Embed Size (px)
Citation preview

1. Background
2. Medical need
3. Existing treatments
4. Current research goals
5. Scientific rationale
6. Competitive environment
7. Potential development issues
8. Conclusion
9. Expert opinion
Review
Emerging EGFR antagonists forbreast cancerAna Lluch†, Pilar Eroles & Jose-Alejandro Perez-Fidalgo†Hospital Clinico Universitario, INCLIVA Biomedical Research Institute, Department of Oncology
and Hematology, Valencia, Spain
Introduction: The EGFR has been associated with the pathogenesis and
progression of breast cancer. Treatment based on an EGFR target is
emerging as a promising option, especially in combination with conventional
therapies. Unfortunately, there are no validated predictor biomarkers, and
combinatorial treatments are meeting new resistance.
Areas covered: The purpose of this review is to summarize the existing
treatments and the current research based on targeting the EGFR pathway.
Expert opinion: The existing EGFR treatments in breast cancer have shown
limited benefit. The combination of the monoclonal antibody cetuximab
and platinum salts achieves a 15 -- 20% response rate. The effectiveness of
tyrosine kinase inhibitors is not completely clear, showing modest or no
benefits. Gefitinib treatment has offered some promising results in estrogen
receptor + breast cancer. However, it has not been identified as a predictive
factor for the appropriate selection of patients. Radioimmunotherapy with
anti-EGFR radiolabeled antibodies is a promising strategy in BRCA-mutated
breast cancer, but it still requires clinical confirmation. Nevertheless, the cross-
talk between pathways frequently leads to treatment resistance. Current
research is focused on increasing knowledge about the mechanisms of
response and the discovery of predictive markers. Targeting several pathways
simultaneously and a correct selection of patients seem essential.
Keywords: angiogenesis, breast cancer, cetuximab, EGFR, erlotinib, gefitinib,
tyrosine kinase inhibitor
Expert Opin. Emerging Drugs (2014) 19(2):165-181
1. Background
The EGFR or HER1 and its ligands have been shown to contribute to the patho-genesis and progression of breast cancer [1-3]. The EGFR-dependent pathwayappears to be a driver mechanism for malignant carcinogenesis, particularly insome breast cancer subtypes. Approximately 50% of all cases of triple-negativebreast cancer (TNBC) and inflammatory breast cancer overexpress EGFR [4]. More-over, the growth of TNBC cell lines overexpressing this receptor is inhibitedby anti-EGFR therapies [5,6]. Hence, the development of anti-EGFR therapy isfocused mainly on TNBC. Nowadays, EGFR-targeted therapies are available,but unfortunately, none of these have identified a validated predictive biomarker[7-9].
2. Medical need
Treatments are becoming more and more heterogeneous depending on the breastcancer subtype. Luminal breast cancer is often susceptible to endocrine therapy,and therefore, this is a preferred strategy in this subset. However, most luminalbreast cancers will develop hormone resistance over time. Strategies to overcomethis resistance have gained interest in recent years. EGFR overexpression has been
10.1517/14728214.2014.903919 © 2014 Informa UK, Ltd. ISSN 1472-8214, e-ISSN 1744-7623 165All rights reserved: reproduction in whole or in part not permitted
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

linked to a poorer prognosis and less benefit for patientstreated with tamoxifen [10,11]. It has been suggested thatEGFR may be involved in the process of de novo resistanceto endocrine therapy [12]. In this context, EGFR is an attrac-tive target to overcome resistance to endocrine therapy.The HER2 breast cancer subtype is characterized by
overexpression of the HER2 receptor. The blockade of theHER2-dependent signaling pathway has been demonstratedto be very beneficial in this subtype of breast cancer.HER2, like EGFR, is a member of the ErbB receptor family.The formation of heterodimers between HER2 and othermembers of the ErbB family leads to the initiation of theHER2-dependant cascade. Thus, a double blockade ofHER2 and other receptors of the ErbB family could helpin increasing the benefit achieved by anti-HER2 therapies.EGFR targeting therapy could be of interest in this breastcancer subtype.
Finally, TNBC is a subtype characterized by the absence ofexpression of estrogen receptors (ERs) and progesteronereceptors (PRs) and of HER2. Treating TNBC is a challeng-ing issue for two reasons: first, it lacks a recognized target formolecular-oriented therapy, and second, it is a subset of breastcancer with a relatively poor prognosis, especially in thosewith advanced-stage disease [13]. Many TNBCs overexpressEGFR, which is an adverse prognostic factor [14]; therefore,the development of EGFR-based targeted strategies is a matterof high concern.
3. Existing treatments (Table 1)
Nowadays, the only anti-EGFR compound approved for thetreatment of breast cancer is lapatinib. However, lapatinibactivity obeys the anti-HER2 effect and not the anti-EGFReffect, and so its use is restricted to HER2+ breast cancer.
Table 1. Most relevant studies focused on anti-EGFR therapy in breast cancer.
Compound Target Study Stage N Regimen Evidence in
breast cancer
Cetuximab EGFR O’Shaughnessy et al. (2007) [48]Carey et al. (2012) [50]Baselga et al. (2013) [51]
Phase IIPhase IIPhase II
72102173
+Irinotecan/carboplatin+Carboplatin+Cisplatin
Advanced TNBC(subgroup)Advanced TNBCAdvanced TNBC
Panitumumab EGFR Nabholtz et al. (2011) [55] Phase II 58 +FEC 100 - docetaxel Neoadj TNBCErlotinib EGFR Twelves et al. (2008) [66]
Dickler et al. (2008) [18]Dickler et al. (2009) [58]Montagna et al. (2012) [65]
Phase I/IIPhase IIPhase IIPhase II
24386924
+capecitabine/docetaxel+BevacizMonotherapy+CC+bevaciz
Advanced BCAdvanced BCAdvanced BCAdvanced TNBC
Gefitinib EGFR Baselga et al. (2005) [77]Von Minckwitz et al. (2005) [73]Polychronis et al. (2005) [75]Ciardiello et al. (2006) [109]Smith et al. (2007) [110]Arteaga et al. (2008) [74]Cristofanilli et al. (2010) [111]Osborne et al. (2011) [76]Bernsdorf et al. (2011) [112]Carlson et al. (2012) [113]
Phase IIPhase IIPhase IIPhase IIPhase IIPhase I/IIPhase IIPhase IIPhase IIPhase II
315856412064193290180141
MonotherapyMonotherapy+Anastrozole+Docetaxel+Anastrozole+Trastuzumab+Anastrozole+Tamoxifen+EC � 4 cycles+Anastrozole orfulvestrant
Advanced BCAdvanced BCNeoadj ER+, EGFR+
Advanced BCNeoadj HR+
Advanced HER2+
Advanced HR+
Advanced HR+
Neoadj ER-
Advanced HR+
Lapatinib* EGFRHER2
Di Leo et al. (2008) [80]Pestrin et al. (2012) [83]
Phase IIIPhase II
40696
+PaclitaxelMonotherapy
Cohort: HER2-
Advanced HER2- butCTC HER2+
Neratinib* EGFRHER2HER4
Bose et al. (2013) [90] Preclinical - Monotherapy HER2- tumor samples
Afatinib* EGFRHER2HER3HER4
Schuler et al. (2012) [94] Phase II 50 Monotherapy Advanced BC: cohortTNBC/cohort HR+
Vandetanib EGFRVEGFR
Miller et al. (2005) [97]Boer et al. (2012) [98]
Phase IIPhase II 64
Monotherapy+Docetaxel Advanced BC
*In order to show the real impact of pure EGFR blockage induced by lapatinib, neratinib or afatinib, avoiding the confounding of the anti-HER2 effect, only those
studies including cohorts of HER2- tumors have been considered. The sample size and characteristics shown are related only to those cohorts including HER2-
patients.
BC: Breast cancer; Bevaciz: Bevacizumab; CC: Metronomic chemotherapy containing capecitabine and cyclophosphamide; CT: Chemotherapy; CTC: Circulant
tumor cells; EC: Epirubicin and cyclophosphamide; ER: Estrogen receptors; FEC: fluouracil, epirubicin and cyclophosphamide; HR: Hormone receptors; N: Sample
size; Neoadj: Neoadjuvant; TNBC: Triple-negative breast cancer.
A. Lluch et al.
166 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

4. Current research goals
The role of EGFR and its ligands in breast cancer prognosis isnot totally defined. However, recent findings are changingthis idea and new molecules are being developed using thisreceptor as a target. Breast cancer treatments based on theEGFR target are emerging as promising options, especiallyin combination with existing therapies. This is the case ofthe combination of gefitinib and hormone therapy [15,16] orthe combination of erlotinib with trastuzumab [17] or bevaci-zumab [18]. Current research is aimed at improving the mosteffective way to make these combinations, something whichoften requires a careful selection of eligible patients fortreatment.
The second line of research that is underway, regardingtreatments that target the EGFR pathway, aims at mitigatingor avoiding, as much as possible, the resistance to treatment.In this regard, it is of great interest to delve into the mecha-nisms involved in angiogenesis, alterations in the internaliza-tion and the degradation processes and mechanism ofnuclear localization of the receptor. Overexpression ofother receptors or growth factors of the HER family mayalso influence the response to the targeted therapy, as well asmany other downstream signaling pathways such as phosphoi-nositide 3-kinase (PI3K)/AKT or those involved in theepithelial-to-mesenchymal transition.
5. Scientific rationale
Activation of the receptor EGFR after ligand binding leads tocell proliferation and metastases via the PI3K/AKT, RAS/RAF/MEK/ERK and PKCg/PKC pathways. EGFR isimportant in the normal regulation of tissues; however, onamplification, protein overexpression or mutation can be adeterminant in the development of a new tumor. To date,three small tyrosine kinase inhibitors (TKIs) and two mono-clonal antibodies have been approved by the FDA for use incancer treatment. The appearance of resistance led to the inves-tigation of the mechanisms responsible and a way to inactivatethem.
High expression of EGFR has been detected in breastcancer, mainly in the basal subtype with poor prognosisgenerally associated with high grade, visceral liver and brainmetastases [19,20]. Even EGFR mutations are rare, the geneshowing amplification in the metaplastic subtype [21], and itsoverexpression is more frequent in breast cancer 1(BRCA1) cases than in sporadic breast cancer (67 vs 18%).Experimental data support the idea that this receptor providesa growth advantage at the early stages of carcinogenesis [22].
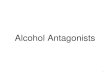
To date, clinical trials do not show a favorable response inunselected patients [21]. The EGFR inhibitor erlotinibincreases the time-to-development of a breast tumor in trans-genic mice, but the effect is exclusive to the ER-subtype(Figure 1) [22].
5.1 Angiogenesis pathway implicationsThe activation of the angiogenic pathway seems responsiblefor some of the resistance to anti-EGFR treatments, and theexperimental evidence [23] provides the rationale for targetingthis pathway.
Inflammatory breast cancer is one of the most aggressiveforms of breast cancer, with frequent positive lymph nodesand distant metastases. It is characterized by MAPK hyperacti-vation, presumably mediated by the overexpression of EGFRand/or ErbB2 [24].
MAPK signaling induces the activation of NF-kB leading toRhoC overexpression and a highly angiogenic phenotype [24].In vitro experiments show that cell lines resistant to EGFRantibodies expressed more VEGF and VEGFR1 mRNA andresponded to antiangiogenic treatment. For example, the dualVEGFR--EGFR TKI vandetanib (ZD6474) is capable of over-coming this resistance. ZD6474 reduces the activation (phos-phorylation) of VEGFR1 and VEGFR2, and the siRNA foreach of these receptors restores the sensitivity to EGFR inhibi-tors and the migratory potential. However, until now, theefficacy of this combinatorial treatment has not been proven.Inmetastatic colorectal cancer, dual VEGF and EGFR targetingwas not promising, as it showed a poor clinical response [25].
Mammalian target of rapamycin (mTOR) is a downstreamsignal regulated by the PI3K/AKT pathway whose activationpromotes the translation of VEGF mRNA into VEGF pro-tein, mediated by the p70S6 kinase [26]. The mTOR inhibitoreverolimus (Ev) has been combined in clinical trials with stan-dard treatments to evaluate the clinical benefits. Two majorPhase III trials, BOLERO 1 and BOLERO 3, are underway.These studies combined trastuzumab and Ev with paclitaxelor with vinorelbine in metastatic breast cancer.
The selective COX-2 inhibitor celecoxib has been proven toexert an antiangiogenic activity in pancreatic cancer. In breastcancer cells, celecoxib is capable of increasing the sensitivityof the cells by the hypermethylation of the MDR1 gene pro-moter that inhibits the expulsion of cytotoxics from thecells [27]. The combination of cetuximab and trastuzumab iswell tolerated, but it is not active in trastuzumab-refractorypatients [28].
5.2 EGFR internalization and degradationDespite the above, impaired EGFR internalization and degra-dation may lead to altered EGFR levels and to resistance.Experiments in cetuximab-resistant colorectal cancer cell linesshow the development of acquired resistance by decreasingEGFR protein levels through the promotion of EGFR associ-ation with Cbl, ubiquitination and degradation. The authorsbelieve that activation of the Src-mediated pathway is a mech-anism to bypass the EGFR-dependent cell signaling. Indeed,the inhibition of Src kinase activity reversed the resistance tocetuximab-induced apoptosis [29].
Other authors show high levels of EGFR in a cetuximab-resistant non-small-cell lung carcinoma cell line secondary to
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 167
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

altered trafficking/degradation of the receptor. The Src-familykinases (SFKs) are highly activated in cetuximab-resistantcells and these cells were resensitized to cetuximab whentreated with the Src inhibitor dasatinib. These data indicatethat SFKs and EGFR cooperate in acquired resistance tocetuximab [30].
5.3 HER familyUpregulation of different HER family members, such asHER2, HER3 or the MET receptor, may lead to ligand-independent receptor dimerization, and consequently, theactivation of downstream pathways [31]. This anomalous acti-vation has been suggested as a mechanism for overcomingcetuximab treatment.The hepatocyte growth factor (HGF) had been a mediator
of motility, invasion and proliferation in breast cancer.Expression of HGF and/or MET is associated with poor prog-nosis, because of its mitogen capacity. There is a crosstalkbetween these receptor tyrosine kinases. EGFR ligandsactivate c-MET, and HGF transactivates EGFR. All of thissupports the use of anti-EGFR therapy that would conse-quently reduce the proliferation and invasion of cancer cells.
The simultaneous blockade of these receptors has beenproposed as a possibility to prevent or reverse resistance.
5.4 Nuclear EGFRThe nuclear EGFR location identified in many breast cancersis a possible prognostic factor. Cells resistant to cetuximabshow increased nuclear EGFR and a high expression ofEGFR-regulated genes such as cyclin D1, B-myb and PCNA.Additionally, the expression of SFKs has been increased incases of cetuximab resistance, and some data suggest itsrequirement for EGFR nuclear translocation. In that sense,treatment with SFK inhibitors (e.g., dasatinib) is a reasonablechoice to overcome resistance.
5.5 Epithelial-to-mesenchymal transitionAnother mechanism proposed to avoid anti-EGFR treatmentis the epithelial-to-mesenchymal transition. The loss of adher-ent junctions and the gain of cytoskeletal filaments increasethe motility and invasiveness of the cells. These changes arecombined with an increased activation of the integrin-linkedkinases STAT3 and the downstream protein AKT. Xenograftmodel experiments confirm that the inactivation of
PTEN
Raf
Ras
PI3K
Nucleus
P
Endosome
Cyclin D PCNAB-MycSTAT3 E2F1
INOS Cox2
P
PAKT
mTOR
S6K1/24EBP1
HSP90GRB2
Mek
Erk1/2
EGFR overexpression
EGFR nuclear
TF
EG
FR
HE
R2
HE
R3
HE
R4
Downstreamactivationpathways
HER family overexpression
HER family growthfactors overexpression
Angiogenesis
Epithelial tomesenchymaltransition
EGF
TGF-α HB-EGF
P P
VEGF
VEGFRs
Lysosome
UbUb
NFκB
ProliferationSurvivalInvasionMetastasis
E-C
adhe
rin
ActincytoskeletonEGFR impaired
internalization/degradation
Potential mechanisms of resistance to anti-EGFR treatments
β-Catenin
α-Catenin
Figure 1. Potential mechanisms of resistance to anti-EGFR treatments are shown.
A. Lluch et al.
168 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

STAT3 restores the sensitivity to EGFR inhibitors [32].Further, low levels of the adherent protein E-cadherin havebeen related to decreased EGFR expression levels in cellularmodels [33] and consequent resistance to EGFR inhibitors.
5.6 Constitutive PI3K/AKT activationGiven the importance of PI3K/ATK pathway in survival andproliferation, the constitutive activation of this pathway hasbeen related to resistance to anti-EGFR therapy. Cetuximab-resistant cells show increased activation of AKT and SFKsand decreased phosphatase and tensin homolog (PTEN)levels. The combination of AKT inhibitors and cetuximab,or Src inhibitors and cetuximab, shows an antiproliferativesynergistic effect, in both cases [34], by decreasing AKT down-stream signaling. Similarly, the Src blockade sensitizes KRAS-mutant colon cancer cells to cetuximab treatment [35].
5.7 Increased expression of HER family growth
factorsAn increase in the HER family growth factors has beenidentified as another potential mechanism of resistance toanti-EGFR therapy. Increased amounts of heparin-bindingEGF are present in head and neck squamous carcinoma,cetuximab-resistant cells, and its decline can sensitize the cellsto the drug [36]. Moreover, the overexpression of the EGFRligand TGF-a has been suggested as a cause of the EGFRpathway deregulation through the development of an auto-crine loop [37]. Downstream components of the EGFR/HER2 pathway, such as Erk1/2 and AKT, can phosphorylateER at the activation domain, leading to a ligand-independentactivation of ER [38,39]. This ER signaling activation couldadditionally induce EGFR ligands, including TGF-a [40-42].These data suggest the importance of the crosstalk betweenER and EGFR receptors and notes that the ER pathway statusshould be considered in EGFR-based treatments.
Among the newly proposed mechanisms to prevent EGFRfunction is the use of heat shock protein 90 (Hsp90) chaperoneinhibitors. In preclinical models, few of them demonstratedpotent antitumor and antiangiogenic activity [43,44]; however,recent clinical trials in metastatic breast cancer are verypromising [45].
6. Competitive environment (Table 2)
6.1 Monoclonal antibodies
6.1.1 CetuximabCetuximab is a chimeric IgG1 monoclonal antibody thattargets the ligand-binding domain of the EGFR and is widelyused in colorectal or head and neck cancer. As an IgG1antibody, cetuximab may exert its antitumor efficacythrough both EGFR antagonism and antibody-dependentcell-mediated cytotoxicity [46].
Preclinical studies have shown that cetuximab presents asynergistic effect when combined with cisplatin in gefitinib-resistant TNBC cell lines [47].
The preliminary results of the USOR-04-070 study, arandomized Phase II trial comparing the combination ofirinotecan and carboplatin with or without cetuximab in first-and second-line metastatic breast cancer patients, resulted inimproved response rates (RRs) among a subset of TNBCpatients (n = 72, overall RR 30 vs 49%). However, noimprovement in progression-free survival (PFS) or overallsurvival (OS) was found for this subgroup. Moreover, thecombination resulted in an important increase of the grade3/4 diarrhea compared with chemotherapy alone (11 vs25%). This results were confirm in a later analysis. Howevera biomarker evaluation have identified PTEN as a predictivefactor to cetuximab therapy in TNBC patients with improvedPFS (HR = 0.40; p = 0.04) [48,49].
More recently, two randomized Phase II trials have assessedthe role of cetuximab in metastatic TNBC in combinationwith platinum salts. In 2012, Carey et al. published the resultsof the TBCRC-001 trial [50], in which 102 TNBC patientswere randomized to receive cetuximab monotherapy withthe addition of carboplatin after disease progression versusthe combination of both drugs from the beginning of the trial.The primary end point was the RR. RRs were 6% for cetux-imab in monotherapy and 16% for the addition of carbopla-tin after progression. In the combination of cetuximab pluscarboplatin arm, from the beginning the RRs were 17%. Ofnote, up to 31% of the patients responded or had prolongeddisease stabilization. The regimen combining cetuximaband carboplatin was well tolerated. Nevertheless, time-to-progression (TTP) and OS were short at 2.1 and 10.4 months,respectively. This study included a genomic analysis ofarchived tumor tissue. Of the 73 patients with available tissue,74% had the basal-like molecular subtype. A total of 16patients had tumor biopsies before therapy and 1 week after,and genomic patterns of the EGFR pathway showed activa-tion in 13 and inhibition by therapy in 5 of the patients.These results demonstrated that despite strong preclinicalevidence, inhibition of the EGFR pathway is a discouragingstrategy with a RR of < 20%. These data suggest that alterna-tive activated pathways are present in the majority of TNBC.
More recently, Baselga et al. [51] conducted a trial, theBALI-1 study, including 115 patients with TNBC who wererandomized in a 2:1 design to receive no > 6 cycles of cisplatinand cetuximab versus cisplatin alone. Patients receiving cis-platin alone were allowed to switch to cetuximab plus cisplatinafter progression. The RR was 20% with cisplatin plus cetuxi-mab versus 10% with cisplatin alone (odds ratio: 2:13; 95%CI: 0.81 -- 5.59; p = 0.11). However, cisplatin plus cetuximabresulted in a longer PFS compared with cisplatin alone(median 3.7 vs 1.5 months; hazard ratio (HR): 0.67; 95%CI: 0.47 -- 0.97; p = 0.032). Median OS was not significantlylonger in the combination arm (median 12.9 vs 9.4 months;HR: 0.82; 95% CI: 0.56 -- 1.20; p = 0.31). The combinationwas well tolerated, with acne-like rash, neutropenia and fatiguebeing the most frequent adverse events. Although this is anegative study, as the primary end point (RR) was not met,
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 169
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

the addition of cetuximab doubled the RR and showedncouraging results in PFS versus cisplatin alone.It should be underlined that in the TBCRC-001 trial, only
3 -- 6% of the patients (depending on the arm considered)had never received chemotherapy before entering the trial;however, in BALI-1, 17% of the patients in both arms hadnot been treated with chemotherapy in either a neoadjuvantor a metastatic setting.In summary, the combination of cetuximab and platinum
salts is feasible and achieves a RR of approximately 15 -- 20%.Nevertheless, the outstanding increase in the median PFS inthe BALI-1 trial, which was more than double in the armwith cetuximab, is promising data.Two trials whose results are pending publication assessed
the combination of ixabepilone with or without cetuximabin TNBC. The NCT00633464 trial in metastatic or locallyadvanced TNBC included 79 patients, but the results havenot yet been communicated [52]. The NCT01097642 trialin the neoadjuvant setting is recruiting patients and itscompletion date is projected as 2014 [53].
6.1.2 PanitumumabPanitumumab, a fully human monoclonal antibody, blocksthe extracellular domain of EGFR. Due to its human origin,it has not been associated with the formation of any antibod-ies against it [54]. Panitumumab has been studied in colorectaland head and neck cancers.In 2011, the preliminary results of a Phase II study
combining panitumumab and FEC100 followed by docetaxelas neoadjuvant therapy for TNBC was communicated atAmerican Society of Clinical Oncology. A total of 58 patientswith stage II -- IIIA were included. The primary end point waspathologic complete response (pCR) which was assessed using
two different methods (Sataloff and Chevallier). The rates ofpCR achieved were 65% (Sataloff) and 56% (Chevallier).After neoadjuvant treatment, conservative surgery was possiblein 87% of the patients. Skin toxicity was the main side effectwith 69% having grade II and 19% grade III skin rashes.Neutropenia grade IV appeared in 27% of the patients [55].
In 2012 and 2013, two studies of biomarkers associated withthis trial were communicated. The first one showed that highKi-67 was predictive of response. However, high EGFR, lowcytokeratin 5 -- 6 and low p53, although associated with a betterresponse, were not statistically significant. Of note, skin rashwas not predictive of a better response [56]. In the more recentstudy, tumor levels of IGFR-1 appeared to play a role as apredictive factor for panitumumab therapy in this context [57].
6.2 Tyrosine kinase inhibitors
6.2.1 EGFR inhibitors6.2.1.1 ErlotinibErlotinib is an oral EGFR TKI used in the treatment ofnon-small-cell lung cancer and pancreatic cancer.
In monotherapy, erlotinib has shown a very limited activityin previously treated, locally advanced or metastatic breast can-cer. In a study published in 2009, 69 patients were recruitedinto two different cohorts (cohort one included patients pro-gressing after previous treatment with anthracyclines, taxanesand capecitabine, and cohort two included patients withadvanced diseased treated in second or latter lines) [58]. Erloti-nib was given orally at 150 mg/day. Only one patient in eachcohort (3%) had a partial response. Common adverse eventswere diarrhea, rash, dry skin, asthenia, nausea and anorexia.
Data from preclinical studies suggested that the EGFRsignaling pathway may play a role in the regulation of angio-genesis [59-62]. Anti-EGFR therapy decreases the production of
Table 2. Competitive environment.
Compound Company Structure Explored Stage of
development
Mechanism of action
Cetuximab Merck Monoclonalantibody
Studies in advanced TNBC Phase II Targets EGFR
Panitumumab Amgem Inc. Monoclonalantibody
Studies in neoadjuvantTNBC
Phase II Targets EGFR
Erlotinib Genetech-Roche TKI Studies in advanced BCand TNBC
Phase II Targets EGFR
Gefitinib AstraZeneca TKI Studies in early andadvanced BC (includingHER2+, HR+ and HR-
tumors)
Phase II Targets EGFR
Lapatinib GSK TKI HER2+
Activity by EGFRinhibition remains unclear
Phase III Targets EGFR and HER2
Neratinib Puma Biotech TKI HER2- tumor samples Preclinical Targets EGFR, HER2 andHER4
Afatinib Boehringer-Ingelheim TKI Studies in advanced BC inTNBC and HR+
Phase II Targets EGFR, HER2,HER3 and HER4
Vandetanib AstraZeneca TKI Advanced BC Phase II Targets EGFR and VEGFR
BC: Breast cancer; HR: Hormone receptors; TKI: Tyrosine kinase inhibitor; TNBC: Triple-negative breast cancer.
A. Lluch et al.
170 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

antiangiogenic factors, including VEGF, basic fibroblastgrowth factor and IL-8 [62]. In xenograft models, anti-EGFRand anti-VEGF therapy has increased activity comparedwith either agent alone [63,64]. In this context, a Phase II studywas performed in order to assess the efficacy of erlotinib150 mg orally in combination with intravenous bevacizumab(an anti-VEGF antibody) 15 mg/kg every 21 days. Again,erlotinib showed limited activity even in this schedule. Only1 patient out of 38 achieved a partial responsefor > 52 months. Only 15 patients had stable disease at9 weeks and only 4 of these patients remained in stable diseasebeyond 26 weeks. The level of EGFR was tested in tumortissue, but it was not predictive of response to therapy [18].
More recently, another trial tried to elucidate the potentialrole of double blockade of EGFR/VEGF. A Phase II studyassessed the combination of metronomic chemotherapy withcapecitabine (500 mg thrice daily) and cyclophosphamide(50 mg/day) with bevacizumab (15 mg/kg every 3 weeks)and erlotinib (100 mg/day) in TNBC patients. Of the 24patients assessable for response, 1 complete response (4%)and 14 partial responses (58%) were obtained. Moreover,21% had stable disease > 9 weeks. The overall clinical benefitdefined as the proportion of partial plus complete responsesplus stable disease > 24 weeks was 75%. Toxicity was mild,and most common grade III adverse events were hypertension(two patients), thrombosis (one patient) and diarrhea (onepatient). The authors concluded that this is an active regimen;however, it is uncertain if these results are due to the additionof erlotinib or if the responses observed could be exclusivelyjustified by the combination of bevacizumab and metronomicchemotherapy in a selected TNBC population [65].
In 2008, a dose-escalation study in patients with metastaticbreast cancer confirmed that erlotinib 100 mg/day continu-ously combined with capecitabine 825 mg/m2/12 h fromdays 1 to 14 and docetaxel 75 mg/m2 every 21 days waswell tolerated. A dose of 100 mg/day was considered themaximal tolerated dose for erlotinib in combination withcapecitabine [66]. Of note, the overall RR was 67%, compris-ing 2 complete and 12 partial responders in 21 assessablepatients. The most common treatment-related adverse eventswere gastrointestinal disorders and skin toxicities.
In fact, skin toxicity is a frequently seen side effect ofanti-EGFR agents with an incidence of 47 -- 100% [67]. It hasbeen speculated that cutaneous toxicity from anti-EGFRtherapy may be a result of an inflammatory response secondaryto EGFR inhibition. A prospective study performed inmetastaticbreast cancer patients treated with erlotinib analyzed differentmarkers in skin biopsies and correlated them to the developmentof skin rash. The AKT phosphorylation at baseline was signifi-cantly associated with not developing a rash, suggesting a poten-tial relationship of the PI3K--AKT pathway and skin rash [68].
6.2.1.2 GefitinibGefitinib is a reversible and specific TKI of the EGFR that hasbeen assessed in several clinical trials. Preclinical studies with
gefitinib in TNBC and HER2+ cell lines have shown thatgefitinib was an active compound for inhibiting the EGFRpathway and that this activity enhanced response to chemo-therapy [14]. Response to gefitinib was associated with reducedphosphorylation of both MAPK and AKT and induction ofG1 arrest. In vitro studies showed that gefitinib reducedEGFR phosphorylation and downstream MAPK signaling [69]
in tamoxifen-resistant cells. Later data confirmed evidence ofproductive crosstalk between the ER and EGFR pathwaysthat were crucial to cell growth [70,71]. In Phase I trials, oraladministration of gefitinib 500 mg was well tolerated [72],and the Phase II trial in breast cancer showed better tolerabil-ity at a lower dose [73].
In Phase I trials, the oral form was well tolerated, with700 mg/day being the dose-limiting toxicity [72]. LaterPhase II trials in breast cancer showed better tolerability at alower dose (250 mg) [74]. Taking into account its oralbioavailability and the preclinical evidence of crosstalkbetween the EGFR and ER pathways, gefitinib became anattractive option in combination with endocrine therapy. Inthis context, several clinical trials have been conducted inhormone receptor-positive breast cancer. Some data suggestedthat gefitinib may have a role in this context. A Phase IIpreoperative study of gefitinib versus gefitinib plus anastrozolein EGFR+ and ER+ postmenopausal patients conducted byPolychronis in 2005 showed a reduction in Ki-67 levels inboth branches, with a higher reduction in the combinationarm [75]. A second randomized Phase II clinical trial thatcompared tamoxifen with tamoxifen plus gefitinib in ER+
metastasis breast cancer patients showed a nonsignificantadvantage for the combination group in terms of PFS [76].These data suggest that gefitinib may have some potential todelay the development of acquired endocrine resistance butnot in the de novo resistance. Nevertheless, most clinical stud-ies conducted in multiple breast cancer subtypes have shownmodest or very limited activity of gefitinib in monotherapyor combined with either anti-HER2 or chemotherapy(Table 3).
Another important concern is toxicity. Despite initialmonotherapy trials that showed gefitinib to be well toleratedat doses < 700 mg [72,73,77], when gefitinib was combinedwith trastuzumab [74] or chemotherapy, toxicity (mainly diar-rhea) was very limited. In 2012, the NCT00319618 study, arandomized Phase II placebo-controlled trial comparingweekly docetaxel with weekly docetaxel plus gefitinib in met-astatic breast cancer, showed unexpectedly high toxicity [78].The most frequent severe adverse events were dehydrationand diarrhea. Adverse events were found in both arms, buttoxicity was increased by the addition of gefitinib. Afterincluding 18 of the planned 66 patients, the study wasprematurely closed due to toxicity.
Moreover, although the expression of EGFR has beentested as a possible biomarker, no predictive factor has beenidentified to date, thus preventing selection of appropriatepatients. In this context, gefitinib in breast cancer can only
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 171
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

Table
3.Relevanttrials
ofgefitinib.
Study
Design
Arm
sN
Primary
endpoint
Compariso
nObservations
Baselgaetal.
(2005)[77]
Single
arm
Phase
IItrial
Previouslytreated
advancedbreast
cancer
Gefitinib
500mg
31
RR:0%
CR;0%
pCR;
38.7%
SD
NA
EGFR
inhibitionshownin
allcasesaftergefitinib
treatm
ent
Decrease
inp26and
Ki-67seenin
skin
butnot
intumortissues
VonMinckwitzetal.
(2005)[73]
Single
arm
Phase
IItrial
Heavily
pretreated
(taxanesand
anthracycline)advanced
breast
cancer
Gefitinib
500mg
58
RR:1.7%
(98.3%
nonresponders
dueto
disease
progressionornot
evaluable)
NA
Inefficacy
inheavily
pretreatedbreast
cancer
Goodtolerance
(only
5.2%
discontinued
therapydueto
toxicity)
Polychronisetal.
(2005)[75]
Randomized
Phase
IItrial
Neoadjuvantsetting
ER+,EGFR
+operable
breast
cancer
Gefitinib
250mg+anastrozole
Gefitinib
250mg+placebo
27
29
Ki-67indexchanges
betw
eenpre-and
post-treatm
entvalues
Reduction:98%
Reduction:92.4%
Difference
betw
een
groups5.6%
(95%
CI:5.1
--6.0;
p=0.0054)
Significantforadditionof
anastrozole
Reductionin
phosphorylationofERat
Ser118wassimilarin
both
groups
Ciardiello
etal.
(2006)[109]
Single
arm
Phase
IItrial(2:5:5)
First-lineadvancedbreast
cancer
Gefitinib
250mg
+docetaxel75mg/m
2
+docetaxel100mg/m
214
27
ORR:54%
(22/41)
NA
Both
dosagesof
docetaxelshowedsimilar
activity
Grade3/4
neutropenia:
49%
ER+more
likely
torespond
Smithetal.
(2007)[110]
Randomized
Phase
IItrial(2:5:5)
Neoadjuvantsetting
HR+,stageIto
IIIB
operable
breast
cancer
Anastrozole
�16weeks:
+gefitinib
250mg�
16weeks
+placebo�
2weeks!
gefitinib
250mg�
14weeks
+placebo�
16weeks
31
90
85
Ki-67changesat2and
16weeksofanastrozole
alonevs
gefitinib
+anastrozole
Betw
eenbaselineand
16weeks!
-77.4
and-83.6%
Betw
eenbaselineand
2weeks!
-80.1
and-71.3%
Betw
een2weeksand
16weeks!
-19.3
and-43%
Geometric
mean
ratio(-1.37;95%
CI:0.79--2.39;
p=0.26)
Geometric
mean
ratio(-0.7;95%
CI:0.39--1.25;
p=0.22)
Geometric
mean
ratio(-1.42;95%
CI:0.86--2.35;
p=0.16)
Nonsignificant
ORR(secondary
end
point)nonsignificant
trendagainst
gefitinib
whichissignificantin
the
PR+subgroup(48%
for
gefitinib
+anastrozole
vs72%
inanastrozole
alone,p=0.03)
*Initialdose
was500mg,butdueto
diarrheathedose
wasreducedto
250mg
CBR:Clinicalbenefitrate;CR:Complete
response;CT:Chemotherapy;
ER:Estrogenreceptor;ev:
Evaluable;HR:Hazard
ratio;NA:Notavailable;ORR:Overallresponse
rate;pCR:pathologic
complete
response;PFS:
Progression-freesurvival;PR:Progesteronereceptor;RR:Response
rate;SD:Stable
disease;TTP:Tim
e-to-progression.
A. Lluch et al.
172 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

Table
3.Relevanttrials
ofgefitinib
(continued).
Study
Design
Arm
sN
Primary
endpoint
Compariso
nObservations
Arteagaetal.
(2008)[74]
Single
arm
Phase
I/IItrial
HER2+advancedbreast
cancer
Gefitinib
250mg+trastuzumab
2mg/kgweekly
Gefitinib
500mg+trastuzumab
2mg/kgweekly
Phase
I:3+3
Phase
II:35
Phase
I:allpatients
treatedwithgefitinib
500mghaddiarrhea
grade3.
Phase
II(only
with
250mg):medianTTP
3and5.3
monthsin
patients
withoutandwith
previousCT,respectively
NA
Gefitinib
250mgisthe
onlytolerable
dosage
withtrastuzumab
Interim
analysisof
efficacy
suggestedthat
thecombinationwas
unlikely
toresultin
clinicalbenefitcompared
withtrastuzumabalone
Cristofanillietal.
(2010)[111]
Randomized
Phase
IItrial
HR+advancedbreast
cancer
Gefitinib
250mg-anastrozole
Placebo-anastrozole
43
50
PFS:14.7
months
PFS:8.4
months
HR:0.55
(95%
CI:0.35--0.94;
pvaluenotgiven)
Significant
Closedprematurely
due
toslow
recruitment
Osborneetal.
(2011)[76]
Stratum
1
Randomized
Phase
IItrial
HR+advancedbreast
cancer
Endocrinetherapy-naı̈ve
orafteradjuvant
tamoxifen
Gefitinib
250mg-tamoxifen
Placebo-tamoxifen
105
101
PFS:10.9
months
PFS:8.8
months
All(n
=206):
HR:0.84(95%
CI:0.59--1.18;
p=0.31)
Naı̈ve(n
=158):
HR:0.78(95%
CI:0.52--1.15)
Afteradjuvanttamoxifen
(n=48):HR:1.47
(95%
CI:0.63--3.45)
Nonsignificant
Biomarkeranalysis!
greaterbenefitof
gefitinib
ifER(-)orlow
levelsofERprotein
Osborneetal.
(2011)[76]
Stratum
2
Randomized
Phase
IItrial
HR+advancedbreast
cancer
Afterfirstlinewith
aromatase
inhibitors
Gefitinib
250mg-tamoxifen
Placebo-tamoxifen
48
36
CBR:29.2%
CBR:31.4%
HR:0.72
(95%
CI:0.26--1.95;
p=0.52)
Nonsignificant
Bernsdorfetal.
(2011)[112]
Randomized
Phase
IItrial
Neoadjuvantsetting
ER(-),‡2cm
,operable
breast
cancer
EC�
4cycles!
gefitinib
250mg�
12weeks
EC�
4cycles!
placebo�
12weeks
94
(71ev)
86
(73ev)
pCR:17%
(12/71)
pCR:12%
(9/73)
Difference
4.57%
(95%
CI:-7.19--6.33;
p=0.44)
Nonsignificant
AsignificantlyhigherpCR
inpost-hocanalysiswas
seenin
TNBC
More
patients
discontinuedgefitinib
due
totoxicity
Carlsonetal.
(2012)[113]
Randomized
Phase
IItrial
HR+advancedbreast
cancer
Gefitinib
250mg*-anastrozole
Gefitinib
250mg*-fulvestrant
72
69
CBR:44%
CBR:41%
Notgiven
Sim
ilaractivity
Grade3--4toxicity:
36and35%
inanastrozole
and
fulvestrantarm
s,respectively
*Initialdose
was500mg,butdueto
diarrheathedose
wasreducedto
250mg
CBR:Clinicalbenefitrate;CR:Complete
response;CT:Chemotherapy;
ER:Estrogenreceptor;ev:
Evaluable;HR:Hazard
ratio;NA:Notavailable;ORR:Overallresponse
rate;pCR:pathologic
complete
response;PFS:
Progression-freesurvival;PR:Progesteronereceptor;RR:Response
rate;SD:Stable
disease;TTP:Tim
e-to-progression.
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 173
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

be recommended in clinical trials. The most relevant trials ofgefitinib are shown in Table 3.
6.2.2 EGFR and HER2 inhibitors6.2.2.1 LapatinibLapatinib is a reversible and selective inhibitor of the intracel-lular domains of the tyrosine kinases HER1 (EGFR) andHER2. It competes with ATP for the ATP-binding pocket,leading to downstream blocking of the PI3K/AKT/mTORpathway [79]. Potentially, the clinical benefit induced bylapatinib could be a result of its EGFR inhibitory effect inHER2-- breast cancer patients.In EGF30001, a Phase III randomized placebo-controlled
trial, lapatinib 1500 mg/day was given orally in combinationwith paclitaxel 175 mg/m2 every 21 days and was comparedwith placebo plus paclitaxel in two cohorts of patients,HER2+ and HER2- [80]. In the cohort of HER2+ patients,the addition of lapatinib resulted in significantly better out-comes in terms of TTP, event-free survival, clinical benefitand RR. However, in the cohort of HER2- or HER2unknown, lapatinib was ineffective. These results suggestedthat the role of EGFR inhibition induced by lapatinib wasmodest in comparison with the effect on the HER2 pathway.A retrospective analysis of data from the EGF3001 trial
showed that lapatinib activity in HER2- breast cancer patientsvaried depending on the PR expression. No benefit or strongexpression of PR was found in the TNBC subtype, but lapa-tinib was efficacious in patients with weak PR expression.On the contrary, lapatinib was deleterious in PR- breast can-cer patients. This retrospective subgroup analysis suggestedthat the hormone receptor could be a surrogate for HER2-or EGFR-dependent therapy. Nevertheless, these resultsmust be taken with caution because of the small sample sizeand the retrospective nature of the analysis [81].The lack of lapatinib activity in HER2- breast cancer was
confirmed in a meta-analysis of three Phase III trials. Thetrials included randomized studies looking at a combinationof lapatinib with chemotherapy or with endocrine therapyin the investigational arm. The HR for PFS and OS inHER2+ breast cancer was 0.69 and 0.76, respectively, andsignificantly favored the addition of lapatinib. However, inHER2- patients, the HR for PFS and OS were 0.98 (95%CI: 0.80 -- 1.19) and 0.89 (95% CI: 0.65 -- 1.21),respectively [82].Moreover, in a Phase II trial evaluating lapatinib in
monotherapy in patients with HER2- tumors, but withHER2+ circulating tumor cells, of the 96 patients includedin the study, only 1 patient achieved a response confirmingthe absence of effect of lapatinib in this subtype [83].Finally, a more recent preclinical study suggested that
instead of controlling the growth, lapatinib increased themigration and invasion when administered to a triple-negativecell line of breast cancer, by upregulating EGFR andCOX-2 [84].
The mTOR inhibitors have shown modest activity inmonotherapy in breast cancer. This issue is thought to bepartly due to an increase in the phosphorylated AKT levelsfollowing an exposure to rapalogues. The AKT activationcan be abrogated by the inhibition of upstream regulators inthe PI3K/AKT pathway. Given the fact that many TNBCsexpress EGFR [85] and that EGFR is an upstream regulatorof the PI3K/AKT pathway, it has been considered thatmTOR inhibitors may play a role as a sensitizer to upstreaminhibitors of the EGFR family. Based on this rationale, thecombination effects of the mTOR inhibitor rapamycin withlapatinib have been examined in TNBC in vitro and in vivo.The combination of EGFR inhibition using lapatinib andmTOR inhibition with rapamycin resulted in significantlygreater cytotoxicity than the single agents alone, and theseeffects were synergistic in vitro. The combination of rapamy-cin and lapatinib significantly decreased growth of TNBCin vivo compared with either agent alone. EGFR inhibitionabrogated the expression of rapamycin-induced activatedAKT in cancer cells in vitro. These results suggest thatmTOR inhibitors could sensitize a subset of TNBC toEGFR inhibitors [86].
6.2.2.2 NeratinibNeratinib is a potent, orally administered, irreversiblepan-HER inhibitor that inhibits EGFR, HER2 and HER4.Some data suggest that neratinib can potentially overcomethe acquired resistance of EGFR T790M mutations, whichare considered responsible for resistance to anti-EGFR inlung cancer. Its development was focused on tumors thatexpress a high level of ErbB2. A Phase I trial was performedin EGFR or HER2+ tumors and the maximum tolerateddose for neratinib was 320 mg/day. Dose-limiting toxicitywas diarrhea grade III. Of the 39 evaluable patients, 25 werebreast cancer patients and 14 were non-small-cell lung cancerpatients. RR in the breast cancer cohort was 32% [87].
Neratinib has been developed mainly in the treatmentof HER2+ breast cancer patients. Some Phase II trialshave shown promising activity in monotherapy [88] or incombination with chemotherapy [89] in this setting.
There are scarce data about the role of neratinib in HER2-
breast cancer. Thus, the real impact of EGFR blockadeinduced by neratinib remains uncertain. A recent preclinicalstudy performed by the University of Washington identified13 HER2 somatic mutations in breast cancers lacking ampli-fication of the HER2 gene. Seven of these mutations wereactivating mutations. Among these, the HER2 in-framedeletion 755 -- 759, which is homologous to the EGFRexon 19 in-frame deletions, had a neomorphic phenotypewith increased phosphorylation of EGFR or HER3. MutationL755S produced lapatinib resistance; however, all of thesemutations were sensitive to the irreversible kinase inhibitor,neratinib. These findings showed that the HER2 somaticmutation may be a valuable predictive biomarker fortreatment with neratinib in HER2- patients [90].
A. Lluch et al.
174 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

6.2.2.3 AfatinibAfatinib is a novel, potent, orally bioavailable, pan-HERblocker, which irreversibly inhibits all ErbB family members,including EGFR, HER2, HER3 and HER4.
As in other pan-HER inhibitors, afatinib has been assessedin HER2+ breast cancer. A Phase II trial administered afatinibmonotherapy in patients with HER2+ breast cancer whose dis-ease progressed after trastuzumab treatment. Afatinib showedpromising activity in this setting in a heavily pretreatedpopulation [91].
As a pan-HER inhibitor, afatinib may play a role byblocking both EGFR and HER2 pathways. In fact, in vitro,afatinib has demonstrated antiproliferative activity inHER2+ and TNBC cell lines [92,93]. The activity of afatinibin HER2- cell lines had been confirmed in vivo in xeno-grafts [92]. In 2012, a European Phase II study assessed theefficacy of afatinib against HER2- breast cancer [94]. The ratio-nale for assessing afatinib in this setting was based on the highEGFR expression in TNBC and the assumption that uncon-trolled ErB signaling is related to an increased oncogenicpotential in TNBC subtypes. Moreover, the transcriptionalrepressor activity of the ER on ErbB family members sug-gested that in ER+ patients, abating the natural activation ofER signaling by its ligand estradiol may bring about the useof alternative proliferation pathways, including the ErbB sig-naling network. A total of 50 patients were included in thetrial in two different cohorts, cohort A with TNBC patients(n = 29) and cohort B with ER or PR+ and HER2- breast can-cer patients (n = 21). Afatinib was given orally at 50 mg/dayand no objective responses were seen in either cohort. Themost frequent afatinib-associated adverse events were gastro-intestinal and skin disorders, which were manageable.Afatinib was ineffective in this setting.
6.2.3 EGFR and VEGFR inhibitors6.2.3.1 VandetanibVandetanib is a novel, orally available inhibitor of differentintracellular signaling pathways involved in tumor growth,progression and angiogenesis, including the VEGFR-2 andEGFR pathways. Phase I trials have shown that vandetanibis well tolerated as a single £ 300 mg/day dose [95]. Vandeta-nib has shown activity in combination with chemotherapyin non-small-cell lung cancer [96].
In metastatic breast cancer, vandetanib in monotherapy hasbeen studied in 46 pretreated patients in one of two cohorts(100 or 300 mg/day) on 28-day cycles. Vandetanib was gen-erally well tolerated. The most common toxicity was diarrheawhich was dose-related (grade II diarrhea occurred in 4.5 and37.5% of patients at 100 and 300 mg dose, respectively).However, the drug showed limited activity, with no objectiveresponses, and only 1 out of 46 patients experienced stabledisease longer than 24 weeks [97].
A randomized, double-blind, placebo-controlled Phase IItrial evaluated the activity and safety of vandetanib 100 mgorally and docetaxel 100 mg/m2 intravenously as a second-line
treatment for metastatic breast cancer. The primary end pointwas the number of progression events. A total of 64 patientswere randomized (n = 35 vandetanib and n = 29 placebo) andthe combination of vandetanib plus docetaxel was well toler-ated. No benefit was shown with the addition of vandetanib.In fact, a slightly greater number of patients experienced a pro-gression event by the data cut-off in the vandetanib trial (69 vs62%; HR: 1.19, two-sided 80% CI: 0.79 -- 1.81; p = 0.59) [98].However, this study has somemethodological problems and themain concern is the primary end point. In fact, considering thenumber of events of progression at a defined cut-off point for allpatients may be an important confounding factor as a longerobservation period prior to the cut-off may have influencedthe final outcome.
Skin toxicity is frequent in patients treated with vandeta-nib. In a meta-analysis of nine trials, including one in patientswith metastatic breast cancer, the incidence of skin rash was46.1% (95% CI: 40.6 -- 51.8%) and the incidence of high-grade skin rash was 3.5% (95% CI: 2.5 -- 4.7%). These resultssuggest that awareness and treatment of this unexpected eventmay be critical to ensure adherence to vandetanib therapy [99].
6.3 Anti-EGFR radioimmunotherapyRadioimmunotherapy or the administration of targeted radio-therapy with radiolabeled antibodies is an old strategy that hasproduced several discouraging results in solid tumors [100].Such unsuccessful results can be partly explained by the impos-sibility of the radiolabeled antibodies to penetrate and deliversufficient doses (typically < 30 Gy) to elicit responses. However,in non-Hodgkin’s lymphoma, lower doses are able to induceresponses [101]. A possible reason for this effect on non-Hodgkin’s lymphoma is the increased radiosensitivity (in arange of 1.3 -- 1.8 Gy) that can be attributed to impairedDNA repair from the inactivation of ataxia telangiectasiamutated (ATM), p53 and otherDNA-repairing complexes [102].
DNA repair system impairment is present in not onlyhematologic malignancies but also some solid tumors. Hered-itary breast cancer associated with BRCA germline mutationspresent alterations in the DNA repair mechanisms, and mostbreast cancer with BRCA mutations are TNBC, whichimportantly show EGFR overexpression. In this sense, anin vivo study in a mouse model of TNBC showed that tumorbreast cancer cells could be targeted by the antibody 213Bi-cetuximab [101]. A second preclinical study analyzed the roleof the combination of the radiolabeled antibody 177Lu-anti-EGFR monoclonal antibody, chemotherapy and poly (ADP-ribose) polymerase 1 (PARP) inhibition in xenograph modelsin mice. TNBC orthotopic and metastatic lesions in the micewere eradicated with this triple combination, and the responsewas associated with apoptosis and eradication of putativebreast cancer stem cells [103].
In conclusion, radioimmunotherapy with anti-EGFRradiolabeled antibodies is a promising strategy in BRCA-mutated breast cancer, but the preclinical observations stillneed to be confirmed in the clinic.
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 175
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

7. Potential development issues
Although the antibody cetuximab directed against EGFR hasbeen successful in many cases, there is still great interest in theidentification of biomarkers that predict response to thistreatment.Another crucial point in treatment is to reverse the resistance.
Cetuximab-resistant cells show activation of the PI3K/AKT/mTOR pathways and deregulation of the non-receptor c-Srccytoplasmic TK. Src and PI3K, together with ER-a , form acomplex involved in non-genomic, estrogen-induced cell prolif-eration [104]. Usually resistance is accompanied by an increase inSrc kinase activity. The Src inhibition exerts effects mainly bypreventing dormant cells from becoming metastatic cells. Useof the Src/Abl kinase inhibitor AZD0530 synergizes with theEGFR inhibitor gefitinib in suppressing the invasive phenotype,at least in vivo [105]. Given the importance of the PI3K/AKTpathway as a key regulator of cell proliferation, another promis-ing approach is the combination with dual inhibitors of PI3Kand mTOR, such as the compound BEZ2235. Further, it hasbeen described that the combination of cetuximab and AKTinhibitors or Src inhibitors shows an antiproliferative synergisticeffect in non-small-cell lung cancer [34].Lapatinib treatment against EGFR and HER2 decreases
the phosphorylation of the Src family and AKT. Accordingly,both pathways seem as relevant potential targets in cases ofresistance.One of the major drawbacks in the development of
successful EGFR therapies is the redundant pathways andthe multiple crosstalks that lead to resistance. Consequently,it is necessary to attack multiple targets to achieve the maxi-mal therapeutic effect and minimize resistance. The combina-tion of therapies against the Src family or against the PI3K/AKT/mTOR pathway with anti-EGFR drugs is the mainstrategy, and it is where research is focused.However, we should not forget to explore other possible
combinations with the thought that they could be used asHER2, IGFR1, VEGFR TKIs and PARP inhibitors orHsp90 and integrin antagonists.
8. Conclusion
A great challenge still lies ahead in order to improve the synthesisof compounds, identify new targets and improve strategies thattarget the EGFR pathway. Among the obstacles faced by EGFRdrugs in order to be effective are the redundancy of pathwaysand the crosstalk mechanisms, leading to resistance in manycases. Targeting several pathways simultaneously seems thestrategy to elect, and future research is headed in this direction.
9. Expert opinion
Based on the existing evidence, EGFR is still far from being avaluable target in breast cancer. Probably the reason for some
of these discouraging results is the absence of an appropriateselection of patients. In fact, it appears that EGFR-targetedtherapy in breast cancer could repeat the story of lung cancer.Anti-EGFR TKI s failed to demonstrate benefits in survival inthe early clinical trials of unselected populations. Only theidentification of a subset of patients defined by EGFR-specificmutations has shown that EGFR has a role in the manage-ment of lung cancer. This could be the future of the anti-EGFR in breast cancer, and future investigations should focuson the identification of a subset of patients that could benefitmore from anti-EGFR therapy. Hypothetically, the basal-likebreast cancer subtype has some characteristics that lead us toconsider that EGFR inhibition could be an attractive alterna-tive in this subtype. First, the important overexpressionof EGFR in this subset which is expressed in up to 60% ofpatients suggests that EGFR could be a driver pathway inthis subtype. Second, there is an unmet medical need inbasal-like breast cancer. This subtype has a worse prognosisand there is a lack of an approved targeted therapy that isspecifically targeted against these tumors. In this context,there is an increasing interest to develop new targeted com-pounds. However, it appears that basal-like subtype is not asufficient predictive factor for response to anti-EGFR therapy.Thus, a valuable predictive biomarker of activity is a strongneed in this context. This biomarker could explain, forinstance, the promising results on PFS with cetuximab inthe BALI-1 trial. KRAS mutations seem not to be a valuablebiomarker for anti-EGFR activity as these mutations areextremely infrequent in breast cancer. Considering the rele-vant role recently identified for NRAS and BRAF mutationsin colorectal cancer, it is easy to establish a potential parallelwith breast cancer. However, all these mutations are extremelyrare in breast cancer [106]. Similar conclusions are drawn byanalyzing the role of EGFR mutations. EGFR genomic aber-rations are a valuable biomarker for anti-EGFR therapy inlung cancer, but the presence of this factor in breast canceris very infrequent ranging from 0 to approximately 11.4%in TNBC cells [8,106,107]. Another topic of potential interestis the presence of a high EGFR gene copy number. A recentstudy in a population of Asiatic patients with TNBC showedthat a high EGFR gene copy number was as frequent as 33%mainly due to high polisomy [108]. All these studies suggest apotential for many different factors that could eventually bepredictive of anti-EGFR therapy, but there is an increasingneed to incorporate a prospective evaluation of these genomicalterations in the upcoming studies.
Another focus that is gaining special interest is the PI3K/AKT/mTOR pathway. Up to 17% of TNBC show PI3Kmutations, with the pH1047R mutation being the mostfrequently identified in this subset. Nevertheless, other altera-tions related to this pathway, such as PTEN loss, could play arelevant role in selecting the most appropriate populationto treat.
In this context, the future trials, not only in anti-EGFRtherapy, must use massive sequencing strategies in order to
A. Lluch et al.
176 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

explore a huge number of relevant mutations that may even-tually be predictive. Only with the help of this technologywill the upcoming investigations find a trace to follow in thesearch for predictive biomarkers.
Apart from the identification of a biomarker, which is a keyissue in the future development of anti-EGFR targeted ther-apy, the strategy of blocking different pathways or the samepathway at different points is a topic with special interest.The double blockage strategy follows the same rationale; thereis a second pathway or messenger that allows the tumor cell toescape from the effect of the anti-EGFR agent. Two situationscould explain this resistance: a crosstalk that allows the cell tosurvive despite the inhibition of the EGFR pathway by usingan alternative pathway or a mutation or specific alteration in adistal point of the EGFR pathway that turns the cell resistanceto any upstream inhibition of this pathway. In both cases,dual blockade is the best alternative to overcome this resis-tance. In this context, future trial design should establish adual inhibition targeting EGFR and a second molecule pre-sumably related to the PI3K/AKT/mTOR or RAS/RAF/MEK pathways. Moreover, the combination of anti-EGFRand MEK inhibitors is other alternative to consider.
Finally, considering the relationship of TNBC and thehomologous recombination deficiency, it appears reasonable
to establish strategies combining an anti-EGFR with a drugtargeting the DNA repair system. Some chemotherapy agentssuch as platin salts, temozolomide or topotecan have mecha-nisms of action against different enzymes involved in DNArepair. In this context, the BALI-01 and TBCRC-001 trialshave explored the combination of cetuximab and a platinsalt in TNBC. Recently, a new family of agents, the PARPinhibitors targeting the base excision repair system, wasexplored in this subset. It appears to be of great interest toexplore the combination of these agents with anti-EGFRtherapies in TNBC.
In summary, EGFR is probably a relevant target in breastcancer. However, clinical evidence of activity is really poorto date. These discouraging results can be explained at leastin part by the poor selection of patients. Identification ofvaluable biomarkers is a need in this setting. Dual blockadestrategies or combination with agents targeting the DNArepair systems could help in overcoming the apparentresistance to these agents.
Declaration of interest
The authors state no conflict of interest and have received nopayment in preparation of this manuscript.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. Ciardiello F, Tortora G. A novel
approach in the treatment of cancer:
targeting the epidermal growth factor
receptor. Clin Cancer Res
2001;7:2958-70
2. Mendelsohn J, Baselga J. Status of
epidermal growth factor receptor
antagonists in the biology and treatment
of cancer. J Clin Oncol 2003;21:2787-99
3. Normanno N, De Luca A, Bianco C,
et al. Epidermal growth factor receptor
(EGFR) signaling in cancer. Gene
2006;366:2-16
4. Masuda H, Zhang D, Bartholomeusz C,
et al. Role of epidermal growth factor
receptor in breast cancer. Breast Cancer
Res Treat 2012;136:331-45
. This review focused on the role of
EGFR in breast cancer.
5. Baselga J, Norton L, Masui H, et al.
Antitumor effects of doxorubicin in
combination with anti-epidermal growth
factor receptor monoclonal antibodies.
J Natl Cancer Inst 1993;85:1327-33
6. Hoadley KA, Weigman VJ, Fan C, et al.
EGFR associated expression profiles vary
with breast tumor subtype.
BMC Genomics 2007;8:258
7. Pintens S, Neven P, Drijkoningen M,
et al. Triple negative breast cancer:
a study from the point of view of basal
CK5/6 and HER-1. J Clin Pathol
2009;62:624-8
8. Teng YH, Tan WJ, Thike AA, et al.
Mutations in the epidermal growth factor
receptor (EGFR) gene in triple negative
breast cancer: possible implications for
targeted therapy. Breast Cancer Res
2011;13:R35
9. Thike AA, Cheok PY, Jara-Lazaro AR,
et al. Triple-negative breast cancer:
clinicopathological characteristics and
relationship with basal-like breast cancer.
Mod Pathol 2010;23:123-33
10. Arpino G, Green SJ, Allred DC, et al.
HER-2 amplification, HER-1 expression,
and tamoxifen response in estrogen
receptor-positive metastatic breast cancer:
a southwest oncology group study.
Clin Cancer Res 2004;10:5670-6
11. Nicholson RI, McClelland RA, Finlay P,
et al. Relationship between EGF-R,
c-erbB-2 protein expression and
Ki67 immunostaining in breast cancer
and hormone sensitivity. Eur J Cancer
1993;29A:1018-23
12. Arpino G, De Angelis C, Giuliano M,
et al. Molecular mechanism and clinical
implications of endocrine therapy
resistance in breast cancer. Oncology
2009;77(Suppl 1):23-37
13. Crown J, O’Shaughnessy J, Gullo G.
Emerging targeted therapies in
triple-negative breast cancer. Ann Oncol
2012;23(Suppl 6):vi56-65
14. Corkery B, Crown J, Clynes M,
O’Donovan N. Epidermal growth factor
receptor as a potential therapeutic target
in triple-negative breast cancer.
Ann Oncol 2009;20:862-7
15. Buzdar A. Anastrozole as adjuvant
therapy for early-stage breast cancer:
implications of the ATAC trial.
Clin Breast Cancer
2003;4(Suppl 1):S42-8
16. Buzdar AU. ’Arimidex’ (anastrozole)
versus tamoxifen as adjuvant therapy in
postmenopausal women with early breast
cancer--efficacy overview. J Steroid
Biochem Mol Biol 2003;86:399-403
17. Britten CD. Targeting ErbB receptor
signaling: a pan-ErbB approach to
cancer. Mol Cancer Ther
2004;3:1335-42
. This review highlights the importance
of the cooperation between ErbB
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 177
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

receptors and the approaches being
developed to concurrently inhibit
multiple of these receptors.
18. Dickler MN, Rugo HS, Eberle CA, et al.
A phase II trial of erlotinib in
combination with bevacizumab in
patients with metastatic breast cancer.
Clin Cancer Res 2008;14:7878-83
. This study is one of the first trials to
assess the combination of an
anti-EGFR and an antiangiogenic
therapy in breast cancer patients.
19. Dawson SJ, Provenzano E, Caldas C.
Triple negative breast cancers: clinical
and prognostic implications.
Eur J Cancer 2009;45(Suppl 1):27-40
. This review focused on triple-negative
breast cancer (TNBC) associated with
high EGFR expression.
20. Sutton LM, Han JS, Molberg KH, et al.
Intratumoral expression level of
epidermal growth factor receptor and
cytokeratin 5/6 is significantly associated
with nodal and distant metastases in
patients with basal-like triple-negative
breast carcinoma. Am J Clin Pathol
2010;134:782-7
. The authors suggest a role for the high
level of intratumoral EGFR expression
in development of nodal or distant
metastases in patients with basal-like
or TNBC tumors.
21. Burness ML, Grushko TA, Olopade OI.
Epidermal growth factor receptor in
triple-negative and basal-like breast
cancer: promising clinical target or only a
marker? Cancer J 2010;16:23-32
22. Burga LN, Hu H, Juvekar A, et al. Loss
of BRCA1 leads to an increase in
epidermal growth factor receptor
expression in mammary epithelial cells,
and epidermal growth factor receptor
inhibition prevents estrogen receptor-
negative cancers in BRCA1-mutant mice.
Breast Cancer Res 2011;13:R30
.. This study relates the loss of BRCA-1
to an increase of EGFR. It also
suggests that increased EGFR
expression confers a growth advantage
to mammary epithelial cells at the
earliest stages of transformation.
23. Ciardiello F, Bianco R, Caputo R, et al.
Antitumor activity of ZD6474, a vascular
endothelial growth factor receptor
tyrosine kinase inhibitor, in human
cancer cells with acquired resistance to
antiepidermal growth factor receptor
therapy. Clin Cancer Res
2004;10:784-93
.. This article shows that the activation
of angiogenesis is responsible for some
of the anti-EGFR resistance, and the
inhibition of VEGF signaling is a
potential anticancer strategy.
24. Van Laere SJ, Van der Auwera I,
Van den Eynden GG, et al. NF-kappaB
activation in inflammatory breast cancer
is associated with oestrogen receptor
downregulation, secondary to EGFR
and/or ErbB2 overexpression and MAPK
hyperactivation. Br J Cancer
2007;97:659-69
. This article linked NF-kB activation to
loss of estrogen receptor (ER)
expression due to EGFR and/or
ErbB2 overexpression.
25. Larsen AK, Ouaret D, El Ouadrani K,
Petitprez A. Targeting EGFR and VEGF
(R) pathway cross-talk in tumor survival
and angiogenesis. Pharmacol Ther
2011;131:80-90
.. This review addressed the failure of
dual VEGF and EGFR targeting in
colorectal cancer. The information
about EGFR and VEGF pathway
crosstalk in tumor survival and
angiogenesis can be used on
breast cancers.
26. Klos KS, Wyszomierski SL, Sun M, et al.
ErbB2 increases vascular endothelial
growth factor protein synthesis via
activation of mammalian target of
rapamycin/p70S6K leading to increased
angiogenesis and spontaneous metastasis
of human breast cancer cells. Cancer Res
2006;66:2028-37
27. Xia W, Zhao T, Lv J, et al. Celecoxib
enhanced the sensitivity of cancer cells to
anticancer drugs by inhibition of the
expression of P-glycoprotein through a
COX-2-independent manner.
J Cell Biochem 2009;108:181-94
28. Dang CT, Dannenberg AJ,
Subbaramaiah K, et al. Phase II study of
celecoxib and trastuzumab in metastatic
breast cancer patients who have
progressed after prior trastuzumab-based
treatments. Clin Cancer Res
2004;10:4062-7
29. Lu Y, Li X, Liang K, et al. Epidermal
growth factor receptor (EGFR)
ubiquitination as a mechanism of
acquired resistance escaping treatment by
the anti-EGFR monoclonal antibody
cetuximab. Cancer Res 2007;67:8240-7
.. This study showed the development of
acquired resistance to cetuximab via
altering EGFR levels through
promotion of EGFR ubiquitination
and degradation, and using Src
kinase-mediated cell signaling to
bypass their dependency on EGFR for
cell growth and survival.
30. Wheeler DL, Iida M, Kruser TJ, et al.
Epidermal growth factor receptor
cooperates with Src family kinases in
acquired resistance to cetuximab.
Cancer Biol Ther 2009;8:696-703
31. Saxena R, Dwivedi A. ErbB family
receptor inhibitors as therapeutic agents
in breast cancer: current status and future
clinical perspective. Med Res Rev
2012;32:166-215
. This review focuses on the rationale
for targeting members of the ErbB
receptor family, the mechanism of
action, preclinical and clinical
trial data.
32. Fuchs BC, Fujii T, Dorfman JD, et al.
Epithelial-to-mesenchymal transition and
integrin-linked kinase mediate sensitivity
to epidermal growth factor receptor
inhibition in human hepatoma cells.
Cancer Res 2008;68:2391-9
33. Basu D, Nguyen TT, Montone KT,
et al. Evidence for mesenchymal-like
sub-populations within squamous cell
carcinomas possessing chemoresistance
and phenotypic plasticity. Oncogene
2010;29:4170-82
.. This article showed that the decreased
EGFR expression in the
mesenchymal-like subset correlates
with diminished regulation of MAPK/
PI3K pathways by EGFR ligands,
showing intrinsic resistance to
cetuximab in vitro and in vivo.
34. Kim SM, Kim JS, Kim JH, et al.
Acquired resistance to cetuximab is
mediated by increased PTEN instability
and leads cross-resistance to gefitinib in
HCC827 NSCLC cells. Cancer Lett
2010;296:150-9
35. Dunn EF, Iida M, Myers RA, et al.
Dasatinib sensitizes KRAS mutant
colorectal tumors to cetuximab.
Oncogene 2011;30:561-74
36. Hatakeyama H, Cheng H, Wirth P,
et al. Regulation of heparin-binding
EGF-like growth factor by miR-212 and
acquired cetuximab-resistance in head
A. Lluch et al.
178 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

and neck squamous cell carcinoma.
PLoS One 2010;5:e12702
37. De Laurentiis M, Arpino G,
Massarelli E, et al. A meta-analysis on
the interaction between HER-2
expression and response to endocrine
treatment in advanced breast cancer.
Clin Cancer Res 2005;11:4741-8
38. Bunone G, Briand PA, Miksicek RJ,
Picard D. Activation of the unliganded
estrogen receptor by EGF involves the
MAP kinase pathway and direct
phosphorylation. EMBO J
1996;15:2174-83
39. Joel PB, Smith J, Sturgill TW, et al.
pp90rsk1 regulates estrogen
receptor-mediated transcription through
phosphorylation of Ser-167.
Mol Cell Biol 1998;18:1978-84
40. Kato S, Endoh H, Masuhiro Y, et al.
Activation of the estrogen receptor
through phosphorylation by
mitogen-activated protein kinase. Science
1995;270:1491-4
.. This article highlights the importance
of the phosphorylation pathway of the
human ER and the crosstalk
with EGFR.
41. Russell KS, Hung MC. Transcriptional
repression of the neu protooncogene by
estrogen stimulated estrogen receptor.
Cancer Res 1992;52:6624-9
42. Wilson MA, Chrysogelos SA.
Identification and characterization of a
negative regulatory element within the
epidermal growth factor receptor gene
first intron in hormone-dependent breast
cancer cells. J Cell Biochem
2002;85:601-14
43. Eccles SA. The epidermal growth factor
receptor/Erb-B/HER family in normal
and malignant breast biology. Int J
Dev Biol 2011;55:685-96
44. Eccles SA, Massey A, Raynaud FI, et al.
NVP-AUY922: a novel heat shock
protein 90 inhibitor active against
xenograft tumor growth, angiogenesis,
and metastasis. Cancer Res
2008;68:2850-60
45. Modi S, Stopeck A, Linden H, et al.
HSP90 inhibition is effective in breast
cancer: a phase II trial of tanespimycin
(17-AAG) plus trastuzumab in patients
with HER2-positive metastatic breast
cancer progressing on trastuzumab.
Clin Cancer Res 2011;17:5132-9
46. Lenz HJ. Cetuximab in the management
of colorectal cancer. Biologics
2007;1:77-91
47. Oliveras-Ferraros C, Vazquez-Martin A,
Lopez-Bonet E, et al. Growth and
molecular interactions of the anti-EGFR
antibody cetuximab and the
DNA cross-linking agent cisplatin in
gefitinib-resistant MDA-MB-468 cells:
new prospects in the treatment of
triple-negative/basal-like breast cancer.
Int J Oncol 2008;33:1165-76
48. O’Shaughnessy J, Weckstein DJ,
Vukelja SJ, et al. Preliminary results of a
randomized phase II study of weekly
irinotecan/carboplatin with or without
cetuximab in patients with metastatic
breast cancer. Cancer Res Treat
2007;106:abstract 308
49. Khambata-Ford S, O’Shaughnessy J,
Brickman D, et al. Candidate predictive
biomarkers of cetuximab benefit in
triple-negative breast cancer.
J Clin Oncol
2010;28:15s (Suppl):abstract 1056
50. Carey LA, Rugo HS, Marcom PK, et al.
TBCRC 001: randomized phase II study
of cetuximab in combination with
carboplatin in stage IV triple-negative
breast cancer. J Clin Oncol
2012;30:2615-23
.. This study analyzed the role of the
combination of carboplatin and
cetuximab in TNBC, one of the first
clinical trials to assess the benefit of
this schedule.
51. Baselga J, Gomez P, Greil R, et al.
Randomized phase II study of the
anti-epidermal growth factor receptor
monoclonal antibody cetuximab with
cisplatin versus cisplatin alone in patients
with metastatic triple-negative breast
cancer. J Clin Oncol 2013;31:2586-92
.. The BALI-1 trial was one of the first
trials to assess a combination of
cetuximab and cisplatin and showed an
improvement in progression-free
survival with this schedule.
52. Available from: http://clinicaltrials.gov/
ct2/show/results/NCT00633464?
term=cetuximab+breast+cancer
&rank=2§=X0125clinicaltrials.gov
53. Available from: http://clinicaltrials.gov/
ct2/show/results/NCT01097642?
term=ixabepilone+cetuximab&rank=3
54. Carteni G, Fiorentino R, Vecchione L,
et al. Panitumumab a novel drug in
cancer treatment. Ann Oncol
2007;18(Suppl 6):vi16-21
55. Nabholtz J, Weber B,
Mouret-Reynier M, et al. Panitumumab
in combination with FEC 100
(5-fluorouracil, epidoxorubicin,
cyclophosphamide) followed by docetaxel
(T) in patients with operable, triple-
negative breast cancer (TNBC):
Preliminary results of a multicenter
neoadjuvant pilot phase II study.
J Clin Oncol 2011;29:abstract e11574
. This study is the first to assess the role
of panitumumab in the neoadjuvant
setting in TNBC.
56. Nabholtz J-MA, Dauplat M-M,
Abrial C, et al. Impact of biomarkers in
predictivity of the efficacy and toxicity of
a combination of panitumumab plus
FEC 100 followed by docetaxel in a
phase II neoadjuvant trial for
triple-negative breast cancer (TNBC)
patients. J Clin Oncol
2012;30:abstract 1051
57. Penault-Llorca F, Dauplat M-D,
Abrial C, et al. Response to the
anti-EGFR antibody panitumumab
combined with standard neoadjuvant
chemotherapy in triple-negative breast
cancer (TNBC): The immune and IGFR
pathways. J Clin Oncol
2013;15(Suppl):abstract 1058
58. Dickler MN, Cobleigh MA, Miller KD,
et al. Efficacy and safety of erlotinib in
patients with locally advanced or
metastatic breast cancer. Breast Cancer
Res Treat 2009;115:115-21
59. Bruns CJ, Solorzano CC, Harbison MT,
et al. Blockade of the epidermal growth
factor receptor signaling by a novel
tyrosine kinase inhibitor leads to
apoptosis of endothelial cells and therapy
of human pancreatic carcinoma.
Cancer Res 2000;60:2926-35
60. Ciardiello F, Caputo R, Bianco R, et al.
Inhibition of growth factor production
and angiogenesis in human cancer cells
by ZD1839 (Iressa), a selective epidermal
growth factor receptor tyrosine kinase
inhibitor. Clin Cancer Res
2001;7:1459-65
61. Hirata A, Ogawa S, Kometani T, et al.
ZD1839 (Iressa) induces antiangiogenic
effects through inhibition of epidermal
growth factor receptor tyrosine kinase.
Cancer Res 2002;62:2554-60
62. Perrotte P, Matsumoto T, Inoue K, et al.
Anti-epidermal growth factor receptor
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 179
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

antibody C225 inhibits angiogenesis in
human transitional cell carcinoma
growing orthotopically in nude mice.
Clin Cancer Res 1999;5:257-65
63. Jung YD, Mansfield PF, Akagi M, et al.
Effects of combination anti-vascular
endothelial growth factor receptor and
anti-epidermal growth factor receptor
therapies on the growth of gastric cancer
in a nude mouse model. Eur J Cancer
2002;38:1133-40
64. Li M, Ye C, Feng C, et al. Enhanced
antiangiogenic therapy of squamous cell
carcinoma by combined endostatin and
epidermal growth factor
receptor-antisense therapy.
Clin Cancer Res 2002;8:3570-8
65. Montagna E, Cancello G, Bagnardi V,
et al. Metronomic chemotherapy
combined with bevacizumab and
erlotinib in patients with metastatic
HER2-negative breast cancer: clinical and
biological activity. Clin Breast Cancer
2012;12:207-14
66. Twelves C, Trigo JM, Jones R, et al.
Erlotinib in combination with
capecitabine and docetaxel in patients
with metastatic breast cancer:
a dose-escalation study. Eur J Cancer
2008;44:419-26
67. Perez-Soler R, Delord JP, Halpern A,
et al. HER1/EGFR inhibitor-associated
rash: future directions for management
and investigation outcomes from the
HER1/EGFR inhibitor rash management
forum. Oncologist 2005;10:345-56
68. Tan AR, Steinberg SM, Parr AL, et al.
Markers in the epidermal growth factor
receptor pathway and skin toxicity during
erlotinib treatment. Ann Oncol
2008;19:185-90
69. Gee JM, Harper ME, Hutcheson IR,
et al. The antiepidermal growth factor
receptor agent gefitinib (ZD1839/Iressa)
improves antihormone response and
prevents development of resistance in
breast cancer in vitro. Endocrinology
2003;144:5105-17
70. Britton DJ, Hutcheson IR,
Knowlden JM, et al. Bidirectional cross
talk between ERalpha and EGFR
signalling pathways regulates
tamoxifen-resistant growth. Breast Cancer
Res Treat 2006;96:131-46
71. Gutteridge E, Agrawal A, Nicholson R,
et al. The effects of gefitinib in
tamoxifen-resistant and hormone-
insensitive breast cancer: a phase II study.
Int J Cancer 2010;126:1806-16
72. Meric JB, Faivre S, Monnerat C, et al.
[Zd 1839 "Iressa"]. Bulletin du Cancer
2000;87:873-6
73. von Minckwitz G, Jonat W, Fasching P,
et al. A multicentre phase II study on
gefitinib in taxane- and anthracycline-
pretreated metastatic breast cancer.
Breast Cancer Res Treat 2005;89:165-72
74. Arteaga CL, O’Neill A, Moulder SL,
et al. A phase I-II study of combined
blockade of the ErbB receptor network
with trastuzumab and gefitinib in
patients with HER2 (ErbB2)-
overexpressing metastatic breast cancer.
Clin Cancer Res 2008;14:6277-83
75. Polychronis A, Sinnett HD,
Hadjiminas D, et al. Preoperative
gefitinib versus gefitinib and anastrozole
in postmenopausal patients with
oestrogen-receptor positive and
epidermal-growth-factor-receptor-positive
primary breast cancer: a double-blind
placebo-controlled phase II randomised
trial. Lancet Oncol 2005;6:383-91
76. Osborne CK, Neven P, Dirix LY, et al.
Gefitinib or placebo in combination with
tamoxifen in patients with hormone
receptor-positive metastatic breast cancer:
a randomized phase II study.
Clin Cancer Res 2011;17:1147-59
77. Baselga J, Albanell J, Ruiz A, et al.
Phase II and tumor pharmacodynamic
study of gefitinib in patients with
advanced breast cancer. J Clin Oncol
2005;23:5323-33
78. Engebraaten O, Edvardsen H,
Lokkevik E, et al. Gefitinib in
combination with weekly docetaxel in
patients with metastatic breast cancer
caused unexpected Toxicity: results from
a randomized phase II clinical trial.
ISRN Oncol 2012;2012:176789
79. Opdam FL, Guchelaar HJ, Beijnen JH,
Schellens JH. Lapatinib for advanced or
metastatic breast cancer. Oncologist
2012;17:536-42
80. Di Leo A, Gomez HL, Aziz Z, et al.
Phase III, double-blind, randomized
study comparing lapatinib plus paclitaxel
with placebo plus paclitaxel as first-line
treatment for metastatic breast cancer.
J Clin Oncol 2008;26:5544-52
. This Phase III trial confirmed the
absence of activity of lapatinib in
HER2- breast cancer in combination
with paclitaxel. The results of this
study suggest that the anti-EGFR effect
has a very limited clinical benefit.
81. Finn RS, Press MF, Dering J, et al.
Estrogen receptor, progesterone receptor,
human epidermal growth factor receptor
2 (HER2), and epidermal growth factor
receptor expression and benefit from
lapatinib in a randomized trial of
paclitaxel with lapatinib or placebo as
first-line treatment in HER2-negative or
unknown metastatic breast cancer.
J Clin Oncol 2009;27:3908-15
82. Amir E, Ocana A, Seruga B, et al.
Lapatinib and HER2 status: results of a
meta-analysis of randomized phase III
trials in metastatic breast cancer.
Cancer Treat Rev 2010;36:410-15
. This meta-analysis confirmed that
lapatinib is ineffective in
HER2- patients.
83. Pestrin M, Bessi S, Puglisi F, et al. Final
results of a multicenter phase II clinical
trial evaluating the activity of single-agent
lapatinib in patients with HER2-negative
metastatic breast cancer and
HER2-positive circulating tumor cells.
A proof-of-concept study. Breast Cancer
Res Treat 2012;134:283-9
84. Hsia TC, Tu CY, Chen YJ, et al.
Lapatinib-mediated cyclooxygenase-2
expression via epidermal growth factor
receptor/HuR interaction enhances the
aggressiveness of triple-negative breast
cancer cells. Mol Pharmacol
2013;83:857-69
85. Reis-Filho JS, Tutt AN. Triple negative
tumours: a critical review.
Histopathology 2008;52:108-18
86. Liu T, Yacoub R, Taliaferro-Smith LD,
et al. Combinatorial effects of lapatinib
and rapamycin in triple-negative breast
cancer cells. Mol Cancer Ther
2011;10:1460-9
87. Wong KK, Fracasso PM, Bukowski RM,
et al. A phase I study with neratinib
(HKI-272), an irreversible pan ErbB
receptor tyrosine kinase inhibitor, in
patients with solid tumors.
Clin Cancer Res 2009;15:2552-8
88. Burstein HJ, Sun Y, Dirix LY, et al.
Neratinib, an irreversible ErbB receptor
tyrosine kinase inhibitor, in patients with
advanced ErbB2-positive breast cancer.
J Clin Oncol 2010;28:1301-7
. This study assessed the role of
neratinib in HER2+ breast cancer.
89. Awada A, Dirix L, Manso Sanchez L,
et al. Safety and efficacy of neratinib
A. Lluch et al.
180 Expert Opin. Emerging Drugs (2014) 19(2)
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.

(HKI-272) plus vinorelbine in the
treatment of patients with ErbB2-positive
metastatic breast cancer pretreated with
anti-HER2 therapy. Ann Oncol
2013;24:109-16
90. Bose R, Kavuri SM, Searleman AC, et al.
Activating HER2 mutations in
HER2 gene amplification negative breast
cancer. Cancer Discov 2013;3:224-37
91. Lin NU, Winer EP, Wheatley D, et al.
A phase II study of afatinib
(BIBW 2992), an irreversible ErbB
family blocker, in patients with
HER2-positive metastatic breast cancer
progressing after trastuzumab.
Breast Cancer Res Treat
2012;133:1057-65
92. Harbeck N, Schmidt M, Harter P, et al.
BIBW 2992, a novel irreversible EGFR/
HER1and HER2 tyrosine kinase
inhibitor for the treatment of patients
with HER2-negative metastatic breast
cancer after failure of no more than two
prior chemotherapies. Cancer Res
2010;69:5062; doi:10.1158/0008-5472.
SABCS-09-5062
93. Willmarth NE, Ethier SP. Autocrine and
juxtacrine effects of amphiregulin on the
proliferative, invasive, and migratory
properties of normal and neoplastic
human mammary epithelial cells.
J Biol Chem 2006;281:37728-37
94. Schuler M, Awada A, Harter P, et al.
A phase II trial to assess efficacy and
safety of afatinib in extensively pretreated
patients with HER2-negative metastatic
breast cancer. Breast Cancer Res Treat
2012;134:1149-59
95. Morabito A, Piccirillo MC, Falasconi F,
et al. Vandetanib (ZD6474), a dual
inhibitor of vascular endothelial growth
factor receptor (VEGFR) and epidermal
growth factor receptor (EGFR) tyrosine
kinases: current status and future
directions. Oncologist 2009;14:378-90
96. Herbst RS, Sun Y, Eberhardt WE, et al.
Vandetanib plus docetaxel versus
docetaxel as second-line treatment for
patients with advanced non-small-cell
lung cancer (ZODIAC): a double-blind,
randomised, phase 3 trial. Lancet Oncol
2010;11:619-26
97. Miller KD, Trigo JM, Wheeler C, et al.
A multicenter phase II trial of ZD6474,
a vascular endothelial growth factor
receptor-2 and epidermal growth factor
receptor tyrosine kinase inhibitor, in
patients with previously treated
metastatic breast cancer. Clin Cancer Res
2005;11:3369-76
98. Boer K, Lang I, Llombart-Cussac A,
et al. Vandetanib with docetaxel as
second-line treatment for advanced
breast cancer: a double-blind,
placebo-controlled, randomized Phase II
study. Invest New Drugs 2012;30:681-7
. This trial showed limited activity with
the addition of vandetanib to docetaxel
in breast cancer patients.
99. Rosen AC, Wu S, Damse A, et al. Risk
of rash in cancer patients treated with
vandetanib: systematic review and
meta-analysis. J Clin Endocrinol Metab
2012;97:1125-33
100. Goldenberg DM. Targeted therapy of
cancer with radiolabeled antibodies.
J Nucl Med 2002;43:693-713
101. Song H, Hedayati M, Hobbs RF, et al.
Targeting aberrant DNA double strand
break repair in triple negative breast
cancer with alpha particle emitter
radiolabeled anti-EGFR antibody.
Mol Cancer Ther 2013;12(10):2043-54
102. M’Kacher R, Bennaceur A, Farace F,
et al. Multiple molecular mechanisms
contribute to radiation sensitivity in
mantle cell lymphoma. Oncogene
2003;22:7905-12
103. Al-Ejeh F, Shi W, Miranda M, et al.
Treatment of triple-negative breast cancer
using anti-EGFR-directed
radioimmunotherapy combined with
radiosensitizing chemotherapy and PARP
inhibitor. J Nucl Med 2013;54:913-21
. This preclinical study suggests a
potential effect of radiolabeled
antibodies targeting EGFR and
PARP inhibitors.
104. Castoria G, Migliaccio A, Bilancio A,
et al. PI3-kinase in concert with Src
promotes the S-phase entry of
oestradiol-stimulated MCF-7 cells.
EMBO J 2001;20:6050-9
105. Hiscox S, Morgan L, Green TP, et al.
Elevated Src activity promotes cellular
invasion and motility in tamoxifen
resistant breast cancer cells. Breast Cancer
Res Treat 2006;97:263-74
106. Tilch E, Seidens T, Cocciardi S, et al.
Mutations in EGFR, BRAF and RAS are
rare in triple-negative and basal-like
breast cancers from Caucasian women.
Breast Cancer Res Treat
2014;143:385-92
107. Jacot W, Lopez-Crapez E, Thezenas S,
et al. Lack of EGFR-activating mutations
in European patients with triple-negative
breast cancer could emphasise geographic
and ethnic variations in breast cancer
mutation profiles. Breast Cancer Res
2011;13:R133
108. Park HS, Jang MH, Kim EJ, et al. High
EGFR gene copy number predicts poor
outcome in triple-negative breast cancer.
Mod Pathol 2014. [Epub ahead of print]
109. Ciardiello F, Troiani T, Caputo F, et al.
Phase II study of gefitinib in
combination with docetaxel as first-line
therapy in metastatic breast cancer.
Br J Cancer 2006;94:1604-9
110. Smith IE, Walsh G, Skene A, et al.
A phase II placebo-controlled trial of
neoadjuvant anastrozole alone or with
gefitinib in early breast cancer.
J Clin Oncol 2007;25:3816-22
111. Cristofanilli M, Valero V, Mangalik A,
et al. Phase II, randomized trial to
compare anastrozole combined with
gefitinib or placebo in postmenopausal
women with hormone receptor-positive
metastatic breast cancer. Clin Cancer Res
2010;16:1904-14
112. Bernsdorf M, Ingvar C, Jorgensen L,
et al. Effect of adding gefitinib to
neoadjuvant chemotherapy in estrogen
receptor negative early breast cancer in a
randomized phase II trial. Breast Cancer
Res Treat 2011;126:463-70
113. Carlson RW, O’Neill A, Vidaurre T,
et al. A randomized trial of combination
anastrozole plus gefitinib and of
combination fulvestrant plus gefitinib in
the treatment of postmenopausal women
with hormone receptor positive
metastatic breast cancer. Breast Cancer
Res Treat 2012;133:1049-56
AffiliationAna Lluch†1,2 MD PhD, Pilar Eroles2 PhD &
Jose-Alejandro Perez-Fidalgo1,2 MD PhD†Author for correspondence1Hospital Clinico Universitario, INCLIVA
Biomedical Research Institute, Department of
Oncology and Hematology, Valencia, Spain
Tel: +0034 963987659;
E-mail: [email protected] Biomedical Research Institute,
Valencia, Spain
Emerging EGFR antagonists for breast cancer
Expert Opin. Emerging Drugs (2014) 19(2) 181
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity L
ibra
ry U
trec
ht o
n 06
/02/
14Fo
r pe
rson
al u
se o
nly.