Embed Size (px)
Citation preview
Thomas M. File, Jr. MD MSc MACP
Chair, Infectious Disease Division
Summa Health System;
Professor of Internal Medicine,
Master Teacher, Chair ID Section
NEOMED
Emerging Infections and some
Pearls
It is time to
“close the book on infectious diseases.”
Congressional testimony by the Surgeon General of the United States, 1969
Congressional testimony by the
Surgeon General of the United
States, 1969
EMERGING INFECTIONS
New,
Re-emerging, or
Drug-resistant
infections whose incidence in humans
has increased within the past 2
decades or whose incidence threatens
to increase in the near future.
Institute of Medicine Report 1992

From:
Woolhouse M
Microbe 2006
1: 511

NEW INFECTIONS (>100)
Campylobacter Chlamydia pneumoniae Clostridium difficile Community associated Methicillin-resistant S. aureus Hantavirus Helicobacter HIV Hepatitis C Human Herpes virus 6,7,8 Influenza H5N1; Influenza 2009 H1N1 Lyme Severe Acute Respiratory Syndrome (novel
coronavirus) West Nile viru
NEJM Feb 1, 2012; 366: 454-61
NEJM Feb 1, 2012; 366: 454-61

NEJM Feb 1, 2012; 366: 454-61
NEJM Feb 1, 2012; 366: 454-61
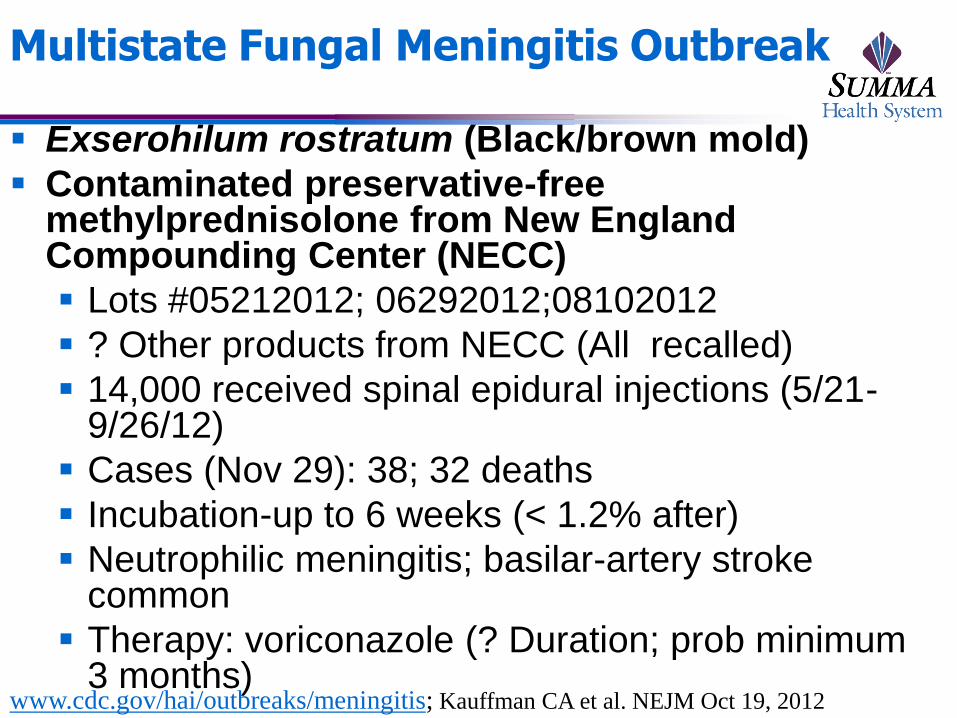
Multistate Fungal Meningitis Outbreak
Exserohilum rostratum (Black/brown mold)
Contaminated preservative-free methylprednisolone from New England Compounding Center (NECC)
Lots #05212012; 06292012;08102012
? Other products from NECC (All recalled)
14,000 received spinal epidural injections (5/21-9/26/12)
Cases (Nov 29): 38; 32 deaths
Incubation-up to 6 weeks (< 1.2% after)
Neutrophilic meningitis; basilar-artery stroke common
Therapy: voriconazole (? Duration; prob minimum 3 months)
www.cdc.gov/hai/outbreaks/meningitis; Kauffman CA et al. NEJM Oct 19, 2012
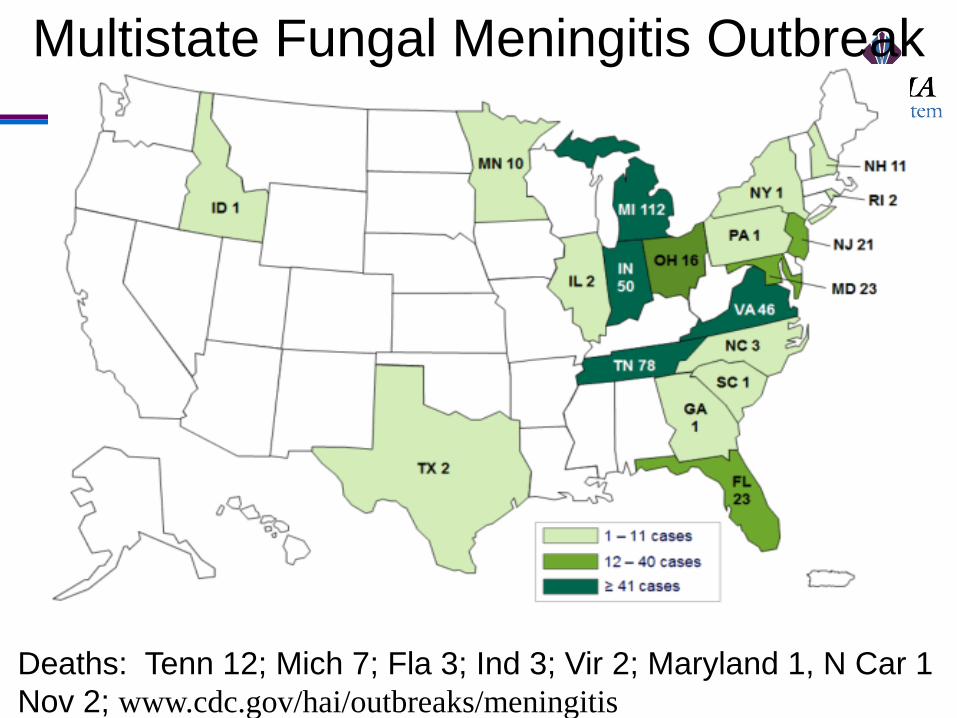
Deaths: Tenn 12; Mich 7; Fla 3; Ind 3; Vir 2; Maryland 1, N Car 1
Nov 2; www.cdc.gov/hai/outbreaks/meningitis
Multistate Fungal Meningitis Outbreak

Date of download:
10/31/2012
Copyright © The American College of Physicians.
All rights reserved.
From: Fatal Exserohilum Meningitis and Central Nervous System Vasculitis after
Cervical Epidural Methylprednisolone Injection
Ann Intern Med.2012;():.doi:10.7326/0003-4819-158-1-
201212040-00557
•51 y/o female presented to ED 9/7 with neck
pain, new occipital HA
•Cervical epidural steroid injection 8/31
•Next day: diploplia, vertigo, nausea, ataxia
•MRI –’normal’
•Day 3: slurred speech, hemiparesis
•MRI-Abn
•LP-Opening press 34, Glucose 36, Protein
153, WBC-850 (84% PMNs)
•Rx: Mulitple antimicrobials/steroids
•Day 7: studies neg for EBV, CMV, WNV,
Crypto, Histo, Bacteria
•Day 9: worse, absent pupillary reflex
•ampho B added
•Day 10: Death
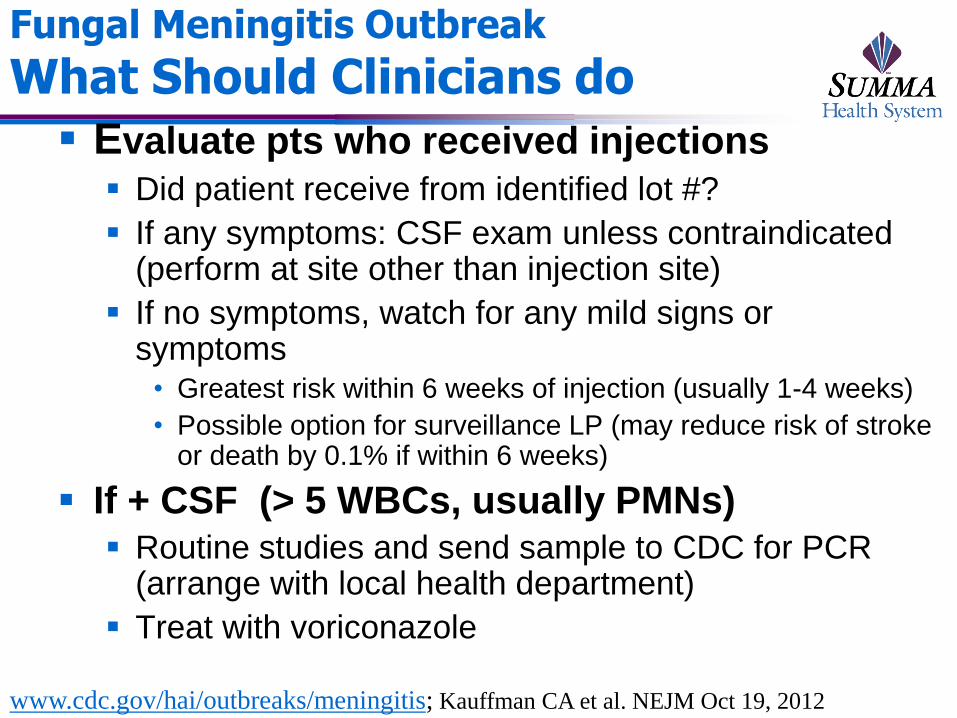
Fungal Meningitis Outbreak
What Should Clinicians do
Evaluate pts who received injections
Did patient receive from identified lot #?
If any symptoms: CSF exam unless contraindicated (perform at site other than injection site)
If no symptoms, watch for any mild signs or symptoms
• Greatest risk within 6 weeks of injection (usually 1-4 weeks)
• Possible option for surveillance LP (may reduce risk of stroke or death by 0.1% if within 6 weeks)
If + CSF (> 5 WBCs, usually PMNs) Routine studies and send sample to CDC for PCR
(arrange with local health department)
Treat with voriconazole
www.cdc.gov/hai/outbreaks/meningitis; Kauffman CA et al. NEJM Oct 19, 2012

SEVERE ACUTE RESPIRATORY
SYNDROME (SARS) Started in Guangdong Province China(11/02); Spread
worldwide; profound impact on travel
Spread by close contact (air droplet)
Highest mortality in elderly and debilitated
Epidemic terminated July 03 No significant numbers of asymptomatic infection
No transmission prior to clinical illness
“We don’t know if we’re going to see anther SARS patient or
not…But I think we’re living in the age of the new normal of
emerging health threats and this preparedness for SARS is
going to pay off sooner or later, because if it’s not SARS, it
will be something else, and we’ll be ready for it”
J. Gerberding (CDC, Sept, 26, 2003)
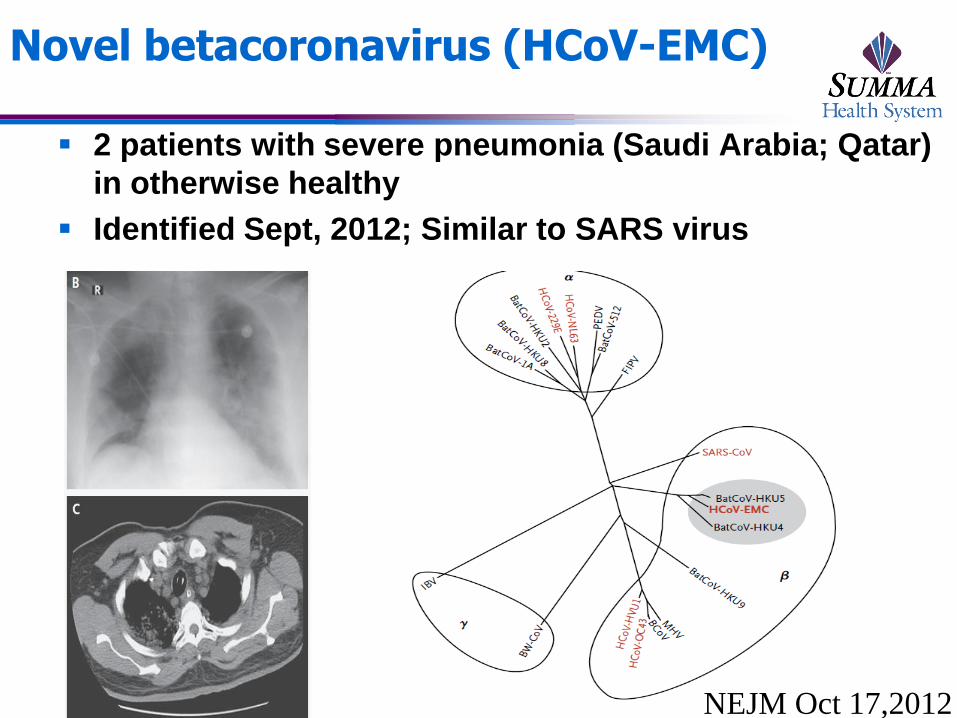
Novel betacoronavirus (HCoV-EMC)
2 patients with severe pneumonia (Saudi Arabia; Qatar)
in otherwise healthy
Identified Sept, 2012; Similar to SARS virus
NEJM Oct 17,2012
AVIAN INFLUENZA
Fall 2003-new outbreak of respiratory illness
Young affected; high mortality
Stimulated worldwide Pandemic Preparedness Plans
Avian Influenza (H5N1) 2003-2012
SE Asia; China; Indonesia;Azerbaijan; Turkey; Iraq; Egypt, Nigeria, + others
Primarily contracted from poultry • Numerous countries with poultry infection
• (Asia, Africa, Europe)
• NONE in Western Hemisphere
NEW OUTBREAK: Influenza
A(H1N1) MMRW Report, April 2009
MMWR, April 24, 2009 Swine Influenza A in two children in Southern
California
No exposure to pigs
MMWR, April 28, 2009 / 58(Dispatch);1-3 47 patients reported to CDC with known ages (out of
64) the median age was 16 years (range: 3-81 years)
38 (81%) were aged <18 years
Of 14 patients with known travel histories • 3 had traveled to Mexico
• 40 of 47 patients (85%) had not been linked to travel or to another confirmed case
Source: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm58d0428a2.htm
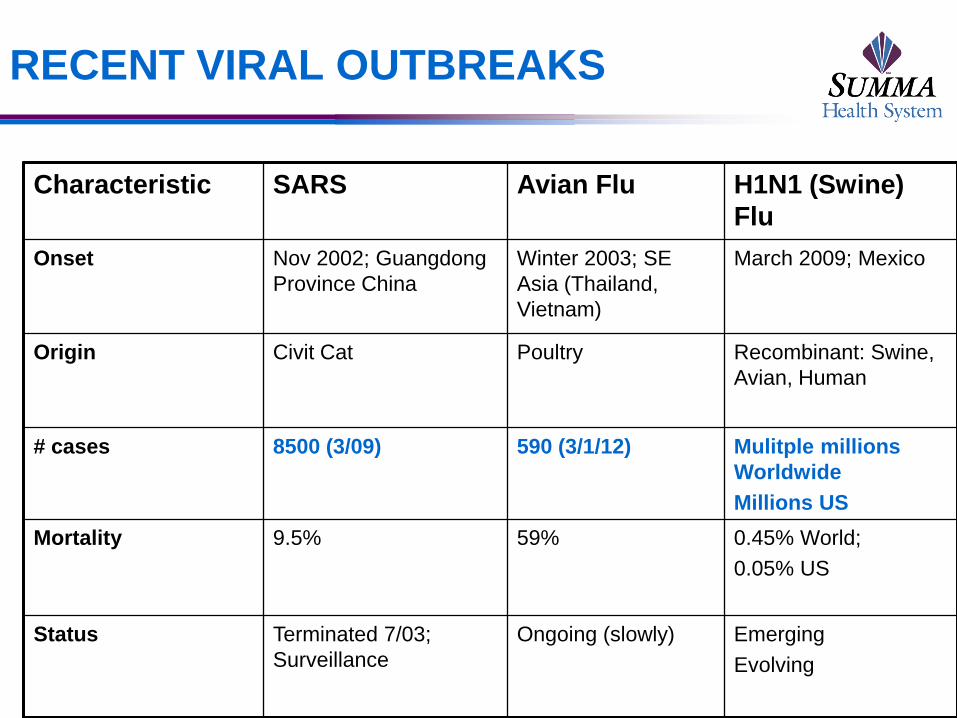
RECENT VIRAL OUTBREAKS
Characteristic SARS Avian Flu H1N1 (Swine)
Flu
Onset Nov 2002; Guangdong
Province China
Winter 2003; SE
Asia (Thailand,
Vietnam)
March 2009; Mexico
Origin Civit Cat Poultry Recombinant: Swine,
Avian, Human
# cases 8500 (3/09) 590 (3/1/12) Mulitple millions
Worldwide
Millions US
Mortality 9.5% 59% 0.45% World;
0.05% US
Status Terminated 7/03;
Surveillance
Ongoing (slowly) Emerging
Evolving
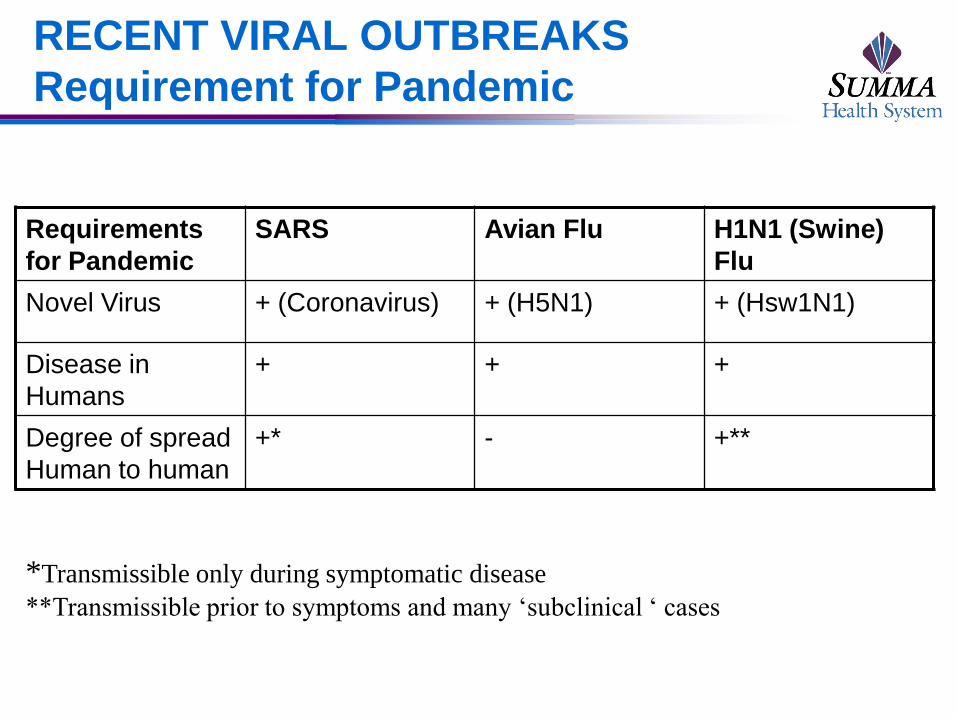
RECENT VIRAL OUTBREAKS
Requirement for Pandemic
Requirements
for Pandemic
SARS Avian Flu H1N1 (Swine)
Flu
Novel Virus + (Coronavirus) + (H5N1) + (Hsw1N1)
Disease in
Humans
+ + +
Degree of spread
Human to human
+* - +**
*Transmissible only during symptomatic disease
**Transmissible prior to symptoms and many ‘subclinical ‘ cases

2009/H1N1 Influenza
Hallmark of influenza virus is ability to undergo constant change
Many different animals get infected, but the virus usually is confined to one species
Flu virus may jump to other species
H1N1 Swine Influenza A is novel virus; contains genetic sequences from: North American swine
North American avian
North American human and
Eurasian swine
2009/H1N1 Influenza-Epidemiology I New Pandemic
Most cases mild but severe cases reported
(often in younger age)
• Highest rate of infection in < 24 year olds
• US mortality 1/2000
– Majority < 50 years of age
– Risks: Asthma, Obesity, Pregnancy, Chronic disease
• Higher rate of GI symptoms than seasonal flu
(virus shed in stool)
• 2nd attack rate (20-30%) higher than seasonal flu
(10-20%)
2009/H1N1 Influenza-Epidemiology II Those > 60 years less susceptible
–Some seroprotection from exposure to H1N1
prior to 1957
–No outbreaks in LTCFs
Severe Infection
• FLAARDS (Flu A Associated ARDS)
• Viral pneumonia
• 2nd Bacterial infection variable
–4-50% in serious/mortality cases--S.
pneumoniae; S. aureus (MRSA), S. pyogenes
2009 H1N1 Mortality
“The pandemic’s impact is better
gauged by the number of life-years lost
because of the younger age of victims
compared with seasonal flu. If you look
at years of personal life lost, it’s much
higher, and that’s the point we have to
get across. A death in an otherwise
healthy 24-year-old, to me, is a major
defeat for society.”
Michael Osterholm, director of the University of Minnesota’s Center for Infectious Disease Research
and Policy in Minneapolis
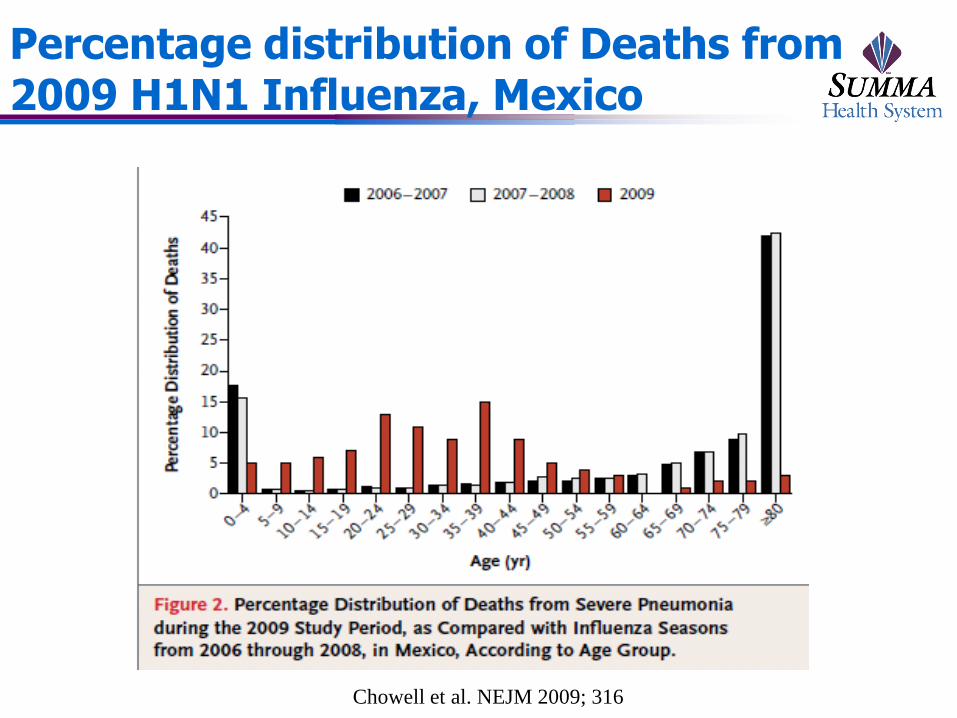
Percentage distribution of Deaths from 2009 H1N1 Influenza, Mexico
Chowell et al. NEJM 2009; 316

Detection of Influenza using Rapid Influenza Diagnostic Tests Laboratory diagnostic tests
Direct antigen detection tests
virus isolation in cell culture
PCR
Rapid tests Rapid influenza diagnostic tests (RIDTs)
• Commercially available; can provide results < 30 minutes
• Cannot differentiate influenza A subtypes
• The sensitivity ranges between 10-70%; a negative test does not exclude influenza infection
PCR Highly sensitive, but not readily available at present or very expensive from outside labs

Susceptibility of Influenza strains to Antiviral agents
Amantadine Rimantadine Oseltamivir Zanamivir
Influenza B 0 0 + +
A/H3N2 0 0 + +
A/seasonalH1N1
+ + 0 +
A/2009H1N1
0 0 + +
Infectious Disease after a Disaster
Skin
MRSA, water borne bacteria (Vibrio spp.; Aeromonas,
Plesiomonas), Mold, insect infestations, trench foot
Diarrhea
E. coli, Cryptosporidiosis, Salmonella, Shigellosis, Norvirus,
Giardiasis
Respiratory
Legionnella,
Systemic
Hepatitis, Leptospirosis, tetanus
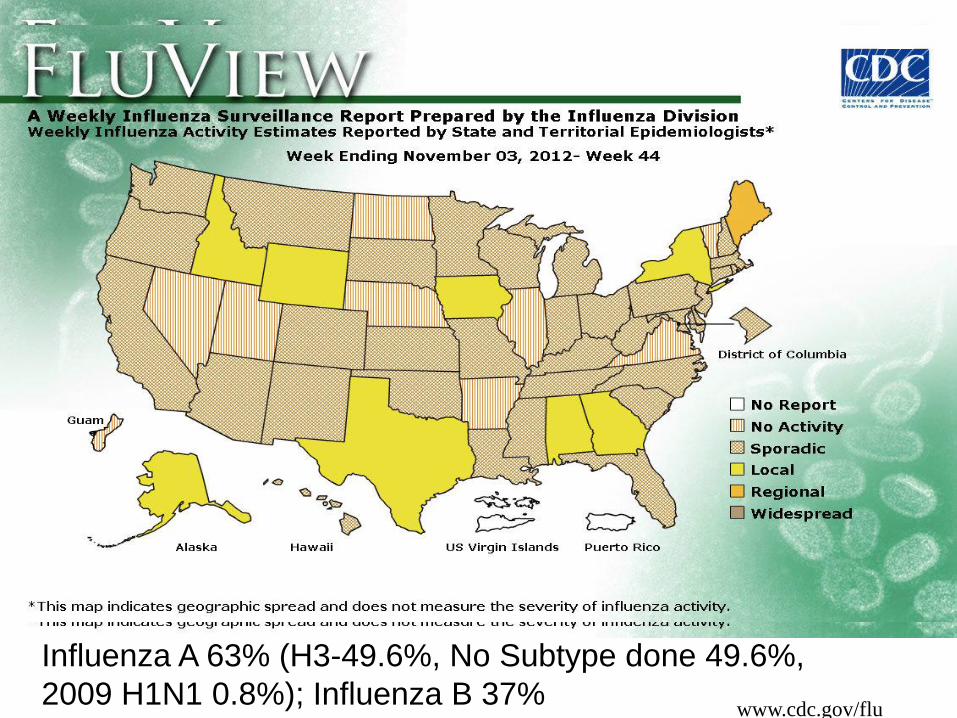
www.cdc.gov/flu
Influenza A 63% (H3-49.6%, No Subtype done 49.6%,
2009 H1N1 0.8%); Influenza B 37%
variant ‘Swine Flu’ virus
Sep 6, 2011 (CIDRAP News) – Two more children in
Pennsylvania were infected with a novel swine
influenza A/H3N2 virus that includes a gene from the
2009 pandemic H1N1 virus.
Nov 28, 2011 (CDC)-Total of 18 cases over past 2
years; associated with mild illness. “Not as bad as the
H1N1 2009 strain
Aug, 2012: CDC confirms new cases of influenza
A/H3N2 variant virus
Twelve new cases of influenza A/H3N2 variant virus were identified
in Hawaii, Indiana and Ohio in the past week, making 29 total cases
since the virus was first detected in humans in July 2011

Why test for Hepatitis C
Hepatitis C: Major public health problem; leading cause
of liver disease and liver CA
4.1 million infected in US (80% viremic)
Mortality (2nd liver failure or CA) expected to increase
Detection and treatment
Reduce illness, death
Reduce transmission
(more deaths than 2nd HIV)
West Nile Fever

West Nile Virus: A newly
emergent epidemic disease
Mosquito borne virus of genus Flavivirus,
closely related to Japanese encephalitis
complex (e.g. St Louis Encephalitis)
WN-wide distribution globally; 1st seen in US in
1999 in NY
Primary reservoir host is birds (esp. crows, blue
jays
Human Infection
Spread by mosquitoes
Rarely by transfusion, transplantation, breast feeding

West Nile Virus activity US, Sept 18, 2012
Total cases (Nov 6, 2012): 2559; 228 deaths
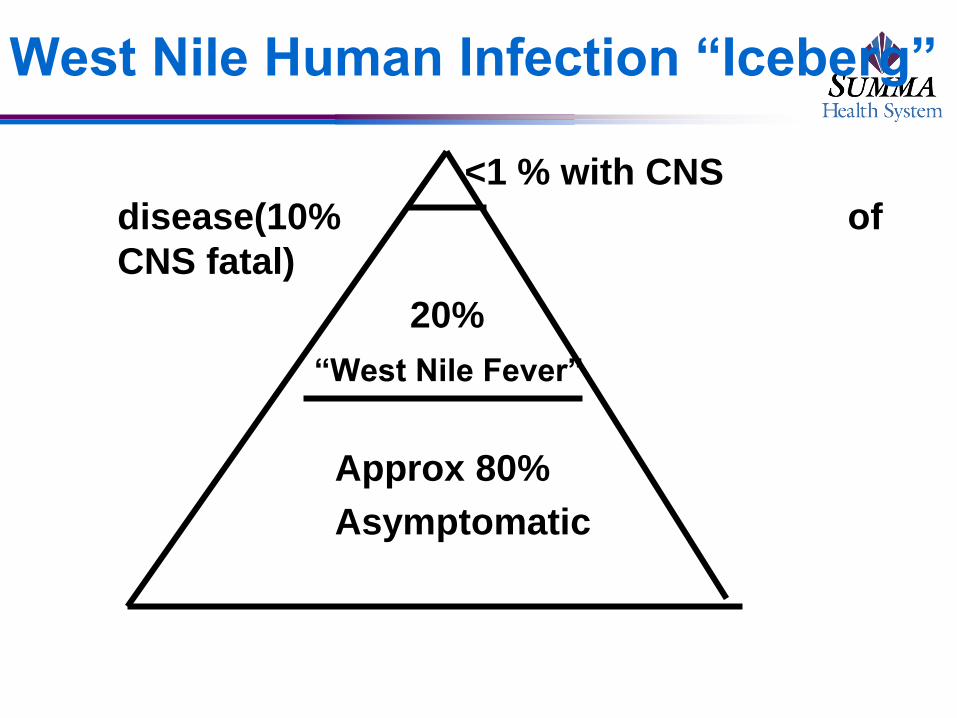
West Nile Human Infection “Iceberg”
<1 % with CNS
disease(10% of
CNS fatal)
20%
“West Nile Fever”
Approx 80%
Asymptomatic
West Nile Virus: therapy/prevention
Supportive
Antiviral agents
Ribavirn, Interferon
Effective in vitro (Anderson and Rahal.
Emerg Infect Dis 2002; 8: 107);
No controlled patient studies
IVIG
Prevention
Mosquito avoidance
DEET (>20%)
Blood supply screening
Vaccine


Emerging and retreating Mosquito- borne Infections: Dengue
Everywhere (most prevalent mosquito-borne disease)
US
Travels, (22 million to risk areas/ year; Most common
cause of fever post travel; Most cases of suspected
malaria)
Mexican border; Hawaii; Key West
Clinical
Incubation: 4-7 days
Dengue Fever: fever, HA, myalgia, arthralgia, some rash
Hemorrhagic fever: Purpura, bleeding, renal
Lab: thrombocytopenia; LFT abnormality

Mosquito- borne Infections: Dengue (H. Margolis. CDC)
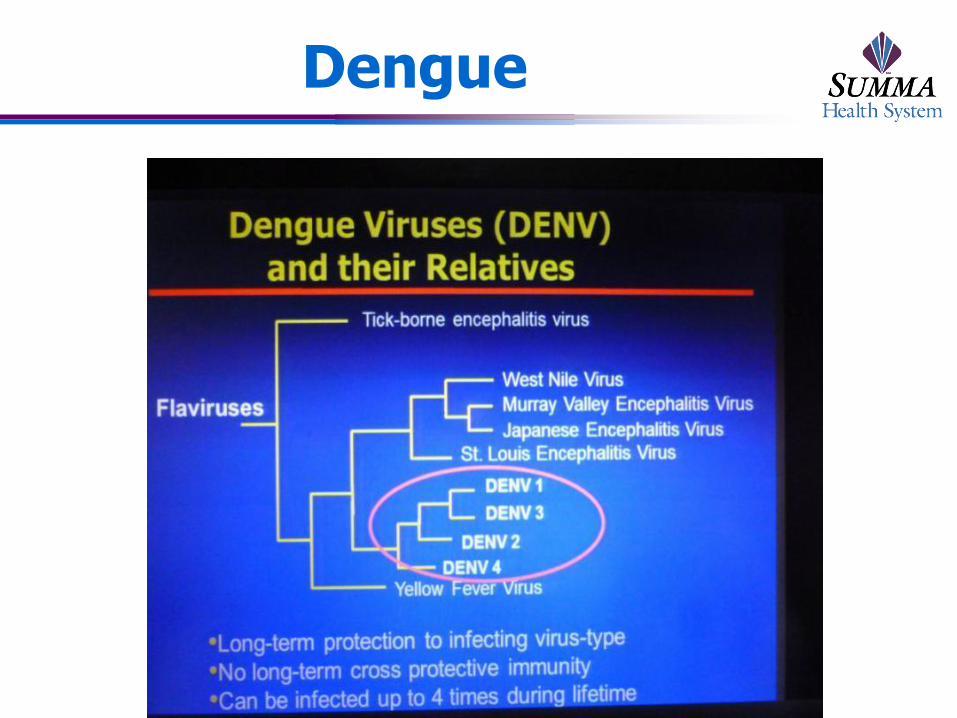
Dengue

Venectomy scar
56 y/o with recurrent cellulitis of leg


Psoriasis
Recurrent Cellulitis of lower extremity in
patients with prior Heart Surgery
Almost always due to hemolytic Streptococcus sp. Usually NOT Grp A Strep
Responsive to most antimicrobials
Associated with disruption of venous and/or lymph drainage Can occur after injury
Can be seen in upper extremeties (e.g., after breast surgery)
Look for associated tinea pedis or other chronic skin condition Treat with antifungal
Use antibacterial soaps
The 3 most common skin and soft tissue infections in
residents of LTCFs are CELLULITIS, INFECTED
PRESSURE SORES and which of the following?
A. B. C. D. E.
20% 20% 20%20%20%
:10
A. Scabies
B. Herpes zoster
C. Herpes simplex
D. Tinea pedis
E. Conjunctivitis
Skin and Soft Tissue Infection
3rd most common infection in LTCF
1-9% or prevalence of 1-2/1000 patient days
Typically results from breaks in skin or mucosa as a consequence of trauma, maceration,pressure, or devices
Most common
Cellulitis
Infected pressure ulcer
scabies
High K. et al. Clin Infect dis. 2009; 48: 149-71; can access via www.idsociety.org
Scabies
Presentation may be atypical
Burrows, inflammatory changes in intertrigenous areas,
pruritis may be absent
May only present with hyperkeratosis, papules, or
vesicles
Often presents by occurrence of > 1 unexplained rash in
residents
Diagnosis: skin scraped with scalpel and examined
under oil immersion (low power)
High K. et al. Clin Infect dis. 2009; 48: 149-71; can access via www.idsociety.org

Scabies
Diagnosis: Scrapping
Treatment
5% permethrin cream (Elimite)
Oral ivermectin (200 mg X 1)

Bed bugs bite U.S.--worst outbreak since WWII
•Bed bugs, Cimex lectularius , feed solely on the blood of animals, can go > 500 days between meals. Adult bugs 1/4 inch long and reddish brown, with oval, flattened bodies. Immatures (nymphs) are smaller and somewhat lighter in color. Do not fly, can move quickly over floors, walls, other surfaces.
52
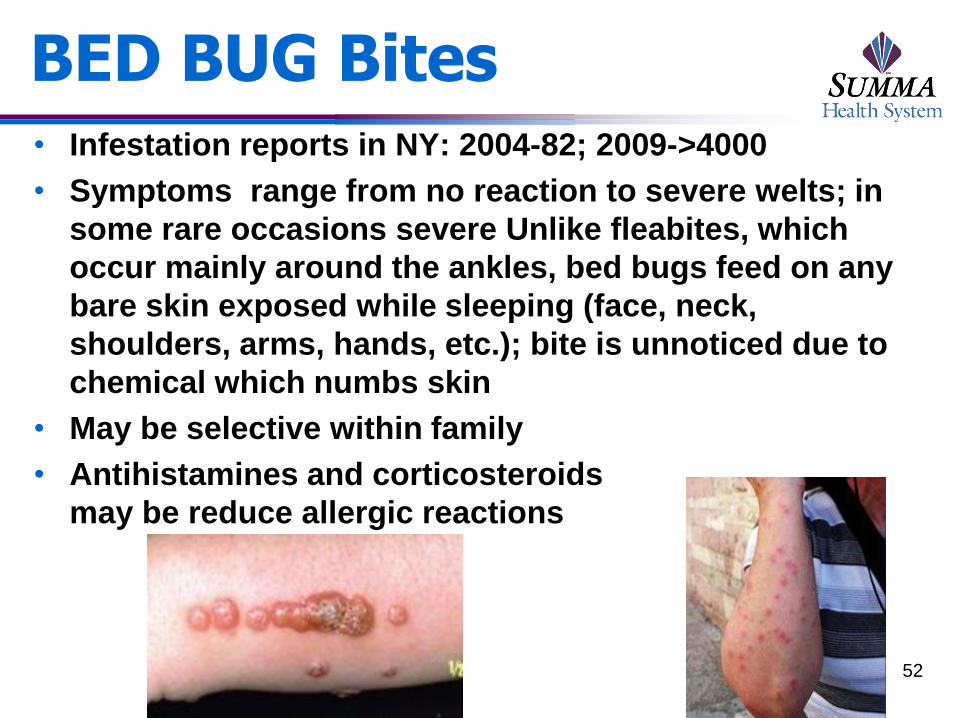
BED BUG Bites • Infestation reports in NY: 2004-82; 2009->4000
• Symptoms range from no reaction to severe welts; in
some rare occasions severe Unlike fleabites, which
occur mainly around the ankles, bed bugs feed on any
bare skin exposed while sleeping (face, neck,
shoulders, arms, hands, etc.); bite is unnoticed due to
chemical which numbs skin
• May be selective within family
• Antihistamines and corticosteroids
may be reduce allergic reactions
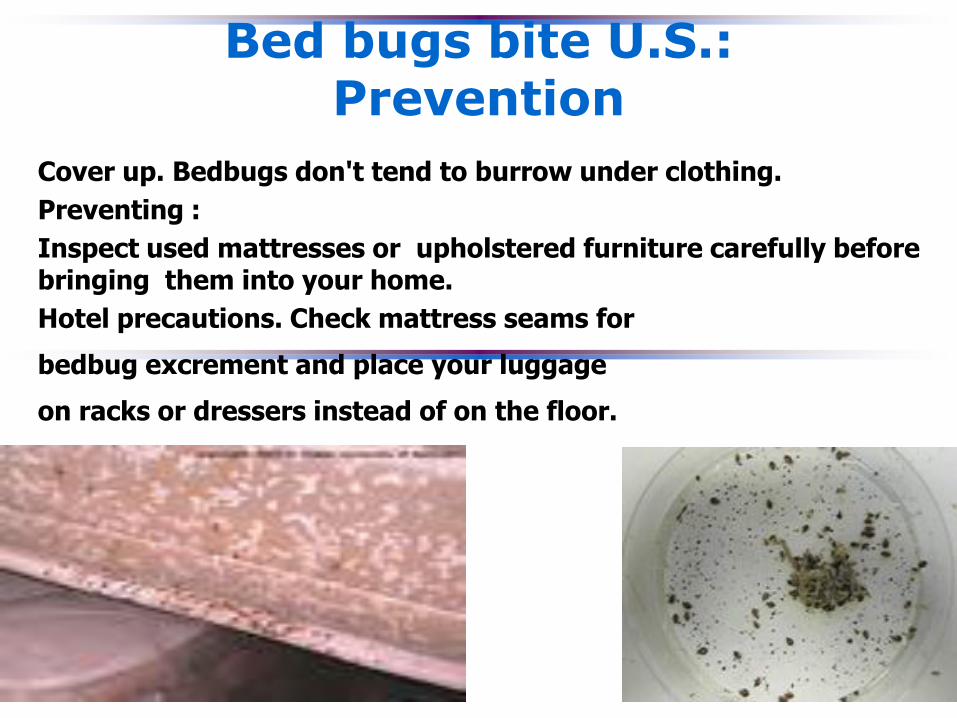
Bed bugs bite U.S.: Prevention
Cover up. Bedbugs don't tend to burrow under clothing.
Preventing :
Inspect used mattresses or upholstered furniture carefully before bringing them into your home.
Hotel precautions. Check mattress seams for
bedbug excrement and place your luggage
on racks or dressers instead of on the floor.
Intra Abdominal Infections:
IDSA Guidelines (IDSA 2010)
62 y/o male with increasing Abd Pain and
Fever
PE: Temp 38.70 C (1.1.70F); Pulse 110; BP
110/60; RR-22; Abd-tender and lower abd
guarding, Bowel sounds
Lab: WBC 19,800
Abd CT:
Source Control for Infections
Patients with diffuse peritonitis should undergo an
emergency operative procedure as soon as is
possible, even if ongoing measures to restore
physiologic stability need to be continued in the
operating room (B-II).
For hemodynamically stable patients without evidence
of acute organ failure, an urgent approach should be
taken. Intervention may be delayed for a longer time, if
appropriate antimicrobial therapy is given and if
careful clinical monitoring is provided. (C-III).
Where feasible, percutaneous drainage of abscesses
and other well-localized fluid collections is preferable
to operative drainage (B-II).
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press

Empiric Therapy
Antibiotics used for empiric treatment of
community-acquired intra-abdominal
infections should be active against enteric
gram-negative aerobic and facultative bacilli
and enteric gram-positive streptococci (A-I)
Coverage for obligate anaerobic bacilli should
be provided for distal small bowel,
appendiceal and colon-derived infections and
for more proximal gastrointestinal perforations
in the presence of obstruction (A-I)
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press

Facultative and Aerobic
Gram-Negatives
Escherichia coli
Klebsiella spp
Pseudomonas
aeruginosa
Proteus spp
Enterobacter spp
Others
71.3%
14.3%
14.1%
5.2%
5.1%
12.3%
Gram-Positive Organisms
Streptococcus spp
Enterococcus faecalis
Enterococcus faecium
Enterococcus spp
Staphylococcus aureus
38.0%
11.6%
3.4%
7.8%
3.5%
Anaerobic Organisms
Bacteroides fragilis
Other Bacteroides
Clostridium spp
Prevotella spp
Peptostreptococcus spp
Fusobacterium spp
Eubacterium spp
Others
34.5%
71.0%
29.2%
12.0%
16.7%
8.6%
16.5%
19.4%
Solomkin JS, Yellin AE, Rotstein OD et al. Ann Surg 2003; 237(2):235-245. Solomkin JS, Wilson SE, Christou NV et al. Ann Surg 2001; 233(1):79-87. Solomkin JS, Reinhart HH, Dellinger EP et al. Ann Surg 1996; 223(3):303-315.
COMMON PATHOGENS IN COMMUNITY-
ACQUIRED INTRA-ABDOMINAL INFECTIONS
Empiric Therapy
Empiric coverage of Enterococcus is not necessary in
patients with community acquired intra-abdominal
infections (A-I)
Empiric therapy for Candida is not recommended for
adult patients with community-acquired intra-abdominal
infections (C-III)
The use of agents listed as appropriate for higher
severity community-acquired infections and healthcare-
associated infections is not recommended for patients
with mild-to-moderate community-acquired infections
since such regimens may carry a greater risk of toxicity
and facilitate acquisition of more resistant organisms (B-
II)
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press
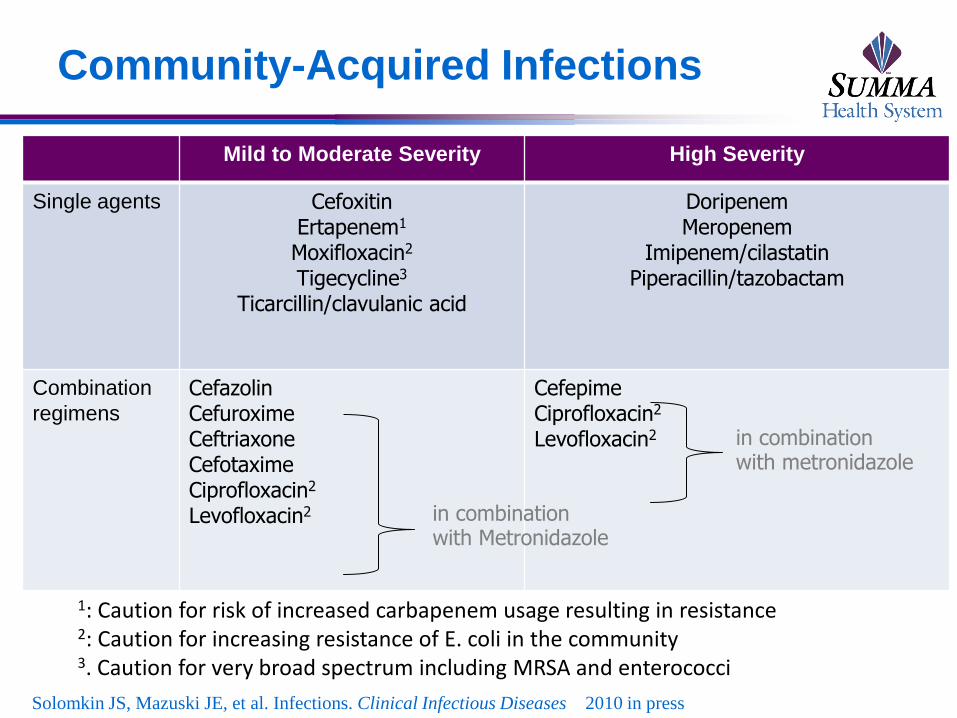
Community-Acquired Infections
Mild to Moderate Severity High Severity
Single agents Cefoxitin Ertapenem1
Moxifloxacin2
Tigecycline3
Ticarcillin/clavulanic acid
Doripenem Meropenem
Imipenem/cilastatin Piperacillin/tazobactam
Combination
regimens
Cefazolin Cefuroxime Ceftriaxone Cefotaxime Ciprofloxacin2
Levofloxacin2
Cefepime Ciprofloxacin2
Levofloxacin2 in combination with metronidazole
1: Caution for risk of increased carbapenem usage resulting in resistance 2: Caution for increasing resistance of E. coli in the community 3. Caution for very broad spectrum including MRSA and enterococci
in combination with Metronidazole
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press
Empiric Therapy
Ampicillin/sulbactam is not recommended for use
because of high resistance rates of community-
acquired E. coli to this agent (B-II)
Cefotetan and clindamycin are not recommended
for use because of increasing resistance of the
Bacteroides fragilis group to these agents (B-II)
Because of the availability of less toxic agents
demonstrated to be of at least equal efficacy,
aminoglycosides are not recommended for routine
use in community-acquired intra-abdominal
infection (A-I)
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press
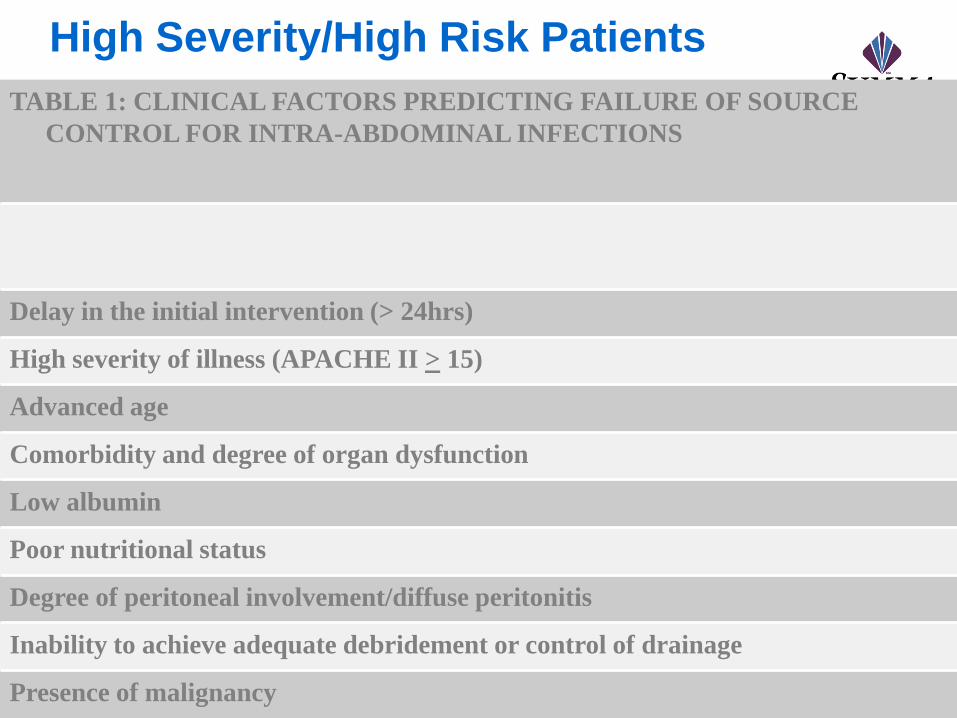
High Severity/High Risk Patients
TABLE 1: CLINICAL FACTORS PREDICTING FAILURE OF SOURCE
CONTROL FOR INTRA-ABDOMINAL INFECTIONS
Delay in the initial intervention (> 24hrs)
High severity of illness (APACHE II > 15)
Advanced age
Comorbidity and degree of organ dysfunction
Low albumin
Poor nutritional status
Degree of peritoneal involvement/diffuse peritonitis
Inability to achieve adequate debridement or control of drainage
Presence of malignancy
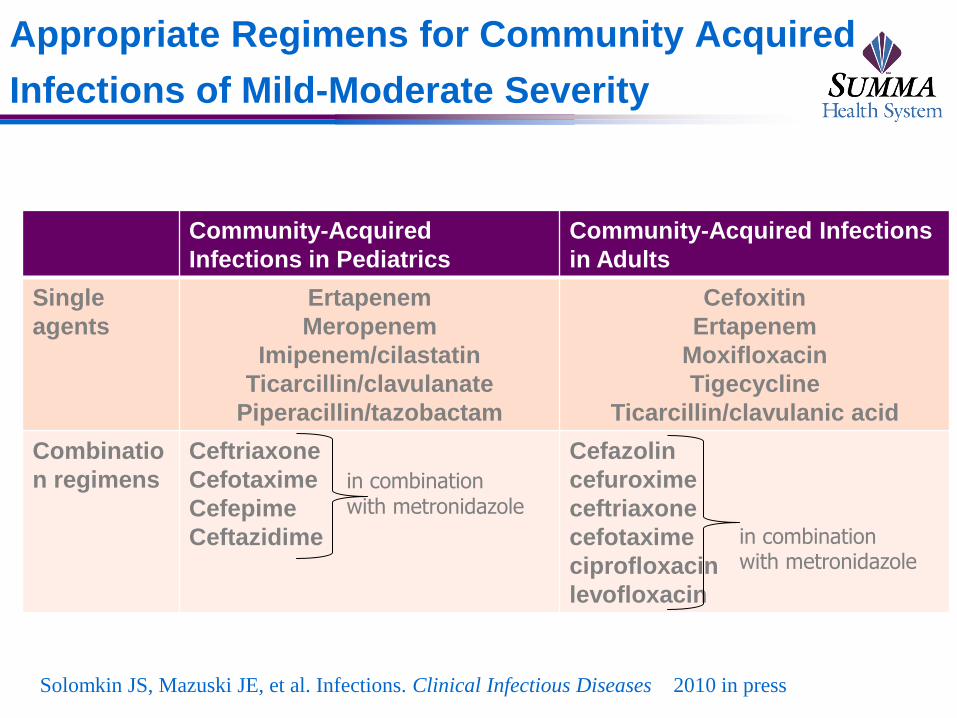
Appropriate Regimens for Community Acquired
Infections of Mild-Moderate Severity
Community-Acquired
Infections in Pediatrics
Community-Acquired Infections
in Adults
Single
agents
Ertapenem
Meropenem
Imipenem/cilastatin
Ticarcillin/clavulanate
Piperacillin/tazobactam
Cefoxitin
Ertapenem
Moxifloxacin
Tigecycline
Ticarcillin/clavulanic acid
Combinatio
n regimens
Ceftriaxone
Cefotaxime
Cefepime
Ceftazidime
Cefazolin
cefuroxime
ceftriaxone
cefotaxime
ciprofloxacin
levofloxacin
in combination with metronidazole
in combination with metronidazole
Solomkin JS, Mazuski JE, et al. Infections. Clinical Infectious Diseases 2010 in press
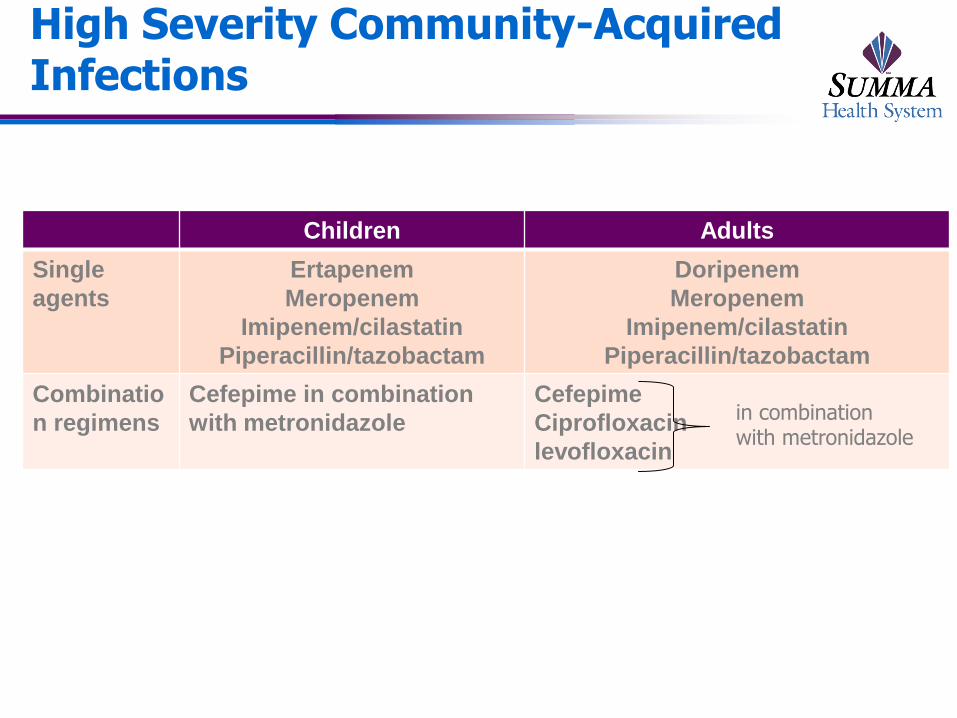
High Severity Community-Acquired Infections
Children Adults
Single
agents
Ertapenem
Meropenem
Imipenem/cilastatin
Piperacillin/tazobactam
Doripenem
Meropenem
Imipenem/cilastatin
Piperacillin/tazobactam
Combinatio
n regimens
Cefepime in combination
with metronidazole
Cefepime
Ciprofloxacin
levofloxacin
in combination with metronidazole
Duration of Therapy for Patients with
Complicated Intra-abdominal Infection
Recommendation
Antimicrobial therapy of established infections should be limited
to no more than four to seven days unless it is difficult to
achieve adequate source control. Longer durations of therapy
have not been associated with improved outcome (B-III).
Evidence Summary
Resolution of clinical signs should be used to judge the
termination point for therapy…risk of subsequent treatment
failure is quite low in patients who have no clinical evidence of
infection at the time of cessation of antimicrobial therapy.
This usually implies that the patients are afebrile, have
normal WBC, and are tolerating an oral diet.
Guidelines by the Surgical Infection Society and the
Infectious Diseases Society of America1
1. Solomkin et al. Clin Infect Dis. 2010;50:133-164. 2. Hedrick TL et al. Surg Infect. 2006;7:419–432.
3. Lennard ES et al. Ann Surg. 1982; 195:19–24.

Painless chronic skin ulcer enlisted person
coming home from Iraq
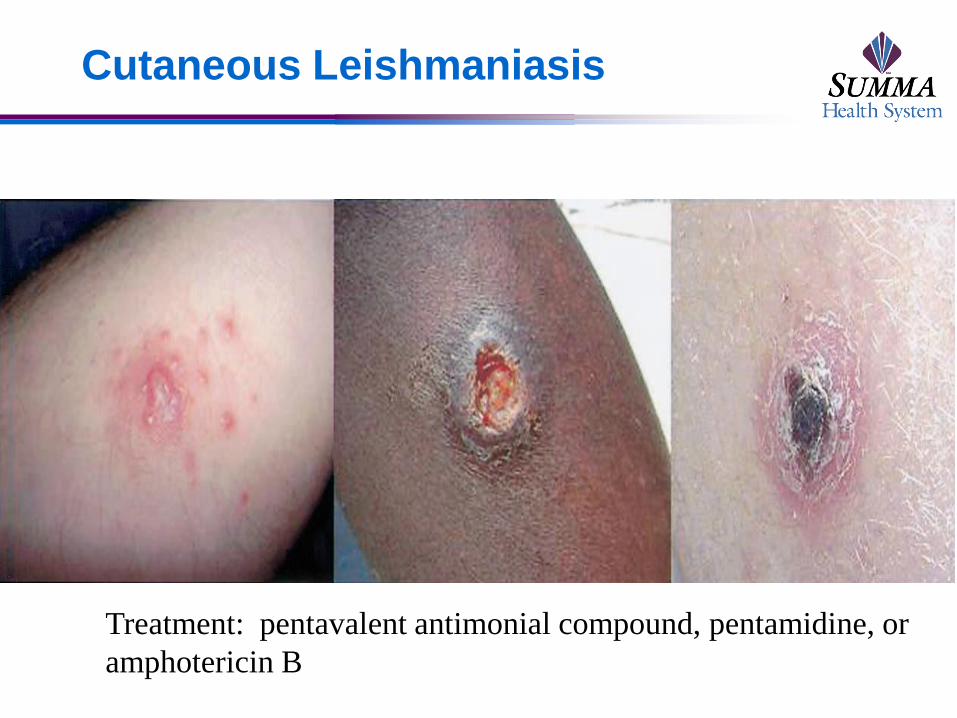
Cutaneous Leishmaniasis
Treatment: pentavalent antimonial compound, pentamidine, or
amphotericin B

Case: Patient presents to ER with
fever, cough, chest pain
The diagnosis is most likely by?
a. Sputum culture
b. Blood culture
c. Sputum PCR
d. IgM ELISA
e. Urinary Antigen

EMERGING INFECTIONS
“Humanity has but three great
enemies: fever, famine and war; of
three by far the greatest, by far the
most terrible, is fever.”
Sir William Osler
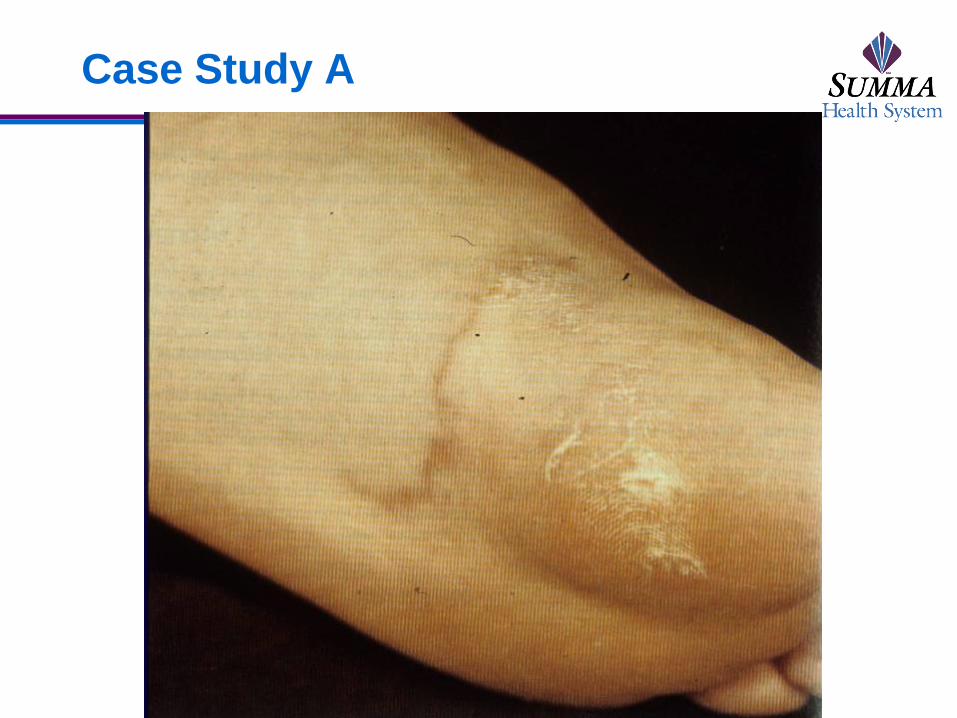
Case Study A
A 42 y.o. man presents to your office 48 hours after returning from his CME trip Fla. Two days previously he noted the onset of a severely pruritic sensation on the medial distal ventral left foot that has progressively worsened during the last 24 hours.
The patient is afebrile but a linear rash appeared about 12 hours after the onset of symptoms and has significantly lengthened in the patient’s visual self-evaluation of the lesion by the time he sees you in the office. See Figure # 1.
Case Study A
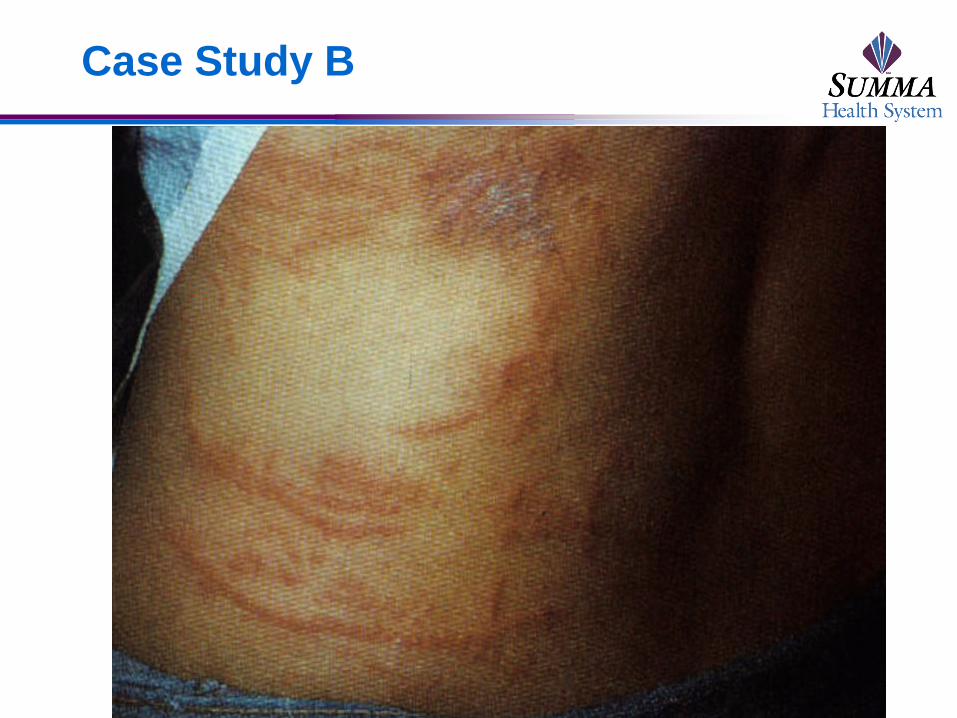
Case Study B A 39 y.o. male falls into the water from a boat
while on a Bahamas cruise. While making his way back to the boat, he noted sudden onset of severe stinging, burning, and almost numbing pain on the right anterior chest extending down to the right lower quadrant of his abdomen.
A couple of hours later, he notes severe burning abdominal and chest pain and has the rash noted on Figure # 7. VS show only a mild tachycardia, but no fever or change in blood pressure.
Case Study B
Case Study B
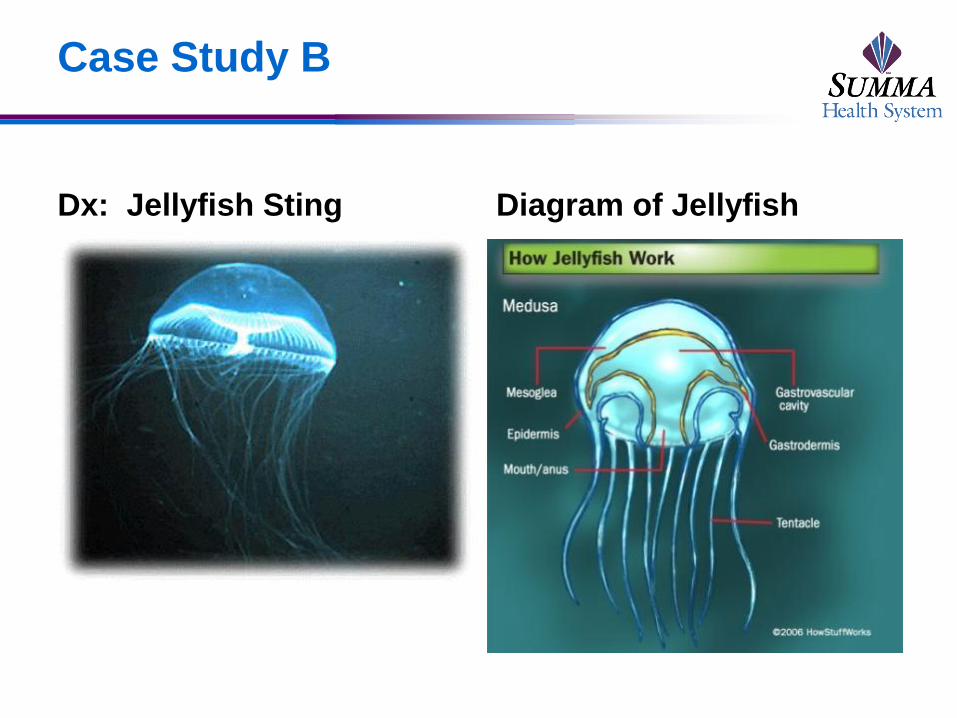
Dx: Jellyfish Sting Diagram of Jellyfish
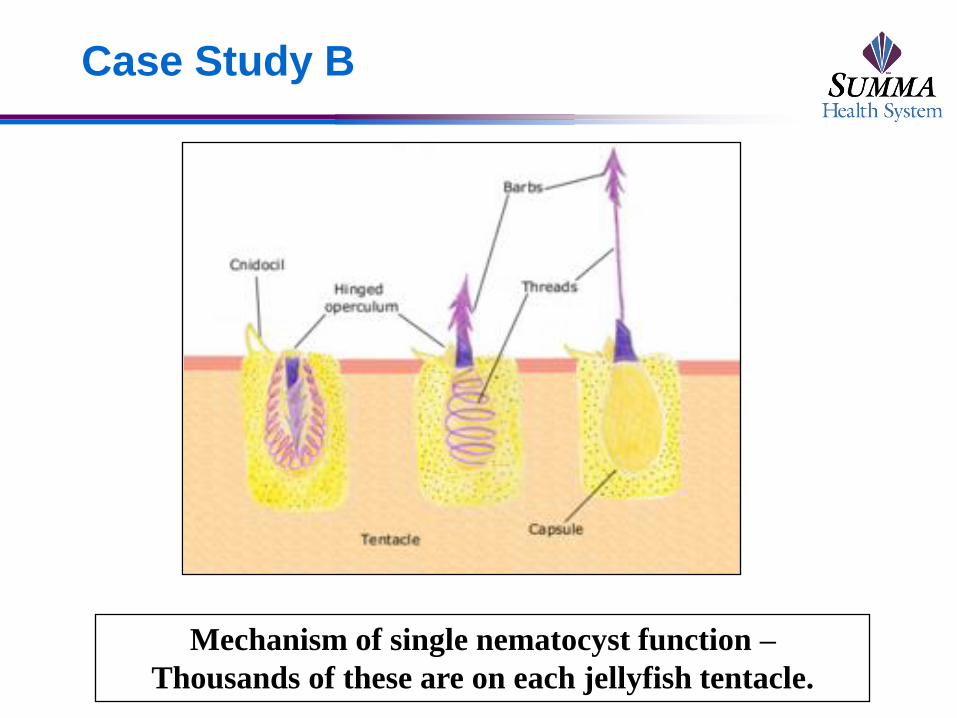
Case Study B
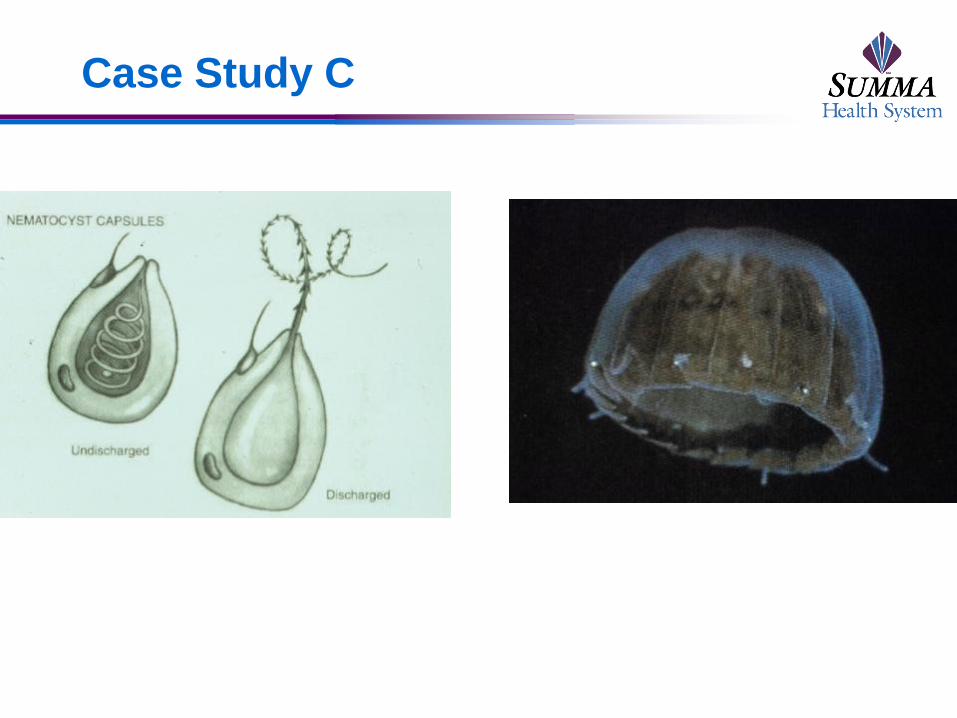
Mechanism of single nematocyst function –
Thousands of these are on each jellyfish tentacle.
Which of the following is/are appropriate
treatment(s)
For jellyfish sting?
a. Prompt removal of tentacles
b. Wash off with SEAWATER
c. Avoidance of cold fresh water
d. Application of acetic acid (e.g.,
vinegar)
e. All Above
Case Study B
Diagnosis: Jellyfish sting – the stinging tentacles
are filled with thousands of stinging nematocysts
Treatment:
Remove any remaining tentacles promptly
Do NOT immerse in cold fresh water (osmotic pressure of fresh
water causes nematocysts to “fire”)
Seawater CAN be used to wash off tentacles
Scrape off with credit card or plastic object
Case Study B
Treatment (continued):
Acetic acid (vinegar) inhibits discharge of nematocysts
Heat vs. cold application: studies have varied BUT heat
appears to be an effective treatment for at least some jellyfish
stings.
Papain meat enderizer: a well-performed study compared hot
water immersion with papain meat tenderizer: hot water
superior in relieving pain to meat tenderizer!
Case Study B
Treatment (continued):
“Other”: in vitro studies of ethanol and human urine show a
marked increase in release of nematocyst toxin from
Australian box jellyfish! So these remedies are neither
proven nor rational.
REMOVAL OF TENTACLES IS THE KEY, THE SOONER THE
BETTER.
Anti-venom is available for severe Australian box jellyfish stings.
Case Study C
A 37 y.o. woman and her husband just returned from a 3-day CME trip to Nassau. She noted the onset of discomfort in the area beneath her swimming suit immediately after coming out of the water on the last day of their vacation (Saturday) before leaving for home that evening.
On her first day at home (Sunday), her rash appeared with redness and raised tender lesions. These lesions also caused tremendous itching.
Her husband developed no such rash but never actually went into the water. He only sunbathed on the beach.
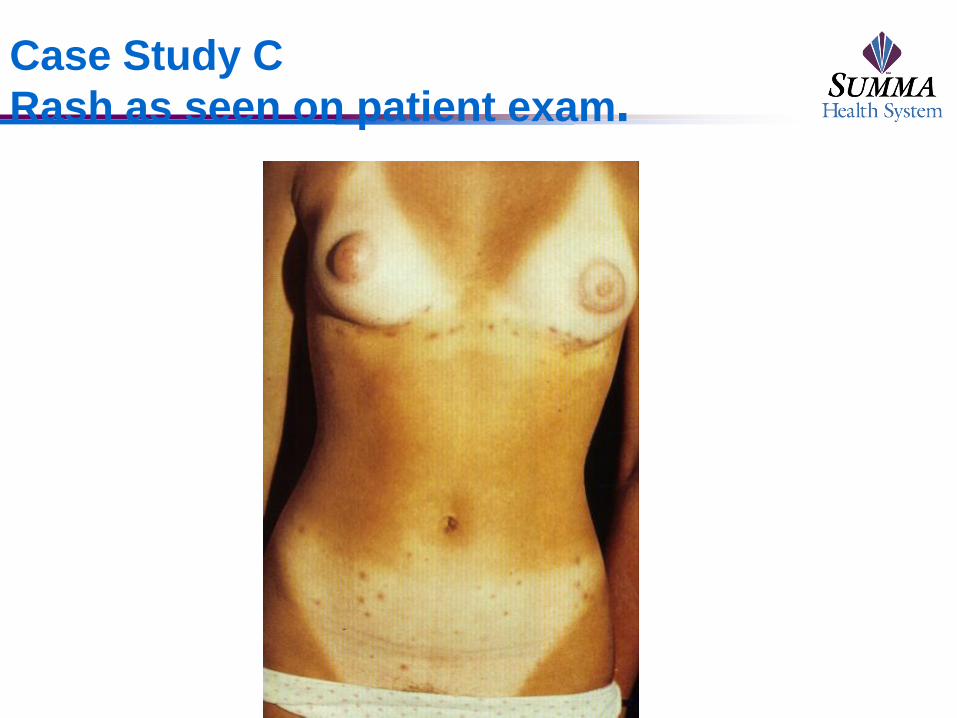
Case Study C
Rash as seen on patient exam.

Case Study C
How rash might look on the buttocks (left) and on a woman with one-
piece suit (right).
Case Study C
Diagnosis: Seabather's eruption is an itchy
dermatitis that occurs on parts of skin that
are covered by a swim-suit and is believed is
caused by jellyfish and sea anemone larvae,
which become trapped and pressed between
the outfit and the person's skin (see next
slide).
The skin reaction may recur when the outfit
is worn again, due to persistence of
nematocysts in the suit.
Malaise, fever, and gastrointestinal
symptoms can also occur in a minority of
patients with this condition.
Case Study C
Case Study C
Diagnosis: Seabather’s eruption – stings, usually
within clothing covered areas, with jellyfish or
sea anemone larvae who sting with their
nematocysts.
Treatment: Usually responds to topical
antihistamines and topical corticosteroids. Must
adequately rinse suit so that all larvae
(nematocysts) are eliminated from inside the suit.