained Staff
▪ Assessment of needs based on the different populations
▪ Develop polices to guide employees
▪ Monitor current policies and make sure they are effective
Source:(www.gih.org)

Federal Civil Rights Policy
Title VI of the Civil Rights Act of 1964
Executive Order (EO) 13166, Improving
Access toServices for Persons with Limited English
Proficiency
CLAS Standards
Some more specific laws and policies vary by state
THE LAWS AND POLICIES THAT ELIMINATE LANGUAGE
BARRIERS
Source:(www.gih.org)

TITLE VI OF THE CIVIL RIGHTS ACT OF 1964
“No person in the United States shall,on the ground of race, color, ornational origin, be excluded fromparticipation in, be denied the benefitsof, or be subjected to discriminationunder any program or activity receiving federal financial assistance”. Source: (justice.gov/crt/about/cor/coord/titlevi.php).

EXECUTIVE ORDER (EO) 13166
Helped create standards
• "Improving Access to Services for Persons with Limited English Proficiency“.
• “Requires Federal agencies to examine the services they
provide, identify any need for services to those with limited English proficiency (LEP), and develop and implement a system to provide those services so LEP persons can have meaningful access to them”.
Source: lep.gov/13166/eo13166.html

The National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care (CLAS
Standards)
A framework for all health care organizations to best serve the nation’s increasingly diverse communities.
1. CULTURALLY COMPETENT HEALTH CARE2. STAFF DIVERSITY3. STAFF EDUCATION AND TRAINING4. QUALFIED LANGUAGE ASSISTANCE SERVICES5. NOTICES TO PATIENTS/CONSUMERS OF THE RIGHT TO LANGUAGE
ASSISTANCE SERVICES6. QUALIFICATIONS FOR BILINGUAL AND INTERPRETER SERVICES7. TRANSLATED MATERIALS8. ORGANIZATIONAL FRAMEWORK FOR CULTURAL COMPETENCE9. ORGANIZATIONAL SELF-ASSESSMENT10. COLLECTION OF DATA ON INDIVIDUAL PATIENTS/CONSUMERS11. COLLECTION OF DATA ON COMMUNITIES12. COMMUNITY PARTNERSHIPS FOR CLAS13. COMPLAINT AND GRIEVANCE RESOLUTION14. INFORMATION FOR THE PUBLIC

INCREASED CASES OF MEDICAL MALPRACTICE DUE TO LANGUAGE BARRIERS
▪ Affect the delivery of adequate care through poor exchange of information
▪ Loss of important cultural information
▪ Misunderstanding of physician instruction
▪ Poor shared decision-making or ethical compromises
▪ Difficulty obtaining informed consent (Poor Documentation regarding Patient info. )
▪ Discrimination is usually claimed along with medical malpractice
Children or family members used as interpreter versus competent Interpreters

Examples of medical malpractice cases 1. Patients Having to Interpret while getting treated (minors/ underage) 2. Allergy Documentation ignored/ patient was unable to tell the physician 3. Overdose due to lack of an interpreter
Study: The High Costs of Language Barriers in Medical MalpracticeWe will discuss three examples from this study.

How can we prepare ourselves as professionals to better serve all of our patients?
Negative Positive

THE CULTURAL COMPETENCE CONTINUUM
▪ Cultural Destructiveness: forced assimilation, subjugation, rights and privileges for dominant groups only
▪ Cultural Incapacity: racism, maintain stereotypes, unfair hiring practices
▪ Cultural Blindness: differences ignored, “treat everyone the same”, only meet needs of dominant groups
Source: (Sockalingum adapted from Hayes, Cultural Competence Continuum, 1993 and Terry Cross Cultural Competency Continuum).
▪ Cultural Pre-competence: explore cultural issues, are committed, assess needs of organization and individuals
▪ Cultural Competence: recognize individual and cultural differences, seek advice from diverse groups, hire culturally unbiased staff
▪ Cultural proficiency: implement changes to improve services based upon cultural needs, do research and teach
Developed to better understand the developmental process of cultural competence on the individual and organization levels

KNOWLEDGE IS POWER FOR THE SUCCESS OF PROFESSIONALS DEALING WITH LANGUAGE BARRIERS
AND CULTURAL DIVERSITY
Acquiring Cultural Competence
• Starts with Awareness• Grows with Knowledge• Is Enhanced with Specific Skills (Cultural Sensitivity)• Using Resources

WHAT ABOUT ISSUES IN SPORTS MEDICINE CAUSED BY LANGUAGE
AND CULTURE BARRIERS? • Culture: Family, community, and personalization. For Example church plays an important
role. • Leisure time: Minority populations might work more than one job or work longer hours
due to the level of jobs they have. (Unprofessional) • Youth: Some may not have parental support to engage in sport and exercise activities due
to the responsibilities at home, or they may have jobs to help the house hold income. • Income: Growing but still lower than the whites, some reasons maybe the lack of
professional jobs these populations hold. Many families will only have one parent bringing in income.
• Language: Can create misunderstanding and lack of knowledge if information is not presented in the native language.
A research study done by: UCLA Anderson School of Management Applied Management Research Program

STRATEGIES HEALTH AND WELLNESS PROFESSIONALS CAN USE WHEN WORKING WITH
MINORITY POPULATIONS?• Be aware of the rapid growth of minority populations.
• For Example: Approximately 1 out of 8 Americans is of Hispanic origin (International Health, Racquet & Sportsclubs Association [IHRSA 2003]).
• Family in the Hispanic culture is very important, offering family orientated activities can increase participation in physical activity.
• Community and friends are also important to this population, having a designated spokesman person can be beneficial.
• Tailor to the needs of the population, some Hispanics might be discouraged by the use of electronic funds transfer and prefer cash methods.
• Offer and develop programs in which each population can relate too. For example, LatinCadio a new workout dance that consist of Latin music and dancing moves.
• Strong nutrition education is needed, selection of ingredients, how foods are prepared, the timing and context of meals, size of portions are all dependent of culture

NEW OPPORTUNITIES WITH MINORITY POPULATION
Let’s take advantage. Let’s not be afraid to work with other populations.

QUESTIONS?

ReferencesAdams, Laura , Kafi Baskerville, Dorothy Lee Lee, and Michael Spruiell . "The Hispanic Community and Outdoor Recreation." http://www.outdoorfoundation.org. Outdoor Industry Foundation, 22 Mar. 2014. Web. 1 Feb. 2014. <http://www.outdoorfoundation.org/pdf/HispanicsOutdoorRecreation.pdf>.
Bau, I., Avery, M. B., Dickson, P., Grainger-Monsen, M., Green, C., & Hernandez, T. (2003, August 1). IN THE RIGHT WORDS: Addressing Language and Culture in Providing Health Care. www.gih.org. Retrieved February 19, 2014, from http://www.gih.org/usr_doc/in_the_right_words_issue_brief.pdf
PERKINS, J. (1999, August 1). Overcoming Language Barriers to Health Care. sogpubs.unc.edu. Retrieved February 20, 2014, from http://sogpubs.unc.edu//electronicversions/pg/f99-3844.pdf?
Quan, K. (2010, January 1). The High Costs of Language Barriers in Medical Malpractice. Publications - National Health Law Program. Retrieved February 20, 2014, from http://www.healthlaw.org/publications/the-high-costs-of-language-barriers-in-medical-malpractice#.UwW-SPldV8E
UCLA. (n.d.). UCLA. Retrieved February 20, 2014, from http://hr.healthcare.ucla.edu/ Putsch III RW. Cross-cultural communication: The special case of interpreters in health care. JAMA 1985;254(23):3344-48
Sockalingum adapted from Hayes, Cultural Competence Continuum, 1993 and Terry Cross Cultural Competency Continuum.
"We're in!." Office of Minority Health. N.p., n.d. Web. 3 Feb. 2014. <http://minorityhealth.hhs.gov/>. APA formatting by BibMe.org.