Embed Size (px)
Citation preview

emoryjohnscreek.com
Cover slide
Reduction in Urinary Catheter Utilization
Emory Johns Creek Hospital
Marcia Postal-Ranney, RN, CIC, Infection PreventionKaren Tatoy, RN, Shift Nurse Manager Medical Unit
Lynn Talmadge, RN, Charge Nurse, Emergency Department

emoryjohnscreek.com
Emory Johns Creek Hospital
110 Bed Community Hospital in Johns Creek, GAOpened February 2007Medical Unit Surgical UnitICUWomen’s Services with level 3 NICUCardiac Catheterization lab with PCI
emoryjohnscreek.com
Team Members• Physician Champion
– Brenda Friedman, MD• Administrative Champion- Hassan
Shabbir, MD, Chief Quality Officer• 4 Surgical-
– Roselyn Laxama– Stephanie Liffick
• 3 Medical– Sayea Vardier– Maila Rallos– Karen Tatoy– Anu Thomas– Muta Okparaocha
• Women’s Services– Melissa Donovan– Lydia Balbuena
• ICU– Allison Tomy– Donna Dyer
• Emergency – Lynn Talmadge– Lindsey Meixner
• Infection Prevention– Marcia Postal-Ranney
• Newnan Hospital– Dr. Karen Clarke

emoryjohnscreek.com
Medical Executive Committee Approval
– Physician champion brought indications for indwelling catheter insertion to MEC
– Cardiology Chairman approved guidelines for cardiac patients will not require indwelling catheter for accurate I&O outside of the ICU
– Nephrology Chairman approved guidelines for dialysis patients to not require indwelling catheter for accurate I&O outside of the ICU
– Alternative methods of daily weights and number of wet sheets per day would suffice

emoryjohnscreek.com
Emergency Room Catheter Insertion Indications
Indication for urinary catheter insertion (Why are you inserting this catheter)Check all that apply Hemodynamically unstable Precise measurement of urinary output needed in ICU Acute urinary retention or obstruction Stage three or four sacral decubitus in incontinent patient Select surgical procedures- urinary and GYN Prolonged immobilization End of life care- Hospice Epidural/ Lumbar catheter in place Replacement of current indwelling catheter Continuous bladder irrigation Other-Obtain from provider_________________

emoryjohnscreek.com
Posters for Approved Use of Indwelling Catheters

emoryjohnscreek.com
Daily Review for Necessity
• Hemodynamically unstable- accurate I&O in ICU
• Obstruction of urinary tract• Need to monitor accurate urine output in
ICU• Preoperative catheterization• Urinary tract hemorrhage• Palliative care• Continuous lumbar epidural anesthesia• Incontinent patient with stage III or IV
decubitus• Chronic Foley catheter prior to admission
Appropriate Reasons for Indwelling Catheter
Inappropriate Reasons for Indwelling Catheter
• Nursing convenience• Not checking daily to see if catheter
can be discontinued• Urinary incontinence with no skin
breakdown• No clear reason for placement of
catheter• Intermittent catheterization is
possible• Patient request

emoryjohnscreek.com
Patient Brochure
Laminated card in the patient room explaining the EJCH philosophy for not using an indwelling catheter

emoryjohnscreek.com
Nurse Attitude
• Nurses want to make sure that the patient does not get a CAUTI
• Importance of a faster recovery to get the patient up to bedside commode or toilet
• Purple pad helps by absorbing one liter of fluid without patient feeling wet. Pads improve ease of changing the bed
• SIBR rounds requires nurse to pick a designated indication to keep the indwelling catheter in place
emoryjohnscreek.com
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Jul-12
Aug-12
Sep-12
Oct-12
Nov-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Series1
11.8694362017804
0 7.59493670886076
7.89473684210526
6.9204152249135
0 4.44444444444445
7.26392251815981
2.55102040816327
8.65800865800866
6.13496932515337
5.81395348837209
5.8252427184466
7.14285714285714
12.3711340206186
6 2.58397932816537
0 0 2.69541778975741
4.68384074941452
2.20264317180617
0 4.70588235294118
0 3.46020761245675
3.40136054421769
6.17283950617284
0 0 0 10.1010101010101
3.93700787401575
0 6.0790273556231
0 3.47222222222222
7.96812749003984
3.44827586206897
3.81679389312977
2.75482093663912
1.00
3.00
5.00
7.00
9.00
11.00
13.00
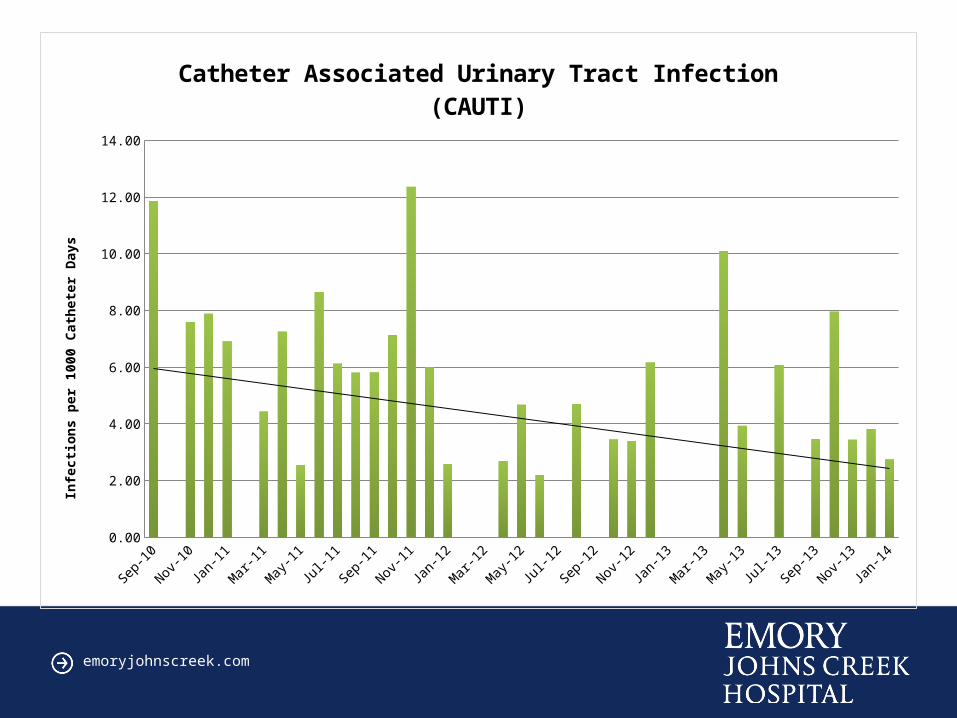
Catheter Associated Urinary Tract Infection (CAUTI)In
fecti
ons p
er 1
000
Cath
eter
Day
s
CAUTI Slide

emoryjohnscreek.com
Urinary Catheter Utilization
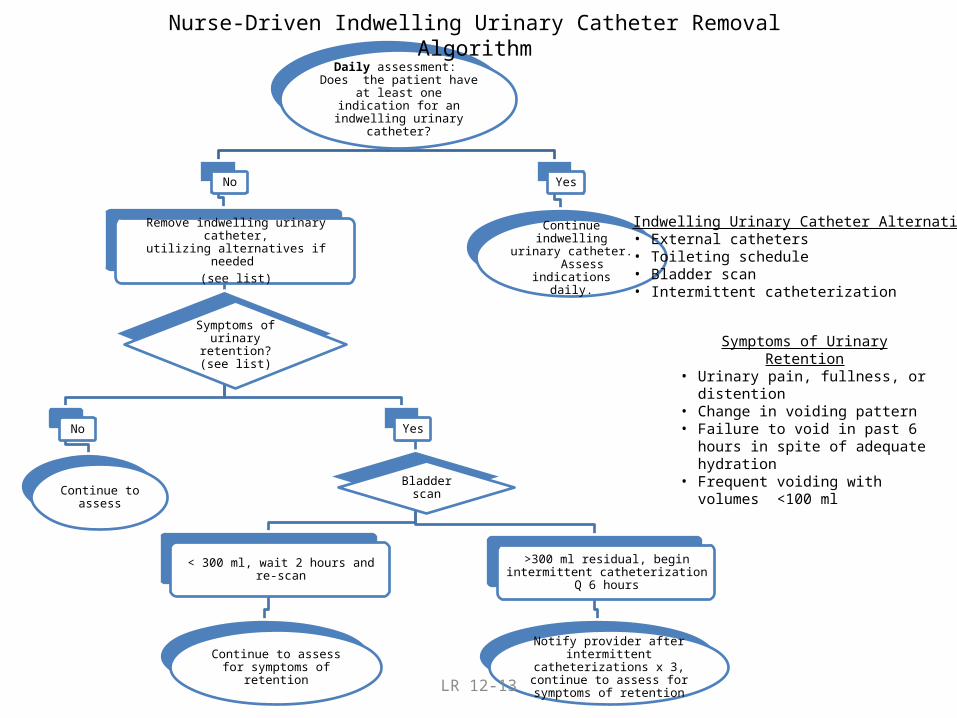
LR 12-13
Daily assessment: Does the patient have at least one
indication for an indwelling urinary catheter?
No
Remove indwelling urinary catheter, utilizing alternatives if needed
(see list)
Symptoms of urinary retention? (see list)
No
Continue to assess
Yes
Bladder scan
< 300 ml, wait 2 hours and re-scan
Continue to assess for symptoms of retention
>300 ml residual, begin intermittent catheterization Q 6 hours
Notify provider after intermittent catheterizations x 3, continue to assess for symptoms of retention
Yes
Continue indwelling urinary catheter. Assess
indications daily.
Nurse-Driven Indwelling Urinary Catheter Removal Algorithm
Symptoms of Urinary Retention• Urinary pain, fullness, or distention• Change in voiding pattern• Failure to void in past 6 hours in spite
of adequate hydration• Frequent voiding with volumes <100
ml
Indwelling Urinary Catheter Alternatives• External catheters• Toileting schedule• Bladder scan• Intermittent catheterization
Catheter Removal Diagram

emoryjohnscreek.com
Ultimate Outcome- culture change
“Many infections are inevitable;
some might be preventable”
“Each infection is potentially preventable, unless proven
otherwise”
• Each adult unit is seeing a reduction in catheter utilization
• Indwelling catheters are not placed immediately in the Emergency Room for every admitted patient
• Staff convenience is no longer a reason for a catheter
• Attitudes changed and staff felt truly concerned when a CAUTI occurred
• Culture was changed to see this and other aspects of preventable harm as a patient safety issue
• Each employee felt committed to personal responsibility for prevention of hospital acquired conditions.