Embed Size (px)
Citation preview

Emotion Perception in Borderline Personality Disorder
by
Alexander R. Daros
A thesis submitted in conformity with the requirements for the degree of Master of Arts
Department of Psychology University of Toronto
© Copyright by Alexander R. Daros 2012

ii
Emotion Perception in Borderline Personality Disorder
Alexander R. Daros
Master of Arts
Department of Psychology University of Toronto
2012
Abstract
Borderline personality disorder (BPD) is a serious mental illness characterized by emotion
dysregulation. Symptoms related to emotion are thought to contribute to difficulties in perceiving
emotional expressions. Individuals with BPD and demographically matched healthy controls
completed a task assessing the recognition of happy, sad, and neutral facial expressions at two
intensities. Patients with BPD demonstrated comparable performance on the recognition of very
happy and very sad facial expression but were significantly less accurate on neutral expressions.
Patients with BPD were also significantly worse in recognizing mildly happy facial expressions,
however the severity of current depressive symptoms intervened this relationship. There was
evidence that perceptual biases within BPD are unique from mood-congruent biases typically
found in major depressive disorder. The findings advance research on the topic of emotion
perception in BPD and suggest important new lines of investigation that may be useful for
delineating the nature of emotion dysregulation in BPD.

iii
Acknowledgements
I am grateful to many people for their assistance and support on this project. From
conception to completion, my graduate advisor and mentor, Dr. Anthony C. Ruocco supported
me throughout the long process. Anthony, thank you for keeping me on track, pushing me to
think critically, and helping me to become a better writer. My subsidiary advisor, Dr.
Konstantine Zakzanis helped shape this project for the better by encouraging me to quantitatively
review previous literature on the topic. In doing so, my understanding on the subject matter has
increased and new skills in summarizing and analyzing data were acquired. I am also gracious
for the helpful comments and support received by Dr. Amanda Uliaszek, my thesis reviewer.
This was a thesis committee so well grounded in clinical research that I have gained considerable
knowledge throughout the entire process.
This project relied on the teamwork of every single one of the members of the Clinical
Neurosciences Laboratory. One person cannot undertake the amount of work that goes into a
clinical research study. To the lot of you, I say thank you for your exceptionally hard work and
commitment to the projects in the lab. The attitude in the lab was always positive thanks to all of
your support and affinity for research.
Friends and family provided an astonishing amount of support and cathartic release
throughout the writing of this thesis. I really do appreciate all of the kind words, praise, and
constructive feedback that I have received during this year of intense research.

iv
Table of Contents
Acknowledgments ........................................................................................................................ iii Table of Contents...........................................................................................................................iv List of Tables .................................................................................................................................vi List of Figures................................................................................................................................vii Chapter 1.........................................................................................................................................1 1 Introduction................................................................................................................................1 1.1 Borderline Personality Disorder and Emotion Dysregulation......................................1 1.2 Measuring Emotion Perception Difficulties in BPD....................................................4 1.3 Emotion Recognition in BPD.......................................................................................7 1.4 Emotional Acuity in BPD ............................................................................................9 1.5 Limitations of Previous Research ..............................................................................10 1.6 The Present Study ......................................................................................................11 Chapter 2.......................................................................................................................................13 2 Method.....................................................................................................................................13 2.1 Participants ..................................................................................................................13 2.2 Measures......................................................................................................................14 2.2.1 Diagnostic Interviews………………………………………………………14 2.2.2 Self-Report Measures………………………………………………………15 2.2.3 Neuropsychological Measures……………………………………………..15 2.2.4 Penn Emotional Acuity Test……………………………………………….16 2.3 Statistical Plan…........................................................................................................17 Chapter 3.......................................................................................................................................19

v
3 Results......................................................................................................................................19 3.1 Demographic and Clinical Characteristics.................................................................19 3.2 PEAT Accuracy..........................................................................................................19 3.3 Analysis of Current Mood…………………………………………………………..20 3.4 Secondary Analyses………………………………………………………………...22 3.4.1 Reaction Time……………………………………………………………...22 3.4.2 Comorbidity and Psychotropic Medications……………………………….22 Chapter 4.......................................................................................................................................23 4 Discussion..............................................................................................................................23 4.1 Strengths and Limitations..........................................................................................28 4.2 Implications and Conclusions....................................................................................29 References.....................................................................................................................................31 Tables............................................................................................................................................40 Figures...........................................................................................................................................46

vi
List of Tables
Table 1. Description of Emotion Perception Tasks……………………………………………40
Table 2. Demographic and Clinical Characteristics of Patients with Borderline Personality
Disorder and Healthy Controls………………………………………….…………………….41
Table 3. Clinical Characteristics for Patients Diagnosed with BPD for the Present Study…..42
Table 4. Accuracy Results from the PEAT for BPD and HC…………………..………………43
Table 5. Response Patterns Based on PEAT Stimulus Classification……………………….…44
Table 6. Reaction Time (RT) Results from the PEAT for BPD and HC………………………..45

vii
List of Figures
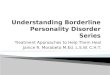
Figure 1. Response patterns on (A) mildly happy stimuli and (B) neutral stimuli of the PEAT for
BPD (n = 30) and HC (n = 27) participants.……………………………………………………46
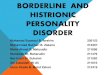
Figure 2. Mediation analyses with BDI score as a mediator and (A) TC score, (B) NC score, (C)
MHC score as dependent variables……………………………………………..……………...47

1
Chapter 1
Introduction 1
1.1 Borderline Personality Disorder and Emotion Dysregulation
Borderline personality disorder (BPD) is a serious mental illness that affects 1-2% of the general
population and is characterized by a pervasive pattern of emotional instability, unstable
interpersonal relationships, impulsive aggression, and suicidality (Lenzenweger & Pastore, 2007;
Torgersen, Kringlen, & Cramer, 2001). Patients with BPD typically suffer from increased
economic hardship and comorbidity with Axis I disorders leading to a disproportionally higher
utilization of inpatient psychiatric services (Comtois et al., 2003; Grant et al., 2008). A
staggering two-thirds of patients with BPD present with three or more Axis I diagnoses, the most
common being major depressive disorder (MDD) and bipolar disorder (BD) (Zimmerman &
Mattia, 1999). Prevalence of BPD among psychiatric outpatients is approximately 15%
(Torgersen et al., 2001) and this illness is often overlooked and underdiagnosed in many patients
(Skodol et al., 2002). Additionally, BPD is associated with a high prevalence of self-injurious
behaviour (Clarkin, Widiger, Frances, Hurt, & Gilmore, 1983; McGlashan et al., 2005), suicide
attempts (Soloff, Lynch, & Kelly, 2002; Soloff, Lynch, Kelly, Malone, & Mann, 2000; Zisook,
Goff, Sledge, & Shuchter, 1994) and completed suicides (Frances, Fyer, & Clarkin, 1986; Paris,
Brown, & Nowlis, 1987).
Emotion dysregulation has been hypothesized as the core clinical feature of BPD (Linehan,
1993; Selby & Joiner, 2009). Difficulties with emotion regulation may, at least in part, account
for the substantial comorbidity of BPD with mood and other related disorders, as well as their
increased risk for suicide. Linehan’s (1993) biosocial developmental model remains a prominent

2
theoretical framework for describing emotion dysregulation in BPD. Biological predispositions
such as a hyperbolic temperament and an emotional vulnerability are hypothesized to lead
individuals with BPD to experience a heightened sensitivity to emotional stimuli, experiences of
emotions as more intense than other individuals, and slow returns to baseline emotional arousal
(Zanarini & Frankenburg, 2007). In conjunction with vulnerabilities, BPD develops in the
context of an invalidating environment in which communication of emotional experience is met
by erratic, inappropriate, and extreme responses by others. The individual’s emotional behavior
is negated, rejected, or dismissed, even though it may be a valid response on the part of the
individual (Linehan, 1993). Emotion dysregulation is also theorized to culminate in the
development of behavioural dysregulation. In particular, acts that these individuals find difficult
to control but are utilized in situations where they seek to shift attention away from unpleasant
emotional states (e.g., self-injurious behaviour). Rumination also appears to play a role in BPD
and can lead to an amplification of negative affect (Donaldson & Lam, 2004; Lavender &
Watkins, 2004) suggesting a second possible link underlying the comorbidity of BPD with
MDD. In one study, patients with BPD reported higher levels of rumination compared to
individuals diagnosed with MDD (Abela, Payne, & Moussaly, 2003). This result was surprising
given the strong and largely specific connection between rumination and depression (Abela et
al., 2003; Just & Alloy, 1997).
Research on affective instability and emotional intensity in BPD has provided support for the
biosocial developmental model. Individuals with BPD have reported more mood variability
throughout the day compared to patients with MDD and healthy individuals (Cowdry, Gardner,
O'Leary, Leibenluft, & Rubinow, 1991). Patients with BPD also have shown greater emotional
lability with regard to anger, anxiety, and the oscillation between depression and anxiety

3
compared to patients with MDD, Bipolar II disorder, and cyclothymia (Koenigsberg et al., 2002).
In one experience sampling study that took place over the duration of one month, patients with
BPD regularly experienced more extreme changes in hostile, fearful, and sad affect than
depressed patients (Trull et al., 2008). Research has also reported a positive correlation between
negative emotional intensity in BPD and intense negative emotions following social interactions
(Russell, Moskowitz, Zuroff, Sookman, & Paris, 2007). Patients with BPD report greater
subjective intensity of negative emotions as compared to healthy controls (Levine, Marziali, &
Hood, 1997), and the magnitude of this intensity is strongly associated with severity of BPD
symptoms (Cheavens et al., 2005; Rosenthal, Cheavens, Lejuez, & Lynch, 2005; Yen, Zlotnick,
& Costello, 2002).
Research from neuroimaging studies generally supports an underlying pathology for emotion
dysregulation in BPD. Decreased amygdala and hippocampal volumes have been reported in
structural neuroimaging studies of patients with BPD, regions thought to be involved in the
regulation of emotional experiences (Driessen et al., 2000; Ruocco, Amirthavasagam, &
Zakzanis, 2012; Schmahl, Vermetten, Elzinga, & Bremner, 2003; Tebartz van Elst et al., 2003).
Functional neuroimaging studies have demonstrated an altered baseline metabolism in limbic
and paralimbic regions linked to emotion generation in response to stressful challenges (Schmahl
et al., 2006). In addition, functional neuroimaging studies have found heightened reactivity to
negatively valenced pictures in the cingulate, insula, and dorsolateral prefrontal cortex of patients
with BPD when compared to healthy controls (see Ruocco, Amirthavasagam, Choi-Kain, &
McMain, 2012). Koenigsberg and colleagues (2009) noted that patients with BPD utilized
different brain areas, an action-prone system, while looking at negatively valenced images
compared to the less reactive system used by controls. These results led the authors to

4
hypothesize that emotion dysregulation has downstream influences on emotion perception in
BPD, which may have implications for the appropriateness of social behavior and interpersonal
interactions in these patients. Perhaps most critical for this process is the role of the prefrontal
cortex in differentiating negative expressions of emotion (Adolphs, 2002; Hariri, Bookheimer, &
Mazziotta, 2000; Narumoto et al., 2000). Recent neuroimaging studies have provided evidence
of a dysfunction of prefrontal systems during negative emotion processing in BPD (Koenigsberg
et al., 2009; Ruocco, Medaglia, Ayaz, & Chute, 2010). Understanding how individuals with BPD
perceive emotions may provide new avenues of research that can implicate brain areas involved
in the neuropathology of BPD. To facilitate regulation of emotional responses to evocative
stimuli, the ability to control attention while in contact with these stimuli is necessary (von
Ceumern-Lindenstjerna et al., 2010). If emotionally valenced stimuli are perceived in a
hyperarousing or hypervigilant manner in BPD, disengaging one’s attention from emotional
stimuli becomes more difficult due to emotion dysregulation (Linehan, 1993). Whether the
recruitment of additional attentional resources leads to benefits or deficits in the perception of
emotionally valenced stimuli within BPD, however, remains to be fully clarified.
1.2 Measuring Emotion Perception Difficulties in BPD
Individuals with BPD have been described as highly vigilant to social stimuli, especially for
social cues that might signal social threat or rejection (Linehan, 1995). Patterns in visually
recognizing and identifying emotional facial expressions may hold clues as to whether
individuals with BPD receive added benefits or consequences from their heightened sensitivity to
such stimuli. Recognition of six basic emotional expressions (happiness, sadness, fear, disgust,
anger, surprise) has been argued to be universal across cultures because of the highly salient and
evolutionary significant information they contain (Ekman, 1992; Ekman, Levenson, & Friesen,

5
1983). Many psychiatric conditions have been associated with deficits in emotion recognition,
including MDD, BD, schizophrenia, panic disorder, generalized anxiety disorder, obsessive-
compulsive disorder, and social phobia, among others (Bolte & Poustka, 2003; Corcoran,
Woody, & Tolin, 2008; Derntl, Seidel, Kryspin-Exner, Hasmann, & Dobmeier, 2009; Feinberg,
Rifkin, Schaffer, & Walker, 1986; Kohler et al., 2003; Rector, Daros, Bradbury, & Richter,
2012). Accurate emotion recognition serves as a cognitive cornerstone for appropriate social
functioning and the capacity to recognize internal states from external cues may be important for
promoting empathy, trust, and prosocial behavior (Marsh, Kozak, & Ambady, 2007). In turn,
enduring misinterpretations due to inaccurate recognition are likely to result in emotional
disturbances, inadequate social behavior, and impaired social functioning in a variety of
psychiatric disorders.
While the literature on emotion perception research is vast, three main aspects of facial emotion
perception have frequently been studied in BPD (see Table 1). The first can be labeled emotion
recognition and is usually measured by presenting a series of single photographs of emotional
facial expressions and having the respondent ascribe a particular emotion to the stimulus in some
fashion. Photographs typically remain static rather than progressively morphed and they
primarily employ prototypic expressiveness for each emotion displayed (i.e., 100%
expressiveness). A second method used to measure emotion perception has frequently been
termed emotion discrimination in which respondents are asked to distinguish between two
emotions. One variation of this experimental design presents a single photo containing, for
example, 40% anger and 60% happiness, and then asks participants to state which emotion they
see (e.g., Domes et al., 2008). A further design presents two stimuli at the same time and asks the
participant to determine which face shows more emotion. This second design has more flexibility

6
in that the participant can be presented with a combination of a neutral face and an emotional
face, two faces displaying negative emotions, or one face with a positive expression and the
other with a negative expression. Finally, a third test of emotional perception involves the acuity
of or threshold for perceiving emotions. These tasks typically present a neutral face first, which
is then followed by an incremental blend of a target emotional expression, which represents a
successive approximation of the target emotion from mild to more extreme representations of
this expression. The respondent is asked to stop the progression of morphs when they are certain
that they perceive an emotion in the face and can articulate that emotion. An alternate variant of
this task randomly presents individual stimuli at different levels of blending of emotions (e.g.,
50% neutral/50% target emotion; 10% neutral/90% target emotion).
A variety of facial emotion stimulus sets have been developed to study emotion recognition in
healthy individuals and patients with psychiatric illnesses. Most emotion recognition studies of
BPD utilized Ekman and Friesen’s (1976) Pictures of Facial Affect (POFA), which includes 14
actors (eight female and six male) and their portrayal of six basic emotions (happy, sad, angry,
fear, disgust, and surprise) and neutral facial expressions. Many researchers favour the POFA
because these photographs have been rated by large normative groups and can be reliably
identified in a number of cultures with agreement rates often close to 100% in Western societies
(Ekman, 1992). There are, however, several drawbacks to using the POFA, including a high
ceiling and a lack of ethnic diversity of the actors (all Caucasian), although a more diverse set of
faces has been developed (i.e., Japanese and Caucasian Facial Expressions of Emotion, or
JACFEE; Ekman and Matsumoto, 1992). The JACFEE collection consists of 56 colour
photographs portraying each of the seven emotional categories as in the POFA. These stimuli
comprise an equal number of male and female actors as well as Caucasian and Japanese actors.

7
An abbreviated recognition task is the Fear-Anger-Neutral (FAN) test, which was designed to
target the more difficult discrimination of negative and neutral facial expressions (Gur et al.,
2002; Schneider et al., 2006). A more recently developed set of standardized facial emotion
stimuli is contained within the Penn Emotion Recognition Task (ER40) (Gur et al., 2002; Kohler,
Turner, Gur, & Gur, 2004), which consists of 40 stimuli displaying five emotions: happy, sad,
anger, fear, and neutral (termed “no emotion”). Advantages of the ER40 are that it contains
ethnically diverse actors and exists in a completely standardized and computerized form. The
POFA and JACFEE, on the other hand, must be assembled into an experimental paradigm by
individual investigators, the specific parameters of which may differ across studies. Importantly,
these tests depict emotional stimuli at 100% expressivity (i.e., the prototypic expression) as
opposed to blending or morphing two emotions together into more emotionally ambiguous facial
expressions.
1.3 Emotion Recognition in BPD
Several studies have demonstrated that patients with BPD may be less accurate than non-
psychiatric comparison participants in their recognition of negative facial emotions, including
anger, fear, disgust, and sadness (Bland, Williams, Scharer, & Manning, 2004; Dyck et al., 2009;
Levine et al., 1997; Unoka, Fogd, Fuzy, & Csukly, 2011). These findings were initially thought
to reflect a more generalized deficit in the perception of negative emotions in BPD. Other
research, however, indicated that these patients may be less accurate in recognizing faces
showing no emotion (i.e., neutral) (Wagner & Linehan, 1999) as well as surprised facial
expressions (Lynch et al., 2006). These findings could not be explained by a speed-accuracy
tradeoff for patients with BPD (Dyck et al., 2009; Merkl et al., 2010; Minzenberg, Poole, &
Vinogradov, 2006). Contrary to these studies were a smaller number of investigations which

8
suggested that patients with BPD may actually be more accurate in their recognition of fearful
(Merkl et al., 2010; Wagner & Linehan, 1999) and surprised facial expressions (Unoka et al.,
2011). Perhaps more consistent, however, is the finding of no significant emotion recognition
deficits in patients with this illness (Dyck et al., 2009; Lynch et al., 2006; Minzenberg et al.,
2006; Robin et al., 2012; von Ceumern-Lindenstjerna et al., 2007). Based on these results, it
remains unclear whether patients with BPD indeed show deficits in facial emotion recognition,
and if they do, whether these deficits might be limited to specific categories of emotion.
Diagnostic comorbidity with BPD may have a significant impact on facial emotion recognition
capacities. Given that mood disorders are prevalent in patients with BPD (Zimmerman & Mattia,
1999), the contribution of mood state to biases in emotion perception is important to consider in
this population. For example, patients with MDD show mood-congruent biases in facial emotion
recognition as well as in their memory for emotion words (Murphy et al., 1999; Watkins, Vache,
Verney, Muller, & Mathews, 1996). Studies of facial emotion recognition have reported no
differences in accuracy or reaction time (RT) for patients with BPD in regards to comorbid
psychiatric conditions (Bland et al., 2004; Domes et al., 2008; Dyck et al., 2009; Robin et al.,
2012; Unoka et al., 2011), while other investigators chose to exclude patients with current
depression to avoid this confound altogether (Dyck et al., 2009; Merkl et al., 2010; Minzenberg
et al., 2006). Unfortunately, the results of mood rating scales were not reported in most emotion
recognition studies of BPD, making it difficult to understand the contributions of patients’
current mood to emotion perception deficits in these studies.
To shed light on this inconsistency, Domes and colleagues (2009) provided a comprehensive
narrative review on the topic of facial emotion perception in BPD, concluding that these patients
may show subtle impairments in labeling emotional expressions along with a tendency to

9
perceive emotionally ambiguous faces (i.e., neutral ones) more negatively. A negative perceptual
bias is consistent with previous research demonstrating a heightened negative perception of other
persons in BPD (Arntz & Veen, 2001; Wagner & Linehan, 1999) and in over-attributing anger to
ambiguous facial stimuli (Domes et al., 2008), which could reflect an anticipation of
interpersonal rejection or social threat. The results of a recent meta-analysis on emotion
recognition in BPD suggests that these individuals may have selective deficits in the recognition
of neutral (no emotion), disgust, and angry facial expressions, although there is some evidence to
suggest a more generalized difficulty recognizing negatively valenced emotions (Daros,
Zakzanis, & Ruocco, 2012).
1.4 Emotional Acuity in BPD
Neuroimaging research on individuals with BPD has found increased metabolic brain reactivity
to negatively valenced pictures accompanied by slower returns to baseline, suggesting a
hypervigilant response when compared with healthy controls (Herpertz et al., 2001; Koenigsberg
et al., 2009). If BPD patients are acutely sensitive (i.e., hypervigilant) to emotional stimuli they
should recognize emotions at lower thresholds when compared to healthy individuals. One way
of testing this hypothesis incorporates the use of morphing tasks, in which emotional stimuli are
morphed from neutral to full expressivity. Three studies used similar methodological designs to
test emotional acuity in BPD. Each presented a series of morphed stimuli in order from 0%
(neutral) to 100% (emotion) in 5% increments. Participants were instructed to press a stop button
when they felt they were aware of the emotion the face was beginning to show. This instruction
was intended to reduce false alarms. Stopping the sequence and then giving the correct answer
for the emotion provided a detection threshold based on the increment value. The increment
value was then averaged for multiple presentations of six basic emotions (happy, sad, anger,

10
fear, disgust, and surprise) (Domes et al., 2008; Jovev et al., 2011; Lynch et al., 2006). Emotion
sensitivity was therefore operationally defined as the ability to recognize emotion at lower levels
of intensity and it was expected that individuals with BPD would exhibit this pattern of response.
In two studies of emotion sensitivity, a comparable detection threshold was found in patients
with BPD and healthy controls (Domes et al., 2008; Jovev et al., 2011), while a third study
demonstrated emotion sensitivity (i.e., lower detection threshold) in patients with BPD that was
consistent for each of the six basic emotions, including happiness (Lynch et al., 2006).
Furthermore, Lynch and colleagues (2006) found that this hypersensitivity to emotional
expressions was not associated with impulsivity and inaccurate responding in the BPD group.
Given that the stimuli were not randomly presented but morphed starting from neutral,
impulsiveness could still play a role in patients’ response styles on this task. Overall, the results
of these studies provide mixed findings for the nature of recognition at milder intensities of
emotion in BPD and how this is related to emotional sensitivity.
1.5 Limitations of Previous Research
There are several limitations to previous studies of emotion perception in BPD. First, most
patient samples contained high levels of diagnostic comorbidity, particularly with mood and
anxiety disorders. Very few of these studies incorporated symptom rating scales at the time of
testing to evaluate possible state-related biases in emotion perception. Second, given that many
studies used the POFA, it is important to consider ceiling effects associated with these stimuli
and the lack of ethnically diverse actors. Third, although patients with BPD have been shown to
be less accurate than healthy individuals in recognizing specific facial displays of emotion, most
patients were at or above 80% accuracy on these tasks. This suggests a subtle deficit as opposed
to a frank impairment in emotion recognition. Fourth, the instructional sets used for facial

11
emotion recognition tasks are important to consider as they may impact the relative emphasis
given to accuracy versus speed, which could lead to systematic biases in test findings. Although
most emotion perception studies place an emphasis on both speed and accuracy, patients with
BPD might employ a strategy that maximizes the quickness of their responses while sacrificing
accuracy. The results of our recent meta-analysis on this topic, however, suggests that this is
likely not the case, as patients were found to be both slower to respond to stimuli and less
accurate in their performances (Daros et al., 2012). Nevertheless, future work should consider
the effects of emphasizing accuracy over speed, or allowing unlimited time to respond, to
determine whether patients with BPD show these subtle deficits in facial emotion perception
under different task conditions.
1.6 The Present Study
The current study seeks to clarify the manner in which individuals with BPD respond to positive,
neutral, and negative facial expressions by taking advantage of a computerized test that assesses
the recognition of emotional facial stimuli presented to participants. This test effectively
combines two areas of perception research (emotion recognition and acuity) because it
determines if participants can recognize and classify varying intensities of three facial
expressions (happy, neutral, and sad). Therefore, it will illuminate the ways in which patients
with BPD may interpret milder expressions of happiness and sadness, as well as examine full-
threshold stimuli. A significant limitation of previous research is that the error patterns on neutral
stimuli are not reported, making it difficult to determine whether BPD patients are misattributing
a positive or negative emotion to these faces. The current study will provide a detailed
assessment of these responses to determine if there are any systematic biases in BPD patients’
responses to these trials. Given that most research on emotion perception in BPD has not

12
examined the relationship of mood state with performance on emotion tasks, the current study
will also examine the potential contribution of current depressive symptomatology on emotional
acuity in BPD.
The specific hypotheses for this study are as follows: (1) Patients with BPD will not differ from
healthy controls in the recognition of very expressive happy and sad faces, however, accuracy at
recognizing neutral expressions is expected to differ significantly, in concordance with earlier
meta-analytic findings. (2) Current mood state, particularly in the form of depressive symptoms,
is expected to be significantly associated with emotion recognition performance in patients with
BPD. This finding was expected to relate only to emotions of positive valence (i.e., very happy
and mild happy expressions) given that mood-congruent biases demonstrated by clinically and
non-clinically depressed samples typically involve decreased recognition accuracy on positive
emotions (Bourke, Douglas, & Porter, 2010; Gray et al., 2006; Surguladze et al., 2004). (3)
Finally, it was expected that BPD would report negative emotional expressions for faces
displaying no emotion (i.e., neutral faces) consistent with literature reporting a negative bias
upon viewing neutral facial stimuli (Dyck et al., 2009; Wagner & Linehan, 1999). In addition to
these specific hypotheses, exploration was planned to determine whether emotion sensitivity
could be demonstrated using the measures in the study.

13
Chapter 2
Method 2
2.1 Participants
As part of a larger study of neurocognitive functioning in individuals with BPD, participants
were enrolled through the Clinical Neurosciences Laboratory at the University of Toronto
Scarborough. They were recruited from the Borderline Personality Disorder outpatient clinic at
the Center for Addiction and Mental Health as well as through online and print advertisements in
Toronto, Canada. Participants were selected for inclusion in this study if criteria were met for
BPD according to the Fourth Edition of the Diagnostic and Statistical Manual of Mental
Disorders (DSM-IV; American Psychiatric Association, 2000). Additional inclusion criteria for
BPD patients were as follows: at least 18 years old at the time of recruitment, English-speaking,
and able and willing to provide written informed consent to participate in this study. Exclusion
criteria included a history of schizophrenia or any psychotic disorder, bipolar I disorder, current
alcohol or non-alcohol substance use disorder, lifetime eating disorder requiring hospitalization,
mental retardation (IQ < 70), any neurological or severe somatic disorder, and significant head
trauma.
Healthy controls were matched to patients with BPD by age, gender, and education. They were
recruited from the community through print and online advertisements. Inclusion criteria for
healthy controls were the following: at least 18 years old at the time of recruitment, English-
speaking, and able and willing to provide written informed consent. Exclusion criteria included
any personal or family history (first- and second-degree relatives) of psychiatric illness, medical
and neurologic illness that could affect brain functioning (e.g., hypothyroidism, seizure disorder,

14
dementia), significant head trauma, and a history of learning or developmental disorders (e.g.,
attention-deficit disorder, autism).
This study received approval from the Research Ethics Board at the Centre for Addiction and
Mental Health and the University of Toronto. Potential participants completed an initial phone
screen to assess the inclusion and exclusion criteria. Eligible individuals were invited to visit the
University of Toronto Scarborough where all procedures took place. After a complete
description of the study, individuals provided written informed consent to participate in the
research protocol. Participants were required to provide a negative urine toxicology screen on the
day of testing before completing the laboratory procedures. They were compensated up to $100
for their participation.
2.2 Measures
All participants completed semi-structured diagnostic interviews administered by bachelor- and
doctoral-level diagnostic interviewers trained to reliably administer these measures and were
directly supervised by a licensed clinical psychologist (ACR). Interviews were conducted
without knowledge of the status of the recruited individual (i.e., whether they were a patient or
healthy control). Narratives for each participant were prepared based on all of the available
information obtained during the interviews and discussed in a diagnostic consensus meeting with
multiple diagnostic interviewers in attendance.
2.2.1 Diagnostic Interviews
The Structural Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-I/P; First,
Spitzer, Gibbon, & Williams, 2002) is a diagnostic interview to assess major psychiatric
disorders in terms of categorical constructs. Multiple studies have found the reliabilities of Axis I

15
diagnoses to be good, although there are differences based on the psychiatric condition (e.g.,
Lobbestael, Leurgans, & Arntz, 2011; Skre, Onstad, Torgersen, & Kringlen, 1991). The SCID-
I/P has also demonstrated superior validity over other standard interviews at clinical intake sites
(e.g., Basco et al., 2000; Fennig, Naisberg-Fennig, Craig, Tanenberg-Karant, & Bromet, 1996).
The Structured Interview for DSM-IV Personality (SIDP-IV; Pfohl, Blum, & Zimmerman, 1997)
is a reliable, semi-structured interview designed to assess for DSM-IV Axis II disorders with
good interrater reliability and validity (Jane, Pagan, Turkheimer, Fiedler, & Oltmanns, 2006). In
accordance with the test manual, a personality disorder diagnosis was made when the diagnostic
criteria were met for at least the past five years and did not occur exclusively during the course
of an Axis I disorder.
2.2.2 Self-Report Measures
Severity of current depressive symptoms was assessed by the Beck Depression Inventory (BDI-
II; Beck, Steer, & Brown, 1996), a 21-item scale with ratings from zero to three. Responses are
summed to reflect the severity of depression over the past two weeks. The BDI-II has
demonstrated good reliability and validity in clinical samples (A. T. Beck, Steer, Ball, & Ranieri,
1996).
2.2.3 Neuropsychological Measures
The Victoria Symptom Validity Test (VSVT; Slick, Hopp, Strauss, & Thompson, 1997) is a test
used to measure the level of effort participants put forward during the testing session. Unusually
poor performance on this task may reflect poor effort, deliberate feigning, exaggeration of real
cognitive deficits, or any combination of the above. Participants were included only if their

16
VSVT scores were within the valid range based on normative data.
To rule out any discrepancies based on intelligence that may arise on emotion perception tasks,
all participants completed the Wechsler Test of Adult Reading (WTAR; Wechsler, 2002),
designed as a tool for estimating intellectual functioning (IQ) of adults aged 16-89. The WTAR
is normed on a nationally representative, stratified American sample, has excellent test-retest
reliability, and extensive research supporting its validity.
The Benton Facial Recognition Test, Short Form (BFRT; Benton, Sivan, Hamsher, Varney, &
Spreen, 1983) was used to evaluate basic facial recognition capacities. The BFRT requires
participants to match a target face with up to three pictures of the same person in a six-stimuli
array of faces that vary in terms of angles and lighting. Short form scores were transformed into
full-scale age-corrected scores using normative data provided in Benton et al. (1983).
2.2.4 Penn Emotional Acuity Test
The Penn Emotional Acuity Test (PEAT) is a subtest of the University of Pennsylvania
Computerized Neurocognitive Test Battery (PennCNP) and is described as a “measurement of
emotional recognition and discrimination” (Erwin et al., 1992; Gur et al., 1992; Gur et al., 2002).
The PEAT presents 40 faces, one at a time, composed of variably happy, sad, and neutral faces
balanced for gender (Sachs, Steger-Wuchse, Kryspin-Exner, Gur, & Katschnig, 2004). The
presentation takes place in two randomly presented blocks, the first of which contains sad and
neutral faces (sad-neutral block) and the second contains happy and neutral faces (happy-neutral
block). The instructions are as follows: “In this test you will see some faces. Look carefully at
each face and decide if the face is happy, sad, or neutral. Use the seven-point scale you see
below to indicate your rating.” The seven-point Likert scale is forced-choice and consists of the

17
following options: very happy, moderately happy, slightly happy, neutral, slightly sad,
moderately sad, and very sad. There is a brief practice session of five faces that follows the
instructions and precedes the forty trials. Outcome measures include the accuracy and RT for
overall performance and five collapsed emotion categories: very happy, mildly happy, neutral,
mildly sad, and very sad. In addition, responses per item were compiled to determine average
deviations from the correct score.
2.3 Statistical Plan
Differences between groups were assessed using Chi-square and independent samples t-tests. A
demographic matching process was used and therefore groups were not expected to significantly
differ in terms of age, gender, education, intelligence, or accuracy on the BFRT. Accuracies and
RTs were considered for six variables on the PEAT, the overall total and subcategories of very
happy, mild happy, neutral, mild sad, and very sad. An independent samples t-test was used to
examine performance differences for the overall PEAT statistics. A 2 X 5 MANOVA (group x
emotion categorization) was used along with independent samples t-tests to determine significant
differences between groups for subcategories of accuracy. Answers on the PEAT were then
arranged into a response matrix to determine whether the response patterns differed between
groups. The interpretation of significant group differences was aided by the calculation of
Cohen’s d, measured as the difference between the two raw means divided by the pooled
standard deviation (SD). Cohen (1988) provided guidance for interpreting effect size statistics
(d) as small (0.2), medium (0.5) and large (≥ 0.8).
Secondary analyses explored the relationship of current moods and performance on the PEAT.
Pearson’s and Spearman’s correlations were utilized to determine the relationships between
variables (e.g., the relationship between overall score on the PEAT and BDI scores). The

18
contribution of Axis I comorbid diagnoses were examined using t-tests for within-group patient
comparisons. Multiple regressions were used to test whether mediation was occurring in the
relationship between BPD and emotion perception performance. Consideration to the
assumptions of normality and heterogeneity were undertaken using a variety of statistical tests.
Variables were analyzed for normality using the Shapiro-Wilk test. Differences between groups
were tested under the assumption of non-normality using non-parametric tests such as the Mann-
Whitney U and Kruskal-Wallis in order to determine if the direction of significance would be
affected. Finally, Spearman’s correlations were used to determine if ranking the data would
significantly alter its association with other variables under an assumption of non-normality.

19
Chapter 3
Results 3
3.1 Demographic and Clinical Characteristics
Demographic information for the BPD patient sample and IQ- and demographically-matched
healthy controls is presented in Table 2. There were no differences between the groups in age,
gender, education or IQ. Patients with BPD and healthy controls performed within the average
range with regard to single-word reading (WTAR) and facial recognition (BFRT). With regard to
clinical characteristics, patients with BPD were more depressed than controls, reporting
moderate levels of depression on average (M = 27.03, SD = 9.76) on the BDI (Beck et al., 1996).
At the time of the study, 89.3% of the patient sample had a history of inpatient hospitalization.
Most patients (89.3%) had completed one or more outpatient treatment programs. Current rates
of psychotropic medication use among patients were as follows: sedatives (34.5%), stimulants
(13.8%), minor tranquilizers (6.9%), antidepressants (62.1%), neuroleptics (10.3%), and mood
stabilizers (20.7%). Table 3 lists the frequencies of Axis I comorbidities for individuals with
BPD. The most common comorbid condition was MDD, with a substantial proportion of patients
in a current episode (40.0%). Other remarkable diagnostic comorbidities included a history of
past substance dependence (33.3%), PTSD (30.0%), eating disorders (26.3%), and anxiety
disorders (23.3%).
3.2 PEAT Accuracy
The total correct (TC) score on the PEAT was calculated using individual answers collapsed into
five categories of response: very happy (VHC), mild happy (MHC), neutral (NC), mild sad
(MSC), and very sad (VSC). Following the scoring guidelines for this task, the two most extreme

20
categories of emotion stimuli comprised two levels of intensity (“very” and “moderately”) that
were combined into one category (“very”). Responses to all stimuli corresponding to these two
intensities were scored as correct if either response was selected.
Overall, patients with BPD were less accurate than controls on the PEAT, t(55) = -2.92, p =
.005, d = .77. A MANOVA examining differences for patients and controls by emotional
intensity category (VHC, MHC, NC, MSC, VSC) was statistically significant, F(5,51) = 3.19, p
= .01. Post-hoc t-tests revealed comparable accuracy between patients and controls for the
categories VHC, MSC, and VSC (all p’s > .55; see Table 4). Patients did, however, score
significantly worse on NC (t(55) = -2.26, p = .03, d = .60), and MHC (t(55) = -2.38, p = .02, d
=.63) when compared to controls.
To explore the patterns of errors that patients with BPD made for each of the emotional intensity
categories, a classification matrix was generated that presents the frequency with which each
response was selected for each respective category of stimuli (see Table 5 and Figure 1). BPD
patients were more than three times more likely to perceive MHC stimuli as more extreme (i.e.,
selecting VHC) than healthy controls. For the NC category, patients appeared to perceive any
emotion (i.e., this finding was not valence-specific) by selecting either MHC or MSC for these
trials.
3.3 Analysis of Current Mood
BDI scores were moderately and significantly correlated with lower overall accuracy on the
PEAT (r = -0.43, p = .001), suggesting that more severe current depression is associated with
poorer recognition of emotional intensities, at least with regard to happy, neutral and sad facial
expressions. Given that BPD is also associated with increased depressive symptomatology,

21
mediation analyses were explored to understand the role of current depression in possibly
mediating the relationship between group status (i.e., patients versus control) and overall
performance accuracy on the PEAT. Following the guidelines presented in Baron and Kenny
(1986), multiple regression analyses were performed using TC on the PEAT as the dependent
variable in relationship to group status and BDI score. The variables TC, group status, and BDI
total were significantly correlated with each other (Figure 2A). In Step 1 of the mediation model,
the regression of TC on BPD status, without including the possible mediator of current
depression, was significant, β = -2.67, t(55) = -2.92, p = .005. Step 2 demonstrated that the
regression of TC on current depression also was significant, β = -0.10, t(55) = -3.34, p = .002.
Step 3 of the mediation analysis demonstrated that current depression, controlling for BPD
status, was no longer statistically significant, β = -0.11, t(55) = -1.75, p = .09. The results of this
analysis did not satisfy the requirements of mediation and therefore the association between BPD
diagnosis and poorer overall recognition accuracy on the PEAT did not appear to be mediated by
current depression severity.
When the same process was followed above for NC as the dependent variable, mediation status
was not achieved (Figure 2B). On the other hand, depression was found to be a significant
mediator of the relationship between group status and poorer accuracy on MHC (see Figure 2C).
In Step 1 of the mediation model, the regression of BPD status on MHC status, without including
the possible mediator of current depression, was significant, β = -0.67, t(55) = -2.38, p = .02.
Step 2 demonstrated that the regression of current depression on MHC was also significant, β = -
5.07, t(55) = -3.06, p = .003. Step 3 of the mediation analysis demonstrated that current
depression, controlling for BPD status, was significant, β = -0.04, t(55) = -2.00, p = .05 and that
the effect of the original variable, BPD group status, was no longer significant (β = 0.34, t(55) =

22
0.60, p = .55). Sobel’s test statistic confirmed the finding of mediation for MHC, t = 2.47 (p <
.01).
3.4 Secondary Analyses
3.4.1 Reaction Time
To achieve normality, RT data were transformed using a square root function of the raw data.
Additionally, three outliers were removed from the patient sample because their scores were
more than three standard deviations above the mean. Although there were no significant
differences with respect to RT, F(1,55) = 0.14, p = .71, analysis of standardized effect sizes
revealed that patients with BPD were faster, on average, across correct trials for all emotional
intensities and valences, t(52) = -0.46, p = .67, d = .12 (Table 6). The largest differences were
seen on VSC trials (d = .38) and MHC (d = .28).
3.4.2 Comorbidity and Psychotropic Medications
There were no differences in overall PEAT accuracy between patients with current MDD and
those without, t(28) = -0.07, p = .94. Similarly, neither a history of PTSD nor substance
dependence was associated with overall performance differences on the PEAT (all p’s > .16).
Patients currently using antidepressant medication were significantly less accurate in recognizing
VHC, t(27) = -2.43, p = .02, and VSC facial expressions, t(27) = -2.06, p = .05, as compared to
those not currently taking these medications.

23
Chapter 4
Discussion 4The present study utilized an established test to determine how patients with BPD and healthy
individuals perceive emotions corresponding to three valences (happy, neutral, and sad) in both
mild and more extreme intensities. This study advanced previous research by accounting for
current mood state and comparing error patterns made by both BPD patients and healthy
controls. Groups were tightly matched on age, education, gender, and IQ. The patient sample
was clinically stable but reported more symptoms of depression than controls, which fell within
the moderate range of severity (Beck et al., 1996).
Several important findings were revealed with the PEAT, a measure of emotion recognition for
happy, neutral, and sad facial expressions at varying levels of emotional intensity. Overall
accuracy on the task differed significantly between the groups, with healthy controls performing
more accurately than patients with BPD. Further inspection of the emotional intensities revealed
that patients were less accurate in recognizing mildly happy and neutral stimuli. On the other
hand, patients with BPD showed comparable levels of recognition accuracy for the emotions at
100% intensity (i.e., very sad and very happy). These results are consistent with a recent meta-
analysis in which patients with BPD were not found to significantly differ from controls in the
recognition of happy and sad expressions (at 100% intensity), but a large effect size difference
for reduced accuracy in recognizing neutral faces (Daros et al., 2012). This difficulty in
recognizing neutral expressions in patients with BPD has now been replicated across multiple
studies using a variety of methodologies. Several studies on emotion recognition have found
decreased accuracy on neutral facial expressions specifically (Bland et al., 2004; Dyck et al.,

24
2009; Levine et al., 1997; Wagner & Linehan, 1999). In addition, previous research suggests that
patients with BPD have more trouble understanding mixed valence feelings and have an inability
to synthesize both positive and negative feelings about themselves and others (Levine et al.,
1997). Individuals with BPD are also known to misinterpret ambiguous social cues more
negatively (Wagner & Linehan, 1999) and process neutral information in a negatively biased
way (Meyer, Pilkonis, & Beevers, 2004). Collectively, the findings of the present study support
the notion that patients with BPD misinterpret neutral stimuli and are more likely to ascribe a
particular valence to them.
This study is among the first to characterize the pattern of errors patients with BPD made on the
PEAT. For mildly happy stimuli, patients with BPD were more likely to select a response in the
direction of a higher intensity of happiness. Patients were more likely than controls to select
mildly happy or mildly sad responses to neutral faces as compared to healthy controls. This latter
finding was not specific to a particular valence, which was unexpected given that individuals
with BPD are thought to process neutral stimuli in a more negatively biased manner (Dyck et al.,
2009; Korfine & Hooley, 2000; Levine et al., 1997; Meyer et al., 2004; Wagner & Linehan,
1999). Specifically, two previous studies of emotion recognition in BPD found evidence for a
negative perceptual bias for neutral stimuli, although the response options did not include milder
intensities of emotions (Dyck et al., 2009; Levine et al., 1997). The misperception of neutral
stimuli as being more positive or negative suggests that patients with BPD may not necessarily
have a bias towards a specific emotional valence (i.e., they may show an affectively non-specific
perceptual aberration for neutral faces). This non-specificity with regards to selection of
emotional valence may reflect the increased tendency that individuals with BPD experience
emotional extremes of both valences (Buie & Adler, 1982). Moreover, the emotional sensitivity

25
that underlies many behaviors in BPD may cause individuals with this illness to overreact to
even minor emotional events, and the task of being confronted with salient emotional (or non-
emotional) faces could lead them to become emotionally unstable and perceive emotions in faces
that healthy individuals do not (Lynch et al., 2006).
Prior research on the topic of emotion recognition in BPD is limited to the extent that current
mood state was not reported and could account for emotion perception in biases associated with
this disorder. As previously mentioned, analyses were carried out to explore whether current
depressive symptomatology might mediate the relationship between group status (i.e., BPD
versus healthy control) and performance indices on the PEAT. The results of these analyses
indicated that current depressive symptomatology mediated this relationship for mildly happy
facial expressions but not neutral faces or total accuracy on this task. The finding that depression
may account for BPD patients’ reduced accuracy in recognizing mild happy faces is in some
ways consistent with documented emotion recognition biases in patient with depression (Gray et
al., 2006; Surguladze et al., 2004). These results, however, also depart significantly from
research on depressed samples in two ways. First, research on depressed patients (with no
personality disorder) suggests that happy faces at 100% intensity would be recognized with less
accuracy; however, the moderately depressed BPD patients in this sample recognized these faces
with near perfect accuracy, and there was no difference in performance in this respect when we
compared currently depressed versus euthymic patients with BPD. Second, reviews on emotion
recognition in MDD have generally found a negative bias in depressed individuals where they
tend to rate all expressions as less positive or sadder (Bourke et al., 2010). Individuals with BPD
did not display the negative perceptual bias that would be expected based on research of
depressed individuals. Unexpectedly, these patients were more likely to perceive mild happy

26
faces as more intensely happy (rather than less neutral or sad). Furthermore, they were equally
likely to select positive or negative responses for neutral faces. Consistent with these findings, a
previous study found that while patients with BPD showed moderate levels of depression, they
were actually more adept at recognizing happy facial expressions than healthy controls (Lynch et
al., 2006).
Also contrary to what would be expected in depression, patients with BPD in a previous study
were quicker at recognizing facial expressions more generally (across all valences), which could
suggest that emotional sensitivity in BPD may be independent of current depressive symptoms
(Lynch et al., 2006). In the present study, patients with BPD recorded faster RTs (albeit not
significantly) on correct trials regardless of emotional valence. Patients were also particularly
fast in recognizing very happy and very sad faces, the latter of which could be associated with a
mood-congruent bias for sad faces given that the sample of patients with BPD was moderately
depressed at the time of testing. Post-hoc comparison between individuals who were currently
depressed versus non-depressed, however, found that there was no significant difference between
groups on the RT for very sad stimuli. As further evidence that emotion sensitivity may be
uniquely contributing to the pattern of results obtained in the present study, Lynch and
colleagues (2006) argue that quick and accurate responding to emotional stimuli in patients with
BPD is unlikely to be due to higher depressive symptoms. Previous research has demonstrated
that clinically depressed individuals display longer reaction times compared with non-depressed
individuals on attention-dependent tasks (Farrin, Hull, Unwin, Wykes, & David, 2003; Thomas,
Goudemand, & Rousseaux, 1999). While RTs were not significantly different between groups in
the present study, it appears that there is some evidence for emotional sensitivity. Non-
significantly faster RTs were present for the BPD group, despite moderate levels of depression in

27
the BPD group, which suggests the possible influence of emotion sensitivity on the results
obtained in the present study (i.e., patients with BPD are able to recognize and/or categorize
emotions faster on average).
Diagnostic comorbidity with respect to current MDD, PTSD, or past substance dependence did
not appear to account for the performance differences revealed in primary analyses for the
PEAT. Current antidepressant medication use, however, was associated with lower accuracy in
recognizing very happy and very sad facial expressions. Importantly, there was no difference in
severity of current depression for patients taking antidepressants versus those who were not.
Nevertheless, it should be noted that patients with BPD were commonly taking more than one
psychotropic medication; however, this was difficult to control in order to ensure stability in the
patient group during the testing procedures. Research on the effects of antidepressants on
emotion recognition is sparse; however, one study has suggested that early reversals in the
decreased recognition of happiness after two weeks of antidepressant treatment predicted
symptomatic improvement at six weeks in patients with MDD (Tranter et al., 2009). One further
study suggests that antidepressant use in patients with MDD may normalize emotion recognition
independently of mood state (Anderson et al., 2011). Therefore, patients with MDD may
subjectively report depressive symptoms while antidepressants manipulate affective processing
systems on a biological basis for improved recognition of emotional expressions (particularly
happiness). In the present study, approximately 60% of the patients with BPD were currently
taking antidepressants and performed well on the recognition of very happy stimuli.
Nevertheless, more research is required in order to understand the effects of antidepressant
medications on state-dependent emotion recognition in patients with MDD and BPD.

28
4.1 Strengths and Limitations
A number of strengths and limitations should be noted as they pertain to the current study. First,
the PEAT is limited in that it provides only three emotional valences: happy, sad, and neutral. It
would be important to examine other emotions in mild and extreme intensities in a fashion
similar to the PEAT, especially given findings of reduced accuracy for facial displays of anger
and disgust in patients with BPD (Daros et al., 2012). Importantly, the paradigm employed by
the PEAT to measure acuity of emotion recognition provides important information that differs
from information obtained from emotion threshold paradigms. The latter puts patients in control
of when they subjectively perceive an emotion. This can create problems when recognition rates
for each emotion are compared across participants because some patients may have stopped the
progression through emotional intensities earlier while others may have stopped the sequence at
a higher intensity. The PEAT avoids this by using preset levels of intensity coupled with a
forced-choice selection approach rather than stopping a morphing sequence. Also, by virtue of
examining emotions at varying levels of intensity (and hence difficulty), the PEAT avoids the
ceiling effect common to POFA tasks; no one completed the task in the present study perfectly.
A further strength of the PEAT in comparison to emotion threshold paradigms is the use of
randomized presentations, which more stringently control for impulsivity. A second limitation of
PEAT is the limited number of stimuli in some emotional categories and the large number of
neutral stimuli included in this task. An improved design might incorporate more stimuli for the
mild and extreme expressions, which could improve the reliability of these more extreme ratings
as well as provide a more adequate measure of these emotional intensities for patients with BPD.
Third, a larger sample size might have allowed us to examine specific indices of the PEAT with
greater statistical power (i.e., RT indices). Fourth, these results do not speak to the specificity of

29
our findings to BPD as compared to other related diagnostic entities, such as MDD. Comparisons
of these findings with individuals diagnosed with MDD may help to strengthen the specificity of
our findings regarding mood-state contributions for patients with BPD. Finally, psychotropic
medication use was not controlled in the present study and the patients were shown to have been
taking a wide variety of medications at the time of testing. It is therefore difficult to know how
pharmacologic treatments might impact the present findings.
4.2 Implications and Conclusions
Notwithstanding these limitations, this study provides novel information about emotion
perception abilities in patients with BPD. There are both diagnostic and treatment implications
based on the findings of this study. Diagnostically, tasks such as the PEAT may be better able to
discriminate between patients with BPD, MDD, and comorbid MDD-BPD. Patients with BPD
are specifically less accurate in recognizing neutral and patients with MDD appear to be less
accurate in recognizing happiness in addition to presenting with a negative bias. Taken together,
clinicians and researchers could differentiate between these conditions, in addition to the
comorbid diagnosis of MDD-BPD, with an experimentally constructed task rather than self-
report or interview measures. With regards to treatment implications, an important aspect of
treatment may include understanding and correcting misinterpretations of neutral stimuli. Similar
to Aaron T. Beck’s cognitive-behavioural therapy for depression (Beck, Rush, Shaw, & Emery,
1987), individuals with BPD should explore with their therapist their cognitive appraisals
regarding neutral and negative information. The patient may also greatly benefit from group
discussion involving cognitive restructuring revolving around the interpretation of neutral
stimuli. Learning to understand and appropriately respond to neutral facial stimuli may help
patients with BPD better regulate their social behavior when in the presence of others.

30
In summary, the findings of the present study indicated that individuals with BPD show
comparable performance with regard to accuracy in recognizing very happy and very sad facial
expressions (i.e., 100% intensity) but significantly lower accuracy on neutral expressions as
compared to healthy controls. Patients with BPD were also significantly worse in recognizing
mildly happy facial expressions and the severity of current depressive symptoms appeared to
mediate this relationship. There was no evidence, however, of a negative perceptual bias on the
PEAT. That is, BPD patients rated mildly happy stimuli as more intensely happy and neutral
stimuli as either mildly happy or sad, suggesting that their perceptual bias is unique from the
mood-congruent biases typical in depressed individuals. Finally, there was some evidence BPD
patients were faster in recognizing emotions across nearly all emotion categories of emotion and
intensity, perhaps providing preliminary evidence for increased emotional sensitivity in BPD.
Taken together, these findings advance prior research on the topic of emotion perception in BPD
and suggest important new lines of investigation that may be useful for delineating the nature of
emotion dysregulation in BPD.

31
References
Abela, J. R., Payne, A. V., & Moussaly, N. (2003). Cognitive vulnerability to depression in individuals with borderline personality disorder. Journal of Personality Disorders, 17(4), 319-329.
Adolphs, R. (2002). Neural systems for recognizing emotion. Current Opinion in Neurobiology, 12(2), 169-177. doi: S095943880200301X
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders. 4th Edition. Text Revision. Washington, DC: Author.
Anderson, I. M., Shippen, C., Juhasz, G., Chase, D., Thomas, E., Downey, D., . . . Deakin, J. F. (2011). State-dependent alteration in face emotion recognition in depression. British Journal of Psychiatry, 198(4), 302-308. doi: bjp.bp.110.078139
Arntz, A., & Veen, G. (2001). Evaluations of others by borderline patients. The Journal of Nervous and Mental Disease, 189(8), 513-521.
Basco, R., Bostic, Q., Davies, D., Rush, J., Witte, B., Hendrickse, W., & Barnett, V. (2000). Methods to Improve Diagnostic Accuracy in a Community Mental Health Setting. The American Journal of Psychiatry, 157(10), 1599-1605. doi: 10.1176/appi.ajp.157.10.1599
Beck, A.T., Rush, J., Shaw, B.F., & Emery, G. (1987). Cognitive Therapy of Depression. New York, NY: Guilford Press.
Beck, A. T., Steer, R. A., Ball, R., & Ranieri, W. (1996). Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. Journal of Personality Assessment, 67(3), 588-597. doi: 10.1207/s15327752jpa6703_13
Beck, A.T., Steer, R.A., & Brown, G.K. (1996). Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation.
Benton, A.L., Sivan, A.B., Hamsher, K.S., Varney, N.R., & Spreen, O. (1983). Contribution to Neuropsychological Assessment. New York: Oxford University Press.
Bland, A. R., Williams, C. A., Scharer, K., & Manning, S. (2004). Emotion processing in borderline personality disorders. Issues in Mental Health Nursing, 25(7), 655-672. doi: 10.1080/01612840490486692
Bolte, S., & Poustka, F. (2003). The recognition of facial affect in autistic and schizophrenic subjects and their first-degree relatives. Psychological Medicine, 33(5), 907-915.
Bourke, C., Douglas, K., & Porter, R. (2010). Processing of facial emotion expression in major depression: a review. The Australian and New Zealand Journal of Psychiatry, 44(8), 681-696. doi: 10.3109/00048674.2010.496359

32
Buie, D.H., & Adler, G. (1982). The definitive treatment of borderline personality. International Journal of Psychoanalytical Psychotherapy, 9, 51-87.
Cheavens, J. S., Zachary Rosenthal, M., Daughters, S. B., Nowak, J., Kosson, D., Lynch, T. R., & Lejuez, C. W. (2005). An analogue investigation of the relationships among perceived parental criticism, negative affect, and borderline personality disorder features: the role of thought suppression. Behaviour Research and Therapy, 43(2), 257-268. doi: S0005-7967(04)00050-6
Clarkin, J. F., Widiger, T. A., Frances, A., Hurt, S. W., & Gilmore, M. (1983). Prototypic typology and the borderline personality disorder. Journal of Abnormal Psychology, 92(3), 263-275.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence
Erlbaum Associates.
Comtois, K. A., Russo, J., Snowden, M., Srebnik, D., Ries, R., & Roy-Byrne, P. (2003). Factors associated with high use of public mental health services by persons with borderline personality disorder. Psychiatric Services, 54(8), 1149-1154.
Corcoran, K. M., Woody, S. R., & Tolin, D. F. (2008). Recognition of facial expressions in obsessive-compulsive disorder. Journal of Anxiety Disorders, 22(1), 56-66. doi: S0887-6185(07)00018-7
Cowdry, R. W., Gardner, D. L., O'Leary, K. M., Leibenluft, E., & Rubinow, D. R. (1991). Mood variability: a study of four groups. The American Journal of Psychiatry, 148(11), 1505-1511.
Daros, A. R., Zakzanis, K. K., & Ruocco, A. C. (2012). Facial emotion recognition in Borderline Personality Disorder. Manuscript submitted for publication.
Derntl, B., Seidel, E. M., Kryspin-Exner, I., Hasmann, A., & Dobmeier, M. (2009). Facial emotion recognition in patients with bipolar I and bipolar II disorder. British Journal of Clinical Psychology, 48(4), 363-375. doi: bjcp682
Domes, G., Czieschnek, D., Weidler, F., Berger, C., Fast, K., & Herpertz, S. C. (2008). Recognition of facial affect in Borderline Personality Disorder. Journal of Personality Disorders, 22(2), 135-147. doi: 10.1521/pedi.2008.22.2.135
Domes, G., Schulze, L., & Herpertz, S. C. (2009). Emotion recognition in borderline personality disorder-a review of the literature. Journal of Personality Disorders, 23(1), 6-19. doi: 10.1521/pedi.2009.23.1.6
Donaldson, C., & Lam, D. (2004). Rumination, mood and social problem-solving in major depression. Psychological Medicine, 34(7), 1309-1318.

33
Driessen, M., Herrmann, J., Stahl, K., Zwaan, M., Meier, S., Hill, A., . . . Petersen, D. (2000). Magnetic resonance imaging volumes of the hippocampus and the amygdala in women with borderline personality disorder and early traumatization. Archives of General Psychiatry, 57(12), 1115-1122.
Dyck, M., Habel, U., Slodczyk, J., Schlummer, J., Backes, V., Schneider, F., & Reske, M. (2009). Negative bias in fast emotion discrimination in borderline personality disorder. Psychological Medicine, 39(5), 855-864. doi: 10.1017/S0033291708004273
Ekman, P. (1992). Are there basic emotions? Psychological review, 99(3), 550-553.
Ekman, P., & Friesen, W. V. (1976). Pictures of Facial Affect: Available from http://www.paulekman.com/research_cds.php.
Ekman, P., Levenson, R. W., & Friesen, W. V. (1983). Autonomic nervous system activity distinguishes among emotions. Science, 221(4616), 1208-1210.
Ekman, P., & Matsumoto, D. (1992). Japanese and Caucasian facial expressions of emotion and neutral faces. San Francisco, CA: Authors.
Erwin, R. J., Gur, R. C., Gur, R. E., Skolnick, B., Mawhinney-Hee, M., & Smailis, J. (1992). Facial emotion discrimination: I. Task construction and behavioral findings in normal subjects. Psychiatry Research, 42(3), 231-240.
Farrin, L., Hull, L., Unwin, C., Wykes, T., & David, A. (2003). Effects of depressed mood on objective and subjective measures of attention. The Journal of Neuropsychiatry and Clinical Neuroscience, 15(1), 98-104.
Feinberg, T. E., Rifkin, A., Schaffer, C., & Walker, E. (1986). Facial discrimination and emotional recognition in schizophrenia and affective disorders. Archives of General Psychiatry, 43(3), 276-279.
Fennig, S., Naisberg-Fennig, S., Craig, T. J., Tanenberg-Karant, M., & Bromet, E. J. (1996). Comparison of clinical and research diagnoses of substance use disorders in a first-admission psychotic sample. American Journal of Addictions, 5(1), 40-48.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. (2002). Structured Clinical Interview for DSM-IV Axis I Disorders — Patient Edition (SCID-I/P, 11/2002 revision). New York, NY: Biometrics Research Department, New York State Psychiatric Institute.
Frances, A., Fyer, M., & Clarkin, J. (1986). Personality and suicide. Annals of the New York Academy of Science, 487, 281-293.
Grant, B. F., Chou, S. P., Goldstein, R. B., Huang, B., Stinson, F. S., Saha, T. D., . . . Ruan, W. J. (2008). Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. The Journal of Clinical Psychiatry, 69(4), 533-545.

34
Gray, J., Venn, H., Montagne, B., Murray, L., Burt, M., Frigerio, E., . . . Young, A. H. (2006). Bipolar patients show mood-congruent biases in sensitivity to facial expressions of emotion when exhibiting depressed symptoms, but not when exhibiting manic symptoms. Cognitive Neuropsychiatry, 11(6), 505-520. doi: 769903065
Gur, R. C., Erwin, R. J., Gur, R. E., Zwil, A. S., Heimberg, C., & Kraemer, H. C. (1992). Facial emotion discrimination: II. Behavioral findings in depression. Psychiatry Research, 42(3), 241-251.
Gur, R. C., Sara, R., Hagendoorn, M., Marom, O., Hughett, P., Macy, L., . . . Gur, R. E. (2002). A method for obtaining 3-dimensional facial expressions and its standardization for use in neurocognitive studies. Journal of Neuroscience Methods, 115(2), 137-143. doi: S0165027002000067
Hariri, A. R., Bookheimer, S. Y., & Mazziotta, J. C. (2000). Modulating emotional responses: effects of a neocortical network on the limbic system. Neuroreport, 11(1), 43-48.
Herpertz, S. C., Dietrich, T. M., Wenning, B., Krings, T., Erberich, S. G., Willmes, K., . . . Sass, H. (2001). Evidence of abnormal amygdala functioning in borderline personality disorder: a functional MRI study. Biological Psychiatry, 50(4), 292-298.
Jane, J. S., Pagan, J. L., Turkheimer, E., Fiedler, E. R., & Oltmanns, T. F. (2006). The interrater reliability of the Structured Interview for DSM-IV Personality. Comprehensive Psychiatry, 47(5), 368-375. doi: S0010-440X(06)00023-X
Jovev, M., Chanen, A., Green, M., Cotton, S., Proffitt, T., Coltheart, M., & Jackson, H. (2011). Emotional sensitivity in youth with borderline personality pathology. Psychiatry Research, 187(1-2), 234-240. doi: 10.1016/j.psychres.2010.12.019
Just, N., & Alloy, L. B. (1997). The response styles theory of depression: tests and an extension of the theory. Journal of Abnormal Psychology, 106(2), 221-229.
Koenigsberg, H. W., Harvey, P. D., Mitropoulou, V., Schmeidler, J., New, A. S., Goodman, M., . . . Siever, L. J. (2002). Characterizing affective instability in borderline personality disorder. The American Journal of Psychiatry, 159(5), 784-788.
Koenigsberg, H. W., Siever, L. J., Lee, H., Pizzarello, S., New, A. S., Goodman, M., . . . Prohovnik, I. (2009). Neural correlates of emotion processing in borderline personality disorder. Psychiatry Research, 172(3), 192-199. doi: 10.1016/j.pscychresns.2008.07.010
Kohler, C. G., Turner, T. H., Bilker, W. B., Brensinger, C. M., Siegel, S. J., Kanes, S. J., . . . Gur, R. C. (2003). Facial emotion recognition in schizophrenia: intensity effects and error pattern. The American Journal of Psychiatry, 160(10), 1768-1774.
Kohler, C. G., Turner, T. H., Gur, R. E., & Gur, R. C. (2004). Recognition of facial emotions in neuropsychiatric disorders. CNS Spectrums, 9(4), 267-274.

35
Korfine, L., & Hooley, J. M. (2000). Directed forgetting of emotional stimuli in borderline personality disorder. Journal of Abnormal Psychology, 109(2), 214-221.
Lavender, A., & Watkins, E. (2004). Rumination and future thinking in depression. British Journal of Clinical Psychology, 43(2), 129-142. doi: 10.1348/014466504323088015
Lenzenweger, M. F., & Pastore, R. E. (2007). On determining sensitivity to pain in borderline personality disorder. Archives of General Psychiatry, 64(6), 747-748; author reply 748-749. doi: 10.1001/archpsyc.64.6.747
Levine, D., Marziali, E., & Hood, J. (1997). Emotion processing in borderline personality disorders. The Journal of Nervous and Mental Disease, 185(4), 240-246.
Linehan, M. M. (1993). Cognitive-behavioral treatment for borderline personality disorder. . New York: Guilford Press.
Linehan, M. M. (1995). Understanding Borderline Personality Disorder: The Dialectical Approach. New York: Guilford Press.
Lobbestael, J., Leurgans, M., & Arntz, A. (2011). Inter-rater reliability of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID I) and Axis II Disorders (SCID II). Clinical Psychology and Psychotherapy, 18(1), 75-79.
Lynch, T. R., Rosenthal, M. Z., Kosson, D. S., Cheavens, J. S., Lejuez, C. W., & Blair, R. J. (2006). Heightened sensitivity to facial expressions of emotion in borderline personality disorder. Emotion, 6(4), 647-655. doi: 2006-21788-010
Marsh, A. A., Kozak, M. N., & Ambady, N. (2007). Accurate identification of fear facial expressions predicts prosocial behavior. Emotion, 7(2), 239-251. doi: 2007-06782-002
McGlashan, T. H., Grilo, C. M., Sanislow, C. A., Ralevski, E., Morey, L. C., Gunderson, J. G., . . . Pagano, M. (2005). Two-year prevalence and stability of individual DSM-IV criteria for schizotypal, borderline, avoidant, and obsessive-compulsive personality disorders: toward a hybrid model of axis II disorders. The American Journal of Psychiatry, 162(5), 883-889. doi: 10.1176/appi.ajp.162.5.883
Merkl, A., Ammelburg, N., Aust, S., Roepke, S., Reinecker, H., Trahms, L., . . . Sander, T. (2010). Processing of visual stimuli in borderline personality disorder: a combined behavioural and magnetoencephalographic study. International Journal of Psychophysiology, 78(3), 257-264. doi: 10.1016/j.ijpsycho.2010.08.007
Meyer, B., Pilkonis, P. A., & Beevers, C. G. (2004). What's in a (neutral) face? Personality disorders, attachment styles, and the appraisal of ambiguous social cues. Journal of Personality Disorders, 18(4), 320-336. doi: 10.1521/pedi.18.4.320.40344
Minzenberg, M. J., Poole, J. H., & Vinogradov, S. (2006). Social-emotion recognition in borderline personality disorder. Comprehensive Psychiatry, 47(6), 468-474. doi: 10.1016/j.comppsych.2006.03.005

36
Murphy, F. C., Sahakian, B. J., Rubinsztein, J. S., Michael, A., Rogers, R. D., Robbins, T. W., & Paykel, E. S. (1999). Emotional bias and inhibitory control processes in mania and depression. Psychological Medicine, 29(6), 1307-1321.
Narumoto, J., Yamada, H., Iidaka, T., Sadato, N., Fukui, K., Itoh, H., & Yonekura, Y. (2000). Brain regions involved in verbal or non-verbal aspects of facial emotion recognition. Neuroreport, 11(11), 2571-2576.
Paris, J., Brown, R., & Nowlis, D. (1987). Long-term follow-up of borderline patients in a general hospital. Comprehensive Psychiatry, 28(6), 530-535.
Rector, N. A., Daros, A. R., Bradbury, C. L., & Richter, M. A. (2012). Disgust recognition in obsessive-compulsive disorder: diagnostic comparisons and posttreatment effects. Canadian Journal of Psychiatry, 57(3), 177-183.
Robin, M., Pham-Scottez, A., Curt, F., Dugre-Le Bigre, C., Speranza, M., Sapinho, D., . . . Kedia, G. (2012). Decreased sensitivity to facial emotions in adolescents with Borderline Personality Disorder. Psychiatry Research. doi: S0165-1781(12)00141-2
Rosenthal, M. Z., Cheavens, J. S., Lejuez, C. W., & Lynch, T. R. (2005). Thought suppression mediates the relationship between negative affect and borderline personality disorder symptoms. Behaviour Research and Therapy, 43(9), 1173-1185. doi: 10.1016/j.brat.2004.08.006
Ruocco, A. C., Amirthavasagam, S., Choi-Kain, L. W., & McMain, S.F. (2012). Neural correlates of negative emotionality in borderline personality disorder: An activation-likelihood-estimation meta-analysis. Biological Psychiatry. Epub Aug 17. doi: 10.1016/j.biopsych.2012.07.014
Ruocco, A. C., Amirthavasagam, S., & Zakzanis, K. K. (2012). Amygdala and hippocampal volume reductions as candidate endophenotypes for borderline personality disorder: A meta-analysis of magnetic resonance imaging studies. Psychiatry Research, 201(3), 245-252. doi: 10.1016/j.pscychresns.2012.02.012
Ruocco, A. C., Medaglia, J. D., Ayaz, H., & Chute, D. L. (2010). Abnormal prefrontal cortical response during affective processing in borderline personality disorder. Psychiatry Research, 182(2), 117-122. doi: S0925-4927(10)00036-3
Russell, J. J., Moskowitz, D. S., Zuroff, D. C., Sookman, D., & Paris, J. (2007). Stability and variability of affective experience and interpersonal behavior in borderline personality disorder. Journal of Abnormal Psychology, 116(3), 578-588. doi: 2007-11737-014
Sachs, G., Steger-Wuchse, D., Kryspin-Exner, I., Gur, R. C., & Katschnig, H. (2004). Facial recognition deficits and cognition in schizophrenia. Schizophrenia Research, 68(1), 27-35. doi: 10.1016/S0920-9964(03)00131-2

37
Schmahl, C., Bohus, M., Esposito, F., Treede, R. D., Di Salle, F., Greffrath, W., . . . Seifritz, E. (2006). Neural correlates of antinociception in borderline personality disorder. Archives of General Psychiatry, 63(6), 659-667. doi: 10.1001/archpsyc.63.6.659
Schmahl, C. G., Vermetten, E., Elzinga, B. M., & Bremner, J.D. (2003). Magnetic resonance imaging of hippocampal and amygdala volume in women with childhood abuse and borderline personality disorder. Psychiatry Research, 122(3), 193-198.
Schneider, F., Gur, R. C., Koch, K., Backes, V., Amunts, K., Shah, N. J., . . . Habel, U. (2006). Impairment in the specificity of emotion processing in schizophrenia. American Journal of Psychiatry, 163(3), 442-447. doi: 163/3/442
Selby, E. A., & Joiner, T. E., Jr. (2009). Cascades of Emotion: The Emergence of Borderline Personality Disorder from Emotional and Behavioral Dysregulation. Review of General Psychology, 13(3), 219. doi: 10.1037/a0015687
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger, T. A., Livesley, W. J., & Siever, L. J. (2002). The borderline diagnosis I: psychopathology, comorbidity, and personality structure. Biological Psychiatry, 51(12), 936-950.
Skre, I., Onstad, S., Torgersen, S., & Kringlen, E. (1991). High interrater reliability for the Structured Clinical Interview for DSM-III-R Axis I (SCID-I). Acta Psychiatrica Scandinavica, 84(2), 167-173.
Slick, D., Hopp, G., Strauss, E., & Thompson, G. (1997). The Victoria symptom validity test. Odessa, FL: Psychological Assessment Resources.
Soloff, P. H., Lynch, K. G., & Kelly, T. M. (2002). Childhood abuse as a risk factor for suicidal behavior in borderline personality disorder. Journal of Personality Disorders, 16(3), 201-214.
Soloff, P. H., Lynch, K. G., Kelly, T. M., Malone, K. M., & Mann, J. J. (2000). Characteristics of suicide attempts of patients with major depressive episode and borderline personality disorder: a comparative study. The American Journal of Psychiatry, 157(4), 601-608.
Surguladze, S. A., Young, A. W., Senior, C., Brebion, G., Travis, M. J., & Phillips, M. L. (2004). Recognition accuracy and response bias to happy and sad facial expressions in patients with major depression. Neuropsychology, 18(2), 212-218. doi: 10.1037/0894-4105.18.2.212
Tebartz van Elst, L., Hesslinger, B., Thiel, T., Geiger, E., Haegele, K., Lemieux, L., . . . Ebert, D. (2003). Frontolimbic brain abnormalities in patients with borderline personality disorder: a volumetric magnetic resonance imaging study. Biological Psychiatry, 54(2), 163-171.
Thomas, P., Goudemand, M., & Rousseaux, M. (1999). Attentional resources in major depression. European Archlives of Psychiatry and Clinical Neuroscience, 249(2), 79-85.

38
Torgersen, S., Kringlen, E., & Cramer, V. (2001). The prevalence of personality disorders in a community sample. Archives of General Psychiatry, 58(6), 590-596.
Tranter, R., Bell, D., Gutting, P., Harmer, C., Healy, D., & Anderson, I. M. (2009). The effect of serotonergic and noradrenergic antidepressants on face emotion processing in depressed patients. Journal of Affective Disorders, 118(1-3), 87-93. doi: S0165-0327(09)00050-0
Trull, T. J., Solhan, M. B., Tragesser, S. L., Jahng, S., Wood, P. K., Piasecki, T. M., & Watson, D. (2008). Affective instability: measuring a core feature of borderline personality disorder with ecological momentary assessment. Journal of Abnormal Psychology, 117(3), 647-661. doi: 2008-11014-013
Unoka, Z., Fogd, D., Fuzy, M., & Csukly, G. (2011). Misreading the facial signs: specific impairments and error patterns in recognition of facial emotions with negative valence in borderline personality disorder. Psychiatry Research, 189(3), 419-425. doi: 10.1016/j.psychres.2011.02.010
von Ceumern-Lindenstjerna, I. A., Brunner, R., Parzer, P., Frey, M., Fiedler, P., & Resch, F. (2007). Wahrnehmung und Bewertung von emotionalen Gesichtsausdruken bei weiblichen Jugendlichen mit einer Borderline-Personlichkeitsstorung. Zeitschrift fur Kinder- und Jugendpsychiatrie und Psychotherapie, 35(5), 333-340. doi: 10.1024/1422-4917.35.5.333
von Ceumern-Lindenstjerna, I. A., Brunner, R., Parzer, P., Mundt, C., Fiedler, P., & Resch, F. (2010). Attentional bias in later stages of emotional information processing in female adolescents with borderline personality disorder. Psychopathology, 43(1), 25-32. doi: 000255960
Wagner, A. W., & Linehan, M. M. (1999). Facial expression recognition ability among women with borderline personality disorder: implications for emotion regulation? Journal of Personality Disorders, 13(4), 329-344.
Watkins, P. C., Vache, K., Verney, S. P., Muller, S., & Mathews, A. (1996). Unconscious mood-congruent memory bias in depression. Journal of Abnormal Psychology, 105(1), 34-41.
Wechsler, D. (2002). WTAR: Wechsler Test of Adult Reading. Manual. San Antonio, TX: The Psychological Corporation.
Yen, S., Zlotnick, C., & Costello, E. (2002). Affect regulation in women with borderline personality disorder traits. The Journal of Nervous and Mental Disease, 190(10), 693-696. doi: 10.1097/01.NMD.0000034744.11140.99
Zanarini, M. C., & Frankenburg, F. R. (2007). The essential nature of borderline psychopathology. Journal of Personality Disorders, 21(5), 518-535. doi: 10.1521/pedi.2007.21.5.518
Zimmerman, M., & Mattia, J. I. (1999). Axis I diagnostic comorbidity and borderline personality disorder. Comprensive Psychiatry, 40, 245-252.

39
Zisook, S., Goff, A., Sledge, P., & Shuchter, S. R. (1994). Reported suicidal behavior and current suicidal ideation in a psychiatric outpatient clinic. Annals of Clinical Psychiatry, 6(1), 27-31.

40
Tables
Table 1
Description of Emotion Perception Tasks
Emotion Recognition Emotion Discrimination Emotional Acuity
Goal of Task Identification of an
emotion known from previous experience.
Understanding the difference between one emotion and another.
Determine the sharpness of recognition for emotional
intensity.
Most Frequent Presentations
(1) Participants are shown series of single
photographs of emotional facial
expressions and the participant is asked to label the emotion in some fashion. It is
important to note that photographs in the
typical emotion recognition task are not
morphed but remain static.
(1) Presentations with singular photos that blend
two emotions (e.g., containing 40% anger and 60% happiness) and asks participants to state which
emotion they see. (2) Presentation of two stimuli at the same time probing
discrimination between the two facial displays of
emotion in various ways. This design is more
flexible.
(1) Neutral faces are incrementally blended
towards a fully expressive target emotion. The
respondent is asked to stop the progression of morphs when they can articulate what emotion is being
displayed. (2) An alternate variant of this task randomly presents morphed stimuli at different levels of saturation, the saliency of the emotional
expression (e.g., 50% neutral, 50% emotion; 10%
neutral, 90% emotion).
Typical Instructions
“What emotion do you see? How does the
person feel?”
“What emotion do you see? Which face displays
an emotion? Which face is angrier? Which face
displays fear (vs. disgust)?”
“When can you tell me the specific emotion that is
forming? When can you start to see an emotion and tell me what emotion that is?”
Response Styles
Open-ended or forced-choice; paper-and-
pencil or computerized
Forced-choice
Computerized
Forced-choice
Computerized

41
Table 2
Demographic and clinical characteristics of patients with borderline personality disorder and healthy controls BPD Group
(n = 30) Healthy Controls
(n = 27)
Variable M SD M SD Statistic p
% Female 93.33 96.30 X2 = 0.25 .62
Age 29.00 (9.34) 27.19 (10.86) t = 0.67 .50
Mean yrs. education 13.83 (2.65) 14.93 (1.96) t = 1.75 .09
FSIQ (WTAR)1 108.55 (7.91) 110.19 (6.16) t = 0.86 .40
BFRT2 47.44 (4.10) 47.37 (5.10) t = 0.05 .96
BDI total 27.03 (9.76) 1.63 (2.12) t = 13.23 <.001 Notes: M = mean; SD = standard deviation.
1FSIQ = Full Scale IQ, based on the WTAR = Wechsler Test of Adult Reading. Standard scores
with M = 100, SD = 15.
2BFRT = Benton Facial Recognition Test. Short-form scores converted to age-corrected long-
form raw scores.

42
Table 3
Clinical characteristics for patients diagnosed with BPD for the present study BPD N
% Medicated 75.86 29
% Antidepressants 62.10 29
% Mood Stabilizers 20.70 29
% Sedatives 34.48 29
% Stimulants 13.79 29
% Neuroleptics 10.34 29
% Minor Tranquilizers 6.90 29
% Major Depression, Past 40.00 30
% Major Depression, Current 40.00 30
% PTSD, Past 20.00 30
% PTSD, Current 10.00 30
% Substance Dependence, Past 33.33 30
% Dysthymia 13.33 30
% Any Anxiety Disorder, Current 23.33 30
% Eating Disorder, Past 26.33 30
Note: One patient’s data was incomplete regarding medication use.

43
Table 4
Accuracy results from the PEAT for BPD and HC BPD (n = 30) HC (n = 27)
Variable M SD M SD t(55) p d
Accuracy
Very Happy (VHC) 4.17 1.32 4.15 1.17 0.06 .97 .02
Mild Happy (MHC) 2.37 1.22 3.04 0.85 -2.38 .02 -.63
Neutral (NC) 15.03 3.53 16.85 2.36 -2.26 .03 -.60
Mild Sad (MSC) 2.77 1.14 2.81 1.33 0.15 .88 .04
Very Sad (VSC) 4.93 1.20 5.11 0.97 0.61 .55 .16
Total Correct1 29.27 3.94 31.96 2.90 -2.92 .01 -.77 Notes: M = mean; SD = standard deviation. d = Cohen’s standardized effect size. 1The subcategories contained the following number of stimuli: VHC = 6, MHC = 4, NC = 20,
MSC = 4, VSC = 6. The total score was out of 40.

44
Table 5
Response patterns based on PEAT stimulus classification
Participant Response
% Respondents VHC MHC NC MSC VSC
Answer 1-2 3 4 5 6-7
VHC BPD 69.44 26.67 3.89 -- --
HC 69.14 29.01 1.85 -- --
MHC BPD 29.17 56.67 14.17 -- --
HC 9.26 75.93 13.89 0.93 --
NC BPD 0.33 10.67 75.83 12.83 0.33
HC -- 6.67 84.26 8.89 0.19
MSC BPD -- 0.83 7.50 70.00 21.67
HC -- 0.93 4.63 70.37 24.07
VSC BPD 0.56 1.11 0.56 15.56 82.22
HC 0.62 -- -- 14.81 84.57

45
Table 6 Reaction Time (RT) results from the PEAT for BPD and HC
BPD (n = 27) HC (n = 27)
M SD M SD t(52)1 p d
Median RT Correct
Very Happy (VHC) 1761.46 450.13 1819.80 393.37 -0.592 .58 -.16
Mild Happy (MHC) 1676.91 463.10 1809.52 495.52 -1.03 .31 -.28
Neutral (NC) 1765.31 530.27 1809.67 638.87 -0.22 .83 -.06
Mild Sad (MSC) 1881.50 560.08 1840.48 647.14 0.33 .74 .09
Very Sad (VSC) 2160.69 796.19 2450.33 794.81 -1.382 .17 -.38
Median RT Correct Total 1786.31 469.51 1830.57 414.47 -0.44 .67 -.12 Notes: M = mean; SD = standard deviation. d = Cohen’s standardized effect size.
1Square root transformation applied before using independent samples t-test.
2 In these cases, one patient in each of these instances got all VHC or VSC incorrect and there
was no correct RT values to be included, df = 51.

46
A
B
Figure 1. Response patterns on (A) mildly happy stimuli and (B) neutral stimuli of the PEAT for
BPD (n = 30) and HC (n = 27) participants.
0%
10%
20%
30%
40%
50%
60%
70%
80%
VHC MHC NC MSC VSC
Perc
ent o
f Res
pond
ents
HC BPD
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
VHC MHC NC MSC VSC
Perc
ent o
f Res
pond
ents
HC
BPD

47
Figure 2. Mediation analyses with BDI score as a mediator and (A) TC score, (B) NC score, (C)
MHC score as dependent variables. The simple correlation (and beta coefficient) for the
association between two variables is represented by r. β1 represents the association for the
mediator, controlling for group status. β2 represents the magnitude of the association between
group status and the dependent variable after the MR with the mediator has been run (* indicates
p < .05).
A
B
C
Sobel’s t: t = 2.47 p < .01