Emerging Infectious Respiratory Diseases (EIRD): the Role of
the Family Physician OCFP Annual Scientific Assembly Brian
Schwartz, MD, MScCH, CCFP(EM), FCFP Chief, Emergency Preparedness,
Public Health Ontario November 28, 2013
Slide 2
PublicHealthOntario.ca Faculty/Presenter Disclosure Faculty:
Brian Schwartz Program: 51 st Annual Scientific Assembly
Relationships with commercial interests: Not applicable
Slide 3
PublicHealthOntario.ca Disclosure of Commercial Support No
commercial support
Slide 4
PublicHealthOntario.ca Mitigating Potential Bias Not
applicable
Slide 5
PublicHealthOntario.ca Acknowledgements PHO MOHLTC Emergency
Management Branch Dr. Doug Sider Anne Winter Dr. Maureen Cividino
5
Slide 6
PublicHealthOntario.ca Objectives of presentation After this
presentation you should be able to: 1.Describe the global emergence
of infectious respiratory diseases and their relevance to Ontario
practice 2.Identify suspect cases of EIRD and institute appropriate
infection prevention and control 3.Identify and treat local
infectious respiratory diseases (e.g. seasonal influenza) 6
Slide 7
PublicHealthOntario.ca Public Health Ontario information 1.
Better information for better public health decisions and actions
knowledge 2. Generate and accelerate application of knowledge for
better public health decisions and actions Support 3. Support the
Ontario public health system in its daily business and enhance
capacity in emergencies GOALS
Slide 8
PublicHealthOntario.ca 1. PHO monitoring for emerging diseases
Monitoring of global surveillance reports Enhance provincial and
local detection (e.g. awareness, screening, lab testing)
Collaboration and information sharing with national, provincial and
local stakeholders Proactive development of containment/
management/response strategies Risk assessment Monitoring of
seasonal respiratory diseases 8
Slide 9
PublicHealthOntario.ca Breaking news, June 2012 Newspaper
headlines 9
Slide 10
PublicHealthOntario.ca 10 There is nowhere in the world from
which we are remote and no one from whom we are disconnected
Microbial threats to health in the US. IOM 1992
www.publichealthontario.ca
Slide 11
PublicHealthOntario.ca Types of coronaviruses 11
Slide 12
PublicHealthOntario.ca 12
Slide 13
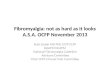
PublicHealthOntario.ca MERS-CoV cases reported WHO, September
20, 2013, by month of illness onset 13 MMWR, September 27, 2013 /
62(38);793-796
Slide 14
PublicHealthOntario.ca Location of MERS-CoV cases by reporting
country, September 25, 2013 14
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20596
Slide 15
PublicHealthOntario.ca Virus origin? Genetically identical
virus fragment from bats Intermediate host? 15 Dromedary camels
found positive for MERS-CoV using serologic testing
Slide 16
PublicHealthOntario.ca Hajj October 13-18, 2013 16
Slide 17
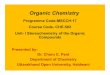
PublicHealthOntario.ca Destinations of Air Travelers Departing
MERS-CoV Source Countries and Origins of Hajj Pilgrims 17
http://currents.plos.org/outbreaks/article/assessing-risk-for-the-international-spread-of-middle-east-
respiratory-syndrome-in-association-with-mass-gatherings-in-saudi-arabia
/
Slide 18
PublicHealthOntario.ca MERS-CoV Mild to severe illness (role of
asymptomatic infection) Limited person to person transmission has
occurred Individuals with underlying illnesses at greater risk of
complications Nosocomial transmission (patients and HCWs) has
occurred, however adherence to recommended IPAC measures unknown
Screening and surveillance are key 18
www.ontario.ca/novelcoronavirus
PublicHealthOntario.ca Background On March 31, 2013 China
notified WHO that a novel influenza A/H7N9 infection was causing
severe illness in humans Human infections with other subgroups of
H7 influenza viruses (H7N2, H7N3, and H7N7) reported previously.
The infections mainly resulted in conjunctivitis and mild upper
respiratory symptoms 20
www.cdc.gov/flu/avianflu/h7n9-images.htm
PublicHealthOntario.ca Avian Influenza A/H7N9 Mild to severe
illness (role of asymptomatic infection) Limited person to person
transmission has occurred Individuals with underlying illnesses at
greater risk of complications Disease reservoirs: ?poultry markets?
Screening and surveillance are key 23
www.ontario.ca/avianinfluenza
Slide 24
PublicHealthOntario.ca 24
www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/mers_decision.pdf
2. Initial Decision Making and Management of Patients Who May Have
an EIRD
PublicHealthOntario.ca Laboratory: how to test?
www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/guidance.aspx
www.health.gov.on.ca/en/pro/programs/emb/avian/workers.aspx 28
MERS-CoVAvian influenza A (H7N9) NP swab/ BAL if indicated EDTA
blood tubeViral throat swab if hospitalized urine Stool if GI
symptoms Acute and convalescent (21 to 28 days later) serology
Slide 29
PublicHealthOntario.ca Principles of Routine Practices (RP)
Based on premise that all patients are potentially infectiousand
the same safe standards of practice should be used routinely to
prevent exposure to blood, body fluids, mucous membranes or
contaminated environment Infection control measures used to prevent
and control transmission of microorganisms from patient to patient,
patient to HCW, HCW to patient and HCW to HCW Perform a risk
assessment before every encounter with the patient or their
environment. Note this will be a dynamic risk assessment as the
patients condition changes 29
Slide 30
PublicHealthOntario.ca Principles of Additional Precautions
(AP) Additional Precautions are used in addition to Routine
Practices for patients known or suspected to be infected or
colonized with certain microorganisms to interrupt transmission AP
include the use of barriers, personal protective equipment (PPE)
and control of the environment In some instances specialized
engineering controls may be required (e.g. referral of a patient
with active tuberculosis or in this case PUI for MERS-CoV or avian
influenza A(H7N9) virus for admission into an airborne infection
isolation room) 30
Slide 31
PublicHealthOntario.ca PPE includes one or more of the
following: gloves, gowns, masks, respirators and eye protection
Clean PPE is applied immediately before providing care, removed and
disposed of immediately after, and hands cleaned Personal
Protective Equipment (PPE) 31
Slide 32
PublicHealthOntario.ca It is important to protect the mucous
membranes of the HCW Eye protection is often forgotten but very
important Eye protection can be goggles, glasses with proper side
coverage or face shield Important to be comfortable; to fit; to
ensure no splash or spray will contact eye Can be disposable or
reusable; ensure proper cleaning procedure that will not
contaminate the worker Facial and Eye Protection 32
Slide 33
PublicHealthOntario.ca N95 respirator must be fit-tested at
least every 2 years as part of a respiratory protection program
Must be seal-checked with each use Must be disposed of after each
use Take great care not to self-contaminate while removing Face
Protection: N95 Respirator 33
Slide 34
PublicHealthOntario.ca Perform hand hygiene as per the JCYH 4
moments of hand hygiene Alcohol-based hand rub (ABHR) at point of
care is preferred Should be 70% concentration of alcohol with
emollients Hand washing with soap and water if hands visibly soiled
Image source: M. Ashcroft Hand Hygiene 34
Slide 35
PublicHealthOntario.ca New England Journal of Medicine Jan 15
2009 Curtis Donskey HCW hand imprint after abd exam After using
ABHR MRSA growth 35
Slide 36
PublicHealthOntario.ca Follow usual Routine Practices Use
Additional Precautions for Droplet/Contact +N95 when history of
symptoms and exposure indicate so Remember proper sequence for
donning and doffing PPE Surgical mask on patient for transport (if
tolerated) Normal cleaning practices for equipment, environment
Normal safe handling practices for linens, sharps Summary of IPAC
36
Slide 37
PublicHealthOntario.ca 3. Dont forget seasonal influenza ILI
with or without travel history Follow PHO influenza bulletins and
information from your local health unit When influenza A and B are
going around (i.e. significant laboratory positivity) consider
early antiviral treatment for patients at risk for complications:
FY Aoki, UD Allen, HG Stiver, GA Evans. The use of antiviral drugs
for influenza: Guidance for practitioners 2012/2013. Can J Infect
Dis Med Microbiol 2012;23(4):e79-e92.
www.ammi.ca/media/48038/14791_aoki_final.pdf.pdf 37
Cardiac/pulmonaryRenal/metabolicMorbid obesity
MalignancyNeurological diseaseAboriginal ImmunocompromiseAge
65Pregnancy
PublicHealthOntario.ca Influenza Treatment 39 Oseltamivir:
adults, children > 40 kg.75 mg. bid Children > 12 months:
23-40 kg.60 mg. bid 15-23 kg.45 mg. bid 7 years)2- 5mg puffs bid FY
Aoki, UD Allen, HG Stiver, GA Evans. The use of antiviral drugs for
influenza: Guidance for practitioners 2012/2013. Can J Infect Dis
Med Microbiol 2012;23(4):e79-e92
www.ammi.ca/media/48038/14791_aoki_final.pdf.pdf
Slide 40
PublicHealthOntario.ca Screen for acute respiratory illness in
your practice and use IPAC routine practices and additional
precautions 2013: include a travel/exposure question if relevant
(e.g. Middle East and China Watch for seasonal influenza and treat
ILI with oseltamivir when activity is high Summary 40
Slide 41
PublicHealthOntario.ca Resources Local public health unit
MOHLTC: www.ontario.ca/novelcoronavirus
www.ontario.ca/avianinfluenza PHOs respiratory virus reports
(seasonal virus circulation) Ontario Respiratory Virus Bulletin
www.publichealthontario.ca/en/ServicesAndTools/SurveillanceServices/Pages
/Ontario-Respiratory-Virus-Bulletin.aspx Laboratory Based
Respiratory Pathogen Report
www.publichealthontario.ca/en/ServicesAndTools/LaboratoryServices/Pages/
PHO-Laboratories-surveillance-updates.aspx 41