Embed Size (px)
Citation preview
1
Essential Medicines List (EML) 2015
Application for the inclusion of delamanid in the WHO Model List of Essential Medicines, as a
reserve second‐line drug for the treatment of multidrug‐resistant tuberculosis (complementary
lists of anti‐tuberculosis drugs for use in adults)
General items
1. Summary statement of the proposal for inclusion, change or deletion
This application concerns the updating of section 6.2.4 Antituberculosis medicines in the 2013 edition of the WHO Model List of Essential Medicines (18th list) (1). The proposal is to add delamanid – a nitro‐dihydro‐imdazooxazole derivative that inhibits mycolic acid synthesis‐ to the complementary list of anti‐tuberculosis medicines in adults.
The applicant considers that delamanid should be viewed as an essential medicine for patients with multidrug‐resistant (MDR‐TB) and extensively drug‐resistant (XDR‐TB) disease. In many low resource settings, patients with these forms of tuberculosis are inadequately treated and often die because not enough medications are available to compose a suitable regimen (3). Second‐line drugs for the treatment of M/XDR‐TB are frequently not available; and global stock outs occur regularly. Delamanid should therefore be available to specialized care centres of national TB programmes and other health care providers treating M/XDR‐TB patients.
The WHO has recently issued interim policy guidance on the use of delamanid (25). Although the WHO Expert Committee expressed concerns regarding the quality of the data concerning delamanid’s efficacy and safety, they believe that the benefits of including delamanid in a WHO recommended MDR‐TB regimen outweigh the risks (25). Delamanid has been studied under a randomized control trial and in EBA (early bacterial activity) studies (5, 6, 7). A major initiative to help enhance the treatment of TB and MDR‐TB patients has recently attracted UNITAID funding up to USD 60 million and aims to create new regimens using combinations of both new medicines, such as delamanid, and older TB medications (8).
This request to the EML is thus very timely and in line with the position of WHO and its technical partners. If approved delamanid would synergise with their concerted efforts to improve outcomes and reduce avoidable mortality for the close to half a million TB patients estimated to develop MDR‐TB in the world every year. Globally, 30% (95%CI: 24%–35%) of patients with MDR‐TB have resistance to a fluoroquinolone, a second‐line injectable agent, or both i.e. XDR‐TB. These patients would be eligible to receive regimens containing new and repurposed TB drugs, when options to treat them with existing drugs have been exhausted [3].
2. Name of the focal point in WHO submitting or supporting the application (where relevant)
The focal point is the Unit of Laboratories, Diagnostics and Drug‐resistance of the Global TB Programme of WHO Headquarters (WHO/HTM/GTB/LDR). The technical personnel directly concerned are Dennis FALZON, Linh Nhat NGUYEN and Ernesto JARAMILLO. This application was prepared in close collaboration with WHO/GTB by Elizabeth HARAUSZ and, for notes associated with Sections 10 and 11, by McGill University (led by Dick MENZIES). The guidance of Nicola MAGRINI of WHO/EMP in this work is acknowledged..
2
3. Name of the organization(s) consulted and/or supporting the application
Not applicable.
4. International Nonproprietary Name (INN, generic name) of the medicine
The WHO INN (generic name) of the medicine concerned is delamanid (9).
5. Formulation proposed for inclusion; including adult and paediatric (if appropriate)
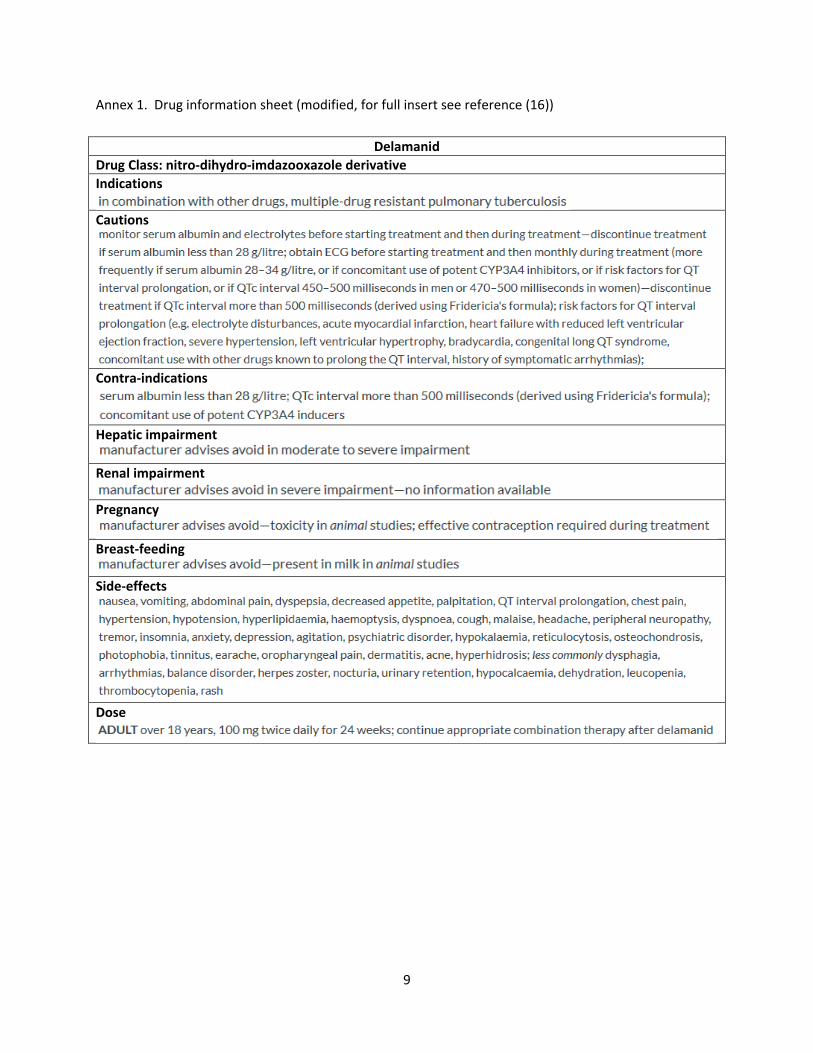
The formulations proposed for adults are 50 mg tablets (9). PK and safety studies have begun in children (10, 11) but there are no data available yet. An abbreviated drug information sheet for delamanid is at Annex 1. The full product package insert is available online(9).
6. International availability ‐ sources, of possible manufacturers and trade names
Delamanid is marketed as Deltyba. The marketing authorization holder is Otsuka Novel Products GmbH (Erika‐Mann‐Straβe 21 ; 80636 Müchen ; Germany), the manufacturer is AndersonBrecon (UK) Ltd. (Wye Valley Business Park ; Brecon Road ; Hay‐on‐Wye ; Hereford, HR3 SPG United Kingdom) (9). It is indicated for the treatment of multidrug‐resistant tuberculosis in adult patients (9). There may be significant challenges in obtaining this medication, and access to its use for compassionate use programmes has been restricted.
7. Whether listing is requested as an individual medicine or as an example of a therapeutic group
This request is for the inclusion of delamanid as an individual medicine without a square box symbol. Delamanid is the only nitro‐dihydro‐imdazooxazole indicated for treatment of tuberculosis.
8. Information supporting the public health relevance (epidemiological information on
disease burden, assessment of current use, target population)
Each year it is estimated that half a million new MDR‐TB cases emerge in the world and over 200,000 MDR‐TB patients die(3). Many MDR‐TB cases go undetected and are not placed on appropriate treatment, increasing the risk that they die and/or transmit drug‐resistant strains to others. In 2013, countries reported that about 100,000 patients started MDR‐TB treatment worldwide. The effectiveness of these efforts vary considerably and data on outcome reporting in recent years showed that about half the MDR‐TB patients complete their treatment successfully (12). The rest die, sustain a treatment failure, interrupt treatment, or are otherwise lost to follow up. The complexity, duration, toxicity, cost and unavailability of the drug regimens for MDR‐TB treatment impedes a global scale‐up of curative services. Given the low treatment success of MDR and XDR‐TB, every effort must be made to ensure that all possible medications used to treat MDR and XDR‐TB are widely available. Facilitating the creation of regimens which are more amenable for patients and providers is therefore a priority.
The contribution of delamanid to MDR‐TB regimens, which cannot otherwise be composed owing to the lack of 4 other effective second‐line drugs, is crucial. This is particularly the case in about one third of MDR‐TB cases who have lost susceptibility to fluoroquinolones, second‐line injectable agents, or both (i.e. XDR‐TB). XDR‐TB represents about 9 % of MDR‐TB cases and some 100 countries have now detected at least one such case (3). The transmissibility of XDR‐TB strains has been documented in outbreaks and regular reports of cases without a previous history of TB treatment [18‐23]; this poses a formidable, additional public health concern making the proper treatment of M/XDR‐TB patients all the more important. The likelihood of treatment success in MDR‐TB patients diminishes with the acquisition of additional resistance and is particularly low in XDR‐TB patients. The availability of
3
delamanid is therefore exceptionally valuable to successfully treat these patients.
9. Treatment details (dosage regimen, duration; reference to existing WHO and other clinical
guidelines; need for special diagnostics, treatment or monitoring facilities and skills)
There are two main indications for delamanid in the treatment of people with drug resistant pulmonary TB:
1) MDR‐TB regimens : A typical MDR‐TB regimen is composed of pyrazinamide plus at least 4 second‐line anti‐TB drugs considered to be effective, including a later‐generation fluoroquinolones, a second‐line injectable, ethionamide (or prothionamide) and cycloserine or PAS(13). When one or more of these drugs are considered ineffective, as a result of in vitro resistance, severe intolerance, or prolonged use in the same patient, the regimen can be bolstered by “Group 5” drugs such as delamanid (4). The standard adult dose is 100 mg twice a day for 24 weeks (9). There are no data on the use of delamanid in children yet, although studies are underway (10, 11).
2) XDR‐TB regimens : XDR‐TB is difficult to treat. WHO guidelines recommend using pyrazinamide and any other Group 1 medication that may be effective, an injectable agent and a higher generation fluoroquinolone (if the strain retains susceptibility)(4). Often these medications are no longer effective. Therefore, use of all Group 4 agents that are likely to be effective, use of 2 or more Group 5 drugs and consideration of high dose isoniazid and investigational drugs is recommended (4). The dosing of delamanid remains the same as for the MDR‐TB treatment regimen.
The WHO interim policy recommendations state that delamanid may be added to a WHO recommended regimen in adult patients with pulmonary MDR‐TB (25). WHO recommends that the use of delamanid occur under 5 conditions (see reference for more details) (25). 1) Proper patient inclusion. See reference for more details, but highlights are that delamanid may
not be warranted if an effective regimen can be composed with other second line drugs. However, in patients at high risk for poor outcomes, delamanid may be particularly justified. Delamanid can be used in people with HIV. Due to concerns about QTc prolongation, people with a QTcF > 500 ms should not receive delamanid.
2) Adherence to the principles of designing a WHO recommended MDR‐TB regimen. Of note, the report states that there are no data on the simultaneous use of bedaquiline and delamanid (therefore there are no recommendations on their joint administration) and that the supervision of delamanid should be adapted to its recommended twice daily regimen (100 mg twice a day).
3) Treatment closely monitored. Particular attention should be paid to QTc prolongation. 4) Active pharmacovigilance and proper management of adverse drug reactions and prevention of
drug‐drug interactions. It is recommended that all patients be monitored for cardiac dysrhythmias or QT interval prolongation (i.e. an electrocardiogram) and for electrolyte disturbances.
5) Patient informed consent is obtained
Public health need and evidence appraisal and synthesis
10. Summary of comparative effectiveness in a variety of clinical settings:
[See Annex 2]
4
11. Summary of comparative evidence on safety:
[See Annex 2]
12. Summary of available data on comparative cost and cost‐effectiveness within the
pharmacological class or therapeutic group:
The range of (published) costs for delamanid is limited. Early data for the United Kingdom and Germany
are available, however, the price of delamanid is still in flux. It is expected that the price of delamanid
will be comparable to that of bedaqualine.
Source Price (US$)
Comments accessed 20.10.2014
Global Drug Facility
not available
MSH International Drug Price Indicator Guide
not available
UNICEF/WHO (14) not available
Médecins sans Frontières (15)
not available
MediPreis (Germany)
1,919 for 40 x 50 mg tabs
https://www.medipreis.de/preisvergleich/Deltyba‐50‐Mg‐Filmtabletten‐40‐Stueck‐Otsuka‐Novel‐Products‐GmbH‐10286871?preiseversand.
British National Formulary
1,690 for 40 x 50 mg tabs
http://www.treatmentactiongroup.org/tb/delamanid‐factsheet
Regulatory information
13. Summary of regulatory status of the medicine (in various countries)
The table below summarizes the regulatory status of delamanid.
Authority Regulatory status and indications
US Food and Drug Administration (FDA)
not approved
European Medicines Agency (EMA) The Otsuka Novel Products GmbH product (Deltyba) was granted conditional marketing authorization on 28 April 2014 (9)
Australian Therapeutic Goods Administration
Not found
Japan Not found
Health Canada Not found
5
WHO List of Prequalified Medicinal Products
Not found
14. Availability of pharmacopoeial standards (British Pharmacopoeia, International
Pharmacopoeia, United States Pharmacopoeia, European Pharmacopeia)
No reference standards for delamanid were found
Standard Reference (accessed 20.10.2014)
British National Formulary not found
British Pharmacopoeia not found
International Pharmacopoeia not found
United States Pharmacopeia not found
European Pharmacopeia not found
15. Proposed (new/adapted) text that could be included in a revised WHO Model Formulary
If this request is approved, it is proposed that identical modifications are made to the tabulations in the WHO Model List of Essential Medicines (18th list)(1) to accommodate the new addition. It is recommended that the suggested change be made as shown hereunder :
Complementary List
Reserve second‐line drugs for the treatment of multidrug‐resistant tuberculosis (MDR‐TB) should be used in specialized centres adhering to WHO standards for TB control. delamanid Tablet: 50 mg
6
References
1. WHO Model List of Essential Medicines [Internet]. 18th list. Geneva, World Health Organization; 2013. Available from: http://apps.who.int/iris/bitstream/10665/93142/1/EML_18_eng.pdf
2. WHO Model List of Essential Medicines for Children [Internet]. 4th list. Geneva, World Health Organization; 2013. Available from: http://apps.who.int/iris/bitstream/10665/93143/1/EMLc_4_eng.pdf
3. Global tuberculosis report 2014 (WHO/HTM/TB/2014.08) [Internet]. Geneva, World Health Organization. 2014. Available from: http://www.who.int/tb/publications/global_report/en
4. Companion handbook to the WHO guidelines for the programmatic management of drug‐resistant tuberculosis. (WHO/HTM/TB/2014.xx). Geneva, World Health Organization. 2014.
5. Saliu OY, Crismale C, Schwander SK, Wallis RS. Bactericidal activity of OPC‐67683 against drug‐
tolerant Mycobacterium tuberculosis. J Antimicrob Chemother. 2007 Nov;60(5):994‐8. Epub 2007
Aug 29.
6. Gler MT, Skripconoka V, Sanchez‐Garavito E, Xiao H, Cabrera‐Rivero JL, Vargas‐Vasquez DE, Gao M, Awad M, Park SK, Shim TS, Suh GY, Danilovits M, Ogata H, Kurve A, Chang J, Suzuki K, Tupasi T, Koh WJ, Seaworth B, Geiter LJ, Wells CD. Delamanid for multidrug‐resistant pulmonary tuberculosis. N Engl J Med. 2012 Jun 7;366(23):2151‐60.
7. Skripconoka V, Danilovits M, Pehme L, Tomson T, Skenders G, Kummik T, Cirule A, Leimane V, Kurve A, Levina K, Geiter LJ, Manissero D, Wells CD. Delamanid improves outcomes and reduces mortality in multidrug‐resistant tuberculosis. Eur Respir J. 2013 Jun;41(6):1393‐400.
8. UNITAID Approves Grants of $160 million [Internet]. [cited 2014 Jul 26]. Available from: http://www.unitaid.org/en/resources/press‐centre/releases/1352‐unitaid‐approves‐grants‐of‐160‐million
9. European Medicines Agency (EMA). Deltyba: EPAR‐Product Information. [cited 20.10.2014] Available at: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002552/human_med_001699.jsp&mid=WC0b01ac058001d124
10. European Medicines Agency (EMA). EMA decision of 29 November 2013 on the acceptance of a
modification of an agreed paediatric investigation plan for delamanid. [cited 20.10.2014] Available
from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/pips/EMEA‐001113‐PIP01‐
10‐M02/pip_000797.jsp&mid=WC0b01ac058001d129
11. ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (U.S.) 2000. Identifier
NCT01859923, A 6‐month safety, efficacy, and pharmacokinetic trial of delamanid in pediatric
7
patients with multidrug resistant tuberculosis; 2013 May 15 (cited 20.10.2014). Available at:
http://clinicaltrials.gov/ct2/show/NCT01859923?term=delamanid&rank=1.
12. Falzon D, Jaramillo E, Wares F, Zignol M, Floyd K, Raviglione MC. Universal access to care for multidrug‐resistant tuberculosis: an analysis of surveillance data. Lancet Infect Dis. 2013 Aug;13(8):690–7.
13. Guidelines for the programmatic management of drug‐resistant tuberculosis, 2011 Update. (WHO/HTM/TB/2011.6) [Internet]. Geneva, World Health Organization. 2011. Available from: http://whqlibdoc.who.int/publications/2011/9789241501583_eng.pdf
14. UNICEF, WHO. Sources and prices of selected medicines for children. Including therapeutic food, dietary vitamin and mineral supplementation [Internet]. 2nd ed. 2010. Available from: http://apps.who.int/medicinedocs/en/d/Js17031e/
15. MSF, UNION. DR‐TB Drugs Under the Microscope [Internet]. Geneva, Switzerland and Paris, France; 2011. Available from: http://www.msfaccess.org/sites/default/files/MSF_assets/TB/Docs/TB_report_UndertheMicro_ENG_2011.pdf
16. British National Formulary. Delamanid. [cited 20.10.2014] Available from:
http://www.openproxy.co.uk/browse.php?u=Oi8vd3d3LmV2aWRlbmNlLm5ocy51ay9mb3JtdWxhcn
kvYm5mL2N1cnJlbnQvNS1pbmZlY3Rpb25zLzUxLWFudGliYWN0ZXJpYWwtZHJ1Z3MvNTE5LWFudGl0
dWJlcmN1bG9zaXMtZHJ1Z3MvZGVsYW1hbmlk&b=13
17. Information note on the use of a new agent, delamanid, for the treatment of multidrug‐resistant tuberculosis. [internet]. Geneva, World Health Organization (WHO). [cited 10.20.2014]. Available from: http://www.who.int/tb/information_note_delamanid/en/
18. Dharmadhikari A S, Basaraba R J, Van Der Walt M L, et al. Natural infection of guinea pigs exposed to
patients with highly drug‐resistant tuberculosis. Tuberculosis (Edinb) 2011; 91: 329–338. 19. Rüsch‐Gerdes S, Pfyffer G E, Casal M, Chadwick M, Siddiqi S. Multicenter laboratory validation of the
BACTEC MGIT 960 technique for testing susceptibilities of Mycobacterium tuberculosis to classical second‐line drugs and newer antimicrobials. J Clin Microbiol 2006; 44: 688–692.
20. Andrews R H, Devadatta S, Fox W, Radhakrishna S, Ramakrishnan C V, Velu S. Prevalence of
tuberculosis among close family contacts of tuberculosis patients in south India and influence of segregation of the patient on the early attack rate. Bull World Health Organ 1960; 23: 463–510.
21. Crofton J. The contribution of treatment to the prevention of tuberculosis. Bull Int Union Tuberc
1962; 32 (2): 643–653. 22. Brooks S M, Lassiter N L, Young E. A pilot study concerning the infection risk of sputum positive with
tuberculosis patients on chemotherapy. Am Rev Respir Dis 1973; 108: 799–804.
8
23. Gunnels J, Bates J, Swindoll H. Infectivity of sputum positive tuberculosis patients on chemotherapy. Am Rev Respir Dis 1974; 109: 323.
24. Rouillon A, Perdrizet S, Parrot R. Transmission of tubercle bacilli: the effects of chemotherapy.
Tubercle 1976; 57: 275–299. 25. The use of delamanid in the treatment of multidrug‐resistant tuberculosis: Interim policy guidance.
[internet]. 2014. Geneva, World Health Organization (WHO). [cited 11.21.2014]. Available from: http://apps.who.int/iris/bitstream/10665/137334/1/WHO_HTM_TB_2014.23_eng.pdf?ua=1&ua=1
9
Annex 1. Drug information sheet (modified, for full insert see reference (16))
Delamanid
Drug Class: nitro‐dihydro‐imdazooxazole derivative
Indications
Cautions
Contra‐indications
Hepatic impairment
Renal impairment
Pregnancy
Breast‐feeding
Side‐effects
Dose
A
(
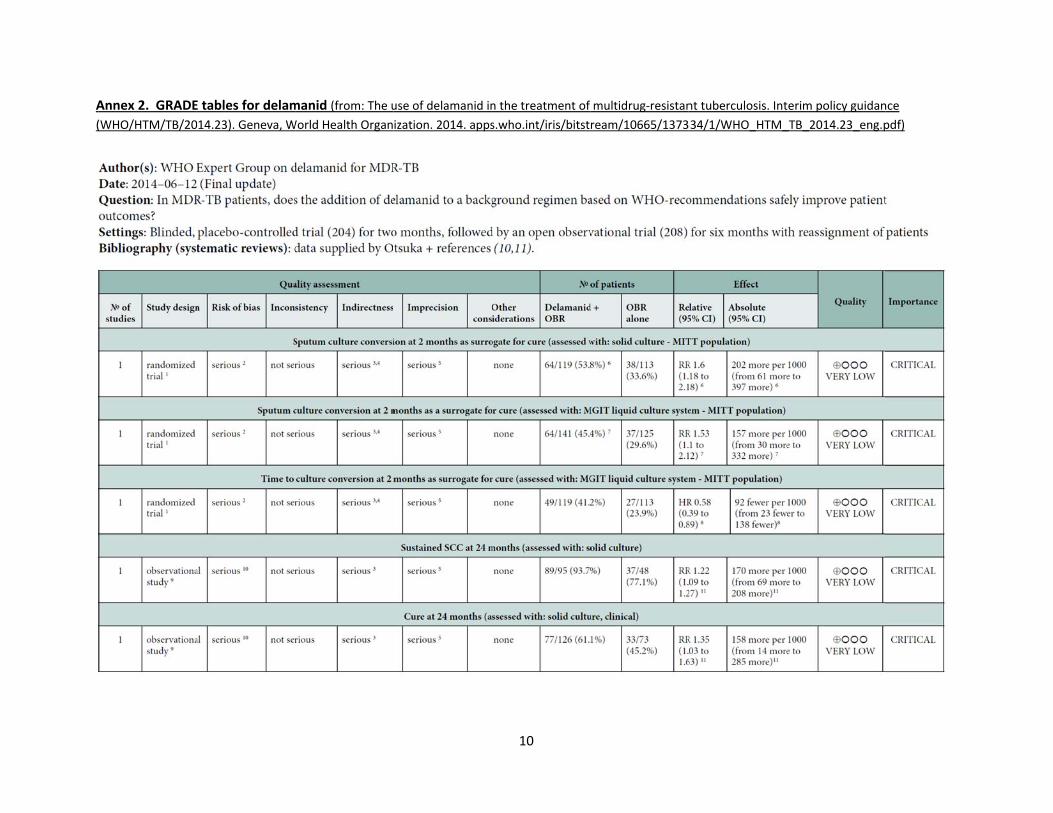
Annex 2. GRADE
(WHO/HTM/TB/20
E tables for delam
014.23). Geneva, W
manid (from: The u
World Health Organ
use of delamanid in
ization. 2014. apps
10
n the treatment of
s.who.int/iris/bitst
multidrug‐resistan
ream/10665/1373
nt tuberculosis. Int
334/1/WHO_HTM_
terim policy guidan
_TB_2014.23_eng.p
nce
pdf)
11
12
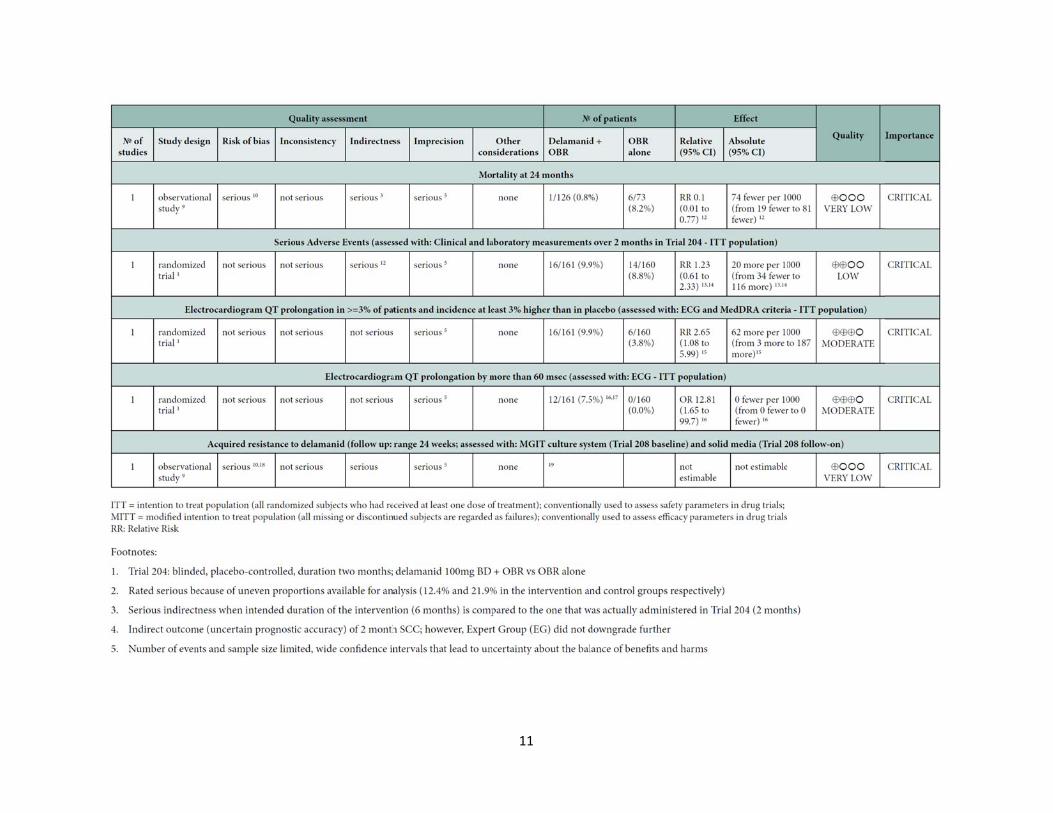
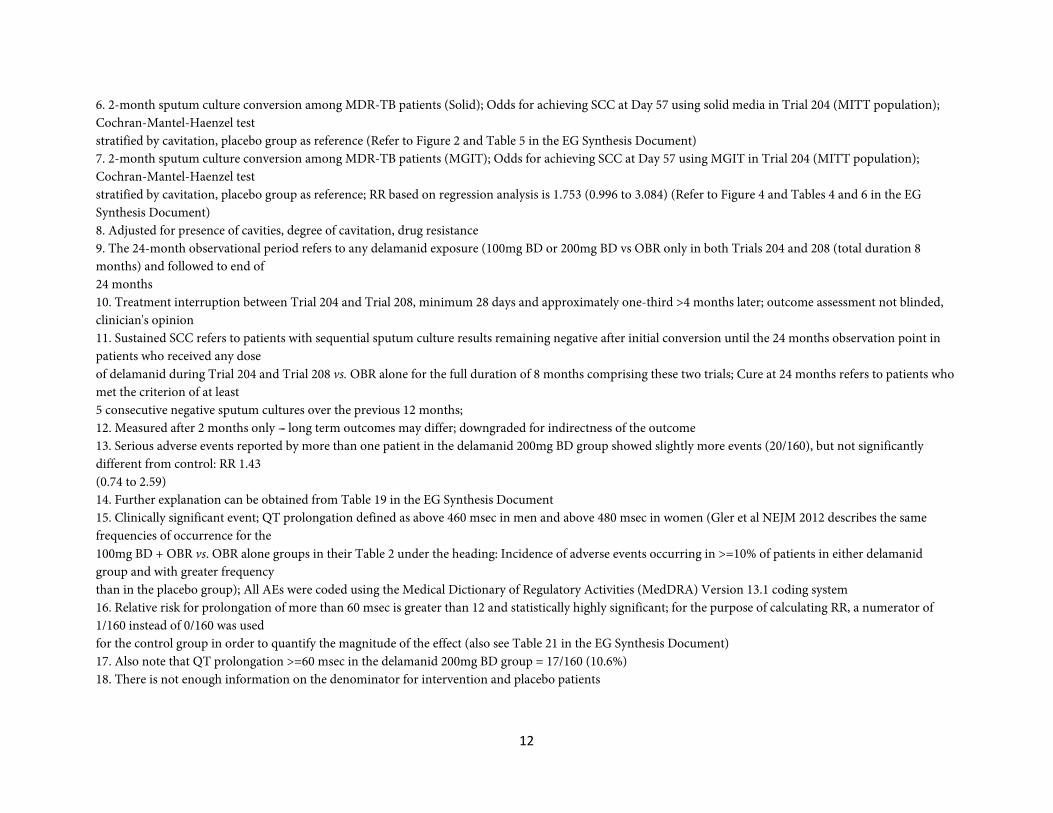
6. 2-month sputum culture conversion among MDR-TB patients (Solid); Odds for achieving SCC at Day 57 using solid media in Trial 204 (MITT population); Cochran-Mantel-Haenzel test stratified by cavitation, placebo group as reference (Refer to Figure 2 and Table 5 in the EG Synthesis Document) 7. 2-month sputum culture conversion among MDR-TB patients (MGIT); Odds for achieving SCC at Day 57 using MGIT in Trial 204 (MITT population); Cochran-Mantel-Haenzel test stratified by cavitation, placebo group as reference; RR based on regression analysis is 1.753 (0.996 to 3.084) (Refer to Figure 4 and Tables 4 and 6 in the EG Synthesis Document) 8. Adjusted for presence of cavities, degree of cavitation, drug resistance 9. The 24-month observational period refers to any delamanid exposure (100mg BD or 200mg BD vs OBR only in both Trials 204 and 208 (total duration 8 months) and followed to end of 24 months 10. Treatment interruption between Trial 204 and Trial 208, minimum 28 days and approximately one-third >4 months later; outcome assessment not blinded, clinician's opinion 11. Sustained SCC refers to patients with sequential sputum culture results remaining negative after initial conversion until the 24 months observation point in patients who received any dose of delamanid during Trial 204 and Trial 208 vs. OBR alone for the full duration of 8 months comprising these two trials; Cure at 24 months refers to patients who met the criterion of at least 5 consecutive negative sputum cultures over the previous 12 months; 12. Measured after 2 months only --- long term outcomes may differ; downgraded for indirectness of the outcome 13. Serious adverse events reported by more than one patient in the delamanid 200mg BD group showed slightly more events (20/160), but not significantly different from control: RR 1.43 (0.74 to 2.59) 14. Further explanation can be obtained from Table 19 in the EG Synthesis Document 15. Clinically significant event; QT prolongation defined as above 460 msec in men and above 480 msec in women (Gler et al NEJM 2012 describes the same frequencies of occurrence for the 100mg BD + OBR vs. OBR alone groups in their Table 2 under the heading: Incidence of adverse events occurring in >=10% of patients in either delamanid group and with greater frequency than in the placebo group); All AEs were coded using the Medical Dictionary of Regulatory Activities (MedDRA) Version 13.1 coding system 16. Relative risk for prolongation of more than 60 msec is greater than 12 and statistically highly significant; for the purpose of calculating RR, a numerator of 1/160 instead of 0/160 was used for the control group in order to quantify the magnitude of the effect (also see Table 21 in the EG Synthesis Document) 17. Also note that QT prolongation >=60 msec in the delamanid 200mg BD group = 17/160 (10.6%) 18. There is not enough information on the denominator for intervention and placebo patients
13
19. Four patients (4/205, 2.0%), 2 in each treatment group, had confirmed resistance to delamanid (defined as growth on solid media in the presence of 200 ng/mL delamanid, the epidemiologic break-point). The clinical significance of resistance as defined in this trial has not yet been established; however, in all four cases, the exposure to delamanid exceeded the optimal threshold established in EBA trials suggesting that the development of resistance to delamanid in these cases was not due to delamanid exposure but rather likely to treatment history and initial drug resistance profile.
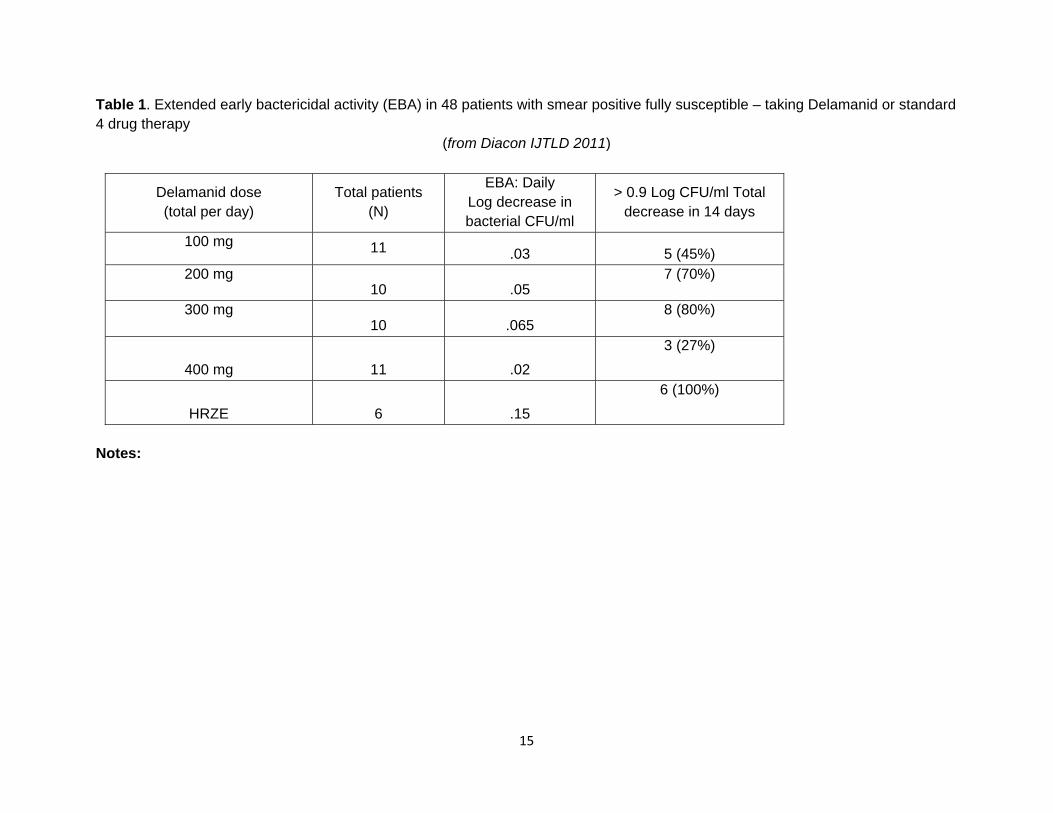
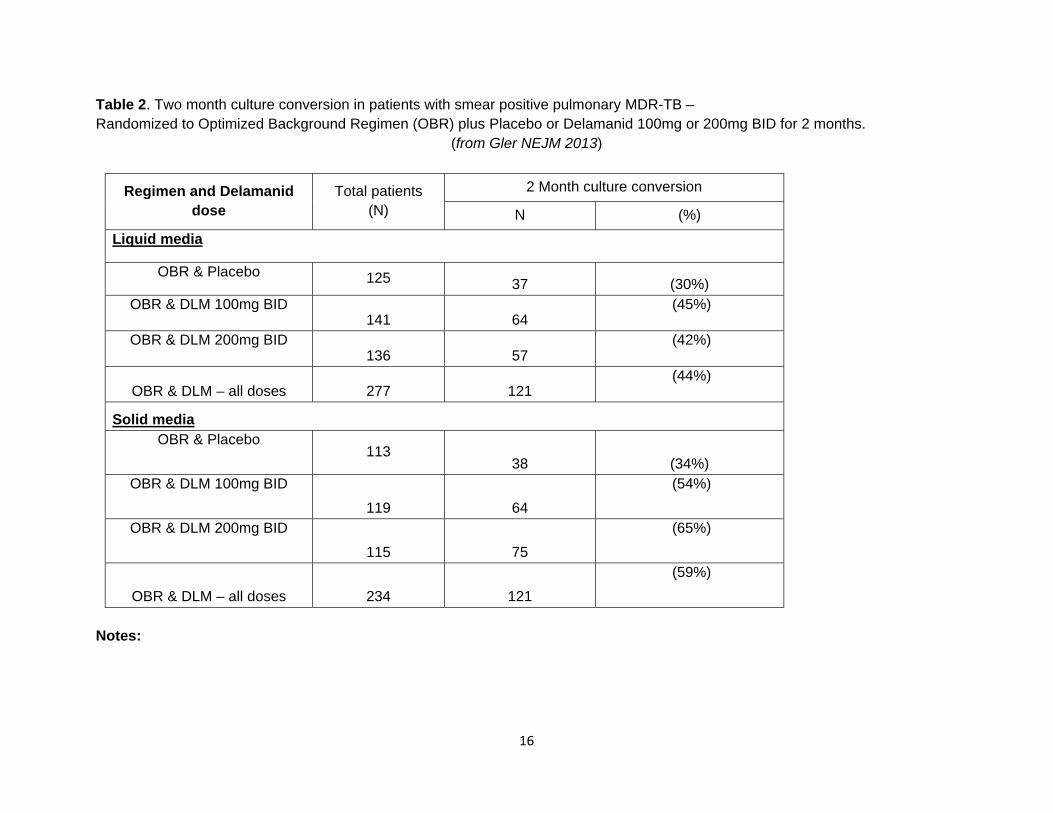
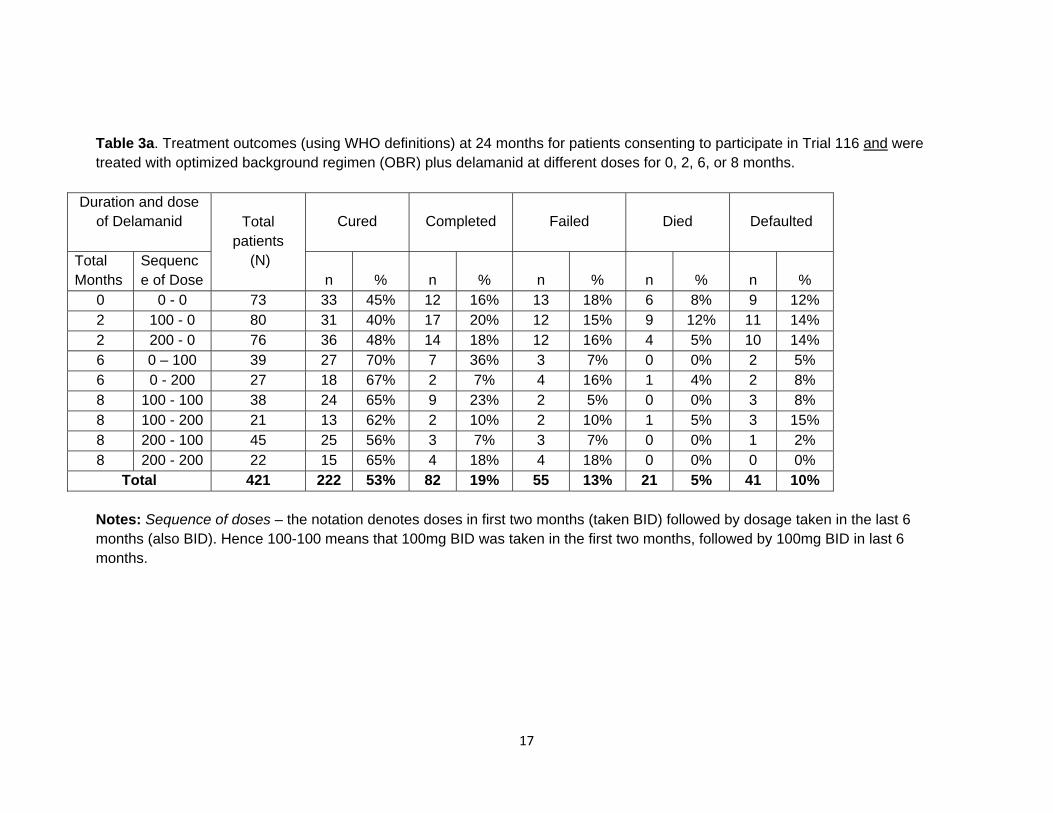
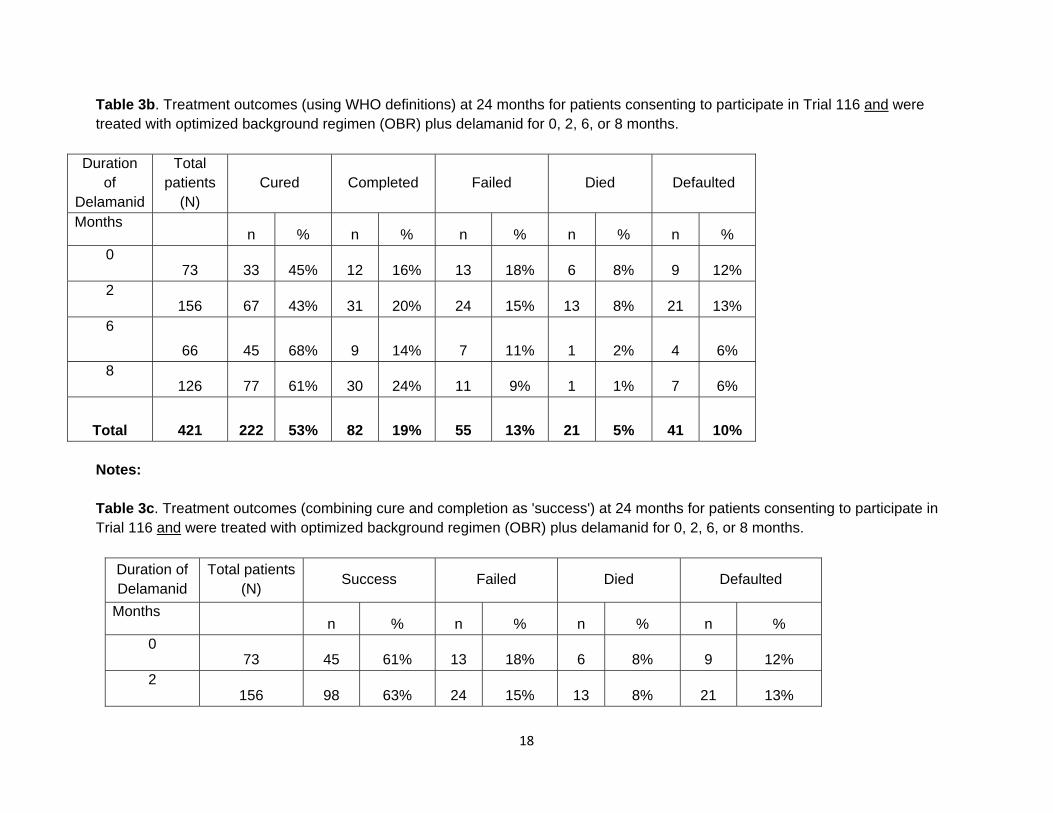
Notes re Tables for Delamanid In one of the earliest studies (Diacon, IJTLD, 2011), DLM was shown to have moderate bactericidal activity, with maximal effect at 200 or 300 mg/day (Table 1). This effect was substantially less than that achieved with the standard full 4 drug regimen (although prior studies have shown that INH alone will achieve EBA similar to that of 4 drugs – hence one can conclude the EBA of DLM is not the same as INH, although these have not been directly compared). In the first published Phase 2 trial (Gler NEJM 2013), with 402 total patients, and DLM (in doses of 100mg or 200mg), or placebo added for the first two months to a standard MDR regimen (optimized background regimen or OBR), two month culture conversion was 30% with placebo & OBR compared to 45% and 42% respectively with doses of 100mg or 200mg BID (see Table 2). Similar differences were seen with cultures on solid media (this was a planned secondary outcome). This was a high quality randomized trial. The patients enrolled and randomized in this Phase 2 trial were then followed up to the end of 24 months treatment. Not all patients were followed to ascertain these final outcomes, but over 90% agreed and were followed successfully. An added feature is that some patients were given 6 more months of DLM therapy. However, 229 patients were not given DLM for the added 6 months. The decision to extend DLM therapy appears to have been a post-hoc decision by the sponsor and study investigators. As a result there were variable, but often substantial delays, between patients completing the first two months of therapy and restarting therapy. In addition the decision to give DLM for the 6 months was individualized and made by the treating physician and patient. Although the clinical characteristics of those that received the additional 6 months of DLM, and those that did not were quite similar, the outcomes were very different, as seen in Table 3a. These differences are more evident when the tables are simplified – by combining doses of DLM together, since the results with 200mg BID were almost identical to results with 100mg BID (Table 3B), and then combining cure and treatment completion as treatment success (Table 3C).
14
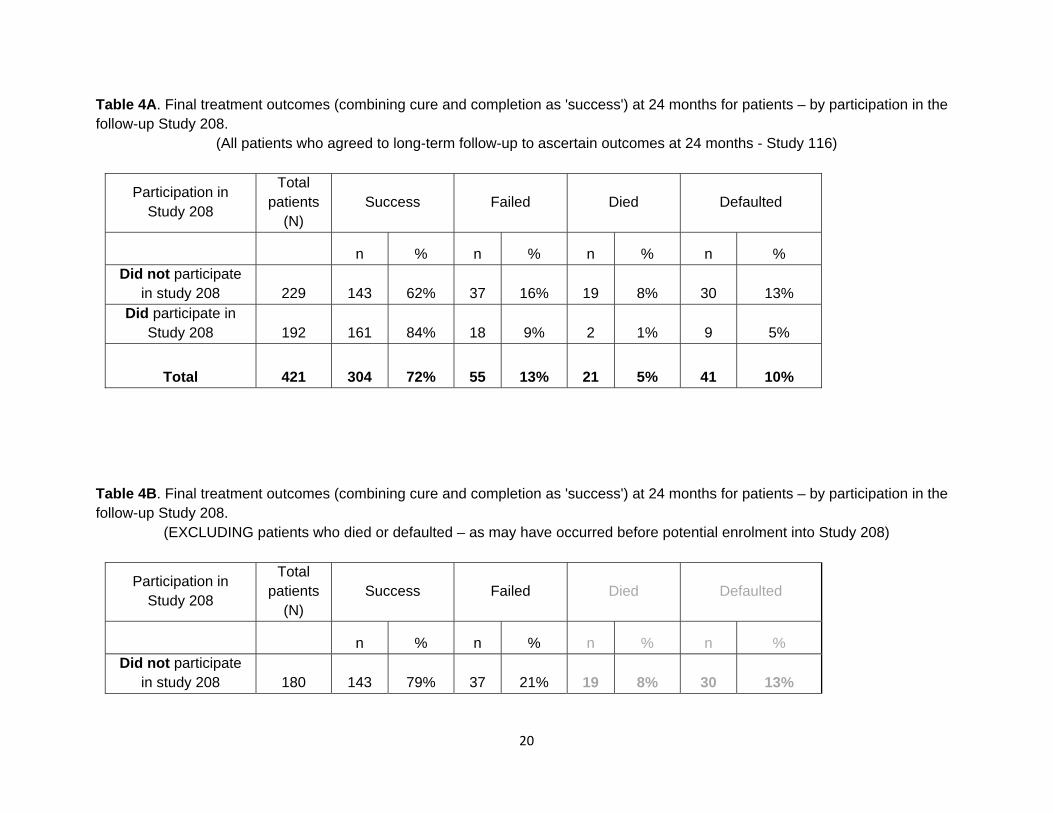
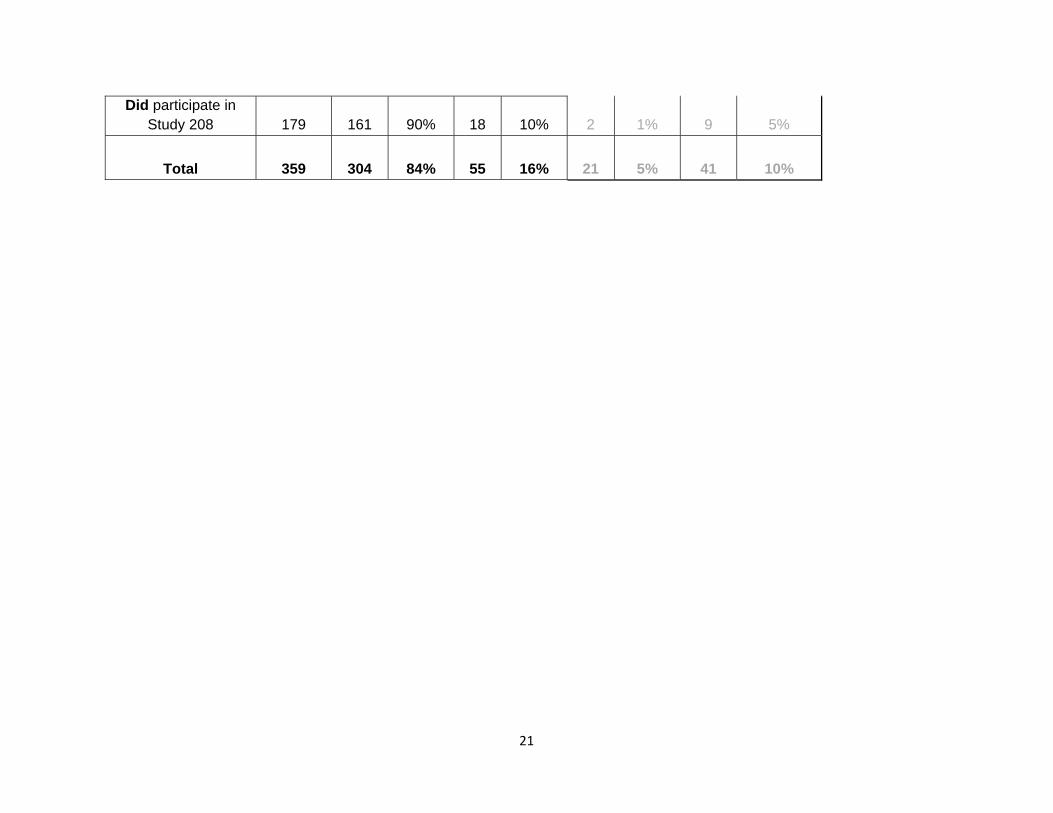
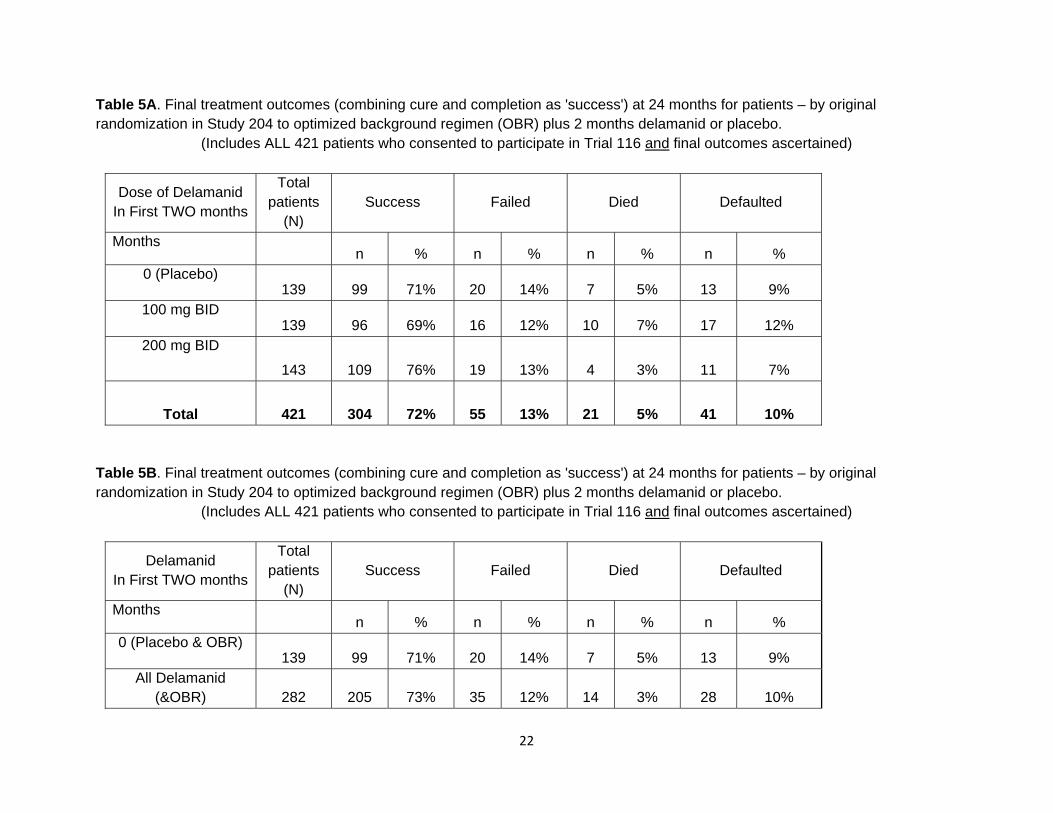
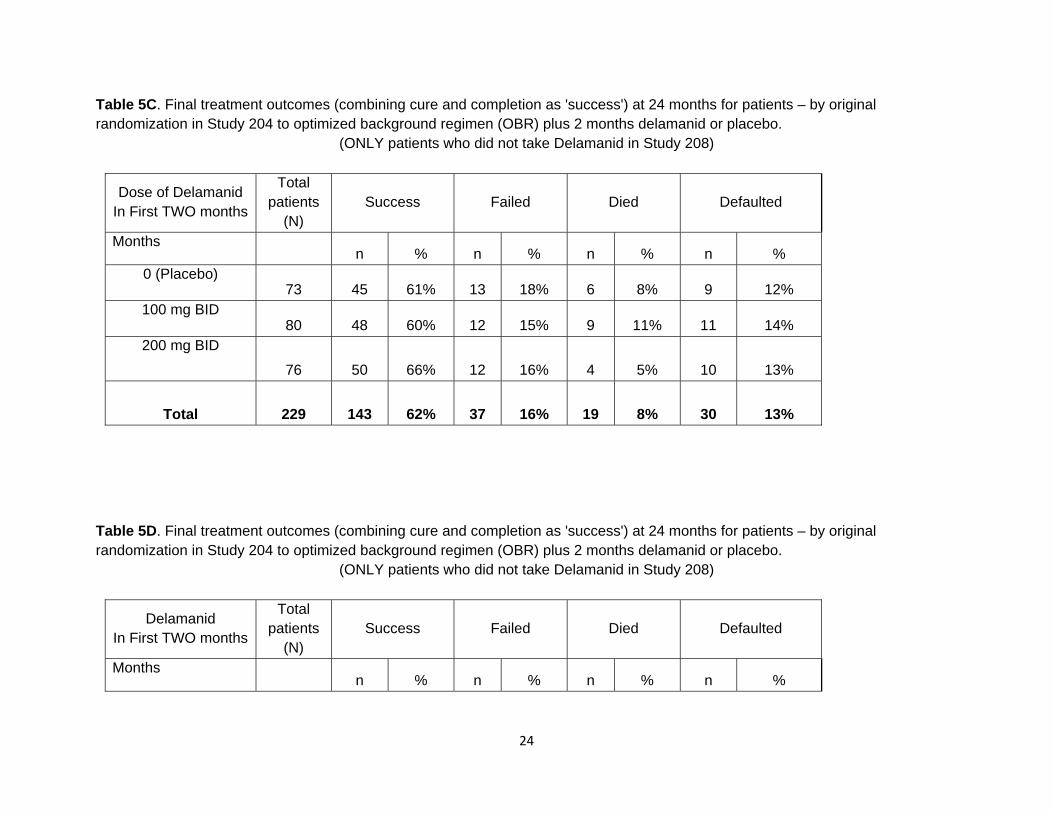
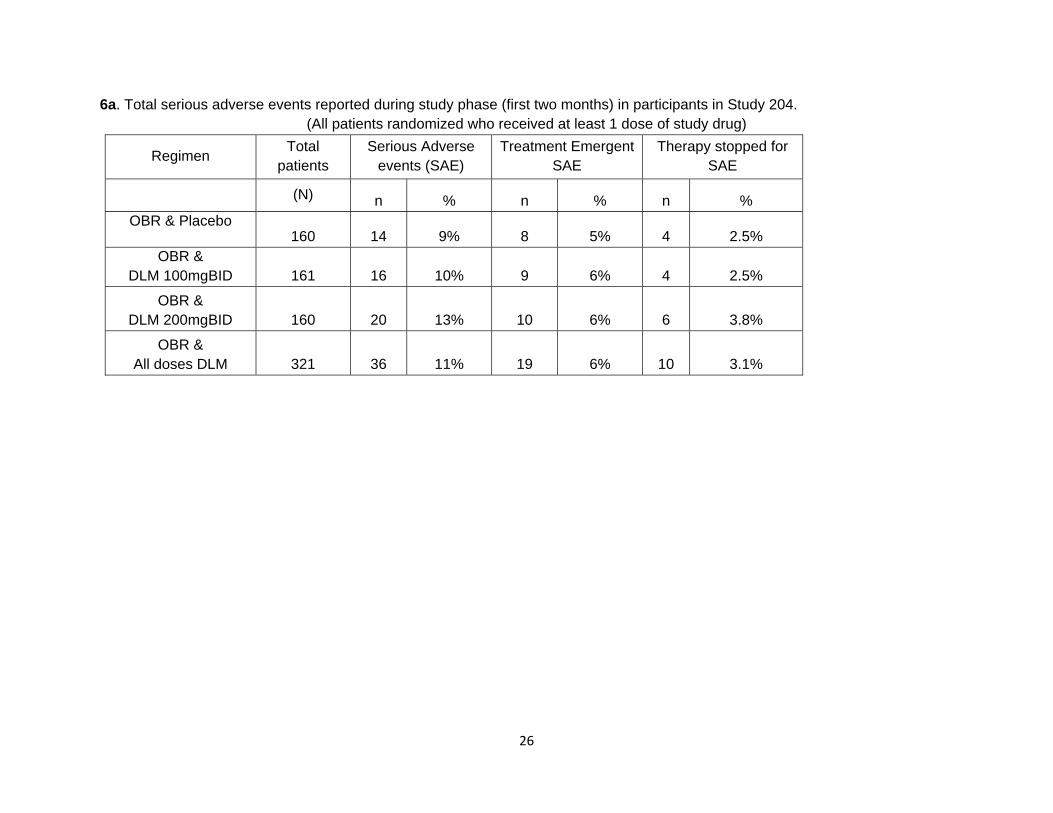
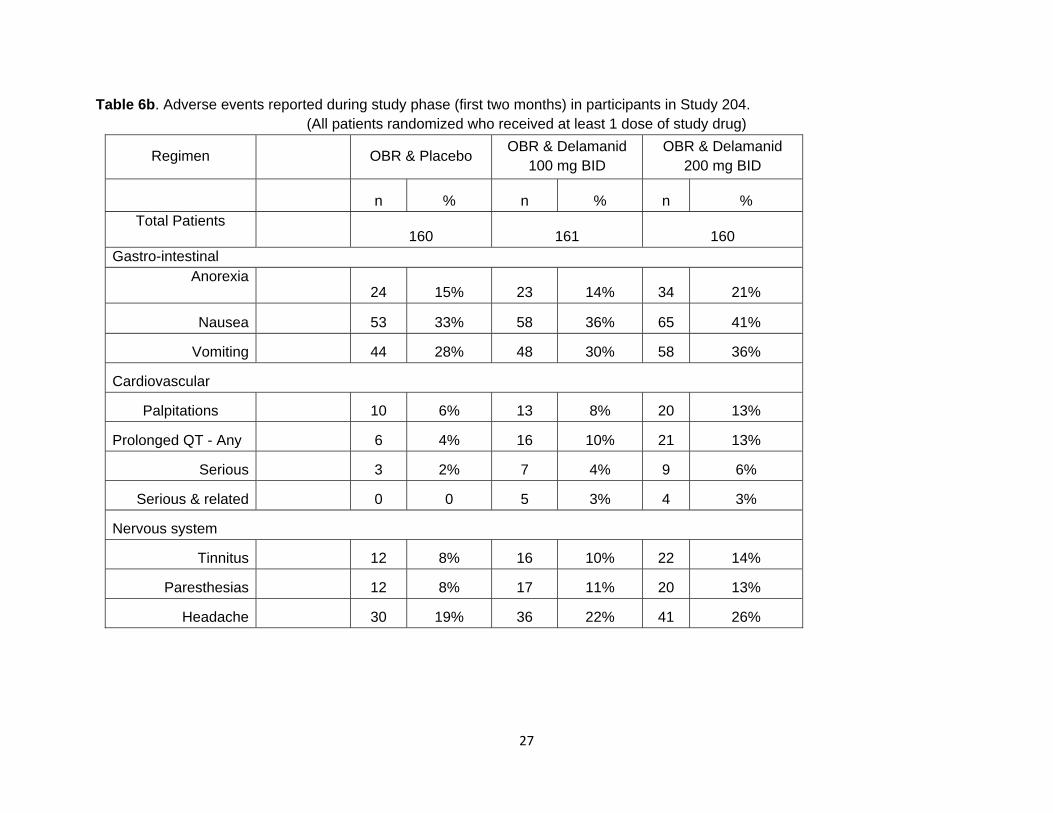
Because of this, the data was re-analyzed to compare outcomes in those who took the additional 6 months (“Participated in Study 208”) vs those who did not. As seen in Table 4A (all patients) there were very substantial differences in death and default between those who were or were not selected by their physicians (and themselves) to receive the added 6 months of DLM. Given the individualized, and non-random selection it is likely that death and default were much more frequent in the non-participants because these outcomes had already occurred – i.e. the outcomes preceded the allocation to extended DLM therapy. When the results were analyzed after excluding all those who died or defaulted, the extra 6 months of DLM was still associated with significantly higher treatment success rates. Since the added 6 months of therapy was not randomized, and indeed appears to have introduced significant bias in the ascertainment of final outcomes, the final treatment outcomes were re-analyzed according to the original randomization. As seen in Tables 5A (DLM doses shown separately) and 5B (DLM doses combined), there were no differences in final outcomes after 24 months of MDR treatment between those randomized to 2 months DLM or two months placebo – at the outset of MDR treatment. Since the added 6 months of therapy would potentially have confounded, or simply obscured any treatment effect or difference resulting from the first two months of therapy, results were re-analyzed after excluding all participants in Study 208 – who took the extra 6 months DLM. As seen in Tables 5Cand 5D – final treatment outcomes were almost identical in those who got DLM or those who got placebo, despite the initial improvement in 2 month culture conversion. Serious adverse events associated with DLM are available only for the first placebo controlled trial – when DLM was given for the first two months. Rates of adverse events can be compared to rates with placebo – of great importance given that OBR regimens meant that patients received multi-drug therapy with second line drugs known to have high rates of adverse events. As seen in Table 6A, rates of serious adverse events (Grade 3 and 4 reactions), treatment emergent adverse events (i.e. during the first two months) and therapy discontinuation for adverse events were all slightly, but not significantly, higher with DLM, especially with the 200mg BID dose. When any adverse event in the first two months was considered – there was a trend to higher rates of gastrointestinal problems with DLM, especially with the higher dose (Table 6B). Of particular interest was that QT prolongation was significantly more frequent with DLM – and there appeared to be a dose effect – as the problem was more frequent at the higher dose of 200mg BID.
15
Table 1. Extended early bactericidal activity (EBA) in 48 patients with smear positive fully susceptible – taking Delamanid or standard 4 drug therapy
(from Diacon IJTLD 2011)
Delamanid dose (total per day)
Total patients (N)
EBA: Daily Log decrease in bacterial CFU/ml
> 0.9 Log CFU/ml Total decrease in 14 days
100 mg 11 .03 5 (45%) 200 mg
10 .05 7 (70%)
300 mg 10 .065
8 (80%)
400 mg 11 .02
3 (27%)
HRZE 6 .15
6 (100%)
Notes:
16
Table 2. Two month culture conversion in patients with smear positive pulmonary MDR-TB – Randomized to Optimized Background Regimen (OBR) plus Placebo or Delamanid 100mg or 200mg BID for 2 months.
(from Gler NEJM 2013)
Regimen and Delamanid dose
Total patients (N)
2 Month culture conversion
N (%)
Liquid media
OBR & Placebo 125 37 (30%) OBR & DLM 100mg BID
141 64 (45%)
OBR & DLM 200mg BID 136 57
(42%)
OBR & DLM – all doses 277 121 (44%)
Solid media OBR & Placebo
113 38 (34%)
OBR & DLM 100mg BID
119 64
(54%)
OBR & DLM 200mg BID
115 75
(65%)
OBR & DLM – all doses 234 121
(59%)
Notes:
17
Table 3a. Treatment outcomes (using WHO definitions) at 24 months for patients consenting to participate in Trial 116 and were treated with optimized background regimen (OBR) plus delamanid at different doses for 0, 2, 6, or 8 months.
Duration and dose of Delamanid
Total
patients (N)
Cured Completed Failed Died Defaulted
Total Months
Sequence of Dose n % n % n % n % n %
0 0 - 0 73 33 45% 12 16% 13 18% 6 8% 9 12% 2 100 - 0 80 31 40% 17 20% 12 15% 9 12% 11 14% 2 200 - 0 76 36 48% 14 18% 12 16% 4 5% 10 14% 6 0 – 100 39 27 70% 7 36% 3 7% 0 0% 2 5% 6 0 - 200 27 18 67% 2 7% 4 16% 1 4% 2 8% 8 100 - 100 38 24 65% 9 23% 2 5% 0 0% 3 8% 8 100 - 200 21 13 62% 2 10% 2 10% 1 5% 3 15% 8 200 - 100 45 25 56% 3 7% 3 7% 0 0% 1 2% 8 200 - 200 22 15 65% 4 18% 4 18% 0 0% 0 0%
Total 421 222 53% 82 19% 55 13% 21 5% 41 10% Notes: Sequence of doses – the notation denotes doses in first two months (taken BID) followed by dosage taken in the last 6 months (also BID). Hence 100-100 means that 100mg BID was taken in the first two months, followed by 100mg BID in last 6 months.
18
Table 3b. Treatment outcomes (using WHO definitions) at 24 months for patients consenting to participate in Trial 116 and were treated with optimized background regimen (OBR) plus delamanid for 0, 2, 6, or 8 months.
Duration of
Delamanid
Total patients
(N) Cured Completed Failed Died Defaulted
Months n % n % n % n % n % 0
73 33 45% 12 16% 13 18% 6 8% 9 12% 2
156 67 43% 31 20% 24 15% 13 8% 21 13% 6
66 45 68% 9 14% 7 11% 1 2% 4 6% 8
126 77 61% 30 24% 11 9% 1 1% 7 6%
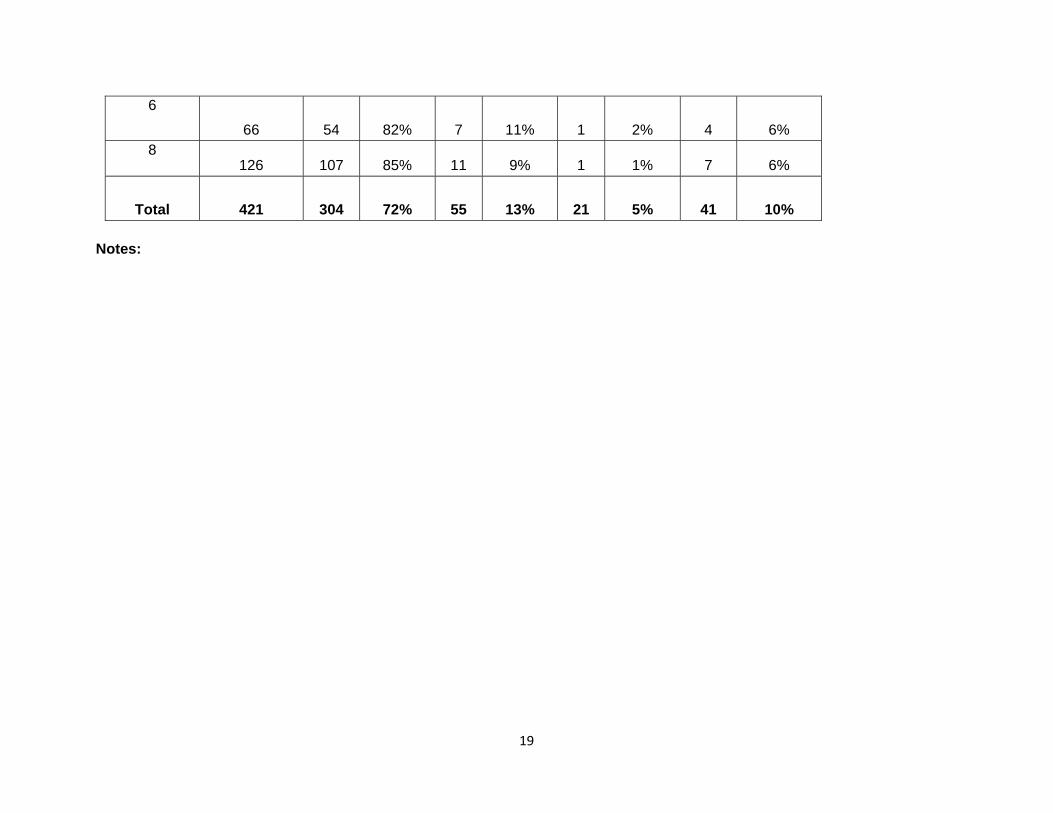
Total 421 222 53% 82 19% 55 13% 21 5% 41 10% Notes: Table 3c. Treatment outcomes (combining cure and completion as 'success') at 24 months for patients consenting to participate in Trial 116 and were treated with optimized background regimen (OBR) plus delamanid for 0, 2, 6, or 8 months.
Duration of Delamanid
Total patients (N)
Success Failed Died Defaulted
Months n % n % n % n % 0
73 45 61% 13 18% 6 8% 9 12% 2
156 98 63% 24 15% 13 8% 21 13%
19
6
66 54 82% 7 11% 1 2% 4 6% 8
126 107 85% 11 9% 1 1% 7 6%
Total 421 304 72% 55 13% 21 5% 41 10% Notes:
20
Table 4A. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by participation in the follow-up Study 208.
(All patients who agreed to long-term follow-up to ascertain outcomes at 24 months - Study 116)
Participation in Study 208
Total patients
(N) Success Failed Died Defaulted
n % n % n % n % Did not participate
in study 208 229 143 62% 37 16% 19 8% 30 13% Did participate in
Study 208 192 161 84% 18 9% 2 1% 9 5%
Total 421 304 72% 55 13% 21 5% 41 10% Table 4B. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by participation in the follow-up Study 208.
(EXCLUDING patients who died or defaulted – as may have occurred before potential enrolment into Study 208)
Participation in Study 208
Total patients
(N) Success Failed Died Defaulted
n % n % n % n % Did not participate
in study 208 180 143 79% 37 21% 19 8% 30 13%
21
Did participate in Study 208 179 161 90% 18 10% 2 1% 9 5%
Total 359 304 84% 55 16% 21 5% 41 10%
22
Table 5A. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by original randomization in Study 204 to optimized background regimen (OBR) plus 2 months delamanid or placebo.
(Includes ALL 421 patients who consented to participate in Trial 116 and final outcomes ascertained)
Dose of Delamanid In First TWO months
Total patients
(N) Success Failed Died Defaulted
Months n % n % n % n % 0 (Placebo)
139 99 71% 20 14% 7 5% 13 9% 100 mg BID
139 96 69% 16 12% 10 7% 17 12% 200 mg BID
143 109 76% 19 13% 4 3% 11 7%
Total 421 304 72% 55 13% 21 5% 41 10% Table 5B. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by original randomization in Study 204 to optimized background regimen (OBR) plus 2 months delamanid or placebo.
(Includes ALL 421 patients who consented to participate in Trial 116 and final outcomes ascertained)
Delamanid In First TWO months
Total patients
(N) Success Failed Died Defaulted
Months n % n % n % n % 0 (Placebo & OBR)
139 99 71% 20 14% 7 5% 13 9% All Delamanid
(&OBR) 282 205 73% 35 12% 14 3% 28 10%
23
Total 421 304 72% 55 13% 21 5% 41 10%
24
Table 5C. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by original randomization in Study 204 to optimized background regimen (OBR) plus 2 months delamanid or placebo.
(ONLY patients who did not take Delamanid in Study 208)
Dose of Delamanid In First TWO months
Total patients
(N) Success Failed Died Defaulted
Months n % n % n % n % 0 (Placebo)
73 45 61% 13 18% 6 8% 9 12% 100 mg BID
80 48 60% 12 15% 9 11% 11 14% 200 mg BID
76 50 66% 12 16% 4 5% 10 13%
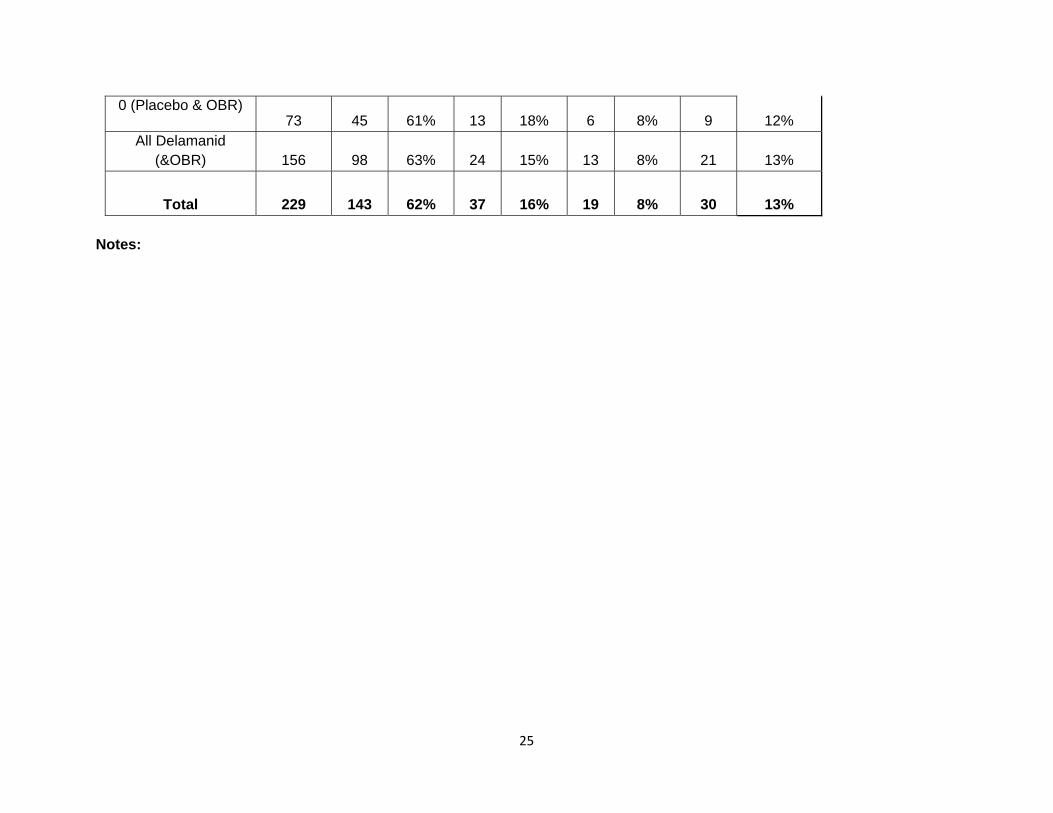
Total 229 143 62% 37 16% 19 8% 30 13% Table 5D. Final treatment outcomes (combining cure and completion as 'success') at 24 months for patients – by original randomization in Study 204 to optimized background regimen (OBR) plus 2 months delamanid or placebo.
(ONLY patients who did not take Delamanid in Study 208)
Delamanid In First TWO months
Total patients
(N) Success Failed Died Defaulted
Months n % n % n % n %
25
0 (Placebo & OBR) 73 45 61% 13 18% 6 8% 9 12%
All Delamanid (&OBR) 156 98 63% 24 15% 13 8% 21 13%
Total 229 143 62% 37 16% 19 8% 30 13% Notes:
26
6a. Total serious adverse events reported during study phase (first two months) in participants in Study 204. (All patients randomized who received at least 1 dose of study drug)
Regimen Total
patients Serious Adverse
events (SAE) Treatment Emergent
SAE Therapy stopped for
SAE
(N) n % n % n % OBR & Placebo
160 14 9% 8 5% 4 2.5% OBR &
DLM 100mgBID 161 16 10% 9 6% 4 2.5%
OBR & DLM 200mgBID 160 20 13% 10 6% 6 3.8%
OBR & All doses DLM 321 36 11% 19 6% 10 3.1%
27
Table 6b. Adverse events reported during study phase (first two months) in participants in Study 204. (All patients randomized who received at least 1 dose of study drug)
Regimen OBR & Placebo OBR & Delamanid
100 mg BID OBR & Delamanid
200 mg BID
n % n % n % Total Patients
160 161 160 Gastro-intestinal
Anorexia 24 15% 23 14% 34 21%
Nausea 53 33% 58 36% 65 41%
Vomiting 44 28% 48 30% 58 36%
Cardiovascular
Palpitations 10 6% 13 8% 20 13%
Prolonged QT - Any 6 4% 16 10% 21 13%
Serious 3 2% 7 4% 9 6%
Serious & related 0 0 5 3% 4 3%
Nervous system
Tinnitus 12 8% 16 10% 22 14%
Paresthesias 12 8% 17 11% 20 13%
Headache 30 19% 36 22% 41 26%





























