Embed Size (px)
Citation preview


Emerging Type 2Diabetes Treatment:
Novel TherapySGLT-2 Inhibitors
Mark E. Molitch, MDProfessor of Medicine
Division of Endocrinology, Metabolism,and Molecular MedicineNorthwestern University
Feinberg School of MedicineChicago, Illinois

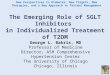
Major Therapeutic Targets in Type 2 Diabetes Mellitus (T2DM)
DeFronzo RA. Ann Intern Med. 1999;131:281-303. Buse JB, et al. In: Williams Textbook of Endocrinology. 10th ed. WB Saunders; 2003:1427-1483.
Glucose absorption
Hepatic glucoseoverproduction
Insulinresistance
Pancreas
Muscle and fat
Liver
MetforminThiazolidinedionesGLP-1 agonistsDPP-4 inhibitors
SulfonylureasMeglitinidesGLP-1 agonistsDPP-4 inhibitors
ThiazolidinedionesMetformin
Alpha-glucosidase inhibitorsGLP-1 agonists
GutGlucose
reabsorption
Kidney
Beta-celldysfunction
Glucose level
SGLT-2 inhibitors

Normal Glomerular Filtration and Renal Glucose Transport

Glomerular Filtration
• 125 mL of filtrate formed/min (180 L/24 h)1
– Urine output 1.5 L/24 h
• 25000 mEq of Na+ filtered2
– Urine Na+ excretion 100 mEq/L
• 162 g glucose filtered/24 h1
– Urine glucose excretion = 0 because reabsorption occurs
1. Abdul-Ghani M, et al. Endocr Pract. 2008;14:782-790. 2. Mount DB, et al. In: Brenner and Rector’s The Kidney. 8th ed. Elsevier Saunders; 2007:156-200.
1.5 L/24-h volume100 mEq Na+/24 h0 g/24-h glucose
180 L/24 h25000 mEq Na+/24 h
Reabsorption
Artery
Afferent Efferent Filtration
Tubular system
Secretion

Renal Glucose Transport
• GLUTs – Facilitative or passive transporters, work along a glucose gradient– Expressed in all cells—GLUT2 in kidney
• SGLTs– Active transport across membranes on lumenal side of cell using the Na+
gradient produced by Na+/K+ ATPase pumps– SGLT-2
S1 and S2 segments of proximal convoluted tubule Low affinity but high capacity for glucose Responsible for 90% of tubular reabsorption of glucose
– SGLT-1 S3 segment of proximal convoluted tubule Responsible for 10% of tubular reabsorption of glucose
Nair S, et al. J Clin Endocrinol Metab. 2010;95:34-42. Marsenic O. Am J Kidney Dis. 2009;53:875-883.

Nair S, et al. J Clin Endocrinol Metab. 2010;95:34-42. Lee YJ, et al. Kidney Int. 2007;72:S27-S35.
Active (SGLT-2) and Passive (GLUT2) Glucose Transport in S1 Renal
Proximal Tubule Cells
Abbreviations: GLUT2, glucose transporter 2; SGLT-2, sodium glucose cotransporter 2.
InterstitiumTubular lumen
Na+
GlucoseSGLT-2
ATPasepumpNa+ K+
GLUT2Glucose
Apical membrane Basolateral membrane
Na+
GlucoseSGLT-2
Na+K+
Glucose GLUT2
ATPasepump

With permission from Marsenic O. Am J Kidney Dis. 2009;53:875-883.
600
400
200
0
0 200 400 600 800
Reabsorbed
ExcretedFiltered
“Splay”
Tm
Plasma Glucose (mg/dL)
Glu
cose
(m
g/m
in)
Renal Glucose Handling
Abbreviation: Tm, transport maximum.

Rationale for SGLT-2 Inhibition in Type 2 Diabetes

SGLT-2 Expression and Glucose Uptake Are Increased in T2DM
• Human exfoliated proximal tubular epithelial cells (HEPTECs)
– Can be isolated from urine– Express a variety of proximal tubular markers, including
SGLT-2
• In HEPTECs isolated from individuals with T2DM
– SGLT-2 levels are 3-fold higher than in individuals with normal glucose tolerance (NGT)
– Renal glucose uptake is also 3-fold higher than with NGT
• Increases in renal glucose transport expression and activity seem to be associated with T2DM
Rahmoune H, et al. Diabetes. 2005;54:3427-3434.

Phlorizin
• Nonselective SGLT-2 inhibitor1
• Development deterred by its other activities
– SGLT-1 inhibition—associated with GI effects/diarrhea2
– GLUT1 inhibition by active metabolite (phloretin)—may affect glucose uptake in the GI tract1
• Effect in rodent diabetes model provided proof-of-concept for SGLT as a therapeutic target in diabetes1
1. Chao EC, et al. Nat Rev. 2010;9:551-559. 2. Wright EM. J Intern Med. 2007;261:32-43.

Phlorizin as Proof-of-Concept for SGLT Inhibition
• Phlorizin also restored fasting plasma glucose, fed plasma glucose, and glucose uptake in pancreatectomized rats
• Glucosuria: 8–9 g/dL in phlorizin vs 0.7–0.8 g/dL in pancreatectomy groups
0 60 1200
50
100
150
200
250
300
350
Placebo
Placebo + phlorizin
Pancreatectomized
Pancreatectomized + phlorizin
Time After Meal (min)
Pla
sma
Glu
cose
(m
g/d
L)
Response to Meal Tolerance Test
Rossetti L, et al. J Clin Invest. 1987;79:1510-1515.
*
*
*
*Significantly different from other groups.

SGLT-2 Inhibition IsSafe and Well Tolerated
• Familial renal glucosuria – Rare kidney disorder associated with SGLT-2 gene mutations– Absence of glucose reabsorption indicated by higher urinary
glucose excretion (1–170 g/d)– Benign, with no corresponding kidney complications
• Intestinal glucose-galactose malabsorption – Due to SGLT-1 gene mutations– Severe diarrhea
■Suggests major role for SGLT-1 in intestinal reabsorption■Corrected by removing glucose, galactose, and lactose from the diet
– Mild glucosuria consistent with minor SGLT-1 role in renal reabsorption
Wright EM. J Intern Med. 2007;261:32-43.

SGLT-2 Inhibitors in Development

Oral SGLT-2 Inhibitors in Development
SGLT-2 Inhibitor Development Phase
Dapagliflozin1 3
Canagliflozin1 3
BI107732 3
ASP19412 3
GSK1890751 2
R72011 2
TS-0713 2
CSG4524 2
LX42112 2/1*
ISIS 3886262 1
BI 448472 1
GSK16142352 1
1. Patel AK, et al. Curr Diab Rep. 2010;10:101-107. 2. ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov. Accessed on: October 2010. 3. Kakinuma H, et al. J Med Chem. 2010;53:3247-3261. 4. JAPIC Clinical Trials Information. Available at: http://www.clinicaltrials.jp/user/showCteDetailE.jsp?japicId=JapicCTI-090859. Accessed on: November 8, 2010. 5. Astellas pipeline. Available at: http://www.astellas.com/en/ir/library/pdf/4q2009_rd_en.pdf. Accessed on: November 9, 2010
Discontinued: YM543,5 AVE2268,1 T-1095,1 TS-033,1 remogliflozin,1 sergliflozin1
*LX4211 phase II efficacy study completed; phase I dosage forms study ongoing.

SGLT-2 Inhibitors in Phase III Development
Dapagliflozin

Phase III Study of Dapagliflozin in Treatment-Naive T2DM
Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224.
2-week single-blind lead-in phase: diet and exercise + placebo
T2DM Age 18–77 yTx-naive N = 591
24-week, double-blind phase
Open-label metformin was allowed for patients with fasting plasma glucose >270 mg/dL at week 4, >240 mg/dL at week 8, or >200 mg/dL at weeks 12–24
Placebo n = 75
Dapagliflozin 10 mg QD PM n = 76
Dapagliflozin 2.5 mg QD AM n = 65
Dapagliflozin 10 mg QD AM n = 70
Dapagliflozin 5 mg QD AM n = 64
Dapagliflozin 2.5 mg QD PM n = 67
Dapagliflozin 5 mg QD PM n = 68
HbA1c 7%–10%n = 485
HbA1c 10.1%–12%
n = 74
n = 35
n = 39

Phase III Study of Dapagliflozin in Treatment-Naive T2DM
Glycemic Control at Week 24
Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224.
Placebo
Dap 2.5 AM
Dap 5 AM
Dap 10 AM
Dap 2.5 PM
Dap 5 PM
Dap 10 PM
0
0.5
1
1.5
2
2.5
3
3.5
HbA1c <10.1%
HbA1c ≥10.1%
Red
uct
ion
in H
bA
1c (
%)

Phase III Study of Dapagliflozin in Treatment-Naive T2DM
Fasting Plasma Glucose Level
Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224.
Placebo Dap 2.5 AM
Dap 5 AM Dap 10 AM Dap 2.5 PM
Dap 5 PM Dap 10 PM0
10
20
30
40
50
60
70
80
90
Red
uct
ion
in F
PG
(m
g/d
L)
HbA1c <10.1%
HbA1c ≥10.1%

Phase III Study of Dapagliflozin in Treatment-Naive T2DMEffect on Body Weight at Week 24
Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224.
Red
uct
ion
in W
eig
ht
(kg
)
Placebo Dap 2.5 AM
Dap 5 AM Dap 10 AM
Dap 2.5 PM
Dap 5 PM Dap 10 PM0
0.5
1
1.5
2
2.5
3
3.5
4
HbA1c <10.1%
HbA1c ≥10.1%

Phase III 24-Wk Study of Dapagliflozin in T2DM Patients on Metformin
Bailey CJ, et al. Lancet. 2010;375:2223-2233.
Red
uct
ion
in H
bA
1c (
%)
†
*
Red
uct
ion
in F
PG
(m
g/d
L)
Dapagliflozin groups averaged 2.2–3.0 kg weight loss
N = 534
Placebo Dap 2.5 Dap 5 Dap 100
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
*P <.0002; †P <.0001; ‡P = .0019.
†
Placebo Dap 2.5 Dap 5 Dap 100
5
10
15
20
25
30
‡
†
†

Phase III 24-Wk Study of Dapagliflozin in T2DM Patients on Glimepiride
*Measured 2 h after ingestion of 75 g glucoseStrojek K, et al. 46th EASD; Sept 20-24, 2010. Abstract 870.
Red
uct
ion
in H
bA
1c (
%)
Red
uct
ion
in P
ost
pra
nd
ial
OG
TT
(m
g/d
L)*
Dapagliflozin groups averaged 1.18–2.26 kg weight loss
N = 597
Placebo Dap 2.5 Dap 5 Dap 100
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Placebo Dap 2.5 Dap 5 Dap 100
5
10
15
20
25
30
35
40

Dapagliflozin Adverse Events
• Nasopharyngitis (~3%–12%)• Diarrhea (~1%–10%)• Headache (~3%–15%)• Hypoglycemia (0%–3% in treatment-naive;
~2%–4% in patients on metformin, ~7%–8% in patients on glimepiride)
• Urinary tract infection (~4%–15%)• Genital infection (~3%–18%)• Hypotensive events (0%–5%)
Ferrannini E, et al. Diabetes Care. 2010;33:2217-2224. Bailey CJ, et al. Lancet. 2010;375:2223-2233. Strojek K, et al. 46th EASD; Sept 20-24, 2010. Abstract 870..

Additional Phase III Trials of Dapagliflozin
Results Pending
• Add-on therapy– To thiazolidinedione– To DPP-4 inhibitor– To insulin
• Special populations; patients with T2DM and– CVD– CVD + hypertension– Hypertension
inadequately controlled on ACE inhibitor or ARB
– Moderate renal impairment
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CVD, cardiovascular disease; DPP-4, dipeptidyl peptidase-4.
ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov. Accessed on: November 2010.

SGLT-2 Inhibitors in Phase III Development
Canagliflozin

Phase IIb Study of Canagliflozin Added to Metformin in Patients with T2DM
451 patients with T2DM
inadequately controlled on
metformin
Canagliflozin 50 mg QD n = 64
Canagliflozin 100 mg QD n = 64
Placebo n = 65
Canagliflozin 200 mg QD n = 65
Canagliflozin 300 mg QD n = 64
Canagliflozin 300 mg BID n = 64
Sitagliptin 100 mg QD n = 65
12-week, double-blind phase
Rosenstock J, et al. 70th ADA; June 25-29, 2010. Abstract 77-OR.

Phase IIb Study of Canagliflozin in T2DM Patients on Metformin
Glycemic Control at Week 12
Can 50 QD
Can 100 QD
Can 200 QD
Can 300 QD
Can 300 BID
Sit 65 QD
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Rosenstock J, et al. 70th ADA; June 25-29, 2010. Abstract 77-OR.
Pla
ceb
o-A
dju
sted
Red
uct
ion
in
Hb
A1c
(%
) vs
Bas
elin
e
Can 50 QD
Can 100 QD
Can 200 QD
Can 300 QD
Can 300 BID
Sit 65 QD
0
5
10
15
20
25
30
35
Pla
ceb
o-A
dju
sted
Red
uct
ion
in F
PG
(m
g/d
L)
vs B
asel
ine
P vs placebo ≤.001 for all groups P vs placebo ≤.001 for all groups

Phase IIb Study of Canagliflozin in T2DM Patients on Metformin
Effect on Body Weight at Week 12
• Placebo-adjusted change in body weight– Canagliflozin groups lost 1.3–2.3 kg (dose-
dependent effect) Significant differences at all doses vs placebo
– Sitagliptin group gained 0.4 kg
Rosenstock J, et al. 70th ADA; June 25-29, 2010. Abstract 77-OR.

Canagliflozin Added to Metformin Adverse Effects
Canagliflozin (All Doses)
Sitagliptin Placebo
Genital infections 3%–8% 2% 2%
Urinary tract infections
3%–9% 2% 6%
Hypoglycemia 0%–6% 5% 2%
Rosenstock J, et al. 70th ADA; June 25-29, 2010. Abstract 77-OR.
No safety signals in laboratory abnormalities, echocardiogram, or vital signs with canagliflozin

Phase III Trials of CanagliflozinResults Pending
• Monotherapy• Add-on to metformin • Add-on to metformin and sulphonylurea• Add-on to metformin and pioglitazone• Patients with cardiovascular risk factors• Elderly patients• Patients with moderate renal impairment
ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov. Accessed on: November 2010.

Other SGLT-2 Inhibitors in Phase III Development
BI10773 and ASP1941

Phase II Study of BI10773
80 patients with T2DM
BI10773 10 mg QD
BI10773 25 mg QD
Placebo
BI10773 100 mg QD
4-week, double-blind phase
Heise T, et al. 70th ADA; June 25-29, 2010. Abstract 629-P.

Phase II Study of BI10773Effect on Glucose Levels
Placebo BI10773 10 mg
BI10773 25 mg
BI10773 100 mg
0
10
20
30
40
50
60
70
80
90
Heise T, et al. 70th ADA; June 25-29, 2010. Abstract 629-P.
Uri
nar
y G
luco
se E
xcre
tio
n (
g)
Placebo BI10773 10 mg
BI10773 25 mg
BI10773 100 mg
0
5
10
15
20
25
30
35
40
45
50
Red
uct
ion
in F
PG
(m
g/d
L)

Phase IIa Study of ASP1941 in T2DM
61 patients with T2DM:
either tx naive,on monotherapy,
or onlow-dose
combination therapy
ASP1941 50 mg QD n = 12
ASP1941 100 mg QD n = 12
Placebo n = 13
ASP1941 200 mg QD n = 12
ASP1941 300 mg QD n = 12
28-day, double-blind phase
Schwartz S, et al. 70th ADA; June 25-29, 2010. Abstract 0566-P.
2-wk washout
for patients already on treatment

Phase IIa Study of ASP1941 in T2DMEffects on Glucose Levels
Placebo
ASP 50
ASP 100
ASP 200
ASP 300
0
100
200
300
400
500
600
Schwartz S, et al. 70th ADA; June 25-29, 2010. Abstract 0566-P.
24-h
Uri
nar
y G
luco
se E
xcre
tio
n (
mm
ol)
Placebo
ASP 50
ASP 100
ASP 200
ASP 300
0
10
20
30
40
50
60
70
80
Red
uct
ion
in F
PG
(m
g/d
L)
*
**
†
*P <.001; †P <.005.Weight loss: 3.2–4.2 kg with
ASP1941, 1.8 kg with placebo

Most Frequent Adverse Events
BI107731
• Frequent urination• Nasopharyngitis• Constipation• Headache
ASP19412
• Constipation• Nausea• Xerosis• Headache
1. Heise T, et al. 70th ADA; June 25-29, 2010. Abstract 629-P. 2. Schwartz S, et al. 70th ADA; June 25-29, 2010. Abstract 0566-P.

BI10773 Phase III StudiesResults Pending
• Monotherapy in treatment-naive T2DM• Monotherapy in T2DM pretreated with metformin• Add-on to metformin or metformin/sulfonylurea• Add-on to pioglitazone or pioglitazone/metformin• Add-on to usual care in patients at high
cardiovascular risk• Add-on to pre-existing therapy in patients with renal
impairment
ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov. Accessed on November 2010.

Phase III Trials of ASP1941Results Pending
• Monotherapy in Japanese patients with T2DM
• Add-on to metformin
• Add-on to thiazolidinedione
• Add-on to sulfonylurea
• Add-on to DPP-4 inhibitor
• Add-on to alpha-glucosidase inhibitor
ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov. Accessed on November 2010.

Where Will SGLT-2 Inhibitor Therapy Fit?
• Combination therapy– Novel mechanism of action– Complementary to available agents
• Second-line therapy
• Monotherapy– Possibly in cases of metformin intolerance
• Use in T1DM and T2DM?

Summary• SGLT-2 is a low-affinity high-capacity glucose
transporter located in the proximal tubule and is responsible for 90% of glucose reabsorption
• Mutations in SGLT-2 transporter linked to hereditary renal glycosuria, a benign condition
• Oral selective SGLT-2 inhibitors in development reduce blood glucose levels by increasing renal excretion of glucose
• Selective SGLT-2 inhibition results in loss of 200–300 kcal/d, associated with weight loss
• SGLT-2 inhibitors are generally well tolerated
Brooks AM, et al. Ann Pharmacother. 2009;43:1286-1293.

Thank you for your participation.
To earn CME/CE credit, please complete the posttest and evaluation. (Click link in the navigation bar above or to the left of the slide presentation.)
Your feedback is appreciated and will help us continue to provide you with clinically relevant
educational activities that meet your specific needs.