Embed Size (px)
Citation preview

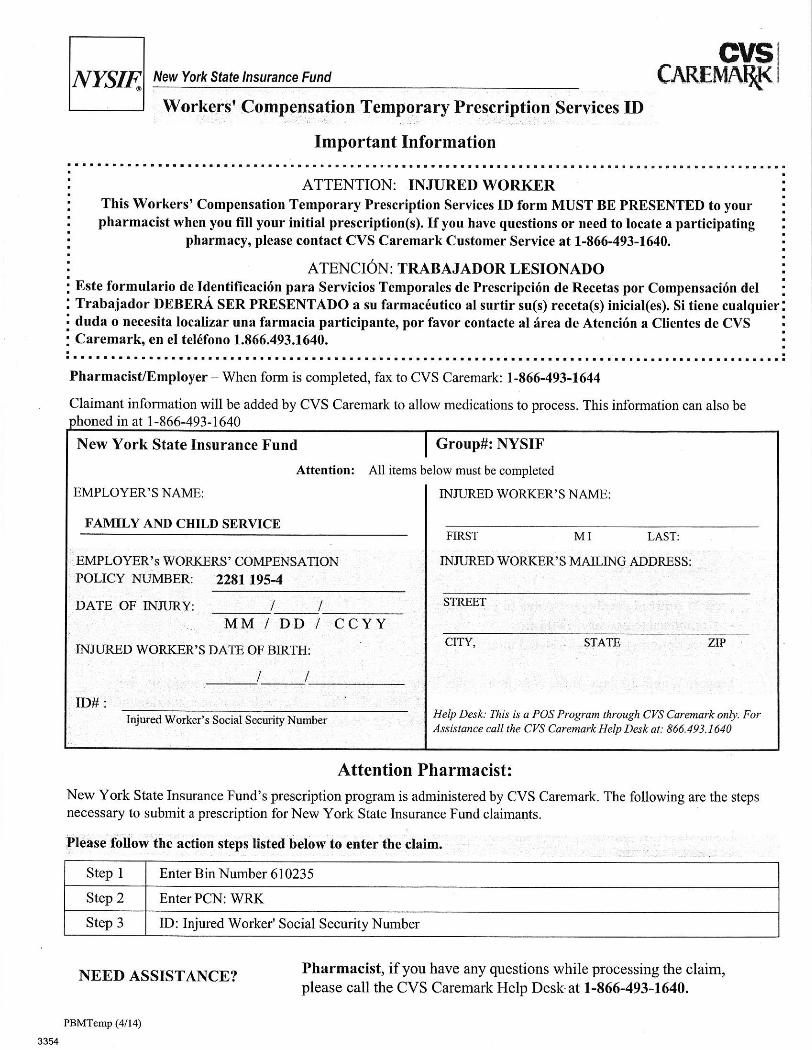
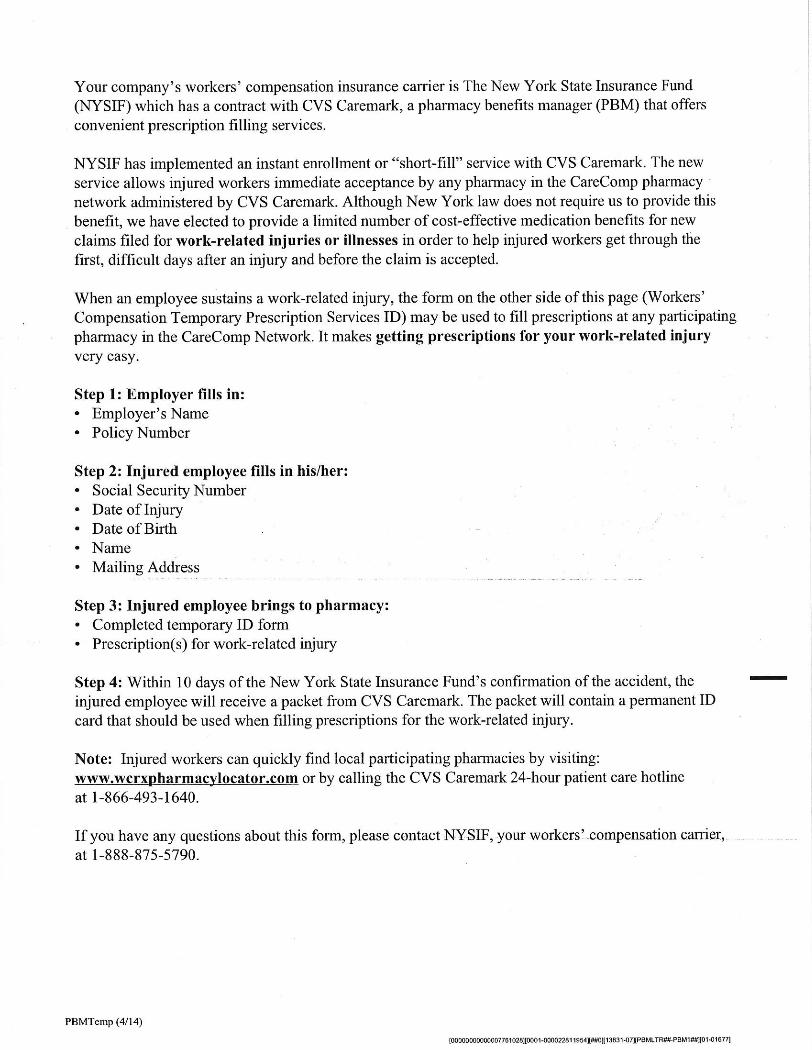
EMPLOYEE PACKET FOR WORKMAN’S COMP This packet contains information for you for your claim of injury while working. Please notify your supervisor as soon as possible after being injured. Please fill out the C-3 form as completely as possible and give a copy to your supervisor. If you need to go to a medical facility there is a list of doctors and facilities that are certified by the Workman Comp Board for treatment. You may use any doctor or facility that you want that accepts payment from WC. This list is for your information. The packet also has a notice with the billing information that the doctor or facility will need to bill for treatment. There is also a temporary prescription card to use if you are prescribed any medication. The last page is for you to fill out and return to your supervisor. If you have any questions, please contact your supervisor.

Tell the employer or supervisor about the injury as soon as possible. Failureto notify the employer, in writing, within 30 days after the accident datecan result in denial of benefits. In case of occupational disease, theclaimant must give notice to the employer within two years of thedisablement, or within two years after the claimant knew or should haveknown that the disease was work-related.
Obtain necessary medical treatment as soon as possible. An injured workermay choose any physician or medical provider authorized by the Workers’Compensation Board (WCB) to provide medical care. Additionally:
An injured worker should not pay a fee directly to the doctor ormedical provider.If the claim is disputed by NYSIF or the employer, the medicalprovider may require the patient to sign a form guaranteeingpayment for a disallowed claim.Follow doctor’s instructions to speed recovery.Follow up with your employer by providing specifics as to when youwill be able to return to work. Notify your employer of any changes inyour ability to work, or work status, as a result of the injury.When contacted by NYSIF, provide details pertaining to your injury,treatment and prognosis. This will speed up our ability to processpayments on your claim.Attend independent medical examinations (IME) when requested.Attend hearings when notified to appear.
M
THIS AGENCY EMPLOYS AND SERVES PEOPLE WITH DISABILITIES WITHOUT DISCRIMINATION
STATE OF NEW YORK WORKERS’ COMPENSATION BOARD
100 BROADWAY-MENANDS ALBANY, NY 12241
(877) 632-4996
You were injured at work. What now? The New York State Workers’ Compensation Board has received notice you suffered a workplace injury or illness, so we’re preparing a workers’ compensation case in your name. You may have already received medical treatment. If you haven’t, you should seek medical care as soon as possible.
A Worker’s Responsibilities You must tell your employer, in writing, when, where and how you were injured.
Do this within 30 days of injury. Medical reports are necessary for your case. Advise your doctors that you have a work-
related injury, and give the name of your employer. Do not pay for your care yourself or use other health insurance. Tell your doctor to file reports with the Board and with your employer or its insurance carrier. If your case is disputed, the Board needs a medical report on your injury to begin resolving your claim.
Starting a Case Once your employer knows of your injury, it must notify this Board by filing a C-2 form. You should file an employee claim (C-3 form) reporting your injury as soon as possible. (You must notify the Board of your injury or illness within two years.) If you injured the same body part before, or had a similar illness, you must also file a Form C-3.3. If you haven’t already filed a C-3 or C-3.3 (if necessary), there are three ways to do it. Visit www.wcb.state.ny.us/content/main/onthejob/howto.jsp to complete the form. Complete the enclosed paper forms, and mail them to the Board. Call 1-866-396-8314. A Board employee will complete the form with you.
Health Care Bills Do not pay your doctor or hospital. Those bills are paid by the insurer unless the Board disallows your case. If your case is disputed, the providers are paid when the Board decides your case. If the Board decides against you, or if you don’t pursue a case, you will have to pay the doctor or hospital.
Your employer’s insurance covers medically necessary drugs and equipment your doctor prescribes. You’re also entitled to carfare or necessary expenses incurred when traveling for treatment. (Get receipts for those expenses.)
Claimant Information Packet
NEW YORK STATE WORKERS' COMPENSATION BOARD
Generally, you can choose any doctor authorized by the Board. You can also use occupational health clinics. However, if your employer’s insurer has a preferred provider organization to provide care for workers' compensation injuries, you must get your initial treatment from those providers. If that insurer also has a pharmacy or diagnostic network, you must get service within these networks. If the carrier uses these networks, it must also tell you its service providers and how to use them.
Benefits for Lost Wages You are entitled to a portion of your lost wages if your injury affects you in one or more ways:
1. It keeps you from work for more than seven days; 2. Part of your body is permanently disabled; 3. Your pay is reduced because you now work fewer hours or do other work.
An employer or insurer can accept your claim and begin paying your lost wage benefit promptly. Sometimes, employers and carriers dispute a claim. When that occurs, the Board strives to resolve most cases within 90 days.
You may hire an attorney or licensed representative, who can be helpful with complex or disputed claims, but it isn’t required. The Board sets their fees and they will be deducted from your lost wages award. You or your family should not pay anything directly to your attorney or licensed representative.
If your case is disputed, you may receive disability benefits while the case is heard. You’d pay them back out of your lost wages award. To get a DB-450 form, visit www.wcb.state.ny.us/content/main/forms/db450.pdf or a Board office, or call (800) 353-3092.
Help is Available People sometimes need help getting back to work. Your employer may have a return to work program that can get you back to work in light duty or an alternative position while you heal. An injury can also cause family or financial problems. The Workers' Compensation Board has rehabilitation counselors and social workers to help. Call (877) 632-4996 for more assistance.
What’s Next? Your employer or its insurance carrier will contact you if your claim is accepted. When that happens, your treatment will be paid and lost wage benefits begin. If your case is challenged, the Board will notify you about resolving the case. If more information is necessary, the Board will contact you and tell you how to file it.
Important Contact Information Workers’ Compensation Board (877)632-4996 [email protected] Disability Benefits (800)353-3092 www.WCB.State.NY.US NYS Bar Association Lawyer Referral and Information Service
(800)342-3661 [email protected].
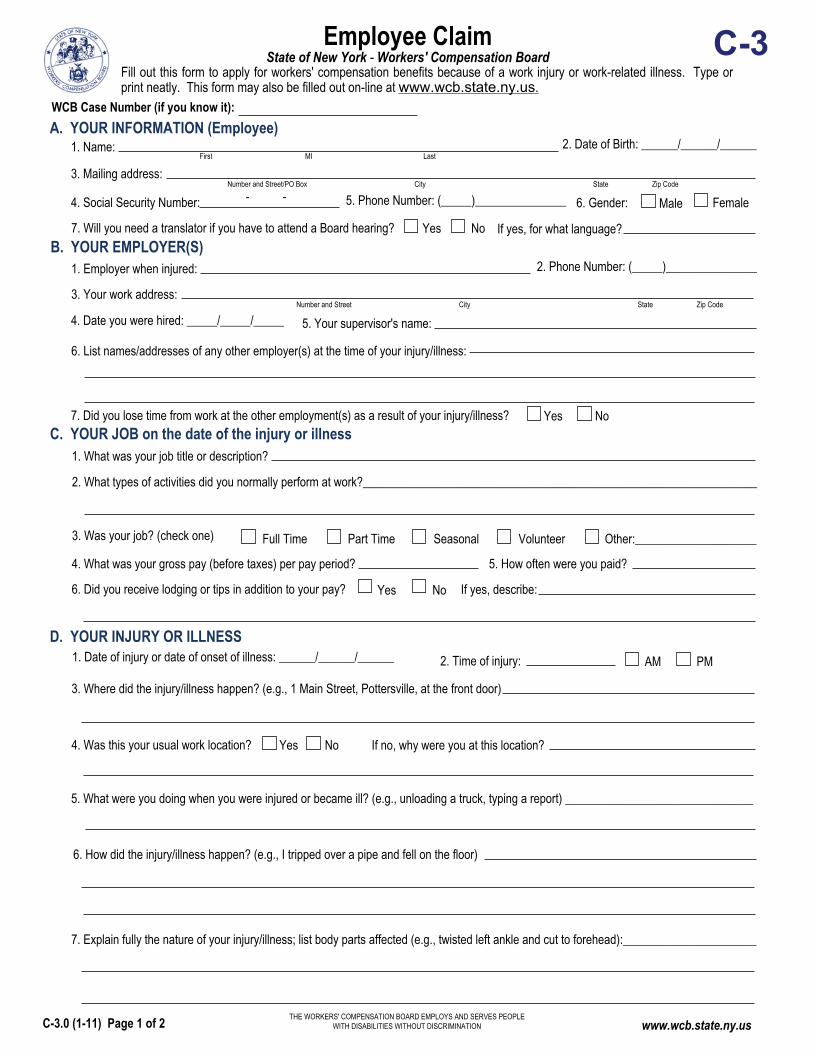
Employee Claim State of New York - Workers' Compensation Board
THE WORKERS' COMPENSATION BOARD EMPLOYS AND SERVES PEOPLE WITH DISABILITIES WITHOUT DISCRIMINATION
C-3
Number and Street City State Zip Code
B. YOUR EMPLOYER(S)1. Employer when injured:
3. Your work address:
6. List names/addresses of any other employer(s) at the time of your injury/illness:
7. Did you lose time from work at the other employment(s) as a result of your injury/illness? NoYes
Female
A. YOUR INFORMATION (Employee)1. Name:
3. Mailing address:
4. Social Security Number: 6. Gender: Male
C. YOUR JOB on the date of the injury or illness1. What was your job title or description?
2. What types of activities did you normally perform at work?_________________________________________________________________
3. Was your job? (check one) Full Time Part Time Seasonal Volunteer Other:____________________
4. What was your gross pay (before taxes) per pay period? 5. How often were you paid?
Yes 6. Did you receive lodging or tips in addition to your pay? If yes, describe:No
D. YOUR INJURY OR ILLNESS
3. Where did the injury/illness happen? (e.g., 1 Main Street, Pottersville, at the front door)
If no, why were you at this location? NoYes 4. Was this your usual work location?
5. What were you doing when you were injured or became ill? (e.g., unloading a truck, typing a report) _______________________________
WCB Case Number (if you know it):
Fill out this form to apply for workers' compensation benefits because of a work injury or work-related illness. Type or print neatly. This form may also be filled out on-line at www.wcb.state.ny.us.
Number and Street/PO Box City State Zip Code
7. Will you need a translator if you have to attend a Board hearing? Yes No If yes, for what language?
6. How did the injury/illness happen? (e.g., I tripped over a pipe and fell on the floor)
7. Explain fully the nature of your injury/illness; list body parts affected (e.g., twisted left ankle and cut to forehead):______________________
First MI Last
5. Your supervisor's name:
2. Date of Birth: ______/______/______
5. Phone Number: (_____)_______________
2. Phone Number: (_____)_______________
4. Date you were hired: _____/_____/_____
1. Date of injury or date of onset of illness: ______/______/______ AM PM2. Time of injury:
www.wcb.state.ny.usC-3.0 (1-11) Page 1 of 2
- -

No
No
D. YOUR INJURY OR ILLNESS continuedIf yes, what? NoYes 8. Was an object (e.g., forklift, hammer, acid) involved in the injury/illness?
9. Was the injury the result of the use or operation of a licensed motor vehicle? If yes, your vehicle employer's vehicle other vehicle License plate number (if known):
If your vehicle was involved, give name and address of your motor vehicle insurance carrier:
10. Have you given your employer (or supervisor) notice of injury/illness?
in writingorally If yes, notice was given to: ____________________________________
11. Did anyone see your injury happen? If yes, list names:________________________________________
F. MEDICAL TREATMENT FOR THIS INJURY OR ILLNESS None received (skip to question F-5)
3. Where did you receive your first off site medical treatment for your injury/illness? none received Doctor's office
Emergency RoomClinic/Hospital/Urgent Care Hospital Stay over 24 hours
Name and address where you were first treated:
4. Are you still being treated for this injury/illness? Give the name and address of the doctor(s) treating you for this injury/illness:
5. Do you remember having another injury to the same body part or a similar illness?
6. Was the previous injury/illness work related? If yes, were you working for the same employer that you work for now?
NoYes
NoYes
Yes
NoYes
No Yes
NoYesYes
An individual may sign on behalf of the employee only if he or she is legally authorized to do so and the employee is a minor, mentally incompetent or incapacitated.
I am hereby making a claim for benefits under the Workers' Compensation Law. My signature affirms that the information I am providing is true and accurate to the best of my knowledge and belief.
Employee's Signature: Print Name:On behalf of Employee: Print Name:
If yes, were you treated by a doctor? NoYes If yes, provide the names and addresses of the doctor(s) who treated you and COMPLETE AND FILE FORM C-3.3 TOGETHER WITH THIS FORM:
Any person who knowingly and with INTENT TO DEFRAUD presents, causes to be presented, or prepares with knowledge or belief that it will be presented to, or by an insurer, or self-insurer, any information containing any FALSE MATERIAL STATEMENT or conceals any material fact, SHALL BE GUILTY OF A CRIME and subject to substantial FINES AND IMPRISONMENT.
YOUR NAME:________________________________________________ DATE OF INJURY/ILLNESS: ______/______/______
Date notice given: _____/_____/_____
limited duty
E. RETURN TO WORK1. Did you stop work because of your injury/illness?
2. Have you returned to work? regular duty
3. If you have returned to work, who are you working for now? Same employer New employer Self employed
4. What is your gross pay (before taxes) per pay period? How often are you paid?
NoYes
NoYes
, on what date? _____/_____/_____ , skip to Section F.
If yes, on what date? _____/_____/_____
Date: _____/_____/_____
Date: _____/_____/_____
1. What was the date of your first treatment? ______/______/______2. Were you treated on site? Yes No
Phone Number: (_____)_______________
Phone Number: (_____)_______________
Unknown
First MI Last
C-3.0 (1-11) Page 2 of 2
I certify to the best of my knowledge, information and belief, formed after an inquiry reasonable under the circumstances, that the allegations and other factual matters asserted above have evidentiary support, or are likely to have evidentiary support after a reasonable opportunity for further investigations or discovery.
Signature of Attorney/Representative (if any):
Print Name: Title:
ID No., if any: R
Date: _______/_______/_______
If Licensed Representative, License No.: Expiration Date: _______/_______/_______

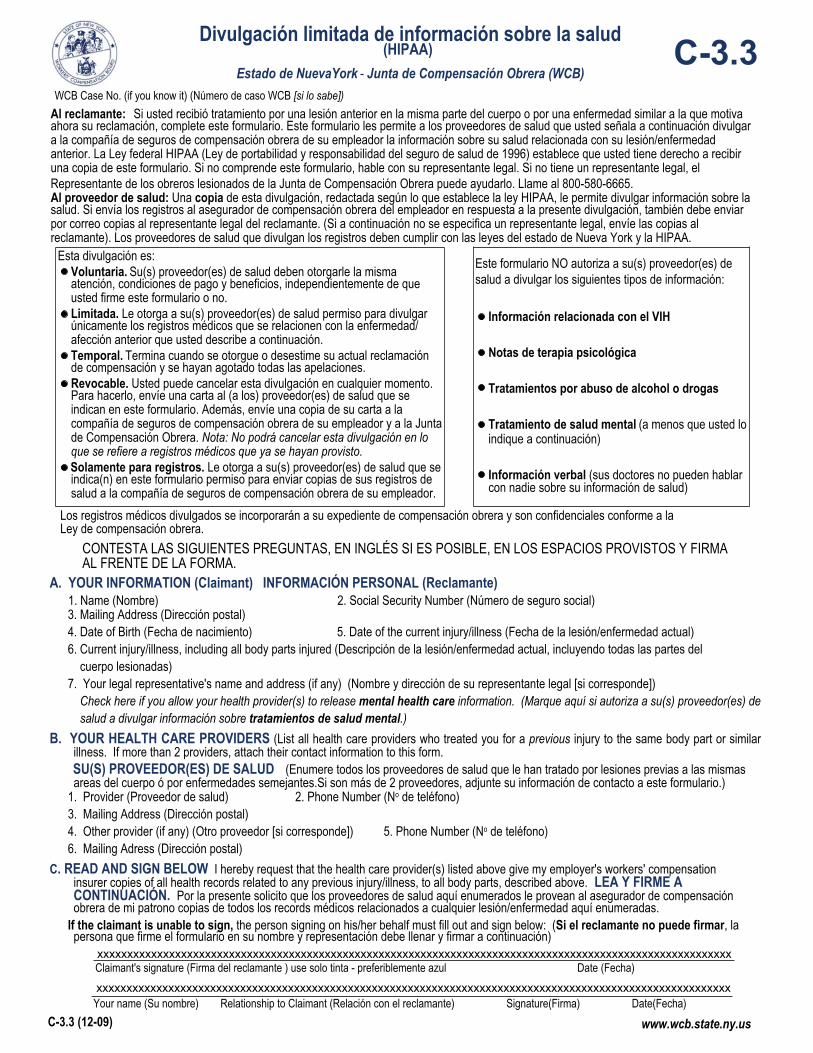
www.wcb.state.ny.usC-3.3 (12-09)
Limited Release of Health Information(HIPAA)
State of New York - Workers' Compensation BoardC-3.3
WCB Case No. (if you know it):___________________________To Claimant: If you received treatment for a previous injury to the same body part or for an illness similar to the one described in your currentClaim, fill out this form. This form allows the health care providers you list below to release health care information about your previous injury/illness to your employer's workers' compensation insurer. The federal HIPAA law (Health Insurance Portability and Accountability Act of 1996)says you have a right to get a copy of this form. If you do not understand this form, talk to your legal representative. If you do not have a legalrepresentative, the Advocate for Injured Workers at the Workers' Compensation Board can help you. Call: 800-580-6665.
To Health Care Provider: A copy of this HIPAA-compliant release allows you to disclose health information. If you send records to theemployer's workers' compensation insurer in response to this release, also mail copies to the Claimant's legal representative. (If no legalrepresentative is listed below, send copies to the Claimant.) Health care providers who release records must follow New York state law andHIPAA.
This release is:Voluntary. Your health care provider(s) must give you the same care,payment terms, and benefits, whether you sign this form or not.Limited. It gives your health care provider(s) permission to release onlythose health records that are related to the previous illness/condition youdescribe below.Temporary. It ends when your current claim for compensation is establishedor disallowed and all appeals are exhausted.Revocable. You can cancel this release at any time. To cancel, send a letterto the health care provider(s) listed on this form. Also, send a copy of yourletter to your employer's workers' compensation insurer and the Workers'Compensation Board. Note: You may not cancel this release with respect tomedical records already provided.
For records only. It gives your health care provider(s) listed on this formpermission to send copies of your health care records to your employer'sworkers' compensation insurer.
This form does NOT allow your health care provider(s)to release the following types of information:
HIV-related information
Psychotherapy notes
Alcohol/Drug treatment
Mental Health treatment (unless you check below)
Verbal information (your health care providers maynot discuss your health care information with anyone)
Any medical records released will become part of your workers' compensation file and are confidential under the Workers' Compensation Law.A. YOUR INFORMATION (Claimant) 1. Name:__________________________________________________________________ 2. Social Security Number:______-_____-______ 3. Mailing Address: _________________________________________________________________________________________________ 4. Date of Birth: ______/______/______ 5. Date of the current injury/illness: ______/_______/_______ 6. Current injury/illness, including all body parts injured:_____________________________________________________________________ ______________________________________________________________________________________________________________ 7. Your legal representative's name and address (if any):___________________________________________________________________ ______________________________________________________________________________________________________________ Check here if you allow your health care provider(s) to release mental health care information.
B. YOUR HEALTH CARE PROVIDER(S) (List all health care providers who treated you for a previous injury to the same body part or similarillness. If more than 2 providers attach their contact information to this form.)
1. Provider:__________________________________________________________________ 2. Phone Number: (______)_______________ 3. Mailing Address: _________________________________________________________________________________________________ 4. Other provider (if any):_______________________________________________________ 5. Phone Number: (______)_______________ 6. Mailing Address:_________________________________________________________________________________________________C. READ AND SIGN BELOW. I hereby request that the health care provider(s) listed above give my employer's workers' compensation
insurer copies of all health records related to any previous injury/illness, to all body parts, described above.
____________________________________________________________________________________________________________
If the claimant is unable to sign, the person signing on his/her behalf must fill out and sign below:
______________________________________________________________________________________________________________
Claimant's signature (ink only -- use blue ballpoint pen, if possible.) Date
Your name Relationship to Claimant Signature (ink only -- use blue ballpoint pen, if possible.) Date
Versión en español al reverso de la forma.
www.wcb.state.ny.usC-3.3 (12-09)
WCB Case No. (if you know it) (Número de caso WCB [si lo sabe])
Divulgación limitada de información sobre la salud(HIPAA)
Estado de NuevaYork - Junta de Compensación Obrera (WCB)C-3.3
Al reclamante: Si usted recibió tratamiento por una lesión anterior en la misma parte del cuerpo o por una enfermedad similar a la que motivaahora su reclamación, complete este formulario. Este formulario les permite a los proveedores de salud que usted señala a continuación divulgara la compañía de seguros de compensación obrera de su empleador la información sobre su salud relacionada con su lesión/enfermedadanterior. La Ley federal HIPAA (Ley de portabilidad y responsabilidad del seguro de salud de 1996) establece que usted tiene derecho a recibiruna copia de este formulario. Si no comprende este formulario, hable con su representante legal. Si no tiene un representante legal, elRepresentante de los obreros lesionados de la Junta de Compensación Obrera puede ayudarlo. Llame al 800-580-6665.Al proveedor de salud: Una copia de esta divulgación, redactada según lo que establece la ley HIPAA, le permite divulgar información sobre lasalud. Si envía los registros al asegurador de compensación obrera del empleador en respuesta a la presente divulgación, también debe enviarpor correo copias al representante legal del reclamante. (Si a continuación no se especifica un representante legal, envíe las copias alreclamante). Los proveedores de salud que divulgan los registros deben cumplir con las leyes del estado de Nueva York y la HIPAA.
Esta divulgación es:Voluntaria. Su(s) proveedor(es) de salud deben otorgarle la mismaatención, condiciones de pago y beneficios, independientemente de queusted firme este formulario o no.Limitada. Le otorga a su(s) proveedor(es) de salud permiso para divulgarúnicamente los registros médicos que se relacionen con la enfermedad/afección anterior que usted describe a continuación.Temporal. Termina cuando se otorgue o desestime su actual reclamaciónde compensación y se hayan agotado todas las apelaciones.Revocable. Usted puede cancelar esta divulgación en cualquier momento.Para hacerlo, envíe una carta al (a los) proveedor(es) de salud que seindican en este formulario. Además, envíe una copia de su carta a lacompañía de seguros de compensación obrera de su empleador y a la Juntade Compensación Obrera. Nota: No podrá cancelar esta divulgación en loque se refiere a registros médicos que ya se hayan provisto.
Solamente para registros. Le otorga a su(s) proveedor(es) de salud que seindica(n) en este formulario permiso para enviar copias de sus registros desalud a la compañía de seguros de compensación obrera de su empleador.
Este formulario NO autoriza a su(s) proveedor(es) desalud a divulgar los siguientes tipos de información:
Información relacionada con el VIH
Notas de terapia psicológica
Tratamientos por abuso de alcohol o drogas
Tratamiento de salud mental (a menos que usted loindique a continuación)
Información verbal (sus doctores no pueden hablarcon nadie sobre su información de salud)
Los registros médicos divulgados se incorporarán a su expediente de compensación obrera y son confidenciales conforme a laLey de compensación obrera.
A. YOUR INFORMATION (Claimant) INFORMACIÓN PERSONAL (Reclamante) 1. Name (Nombre) 2. Social Security Number (Número de seguro social) 3. Mailing Address (Dirección postal) 4. Date of Birth (Fecha de nacimiento) 5. Date of the current injury/illness (Fecha de la lesión/enfermedad actual) 6. Current injury/illness, including all body parts injured (Descripción de la lesión/enfermedad actual, incluyendo todas las partes del cuerpo lesionadas) 7. Your legal representative's name and address (if any) (Nombre y dirección de su representante legal [si corresponde]) Check here if you allow your health provider(s) to release mental health care information. (Marque aquí si autoriza a su(s) proveedor(es) de salud a divulgar información sobre tratamientos de salud mental.)B. YOUR HEALTH CARE PROVIDERS (List all health care providers who treated you for a previous injury to the same body part or similar
illness. If more than 2 providers, attach their contact information to this form. SU(S) PROVEEDOR(ES) DE SALUD (Enumere todos los proveedores de salud que le han tratado por lesiones previas a las mismas
areas del cuerpo ó por enfermedades semejantes.Si son más de 2 proveedores, adjunte su información de contacto a este formulario.) 1. Provider (Proveedor de salud) 2. Phone Number (No de teléfono) 3. Mailing Address (Dirección postal) 4. Other provider (if any) (Otro proveedor [si corresponde]) 5. Phone Number (No de teléfono) 6. Mailing Adress (Dirección postal)C. READ AND SIGN BELOW I hereby request that the health care provider(s) listed above give my employer's workers' compensation
insurer copies of all health records related to any previous injury/illness, to all body parts, described above. LEA Y FIRME ACONTINUACIÓN. Por la presente solicito que los proveedores de salud aquí enumerados le provean al asegurador de compensaciónobrera de mi patrono copias de todos los records médicos relacionados a cualquier lesión/enfermedad aquí enumeradas.
If the claimant is unable to sign, the person signing on his/her behalf must fill out and sign below: (Si el reclamante no puede firmar, lapersona que firme el formulario en su nombre y representación debe llenar y firmar a continuación)
Claimant's signature (Firma del reclamante ) use solo tinta - preferiblemente azul Date (Fecha)
Your name (Su nombre) Relationship to Claimant (Relación con el reclamante) Signature(Firma) Date(Fecha)
CONTESTA LAS SIGUIENTES PREGUNTAS, EN INGLÉS SI ES POSIBLE, EN LOS ESPACIOS PROVISTOS Y FIRMAAL FRENTE DE LA FORMA.
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
C-3.0 (1-11)
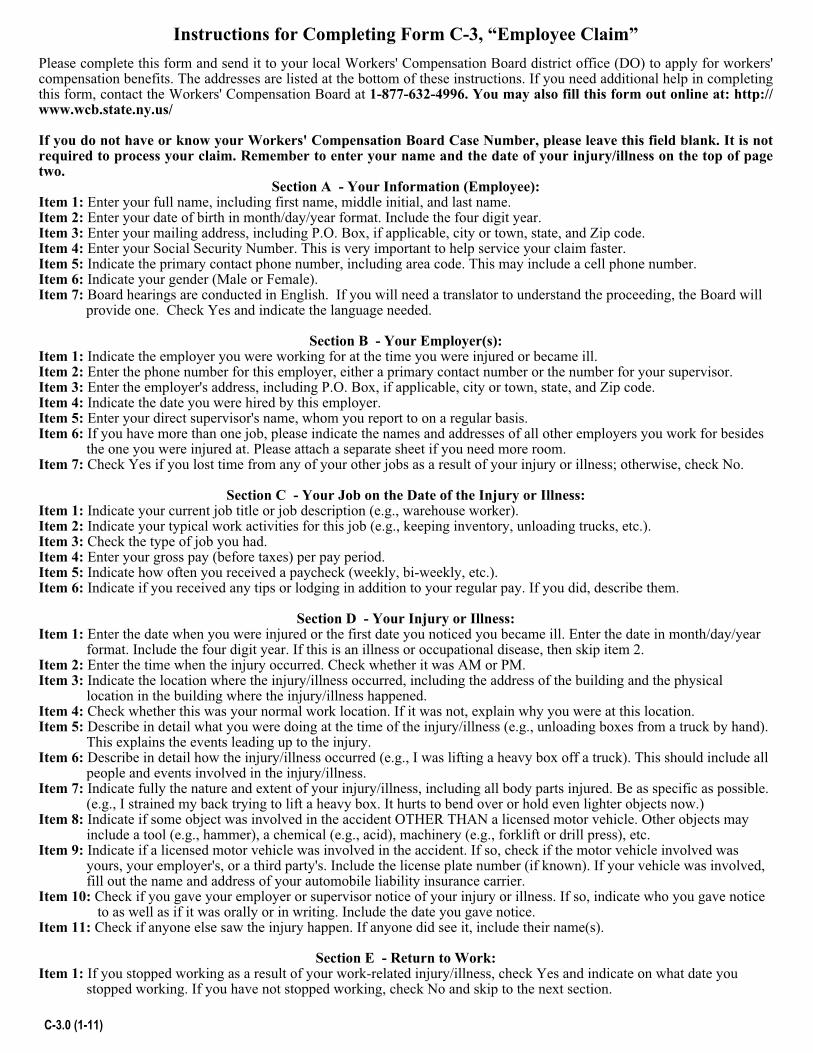
Instructions for Completing Form C-3, “Employee Claim”
Please complete this form and send it to your local Workers' Compensation Board district office (DO) to apply for workers' compensation benefits. The addresses are listed at the bottom of these instructions. If you need additional help in completing this form, contact the Workers' Compensation Board at 1-877-632-4996. You may also fill this form out online at: http://www.wcb.state.ny.us/
If you do not have or know your Workers' Compensation Board Case Number, please leave this field blank. It is not required to process your claim. Remember to enter your name and the date of your injury/illness on the top of page two.
Section A - Your Information (Employee): Item 1: Enter your full name, including first name, middle initial, and last name. Item 2: Enter your date of birth in month/day/year format. Include the four digit year. Item 3: Enter your mailing address, including P.O. Box, if applicable, city or town, state, and Zip code. Item 4: Enter your Social Security Number. This is very important to help service your claim faster. Item 5: Indicate the primary contact phone number, including area code. This may include a cell phone number. Item 6: Indicate your gender (Male or Female). Item 7: Board hearings are conducted in English. If you will need a translator to understand the proceeding, the Board will provide one. Check Yes and indicate the language needed.
Section B - Your Employer(s): Item 1: Indicate the employer you were working for at the time you were injured or became ill. Item 2: Enter the phone number for this employer, either a primary contact number or the number for your supervisor. Item 3: Enter the employer's address, including P.O. Box, if applicable, city or town, state, and Zip code. Item 4: Indicate the date you were hired by this employer. Item 5: Enter your direct supervisor's name, whom you report to on a regular basis. Item 6: If you have more than one job, please indicate the names and addresses of all other employers you work for besides
the one you were injured at. Please attach a separate sheet if you need more room. Item 7: Check Yes if you lost time from any of your other jobs as a result of your injury or illness; otherwise, check No.
Section C - Your Job on the Date of the Injury or Illness: Item 1: Indicate your current job title or job description (e.g., warehouse worker). Item 2: Indicate your typical work activities for this job (e.g., keeping inventory, unloading trucks, etc.). Item 3: Check the type of job you had. Item 4: Enter your gross pay (before taxes) per pay period. Item 5: Indicate how often you received a paycheck (weekly, bi-weekly, etc.). Item 6: Indicate if you received any tips or lodging in addition to your regular pay. If you did, describe them.
Section D - Your Injury or Illness: Item 1: Enter the date when you were injured or the first date you noticed you became ill. Enter the date in month/day/year format. Include the four digit year. If this is an illness or occupational disease, then skip item 2. Item 2: Enter the time when the injury occurred. Check whether it was AM or PM. Item 3: Indicate the location where the injury/illness occurred, including the address of the building and the physical
location in the building where the injury/illness happened. Item 4: Check whether this was your normal work location. If it was not, explain why you were at this location. Item 5: Describe in detail what you were doing at the time of the injury/illness (e.g., unloading boxes from a truck by hand).
This explains the events leading up to the injury. Item 6: Describe in detail how the injury/illness occurred (e.g., I was lifting a heavy box off a truck). This should include all
people and events involved in the injury/illness. Item 7: Indicate fully the nature and extent of your injury/illness, including all body parts injured. Be as specific as possible.
(e.g., I strained my back trying to lift a heavy box. It hurts to bend over or hold even lighter objects now.) Item 8: Indicate if some object was involved in the accident OTHER THAN a licensed motor vehicle. Other objects may
include a tool (e.g., hammer), a chemical (e.g., acid), machinery (e.g., forklift or drill press), etc. Item 9: Indicate if a licensed motor vehicle was involved in the accident. If so, check if the motor vehicle involved was yours, your employer's, or a third party's. Include the license plate number (if known). If your vehicle was involved, fill out the name and address of your automobile liability insurance carrier. Item 10: Check if you gave your employer or supervisor notice of your injury or illness. If so, indicate who you gave notice to as well as if it was orally or in writing. Include the date you gave notice. Item 11: Check if anyone else saw the injury happen. If anyone did see it, include their name(s).
Section E - Return to Work: Item 1: If you stopped working as a result of your work-related injury/illness, check Yes and indicate on what date you
stopped working. If you have not stopped working, check No and skip to the next section.
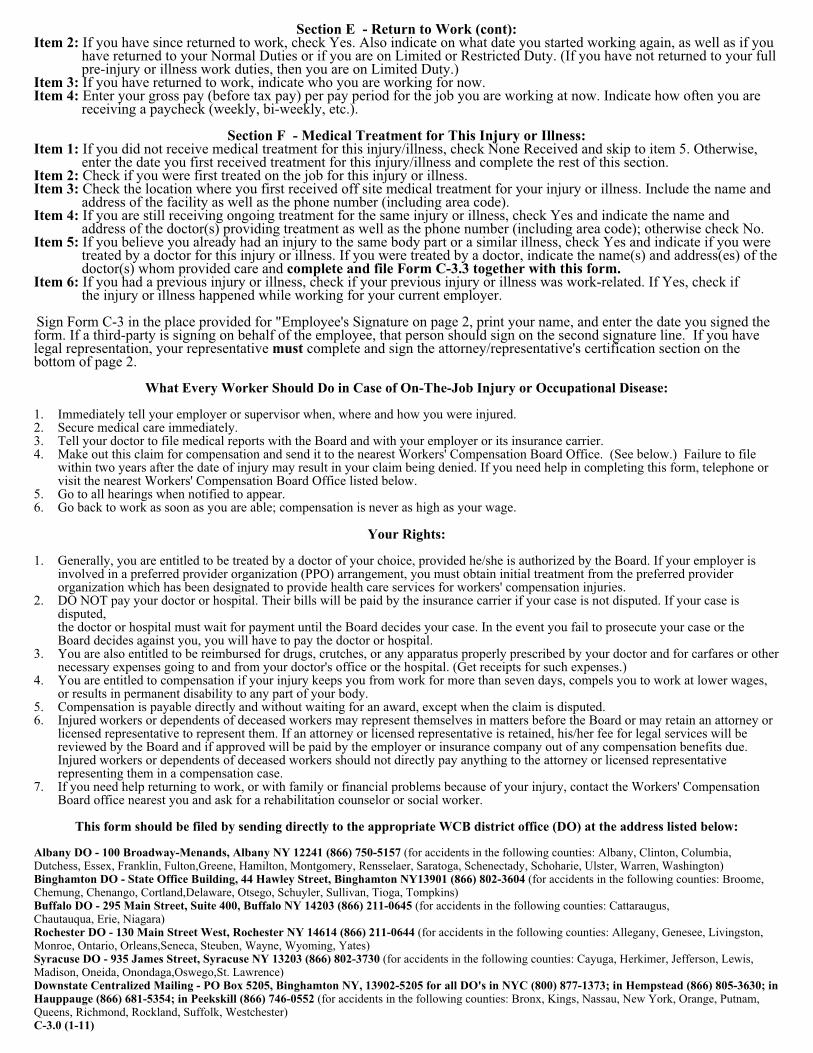
Section E - Return to Work (cont): Item 2: If you have since returned to work, check Yes. Also indicate on what date you started working again, as well as if you
have returned to your Normal Duties or if you are on Limited or Restricted Duty. (If you have not returned to your full pre-injury or illness work duties, then you are on Limited Duty.)
Item 3: If you have returned to work, indicate who you are working for now. Item 4: Enter your gross pay (before tax pay) per pay period for the job you are working at now. Indicate how often you are
receiving a paycheck (weekly, bi-weekly, etc.).
Section F - Medical Treatment for This Injury or Illness: Item 1: If you did not receive medical treatment for this injury/illness, check None Received and skip to item 5. Otherwise,
enter the date you first received treatment for this injury/illness and complete the rest of this section. Item 2: Check if you were first treated on the job for this injury or illness. Item 3: Check the location where you first received off site medical treatment for your injury or illness. Include the name and
address of the facility as well as the phone number (including area code). Item 4: If you are still receiving ongoing treatment for the same injury or illness, check Yes and indicate the name and
address of the doctor(s) providing treatment as well as the phone number (including area code); otherwise check No. Item 5: If you believe you already had an injury to the same body part or a similar illness, check Yes and indicate if you were
treated by a doctor for this injury or illness. If you were treated by a doctor, indicate the name(s) and address(es) of the doctor(s) whom provided care and complete and file Form C-3.3 together with this form.
Item 6: If you had a previous injury or illness, check if your previous injury or illness was work-related. If Yes, check if the injury or illness happened while working for your current employer.
Sign Form C-3 in the place provided for "Employee's Signature on page 2, print your name, and enter the date you signed the form. If a third-party is signing on behalf of the employee, that person should sign on the second signature line. If you have legal representation, your representative must complete and sign the attorney/representative's certification section on the bottom of page 2.
What Every Worker Should Do in Case of On-The-Job Injury or Occupational Disease:
1. Immediately tell your employer or supervisor when, where and how you were injured. 2. Secure medical care immediately. 3. Tell your doctor to file medical reports with the Board and with your employer or its insurance carrier. 4. Make out this claim for compensation and send it to the nearest Workers' Compensation Board Office. (See below.) Failure to file
within two years after the date of injury may result in your claim being denied. If you need help in completing this form, telephone or visit the nearest Workers' Compensation Board Office listed below.
5. Go to all hearings when notified to appear. 6. Go back to work as soon as you are able; compensation is never as high as your wage.
Your Rights:
1. Generally, you are entitled to be treated by a doctor of your choice, provided he/she is authorized by the Board. If your employer is involved in a preferred provider organization (PPO) arrangement, you must obtain initial treatment from the preferred provider organization which has been designated to provide health care services for workers' compensation injuries.
2. DO NOT pay your doctor or hospital. Their bills will be paid by the insurance carrier if your case is not disputed. If your case is disputed, the doctor or hospital must wait for payment until the Board decides your case. In the event you fail to prosecute your case or the Board decides against you, you will have to pay the doctor or hospital.
3. You are also entitled to be reimbursed for drugs, crutches, or any apparatus properly prescribed by your doctor and for carfares or other necessary expenses going to and from your doctor's office or the hospital. (Get receipts for such expenses.)
4. You are entitled to compensation if your injury keeps you from work for more than seven days, compels you to work at lower wages, or results in permanent disability to any part of your body.
5. Compensation is payable directly and without waiting for an award, except when the claim is disputed. 6. Injured workers or dependents of deceased workers may represent themselves in matters before the Board or may retain an attorney or
licensed representative to represent them. If an attorney or licensed representative is retained, his/her fee for legal services will be reviewed by the Board and if approved will be paid by the employer or insurance company out of any compensation benefits due. Injured workers or dependents of deceased workers should not directly pay anything to the attorney or licensed representative representing them in a compensation case.
7. If you need help returning to work, or with family or financial problems because of your injury, contact the Workers' Compensation Board office nearest you and ask for a rehabilitation counselor or social worker.
This form should be filed by sending directly to the appropriate WCB district office (DO) at the address listed below:
Albany DO - 100 Broadway-Menands, Albany NY 12241 (866) 750-5157 (for accidents in the following counties: Albany, Clinton, Columbia, Dutchess, Essex, Franklin, Fulton,Greene, Hamilton, Montgomery, Rensselaer, Saratoga, Schenectady, Schoharie, Ulster, Warren, Washington) Binghamton DO - State Office Building, 44 Hawley Street, Binghamton NY13901 (866) 802-3604 (for accidents in the following counties: Broome, Chemung, Chenango, Cortland,Delaware, Otsego, Schuyler, Sullivan, Tioga, Tompkins) Buffalo DO - 295 Main Street, Suite 400, Buffalo NY 14203 (866) 211-0645 (for accidents in the following counties: Cattaraugus, Chautauqua, Erie, Niagara) Rochester DO - 130 Main Street West, Rochester NY 14614 (866) 211-0644 (for accidents in the following counties: Allegany, Genesee, Livingston, Monroe, Ontario, Orleans,Seneca, Steuben, Wayne, Wyoming, Yates) Syracuse DO - 935 James Street, Syracuse NY 13203 (866) 802-3730 (for accidents in the following counties: Cayuga, Herkimer, Jefferson, Lewis, Madison, Oneida, Onondaga,Oswego,St. Lawrence) Downstate Centralized Mailing - PO Box 5205, Binghamton NY, 13902-5205 for all DO's in NYC (800) 877-1373; in Hempstead (866) 805-3630; in Hauppauge (866) 681-5354; in Peekskill (866) 746-0552 (for accidents in the following counties: Bronx, Kings, Nassau, New York, Orange, Putnam, Queens, Richmond, Rockland, Suffolk, Westchester) C-3.0 (1-11)

This Provider Directory is provided by Coventry Workers' Comp Services to present to you information on hospitals, physicians and other providers w ho have agreed to provide their usual services to you at specially
contracted rates of payment. All decisions about the type of care you receive are the responsibility of you and the physician whom you select. The quality and results of the care provided are the responsibility of the
physician. Some health services may be provided by resident physicians under the supervision of the listed physicians. While Conventry Workers' Comp Services make every effort to maintain accurate and up-to-date
information, we cannot be responsible for any omissions or errors after publication. Please confirm provider participation prior to your visit.
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
1 of 8 7/18/2013 9:59 AM

PROVIDER DIRECTORYPrepared For
NY 12305
Policy Number:2281195-4
IF EMERGENCY MEDICAL CARE IS NEEDED: Call 911, fire or police whenever emergency medical care isneeded. This directory is NOT intended to identify emergency medical providers.
The following pages are a directory of physicians and medical facilities for your use in obtaining workers'compensation medical care. The physicians and medical facilities listed in this directory are independent contractorsand are not the agents or employees of Coventry. The information identifying physicians and medical facilities isintended to assist you in directing the medical care of employees who have injuries or illnesses covered by theworkers' compensation system in accordance with state law.
We have endeavored to make the following information complete and accurate as of the date this directory ispublished. However, the status of providers changes, and new providers join our network. Accordingly, theinformation contained herein is subject to change without notice, and Coventry does not warrant the completeness oraccuracy of the information.
Privacy Policy | Contact UsFirst Health ® and the heart logo are registered services marks of First Health Group Corp.
The torch logo is a registered service mark of Coventry Health Care, Inc.
The informat ion herein is prot ec t ed propriet ar y informat ion of Covent r y Hea lt h Care Workers Compensat ion, Inc. Use of t his informat ion for anypur pose ot her t han for which it is p rovided is p rohib it ed .
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
2 of 8 7/18/2013 9:59 AM
Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
Airhienbuwa, Noghama, MDEllis HospitalInternal Medicine1101 Nott St InpatientPsychiatrySchenectady, NY 12308518-243-4000
Balasubramaniam, Nadarajah,MDEllis Pathology Assocs PcSchenectady PathologyAssociates PCFamily Practice1101 Nott StSchenectady, NY 12308518-243-4059, 518-372-4124
Balulad, Sujata, MDEllis HospitalFamily Practice1101 Nott StSchenectady, NY 12308518-243-4000
Jones-Assini, Carolyn Marie,MDEllis Neuro Science CenterInternal Medicine1101 Nott St InpatientPsychiatrySchenectady, NY 12308518-243-4178
Kessler, R. Blake, MDEllis Neuro Science CenterInternal Medicine1101 Nott St InpatientPsychiatrySchenectady, NY 12308518-243-4178
Kraev, Igor A., MDEllis Neuro Science CenterFamily Practice1101 Nott St Ste C5Schenectady, NY 12308518-243-1500
Phelps, David M., MDEllis Neuro Science CenterInternal Medicine1101 Nott StSchenectady, NY 12308518-243-4000
Schenectady Family HealthServices
(cont)Family Practice1044 State StSchenectady, NY 12307518-370-1441
Liebers, David M., MDEllis Hospital-InfectiousDiseaseInternal Medicine1204 Nott St Ste 304Schenectady, NY 12308518-243-4134
Voleti, Venkateswararao R.,MDKerry E YakawiakInternal Medicine700 McClellan St Ste 103 StClairs Medical Arts BldgSchenectady, NY 12304518-374-2525
Cospito, Peter D., DOCardiology Associates OfSchenectady PCInternal Medicine624 McClellan St Ste 201Schenectady, NY 12304518-382-7626
Ellis Family Health CenterFamily Practice624 McClellan StSchenectady, NY 12304518-382-2260
Ellis Health CenterOccupational Medicine Clinic600 McClellan StSchenectady, NY 12304518-382-2000
Ellis HospUrgent Care Clinic600 McClellan StSchenectady, NY 12304518-243-4000
Murphy, Christopher, MDEllis Family Health CenterFamily Practice624 McClellan St Ste 101Schenectady, NY 12304518-382-2260
Murphy, Suzanne M., MDEllis Pediatric Health Center
(cont)Family Practice624 McClellan St Suite 202Schenectady, NY 12304518-347-5113
Murphy, Suzanne M., MDEllis HospitalFamily Practice600 McClellan St Ste 202Schenectady, NY 12304518-382-2200
Petrillo, John M., DOEllis Family Health CenterFamily Practice624 McClellan St Suite 101Schenectady, NY 12304518-382-2260
Phelps, David M., MDEllis Residential &Rehabilitation CenterInternal Medicine600 McClellan StSchenectady, NY 12304518-382-2250
Reyes, Juanito, MDEllis HospitalFamily Practice624 McClellan St Ste 101Schenectady, NY 12304518-382-2290
Sapio, Nancy, MDEllis HospitalFamily Practice624 McClellan St Ste 101Schenectady, NY 12304518-382-2290
Vacca, William M., MDCardiology Associates OfSchenectady PCInternal Medicine624 McClellan St Ste 201Schenectady, NY 12304518-382-7626
Welch, Michael, MDEllis Family Health CenterFamily Practice624 McClellan St Ste 101Schenectady, NY 12304518-382-2260
Yee, Bong, MDBong K Yee Md
(cont)Internal Medicine1545 Chrisler AveSchenectady, NY 12303518-370-0010
Cohen, David P., MDDigestive Disease AssociatesOf SchInternal Medicine2147 Eastern PkwySchenectady, NY 12309518-382-1151
Litynski, James, MDDigestive Disease Associatesof SchenectadyInternal Medicine2147 Eastern PkwySchenectady, NY 12309518-382-1151
Reyes, Juanito, MDFive Corners Family PracticeFamily Practice361 Duanesburg RdSchenectady, NY 12306518-357-2011
Armenia, David C., MDCardiology Associates OfSchenectady PCInternal Medicine2546 Balltown Rd Ste 300Schenectady, NY 12309518-377-8184
Dworkin, Paul, MDCardiology Associates OfSchenectady PCInternal Medicine2546 Balltown Rd Ste 300Schenectady, NY 12309518-377-8184
Nolan, John A., MDCardiology Associates OfSchenectady PCInternal Medicine2546 Balltown Rd Ste 300Schenectady, NY 12309518-377-8184
Vassolas, George A., MDCardiology Associates OfSchenectady PCInternal Medicine2546 Balltown Rd Ste 300
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Page 1: 1.2 MI to 2.8 MI
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
3 of 8 7/18/2013 9:59 AM
Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
(cont)Schenectady, NY 12309518-377-8184
Goldberg, Steven M., MDCommunity Care PhysiciansInternal Medicine2121 River RdSchenectady, NY 12309518-381-9355
Weiner, Laurence A., MDCommunity Care PhysiciansInternal Medicine2121 River RdSchenectady, NY 12309518-381-9355
Chakraborty, Ranen K.,DOCommunity Care UrgentCare-NiskayunaFamily Practice2125 River Rd Ste 104Schenectady, NY 12309518-713-5341
Gupta, Saaket, MDNiskayuna Internal MedicineInternal Medicine2125 River Rd Ste 103Schenectady, NY 12309518-381-9355
Mirza, Shahida Parveen,MDCommunity Care FamilyMedicine-NiskayunaCommunity Care UrgentCare-NiskayunaFamily Practice2125 River Rd Ste 104Schenectady, NY 12309518-713-5341
Osborn, Kyle Thomas, MDCommunity Care UrgentCare-NiskayunaFamily Practice2125 River Rd Ste 104Schenectady, NY 12309518-713-5341
Parikh, Shirish, MDImage Care NiskayunaInternal Medicine2125 River Rd Ste 104Schenectady, NY 12309518-640-6775
Yoon, Edward B., MDNiskayuna Internal MedicineFamily Practice2125 River Rd Ste 103Schenectady, NY 12309518-381-9355
Yousuf, Asim, MDNiskayuna Internal MedicineInternal Medicine2125 River Rd Ste 103Schenectady, NY 12309518-381-9355
Welch, Michael, MDFamily Care NursePractitioner PCFamily Practice123 Saratoga Rd CollaboratingPhysician/MichaeSchenectady, NY 12302518-399-0200
Petersen, Lauris, MDLauris J Petersen MdFamily Practice15 Glenridge RdSchenectady, NY 12302518-399-0909
Schlossberg, Howard Robert,MDNew York OncologyHematologyPcInternal Medicine896 Riverview RdRexford, NY 12148518-399-4600
Silvers, Stewart A., MDNew York OncologyHematologyPcInternal Medicine896 Riverview RdRexford, NY 12148518-399-4600
Sukumaran, Sunitha, MDNew York OncologyHematologyPcInternal Medicine896 Riverview RdRexford, NY 12148518-399-4600
Tai, Muhammad Siddique,MDNew York OncologyHematologyPc
(cont)Internal Medicine896 Riverview RdRexford, NY 12148518-399-4600
Valentine, Elizabeth A., MDNew York OncologyHematologyPcInternal Medicine896 Riverview RdRexford, NY 12148518-399-4600
Glenville Healthcare CenterFamily Practice460 Saratoga RdScotia, NY 12302518-243-3360
Sun, Mina, MDSun Medical CareInternal Medicine463 Saratoga RdScotia, NY 12302518-399-2233
Borrelli, Karin E., MDSaratoga HospitalFamily Practice112 Charlton Rd ScotiaGlenville Family PhysiciansBallston Lake, NY 12019518-399-7723
Buff, Christopher, DOSaratoga HospitalFamily Practice112 Charlton Rd ScotiaGlenville Family PhysiciansBallston Lake, NY 12019518-399-7723
Ricker, Kerry, DOSaratoga HospitalFamily Practice112 Charlton Rd ScotiaGlenville Family PhysiciansBallston Lake, NY 12019518-399-7723
Kamath, Giridhar, DOSurya Immediate Medical CarePcFamily Practice1182 Troy Schenectady Rd SteLL01Latham, NY 12110
(cont)518-867-8080
Surya Immediate MedicalCarePCUrgent Care Clinic1182 Troy Schenectady Rd SteLL01Latham, NY 12110518-867-8080
Cohen, David Paul, MDDigestive Disease AssociatesOf SchInternal Medicine989 Route 146Clifton Park, NY 12065518-383-3576
Migden, Hedy L., MDAltamont Internal Medicine &PediatricsSt Peter`s Health PartnersMedical Associates PCInternal Medicine24 Madison Avenue ExtAlbany, NY 12203518-452-5447
Kumar, Arbind, MDArbind Kumar MdInternal Medicine531 Moe RdClifton Park, NY 12065518-271-9155
Arnold Jr., Hendrick K., MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065518-383-4198
Gradner, Jill A., MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065518-383-4198
Kronick, Gary A., MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Page 2: 2.8 MI to 8.2 MI
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
4 of 8 7/18/2013 9:59 AM

Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
(cont)518-383-4198
Parikh, Nita, MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065518-383-4198
Rios-Rivera, Zandra M.,MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065518-383-4198
Tumuluri, Srilaxmi, MDLatham Internal Medicine ofClifton ParkInternal Medicine2 Emma Ln Bldg 2, Ste 202Clifton Park, NY 12065518-383-4198
Argubano, Renee, MDSeton Health SystemFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Balsamo, Steven J., DOSeton Health System PrimaryCare Provider NetworkFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Boska, Robert, MDSeton Health System MediCareUrgenFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Carrozza, Joseph K., MDSeton Health System IncInternal Medicine1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Clifton Park Family
(cont)Occupational Medicine ClinicUrgent Care Clinic1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Craig, James C., MDSeton Health System PrimaryCare Provider NetworkFamily Practice1 Tallow Wood Dr Ste 8Clifton Park, NY 12065518-373-4500
Cunningham, Matthew,MDClifton Park Family HealthCare CenFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Gregorian, Antonio, MDSeton Health System IncFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500, 518-373-4555
Mabry, Paul, MDSeton Health SystemFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Medi CallUrgent Care Clinic1 Tallow Wood Dr Ste 2Clifton Park, NY 12065518-373-4444
Petersen, Lauris, MDSeton Health SystemFamily Practice1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Stracke, Carsten, MDSeton Health System IncFamily Practice1 Tallow Wood Dr Ste 2Clifton Park, NY 12065518-373-4555
Tawfik Guirguis, Youssef,MDSeton Health System
(cont)Internal Medicine1 Tallow Wood DrClifton Park, NY 12065518-373-4500
Diaz, Miguel R., MDThe Urological Institute ofNortheastern New YorkFamily Practice5 Southside Dr ste 204Clifton Park, NY 12065518-262-3341
Schnakenberg, Eric C., MDThe Urological Institute ofNortheastern New YorkFamily Practice5 Southside Dr ste 204Clifton Park, NY 12065518-262-3341
Concentra Medical CenterOccupational Medicine Clinic1971 Western AveAlbany, NY 12203518-452-2597
Pozniakas, James T., MDConcentra Medical CtrFamily PracticeOccupational Medicine1971 Western AveAlbany, NY 12203518-452-2597
US Medgroup of New York PAPCUrgent Care Clinic1971 Western AveAlbany, NY 12203518-452-2597
Armenia, David C., MDCardiology Associates OfSchenectady PCInternal Medicine103 Sitterly Rd Ste 2100Clifton Park, NY 12065518-383-9373
Mazzei Klokiw, Renata N., MDEllis Primary Care of CliftonParkFamily Practice103 Sitterly Rd Ste 2300Clifton Park, NY 12065518-579-2650
Nolan, John A., MDCardiology Associates OfSchenectady PCInternal Medicine103 Sitterly Rd Ste 2100Clifton Park, NY 12065518-383-9373
Platzman, Michael, DOEllis Medical Center ofClifton ParkFamily Practice103 Sitterly Rd Ste 1100Clifton Park, NY 12065518-579-2555
Kim, Jai, MDFamily Practice1 Abele DrClifton Park, NY 12065845-417-1060
Smith, Steven P., MDAlbany Advanced ImagingPLLCAlbany Radiology Assoc PcInternal Medicine648 Plank RdClifton Park, NY 12065518-688-1177
Carrelle, Raymond J., MDCommunity Care PhysiciansPCFamily Practice713 Troy Schenectady Rd Ste224Latham, NY 12110518-785-5881
Chakraborty, Ranen K., DOCommunity Care PhysiciansPCFamily Practice713 Troy Schenectady Rd Ste224Latham, NY 12110518-785-5881
Cleney, Holly K., MDCommunity Care PhysiciansPCFamily Practice713 Troy Schenectady Rd Ste224Latham, NY 12110518-785-5881
Gregorian, Antonio, MDSeton Health System IncFamily Practice713 Troy Schenectady RdSetonHealth Ob Gyn
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Page 3: 8.2 MI to 9.1 MI
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
5 of 8 7/18/2013 9:59 AM
Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
(cont)Latham, NY 12110518-786-6270
Stam, Katherine Lynn, DOWE Care at Community CareFamily Practice713 Troy Schenectady Rd Ste215Latham, NY 12110518-713-5347
Stetzer, Lee M., MDCommunity Care PhysiciansPcFamily Practice713 Troy Schenectady Rd Ste131Latham, NY 12110518-785-6565
Arnold Jr., Hendrick K.,MDLatham Internal MedicineInternal Medicine711 Troy Schenectady Rd Ste104Latham, NY 12110518-783-3110
Esposito, Russell J., DOUrgent Care Center of LathamFamily Practice711 Troy Schenectady Rd Ste102Latham, NY 12110518-783-3110
Kronick, Gary A., MDLatham Internal MedicineInternal Medicine711 Troy Schenectady Rd Ste104Latham, NY 12110518-783-3110
Parikh, Nita, MDLatham Internal MedicineInternal Medicine711 Troy Schenectady Rd Ste104Latham, NY 12110518-783-3110
Parikh, Shirish, MDImage Care LathamInternal Medicine711 Troy Schenectady Rd Ste114Latham, NY 12110
(cont)518-786-1600
Rios-Rivera, Zandra M.,MDLatham Internal MedicineInternal Medicine711 Troy Schenectady Rd Ste104Latham, NY 12110518-782-3700
Scialdone, Claude J., MDCommunity Care PhysiciansImage Care LathamInternal Medicine711 Troy Schenectady Rd Ste114Latham, NY 12110518-786-1600
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Page 4: 9.1 MI
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
6 of 8 7/18/2013 9:59 AM
Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
A
Airhienbuwa, Noghama, MD 0 Argubano, Renee, MD 3 Armenia, David C., MD 1,3 Arnold Jr., Hendrick K., MD 2,4
B
Balasubramaniam, Nadarajah, MD 1 Balsamo, Steven J., DO 3 Balulad, Sujata, MD 1 Borrelli, Karin E., MD 2 Boska, Robert, MD 3 Buff, Christopher, DO 2
C
Carrelle, Raymond J., MD 3 Carrozza, Joseph K., MD 3 Chakraborty, Ranen K., DO 2,3 Cleney, Holly K., MD 3 Clifton Park Family 3 Cohen, David P., MD 1 Cohen, David Paul, MD 2 Concentra Medical Center 3 Cospito, Peter D., DO 1 Craig, James C., MD 3 Cunningham, Matthew, MD 3
D
Diaz, Miguel R., MD 3 Dworkin, Paul, MD 1
E
Ellis Family Health Center 1 Ellis Health Center 1 Ellis Hosp 1 Esposito, Russell J., DO 4
G
Glenville Healthcare Center 2
Goldberg, Steven M., MD 2 Gradner, Jill A., MD 2 Gregorian, Antonio, MD 3 Gupta, Saaket, MD 2
J
Jones-Assini, Carolyn Marie, M 1
K
Kamath, Giridhar, DO 2 Kessler, R. Blake, MD 1 Kim, Jai, MD 3 Kraev, Igor A., MD 1 Kronick, Gary A., MD 2,4 Kumar, Arbind, MD 2
L
Liebers, David M., MD 1 Litynski, James, MD 1
M
Mabry, Paul, MD 3 Mazzei Klokiw, Renata N., MD 3 Medi Call 3 Migden, Hedy L., MD 2 Mirza, Shahida Parveen, MD 2 Murphy, Christopher, MD 1 Murphy, Suzanne M., MD 1
N
Nolan, John A., MD 1,3
O
Osborn, Kyle Thomas, MD 2
P
Parikh, Nita, MD 3,4
Parikh, Shirish, MD 2,4 Petersen, Lauris, MD 2,3 Petrillo, John M., DO 1 Phelps, David M., MD 1 Platzman, Michael, DO 3 Pozniakas, James T., MD 3
R
Reyes, Juanito, MD 1 Ricker, Kerry, DO 2 Rios-Rivera, Zandra M., MD 3,4
S
Sapio, Nancy, MD 1 Schenectady Family Health Serv 1 Schlossberg, Howard Robert, MD 2 Schnakenberg, Eric C., MD 3 Scialdone, Claude J., MD 4 Silvers, Stewart A., MD 2 Smith, Steven P., MD 3 Stam, Katherine Lynn, DO 4 Stetzer, Lee M., MD 4 Stracke, Carsten, MD 3 Sukumaran, Sunitha, MD 2 Sun, Mina, MD 2 Surya Immediate Medical Care P 2
T
Tai, Muhammad Siddique, MD 2 Tawfik Guirguis, Youssef, MD 3 Tumuluri, Srilaxmi, MD 3
U
US Medgroup of New York PA PC 3
V
Vacca, William M., MD 1 Valentine, Elizabeth A., MD 2 Vassolas, George A., MD 1 Voleti, Venkateswararao R., MD 1
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Index 1
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
7 of 8 7/18/2013 9:59 AM
Prov ider Lis ting Provider data last updated: 07/12/2013
Last Update: 07/12/2013
W
Weiner, Laurence A., MD 2 Welch, Michael, MD 1,2
Y
Yee, Bong, MD 1 Yoon, Edward B., MD 2 Yousuf, Asim, MD 2
^ = No New WCTHIS LIST IS SUBJECT TO CHANGE.
The information herein is protected proprietary information of Coventry. Use of this information for any purpose other than forwhich it is provided is prohibited.
Index 2
TalisPoint® * Provider Directory http://www-va.talispoint.com/talispoint/directory_default.pl
8 of 8 7/18/2013 9:59 AM
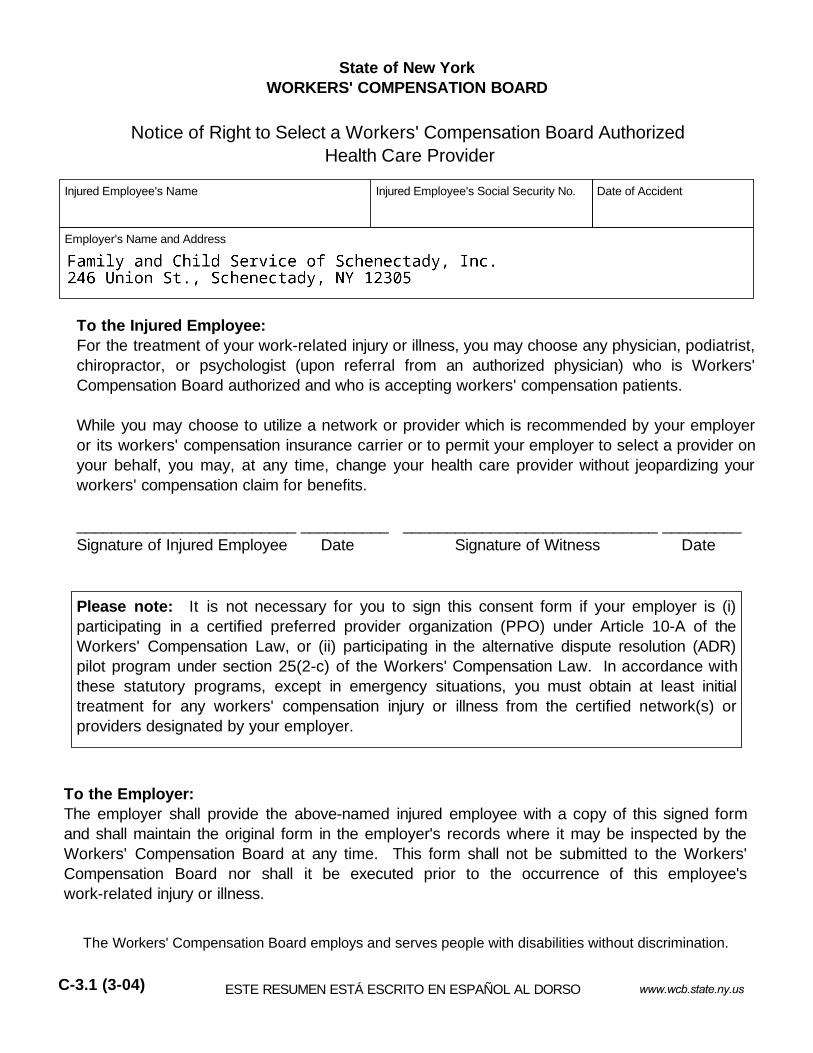
State of New YorkWORKERS' COMPENSATION BOARD
Notice of Right to Select a Workers' Compensation Board Authorized Health Care Provider
To the Injured Employee:For the treatment of your work-related injury or illness, you may choose any physician, podiatrist,chiropractor, or psychologist (upon referral from an authorized physician) who is Workers'Compensation Board authorized and who is accepting workers' compensation patients. While you may choose to utilize a network or provider which is recommended by your employeror its workers' compensation insurance carrier or to permit your employer to select a provider onyour behalf, you may, at any time, change your health care provider without jeopardizing yourworkers' compensation claim for benefits. _________________________ __________ _____________________________ _________Signature of Injured Employee Date Signature of Witness Date
To the Employer:The employer shall provide the above-named injured employee with a copy of this signed formand shall maintain the original form in the employer's records where it may be inspected by theWorkers' Compensation Board at any time. This form shall not be submitted to the Workers'Compensation Board nor shall it be executed prior to the occurrence of this employee'swork-related injury or illness.
Please note: It is not necessary for you to sign this consent form if your employer is (i)participating in a certified preferred provider organization (PPO) under Article 10-A of theWorkers' Compensation Law, or (ii) participating in the alternative dispute resolution (ADR)pilot program under section 25(2-c) of the Workers' Compensation Law. In accordance withthese statutory programs, except in emergency situations, you must obtain at least initialtreatment for any workers' compensation injury or illness from the certified network(s) orproviders designated by your employer.
Injured Employee's Name Injured Employee's Social Security No. Date of Accident
Employer's Name and Address
www.wcb.state.ny.us ESTE RESUMEN ESTÁ ESCRITO EN ESPAÑOL AL DORSO C-3.1 (3-04)
The Workers' Compensation Board employs and serves people with disabilities without discrimination.

Estado de Nueva York JUNTA DE COMPENSACIÓN OBRERA
Aviso de Aceptación de Uso de Proveedor de Servicios o Red de Salud Recomendado porPatrono o Compañía de Seguros
La Junta de Compensación Obrera emplea y sirve a personas con impedimentos sin discriminar.
C-3.1S (3-04)
Al Empleado Lesionado: Para el tratamiento de su lesión o enfermedad relacionada con su trabajo, usted puede escogercualquier médico, podiatra, quiropráctico o sicólogo (con referido de un médico autorizado) queesté autorizado por la Junta y que esté aceptando pacientes de la Junta de CompensaciónObrera. Usted debe firmar esta forma de consentimiento si decide escoger usar una "Red" oProveedores que sean recomendados por su patrono o por el seguro ó permitir que su patronoseleccione un proveedor en su nombre. Usted puede, en cualquier momento en el futurocambiar su proveedor de salud de compensación obrera.
_________________________ __________ _____________________________ _________ Firma Empleado Lesionado Fecha Firma Testigo Fecha
Al Patrono: El patrono deberá proveer al empleado lesionado antes mencionado con una copia de esta formafirmada y deberá conservar el original en los records del empleado, donde pueda serinspeccionada por la Junta de Compensación Obrera en cualquier momento. Esta forma nodeberá ser sometida a la Junta de Compensación Obrera, ni deberá ser procesada conanterioridad a la lesión o enfermedad del empleado.
Nota: No es necesario que usted firme este documento, si su patrono (1) participa en laorganización certificada de proveedor preferido (PPO) acuerdo bajo el Artículo 10 A de la leyde Compensación Obrera, o (2) participa en el programa piloto de de resolución dealternativas de disputa (ADR) bajo la sección 25(2-C) de la ley de Compensación Obrera. Deacuerdo con estos programas establecidos por ley, excepto en situaciones de emergencia,usted deberá al menos inicialmente, recibir tratamiento por lesiones o enfermedad en eltrabajo, de una red certificada o de un proveedor designado por su patrono.
Nombre Empleado Lesionado Seguro Social Empleado Lesionado Día de Accidente
Nombre y Dirección del Patrono
www.wcb.ny.govTHIS NOTICE IS WRITTEN IN ENGLISH ON THE REVERSE SIDE.












![index []...p 104—109 comp. 190 p 110—115 comp. 191 p 116—121 comp. 192 p 122—127 comp. 193 p 128—133 comp. 194 p 134—139 comp. 195 p 140—147 comp. 196 p 148—153 comp](https://img.pdfslide.us/doc/110x75/5f95526362174b59db2f2d15/index-p-104a109-comp-190-p-110a115-comp-191-p-116a121-comp-192.jpg)







![index [] · comp. 41 index p 02—09 comp. 23 p 10—15 comp. 24 p 16—21 comp. 25 p 22—29 comp. 26 p 30—35 comp. 27 p 36—41 ... Свет подчеркивает структуру](https://img.pdfslide.us/doc/110x75/5f3c529d6f430b30851577ee/index-comp-41-index-p-02a09-comp-23-p-10a15-comp-24-p-16a21-comp-25.jpg)








