Embed Size (px)
Citation preview

emoryhealthcare.org

emoryhealthcare.org
N.E.W.T. Level
Measurement: Voldemort or Dumbledore?
Georgia Chapter Scientific Meeting
American College of Physicians
Savannah, Georgia
October 6, 2013
Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital
Richard Gitomer, MD, FACP President, CQO and Director of Medical Svcs Emory Healthcare Network

emoryhealthcare.org
OBJECTIVES
• After this session you should be able to:
– Name at least 3 goals of performance measurement
– Describe challenges to validity of measures for
comparison of health care providers
– Articulate ways performance measurement can help
us improve medical practice and the care of patient
populations
• Neither Dr. Spell nor Dr. Gitomer have conflicts of interest

WHAT’S YOUR LEVEL?
1. Practicing physician
2. Resident or fellow
3. Medical student
4. Other
1. 2. 3. 4.
0% 0%0%0%
10

IF IN PRACTICE, WHAT KIND?
1. Solo or small
group (<10)
2. Large group
10 or more)
3. Academic faculty
practice
4. Military or VA
1. 2. 3. 4.
0% 0%0%0%
9

DO YOU HAVE AN EHR THAT IS
MEANINGFUL USE LEVEL 1 CERTIFIED?
1. Yes
2. No
3. Not sure
4. Do not have an EHR
1. 2. 3. 4.
0% 0%0%0%
9
DO YOU PARTICIPATE IN A HEALTH
INFORMATION EXCHANGE?
1. Yes
2. No
3. Not sure
1. 2. 3.
0% 0%0%
9

DO YOU HAVE COMMERCIAL INSURANCE
CONTRACTS WITH COMPENSATION TIED TO
PERFORMANCE ON QUALITY AND/OR COST
MEASURES?
1. Yes
2. No
3. Not sure
4. Does not apply
(military/VA/resident/
fellow)
1. 2. 3. 4.
0% 0%0%0%
9
DO YOU HAVE MEDICAL HOME
CERTIFICATION?
1. Yes
2. No
3. Does not apply
1. 2. 3.
0% 0%0%
9

IN YOUR PRACTICE ARE YOU DOING
IMPROVEMENT WORK USING DATA OTHER
THAN FOR MOC?
1. True
2. False
True False
0%0%
9
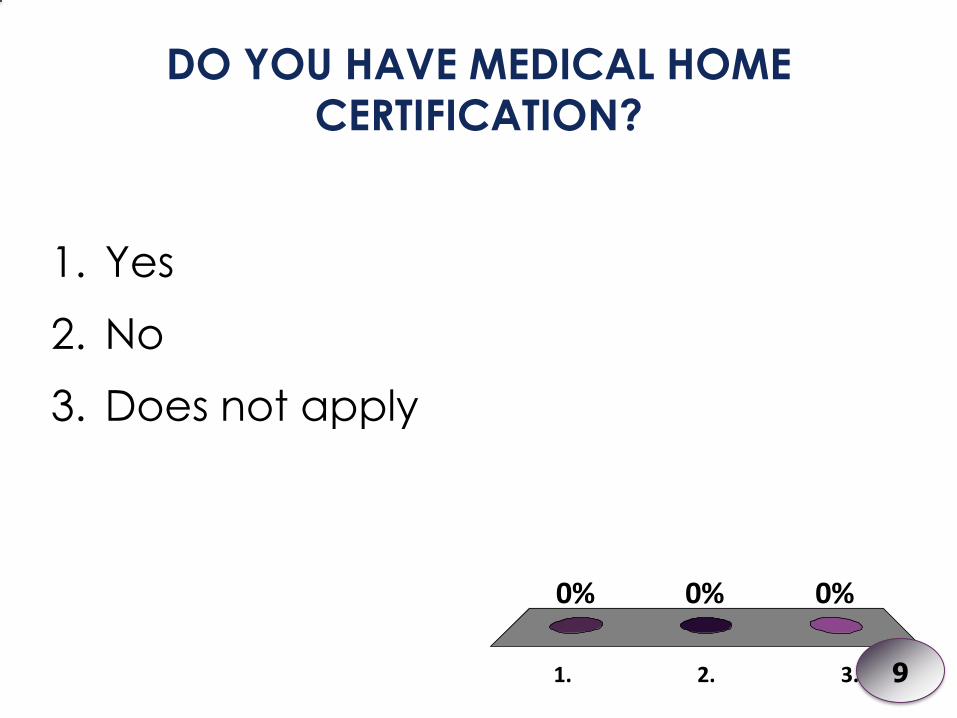
18
CMS Medpar/PQRS
Administrative Data
Abstracted Data
Payors
Q-HIP
physiciancompare.hhs.gov (group practice performance data
coming 2014)
Hospitalcompare.hhs.gov
Clinically Enriched Data from EMR
(near future)

emoryhealthcare.org
DATA SOURCES FOR MEASUREMENT
• Administrative data (billing)
– CPT and ICD-9 codes
– DRG and CPT codes (inpatient HAC, mortality,
readmission, etc.)
• Clinical data
– Discrete electronic v. manually abstracted
• Paid claims data
– Source – insurance company

emoryhealthcare.org
ADMINISTRATIVE DATA
Strengths
• Generated out of our usual
activities
• We have access to what we
have billed
• Incentives for accuracy
through payer audits
(hospital >> ambulatory)
Weaknesses
• Very high level
• Variable degrees of thoroughness across providers – Professional coders may miss
important clinical detail
– Physicians code variably and for different incentives
• Cannot identify valid exceptions to most measures
• Only captures what we billed for

emoryhealthcare.org
CLINICAL DATA
Strengths
• Much richer data
• Gives nuance
• Allows for identifying exceptions to measure compliance
• Discrete, identifiable data elements can be built into EMRs
• Can use prompts for data entry
Weaknesses
• Expensive when manual chart abstraction is required
– Core Measures
– NSQIP, ACC/AHA, etc
– PQRS sampling option
• Current EMRs make data entry awkward and usually increase the amount of time for documentation
• Can be “gamed”
• Only captures what we entered

emoryhealthcare.org
PAID CLAIMS DATA
Strengths
• Generated through
usual activities
• Captures data outside
of our own practice
and health systems
Weaknesses
• Usually unobtainable
by physicians and
health systems
• Accuracy not verifiable
• All the weaknesses of
our own billing data

emoryhealthcare.org
ARE YOU CONSIDERED
MAGICAL OR MUGGLE?

emoryhealthcare.org
RANDOM VARIATION – EFFECTS OF
SAMPLE SIZE ON RATINGS
• Implications?
– Multiple insurers assessing only their covered patients

emoryhealthcare.org
SPECIAL CAUSES OF VARIATION
• Patient factors
– SES, race, proper risk adjustment for comorbidities
• Provider factors
– Billing, coding, charting practices
– Legitimate differences in processes of care

emoryhealthcare.org
CAN WE SEE THE FUTURE OF PUBLIC
REPORTING?
The crystal ball is only
becoming more
transparent
– Performance
– Costs
– Patient experience

emoryhealthcare.org
APPROPRIATE USE OF
MEASURES
• Public reporting
• Public health/disease surveillance
• Payment program
• Regulatory and accreditation programs
• Professional certification or recognition programs
• Quality improvement with benchmarking(external
benchmarking to multiple organizations)
• Quality improvement (internal to specific organization)
www.qualityforum.org

emoryhealthcare.org
PUBLIC REPORTING: AN EMORY EXPERIENCE
VASCULAR CATHETER-ASSOCIATED INFECTION
Location Number Rate* % of
National
Nationwide 6,868 0.367 100%
Emory University Hospital 36 2.313 630%
WellStar Kennestone Hospital 21 1.011 275%
Emory University Hospital Midtown 13 1.045 285%
Atlanta Medical Center 8 1.862 507%
*Events per 1000 Medicare patients

emoryhealthcare.org
NATIONAL INITIATIVES USING MEASURES
CMS HOSPITAL QUALITY • IP Quality • OP Quality • IP Rehab • Long-Term Care • Meaningful Use • Value-Based Purchasing
CMS MD QUALITY • Medicaid Adult • Meaningful Use • PQRS • Value-Based Modifier
OTHER HOSPITAL QUALITY • HHS Hospital Compare • Leapfrog Hospital
OTHER MD QUALITY • NCQA HEDIS Physician • ONC Beacon • Bridges to Excellence
HEALTHPLAN OR SYSTEM • NCQA HEDIS Health Plan • Shared Savings Program

emoryhealthcare.org
CMS PUBLIC REPORTING SITES
www.hospitalcompare.hhs.gov
Medicare Claims MedPAR (Medicare Provider
Analysis & Review)
www.medicare.gov/physiciancompare
CMS PQRS & ePrescribing

emoryhealthcare.org
HEALTHGRADES
www.healthgrades.com
Publically Available Demographics Future: PhysicianCompare
CMS MedPAR & Proprietary Algorithm HospitalCompare
emoryhealthcare.org
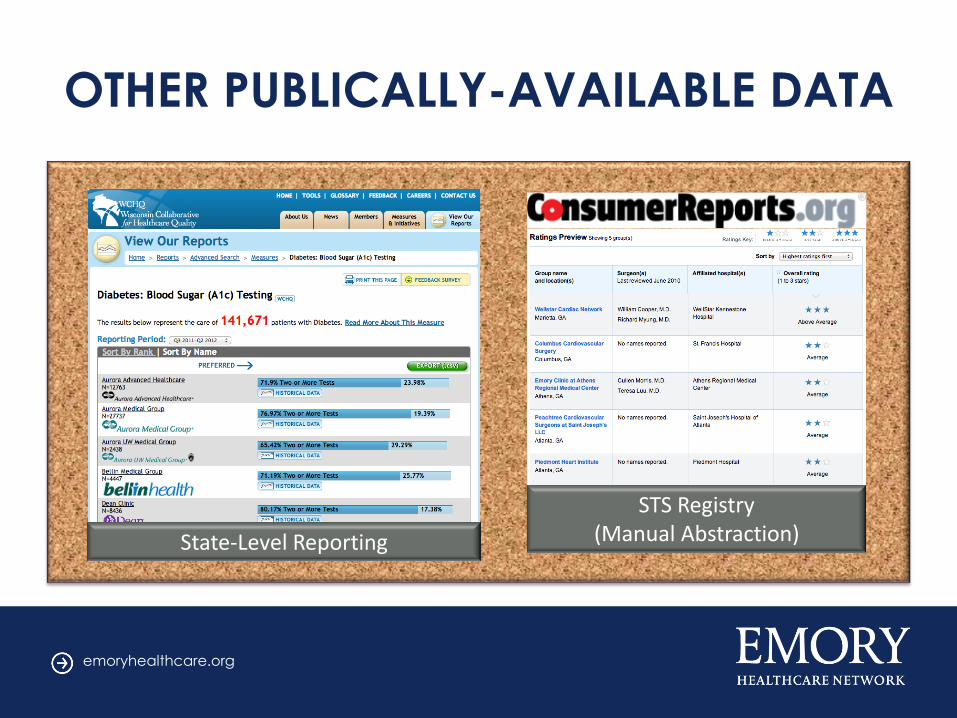
OTHER PUBLICALLY-AVAILABLE DATA
State-Level Reporting
STS Registry (Manual Abstraction)

emoryhealthcare.org
“ACCOUNTABLE CARE”
• Foundational to current healthcare financing strategy
• Legacy from the 1990’s – Perception of rationing
• Purpose of measurement (payout mechanism)
– Ensure quality in the setting of cost-reduction incentives
– Incentivize improved quality
– Discern (pay for) differences between organizations
– Align incentives with payer
– Limit provider payout
• Data availability – administrative vs. EHR

emoryhealthcare.org
COMMERCIAL VALUE CONTRACT
MODEL Cost Target Cost Performance Savings • 30% Available
• 18% Quality • 12% Utilization
VALUE SCORECARD Weighted Scoring Normalized Standards Tiers - % Total Points 50% Quality Threshold Metrics HEDIS • Claims Data • Wellness • Chronic Conditions Utilization Measures

emoryhealthcare.org
SHARED SAVINGS MODEL OF
REIMBURSEMENT C
ost
per
pat
ien
t p
er
year
Time
Distributed based on quality performance
OTHER EXAMPLES: Shared Savings ACO (Pioneer & Shared-Savings ACO) IMPACT: • Larger returns can support substantive infrastructure change. • Diminishing returns over the years.

emoryhealthcare.org
COMMERCIAL VALUE CONTRACT
ACUTE & CHRONIC CONDITIONS
• Rx acute bronchitis • Depression • AMI • CAD • C/V disease • CHF • Diabetes • Med Adherence • Medication monitoring • DMARD • Osteoporosis • Asthma
PREVENTION • Breast cancer screening • Cervical cancer screening • Chlamydia screening • Glaucoma screening
UTILIZATION
• Avoidable ER visits • Ambulatory sensitive
admissions • Generic drug rate
emoryhealthcare.org
PUBLIC REPORTING
BENEFITS
• Focuses quality efforts
• Engenders
organizational will
• Facilitates
transparency
CONSEQUENCES
• Can diffuse focus
• Collection burden
• Inappropriate use for
comparison

Responses remain anonymous!

1. Poor
2. Fair
3. Average
4. Good
5. Excellent
1. 2. 3. 4. 5.
0% 0% 0%0%0%
10

1. Poor
2. Fair
3. Average
4. Good
5. Excellent
Poor
Fair
Aver
age
Good
Excel
lent
0% 0% 0%0%0%
10

0%
0%
0%
10
1. Yes
2. No
3. N/A

1. Poor
2. Fair
3. Average
4. Good
5. Excellent
1. 2. 3. 4. 5.
0% 0% 0%0%0%
10

0%
0%
10
1. Yes
2. No