Embed Size (px)
Citation preview

TheProstate 72:338^349 (2012)
EmergingTreatmentOptions for PatientsWithCastration-Resistant ProstateCancer
Daniel George1* and Judd W. Moul2y
1DivisionsofMedical OncologyandUrology,DukeUniversityMedical Center,Durham,NorthCarolina2DivisionofUrology,Departmentof Surgery, andDuke Prostate Center,DukeCancer Institute,
DukeUniversityMedical Center,Durham,NorthCarolina
BACKGROUND. Most prostate cancer-related deaths occur in patients with castration-resistant prostate cancer (CRPC). Recent preclinical and clinical studies have identified intra-cellular signaling pathways and changes in the tumor and bone microenvironment as poten-tial key drivers of CRPC. This increased understanding of mechanisms associated with CRPChas driven the development of numerous new agents, many of which are poised to alter thecurrent CRPC treatment landscape.METHODS. A review of literature was conducted to identify ongoing and planned phase IIIstudies of novel agents to treat CRPC.RESULTS. Multiple studies were identified, including novel androgen biosynthesis inhibi-tors (abiraterone, TAK-700), androgen-receptor inhibitors (MDV3100), angiogenesis inhibi-tors (aflibercept, tasquinimod), endothelin antagonists (zibotentan, atrasentan), a Src tyrosinekinase inhibitor (dasatinib), a novel radiotherapy (radium-223), and new immunotherapies(ipilimumab and ProstVac). In addition, both sipuleucel-T (an immunotherapy) and cabazi-taxel (third-generation taxane) and the RANK-L inhibitor, denosumab, have recently beenapproved by the US Food and Drug Administration.CONCLUSIONS. Various combinations of these agents could theoretically be used to treatfuture patients with CRPC by targeting multiple signaling pathways as well as aspects ofthe tumor and bone microenvironments. Additional research will be needed to understandhow to best use these agents and individualize care to optimize CRPC patient outcomes.Prostate 72: 338–349, 2012. # 2011 Wiley Periodicals, Inc.
KEY WORDS: androgen-independent prostate cancer; targeted agent; progression;resistance
INTRODUCTION
Prostate cancer growth is initially dependent oncirculating androgens, as evidenced by declines in se-rum prostate-specific antigen (PSA) levels and clinicalimprovement in patients with prostate cancer treatedwith androgen deprivation therapy (ADT) via medi-cal or surgical castration. Over time, and despite cas-trate levels of androgen, many patients developcastration-resistant prostate cancer (CRPC) and dis-ease progression noted by rising serum PSA, radio-graphic progression, or symptoms. CRPC is alsoassociated with significant morbidities (i.e., fatigue,anorexia, weight loss, bone pain, bone fracture,urinary tract obstruction, spinal cord compression,hematologic disturbances, and edema) ultimatelyresulting in prostate cancer-related deaths.
Disclosures: Daniel George, MD, serves as a speaker for Dendreon,Genentech/Roche, Novartis, Pfizer, and Sanofi-Aventis; is a consul-tant for Astellas, Dendreon, Genentech/Roche, J&J, Medivation,Novartis, Pfizer, and Sanofi-Aventis; and receives research grantsfrom AstraZeneca, Dendreon, GlaxoSmithKline, J&J, Novartis, andPfizer. Judd W. Moul, MD, serves as a speaker for Sanofi-Aventis, isa consultant for Amgen, AstraZeneca, Bayer, and Medivation, andis a clinical trial investigator for AstraZeneca.yDirector, Duke Prostate Center, Division Chief.
*Correspondence to: Daniel George, MD, Associate Professorof Medicine and Surgery, Director of Genitourinary Oncology,Divisions of Medical Oncology and Urology, Duke University Med-ical Center, Durham, NC 27705. E-mail: [email protected] 15 March 2011; Accepted 12 May 2011DOI 10.1002/pros.21435Published online 11 July 2011 in Wiley Online Library(wileyonlinelibrary.com).
� 2011WileyPeriodicals,Inc.

The clinical course of CRPC varies: patients may havenonmetastatic disease, asymptomatic metastatic dis-ease, or symptomatic metastatic disease. For patientswith nonmetastatic CRPC, active surveillance coupledwith continued ADT is a reasonable alternative to ad-ditional treatment. However, many patients, especial-ly those with rapid PSA doubling times (<6 months)and PSA levels >20 ng/ml, will receive treatmentsemploying a variety of strategies to interfere with pro-gression and prevent metastases [1].
Recent preclinical and clinical studies haveidentified key drivers of prostate cancer progression,including compensatory signaling, crosstalk thatinfluences the transition from an androgen-dependentto an androgen-independent phenotype, and changesin the tumor-bone microenvironment. As these path-ways are characterized, there is growing interestin the development of novel agents that have thepotential to expand the armamentarium available tourologists and oncologists. Several agents are underdevelopment or are nearing regulatory approval,which places clinicians at the cusp of an exciting peri-od in the treatment of CRPC. This review will providean overview of CRPC and discuss emerging treatmentoptions for this disease including novel targetedagents, hormonal therapies, chemotherapies, immu-notherapies, and radiotherapies.
OverviewofMechanismsofProstateCancerProgressionandDevelopmentofCRPC
During disease progression, CRPC increasingly uti-lizes salvage pathways to evade therapeutic attemptsto block growth. Multiple mechanisms that may driveprogression involve the androgen-receptor (AR) path-way, including: (1) overexpression of AR; (2) ARmutations that increase androgen sensitivity to or ac-tivation by other steroids; (3) increased local andro-gen production by prostate cells via expression ofsteroidogenic enzymes; (4) AR activation via crosstalkof signal transduction pathways (e.g., epidermalgrowth factor [EGF], insulin-like growth factor[IGF], interleukin-6); (5) modulated expression of co-activators or co-repressors of AR; and (6) proteolyticprocessing of AR to an androgen-independentisoform [2].
Mounting evidence also implicates the interplaybetween prostate cancer cells and the bone microenvi-ronment in promoting tumor cell growth as well asstimulating angiogenesis and metastasis. The stromasurrounding the healthy prostate contains fibroblasts,and smooth muscle cells that secrete growth factorsand respond to extracellular signals. With diseaseprogression, the stroma shows progressively abnor-mal cellular composition, histology, and dysregulated
intercellular communication. These carcinoma-reactivestromal cells secrete enzymes involved in the degra-dation of extracellular matrix and several solublefactors (e.g., transforming growth factor b [TGFb],vascular endothelial growth factor [VEGF], platelet-derived growth factor [PDGF] and its receptor[PDGFR], IGF-1, EGF, and fibroblast growth factor)that engage in crosstalk with tumor cells and maydrive progression [3].
Although bone is the most common site of CRPCmetastasis, the precise mechanisms by which prostatecancer cells metastasize to bone remains unknown.However, the pattern of bone involvement (usuallyaxial versus appendicular bones), suggests involve-ment of the bone marrow. Alternatively, CRPC maytarget bone because of soluble and insoluble factorssecreted by the bone that may promote tumor coloni-zation. As a result, the combined targeting of tumorand bone microenvironments is promising.
Late-Stage InvestigationalAgents
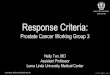
Several agents targeting important cell signalingpathways within the tumor-bone microenvironmentare in late-stage clinical development as monothera-pies or combined with other agents (Fig. 1). Key char-acteristics for these agents are listed in Table I.Table II summarizes ongoing phase III clinical trialsinvestigating the use of these agents in CRPC.
Novel Androgen Biosynthesis Inhibitors and Anti-Androgens. Despite castration levels of testosterone,CRPC retains some androgen responsiveness, whichmay be related to AR upregulation or local androgensynthesis. Several potential mechanisms underlyingandrogen dependence are important, including intra-tumoral androgen concentrations at levels sufficientlyhigh to activate AR [4], and increased expression ofenzymes crucial for androgen synthesis [5]. Thesedata support the hypothesis that additional hormonalinhibition via next generation androgen inhibitorssuch as abiraterone and MDV3100 are effectiveoptions for treating CRPC.
Abiraterone acetate is an oral, irreversible selectiveinhibitor of cytochrome P17, a microsomal enzymekey to androgen and estrogen synthesis [6]. In dose-escalation phase I studies, abiraterone monotherapydid not result in dose-limiting toxicities (DLTs) andresulted in �50% declines in PSA in chemotherapy-naive CRPC patients [6], and those previously treatedwith ketoconazole [7]. In a phase II study of 47 meta-static CRPC patients previously treated with doce-taxel, 51% of patients had �50% declines in PSA frombaseline at least once and 27% of those with measur-able disease experienced a partial response (PR) by
EmergingTreatmentOptionsinCRPC 339
The Prostate

investigator’s assessment per RECIST [8]. The mostcommon toxicities were hypokalemia, hypertension,peripheral edema, and fatigue [6–8].
Results from the phase II portion of a phase I/IIstudy showed that 67% of chemotherapy-naive CRPCpatients had �50% declines in PSA and 38% ofpatients had PRs per independent RECIST assessment[9]. In a phase II study of abiraterone plus prednisonein 58 patients with progressive metastatic CRPCand docetaxel-based chemotherapy failure, 36% ofpatients had �50% decline in PSA and 18% of patientshad PRs [10].
Two placebo-controlled phase III trials have com-pleted enrollment and are comparing abirateroneplus prednisone/prednisolone versus prednisone/prednisolone alone: one in patients with asymptomat-ic or mildly symptomatic metastatic CRPC (NationalClinical Trials [NCT] Identifier; NCT00887198) andone in metastatic CRPC patients after docetaxel fail-ure (NCT00638690). Recently, the phase III trial ofpatients with metastatic CRPC after docetaxel failurewas unblinded after a preplanned interim analysisdemonstrated significant improvement in overall
survival (OS). Median OS was 14.8 months forabiraterone compared with 10.9 months for placebo(hazard ratio [HR] 0.65, 95% confidence interval [CI]0.54–0.77; P < 0.0001). There were also highly signi-ficant improvements in time to PSA progression(TTPSA), radiographic progression-free survival(PFS), and PSA response rate [11]. Patients receivingplacebo were permitted to cross over to the abirater-one arm [12].
TAK-700 is an oral inhibitor of the 17,20-lyase en-zyme, another key steroidogenic enzyme involved inandrogen biosynthesis [13]. The phase I portion of aphase I/II study evaluated five doses of TAK-700(100, 200, 300, 400, and 600 mg BID) in 26 metastaticCRPC patients (in 19% of patients, TAK-700 mg BIDplus prednisone 5 mg BID were administered). Allpatients given �300 mg BID experienced decreases inPSA. The most common treatment-related toxicitieswere fatigue, nausea, constipation, anorexia, andvomiting.
MDV3100 is an AR antagonist with no agonistactivity in experimental CRPC models [14]. In a phaseI/II study of 140 patients with progressive metastatic
Fig. 1. Overviewof tumor-bonemicroenvironment andnovel therapeutics (red font) inCRPC.These agents stimulate the immune system,inhibit steroid or tyrosine kinase-mediated signaling, block angiogenesis, interferewith endothelin signaling, and impair osteoclast function.Novel chemotherapies (e.g., cabazitaxel) are not shown and inhibit the cell cycle. Abbreviations: APC, antigenpresenting cell; AR, androgenreceptor; CTLA-4, cytotoxicT-lymphocyte antigen-4; CoAct, co-activating factors; DHEA, dehydroepiandrosterone; DHT, dihydrotesto-sterone; ETA, endothelin receptor type A; PAP, prostate acid phosphatase; MHC1, major histocompatibility complex class I; VEGF, vascularendothelial growth factor; RANK, receptor activator of nuclear factor-kB; RANKL, receptor activator of nuclear factor-kB ligand; RTK,receptor tyrosinekinase;T, testosterone.
340 George andMoul
The Prostate

TABLE
I.Inve
stigationalAge
ntsinLate-Stage
Dev
elop
men
tfor
Castration-Resistant
Pro
stateCan
cer(C
RPC)
Agen
tPatientpopulation
Class
Efficacy
Most
commontoxicities
Stage
Abiraterone[6–8
]MetastaticornonmetastaticCRPC
asmeasu
redbyPSA
rise;
chem
otherap
ynaive[6,7];prior
docetaxel
chem
otherap
y[8]
Androgen
biosynthesis
inhibitor
51%
declinein
PSA�5
0%;27%
PR
inphaseII.O
Sben
efitin
interim
analysisofphaseIIItrialafter
docetaxel
failure
Hypokalem
ia,hypertension,
fluid
retention,fatigue
FDA
approved
(4-201
1)
TAK-700
[13]
MetastaticCRPC
Androgen
biosynthesis
inhibitor
100%
PSA
resp
onse
rate
inpatientsreceiving�3
00mgBID
Fatigue,nau
sea,
constipation,
anorexia,vomiting
PhaseII
MDV3100
[14,15]
MetastaticCRPCas
measu
redby
PSA
rise;ch
emotherap
ynaive
[14,15
];failure
oftaxan
e-based
chem
otherap
y[14]
Anti-androgen
62%
forpatients
withnoprior
chem
otherap
yan
d51
%forpatients
withprior
chem
otherap
ydeclinein
PSA
�50%
;22
%PRs
Fatigue
PhaseIII
Bev
acizumab
[19]
MetastaticCRPCwithev
iden
ceofprogressivedisease;
chem
otherap
ynaive
Anti-angiogen
icNoim
provem
entin
OSwhen
added
toDP
More
morbidityan
dmortality
compared
withDPþ
placebo
FailedphaseIII
Aflibercept[21,22]
Refractory
solidtumors;ch
e-motherap
ynaive
Anti-angiogen
icNodatafrom
phaseIItrialsin
prostatecancer
Proteinuria,
hypertension
PhaseIII
Tasquinim
od[25]
MetastaticCRPC
Anti-angiogen
ic6-month
PFS69
%vs.placebo34
%;
med
ianPFS8.4monthsvs.3.8
monthsforplacebo
Most
commongrade3–
4AEs
wereincreasedlipaseor
amylase,muscularweakness,
pain
PhaseIIIunderway
Zibotentan
(ZD4054
)[31,32]
NonmetastaticCRPCan
dasymptomatic
orsymptomatic
forpain(N
CT0062
6548,
NCT00
5542
29);metastatic
CRPCan
dsymptomatic
for
pain(N
CT0061
7669
);ch
e-motherap
ynaive[31,32]
Endothelin
receptorA
inhibitor
Noim
provem
entin
TTP;med
ian
OS17
.3monthsforplacebovs.
24.5
monthsfor10
-mgdose
vs.
23.5
monthsfor15
-mgdose
[31].Updated
OS:med
ianOS
19.9monthsforplacebovs.23
.5monthsfor10
-mgvs.23
.9monthsfor15
-mgdose
[32]
Peripheral
edem
a,headache,
nasal
congestion;few
grade
3–4AEs
PhaseIII
Dasatinib
[35]
Metastaticornonmetastatic
CRPCas
measu
redbyPSA
rise;ch
emotherap
ynaive
Src,BCR-A
BL,PDGFR,
andc-KIT
inhibitor
NoCRsorPRs,butlastingSDseen
inaphaseIIstudy
Pleuraleffusions,diarrhea,
nau
sea,
fatigue
PhaseIII
Sipuleucel-T[37,39]
Metastaticornonmetastatic
CRPCas
measu
redbyPSA
rise;priorch
emotherap
ywithin
theprevious3months
Immunotherap
yNodifference
inTTP,but
significan
tlyim
proved
OS
compared
withplaceboin
phaseIIan
dIIIstudies
Infusion-related
even
ts,myalgia,
hypertension,hyperhidrosis,
groin
pain
FDA
approved
(4-201
0)
ProstVac
[41]
MetastaticCRPCas
measu
red
byPSA
rise
orradiography;
chem
otherap
ynaive
Immunotherap
yNodifference
inPFSbut
improved
OScompared
with
placeboin
aphaseIIstudy
Infusion-related
even
ts,fatigue,
fever,nau
sea
PhaseIIIstudiesunderway
Ipilim
umab
[42,43]
MetastaticCRPCas
measu
red
byPSA;priorch
emotherap
ywithin
theprevious1month
Monoclonal
antibody
More
patients
treatedwith
ipilim
umab
þAA
had
undetectable
PSA
at3months
compared
withAA
alonein
aphaseIIstudy
Colitis,diarrhea,cu
taneo
us
chan
ges
PhaseIII
(Continued)
EmergingTreatmentOptionsinCRPC 341
The Prostate

CRPC treated with MDV3100, 56% had a �50%reduction in PSA and 22% of 59 patients with softtissue disease had PRs [15]. PSA declines �50%were reported in 62% of the 65 chemotherapy-naivepatients and 51% of 75 patients previously treatedwith chemotherapy. MDV3100 treatment also resultedin a 25% improvement from baseline in TTPSA [15].Fatigue was the most common toxicity. The ongoingAFFIRM phase III trial is comparing MDV3100 versusplacebo in CRPC patients who previously receiveddocetaxel (NCT00974311), while the PREVAIL trial willcompare MDV3100 versus placebo in chemotherapy-naive CRPC patients (NCT01212991).
Anti-Angiogenic Therapies. Angiogenesis has beenimplicated in prostate cancer progression and metas-tasis and retrospective studies suggest measures suchas plasma VEGF levels [16], and microvessel density[17] may have prognostic significance. Several anti-angiogenic agents are being clinically investigated in-cluding bevacizumab, aflibercept, and tasquinimod.
In a phase II trial of 60 patients with progressivemetastatic CRPC, the combination of bevacizumab,thalidomide, and docetaxel resulted in 90% ofpatients having a �50% PSA decline and 64% of 33evaluable patients achieving PRs [18]. Median PFSwas 18.3 months and median OS was 28.2 months.Despite these promising results, bevacizumab hasbeen unsuccessful in the phase III setting. In the ran-domized, double-blind, placebo-controlled CALGB90401 study, the addition of bevacizumab to docetaxeland prednisone (DP) did not improve OS (the prima-ry endpoint) in 1,025 metastatic CRPC patients andwas associated with a higher incidence of morbidityand mortality [19]. Median OS was 22.6 months forbevacizumab plus DP compared with 21.5 months forDP (HR 0.91, 95% CI 0.78–1.05; P ¼ 0.181). The sec-ondary endpoint of median PFS was higher in thebevacizumab group compared with the placebogroup (9.9 months vs. 7.5 months; HR 0.77, 95% CI0.68–0.88; P < 0.0001). In addition, objective and PSAresponse rates were greater in the bevacizumab arm.Patients given bevacizumab had significantly moregrade 3–4 toxicities (74.8% vs. 55.3%, respectively;P < 0.001) and treatment-related deaths (4.4% vs.1.1%, respectively; P < 0.0014).
Aflibercept is a soluble form of human VEGF re-ceptor that avidly binds VEGF and inhibits preclinicalCRPC models [20]. A phase I study of aflibercept inpatients with refractory solid tumors or non-Hodgkinlymphoma resulted in three PRs in patients with thy-mic and ovarian cancers [21]. Rectal ulceration andproteinuria were the DLTs observed and no patientsdeveloped anti-aflibercept antibodies. In a phase Istudy of aflibercept in 38 patients with advanced solidTA
BLE
I.(C
ontinu
ed)
Agen
tPatientpopulation
Class
Efficacy
Most
commontoxicities
Stage
Den
osu
mab
[45]
CRPCan
dat
least1bone
metastasis,butnoprior
bisphosp
honateuse
Monoclonal
antibody
Delay
edtimeto
firston-study
SREan
ddelay
edtimeto
multiple
SREscompared
with
zoledronic
acid
Anem
ia,backpain,decreased
appetite,nau
sea,
fatigue
FDA
approved
(11-20
10)
Cab
azitax
el[46,47]
MetastaticCRPC[47];refractory
solidtumors
[46];prior
horm
onetherap
y[47]
or
chem
otherap
y
Chem
otherap
yCbzP
improved
OS,P
FS,response
rate,T
TPcompared
withMPin
phaseIIIstudy
Feb
rile
neu
tropen
ia,diarrhea
FDA
approved
(6-201
0)
Rad
ium-223
[49,50]
MetastaticCRPCas
measu
red
byPSA
rise
andbonepainRT
Injectab
leform
of
radium-223
Survival
ben
efitsu
rvival,PSA
resp
onse,an
dpainpalliation
inphaseIIstudies
Gastrointestinal,musculoskeletal
PhaseIII
AA,an
drogen
ablation;AE,ad
verse
even
t;CbzP
,cabaz
itax
elþ
prednisone;
CR,complete
resp
onse;DP,docetaxel
þprednisone;
MP,mitoxan
troneþ
prednisone;
NCT,
National
Clinical
Trial;O
S,o
verallsu
rvival;P
DGFR,p
latelet-derived
growth
factorreceptor;PFS,p
rogression-freesu
rvival;P
R,p
artial
resp
onse;P
SA,p
rostate-sp
ecifican
tigen
;RT,rad
iotherap
y;S
D,stable
disease;SRE,skeletal-related
even
t;TTP,tim
eto
progression;F
DA,U
SFoodan
dDrugAdministration.
342 George andMoul
The Prostate

tumors, 53% of patients maintained stable disease(SD) for at least 1 month and 2 patients (1 withadvanced-stage bronchoalveolar carcinoma and 1with thyroid cancer) maintained SD for more than ayear [22]. Here, the maximum tolerated dose was notreached because of solubility and dosing issues relat-ed to the subcutaneous formulation. Few patients(7%) experienced grade 3–4 toxicities and the mostcommon dose-related toxicities were hypertension,hoarseness, and anorexia. The ongoing VENICEplacebo-controlled, double-blind phase III trial iscomparing treatment with DP versus aflibercept plusDP in metastatic CRPC patients (NCT00519285).
The quinoline-3-carboxamide derivative tasquini-mod is an anti-angiogenic agent thought to upregu-late thrombospondin-1 as part of a mechanisminvolving downregulation of hypoxia-inducible factor-1a and VEGF [23]. In phase I studies, treatment forup to 1 year with tasquinimod led to PSA declines�50% in two CRPC patients [24]. The DLTs observedwere sinus tachycardia and asymptomatic amylase
elevation. In a phase II randomized study of 200metastatic CRPC patients, tasquinimod monotherapyimproved the primary endpoint of PFS at 6 monthsversus placebo (69% vs. 34%, respectively; P < 0.0001),as well as median PFS (8.4 months vs. 3.8 months,respectively; P ¼ 0.0045) [25]. The most commontasquinimod-related toxicities were gastrointestinaldisorders, fatigue, and musculoskeletal pains.
Endothelin Antagonists. The endothelin signalingpathway, composed of three vasoconstricting 21-aminoacid endothelin (ET) peptides (ET-1, ET-2, ET-3) and2 G-protein-coupled receptors (ETA and ETB), isinvolved in the growth and progression of solidtumors, including prostate cancer, through inductionof cell proliferation, survival, angiogenesis, andmetastasis [26]. Of agents targeting this signalingpathway, atrasentan and zibotentan are at the mostadvanced stages of development.
Atrasentan is a competitive inhibitor of ET-1 thatbinds to ETA with an 1,800-fold higher affinity than
TABLE II. OngoingRandomizedPhase IIIClinicalTrialsWithLate-Stage InvestigationalAgentsinMenPatientsCastration-ResistantProstateCancer(CRPC)
AgentTrial (NCTidentifier) Treatment regimen/study arms
Disease state/inclusioncriteria
Primaryendpoint
PlannedN Status
Abiraterone OU-AA-301(NCT00638690)
Abirateroneþprednisone/prednisolone pboþprednisone/prednisolone
Metastatic, previous docetaxel OS 1,158 Open
Abiraterone COU-AA-302(NCT00887198)
Abirateroneþprednisone/prednisolone vs. pboþprednisone/prednisolone
Metastatic, asymptomatic ormildly symptomatic
OS and PFS 1,000 Open
MDV3100 AFFIRM(NCT00974311)
MDV3100 vs. pbo Progressive disease, 1–2 priorchemotherapy, priordocetaxel
OS NA Open
Aflibercept VENICE(NCT00519285)
Afliberceptþdocetaxelþprednisone/prednisolone vs. pboþdocetaxelþprednisone/prednisolone
Progressive metastatic disease OS 1,200 Open
Zibotentan ENTHUSE M1(NCT00554229)
ZibotentanþBSC vs. pboþBSC Progressive disease with bonemetastases, no or mild pain
OS 848 Completed[33]
Zibotentan ENTHUSE M0(NCT00626548)
ZibotentanþBSC vs. pboþBSC Progressive disease, nometastases
PFS 1,500 Stopped[34]
Zibotentan ENTHUSE M1C(NCT00617669)
Zibotentanþdocetaxel vs.pboþdocetaxel
Progressive metastatic diseasewith bone metastases
OS 1,445 Open
Atrasentan SWOG-S0421(NCT00134056)
Atrasentanþdocetaxelþprednisonevs. pboþdocetaxelþprednisone
Stage IV disease with bonemetastases
OS and PFS 930 Stopped
Dasatinib CA180-227(NCT00744497)
Dasatinibþdocetaxelþprednisonevs. pboþdocetaxelþprednisone
Progressive metastatic disease OS 1,380 Open
Ipilimumab CA184-043(NCT00861614)
Ipilimumab vs. pbo Metastatic disease with �1bone metastasis, priordocetaxel
OS 800 Recruiting
Ipilimumab CA184-095(NCT01057810)
Ipilimumab vs. pbo Progressive metastatic disease,asymptomatic or minimallysymptomatic, no priorimmunotherapy orchemotherapy
OS 600 Recruiting
Radium-223 ALSYMPCA(NCT00699751)
Radium-223 chloride vs. pbo Metastatic disease with bonemetastases, no intent to usecytotoxic chemotherapy�6 months
OS 900 Open
BSC, best supportive care; OS, overall survival; NA, not available; NCT, National Clinical Trial; pbo, placebo; PFS, progression-freesurvival.
EmergingTreatmentOptionsinCRPC 343
The Prostate

ETB; because of this lower but measurable bindingaffinity for ETB, atrasentan is considered less selectivethan zibotentan [27]. The intracellular signals mediat-ed by ETB are thought to mitigate ET-1 signaling viaETA. In a double-blind, placebo-controlled study of809 metastatic CRPC patients, atrasentan did notimprove the primary endpoint of time to progression(TTP) compared with placebo (HR 0.89; 95% CI 0.76–1.04; P ¼ 0.136) [28]. The secondary endpoints ofOS and TTPSA were also not improved. In anotherstudy conducted in 941 progressing nonmetastaticCRPC patients, atrasentan did not improve TTP, OS,and TTPSA over placebo (P ¼ 0.288) [29]. Notably,patients randomized to atrasentan in the UnitedStates had a shorter median TTP compared withpatients randomized to atrasentan in sites outside theUnited States; this difference appeared to be linked toregional care differences and higher treatment discon-tinuation rates in the United States. Because of earlydrug withdrawals from progression events, patientsmay have had insufficient atrasentan exposure.The most common toxicities in both studies wereperipheral edema, nasal congestion, and headache[28,29].
The SWOG S0421 placebo-controlled phase IIIstudy is comparing docetaxel plus prednisone with orwithout atrasentan in patients with stage IV CRPCand bone metastases (NCT00134056). Recently, thisstudy was halted after the Data and Safety Monitor-ing Committee concluded that the addition of atra-sentan did not improve OS or PFS compared withpatients who received a placebo.
Zibotentan (ZD4054) is an orally bioavailable spe-cific inhibitor of ETA [30]. A phase II double-blind,randomized study tested two doses of zibotentanmonotherapy against placebo in 312 patients withCRPC and bone metastases who were pain freeor mildly symptomatic and had rising PSA levels[31]. Although there was no improvement in TTP(3.7 months vs. 4.6 months vs. 3.8 months), the prima-ry endpoint, there was an encouraging >6-monthmedian OS improvement (17.3 months vs. 24.5months vs. 23.5 months) when comparing the place-bo, zibotentan 10-mg, and zibotentan 15-mg groups,respectively [31]. There were no responses perRECIST in any of the treatment groups. Few patientsexperienced grade 3–4 toxicities. The most commontoxicities associated with zibotentan treatment wereperipheral edema, headache, and nasal congestion.In the mature data analysis, there was a trend towarda 3.6-month improvement in OS for patients inthe zibotentan 10-mg group compared with placebo(23.5 months vs. 19.9 months, respectively; P ¼ 0.254)and a 4.0-month improvement in OS for patients inthe zibotentan 15-mg group versus placebo (23.9
months vs. 19.9 months, respectively; P ¼ 0.103) [32].These findings were not confirmed in the recentlycompleted phase III trial (NCT00554229; Study 14) aszibotentan did not show a significant improvementin the primary endpoint of OS [33]. In addition, aphase III study comparing zibotentan with placeboin patients with nonmetastatic-progressing CRPC(NCT00626548; ENTHUSE M0; Study 15) has alsobeen stopped following the results of an earlyefficacy review by the Independent Data MonitoringCommittee [34].
Zibotentan is being further studied in CRPC in anongoing multinational phase III trial called ENTHUSEM1C (NCT00617669). This study is comparing doce-taxel with or without zibotentan in patients with met-astatic-progressing CRPC.
Src Tyrosine Kinase Inhibitor. In addition to its rolein bone metabolism, Src has been implicated in theprogression of bone metastases [27] and interest hastherefore grown in exploring Src as a potential targetfor the treatment of CRPC. Dasatinib is an inhibitorof the Src family kinases (SFK), BCR-ABL, PDGF,and c-Kit [35]. In preclinical experiments, dasatinibinhibited SFKs, focal adhesion kinase (FAK), andCrk-associated substrate (p130CAS) signaling leadingto inhibition of cell adhesion, migration, and invasion[36].
In a phase II study of 47 chemotherapy-naivepatients with progressing metastatic CRPC, 43% ofpatients at week 12 and 19% of patients at week 24did not exhibit progression by both RECIST and bonescan analysis [35]. Although no complete responses orPRs were observed in this study, 52% of patients hadSD after 12 weeks. The most common toxicities werepleural effusion, diarrhea, nausea, and fatigue. An on-going phase III placebo-controlled randomized studyis comparing docetaxel plus prednisone with or with-out dasatinib in patients with metastatic progressingCRPC (NCT00744497).
Immune Modulators. Stimulating the immune sys-tem to attack CRPC has been extensively explored.Past investigations have focused on a multitude ofimmune stimulators including interleukins or inter-ferons, infusions of antibodies, or activated immunecells, and vaccines. Recently, several immune modu-lators, sipuleucel-T (Provenge), ProstVac, and ipili-mumab, have shown clinical promise in CRPC.
Sipuleucel-T is a cellular immunotherapy consist-ing of autologous peripheral blood mononuclear cells,obtained by leukapheresis and cultured with prostaticacid phosphatase (PAP) fusion protein, and reinfusedinto patients to induce an immune response to PAP-expressing prostate cancer cells [37]. The D9901 phase
344 George andMoul
The Prostate

III placebo-controlled trial of 127 patients with pro-gressive metastatic CRPC did not improve medianTTP (primary endpoint) in the sipuleucel-T—treatedarm versus placebo (11.7 weeks vs. 10.0 weeks,respectively; HR, 1.45; 95% CI, 0.99–2.11; P ¼ 0.052)[37]. However, median OS was significantly im-proved according to the intent-to-treat analysis(25.9 months vs. 21.4 months, respectively; HR 1.70;95% CI, 1.13–2.56; P ¼ 0.01). The most commontoxicities associated with sipuleucel-T were infusion-related rigors and pyrexia, tremors, and chills. Therewere no treatment-related study discontinuations.
A combined analysis from D9901 and the similarlydesigned D9902B showed a significant OS improve-ment in the sipuleucel-T group (n ¼ 147) versusplacebo (n ¼ 78), (23.2 months vs. 18.9 months,respectively; HR 1.50; 95% CI, 1.10–2.05; P ¼ 0.01)[38]. As in the individual studies, the combined analy-sis did not detect an improvement in median TTP(sipuleucel-T 11.1 vs. placebo 9.7 weeks; HR 1.26; 95%CI, 0.95–1.68; P ¼ 0.111).
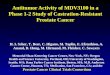
Because of results of these first two phase III stud-ies, the larger IMPACT phase III study randomized512 metastatic CRPC patients in a 2:1 ratio to sipuleu-cel-T or placebo [39]. After a median follow-upof 34.1 months, median OS (primary endpoint) was25.8 months for the sipuleucel-T group versus21.7 months for placebo (HR 0.78; 95% CI, 0.61–0.98;P ¼ 0.03; Fig. 2). The most common toxicities were in-fusion-related events (chills, fever, fatigue, headache,nausea), myalgia, hypertension, hyperhidrosis, andgroin pain. Based on these results, sipuleucel-Treceived approval from the US Food and DrugAdministration (FDA) in April 2010 for treatment
of patients with asymptomatic or minimally symp-tomatic metastatic CRPC.
ProstVac is a prostate cancer vaccine composed offowlpox and vaccinia PSA vaccines given in combina-tion with the co-stimulatory molecule transgenesintracellular adhesion molecule-1, B7, and leukocytefunction-associated antigen 3, which are administeredin a combination known as TriCom [40]. In a double-blind, placebo-controlled phase II study of 203patients with progressing metastatic CRPC, treatmentwith ProstVac did not significantly improve the pri-mary endpoint of median PFS compared with placebo(3.8 months vs. 3.7 months, respectively; HR 0.88; 95%CI, 0.57–1.38; P ¼ 0.60) [41]. However, median OSwas 25.1 months for the ProstVac group versus 16.6months for placebo (HR 0.56; 95% CI, 0.37–0.85;P ¼ 0.0061). The most common toxicities were injec-tion-site reactions, fatigue, fever, and nausea. PhaseIII studies are ongoing.
Ipilimumab is a human anti-cytotoxic T-lympho-cyte antigen-4 (CTLA-4) monoclonal antibody thatprevents CTLA-4 activation, thereby promoting andprolonging the T-cell immune response [42]. Prelimi-nary results from a randomized phase II study foundthat advanced prostate cancer patients given a singledose of ipilimumab plus ADT were more likely tohave undetectable PSA by 3 months compared withpatients given ADT alone (55% vs. 38%) [43]. Themost common grade 3–4 immune-related toxicitiesassociated with ipilimumab were colitis (4.5%) anddiarrhea (4.5%). Also, 27.7% of ipilimumab-treatedpatients experienced cutaneous changes such as local-ized vitiligo and desquamation of atypical nevi.
Ipilimumab is being further studied in twophase III randomized placebo-controlled studies,one in CRPC patients who received prior docetaxel(NCT00861614) and one in chemotherapy-naiveCRPC patients (NCT01057810).
Bone-Targeting Agents. The development of osteo-blastic metastases likely involves complex interplaybetween osteoblasts, osteoclasts, tumor cells, and thebone microenvironment, all mediated by a myriad ofsignaling molecules. For example, prostate cancercells secrete ET-1 and adrenomedullin, which canstimulate osteoblast proliferation. Osteolytic cyto-kines (e.g., parathyroid hormone, interleukin-11) inturn stimulate immature osteoblasts to express recep-tor activator of nuclear factor-kB (RANK) ligand(RANK-L), which promotes bone resorption by osteo-clasts, leading to the release of transforming growthfactor beta (TGFb) and other growth factors from themineralized bone matrix. Mature osteoblasts can alsorelease growth factors into the bone microenviron-ment. These growth factors can stimulate tumor cells,
100
80
60
40
20
00 12 24 36 48 60 72
Pro
bab
ility
of
Sur
viva
l (%
)
Months Since Randomization
PlaceboSipuleucel-T
Number at RiskSipuleucel-TPlacebo
341171
274123
129 55
4919
14 4
11
Fig. 2. Sipuleucel-T treatment improved OS compared withplacebo in the IMPACT phase III trial in patients with progressingmetastatic CRPC [39]. Adapted fromKantoff et al. [39].Copyright2010MassachusettsMedical Society.Usedwithpermission.
EmergingTreatmentOptionsinCRPC 345
The Prostate

further feeding the vicious cycle. In addition to theendothelin pathway discussed above, other molecularplayers in the cycle of bone metastases formationhave been identified as viable therapeutic targets inCRPC.
Zoledronic acid is a bisphosphonate that mini-mizes bone resorption and reduces the risk ofskeletal-related events (SREs; i.e., prevents the devel-opment of new lesions, reduces the risk of pain,reduces risk of fractures) in prostate cancer patients.Numerous ongoing phase III studies seek to broadenthe use of zoledronic acid in prostate cancer. Forexample, the CALGB-90202 study is evaluatingzoledronic acid versus placebo in preventing SREs inpatients who are receiving ADT (NCT00079001).
Denosumab is a human monoclonal antibody withspecificity for RANK-L, an important modulator ofintracellular signaling pathways involved in osteo-clast formation, function, and survival [27].
In a phase III clinical study of 1,456 men receivingADT for prostate cancer, denosumab treatment im-proved bone mineral density and reduced the cumu-lative incidence of new vertebral fractures comparedwith placebo [44]. A recent study of 1901 men withCRPC and at least one bone metastasis showed thatdenosumab was better than zoledronic acid in delay-ing or preventing SREs [45]. The median time to firston-study SRE, the primary endpoint, was 20.7 monthsfor denosumab compared with 17.1 months for zole-dronic acid (HR 0.82; 95% CI, 0.71–0.95; P ¼ 0.0002for noninferiority and P ¼ 0.008 for superiority). Thesecondary endpoint of time to first and subsequenton-study SRE also favored denosumab (denosumab494 events vs. zoledronic acid 584 events; P ¼ 0.008).However, there were no differences in PSA timecourse, overall disease progression, and OS. The twotreatment groups had a similar frequency of serioustoxicities (denosumab 63% vs. zoledronic acid 60%).The cumulative incidence of osteonecrosis of the jawwas similar in the two groups (denosumab 2.3% vs.zoledronic acid 1.3%); whereas, hypocalcemia wasmore frequent with denosumab compared with zole-dronic acid (12.8% vs. 5.8%, respectively). These andthe results of two other pivotal phase III trials com-paring denosumab with zoledronic acid in the reduc-tion of SREs have led to the recent FDA approval ofdenosumab (Xgeva) for prevention of skeletal compli-cations in patients with bone metastases from solidtumors.
Novel Chemotherapies. Cabazitaxel (XRP6258) is anovel taxane that (unlike paclitaxel and docetaxel) is apoor substrate for the drug efflux pump, P-glycopro-tein, and can evade the actions of multidrug-resistantproteins [46]. In a phase I study in patients with
advanced solid tumors, cabazitaxel could beadministered with fewer premedications than othertaxanes and was associated with a low frequency ofneurotoxicity, fluid retention, and alopecia [46].
The TROPIC randomized phase III study com-pared prednisone plus cabazitaxel or mitoxantrone(MP) in 755 metastatic CRPC patients previouslytreated with docetaxel [47]. With a median follow-upof 13.7 months, cabazitaxel significantly improvedmedian OS, the primary endpoint, compared withMP (15.1 months vs. 12.7 months, respectively; HR0.72; 95% CI 0.61–0.84; P < 0.0001), for a 28% risk re-duction. Secondary endpoints such as PFS (2.8months vs. 1.4 months; P ¼ 0.0002), response rate bytumor assessment (14.4% vs. 4.4%; P ¼ 0.0005), andmedian TTP by tumor assessment (8.8 months vs. 5.4months; P < 0.0001) were also improved in the caba-zitaxel arm compared with the MP arm. All gradesand grade 3–4 febrile neutropenia and diarrhea, aswell as grade 3–4 neutropenia and leukopenia, weremore common in the cabazitaxel treatment arm. Therewere more deaths attributed to toxicities in the cabazi-taxel arm compared with the MP arm (4.95% vs. 1.9%,respectively). The TROPIC investigators recom-mended proactive management of neutropenia anddiarrhea. In June 2010, cabazitaxel (Jevtana) was ap-proved by the FDA for the treatment of patients withmetastatic CRPC previously treated with a docetaxelregimen [48].
Novel Radiotherapies. Radium-223 chloride (223Ra,Alpharadin) is an injectable form of a-particle emit-ting radium-223 that preferentially targets bone. In arandomized, double-blind, placebo-controlled phaseII study, 64 patients with symptomatic-progressingCRPC scheduled to receive local-field external-beamradiation therapy (EBRT) to relieve pain from bonemetastases were treated with 223Ra or placebo at thetime of EBRT or within 1 week [49]. The study met itsprimary endpoints of showing a significant effect of223Ra on bone-alkaline phosphatase 4 weeks after thelast treatment and prolonging time to SREs; second-ary efficacy endpoints of TTPSA and OS were alsopositive. A combined analysis of phase I and II datacollected in metastatic CRPC patients treated with223Ra versus placebo reported reduction in bonemarkers and PSA, and improved survival [50]. Nota-bly, few patients treated with 223Ra had grade 3–4hematologic malignancies. The most common toxic-ities were nausea, bone pain, fatigue, diarrhea, vomit-ing, and constipation. Based on these promisingresults, the ongoing ALSYMPCA phase III study iscomparing treatment with 223Ra or placebo in patientswith symptomatic CRPC and skeletal metastases(NCT00699751).
346 George andMoul
The Prostate

DISCUSSION
Recent studies have identified signaling pathwaysand changes in the tumor and bone microenviron-ment as potential key drivers of CRPC. The improvedunderstanding of mechanisms associated with CRPChas resulted in the development of new agents, in-cluding several that are at advanced stages of clinicaldevelopment. The clinical successes of these agentswith differing mechanisms of action suggest that weare entering a new era of CRPC treatment. With theadvent of these novel agents and in the absence ofcomparative effectiveness data, it is likely that prac-tice patterns will vary in terms of access to and se-quencing of these treatments.
Additional research is needed to better designfuture trials and to better understand how to use eachof these agents in sequence for treating CRPC. Impor-tant strides are being made in improving patientselection through investigations of risk stratificationand of clinical or biologic predictors (e.g., biomarkersor tumor/patient characteristics) of treatmentresponses. For example, investigators have developeda potentially useful nomogram to estimate individualsurvival probabilities for patients with CRPC and tohelp stratify these patients in phase III randomizedtrials [51]. Advances in genomic approaches to identi-fy molecular signatures for tumor progression andtreatment response are also being made.
Optimized placement of each agent in the diseasecontinuum includes developing an understandingof when and how to sequence therapies and how tobest use these agents in combination with chemo-therapy. Advances are also needed in the develop-ment of clinical and biologic measures of responsesuch as tumor imaging, additional PSA measure-ments (e.g., PSA-doubling time), additional bio-markers (e.g., angiogenic, inflammatory/cytokines, orbone turnover markers), and quality-of-life measures(e.g., pain, use of opioids, and other patient-reportedoutcomes).
Theoretically, various combinations of these thera-pies may be used to target multiple aspects of thetumor microenvironment to overcome drug resis-tance. Given the variety of agents in development andin ongoing trials, there is potential for substantialstrides to be made in the treatment of CRPC. An in-crease in the number of safe and effective treatmentoptions will help patients live longer with an im-proved quality of life.
Despite these individual significant advancementsin the treatment of CRPC, the best outcomes arelikely to result from the sequential use of multipletreatments. Therefore, multidisciplinary interactionsamong urologists, medical oncologists, and radiation
oncologists will be critical to optimally manageCRPC. As no single treatment sequence is likely tobe ideal for all patients, communication and regularinteraction among treating physicians is essentialthrough the course of prostate cancer.
ACKNOWLEDGMENTS
We thank Monica Nicosia, PhD, and Brad Imwalle,PhD, from Ogilvy CommonHealth Scientific Commu-nications, who provided writing assistance funded byAstraZeneca.
REFERENCES
1. Smith MR, Kabbinavar F, Saad F, Hussain A, Gittelman MC,Bilhartz DL, Wynne C, Murray R, Zinner NR, Schulman C,Linnartz R, Zheng M, Goessl C, Hei YJ, Small EJ, Cook R,Higano CS. Natural history of rising serum prostate-specificantigen in men with castrate nonmetastatic prostate cancer.J Clin Oncol 2005;23:2918–2925.
2. Devlin HL, Mudryj M. Progression of prostate cancer: Multiplepathways to androgen independence. Cancer Lett 2009;274:177–186.
3. Niu YN, Xia SJ. Stroma-epithelium crosstalk in prostate cancer.Asian J Androl 2009;11:28–35.
4. Titus MA, Schell MJ, Lih FB, Tomer KB, Mohler JL. Testo-sterone and dihydrotestosterone tissue levels in recurrent pros-tate cancer. Clin Cancer Res 2005;11:4653–4657.
5. Stanbrough M, Bubley GJ, Ross K, Golub TR, Rubin MA, Pen-ning TM, Febbo PG, Balk SP. Increased expression of genesconverting adrenal androgens to testosterone in androgen-independent prostate cancer. Cancer Res 2006;66:2815–2825.
6. Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, SettatreeS, Barrett M, Parker C, Martins V, Folkerd E, Clark J, CooperCS, Kaye SB, Dearnaley D, Lee G, de Bono JS. Phase I clinicaltrial of a selective inhibitor of CYP17, abiraterone acetate, con-firms that castration-resistant prostate cancer commonlyremains hormone driven. J Clin Oncol 2008;26:4563–4571.
7. Ryan CJ, Smith MR, Fong L, Rosenberg JE, Kantoff P, RaynaudF, Martins V, Lee G, Kheoh T, Kim J, Molina A, Small EJ. PhaseI clinical trial of the CYP17 inhibitor abiraterone acetate dem-onstrating clinical activity in patients with castration-resistantprostate cancer who received prior ketoconazole therapy.J Clin Oncol 2010;28:1481–1488.
8. Reid AH, Attard G, Danila DC, Oommen NB, Olmos D, FongPC, Molife LR, Hunt J, Messiou C, Parker C, Dearnaley D,Swennenhuis JF, Terstappen LW, Lee G, Kheoh T, Molina A,Ryan CJ, Small E, Scher HI, de Bono JS. Significant and sus-tained antitumor activity in post-docetaxel, castration-resistantprostate cancer with the CYP17 inhibitor abiraterone acetate.J Clin Oncol 2010;28:1489–1495.
9. Attard G, Reid AH, A’Hern R, Parker C, Oommen NB, FolkerdE, Messiou C, Molife LR, Maier G, Thompson E, Olmos D,Sinha R, Lee G, Dowsett M, Kaye SB, Dearnaley D, Kheoh T,Molina A, de Bono JS. Selective inhibition of CYP17 withabiraterone acetate is highly active in the treatment of castra-tion-resistant prostate cancer. J Clin Oncol 2009;27:3742–3748.
10. Danila DC, Morris MJ, de Bono JS, Ryan CJ, Denmeade SR,Smith MR, Taplin ME, Bubley GJ, Kheoh T, Haqq C, Molina A,Anand A, Koscuiszka M, Larson SM, Schwartz LH, Fleisher M,
EmergingTreatmentOptionsinCRPC 347
The Prostate

Scher HI. Phase II multicenter study of abiraterone acetateplus prednisone therapy in patients with docetaxel-treatedcastration-resistant prostate cancer. J Clin Oncol 2010;28:1496–1501.
11. de Bono JS, Logothetis CJ, Fizazi K, North S, Chu L, Chi KN,Kheoh T, Haqq C, Molina A, Scher HI, on behalf of theCOU-AA-301 Investigators. Abiraterone acetate (AA) plus lowdose prednisone (P) improves overall survival (OS) in patients(PTS) with metastatic castration-resistant prostate cancer(MCRPC) who have progressed after docetaxel-based chemo-therapy (CHEMO): Results of COU-AA-301, a randomized,double-blind, placebo-controlled phase III study [abstract].Ann Oncol 2010;21:viii3. Abstract LBA5.
12. Study of Investigational Agent Abiraterone Acetate forMetastatic Advanced Prostate Cancer Unblinded After Meet-ing Pre-Determined Criteria. http://www.jnj.com/connect/news/product/Study-of-Investigational-Agent-Abiraterone-Acetate-for-Metastatic-Advanced-Prostate-Cancer-Unblinded-After-Meeting-Pre-Determined-Criteria. Accessed March 9,2011.
13. Dreicer R, Agus DB, MacVicar GR, MacLean D, Zhang T,Stadler WM. Safety, pharmacokinetics, and efficacy ofTAK-700 in castration-resistant, metastatic prostate cancer: Aphase I/II, open-label study. Abstract presented at: 2010 Geni-tourinary Cancers Symposium; March 5–7, 2010; San Francisco,CA.
14. Tran C, Ouk S, Clegg NJ, Chen Y, Watson PA, Arora V,Wongvipat J, Smith-Jones PM, Yoo D, Kwon A, WasielewskaT, Welsbie D, Chen CD, Higano CS, Beer TM, Hung DT, ScherHI, Jung ME, Sawyers CL. Development of a second-genera-tion antiandrogen for treatment of advanced prostate cancer.Science 2009;324:787–790.
15. Scher HI, Beer TM, Higano CS, Anand A, Taplin ME, Efsta-thiou E, Rathkopf D, Shelkey J, Yu EY, Alumkal J, Hung D,Hirmand M, Seely L, Morris MJ, Danila DC, Humm J, LarsonS, Fleisher M, Sawyers CL. Antitumour activity of MDV3100 incastration-resistant prostate cancer: A phase 1–2 study. Lancet2010;375:1437–1446.
16. George DJ, Halabi S, Shepard TF, Vogelzang NJ, Hayes DF,Small EJ, Kantoff PW. Prognostic significance of plasma vascu-lar endothelial growth factor levels in patients with hormone-refractory prostate cancer treated on Cancer and LeukemiaGroup B 9480. Clin Cancer Res 2001;7:1932–1936.
17. Weidner N, Carroll PR, Flax J, Blumenfeld W, Folkman J.Tumor angiogenesis correlates with metastasis in invasiveprostate carcinoma. Am J Pathol 1993;143:401–409.
18. Ning YM, Gulley JL, Arlen PM, Woo S, Steinberg SM, WrightJJ, Parnes HL, Trepel JB, Lee MJ, Kim YS, Sun H, Madan RA,Latham L, Jones E, Chen CC, Figg WD, Dahut WL. Phase IItrial of bevacizumab, thalidomide, docetaxel, and prednisonein patients with metastatic castration-resistant prostate cancer.J Clin Oncol 2010;28:2070–2076.
19. Kelly WK, Halabi S, Carducci MA, George DJ, Mahoney JF,Stadler WM, Morris MJ, Kantoff PW, Monk JP, Small EJ.A randomized, double-blind, placebo-controlled phase III trialcomparing docetaxel, prednisone, and placebo with docetaxel,prednisone, and bevacizumab in men with metastatic castra-tion-resistant prostate cancer (mCRPC): Survival results ofCALGB 90401 [abstract]. J Clin Oncol 2010;28: AbstractLBA4511.
20. Holash J, Davis S, Papadopoulos N, Croll SD, Ho L, Russell M,Boland P, Leidich R, Hylton D, Burova E, Ioffe E, Huang T,Radziejewski C, Bailey K, Fandl JP, Daly T, Wiegand SJ,
Yancopoulos GD, Rudge JS. VEGF-Trap: A VEGF blocker withpotent antitumor effects. Proc Natl Acad Sci USA 2002;99:11393–11398.
21. Lockhart AC, Rothenberg ML, Dupont J, Cooper W, ChevalierP, Sternas L, Buzenet G, Koehler E, Sosman JA, Schwartz LH,Gultekin DH, Koutcher JA, Donnelly EF, Andal R, Dancy I,Spriggs DR, Tew WP. Phase I study of intravenous vascularendothelial growth factor trap, aflibercept, in patients withadvanced solid tumors. J Clin Oncol 2010;28:207–214.
22. Tew WP, Gordon M, Murren J, Dupont J, Pezzulli S,Aghajanian C, Sabbatini P, Mendelson D, Schwartz L,Gettinger S, Psyrri A, Cedarbaum JM, Spriggs DR. Phase 1study of aflibercept administered subcutaneously to patientswith advanced solid tumors. Clin Cancer Res 2010;16:358–366.
23. Olsson A, Bjork A, Vallon-Christersson J, Isaacs JT, LeandersonT. Tasquinimod (ABR-215050), a quinoline-3-carboxamideanti-angiogenic agent, modulates the expression of thrombo-spondin-1 in human prostate tumors. Mol Cancer 2010;9:107.
24. Bratt O, Haggman M, Ahlgren G, Nordle O, Bjork A, DamberJE. Open-label, clinical phase I studies of tasquinimod inpatients with castration-resistant prostate cancer. Br J Cancer2009;101:1233–1240.
25. Pili R, Haggman M, Stadler WM, Gingrich JR, Assikis VJ, BjorkA, Forsberg G, Carducci MA, Armstrong AJ. A randomized,multicenter, international phase II study of tasquinimod in che-motherapy naıve patients with metastatic castrate-resistantprostate cancer (CRPC) [abstract]. J Clin Oncol 2010;28:Abstract 4510.
26. Bagnato A, Rosano L. The endothelin axis in cancer. Int JBiochem Cell Biol 2008;40:1443–1451.
27. Chi KN, Bjartell A, Dearnaley D, Saad F, Schroder FH, Stern-berg C, Tombal B, Visakorpi T. Castration-resistant prostatecancer: From new pathophysiology to new treatment targets.Eur Urol 2009;56:594–605.
28. Carducci MA, Saad F, Abrahamsson PA, Dearnaley DP,Schulman CC, North SA, Sleep DJ, Isaacson JD, Nelson JB.A phase 3 randomized controlled trial of the efficacy and safetyof atrasentan in men with metastatic hormone-refractory pros-tate cancer. Cancer 2007;110:1959–1966.
29. Nelson JB, Love W, Chin JL, Saad F, Schulman CC, Sleep DJ,Qian J, Steinberg J, Carducci M. Phase 3, randomized,controlled trial of atrasentan in patients with nonmetastatic,hormone-refractory prostate cancer. Cancer 2008;113:2478–2487.
30. Warren R, Liu G. ZD4054: A specific endothelin A receptorantagonist with promising activity in metastatic castration-re-sistant prostate cancer. Expert Opin Invest Drugs 2008;17:1237–1245.
31. James ND, Caty A, Borre M, Zonnenberg BA, Beuzeboc P,Morris T, Phung D, Dawson NA. Safety and efficacy of thespecific endothelin-A receptor antagonist ZD4054 in patientswith hormone-resistant prostate cancer and bone metastaseswho were pain free or mildly symptomatic: A double-blind,placebo-controlled, randomised, phase 2 trial. Eur Urol 2009;55:1112–1123.
32. Dawson NA, Growcott JW, Morris T, Phung DH, James ND.Zibotentan (ZD4054): A specific endothelin-A receptor antago-nist with potential for the treatment of castrate-resistantprostate cancer. Poster presented at: Society of UrologicOncology’s 10 Annual Meeting in Conjunction with the WorldUrological Oncology Federation; December 3–4, 2009;Bethesda, MD.
348 George andMoul
The Prostate

33. Results of Zibotentan Phase III trial in castration resistantprostate cancer. http://www.astrazeneca.com/Media/Press-releases/Article/Results-of-Zibotentan-Phase-III-trial-in-castration-resistant-pr. Accessed March 9, 2011.
34. AstraZeneca halts phase III trial of ZIBOTENTAN in non-metastatic castrate resistant prostate cancer. http://www.astrazeneca.com/Media/Press-releases/Article/0022011AstraZeneca-halts-phase-III-trial-of-ZIBOTENTAN. Accessed March9, 2011.
35. Yu EY, Wilding G, Posadas E, Gross M, Culine S, Massard C,Morris MJ, Hudes G, Calabro F, Cheng S, Trudel GC, PaliwalP, Sternberg CN. Phase II study of dasatinib in patients withmetastatic castration-resistant prostate cancer. Clin Cancer Res2009;15:7421–7428.
36. Nam S, Kim D, Cheng JQ, Zhang S, Lee JH, Buettner R, Mirose-vich J, Lee FY, Jove R. Action of the Src family kinase inhibitor,dasatinib (BMS-354825), on human prostate cancer cells.Cancer Res 2005;65:9185–9189.
37. Small EJ, Schellhammer PF, Higano CS, Redfern CH, Nemu-naitis JJ, Valone FH, Verjee SS, Jones LA, Hershberg RM. Place-bo-controlled phase III trial of immunologic therapy withsipuleucel-T (APC8015) in patients with metastatic, asymptom-atic hormone refractory prostate cancer. J Clin Oncol 2006;24:3089–3094.
38. Higano CS, Schellhammer PF, Small EJ, Burch PA, NemunaitisJ, Yuh L, Provost N, Frohlich MW. Integrated data from 2 ran-domized, double-blind, placebo-controlled, phase 3 trials ofactive cellular immunotherapy with sipuleucel-T in advancedprostate cancer. Cancer 2009;115:3670–3679.
39. Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ,Penson DF, Redfern CH, Ferrari AC, Dreicer R, Sims RB, Xu Y,Frolich MW, Schellhammer PF, for the IMPACT Study Investi-gators. Sipuleucel-T immunotherapy for castration-resistantprostate cancer. N Engl J Med 2010;363:411–422.
40. Dipaola RS, Plante M, Kaufman H, Petrylak DP, Israeli R,Lattime E, Manson K, Schuetz T. A phase I trial of pox PSAvaccines (PROSTVAC-VF) with B7-1, ICAM-1, and LFA-3 co-stimulatory molecules (TRICOM) in patients with prostatecancer. J Transl Med 2006;4:1.
41. Kantoff PW, Schuetz TJ, Blumenstein BA, Glode LM, BilhartzDL, Wyand M, Manson K, Panicali DL, Laus R, Schlom J,Dahut WL, Arlen PM, Gulley JL, Godfrey WR. Overall survivalanalysis of a phase II randomized controlled trial of a Poxviral-based PSA-targeted immunotherapy in metastatic castration-resistant prostate cancer. J Clin Oncol 2010;28:1099–1105.
42. Small EJ, Tchekmedyian NS, Rini BI, Fong L, Lowy I, AllisonJP. A pilot trial of CTLA-4 blockade with human anti-CTLA-4in patients with hormone-refractory prostate cancer. ClinCancer Res 2007;13:1810–1815.
43. Tollefson MK, Karnes RJ, Thompson RH, Granberg CF,Hillman DW, Breau RH, Allison JP, Blute ML, Kwon ED.A randomized phase II study of ipilimumab with androgenablation compared with androgen ablation alone in patientswith advanced prostate cancer. Abstract presented at: TheAmerican Society of Clinical Oncology Genitourinary CancersSymposium; March 5–7, 2010; San Francisco, CA.
44. Smith MR, Egerdie B, Hernandez TN, Feldman R, TammelaTL, Saad F, Heracek J, Szwedowski M, Ke C, Kupic A, LederBZ, Goessl C. Denosumab in men receiving androgen-depriva-tion therapy for prostate cancer. N Engl J Med 2009;361:745–755.
45. Fizazi K, Carducci MA, Smith MR, Damiao R, Brown JE, KarshL, Milecki P, Wang H, Dansey RD, Goessl CD. A randomizedphase III trial of denosumab versus zoledronic acid in patientswith bone metastases from castration-resistant prostate cancer[abstract]. J Clin Oncol 2010;28: Abstract LBA4507.
46. Mita AC, Denis LJ, Rowinsky EK, Debono JS, Goetz AD, OchoaL, Forouzesh B, Beeram M, Patnaik A, Molpus K, Semiond D,Besenval M, Tolcher AW. Phase I and pharmacokinetic studyof XRP6258 (RPR 116258A), a novel taxane, administered as a1-hour infusion every 3 weeks in patients with advanced solidtumors. Clin Cancer Res 2009;15:723–730.
47. de Bono JS, Oudard S, Ozguroglu M, Hansen S, Machiels JP,Kocak I, Gravis G, Bodrogi I, Mackenzie MJ, Shen L, RoessnerM, Gupta S, Sartor AO. Prednisone plus cabazitaxel or mitox-antrone for metastatic castration-resistant prostate cancer pro-gressing after docetaxel treatment: A randomised open-labeltrial. Lancet 2010;376:1147–1154.
48. Jevtana1 (cabazitaxel) Injection Approved by U.S. FDAAfter Priority Review. http://sanofi-aventis.mediaroom.com/index.php?s¼43&item¼288. Accessed March 9, 2011.
49. Nilsson S, Franzen L, Parker C, Tyrrell C, Blom R, Tennvall J,Lennernas B, Petersson U, Johannessen DC, Sokal M, Pigott K,Yachnin J, Garkavij M, Strang P, Harmenberg J, Bolstad B,Bruland OS. Bone-targeted radium-223 in symptomatic, hor-mone-refractory prostate cancer: A randomised, multicentre,placebo-controlled phase II study. Lancet Oncol 2007;8:587–594.
50. Nilsson S, Parker C, Haugen I, Lokna A, Aksnes A, Bolstad B,O’Bryan-Tear G, Bruland OS. Radium-223 chloride, a first-in-class alpha-pharmaceutical with a benign safety profile forpatients with castration resistant prostate cancer (CRPC) andbone metastases: Combined analysis of phase I and II clinicaltrials [abstract]. J Clin Oncol 2010;28: Abstract 4678.
51. Halabi S, Small EJ, Kantoff PW, Kattan MW, Kaplan EB, Daw-son NA, Levine EG, Blumenstein BA, Vogelzang NJ. Prognos-tic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J Clin Oncol 2003;21:1232–1237.
EmergingTreatmentOptionsinCRPC 349
The Prostate