Embed Size (px)
Citation preview

Emerging MedicolegalIssues in the Practiceof Pediatric SleepMedicine
Ramesh C. Sachdeva, MD, PhD, DBA, JDa,b,*, Lynn A. D’Andrea, MDc
KEYWORDS
� Medicolegal � Pediatric sleep medicine� Medical malpractice � Minors � Pediatrics
With the rapid growth in the field of pediatric sleep, health care providers need to beaware of several emerging legal issues that have the potential of impacting their clin-ical practice. Although there is limited case law related to the practice of pediatricsleep medicine, the emerging legal issues may have a significant impact potential inthe future. This article provides an overview of emerging legal areas that have thepotential to impact the practice of pediatric sleep medicine.
The article is divided into 3 parts. First, an overview of the various legal areas thatmay impact health care providers involved with taking care of children with pediatricsleep disorders is described, with particular emphasis on civil liability emerging frommedical malpractice. Second, some of the unique issues that health care providersmust be aware of, including issues related to providing care for minors, is discussed.Third, newer areas that relate to legal prosecution for health care fraud as it may relateto violations of quality of care are introduced, with relevance for the practice ofpediatric sleep medicine.
The information contained in this article is for educational purposes and is not intended toprovide legal advice. You should consult an attorney for individual advice regarding yoursituation.a National Outcomes Center, Quality and Outcomes, Children’s Hospital of Wisconsin, MedicalCollege of Wisconsin, 9000 W. Wisconsin Avenue, MS-950, Milwaukee, WI 53226, USAb Marquette University Law School, Sensenbrenner Hall, Room 116, 1103 West WisconsinAvenue, Milwaukee, WI 53233, USAc Division of Pediatric Pulmonary and Sleep Medicine, Medical College of Wisconsin, Children’sHospital of Wisconsin, 9000 W. Wisconsin Avenue, B620, Milwaukee, WI 53226, USA* Corresponding author. National Outcomes Center, Quality and Outcomes, Children’s Hospitalof Wisconsin, Medical College of Wisconsin, 9000 W. Wisconsin Avenue, MS-950, Milwaukee,WI 53226, USA.E-mail address: [email protected] (R.C. Sachdeva).
Child Adolesc Psychiatric Clin N Am 18 (2009) 1017–1025doi:10.1016/j.chc.2009.06.003 childpsych.theclinics.com1056-4993/09/$ – see front matter ª 2009 Elsevier Inc. All rights reserved.

Sachdeva & D’Andrea1018
OVERVIEWOF LEGAL ISSUES FOR THE PRACTICE OF PEDIATRIC SLEEP MEDICINE
Health care providers may interact with the law in areas that span liability emergingfrom: tort claims, issues related to informed consent, contract law, including allegationsof breach of contract, corporate law, related to mergers and acquisitions of health caresystems; challenges to medical staff privileges, including issues related to impairedphysicians; insurance regulations, with respect to managed care organizations andEmployee Retirement Income Security Act (ERISA); and from the rapidly emergingarea of health care fraud statutes including Stark laws, Anti Kickback statutes, andthe potential application of the False Claims Act for violations of quality of care. A viola-tion of this law could potentially involve a situation whereby an individual has ownershipinterest in a sleep center and refers patients to that sleep laboratory for studies.
CIVIL LIABILITY FOR HEALTH CARE PROVIDERS
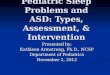
Health care providers will be confronted most frequently with civil liability emerging froma medical malpractice claim. Medical malpractice claims typically relate to negligenceclaims, that is, there is no underlying intent for injury. A negligence claim requires theplaintiff (the injured party) to prove 4 distinct elements: duty, breach, causation, andharm. A typical claim follows some distinct process steps, which are depicted in Fig. 1.
As illustrated in Fig. 1, a plaintiff is limited in the ability to bring forth a lawsuit by thestatute of limitations. The duration of the statute of limitations varies across states andfor various claims. Accordingly, a plaintiff may not be permitted to sue the defendant ifthe lawsuit is brought after the permitted duration within the statute of limitations. Thestatute of limitations has unique implications in the pediatric setting, where this durationmay be much longer than the typical time period in the adult setting. After the claim isfiled, states may require mediation. The discovery phase involves the plaintiff seekinginformation from the defendant, which can include written questions (interrogatories)and depositions. Motions for summary judgment relates to a decision made by a courtbased on the evidence or facts without a trial and is generally used when there is nomaterial dispute of facts and a party is entitled to a decision as a matter of law. Settle-ment opportunities for medical malpractice claims typically span the entire duration ofa lawsuit. Expert testimony is crucial in determining the strength of the case. For the fewcases that do result in a jury trial, there is a unique and important role of jury instructions,which relates to the guidelines provided by a court to the jurors in interpreting law whenmaking their decisions. Even after a jury trial is concluded there may be an opportunityfor appeal. Therefore, both parties typically make a record of their objections during thediscovery and trial phase to ensure the opportunity for an appeal.
As indicated earlier, the plaintiff must prove all 4 elements related to negligence. Ingeneral, there is not much dispute with respect to duty, causation, and harm unlessthere is an underlying frivolous claim. Duty relates to the legal obligation that is createdby a physician (or any health care provider) to patient relationship. Breach relates toa violation of the standard of care. This standard of care is typically established byan expert witness. Causation relates to the notion that the action of the physician orhealth care provider resulted in the alleged injury. Harm relates to the actual injurysustained by the plaintiff. This injury may potentially be physical or emotional.
Most litigation surrounds the issue of breach. The issue, related to breach, emergesfrom the concept of standard of care. The standard of care represents a nationalstandard of care as articulated in the case Hall v. Hillbun.1 In this case, the patientunderwent an exploratory laparotomy that was complicated by a cardiorespiratoryarrest, resulting in death. The issue in this case was the extent of liability incurredby the surgeon for postoperative care, as the surgeon was at home when this incident

Process Steps of a Claim
Perceived or real injury
Plaintiff contacts attorney
Determine statute oflimitations
Attorney conducts initial investigation
Claim filed–served on defendant
State based mediationrequirements
Obtain andreview
Medical Records
Review by Expert
Discovery -Interrogatories and deposition
Motion for summary judgment
Settlement negotiations
Jury trial – expert testimonyand role of Jury Instructions
Post trial motions andappeals
Payments – plaintiff and attorney
Fig.1. Process Steps of a typical medical malpractice claim.
Pediatric Sleep Medicine 1019
occurred. The trial court adopted a locality rule, which meant that the standard of carewould be based on the common practice in the local region. However, on appeal theSupreme Court of Mississippi reversed the decision for the plaintiff and adopted anobjective standard, which is the same everywhere and emerges from an underlyingnational standard. This national standard approach is now generally used in medicalmalpractice litigation. In the practice of pediatric sleep medicine, a hypothetical situ-ation that potentially illustrates this notion involves a case in which a health careprovider does not perform a polysomnography study because of local practiceswhen such a study would be considered the standard of care by national experts toevaluate obstructive sleep apnea within a particular clinical situation.
It may be asked as to who determines the standard of care? Standard of care is deter-mined by a testimony from an expert. Of importance is that an expert does not need tobe board certified and a court could allow expert testimony based on the expert’s

Sachdeva & D’Andrea1020
experience. Also, it is noteworthy that publications such as the Physicians Desk Refer-ence are not in themselves standards of care and would typically require an expert tohelp interpret the underlying information. Furthermore, practice guidelines may providea presumptive evidence of care, which could be rebutted with additional evidence.
What are some of the options that the defendant (the health care provider beingsued) has against allegations of negligence? Applicable theories of defense discussedin greater detail in the text9 include the following.
Practice Guidelines as an Affirmative Defense
The application of this defense varies across the different states in the United States;some may allow the use of practice guidelines as an affirmative defense and othersmay not. Therefore, it is important for health care providers to carefully evaluate thelaws within their individual states of practice.
Theory of Clinical Innovation Defense
The theory for this defense is best illustrated in the case of Brook v. St. John’s HickeyMemorial Hospital.2 The case relates to a 23-month-old child who needed contrast fora urological procedure. The radiologist could not find the vein and injected the contrastin the calf. Unfortunately, the child developed a contracture. In this case, the courtruled that this was not experimentation, but rather innovation, which was supportedby medical journals that had described this procedure and that the defendant hadused this procedure successfully in previous clinical settings.
Theory of Good Samaritan Acts
Most states have adopted legislation to protect individuals who may be called on ina situation whereby they are performing an intervention as a Good Samaritan. Evenif the intervention results in a less than optimal outcome, the individual would be pro-tected from civil liability. This defense is best illustrated in the case McKenna v. Cedarsof Lebanon Hospital.3 In this case, the plaintiff had a tubal ligation. Postoperatively thepatient had a seizure and a respiratory arrest, leading to death. The defendant in thiscase was a chief resident who responded to the code. The underlying issue waswhether the Good Samaritan Act defense applies within a hospital. The court ruledthat the Good Samaritan Act defense did apply in this setting because the defendantwas essentially functioning as a volunteer who did not have a direct duty or contract torender emergency treatment to the patient.
Theory of Contributory Fault of the Patient
The defendant can argue that the patient was at fault, resulting in harm to himself orherself. The underlying issue typically relates to whether the pretreatment healthhabits may have contributed to the extent of the medical malpractice claim. A casethat illustrates this point is Ostrowski v. Azzara.4 In this case the plaintiff was a smoker,obese, and diabetic, and saw a podiatrist for a foot condition. The plaintiff hada surgical complication. The jury found the plaintiff to be 51% negligent, resulting inno recovery to the plaintiff.
It is important to distinguish between various doctrines that inform this area. Thedoctrine of contributory negligence relates to actions before the harm occurs. Incontrast, the doctrine of avoidable consequences relates to activity after the harmhas occurred, and the doctrine of comparative negligence relates to the relativecomparison of the proportion of fault leading to the harm between the plaintiff andthe defendant. As an illustration, a potential hypothetical situation in the practice ofpediatric sleep medicine can relate to a scenario in which a teenager has poor sleep

Pediatric Sleep Medicine 1021
hygiene and despite counseling by the health care provider, continues to maintain thepoor sleep hygiene. In a sleep-deprived state, this teenager gets involved in a motorvehicle accident. In a lawsuit that emerges, a defense of comparative negligencemay be applicable because the teenager’s actions for not following the recommenda-tions were, in part, related to the accident.
Theory of Multiple Defendants
Multiple parties may act together in complex clinical situations, resulting in a singleinjury. In such situations the defendants are considered as joint tortfeasors. Anexample of this situation would be when a physician may fail to diagnose a certaindisease and later another doctor is negligent in treating it. In such a situation, the firstdoctor may be held liable for all foreseeable injuries. Furthermore, if only one party isresponsible for the underlying harm but is unable to prove which party is responsible,the court may apply the concept of burden shifting, which means that the burden is oneach party to prove that they have not caused the harm. As an illustration, a potentialhypothetical situation in the practice of pediatric sleep medicine may involve the situ-ation whereby a patient is seen by a health care provider for a diagnosis that wasincorrectly made previously by another health care provider. If this health care providerdoes not correct the misdiagnosis, it may not be a viable defense that the diagnosiswas missed previously and the new health care provider may be responsible for allthe damages that follow.
MINIMIZING LEGAL RISKS IN THE PRACTICE OF PEDIATRIC SLEEP MEDICINE
What can the health care provider do to minimize risk from medical malpracticeemerging from negligence cases? There are several steps that need to be considered.First, it is important for health care providers involved with taking care of children withpediatric sleep disorders to be aware of national standards surrounding care of chil-dren with sleep disorders and not be limited to standards within a local practice.Second, excellent medical record documentation remains important, including havinglegible and chronologic entries that are complete and timely. Third, communicatingwith families of children in a timely and thorough manner will minimize potential claimsin the future. Fourth, full and timely disclosure of errors is important to further minimizeclaims that may emerge later. Fifth, professionalism with the plaintiff’s attorney isimportant. Although being sued may result in feelings of anger and hostility towardthe plaintiff and plaintiff’s attorney, it is important to remain professional with the otherparty. Finally, it is important to state facts, not consequences, and always tell the truth.
UNIQUE ISSUES RELATED TO THE PRACTICE OF PEDIATRIC SLEEP MEDICINEUnderdiagnosis or Misdiagnosis of Pediatric Sleep Problems
It is estimated that 25% to 40% of all children and adolescents experience sleep prob-lems.5 A survey performed by Owens found that pediatricians rated the impact ofsleep problems on children as important or very important, from 49.7% related to non-intentional injuries to 92.6% related to academic performance.6 This study also foundthat less than one-half of the pediatricians felt confident or very confident in their abilityto screen for sleep problems and in managing pediatric sleep problems.6 Thesestudies highlight the large proportion of children and adolescents who are at risk ofsleep-related problems that may be underdiagnosed or inappropriately managed inthe community setting. These issues open the door for potential legal risks for healthcare providers in the future because pediatric sleep problems in the community maybe underdiagnosed or misdiagnosed, and it will be the responsibility of the health care

Sachdeva & D’Andrea1022
provider evaluating a child for a sleep problem to ensure that the correct diagnosis andmanagement plans are in place. As discussed earlier in the theory of multiple defen-dants, it may not be a defense for the health care provider evaluating a child for a sleepproblem to rely on previous diagnoses made in the community.
Misdiagnosing sleep disorders as primary psychiatric conditions, particularlyregarding parasomnias, poses a unique legal risk.7 Underdiagnosing or misdiagnosingparasomnias in children may result in preventable injury to the child or others, whichcould result in a potential liability for the health care provider. To illustrate thecomplexity of this clinical situation, a hypothetical situation may involve a child whosleepwalks, and walks outdoors and falls into a lake or gets hit by an automobile.The health care provider who has examined the child for the sleep problem may bepotentially liable if there is not adequate documentation of counseling performedwith the family regarding these risks.
Another complex situation may involve a child with underlying psychiatric issueswho also has a sleep problem. Families in this situation may have the perceptionthat if the sleep problems are treated, the psychiatric problems will also resolve.However, although the psychiatric issues may improve if the child is sleeping better,they may not completely resolve by addressing the sleep problems alone. Psychiatricissues are frequently intertwined with the sleep issues. As a hypothetical situation,a health care provider treating a child for a sleep problem may be potentially exposedto liability if the child becomes suicidal. Therefore, it is important to be vigilant andthorough in appropriately diagnosing these conditions and providing the necessarycounseling to families to minimize injuries resulting from such events.
Consent from Minors
Obtaining consent for treating minors can pose some unique challenges for the healthcare provider. Under common law, minors cannot give informed consent for treat-ment.8 State law defines the age for minors. If an individual is determined to be a minorunder state law, a parent or the minor’s court-appointed guardian has the authority togive consent for treatment.8 The health care provider may not be legally protected byobtaining consent from an adult who is not the parent, unless that adult has been ap-pointed as the legal guardian for the minor by a court or has written permission by theparent to give consent.8 In general, divorce does not result in a change in the legal rightof a parent to give consent for treatment of a child.8 However, a court may determineotherwise, and some states have created specific exemptions related to obtainingparental consent.8 Health care providers should evaluate these rules within the statewhere they practice. Besides the exceptions created by state statutes, a minor may betreated in a situation of a medical emergency in the absence of consent from theparents. In the practice of pediatric sleep medicine, there can be unique issues thatmay not have clear legal answers at this point. For example, a hypothetical situationinvolves a parent who believes that it is the child’s responsibility for his or her treat-ment and leaves it to the child to use a continuous positive airway pressure apparatusin an effective manner.
LEGAL ISSUES RELATED TO HEALTH CARE FRAUDAS A RESULT OF QUALITYOF CARE VIOLATIONS
Health care fraud laws can result in criminal liability. These laws include the FalseClaims Act, the Medicare and Medicaid Anti Fraud and Anti Kickback statutes, andStark laws. The False Claims Act relates to fraudulent billing. However, extreme viola-tions in quality of care may be construed as no care being delivered and the

Pediatric Sleep Medicine 1023
application of the False Claims Act if that service was billed for. The Anti Kickbackstatutes aim at targeting situations whereby payments are made to induce patientreferrals. Stark laws aim at targeting situations whereby patients are self-referred.Self-referral includes referral to family members. A discussion of the full implicationsfor such laws is beyond the scope of this article. It must be pointed out that althoughinitially many of these laws were at the federal level, they are being increasinglyexpanded for application at the state level. This section provides an overview of theunique application of health care fraud laws, particularly in the area of allegations orviolations of health care quality.
It is estimated that in 2001, the Federal Government recovered 1.3 million dollarsfrom health care fraud related cases. The Centers for Medicare and Medicaid estimatethat health care spending in the United States will reach 3.4 trillion dollars annually by2013. The Institute of Medicine report from 1999 suggests that 98,000 patients die peryear in hospitals because of medical errors. All of these underlying factors have re-sulted in a greater interest in prosecution of violations of extreme breaches of qualityof care under health care fraud laws. In general, the health care fraud law used in suchsituations relates to the qui tam provisions of the False Claims Act.9 Qui tam hasorigins in common law and comes from the Latin phrase qui tam pro domino regequam pro sic ipso in hoc parte sequitur, which means that a person sues for a matterfor the king and themselves. In practice, the qui tam provisions relate to situationswhereby a relator, or a whistleblower, can file a potential case against the defendantof health care fraud. In such situations, the relator or whistleblower normally canbenefit from a financial standpoint in the recovery but also has specific provisionsagainst retaliation.
Although qui tam lawsuits may emerge from a variety of allegations of healthcare fraud, its application in situations of violation of quality of care is uniqueand distinct. Some of the following cases highlight this point. In the case of UnitedStates ex rel. Aranda v. Cmty. Psychiatric Ctrs. of Oklahoma,10 patients sufferedcomplications in a nursing home setting due to understaffing. The court heldthat there was a liability as a result of violation of quality of care due to the under-staffing. However, in the case of United States ex rel. Mikes v. Strauss,11 the alle-gation was that the quality of spirometry tests done to assess pulmonary functionwas inadequate and therefore, the resulting charges were fraudulent. However, thecourt did not find liability because, although the quality of tests was based onphysician decision making, the tests were indeed performed. In contrast, in thecase of United States v. NHC Health care Corp.,12 another nursing home case,patients suffered pressure sores due to understaffing. The nursing home obtainedglobal daily charges. In this case, the court found liability. Therefore, in summary,there are emerging cases whereby significant understaffing of a health care entityand the related injury to a patient may be viewed under the theory of fraudulentbilling because of a significant violation of quality of care.
It will be important to monitor the application of this theory in the pediatric sleepmedicine setting. The application of qui tam litigation is likely to be particularly relevantin the future for the practice of pediatric sleep medicine in situations that may involvedifferences in quality of tests performed, such as polysomnograms. Given the currentheterogeneity in the practice of pediatric sleep medicine, including differences in staff-ing, business, and operational practices within pediatric sleep centers, there maypotentially be legal issues related to quality of care and billing that emerge in the future.To minimize such risks, health care providers involved in pediatric sleep medicinemust remain abreast of emerging national standards and policies for pediatric sleepcenters, and ensure full compliance and documentation of their practices.

Sachdeva & D’Andrea1024
With the availability of quality and outcomes data related to physicians and healthcare organizations, there is likely to be a greater interest in using these data to estab-lish standard of care.13 However, a unique application in this situation relates to ob-taining informed consent. In the case of Johnson v. Kokemoor,14 a neurosurgeonfailed to share comparative outcomes information related to aneurysmal surgery inhis practice with the Mayo Clinic, which was in the region where the defendant prac-ticed. The Supreme Court of Wisconsin found liability against the surgeon, holding thatit was a material duty by the surgeon, while obtaining informed consent, to haveshared the information related to the comparative outcomes information for the proce-dure. As the field of outcomes research continues to expand in pediatric sleep medi-cine, it will be important to monitor how such outcomes information is potentially usedas part of obtaining informed consent and establishing standards of care in the future.
The interaction between outcomes and law has potential implications for health careproviders involved in pediatric sleep medicine at 2 levels. First, as the outcomes ofnew medications being used to treat pediatric sleep and pediatric psychiatric issuesare identified, it will be important to share these outcomes with families when makingtreatment choices. Second, with the national movement toward health care transpar-ency in quality of care, as the outcomes of hospitals and the pediatric sleep centersare measured, it will be important to share such information with families to facilitatefull informed choice for selecting treatment options for their children.
SUMMARY
Health care providers involved in the care of children with sleep disorders must remainup to date with the laws within the state(s) where they practice. Although civil litigationin the form of medical malpractice will continue to evolve as new standards of care inpediatric sleep are established, given the high rate of underdiagnosis or misdiagnosisof pediatric sleep disorders it remains important to reevaluate and verify diagnoses ofnew children entering the practice. Finally, health care providers practicing pediatricsleep medicine need to recognize that medical malpractice is not the only legal riskto which they are potentially exposed. The scope of criminal laws, which traditionallyincludes Stark laws, Anti Kickback statutes, and False Claims Act, may be furtherexpanded to violations of quality of care, particularly as quality and outcomes informa-tion becomes more available. Such laws have been increasingly applied in a variety ofhealth care settings in the past. Given that pediatric sleep medicine is a relatively newfield, there is limited case law currently available. However, these laws such as theStark laws focusing on self referrals, Anti Kickback statutes focusing on paymentsfor inducing referrals, and the False Claims Act focusing on fraudulent billing includingsituations involving extreme violations in quality of care, have the potential of signifi-cantly impacting the practice of pediatric sleep medicine in the future.
ACKNOWLEDGMENTS
The authors would like to thank Lisa Ciesielczyk, Lara Dynek, and Caroline Hack-stein for their assistance in the preparation of this article.
REFERENCES
1. Hall v. Hillbun, 466 So.2d 856 (Sup. Ct. Miss., 1985).2. Brook v. St. John’s Hickey Memorial Hospital, 269 Ind. 270 (Sup. Ct. Ind., 1978).3. McKenna v. Cedars of Lebanon Hospital, 93 Cal. App.3d 282 (Ct. App., 1979).4. Ostrowski v. Azzara, 111 N.J. 429 (Sup. Ct., 1988).

Pediatric Sleep Medicine 1025
5. Kothare SV, Porneroy SL. Pediatric sleep medicine in 2008: state-of-the-art. CurrOpin Pediatr 2008;20(6):639–40.
6. Owens JA. The practice of pediatric sleep medicine: results of a communitysurvey. Pediatrics 2001;108(3):E51.
7. Stores G. Misdiagnosing sleep disorders as primary psychiatric conditions. AdvPsychiatr Treat 2003;9(1):69–77.
8. Barratt K. A physician’s guide to Wisconsin health law. Madison (WI): StateMedical Society of Wisconsin; 1997. A-1–I-6.
9. Furrow BR, Greaney TL, Johnson SH, et al. Health law: cases, materials and prob-lems, American case-book series. 4th edition. St. Paul (MN): West Group; 2001.
10. United States ex rel. Aranda v. Cmty. Psychiatric Ctrs. of Oklahoma, 945 F. Supp.1485 (W.D. Okla., 1996).
11. United States ex rel. Mikes v. Strauss, 84 F. supp. 2d 427, 431 (S.D.N.Y., 1999).12. United States v. NHC Healthcare Corp., 115 F. Supp. 2d 1149, 1152 (W.D. Mo.,
2000).13. Sachdeva RC. Electronic health care data collection and pay-for-performance:
translating theory into practice. Ann Health Law 2007;16(2):291–311.14. Johnson v. Kokemoor, 199 Wis. 2d 615 (1996).