Embed Size (px)
Citation preview
EmpanelmentBuilding Relationships and the Capacity for Population
Health Management and Establishing the Foundation for Team-based Care
Presented by: Regina Neal, MPH, MS
Webinar for the Washington Association for Community and Migrant Health Centers
August 14, 2013

2
Learning Objectives
At the end of this workshop you will be able to:
• Describe the important role of empanelment in the development of a PCMH practice
• Describe and use a process for establishing right-sized patient panels for each provider in your practice
• Describe and implement the requirements to maintain and support panels in your practice
• Describe and use registries to implement population health management within the practice
• Develop data to monitor and measure outcomes for each team and panel to drive continued improvement

3
Expectations in a PCMH• The care, organization and design of the practice is
patient-centered
• Continuity between patients and a specific provider and care team is a reliable property of the practice
• Practice has an organized, proactive approach for managing and improving the care of a population of patients
• Every patient receives optimal care including preventive, chronic and acute through their life cycle
• Access systems are designed to promote continuity
Empanelment is a key to meeting these expectations
4
Empanelment and PCMH Practice Transformation

5Wagner EH, Coleman K, Reid RJ, Phillips K, Abrams MK, Sugarman JR. The Changes Involved in Patient-Centered Medical Home Transformation. Primary Care: Clinics in Office Practice. 2012; 39:241-259.
Change Concepts for Practice Transformation

6
Empanelment Key Changes
PCMH practices:
• Assign all patients to a provider panel and confirm assignments with providers and patients; review and update panel assignments on a regular basis
• Assess practice supply and demand, and balance patient load accordingly
• Use panel data and registries to proactively contact and track patients by disease status, risk status, self-management status, community and family needs
7
Think Different

8
Empanelment
A deliberate set of actions to identify the group of patients for whom a
primary care clinician and care team are responsible
9
Whose Patient Is It?

10
My Patients
New Goals, New Thinking

11
Empanelment Requires a Team
12
What Empanelment Makes Possible• Patient-centeredness; brings patients into focus
• Population health management─ Shifts focus from reactive care for acute or urgent needs to proactive health
care
• Development of high-performing care teams─ Needs of our patients as focus of joint effort
• Access with continuity─ Empanelment elevates our ability to provide the best care by making
continuity a key objective in providing access
─ Contributes to reduction in unnecessary demand and our knowledge of
patients which both contribute to our capacity and access
• Results─ Improved experience, improved care

13
Benefits from Empanelment
• Helps to create equitable distribution of workload among providers and care teams
• Allows for data-based decisions (closing and opening panels, adding provider FTE, etc.)
• Increases opportunities for team-based care, access, continuity, population management, better health outcomes, improved experience
Slide Source Amit Shah, MD, Multnomah County, OR

14
Empanel Patients
Team –based Care
Enhanced Access
15
Empanelment Process Overview• Leaders commit organization, time and resources to initial
and ongoing processes for empanelment• Establish panels: use supply, demand, 4-cut method,
engage providers and patients; tackle gnarly issues (e.g., part-time providers, panel size for NP, PA)
• Implement changes to support continuity and population health management– team-based care– scheduling for access with continuity– data on the panel available, used by team: registries and
patient data– vacation and time off policies, coverage, minimum FTE

16
Empanelment Process Overview• Implement processes to maintain panels over time (panel
management)– assign a panel manager with clear roles & responsibilities– empaneling new patients– adjustments for patients leaving practice, requesting change in
panel– empaneling new providers to the practice– timely adjustments, process for how to care for/re-empanel
patients of providers leaving the practice (including graduating residents) or changing clinical time (especially reducing it)
• Use data (visible, transparent) to monitor panel and practice level performance against goals and standards; act based on results – % patients empaneled; continuity rate, % patients meeting
specific health goals of importance to your community of patients

17
Create panel for one provider
Begin team-based care
Create panel for 2nd provider
Develop, Implement changes to support continuity
Develop, implement policies to support empanelment
Create panels for remaining providers
Provide registries, patient data
Develop, use performance data Empanelment Tasks
1 2 3 4 5 6 7 8 9 10 11 12Months
Implementation Timeline (Example and Estimates)
Build commitment for the change throughout the practice

18
Results from Multnomah County• Started with pilot clinic to
ensure the process worked
• Process took 6 months for all clinics
• Had empanelled 99% of patients within 8 months; had started with 6,000 unassigned patients & many more assigned to an incorrect provider
• Implementation of new processes were maintained post-empanelment
Slide Source Amit Shah, MD, Multnomah County, OR

19
The Mechanics of Empanelment: Building Patient Panels
Key Changes:
Assign all patients to a provider panel and confirm assignments with providers and patients
Assess practice supply and demand, and balance patient load accordingly
20
Steps in the Process
• Determine target panel size based on the number of patient’s in the practice– How many patients are in our practice? If distributed evenly across all
providers, what is the target practice panel size? • Determine current panel for each provider based on
actual patient visit data– Who did each patient see for each visit? Use this data to assign patients
to the panel of one provider (four-cut method)
• Determine supply-demand balance panel size for each provider based on supply of and demand for visits– How many visits do patients make per year? How many visits does the
provider have available per year?
Target Practice Panel
Current Panel
Ideal Panel
Supply-Demand Balance

21
# in Target
Practice Panel
# in Current Panel
# in Ideal Panel
# in Supply-Demand
Panel
Examining the Results of the Process

22
Why Supply and Demand Matter
• Supply and demand need to be in balance for access and continuity to be reliable features of the practice
• When not in balance, panels end up being too large or too small
• Too large: delays for appointments, deflections, discontinuity, rework, overwork
• Too small: demand may not be adequate to support the practice– Financial– Work load equity among providers
23
Measuring Supply and Demand
• Supply = availability of provider capacity as measured by number of appointments
• Demand = care and service needs of current patient population estimated by number of visits per patient– Adult patients– Pediatrics

24
The Ideal Panel Size
Calculate:
(provider appointment slots/year)-------------------------------------------------------
(average number of visits / patient/year)
Solve: 4520 = 1417
3.19

25
Who’s on the Current Panel?
• Determine the current de facto panel to determine if patients are all assigned to the right provider – Who did each patient actually see for each visit?
– Often patients see providers other than assigned provider
– Patients often see more than one and sometimes more than two providers in the practice
– These data will be used to assign patients to the panel of one provider
• Compare current panel with ideal panel to ensure right-sized panels

26
Possible Risk Adjustments to Panel Size
• Patient age and gender can predict demand and reflect acuity– Need adjustment factors to apply– Need information system to do calculations to apply
adjustments
• Apply variance for specialty of practice– Family practice, Internal Medicine, Pediatrics
• Weight by complexity, acuity, morbidity– Age, gender adjust captures much of acuity impact– Complex process: what are the right factors to use?
27
Consider This
• Remember: One panel adjusted down requires another to be adjusted up– Can lead to a complicated process within the practice– Can stall or delay the process without material
improvement in panel sizes
“Practices should consider whether many of the age and acuity factors could be managed more effectively by
providing focused team support than by adjusting panels.”
-- Mark Murray

28
How Big Can a Panel Be?
• Panel size has some elasticity• Practice patterns and system design can influence
maximum panel size possible• Using teams who “share the care” is a key
contributor to being able to manage larger panel sizes – recent study suggests delegation of preventive and
chronic care tasks to non-physician team members can allow team to care for a larger panel than would otherwise be possible
29
Practice Patterns Influence Panel Size• Visits per patient per year
– Can decrease with continuity; lower visit return rate; provide more service at each visit; increase role of team members so all care not delivered by provider; use alternatives to traditional visits, e.g., telephone, email, group visits
• Provider visits per day– Increase by improving visit show rates; share the care among
team members; improve workflow efficiency; increase number of exam rooms; remove all unnecessary work from providers to maximize appointment supply
• Provider sessions or days per year– Do as much as possible to protect provider time during patient
care hours from non-patient care activities; e.g., incorporate administrative time duties into the work of the team; use non-patient care hours for meetings

30Source: Murray et .al,. Panel Size: How Many Patients Can One Doctor Manage? Family Practice Management, April 2007.

31
Team-Based Care Influence on Panel Size• Findings from recent study
– If portions of preventive and chronic care services are delegated to non-physician team members, practice panels of larger size are possible
Type of Delegation
Prevent/ChronicDelegation NONE(% = 0/0)
Prevent/Chronic Delegation LOW (% =50/25)
Prevent/ChronicDelegation MED(% = 60/30)
Prevent/ChronicDelegation HIGH(% = 77/47)
Panel Size 983 1,387 1,523 1,947% Increase from Base 41% 55% 98%
Source: Altschuler, et.al., Estimating a Reasonable Panel Size for Primary Care Physicians with Team-based Task Delegation. Annals of Family Medicine, Vol 10, No. 5; September/October 2012
32
Are There Limits To Panel Size?• Saying “yes” can mean “no” if we can’t provide what the patient
needs and wants, can’t maintain access with continuity
• Leads to escalating chaos within the practice, increase in
rework, decrease in outcomes and experience; burnout,
decreased patient experience and poorer outcomes
• To maintain panels at right size, you may find you need to add
more providers. But this is a last step
• First─ build teams; redesign workflows; exploit power of technology;
eliminate needless work and re-work; add staff to do the right
work e.g., care coordinators, care managers, pharmacists,
behavioral health, etc.
33
Adjusting a Panel That Is Too Large
• Bolster the care team: shift more resources to support the provider and care team, e.g., additional nursing and/or clerical support; additional exam rooms
• Excuse the provider from seeing patients of absent providers
• Let attrition take its course• Close the panel temporarily• Move patients to another panel. Develop a patient-
centered and thoughtful process– Providers need to inform their patients directly– Patients need to agree to any transfer
34
What if the Panel is Too Small?
• Develop a plan to grow a small panel– Consider whether the provider is new to practice or is an
experienced provider
• Consider moving patients from panels that may be too large– Always consider the patient’s desires in any plan to
redistribute patients to a different panel– Providers need to be part of direct communications with
patients about moving to another panel
35
How Do We Know Panels Are Right-Sized?
• Use metrics to assess• Ask patients how it is working for them
(experience)– Can they get an appointment easily when they want it?– Are they seeing their provider and care team regularly?
• Ask staff how it is working from their point of view• Monitor panel size to compare data to panel size• Use these data to determine if panel sizes for any
provider need adjustment

36
Empanelment & Continuity Metrics
• % of total clinic patients empanelled• % of patient visits to assigned PCP (continuity)• % of panel patients who are new / reassigned /
dropped (at team and clinic level)• 3rd next available appointment• Patient experience with access and continuity• Provider/team experience with panel
sustainability• Clinical process & outcome metrics for by panel
37
The Process of Empanelment
Ensuring Success in Implementation

38
Fears and Misperceptions About Empanelment
“My patients will have less access since they must see the same provider and care team. My schedule is fully booked for the next five months. Assigning
patients to me will only make this worse”
“This is only leadership’s way of tracking productivity. This won’t benefit me or my patients.”
39
Engage Providers & Teams in the Process
• Use a process designed to engage providers and care teams so panels are accepted, embraced, owned
• Allow all providers to review their panel for correctness; encourage discussion, questions
Slide Source Amit Shah, MD, Multnomah County, OR
40
Confirm Panel with Providers• Review de facto panel and ideal panel size with
providers to engage them in process and develop ownership of their panel– This is an ongoing process from beginning
– Medical leadership is essential
– Start with goals, benefits
– Review process, methods, data
– Have a dialogue (on-going) about goals, benefits, concerns, process for assessment, making adjustments
– What data will you use to assess outcome goals and panel size over time?

41
Engage Patients in the Process Too
• Involve patients by checking with them when they come into the clinic or call to schedule an appointment to confirm that they agree that Dr. Smith or the NP, Ms. Jones, is their provider
• When patients call the clinic always ask “who is your assigned provider?” and ensure that the call is routed to the right care team
• Communicate and reinforce provider – patient link in as many ways as possible
42
Challenging Circumstance
• Our patients are more interested in getting access than in seeing the same provider. Empaneling patients doesn’t seem to be worth the time and effort under these circumstances.– Improve access for patients– Ask patients more about their preferences to
understand them– Work with patients to help them understand why seeing
the same clinician is important– Form a coverage plan to limit randomness of provider
seen while you establish better access and acceptance of empanelment

43
Sustaining Empanelment in the Practice

44
Empanelment – Real Culture Change and Deliberate Leadership-Driven Process
• Push for shift in thinking, goals & system design• Operational support for initial panel development &
maintenance over time• Policies to ensure continuity in scheduling processes• Support for care teams to successfully take on population
management activities and tasks• Providing time (for huddles, planned care preparation)• Providing population-based registry tools for use in daily
planning and practice

45
Creating Patient Panels is Only One Step in the Process
• Patient panels need to be maintained over time
• System design must specifically support access and continuity for patients
• Care teams need panel data and registries for proactive care; time for team to work/plan for care & self management, outreach and follow-up

46
Maintaining Panels in Practice
• The empanelment process needs to be used regularly
to keep panels right-sized over time• Develop processes to ensure all new practice patients
are linked to a specific provider as soon as they are
assigned or choose the practice as their medical home• Have a process to use to adjust panels for patients who
are leaving the practice or want to switch providers• Use to re-empanel patients whose providers leave the
practice or to adjust panels for providers who cut back
their clinical time
47
Build an Empanelment Process• Define Roles and Responsibilities
– Assign a Panel Manager to oversee all processes for
empanelment
– Use scripts at clinic reception during check-in, when making
appointments to validate patient’s provider and patient preference
• Develop standard process for PCP assignments– Initial for new patients
– Patients leaving practice, providers leaving practice or changing
their clinical FTE
• Run supply and demand data periodically to ensure panel size is neither too large or too small
• Identify unassigned patients monthly and develop process for assigning
48
Establish Standards for Part-time Provider Staffing, Scheduling & Coverage
• Minimum number of days per provider in clinic
• Partner part-time providers (2-3) for coverage of panel over all sessions for a week, no gaps
• No overlapping vacation schedules
• Requires significant medical leadership involvement and time to establish standards, communicate them and implement
Slide Source Amit Shah, MD, Multnomah County, OR
49
Dimensions of Change• Conceptual/cognitive – why are we doing this?
Making the case for change: target hearts & mind• Technical – what do we have to do? how do we do
it? Teaching, knowledge, new skills, confidence• Structural – who am I working with? Will I have a
new boss? Changes in relationships; role, position and status changes
• Adaptive (human/psychological response) – How do I feel about this? What do these changes mean for me? Can I do it? Will I succeed? Will I like it? Do I want to?

50
Pre
p P
hase
Acc
epta
nce
Pha
seC
omm
itmen
tP
hase
Building Commitment in Change ProcessD
egre
e of
Sup
port
for
the
Cha
nge
Time
Contact
Awareness
Understanding
+ Perception
Installation
Adoption
Institutionalize
Internalize
Source: Conner, D. Managing at the Speed of Change. 1st ed. New York, NY: Random House; 1993.

51
PCMH-A

52
Linking Empanelment to Appointment Scheduling for Continuity
• Ensure that scheduling is done to prioritize continuity for patient with provider and care team
• It is easy for scheduling process to revert to look for next available provider vs. the assigned provider
• Use scripting for appointment scheduling to assist staff and to standardize the process
• Monitor data to ensure access and continuity
53
Create Access
• Reduce No-Shows to avoid guess work• Make same day appointments available• Confirm scheduled appointments in advance• Use the team to provide care and consider
alternatives to a return visit for all patients – use team for follow-up
• Measure to understand your system– No show rate by provider– Third next available by provider– Demand for appointments– Supply of appointments

54
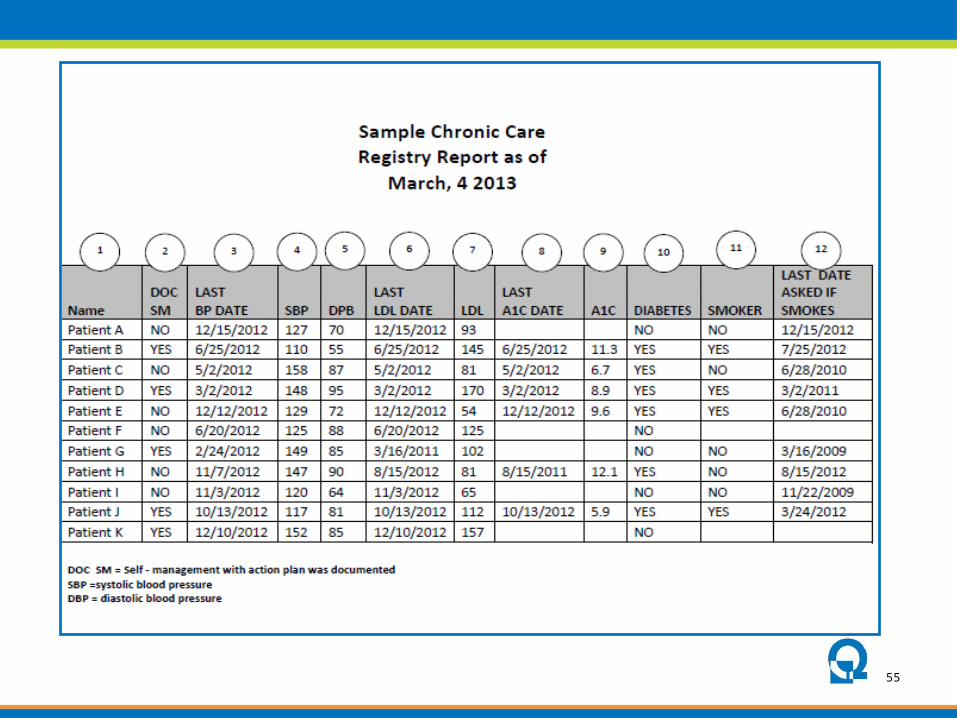
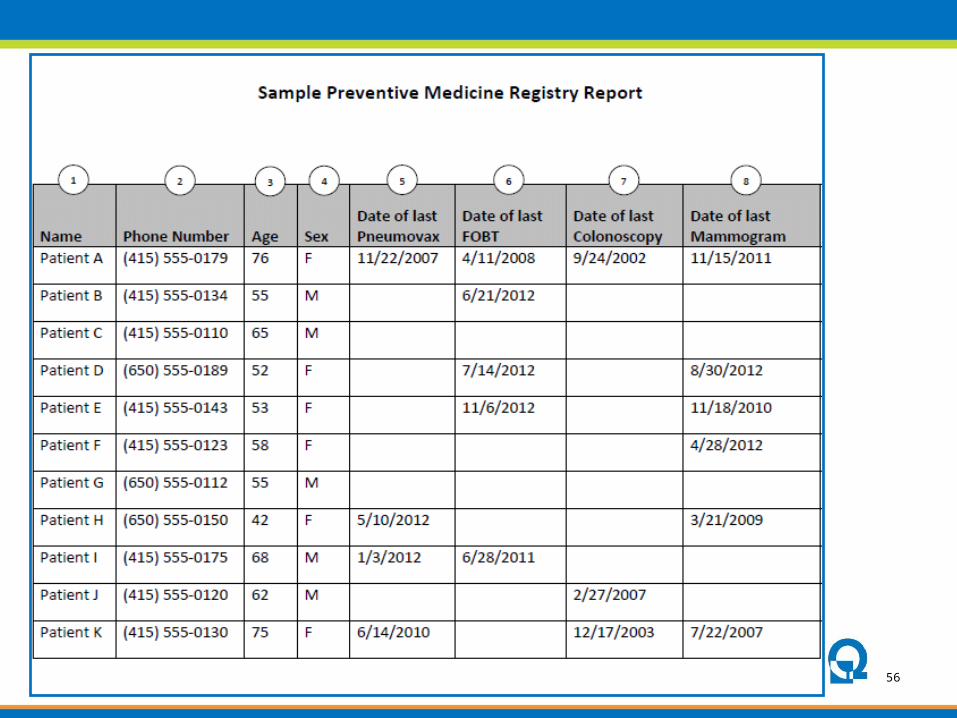
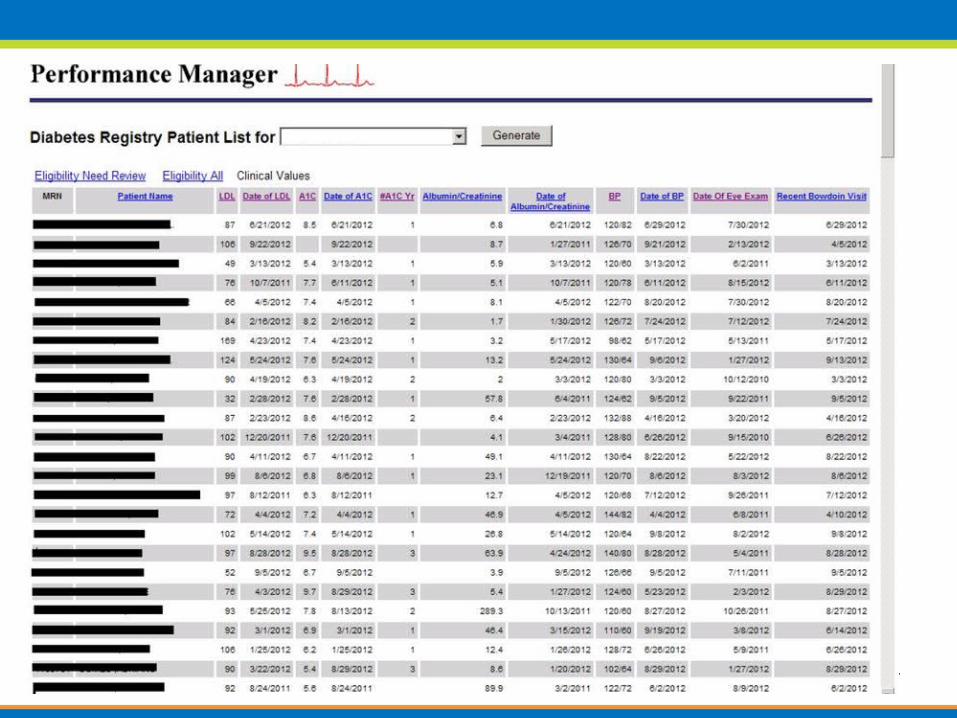
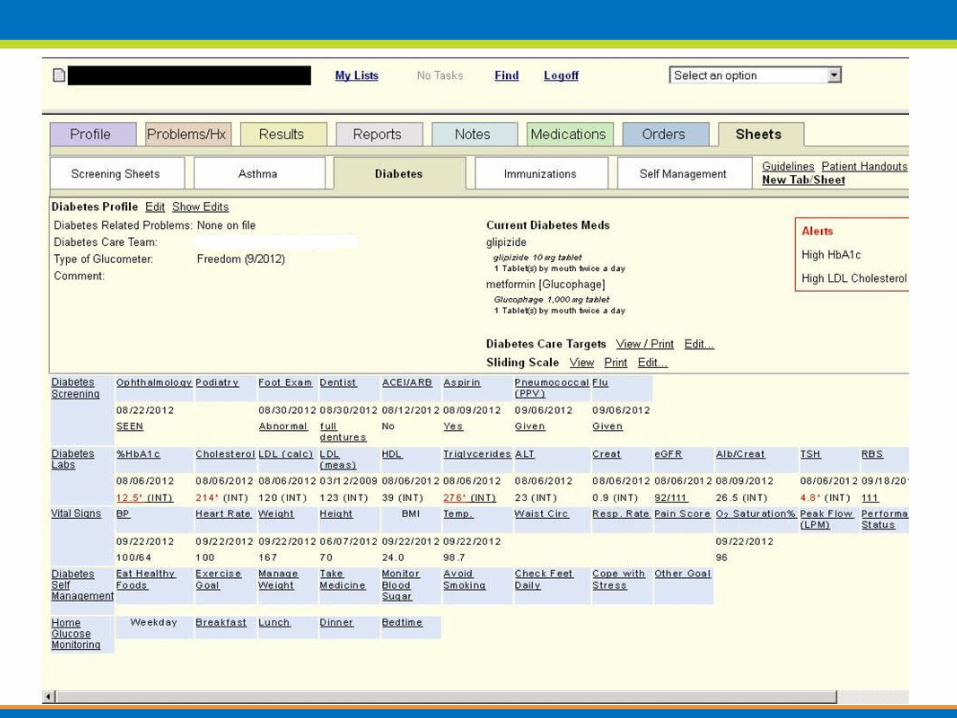
Opportunity from Empanelment: Population Health, Planned Care
and Reducing Gaps in Care
Key Change: Use panel data and registries to proactively contact, track
and engage patients in care
55
56
57
58

59
60
Using Panel Data for Planned Care

61
Key Activities for Practice Transformation
“The best way to have a good idea is to have a lot of ideas.”
-Linus Pauling

62
Key Activities Checklist
63
Resources
Safety Net Medical Home Initiative Web-sitehttp://www.safetynetmedicalhome.org/change-concepts/empanelment
64

65
Questions & Discussion

Regina NealSenior Consultant, Qualis Health
888-432-0261 x2066
For more information: www.QualisHealth.org