Embed Size (px)
Citation preview

National Patient Safety OfficeOifig Náisiúnta um Shábháilteacht Othar
Emergency Medicine Early Warning System (EMEWS)National Clinical Guideline No. 18
Annex 1: Systematic Review

AcknowledgmentsThe research team commissioned by the Department of Health, Clinical Effectiveness Unit, undertook the work described in this report. We thank the Steering Group for this project for their insight and support through the conduct of this work.
We thank Sinead Duane for assistance with initial screening of citations, and Rachel Lee for assisting with inputting citations from additional resources.
This report should be cited as:Wuytack F, Meskell P, Conway A, McDaid F, Santesso N, Hickey F, Gillespie P, Smith V, Devane D. (2016) Clinical and cost-effectiveness of physiologically based early warning or track and trigger or scoring systems after triage in adult patients presenting to emergency departments: A systematic review. National Clinical Effectiveness Committee, Department of Health: Dublin.
Published by:The Department of HealthBlock 1, Miesian Plaza50-58 Lower Baggot StreetDublin 2D02 XW14www.health.gov.ieISSN 2009-6259© Department of Health

Clinical effectiveness and cost-effectiveness of physiologically based early warning or track and trigger or scoring systems after triage in adult patients presenting to emergency departments: A
systematic review
AuthorsFrancesca Wuytack,1 Pauline Meskell,1 Aislinn Conway,1 Fiona McDaid,2,3 Nancy Santesso,4 Fergal Hickey,5 Paddy Gillespie,1 Valerie Smith,1 Declan Devane.1
1 NationalUniversityofIrelandGalway,Ireland.2 NaasGeneralHospital,Ireland.3 NationalEmergencyMedicineProgramme,Ireland.4 McMasterUniversity,Canada.5 SligoUniversityHospital,Ireland.

National Clinical Effectiveness Committee (NCEC)
Clinicaleffectivenessisakeycomponentofpatientsafetyandquality.Theintegrationofbestevidencein serviceprovision, throughclinical effectivenessprocesses,promoteshealthcare that isup todate,effectiveandconsistent.
TheNationalClinicalEffectivenessCommittee(NCEC)isaMinisterialcommitteeestablishedin2010aspartofthePatientSafetyFirstInitiative.TheNCECissupportedbytheClinicalEffectivenessUnit(CEU),DepartmentofHealth. TheNCEC is apartnershipbetweenkey stakeholders inpatient safetyand itsmissionistoprovideaframeworkfornationalendorsementofclinicalguidelinesandaudittooptimisepatientandserviceusercare.
InDecember2013, thefirstNationalClinicalGuideline (NCG)waspublished.ThiswasNCECNationalClinical GuidelineNo. 1National EarlyWarning Score (NEWS). It relates to the situation in an acutehospital setting where an adult patient’s physiological condition is deteriorating. It was updated inAugust2014toensurealignmentwithNCGNo.6SepsisManagement.
Invitations to tender were issued in July 2015 and a public procurement competition held for theprovisionof systematic literature reviewsandbudget impactanalysis to support thedevelopmentofNational Clinical Guidelines. Subsequently, a series of reportswere commissioned by the CEU/NCECDepartmentofHealth.Thisreportisthefirstpublishedunderthiscontract.Itsupportsthedevelopmentof aNational ClinicalGuidelineon EmergencyMedicine EarlyWarning System (EMEWS).A guidelineproposalwassubmittedtotheNCECbytheHSENationalClinicalProgrammeforEmergencyMedicineandwasprioritisedfordevelopmentasaNationalClinicalGuidelineinSeptember2015.
TheEmergencyMedicineEarlyWarningSystem(EMEWS)ispartofasuiteofNationalClinicalGuidelinesonClinicalDeterioration.Thesuitecurrentlyconsistsof:
NCG No Title Date
NCG No. 1 NationalEarlyWarningScore(NEWS) February2013withclinicalupdateAugust2014Currentlybeingupdated.
NCG No. 4 MaternityEarlyWarningScore(IMEWS) November2014
NCGNo.6 Sepsis Management November2014withNICEaccreditationMar2015
NCG No. 12 Paediatric Early Warning Score system(PEWS)
November2015
Emergency Medicine Early WarningSystem(EMEWS)(Note this was previously known as“Emergency Department Monitoring andClinicalEscalationtoolforadults”)
Prioritised by the NCEC in September2015anddevelopmentsupportedbythisreport.
Further information on the NCEC and National Clinical Guidelines is available at www.health.gov.ie/patient-safety/ncec

AbstractBackgroundChangestophysiologicalparametersprecededeteriorationofillpatients.Earlywarningandtrackandtriggersystems(TTS)useroutinephysiologicalmeasurementswithpre-specifiedthresholdstoidentifydeteriorating patients and trigger appropriate and timely escalation of care. Patients presenting tothe emergency department (ED) are undiagnosed, undifferentiated and of varying acuity, yet theeffectivenessandcost-effectivenessofusingearlywarningsystemsandTTSinthissettingisunclear.
AimTo provide a rapid systematic review of the evidence of the clinical and cost-effectiveness ofphysiologicallybasedearlywarningsystemsandTTSforthedetectionofdeterioration(post-triage)inadultpatientspresentingtoED.
Search methodsA comprehensive search of published and unpublished literature, including scientific databases andgreyliteratureresourceswascarriedout.Notimefilterwasusedbutafiltertoincludeadultpatientswasapplied.Nolanguagefilterwasused,butonlyinformationavailableinEnglishwasincluded.
Selection criteriaParticipants were ED adult patients, post-triage. Only early warning systems and TTS that includedroutinephysiologicalparameterswereincluded.Studieswereclassifiedas:(1)Descriptivestudies–typeandextentofuse; (2)Descriptivestudies–educationalprogrammes; (3)Guidelines; (4)Effectivenessstudies;(5)Developmentand/orvalidationstudies;and(6)Healtheconomicsstudies.
Data collection, analysis and quality assessmentTworeviewersindependentlyscreenedsearchresultsbytitle/abstractandfull-text.Dataextractionwasdonebyonereviewerwithindependentverificationchecksof50%ofrecordsbyasecondreviewer.Tworeviewersconductedqualityassessmentindependently.Dataarepresentedinevidencetables.
Main resultsAtotalof6397citationswereidentified,ofwhich47studies,3guidelinesand1clinicaltrialregistrationform were included. Although early warning systems are increasingly used in ED, compliancevaries. One effectiveness study provided very low quality evidence (assessed using the Grading ofRecommendationsAssessment,DevelopmentandEvaluation(GRADE))thattheuseofanearlywarningsystem in theEDmay lead to a change inpatientmanagementbutdoesnot reduce thenumberofadverseevents;howeverthis isuncertain,consideringthequalityofevidence.Atotalof27differentearlywarningsystemsweredeveloped/validatedin35studies.ThereisrelativelygoodevidenceonthepredictiveabilityofcertainearlywarningsystemsonmortalityandICU/hospitaladmission.Nohealtheconomicstudiesofhealtheconomicdatainclinicalstudieswereidentified.
ConclusionEarlywarningsystemsseemtobeabletopredictadverseoutcomesinadultpatientsofvaryingacuitypresentingtotheED,but there isa lackofhighqualitycomparativestudies toexaminetheeffectofusingearlywarningsystemsonpatientoutcomes.Thisshouldincludeahealtheconomicsassessment.Strategiesforensuringcomplianceshouldbedevelopedandtested.


Table of contents
1. Background ................................................................................................................................ 102. Aim&Objectives ........................................................................................................................ 113. Methods ..................................................................................................................................... 12
3.1 Selectioncriteria .............................................................................................................. 123.1.1Population,Intervention,Comparison,Outcome(PICO) ....................................... 123.1.2Typesofstudies/reports ........................................................................................ 14
3.2 Search methods ............................................................................................................... 153.3 Screeningforinclusion ..................................................................................................... 153.4 Riskofbias/methodologicalqualityassessment .............................................................. 153.5 Dataextraction ................................................................................................................. 163.6 Dataanalysisandsynthesis .............................................................................................. 173.7 Reportingofthereview ................................................................................................... 17
4. Results ........................................................................................................................................ 184.1 Search results ................................................................................................................... 184.2 Riskofbias/methodologicalqualityofincludedreports.................................................. 204.3 Findings ............................................................................................................................ 21
5. Conclusion .................................................................................................................................. 72
References ......................................................................................................................................... 73
AppendicesAppendix 1: Search strategies..........................................................................................................78Appendix 2: Checklists for rapid reviews..........................................................................................90Appendix 3: Risk of bias and quality assessment..............................................................................91

List of abbreviations*Note the difference in the abbreviations for MEWS and I-MEWS
+LR PositiveLikelihoodRatioAa gradient Alveolar to arterial oxygen gradientAAEM AmericanAcademyofEmergencyMedicineACDN Alertandorientated,Confused,Drowsy,NotresponsiveoronlytonailpressureACEM AustralasianCollegeofEmergencyMedicineACEP AmericanCollegeofEmergencyPhysiciansACT AustralianCapitalTerritoryAGREE II AppraisalofGuidelinesforResearch&EvaluationAHRQ AgencyforHealthcareResearchandQualityAMSTAR AssessingtheMethodologicalqualityofSystematicReviewsAPACHE II AcutePhysiologyandChronicHealthEvaluationscoreASEM AustralasianSocietyforEmergencyMedicineASSIST AssessmentScoreforSickpatientIdentificationandStep-upinTreatmentAUROC AreaUndertheReceiverOperatingCurveAVPU Alert,Voice,Pain,UnresponsiveBP Blood PressureBEWS BispebjergEarlyWarningScoreCBA ControlledBefore-and-AfterstudiesCCI CharlsoncomorbidityindexCD CannotbeDeterminedCEM CollegeofEmergencyMedicineCENNZ-NZNO CollegeofEmergencyNurses(NewZealand)CI ConfidenceIntervalCINAHL CumulativeIndextoNursingandAlliedHealthLiteratureCURB-65 Confusion,Urea,Respiratoryrate,Bloodpressure,Age65orolderDIST AnEuclideanDistance-basedScoringSystemEC EmergencyCallECG ElectrocardiogramED EmergencyDepartmentEDWIN EmergencyDepartmentWorkINdexED CIC EDCriticalInstabilityCriteriaEPOC EffectivePracticeandOrganisationofCareESI EmergencyseverityindexESS ProposedEnsemble-BasedScoringSystemeTTS ElectronicallycalculatedTrack&TriggerScoreEuSEM EuropeanSocietyforEmergencyMedicineEWS EarlyWarningScoreFiO2 FractionofinspiredoxygenGCS Glasgow Coma ScaleGIN GuidelinesInternationalNetworkGRADE GradingofRecommendationsAssessment,DevelopmentandEvaluationHDU HighDependencyUnitHEED HealthEconomicEvaluationDatabaseHIQA HealthInformationandQualityAuthorityHR Heart RateHRV HeartRateVariabilityHSE HealthServicesExecutiveIAEM IrishAssociationforEmergencyMedicineICER IncrementalCost-EffectivenessRatios(ICERs)ICTRP InternationalClinicalTrialsRegistryPlatformICU IntensiveCareUnitIFEM InternationalFederationofEmergencyMedicine

IHCA In-HospitalCardiacArrestIMEWS* IrishMaternityEarlyWarningSystemIQR InterquartileRangeNEWS (Ireland) IrishNationalEarlyWarningScoreISBAR Identify,Situation,Background,AssessmentandRecommendationITS InterruptedTimeSeriesdesignsLOC LossOfConsciousnessLODS LogisticOrganDysfunctionSystemMT MedicalTeamMEES MainzEmergencyEvaluationScoreMeSH MedicalSubjectHeadingsMET MedicalEmergencyTeamMEWS* ModifiedEarlyWarningScoreMEWS plus ModifiedEarlyWarmingScoreplusMI MyocardialInfarctionML MachineLearningMEDS Mortality in emergency department sepsisMPM0 II MorbidityProbabilityModelatadmissionmREMS ModifiedRapidEmergencyMedicineScoreMTS ManchesterTriageSystemNCCHTA NationalCoordinatingCentreforHealthTechnologyAssessmentNEDS NationwideEmergencyDepartmentSampleNEWS NationalEarlyWarningScoreNEWS-L NationalEarlyWarningScore+LactateNHS NationalHealthServiceNHSEED NHSEconomicEvaluationDatabaseNICE NationalInstituteforHealthandCareExcellenceNIHR-HTA NationalInstituteforHealthResearch–HealthTechnologyAssessmentNPT Near-Patient-TestNPV NegativePredictiveValueNRCT Non-RandomisedControlledTrialOR OddsRatioOTC Over-The-CounterPACS PatientAcuityCategoryScalePARS PatientAtRiskScorePEDS PrinceofWalesEDScorePEWS PaediatricEarlyWarningSystempH Acidic/basicmeasurePIRO Predisposition,Insult/Infection,Response,andOrgandysfunctionPOTTS PhysiologicalObservationTrackandTriggerSystemPPV PositivePredictiveValuePSI PatientStatusIndexQALYs QualityAdjustedLifeYearsRAPS Rapid Acute Physiology ScoreRCEM RoyalCollegeofEmergencyMedicineRCN RoyalCollegeofNursingRCoP RoyalCollegeOfPhysiciansRCT RandomisedControlledTrialREMS RapidEmergencyMedicineScoreROB RiskOfBiasROC ReceiverOperatingCurveRR RiskRatioRTS RevisedTraumaScoreSAEM SocietyforAcademicEmergencyMedicine

SAPS II NewSimplifiedAcutePhysiologyScoreSBP Systolic Blood PressureSCS Simple Clinical ScoreSD StandardDeviationSIGN ScottishIntercollegiateGuidelinesNetworkSIRS SystemicInflammatoryResponseSyndromeSOFA SequentialOrganFailureAssessmentSOS SepsisinObstetricsScoreSS SepticShockSSSS SevereSepsisandSepticShockscoreTC TraumaCallTemp TemperatureTEWS TriageEarlyWarningScoreTHERM TheResuscitationManagementscoreTIMI ThrombolysisInMyocardialInfarctionTRISS Trauma–InjurySeverityScoreTTS TrackandTriggerSystemUK UnitedKingdomVIEWS VitalPACEarlyWarningScoreVIEWS-L VitalPACEarlyWarningScore-LactateWBC White Blood Cell countWHO WorldHealthOrganisation

List of tablesTable1. RiskofBiasandqualityofevidencecriticalappraisalinstruments ....................................15Table2. Dataextractedfromincludedreports ................................................................................16Table3. Numberandtypesofstudiesincludedinthereview .........................................................20Table4. EvidenceTable:Descriptivestudies-Extentofuse............................................................23Table5. Evidencetable:Descriptivestudies–Compliance .............................................................28Table6. Evidencetable:Guidelines ................................................................................................ 32Table7. EvidenceTable:Effectivenessstudies ................................................................................ 36Table8. Earlywarningsystemsincludedinthereviewbytypeofsystem ..................................... 38Table9. Evidencetable:Developmentandvalidationstudies–ScopingReview ........................... 40Table10. Evidencetable:Developmentandvalidationstudies–Patientgroupsdifferentiated
bytriagecategory.............................................................................................................. 41Table11. Evidencetable:Developmentandvalidationstudies–Patientgroupsdifferentiated
by(suspected)condition ................................................................................................... 51Table12. Evidencetable:Developmentandvalidationstudies–Undifferentiatedpatient
groups .............................................................................................................................. 62
List of figuresFigure 1. Search Results ....................................................................................................................19

10
1 Background
Seriousclinicaladverseeventsarerelatedtophysiologicalabnormalitiesandchanges inphysiologicalparameters suchasbloodpressure,pulse rate, temperature, respiratory rate, levelof consciousness,oftenprecede thedeteriorationof patients.1-4 Early interventionmay improvepatient outcomes andfailure to recognise acutedeterioration inpatientsmay lead to increasedmorbidity andmortality.5,6 Early warning systems and track and trigger systems (TTS) use routine physiologicalmeasurements,which are totalled to generate a score with pre-specified alert thresholds. Their aim is to identifypatientsatriskofdeteriorationearlyandtriggerappropriateandtimelyresponses,knownasescalationofcare.
EarlywarningsystemsareusedincreasinglyinacutecaresettingsandseveralcountrieshavedevelopedNationalEarlyWarningScores(NEWS). In Ireland,theNationalClinicalGuidelineontheuseofNEWSforadultpatientscameintoeffectin2013.7IntheUK,TheRoyalCollegeofPhysicians(RCoP)publisheda National EarlyWarning Score in 2012,8 and the National Institute for Health and Care Excellence(NICE)recommendstheuseofaTTStomonitorhospitalpatients.9InAustralia,theEarlyRecognitionofDeterioratingPatientProgramintroducedaTTSandcorrespondingeducationalprogramme.10 Similarly, intheUSA,RapidResponseSystemswithfixed“CallingCriteria”arerecommendedtotriggeradequatemedical response.11Earlywarningsystemshavealsobeenadaptedtoseveralspecificcontextssuchasmaternity care12-14andpaediatriccare;forexample,theIrishMaternity(I-MEWS)andPaediatricEarlyWarningSystems(PEWS).12, 15
Many acutely ill patients first present to the emergency department (ED). The ED is a unique andcomplex environment, distinctly different from other hospital departments inmanyways. Visits areunscheduled and patients attend with undiagnosed, undifferentiated conditions of varying acuity.Medicalstaffmustcareforseveralpatientssimultaneously,dealwithconstantlyshiftingprioritiesandrespondtomultipledemandsduetotheunpredictablenatureoftheEDenvironment.16,17Initialtriagedeterminesthepriorityofpatients’treatmentsbasedontheseverityoftheircondition,but,followingtriage, continuousmonitoring and prompt recognition of deteriorating patients is crucial to escalatecare and transfer patients appropriately, particularly as there is a high prevalence of acute illness inthe ED. Earlywarning systems are sometimesused as an adjunct to triage for early identificationofdeterioration in theED,particularly in situationsof crowding.18 Common early warning systems such as the Modified Early Warning Score (MEWS)19 are used frequently and validated against specificsubgroupsofpatients(e.g.acuterenalfailure)20butmaynotbedirectlytransferabletoanEDsetting18 wherepatientspresentwithavarietyofunspecifiedconditions.Thereis,therefore,aneedtoreviewtheuse,effectivenessandcost-effectivenessofearlywarningsystemsspecifically inanEDcontext toguidepractice,futureresearchandearlywarningsystemdevelopment.

11
2 Aim and objectives
The aim of this review is to provide a rapid synthesisa of the evidence of the clinical effectivenessand cost-effectiveness of physiologically based early warning systems and TTS for the detection ofdeterioration(post-triage)inadultpatientspresentingtoED.
Theprojectaddressedfivemainobjectives:1. Todescribetheuse internationally, includingthe levelofuseandthevarietyofsystems inuse,
of physiologically based early warning systems or TTS or scoring systems for the detection ofdeteriorationinadultpatientspresentingtotheED;
2. To evaluate the clinical effectiveness of physiologically based early warning systems or TTS orscoringsystemsinadultpatientspresentingtotheED;
3. Todescribethedevelopmentandvalidationofsuchsystems;
4. To evaluate the cost effectiveness, cost impact and resources involved in physiologically basedearlywarningsystemsorTTSorscoringsystemsforthedetectionofdeteriorationinadultpatientspresentingtotheED;
5. Todescribetheeducationprogrammes, includingtheevaluationofsuchprogrammesthathavebeenestablishedtotrainhealthcareprofessionals,andothernon-professionalstaff,inthedeliveryofsuchsystems.
a Arapidreviewhasbeendefinedasasystematicreviewthatislimitedintimeand/orscope;however,thereisnosingledefinitionofthiscapacityandlargevariationexists(31).Thissystematicreviewtookplaceina12weekperiodwithonlyminorrestrictionstothemethodsused.ThemethodsappliedinthisreviewaredescribedfullyinSection3.

12
3 Methods
3.1 Selection criteria
3.1.1 Population, Intervention, Comparison, Outcome (PICO)ThePICOformatwasusedtoinformthesearchstrategyaccordingtothefiveobjectives:
a . To describe the use internationally, including the level of use and the variety of systems in use, of physiologically based early warning systems or TTS or scoring systems for the detection of deterioration in adult patients presenting to Emergency Departments
P Adult patients presenting to the ED following initial triage. (Studies/reports that focussedontriagingpatientsorthatwerenotsetintheED,wereexcluded.)
I Earlywarning systemsorTTSor scoring systems, relyingonperiodicobservationof selected,routinelyrecorded,physiologicalparameters,topromptlyrecognisedeterioratingpatientsandtriggerescalationofcarebasedonpresentresponsecriteria.
C N/A
O ExtentofuseofearlywarningsystemsorTTSorscoringsystems• TypesofearlywarningsystemsorTTSorscoringsystemsinuse• Numberandtypeofclinicalguidelines(regional,national,international)
b. To evaluate the clinical effectiveness of physiologically based early warning systems or TTS or scoring systems in adult patients presenting to the ED
P AdultpatientspresentingtotheEDfollowinginitialtriage.
I Earlywarning systemsorTTSor scoring systems, relyingonperiodicobservationof selected,routinelyrecorded,physiologicalparameters,topromptlyrecognisedeterioratingpatientsandtriggerescalationofcarebasedonpre-setresponsecriteria.
C Non-useofthesystemsortheuseofalternativesystemsofphysiologicalmonitoring.
O Clinical outcomes• Death• Criticalillness(collapse–cardiacorrespiratoryarrest,haemorrhage,sepsisetc.)• Admissiontointensivecareunit(ICU)Lengthofhospitalstay(days)

13
c. To describe the development and validation of such systems
P AdultpatientspresentingtotheEDfollowinginitialtriage.
I Earlywarning systemsorTTSor scoring systems, relyingonperiodicobservationof selected,routinelyrecorded,physiologicalparameters,topromptlyrecognisedeterioratingpatientsandtriggerescalationofcarebasedonpre-setresponsecriteria.
C N/A
O Clinical outcomes• Death
• Criticalillness(collapse–cardiacorrespiratoryarrest,haemorrhage,sepsisetc.)• Admissiontointensivecareunit(ICU)• Lengthofhospitalstay(days)
• SensitivityofearlywarningsystemsorTTSorscoringsystemsforadverseoutcome/criticalillness criterion
• SpecificityofearlywarningsystemsorTTSorscoringsystemsforadverseoutcome/criticalillness criterion
• Positive predictive value of early warning systems or TTS or scoring systems for adverseoutcome/criticalillnesscriterion
• Negative predictive value of earlywarning systems or TTS or scoring systems for adverseoutcome/criticalillnesscriterion
d. To evaluate the cost effectiveness, cost impact and resources involved in physiologically based early warning systems or TTS or scoring systems for the detection of deterioration in adult patients presenting to the ED
P AdultpatientspresentingtotheEDfollowinginitialtriage.
I Earlywarning systemsorTTSor scoring systems, relyingonperiodicobservationof selected,routinelyrecorded,physiologicalparameters,topromptlyrecognisedeterioratingpatientsandtriggerescalationofcarebasedonpre-setresponsecriteria.
C Non-useofthesystemsortheuseofalternativesystemsofphysiologicalmonitoring.
O Economicmeasuresofhealthcare:• UseofhealthcareresourcesassociatedwithearlywarningsystemsorTTSorscoringsystems
useincludingdirectmedicalresourcecosts(stafftime,educationtimeandcost,additionalreferrals), indirectcosts (associatedwith lossofproductivity)andothernon-medicalcosts(e.g.patientoutofpocketexpenses)
• Cost savings, cost effectiveness measures such as Incremental Cost-Effectiveness Ratios(ICERs),QualityAdjustedLifeYears(QALYs).

14
e. To describe the education programmes, including their evaluation that have been established to train healthcare professionals, and other non-professional staff, in the delivery of such systems
P Healthcare professionals using physiologically based earlywarning systems or TTS or scoringsystemsandassociatedescalationprotocolsorcommunicationtoolsinEDsettings.Non-healthcareprofessionalstaffinvolvedinthedeliveryofsuchsystems.
I EducationalprogrammesforhealthcareprofessionalsconcerningsuchearlywarningsystemsorTTSorscoringsystems
C Comparatorsincludednon-useoruseofalternativeeducationalprogrammesconcerningearlywarningsystemsorTTSorscoringsystems
O • Typesofeducationprogrammes• StrategiesandmethodstoevaluateeducationprogrammesofearlywarningsystemsorTTS
or scoring systems
3.1.2 Types of studies/reports Thefollowingsixtypesofstudiesorreportswereincluded:
a. Descriptive studies – types and use of systems: Studies thatdescribed typesor varietyof earlywarningsystemsorTTSorscoringsystemsusedandtheextenttowhichtheywereusedinclinicalpractice.
b. Descriptive studies – education programmes: Studies that described education programmes totrainhealthcareprofessionalsindeliveringearlywarningsystemsorTTSorscoringsystems.
c. Guidelines: Regional,nationalandinternationalguidelinesthatdescribedearlywarningsystemsorTTSorscoringsystems.
d. Effectiveness studies:StudiesthatexaminedtheeffectivenessofanearlywarningsystemorTTSor scoring systemon outcomes for adults admitted to the ED following triage, and that had acontrolleddesign(i.e.,randomisedcontrolledtrials[RCTs],non-randomisedcontrolledtrials[NRCT],controlledbefore-and-afterstudies[CBA],interruptedtimeseriesdesigns[ITS]andcohortstudieswithhistoricalcontrols).Studies thatevaluatedtheeffectsof thesystemonrelevantoutcomeswithoutcontrol(e.g.caseseries,cohortstudieswithouthistoricalcontrol),wereincludedinthedescriptivecategory.
e. Development and validation studies: DevelopmentstudiesweredefinedasstudiesthatfocusedonthedevelopmentofearlywarningsystemsorTTSorscoringsystemswhilevalidationstudiesassessedthepredictiveabilityofsuchsystems.Studies inthiscategoryneededto includeadultpatientsbothwithandwithout the referenceoutcome (suchasadmission to intensive careormortality)orwereotherwiseconsideredadescriptivestudy.Forthepurposeofclassification,weregardedstudiesas‘development’studiesifreferenceranges,parameters,and/ordesignofscoringsystemswereidentifiedbasedontheoutcomesofthestudysample(forexample,throughtheuseof receiveroperatingcharacteristics [ROC] curves). In validation studies, such referencecriteriawerealreadydeterminedandtheirpredictiveabilitywasevaluatedinanewsampleofpatients.
f. Health economics: Fulleconomicevaluationstudies(cost-effectivenessanalysis,cost-utilityanalysisand cost-benefit analysis), cost analysis and comparative resource use studies comparing earlywarningsystemsorTTSorscoringsystemstooneormorestandardtreatments.Thesemayhaveincludedanystudythatmettheeligibilitycriteriaforthereviewofeffectiveness;hencestudiesinothercategoriesmighthavebeenalsobeenincludedhere.

15
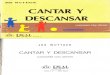
3.2 Search methods Acomprehensivesearchwasconductedforevidenceonearlywarningsystems,TTSorscoringsysteminED,andincludedbothdatabaseandgreyliteraturesearches.Individualsearchstrategiesweredevelopedforfourmajorelectronicdatabases:theCochraneLibrary(alldatabasestherein),OvidMedline,Embaseand CINAHL. Additional resources that were searched included: specific cost-effectiveness resources(n=4),guidanceresources(n=6),professionalbodiesresources(n=22),greyliteratureresources(n=3),andclinicaltrialregistries(n=4).Nolanguagerestrictionswereapplied,butconsideringthiswasarapidreview,notranslationcouldtakeplace.Nofilterwasappliedtothetimeofpublicationofresources.Afilter(freetextterms)wasappliedtolimitretrievaltotheadultpopulationwhereavailable.Fulldetailsof individual search strategies, including the searchdates,areprovided inAppendix1.Detailsof thesearchresultsarepresentedinaPRISMAflowdiagram(Figure1),21 produced in RevMan.22
3.3 Screening for inclusionThreereviewers(FW,PMandSD)screenedthetitles/abstractsfromthedatabasesearchessothateachcitationwasscreenedbyatleasttworeviewersindependently.Foradditionalresources,theinformationspecialist(AC)siftedthesearchresultsforpotentiallyeligiblestudies(seeAppendix1).Fulltextreportsfrom databases and from additional resources were assessed for inclusion, based on the selectioncriteria(section3.1)bytworeviewersindependently(FWandPM)anddiscrepancieswereresolvedbydiscussionand,wherenecessary,byinvolvingathirdperson(DD).
3.4 Risk of bias/methodological quality assessmentTworeviewers(fromFWand/orVSand/orDD) independentlyassessedtheRiskofBias(ROB)and/ormethodologicalqualityoftheincludedreports,usingthecriticalappraisalinstrumentslistedinTable1.
Table 1. RiskofBiasandqualityofevidencecriticalappraisalinstruments
Study design Risk of bias (ROB)/quality assessment tool
Descriptive studies AdaptedfromNationalInstituteofHealthchecklist23
Descriptive studies – educational programmes
AdaptedfromNationalInstituteofHealthchecklist23
Guidelines AGREEIItool24
Effectiveness studies – RCTs
CochraneROBtool25andGRADEqualityofevidenceassessment26
Effectiveness studies – non-RCTs
EPOCqualityassessmentforquantitativestudies25,27andGRADEqualityofevidenceassessment26
Systematic reviews AMSTAR
Economic evaluations BritishMedicalJournalChecklistforauthorsandpeer-reviewersofeconomicsubmission28;Checklistforqualityassessmentineconomicdecision-analyticmodels29
Development and validation studies
QualityAssessmentTooladaptedfromKansagaraetal(2011)30

16
3.5 Data extractionSeparatedataextractionformsweredesignedforeachofthesixtypesofstudiesincludedinthisreview(section3.1.4).Dataextractionwascompletedbytworeviewers(FWandPW).Eachreviewerextracteddatafromhalfoftheincludedreportsand50%ofentrieswerecheckedbyasecondreviewer.ThedataelementsthatwereextractedarepresentedinTable2below.
Table 2.Dataextractedfromincludedreports
Descriptive studies – types and use of systems
Authors,timeandcountryofstudyStudy aim and designNumberofparticipantsandcharacteristicsMethod(s)ofdatacollectionandanalysisContent(parameters)oftheearlywarningsystemorTTSorscoringsystem,andescalationcriteriaFindingsontheuseofearlywarningortrackandtriggersystem(s)
Descriptive studies – education programmes
Authors,timeandcountryofstudyStudy aim and designNumberofparticipantsandcharacteristicsMethod(s)ofdatacollectionandanalysisContent(parameters)oftheearlywarningsystemorTTSorscoringsystem,andescalationcriteriaInformationontheeducationalprogrammeorcommunicationtoolFindingsontheuseofeducationalprogrammeorcommunicationtoolconcerninganearlywarningsystemorTTSorscoringsystem
Guidelines
Guidelineteam(includingqualifications),timeandcountryofguidelineGuideline development strategyScopeKeyrecommendationsImplementationstrategyAudit strategy
Effectiveness studies
Authors,timeandcountryofstudyStudy aim and designNumberofparticipantsandcharacteristicsMethod(s)ofdatacollectionandanalysisIntervention (content (parameters) of the early warning system or TTS or scoring system, andescalationcriteria)andcontrolOutcomesFindings,includingeffectestimates
Development and validation studies
Authors,timeandcountryofstudyStudy aim and designNumberofparticipantsandcharacteristicsMethod(s)ofdatacollectionandanalysisContent(parameters)oftheearlywarningsystemorTTSorscoringsystem,andescalationcriteriaReferencecriteria(outcomes)Findings,includingpredictiveabilitymeasures

17
Health economics
Authors,timeandcountryofstudyStudy aim and designNumberofparticipantsandcharacteristicsMethod(s)ofdatacollectionandanalysisMeasuresofcostOutcomes
3.6 Data analysis and synthesisDatawere collated in evidence tables for eachof the six types of studies included in this review. Inaddition, we provide a concise narrative synthesis of the findings of descriptive studies, descriptivestudies of educational programmes, guidelines, and development and validation studies related toearly warning systems or TTS or scoring systems in ED. For effectiveness studies, a meta-analysiswas plannedbutwas not performeddue to the limitednumber of studies (n=1), hence, a narrativesummary isprovided.Forhealtheconomicsstudies,weplannedtoexaminethecost-effectivenessofusingearlywarningsystemsorTTSorscoringsystemsinED,butnosuchstudieswereidentifiedinthecomprehensivesearchforthisreview.
3.7 Reporting of the reviewNo reporting guidelines for rapid systematic reviews exist at present although one is currently indevelopment(personalcommunicationwithD.Moher,Ottawa).ThereportingchecklistforbriefreviewsbyAbramietal31wascompletedtoensureadequatereporting(Appendix2).

18
4 Results
4.1 Search resultsA total of 6397 citationswere identified (1307 fromdatabases and5090 fromadditional resources).Afterduplicateremoval,1147databasecitationswerescreenedagainsttheselectioncriteriabytitle/abstract.Fulltextsof83reportswereassessedofwhich44reports(43studies)werefinallyincluded.Themostcommonreasonforexclusionwas‘nonEDsetting’(n=24).OnestudyinChinesewasidentifiedand only data from the abstract (in English)was included.32 Nineteen of the 56 screened additionalresourceswereincluded,ofthese14reportsrelatedtothreeclinicalguidelinesandonetoaregisteredtrial.TheresultsofthecompletesearchstrategyarepresentedinFigure1.

19Fi
gure
1. S
earc
h Re
sults
1307
ofrecordsid
entifi
edth
roug
hda
taba
sese
arching:
Cochrane
library(n=3
8)
OvidMed
line(n=3
62)
Emba
se(n
=254
)CINAH
L(n=6
53)
5090
ofa
ddition
alre
cordside
ntifie
dthroug
hothe
rsources:
Costeffe
ctivene
ssre
sources(n=
138)
Guidan
cere
sources(n=
3259
)Professio
nalb
odiesresou
rces(n
=196
)Greyliterature(n
=175
)ClinicalTria
lRegistrie
s(n=
131
6)
Expe
rtsinthefie
ld(n
=4)
Other(n
=2)
56ofa
ddition
alre
cordsd
eemed
poten
tiallyre
levant
aftersifting
:Co
steffe
ctivene
ssre
sources(n=
3)Gu
idan
cere
sources(n=
23)
Professio
nalb
odiesresou
rces(n
=7)
Greyliterature(n
=6)
ClinicalTria
lRegistrie
s(n=
11)
Expe
rtsinthefie
ld(n
=4)
Other(n
=2)
39offull-texta
rticlesexclude
d,with
reason
sNotin
ED(n=2
4)
Cond
ition
-spe
cificto
ol/diagn
ostic
tool(n
=S)
Notaro
utine
assessm
ent(n=
4)
Assessesth
eeff
ectiv
enesso
fanti
bioti
csfo
rsep
sis(n
=1)
Evalua
tesa
carebu
ndleand
areasotherth
anED(n=1
)Notaclin
icalstud
y(n=1
)
1114
7ofre
cordss
cree
ned
83offull-texta
rticlesassessedfor
eligibility
43stud
ies(44
repo
rts)-+
-Sadd
ition
alre
cords(19
repo
rts)
includ
edin
qua
litati
vesy
nthe
sis(Totaln=5
1)
Descrip
tivestud
ies(n=
10)
Guidelines(n
=3)
Effectiv
enesss
tudies(n
=1)
Developm
ent/Va
lidati
onstud
ies(n=
36)
Healthecono
micstud
ies(n=
0)
Clinicaltrialregistratio
n(n=1
)
0ofstud
iesinclude
dinqua
ntitativ
esynthe
sis(m
eta-an
alysis)
160du
plicates
rem
oved
1064
records
excl
uded
56add
ition
alre
cordsa
ssessedfore
ligibility 37add
ition
al
reco
rds
excl
uded
, w
ith re
ason
s

20
Thenumberofincludedstudies/reportsbytypeofstudy/report(asspecifiedinsection3.1)ispresentedin Table3below.
Table 3.Numberandtypesofstudiesincludedinthereview
Type of study/report n
Descriptivestudies–type,extentofuseandcomplianceanduseofsystems(Note: 2 study sub-types (extent of use and compliance) emerged and arepresentedseparatelyintables4and5below)
10
Descriptivestudies–educationalprogrammes 0
Guidelines(andrelateddocuments) 3
Effectivenessstudies 1
Validation&Developmentstudies 35(+1review)
Health economics studies 0
4.2 Risk of bias and methodological quality of included reportsTheriskofbiasandqualityassessmentoftheincludedreportsispresentedinAppendix3.Detailsofthecriticalappraisalinstrumentsusedareoutlinedintable1above.
Weexaminedthequalityofsixdescriptivestudiesthatexaminedtheextentofearlywarningsystem(s)use. One report was a conference abstract and was rated of poor quality because only limitedinformationwasreportedforqualityassessment.33Theremainingfivestudieswereoffairquality.34-37
The fourdescriptivestudiesassessingcompliancewithusingearlywarning systemswereofgood38-40 andfairquality.41
Oneeffectivenessstudyinthereviewwasratedashighriskofbiasoverall.Shuk-Ngoretal42 included anon-randomsampleanddidnotprovidesufficientinformationtoassessallocationbiasandsimilarityin baseline characteristics between the two groups. Using the GRADE system for grading evidence,thequalityofevidenceof this studywasvery lowfor theeffectofusingMEWScomparedtoclinicaljudgementonachangeinEDpatientmanagementandadverseevents.Thiswasbecausethestudyhadahighriskofbiasandconsideredalownumberoffewevents.
Eight studies that developed and validated a system (in the same sample)were rated as having low(n=6)andunclear (n=2)riskofbias.The27studiesthatvalidatedanexistingsysteminanewcohortofpeoplewerejudgedashavinglow(n=16),unclear(n=8)andhighriskofbias(n=3).43-45 Studies with unclearriskofbiasgenerallydidnotspecifythemethodsofsampling(n=9),didnotstatecut-offvaluesused(n=12)ordidnotpre-specifytheoutcomesclearly(n=1).Onescopingreviewofpredictiveabilityofearlywarningsystems46wasratedofgoodquality.
The three included guidelines were assessed using the AGREE II tool and scores given by the tworeviewers independently were averaged for each domain. The Irish National Early Warning ScoreGuidelineandtheguidelineoftheNationalInstituteforHealthandCareExcellencewereratedofhighqualitywiththepercentagescoresforthesixdomainsvaryingbetween91.7-97.2%and87.5-100%respectively,andtheoverallqualityscoregivenbythereviewerswas91.7%forbothguidelines.7,9Theguideline produced by the Royal College of Physicianswas rated lower in quality (range 62.5-100%;overallquality66.7%)mainlybecauseoflimitedinformationavailableabouttheirsearchstrategyand

21
noclearstatementofhowrecommendationswerederivedfromevidence.Theyciteasystematicreviewas source of their evidence but the scope of the guidelinewas broader than that addressed in thisreview.8
4.3 FindingsThefindingsofthisreviewarestructuredbytypeofstudy.
4.3.1 Descriptive studies – Type, extent of use, and complianceTen descriptive studies were included of which six examined the extent of using early warningsystems33-37, 47 and four examined compliance with such systems38-41 One report was a conferenceabstractinwhichanearlywarningsystemwasdescribedbutlimiteddatawereavailable.33
ExtentofuseSixreportspublishedinthelastsixyearsdescribedtheuseofearlywarningsystemswithintheED(SeeTable4Evidencetablebelow).Thereportscollecteddatafrommedicalrecords,34, 35 a survey,36aweb-survey,47aprospectiveobservationalcohortstudy37,andthroughparticipatoryactionresearch.33Onereportwas a conference abstract inwhich the authors refer to a newmonitoring system to identifytheneedforescalationofcare,butthesystemwasnotdescribedfully intheabstract.33 Considine et al 34describedapilotstudyinahospitalinAustraliaexaminingtheuseofanearlywarningsystemthatconsideredcriteriarelatedtoapatients’airway,circulation,disabilityandanysuddendeterioration.Theescalationprotocolconsistedofareviewofthepatientbyanemergencyphysicianwithinfiveminutesifanyofthecriteriaweremet,followedwithadditionalinterventions,ifappropriate.AnationalsurveyinsevenjurisdictionsinAustralia,foundthat20of220hospitalshadaformalrapidresponsesystemintheED,buttheprevalenceofearlywarningsystemsinEDswasnotreported.47Wedidnotfindanyotherstudiesreportinganyaspectsoftheescalationprotocols.
Wilson et al 37 included the parameters heart rate (HR), blood pressure, respiratory rate, peripheraloxygen saturation, temperature and theGlasgowComa Scale (GCS) in their TTS hospital chart. Theycompared the TTS scores recorded in the charts with scores calculated retrospectively and foundthat 20.6% (n=211)were incorrect. Thiswasmainlybecauseof incorrect assignmentof the score toan individualvital sign,which led tounderscoringof the totalTTSand reducedescalationactivation.Correia et al 35didnotprovidedetailsonthecontentoftheearlywarningsystemtheyusedinasmallstudy(n=69)inPortugal,butfoundthatathresholdofascore≥3wouldhaveincreasedearlymedicalattentionby40%comparedtoclinical judgementalone.Asurveyin2012of145(57%responserate)clinicalleadsofEDsintheUKshowedthat71%usedanearlywarningsystem,withtheModifiedEarlyWarningScore(MEWS)beingthemostcommonsystemused(80%).
Insummary,multipleearlywarningsystemsareavailableandtheextentoftheiruseintheEDmayvarygeographicallybutlimiteddataprecludescomparisonsbetweencountries.Someevidencesuggeststhatincorrectcalculationorrecordingofscoresmayleadtoinappropriateescalationactivationoralackofsuchactivation,drawingattentiontotheimportanceofadequateimplementationofsuchsystems.
ComplianceThree retrospective studies38-40 and one audit41 conducted in the UK, Denmark, the USA and NewZealand in the last five years examined compliancewith recording earlywarning systemparametersand escalationof care (See Table 5 Evidence table below). The vital signparameters included in theearlywarningsystemwererespiratoryrate,HR,systolicbloodpressure(SBP),temperatureandlevelofconsciousness(LOC)foronestudybyChristensenetal38.AnotherstudybyHudsonetal41 also included urinary output, pain scores and the presence of recurrent/prolonged seizures or uncontrollable/

22
newpain, in addition to the vital signparameters.Austenet al 40 included urine output and oxygen saturationsaswellasthevitalsignparameters.Christensenetal38reportedarateof7%(22/300)ofcalculatedscoresintheclinicalnotes;however,16%ofrecordsincludedallfivevitalsigns,andHR,SBP,andLOCwerereportedin90-95%ofrecords.Compliancewithescalationofcarevaried;allninepatientsthatmetthetraumacallactivationcriteria(immediatelylife-threateningsigns/symptomsorBEWS≥5)hadtriggeredatraumacall,butonly24ofthe48emergencycallactivationcriteria(immediatelylife-threateningsigns/symptomsorBEWS≥5)hadbeenresponded tobyanemergencycall.Austenetal40 foundamuchhighercompliancewith66%ofrecordscontaininganaggregatescore,althoughonly72.6%of thesewereaccurate. Inanaudit, thepre-implementation rate (30%)ofabnormalvital signidentificationwassignificantlylowerthanthepost-implementation(53.5%)rate(p=0.007)andpatientswere less likely to receivemedication (p=0.001), but no details of the implementation strategy theyusedweredescribed.41
Insummary,fourstudiesexaminedcomplianceandthefactorsaffectingmonitoringvitalsignsinanEDsetting.Compliancewith recordingand responding toearlywarning systemsappeared relatively lowalthoughthisvariedacrosstheincludedstudies.Therateofvitalsignmonitoringforsomebutnotallindividualvitalsignswashigh.ThefrequencyofrecordingofHRandBPwereparticularlyhigh,butthefrequencyofrecordingoftemperature(65.0%-96.8%)andrespiratoryrate(18.0%-98.9%)variedacrossthe included studies. While certain factors, including patients’ triage category, age, and number ofmedicationsseemto increasefrequencyofvitalsignmonitoring, italsoappearsthatcrowdingattheED,increasedlengthoftimeintheEDandadecreasednumberofroutesofmedicationadministrationmay lead to reduced monitoring.39

23Ta
ble
4.Evide
nceTable:Descriptiv
estud
ies-Exten
tofu
se(M
etho
dologicalq
ualitywasrated
usin
gan
ada
pted
Nati
onalInstituteofH
ealth
che
cklist.23
Fulld
etails
ofthe
metho
dologicala
ssessm
entare
availableinApp
endix3.)
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/
tool
Resu
lts
Aust
ralia
n Co
mm
issio
n on
Safety
andQua
lity
in H
ealth
Ca
re(2
011),47
Au
stra
lia
Qua
lity
Ratin
g: F
air
Todescribe
recogn
ition
and
re
spon
se sy
stem
s in
Aust
ralia
n ho
spita
ls.
Web
-based
Su
rvey
Publicand
priv
ate
hospita
lsin7Australian
jurisdicti
onsb
etwee
nSeptand
Dec201
0.227
no
min
ees w
ere
prov
ided
to
the
Com
miss
ion,
and
18
2(rep
resenti
ng220
ho
spita
ls;143
pub
licand
77
priv
ate)ofthe
se(8
0%)
com
plet
ed th
e su
rvey
.
Exam
inesexten
tof
useofsy
stem
s.(N
ode
tails
pro
vide
d on
individu
alsy
stem
s.)
Syst
ems f
or re
cogn
isin
g cl
inic
al d
eter
iora
tion
•77
%had
writt
enpolicies,protocolo
rguide
lines
regardingthemea
suremen
tofp
hysio
logical
observati
ons(%fo
rEDno
tstated)
•77
%had
afo
rmalescalati
onprotocol(ofwhich45%
ha
dagrad
edre
spon
se)
•35
%usedform
alearlywarning
system
orT
TS(o
fwhich58%
weresin
gleorm
ultip
leparam
eter
system
s,10%
aTTSth
atre
quire
dscorecalculati
on,
and26
%usedacombine
dsystem
).•50
%usedastructured
protocolo
rtoo
lforhan
dover
commun
icati
ons(common
toolsw
ereSB
AR(3
4%)
ISOBA
R(33%
)and
ISBA
R(21%
)).
Syst
ems f
or re
spon
ding
to d
eter
iora
tion
•66
%had
afo
rmalra
pidrespon
sesy
stem
(larger
hosp
itals
and
thos
e in
met
ropo
litan
are
as w
ere
mor
e likelytohavethesesystem
s),o
fwhich24%
(n=2
0)
wereinED
•In100
%ofh
ospitals,nurseso
nthewardcouldcall
the
rapi
d re
spon
se sy
stem
. Doc
tors
on
call
in c
ould
calltherapidrespon
sesy
stem
in89%
ofh
ospitals,
othe
rhospitalstaffin69%
,and
families,p
atien
tsand
carersin
18%
ofh
ospitals.
Org
anis
ation
al sy
stem
s to
supp
ort t
he re
cogn
ition
of
and
resp
onse
to d
eter
iora
tion
•70
%had
iden
tified
staff
inth
eirh
ospitalswith
prim
aryrespon
sibilityfo
rdevelop
ing,im
plem
entin
g,
sustaining
and
mon
itorin
grecogn
ition
and
respon
se
syst
ems
•6%
had
bee
nallocatedspecificfund
ingforthe
op
erati
onofthe
irrapidrespon
sesy
stem

24Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
Setti
ng &
Par
ticip
ants
Cont
ent o
f sys
tem
/to
olRe
sults
•72
%had
acom
mittee
thatoversaw
theop
erati
onof
thes
e sy
stem
s•69
%provide
dregu
lartrainingan
ded
ucati
onto
supp
ortstaff
•48
%collected
specificda
taabo
utth
eeff
ectiv
eness
ofth
eirrecog
nitio
nan
drespon
sesy
stem
sCo
nsid
ine
et
al(2
012),34
Au
stra
lia
Qua
lity
Ratin
g:Fair
Evalua
teth
eup
take
ofEDEarly
Warning
Scoreforrecog
nitio
nofand
respon
seto
clinicaldeterioratio
n.
Pilo
t De
scrip
tive
expl
orat
ory
stud
y
300-be
durba
ndistric
tho
spita
l.System
atic
sampleof204
pati
ents
forw
homEDEW
Sha
dbe
enacti
vated(every
10thpati
entinED
EWS
logbo
okover2
4mon
ths
perio
d).
Criti
cal i
nsta
bilit
y cr
iteria
•Airw
ay/breathing
:St
ridor
, upp
er
airw
ayobstructio
n,
or th
reat
ened
airw
ay,SpO
2<
90%,A
rterialb
lood
gasesp
H<7.20
,Re
spira
toryra
te<
10or>
30breaths/
min
•Circulati
on:H
eart
rate<50or>120
be
ats/min,SBP
<
90or>
200
mmHg
,Urin
eou
tput<20
or<100
mL/6h
•Disability:Sud
den
decr
ease
in
cons
ciou
snes
s (fa
llinGCS
score
>2),R
epeatedor
prol
onge
d se
izure
s •Worrie
d?:P
atien
ts
who
may
not
mee
t ab
ovecrite
riabut
have
a su
dden
de
terio
ratio
n,
requ
iring
urgen
tm
edic
al re
view
.
•20
4pa
tients(ofwhich16pa
tients<
16yea
rs)
•Nursesm
ade93
.1%ofE
DEW
Sactiv
ation
s.
•Mostcom
mon
reason
sforEDEW
Sactiv
ation
were:
respira
tory(2
5%)a
ndcardiac(2
2.5%
)(Hy
potension
(27.7%
)and
tachycardia(23.7%
)weremostcom
mon
reason
sforEDEW
Sactiv
ation
.)•82
.4%ofp
atien
tswereseen
bymed
icalstaff
before
EDEWSactiv
ation
.•Med
iandu
ratio
nofclin
icalin
stab
ilitywas39minutes
(IQR,5–129
minutes).
•Med
iantim
ebe
twee
ndo
cumen
tingph
ysiological
abno
rmalitiesand
EDEW
Sactiv
ation
was5m
inutes
(rang
e0–20
).•Mostp
atien
ts(5
7.8%
)req
uiredho
spita
ladm
ission:
4.4%
ofp
atien
tsre
quire
dICUadm
ission.

25
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/
tool
Resu
lts
Corr
eia
et
al(2
014),35
Po
rtug
al
Qua
lity
Ratin
g:Fair
Toassessthe
Early
Warning
Score(E
WS)
insp
ecifictim
ew
indo
ws p
rece
ding
an
acu
te e
vent
, to
stud
y its
tem
pora
l be
haviou
rand
its
relatio
ntooutcomes,
to c
ompa
re it
with
establish
edward
care
.
Retrospe
ctive
coho
rtFirstcon
secutiv
e10
0ad
ultw
ardpa
tients
assis
tedbyth
eou
trea
ch
team
and
tran
sferredto
EDfrom
1Ja
nto31Ap
ril
2009
.
EWS:param
eters
notc
learlysp
ecified
.Scorethresholdof>3
as tr
igge
r.
n=65
(65%
ofe
ligiblesa
mple)
•Maincauseofdeterioratio
n:Respiratoryproblem
s(44.6%
);cardiovascular(2
7.7%
)and
neu
rological
deterio
ratio
n(27.7%
).•EW
Sscoreatth
reepe
riodspreceding
wardtran
sfer
toth
eED
(EWSMea
n/SD
): 72h:2.6±1.9
24h:2.4±1.8
12h:3.8±1.7
•Scoreat24h
and
12h
seem
edto
predictboth
leng
thofstayan
dmortality(p<0.05).
•63
%weread
mitted
inIC
UorIntermed
iateCare
Units*(26%
and
37%
,respe
ctively),20
%re
turned
toth
eiro
riginwards,and
17%
diedinth
eED
.The
overallin-ho
spita
lmortality=53
.8%
•Th
eEW
Swou
ldhaveincrea
sedea
rlym
edical
atten
tionby40%
ifath
resholdof≥3wasused.
*Th
isstud
yde
scrib
es3levelsofcare(returntoward,
admiss
iontoIn
tensiveorIn
term
ediateUnits)
Coug
hlan
et
al(2
015),33
Ire
land
(Con
ference
abstract)
Qua
lity
Ratin
g:Poo
r
Toprovide
a
nove
l lon
gitu
dina
l m
onito
ring
syst
em
tailo
redtoid
entifyan
escalatio
nprotocol
inED
Participa
tory
Actio
nRe
sear
ch
NR
Describ
esanew
system
(see
results)
Mon
itorin
gan
drespon
sesy
stem
includ
es:
a)M
onito
ringchartforadu
ltpa
tients
b)Stand
ardisedap
proa
chto
mon
itorin
g&
reassessmen
tofp
atien
tsafte
rtria
geunti
lmed
ical
asse
ssm
ent
c)IS
BARtool
d)Tem
plateforp
atien
tspe
cificm
onito
ringplan
e)Tem
platefore
scalati
onprotocol

26Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
Setti
ng &
Par
ticip
ants
Cont
ent o
f sys
tem
/to
olRe
sults
Griffi
thse
tal
(201
2),36UK
Qua
lity
Ratin
g:Fair
Toassessthe
use
ofearlywarning
system
sinUK
EDsa
ndwhe
ther
the
resp
onde
nt
supp
ortedtheuseof
early
war
ning
syst
ems
inth
eED
.
Surv
ey
254ad
ultE
Dclinicallead
sExam
inesexten
tof
useofsy
stem
s.(N
ode
tails
pro
vide
d on
individu
alsy
stem
s.)
Respon
sera
te=57%
(145
/254
).Ofthe
145
,87%
used
anearlywarning
system
.•71%
usedea
rlywarning
sy
stem
s to
trig
ger s
enio
r rev
iew
. •Type
sofe
arlywarning
system
sused:80%
MEW
S,
10%PAR
S,10%
other(M
EWS&PAR
Sarebo
th
aggregatescores)
•In76%
pati
entswith
highscoresarecared
forw
ith
incr
ease
d m
onito
ring.
•In44%
increa
sedscorestriggeredcriticalcareinpu
t.•93
%ofclin
icallead
ssup
ported
theuseofearly
warning
system
sinED
.•Discha
rgeofpati
entswith
highscores:con
sulta
nt
review
(32%
),ad
mitted
(22%
),no
seniorre
view
(23%
),othe
r(17
%),no
answer(6
%).
Wils
on e
t al
(201
3),37UK
Qua
lity
Ratin
g:Fair
Toevaluatethe
utilisati
onofp
aper
basedTrackan
dTrigger(TT
S)cha
rts
inaUKem
ergency
depa
rtm
ent.
Prospe
ctive
observati
onal
coho
rt
472ad
ults(o
ver1
8years)
enterin
gon
eofth
ree
clinicalareasofthe
ED
(resuscitatio
nroom
,‘m
ajors’,ob
servati
on
ward)
Vita
l sig
n an
d TT
S da
ta: P
aram
eter
s:
Heartrate(HR),
syst
olic
and
dia
stol
ic
bloo
dpressure(B
P),
resp
irato
ry ra
te,
perip
hera
l oxy
gen
saturatio
n(SpO
2),
tem
pera
ture
and
Gl
asgo
w C
oma
Scal
e (GCS
)score.
Com
pleti
on o
f obs
erva
tions
85
.8%had
≥1seto
fobservatio
nsdocum
entedto
theCo
llegeofE
mergencyMed
icine(CEM
)stand
ard
ofsixpa
rameters(HR
,respiratoryra
te,B
Pan
dSp
O2,
tempe
rature,G
CS).
Com
pleti
on o
f TTS
scor
es
60.6%had
≥1TT
Sscoredo
cumen
tedinED
34.5%ofo
bservatio
nscon
tained
aTTSsc
ore,ofw
hich
20.6%(2
11)w
ereincorrect(79
.1%ofthe
incorrect
TTStotalswereun
derscored,poten
tiallypreventi
ng
atriggere
ventfrom
being
recogn
ised;93.4%
of
theerrorscan
besolelyattrib
uted
toth
eincorrect
assig
nmen
tofthe
scoretoanindividu
alvita
lsign;
incorrecta
ddition
ofind
ividua
lTTSsc
oresoccurredin
2.8%
ofe
rrors).
Esca
latio
ns
≥1escalati
on:2
04(e
scalati
onatE
Darriv
al(n
=163
with
red/oran
getriage),ofwhich37ha
d2nd
escalati
on;
escalatio
naft
erarrival(n
=41),o
fwhich9had
2nd
escalatio
n).

27
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/
tool
Resu
lts
Com
pleti
on o
f pap
er T
TS c
hart
s (‘R
eal T
TS’)
TTSscoreexceed
ingalertin
gthreshold:
Escalatio
n(n=2
9);N
oescalatio
n(n=2
2)
TTSscoreno
texcee
ding
alerting
threshold:
Escalatio
n(n=9
4);N
oescalatio
n(n=1
41)
TTSscoresnotcalculated:
Escalatio
n(n=8
1);N
oescalatio
n(n=1
05)
Retr
ospe
ctive
TTS
com
pleti
on (‘
Pote
ntial
TTS
’) TT
Sscoreexceed
ingalertin
gthreshold:
Escalatio
n(n=1
10);Noescalatio
n(n=8
0)TTSsc
oreno
texceed
ingalertin
gthreshold:
Escalatio
n(n=9
4);N
oescalatio
n(n=1
88)

28Ta
ble
5. Evide
ncetable:Descriptiv
estud
ies–
Com
pliance
(Metho
dologicalq
ualitywasrated
usin
gan
ada
pted
Nati
onalIn
stituteofHe
althche
cklist23
.Fulld
etails
ofthe
metho
dologicala
ssessm
entare
availableinApp
endix3.)
Auth
ors (
year
), co
untry
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/t
ool
Resu
lts
Aust
en e
t al
(201
2),U
K
Qua
lity
Ratin
g:Goo
d
Toassessthe
degree
ofadh
eren
ceto
the
ChelseaEarly
Warning
Score(CEW
S).
Retrospe
ctive
char
t rev
iew
94con
venien
tlysa
mpled
pa
tientre
cords(on
ly
EDdatainclud
edin
this
review
).
CEW
SPa
ram
eter
s:Respiratory
rate,o
xygensaturatio
ns,
tempe
rature,SBP,H
R,LO
C(AVP
U),urineou
tput
% o
f pati
ents
in w
hom
par
amet
er w
as
reco
rded
:•Tempe
rature:9
6.8%
•HR
:100
%•Bloo
dpressure:1
00%
•Re
spira
toryra
te:9
8.9%
•Oxygensaturatio
ns:9
7.9%
•AV
PU:9
6.8%
•Urin
eou
tput:4
7.9%
% o
f pati
ent w
ith a
ggre
gate
CEW
S re
cord
ed:
66.0%(6
2/94
)
% o
f pati
ent w
ith a
ggre
gate
CEW
S co
rrec
tly
calc
ulat
ed:7
2.6%
(45/62
)Re
sulte
din10pa
tientsforwho
mcarewasnot
escalatedbu
tsho
uldha
ve.
Chris
tens
en
etal(20
11),38
De
nmar
k
Qua
lity
Ratin
g:Goo
d
Exam
inewhe
therth
eBispeb
jergEWS(BEW
S)
tria
ge sy
stem
is u
sed
system
aticallyand
correctly
inam
ixed
ED
popu
latio
n.
Retrospe
ctive
crosss
ectio
nal
anal
ysis
600-be
durba
nteaching
ho
spita
l.30
0rand
omly
selected
‘red
’(most
severelyill/injured
)catego
rypati
entsover
a6mon
thperiodin
2009
(=1/9ofto
tal‘red’
popu
latio
ndu
ringstud
ype
riod).
BEWS:Score0-3on5
vitalsigns:R
esprate,H
R,
SBP,Te
mp,LO
C.BEW
S≥
5activ
ated
emergencyor
trau
ma
call
•BE
WScalculated
innotes:7
%(n
=22/30
0)
•HR
,BP,LO
Cdo
cumen
tedin90-95
%ofcases;
tempin65%
ofcases;R
espiratoryra
tein
18
%ofcases.
•All5vita
lsignsdocum
entedin16.0%
of
case
s.•Trau
maCa
ll(TC)acti
vatio
ncrite
rion(n=9
);in
allthe
secasesaTCwasacti
vated.
•Em
ergencycall(EC)ECactiv
ation
criterion
(n=4
8),b
utanEC
wasonlyactiv
ated
in
24pati
ents.A
mon
gthe24
pati
entsfo
rwho
manEC
had
notbee
nactiv
ated
,eight
hada“prim
arycrite
rion”(life
-threatening
sig
ns/sym
ptom
s)and
16pa
tientsh
ada
retrospe
ctiveBEW
S≥5.

29
Auth
ors (
year
), co
untry
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/t
ool
Resu
lts
Huds
on e
t al
(201
5),41
New
Zealan
d
Qua
lity
Ratin
g:Fair
Tostan
dardise
an
emergencyob
servati
on
char
t, th
e Ad
ult
EmergencyDe
partmen
tFl
ow C
hart
, whi
ch
inco
rpor
ates
ele
men
ts
desig
ned
to a
llow
cl
inic
ians
to m
ore
read
ily re
cogn
ise
thetren
dsofp
atien
tde
terio
ratio
n.
Audi
t18
1 m
edic
al re
cord
s,
rand
omly
sele
cted
from
twometropo
litan
ho
spita
ls:
•80
duringthepre-
implem
entatio
nau
dit
•10
1du
ringthepo
st-
implem
entatio
nau
dit.
AdultE
mergency
Depa
rtm
ent
Flow
Cha
rt:P
aram
eter
s:
SBP,
pul
se ra
te, r
espi
rato
ry
rate
, urin
ary
outp
ut,
painsc
ore,new
/cha
nge/
uncontrollablepa
in,
Glas
gow
Com
a Sc
ore,
Re
curren
t/Prolon
ged
Seizu
res,O
2 saturatio
n
•Patie
ntsa
tthe
pre-im
plem
entatio
nau
dit
werelesslikelyto
beiden
tified
ash
avingan
ab
norm
alvita
lsignwhe
ncompa
redtoth
ose
atth
epo
st-im
plem
entatio
nau
dit(30
%pre,
53.5%post;Ch
isqu
are=14
.261
,p=0.007
).•Timetakenfrom
triageto
iden
tificatio
nofin
dividu
alabn
ormalvita
lsigns:n
odiffe
rences(p
-value
sran
gefrom
0.2to
0.5).
•Timetakenfrom
iden
tificatio
nofan
abno
rmalvita
lsigntoitss
ubsequ
ent
man
agem
ent:sligh
tlylo
ngeratthe
pre-im
plem
entatio
nau
dit(Mea
n=40
minutes,SD=57
minutes)tha
natth
epo
st-
implem
entatio
nau
dit(Mea
n=30
minutes,
SD=44minutes),bu
tnostati
stically
significan
tdifferen
ce.
•Do
cumen
tatio
nofam
edicalofficer
beinginatte
ndan
ce:Low
eratthe
pre-
implem
entatio
nau
dit(Mea
n=0.2,SD=
0.5)th
anatthe
post-implem
entatio
nau
dit
(Mea
n=0.5,SD=0.7;t=2.6,p=0.01).
•Patie
ntsa
tthe
pre-im
plem
entatio
nau
dit
werelesslikelyto
receivemed
icati
onto
man
agetheira
bnormalvita
lsign(Pre:M
ean
=0.2,SD=0.4;Post:Mea
n=0.4,SD=0.6;t
=3.3,p=0.001
).

30Au
thor
s (ye
ar),
coun
trySt
udy
aim
Stud
y de
sign
Setti
ng &
Par
ticip
ants
Cont
ent o
f sys
tem
/too
lRe
sults
John
sonetal
(201
4),39USA
Qua
lity
Ratin
g:Goo
d
(1)W
hata
reth
epe
rson
alhea
lthfa
ctors
(num
bero
fprescrip
tion
med
icati
ons,num
ber
ofOTC
med
icati
ons,
comorbiditie
s,
age,
gen
der,
tria
ge
catego
ry)tha
taffe
ct
thefreq
uencyof
vita
l sig
n m
onito
ring
in th
e em
erge
ncy
depa
rtmen
t?(2
)Wha
tsocialfa
ctors(insurance
status,ethnicity)
affectthe
freq
uencyof
vita
l sig
n m
onito
ring
in th
e em
erge
ncy
depa
rtmen
t?(3
)Doe
stheeff
ecto
fpersona
lfactorso
nthefreq
uency
ofvita
lsignmon
itorin
gin
the
emer
genc
y de
part
men
t cha
nge
whe
n en
viro
nmen
tal
factors(familypresence,
crow
ding
leve
l, le
ngth
ofstay,n
umbe
rof
routesofm
edicati
ons
adm
inist
ered
in
emergencyde
partmen
t)
are
take
n in
to a
ccou
nt?
Descrip
tive,
retrospe
ctive
char
t rev
iew
Selected
165
cha
rtsfrom
apo
ssible3,727
subjects
from
thecrow
dedpe
riods
EmergencyDe
partmen
tWorkInde
x(EDW
IN≥2)
and60
ofa
possib
le
73su
bjectsfrom
non
-crow
dedpe
riods(E
DWIN
<2),fora
totalo
f225
re
view
ed c
hart
s.
Asse
ssm
ent o
f im
pact
of
follo
win
g fa
ctor
s on
vita
l sig
n m
onito
ring
freq
uenc
y:
Person
alhea
lthfa
ctors
No.ofp
rescrip
tion
med
icati
ons
No.ofO
TCm
edicati
ons
No.ofcom
orbiditie
s Ag
e Ge
nder
Triagecategory
Socialfa
ctors
Ethn
icity
Insurance
Environm
entalfactors
ED
WIN(m
easureof
crow
ding
) Leng
thofstay
Fam
ily p
rese
nce
Routesofm
edicati
on
Influ
ence
of p
erso
nal h
ealth
fact
ors
•Num
bero
fprescrip
tionmed
icati
ons
(p<0
.01),com
orbiditie
s,age(p
<0.01),
gend
er(p
<0.05),and
triagecategory
(p<0
.001
)had
sign
ificantcorrelatio
nwith
thefreq
uencyofvita
lsignmon
itorin
g.
•Strong
estp
redictorofthe
freq
uencyofvita
lsig
nmon
itorin
g:triagecategory(t=2.1,P
=
0.04
).•Triagecategoryha
dthegreatestim
pact
onth
etim
ebe
twee
nvitalsigns.(For
everyincrea
seof1
inth
etriagecategory
(becom
inglessacute),thetim
ebe
twee
nvitalsignswasin
crea
sedby34minutes.)
Influ
ence
of s
ocia
l fac
tors
Non
ecorrelated
with
thefreq
uencyofvita
lsig
n m
onito
ring.
Influ
ence
of e
nviro
nmen
tal f
acto
rsCrow
ding
level(t=
2.3,P
=0.02),len
gthofstay
(t=2.7,P
=0.008
),an
dnu
mbe
rofrou
teso
fmed
icati
ons(t=
–2.5,P=0.02)werefoun
dto
besign
ificantpredicators.A
sthe
EDW
INsc
ore
increa
sedby1,the
leng
thofti
mebe
twee
nrecordingvitalsignsin
crea
sedby1.5m
inutes.

31
4.3.2 Descriptive studies – Educational programmesWe did not identify any studies that described educational programmes related to early warningsystemsorTTS,althoughthethreeguidelinesincludedinthereviewcontainaneducationaltool(seesection4.2.3).
4.3.3 GuidelinesThreeclinicalguidelineswereidentified;onefromIreland7andtwofromtheUK,8,9publishedbetween2007and2013(SeeTable6Evidencetablebelow).NonewerespecifictoanEDsetting;allthreeapplyto all acutely ill adult patients, but do not specifically exclude ED. The Irish National EarlyWarningScore(IrishNCGNo.1NEWS)7andtheNEWSguidelineoftheUKRoyalCollegeofPhysicians(RCoP)8 both include appended observation charts using a colour system to trigger escalation of carewhenappropriate,whereas theUKNational Institute forHealthandCareExcellenceguideline (NICECG50)recommendtheuseofaTTSbutdonotprovideanexemplarchart.9
Allthreeguidelinesrecommendthesamesixparameterstobemeasured:respiratoryrate,heartrate,systolicbloodpressure,temperature,oxygensaturations,andlevelofconsciousness.TheIrishNCGNo.1NEWSalsotakesintoaccountifapatientisoninspiredoxygen(FiO2)andtheNICEguidelineincludesastatementonadditionalparameterssuchasurineoutputincertaincircumstances.
Eachguidelineisaccompaniedbyaneducationaltool.TheIrishNCGNo.1NEWSguidelineadaptedtheCOMPASSeducationalprogram(HealthDirectorateACTGovernment,Australia) for Irishuse,and theNICEandRCoPguidelinesdevelopedonline learning tools.Only the IrishNCGNo.1NEWSandNICEguidelinesprovideaclearauditstrategyforimplementationoftheguideline.
Insummary,currentguidelinesonearlywarningsystemsformonitoringacutepatientsarenotspecifictotheEDcontext.Commonparametersacrossexistingguidelines includerespiratoryrate,heartrate,systolicbloodpressure,temperature,oxygensaturations,andlevelofconsciousness.

32Ta
ble
6. Evide
ncetable:Guide
lines
(Metho
dologicalq
ualitywasra
tedusingtheAG
REEIItool.24Fulld
etailsofth
emetho
dologicalassessm
enta
reavailableinApp
endix3.)
Auth
ors
(yea
r),
coun
try
Popu
latio
n/se
tting
Cont
ent o
f sys
tem
Freq
uenc
y of
reco
rdin
gEs
cala
tion
prot
ocol
Impl
emen
tatio
n st
rate
gyAu
dit
stra
tegy
Ed
ucati
onal
tool
Sum
mar
y of
key
re
com
men
datio
ns fr
om
guid
elin
eDe
part
men
t ofHea
lth,
Nati
onal
Clin
ical
Gu
idel
ine
No.
1 NEW
S(201
3),7
Ireland
AGRE
E II
scor
e:91.7%
All a
dult
patie
nts
in a
cute
ho
spita
ls (exclude
sob
stetric
pa
tients).
Resp
irato
ry ra
te
Oxygensaturatio
n(SpO
2),Hea
rtra
te,
Bloo
d pr
essu
re,
Tempe
rature,Levelof
cons
ciou
snes
s.
Whe
reapati
entiso
ninspire
doxygen
(FiO
2)a
scoreof3isadd
ed.
Yes
(Minim
um
observati
on
freq
uencyis
provided
by
score).
Yes(Re
commen
datio
ns
aremad
ebu
titisthe
respon
sibilityofe
ach
indi
vidu
al h
ospi
tal t
o ou
tline
theire
scalati
on
protocol).
Yes(roles/
respon
se-abiliti
es
andba
rriers/
enab
lers
iden
tified
)
Yes(Tool
provided
)Yes(CO
MPA
SS
educati
onalto
ol
(onlineman
ualfor
inde
pend
ent l
earn
ing
+multip
lecho
ice
quiz+face-to
-face
session),and
ISBA
R(Id
entify,situa
tion,
backgrou
nd,
asse
ssm
ent,
recommen
datio
ns
commun
icati
onto
ol)
Thereare60
recommen
datio
ns;n
okey
recommen
datio
nslisted
.(Fullguide
lineavailableat
http://he
alth.gov.ie
/wp-
conten
t/up
load
s/20
15/01/
NEW
SFull-
Repo
rtAu
gust20
14.pdf)
Roya
l Col
lege
ofPhysic
ians;
NEW
S;re
port
ofaworking
pa
rty,8 U
K
AGRE
E II
scor
e:66.7%
Acut
ely
ill a
dult
patie
ntsin
hosp
ital,
buta
lso
preh
ospi
tal
1 re
spira
tory
rate
2oxygen
saturatio
ns
3 te
mpe
ratu
re
4systolicblood
pr
essu
re
5 pu
lse ra
te
6levelo
fco
nsci
ousn
ess.
Yes
(Minim
um
observati
on
freq
uencyis
provided
by
score).
Yes(Clinicalre
spon
ses
areprovided
forthe
diffe
rentsc
ores)
Yes(recommen
dtr
aini
ng sh
ould
be
man
datory
forh
ealth
care
professio
nals
and
stud
ents
, an
dthen
referto
educati
onalto
ol)
No
Yes(e-learning
sessions&field
specificcasestud
ies)
NEW
Sshou
ldbeused
whe
npa
tientsp
resentacutelyto
ho
spita
land
inpre-hospital
assessmen
ti.e.b
yprim
ary
careand
ambu
lance
services.The
new
Nati
onal
Early
Warning
Score(N
EWS)
repo
rt, w
hich
adv
ocat
es
stan
dardising
theuseof
aNEW
Ssystem
across
the
NHS
to d
rive
the
‘step
chan
ge’req
uiredinth
eas
sess
men
t and
resp
onse
toacuteillness.NEW
Scouldalsobead
optedas
asurveillancesystem
for
allp
atien
tsin
hospitalsfor
tracking
theirc
onditio
n,
alertin
gtheclinicalte
amto
med
icaldeterioratio
nan
dtriggerin
gatim
elyrespon
se.
(Fullguide
lineathttps://
www.rc
plon
don.ac.uk/
projects/outpu
ts/nati
onal-
early
-warning
-score-new
s)

33
Auth
ors
(yea
r),
coun
try
Popu
latio
n/se
tting
Cont
ent o
f sys
tem
Freq
uenc
y of
re
cord
ing
Esca
latio
n pr
otoc
olIm
plem
enta
tion
stra
tegy
Audi
t st
rate
gy
Educ
ation
al
tool
Nati
onal
Institute
forH
ealth
an
d Ca
re
Excellence
CG50
,9 UK
AGRE
E II
scor
e:
91.7%
Acut
ely
ill a
dult
patie
ntsinho
spita
l.Multip
le-param
eteror
aggr
egat
e w
eigh
ted
scor
ing
system
susedfortrackand
tr
igge
r sys
tem
s sho
uld
mea
sure:
• he
art r
ate
• re
spira
tory
rate
•systolicblood
pressure
•levelo
fcon
sciousne
ss•oxygen
saturatio
n•
tem
pera
ture
.
Insp
ecificclinical
circum
stan
ces,add
ition
al
mon
itorin
gshou
ldbe
considered
;forexample:
• ho
urly
urin
e ou
tput
•bioche
micalana
lysis
,suchaslactate,b
lood
glucose,basede
ficit,
arte
rial p
H•
pain
ass
essm
ent.
Nospecific
char
t pro
vide
d.
Reco
mm
ende
d to
use
a tr
ack
and
trig
ger s
yste
m.
Nospecificserviceconfi
guratio
ncanbe
recommen
dedasa
preferredrespon
sestrategyfo
rindividu
alside
ntifie
dashavinga
deterio
ratin
gclinicalcon
ditio
n.
Agrad
edre
spon
sestrategyfo
rpa
tientside
ntifie
dasbeing
atrisk
ofclin
icaldeterioratio
nshou
ld
beagree
dan
dde
livered
locally.
Itshou
ldcon
sisto
fthe
follo
wing
threelevels:lo
w,m
ediumand
hi
gh sc
ore
grou
ps.
Yes(Im
plem
entatio
ntools
provided
:htt
ps://w
ww.nice.org.
uk/guida
nce/cg50
/resources/im
plem
entatio
n-ad
vice-433
5754
69)
Yes(Tool
provided
)Yes(presen
ter
slide
s and
sh
ared
e-learning
prog
ram)
Sum
mar
y of
key
reco
mm
enda
tions
from
the
NIC
E gu
idel
ine
(Ful
l gui
delin
e av
aila
ble
at h
ttps
://w
ww
.nic
e.or
g.uk
/gui
danc
e/cg
50)
1.Ad
ultp
atien
tsin
acutehospitalsetti
ngs,in
clud
ingpa
tientsintheem
ergencyde
partmen
tforwho
maclin
icaldecision
toadm
itha
sbee
nmad
e,sh
ouldhave:
a.ph
ysiologicalo
bservatio
nsre
corded
atthe
timeofth
eira
dmiss
ionorin
itialassessm
ent
b.aclea
rwritt
enm
onito
ringplan
thatsp
ecifieswhichphysio
logicalo
bservatio
nssh
ouldberecorded
and
how
ofte
n.The
planshou
ldta
keaccou
ntofthe
:
-p
atien
t’sdiagn
osis
-presenceofcom
orbiditie
s
-a
gree
dtreatm
entp
lan
Physiologicalo
bservatio
nssh
ouldberecorded
and
acted
upo
nbystaff
who
havebe
entraine
dtound
ertaketh
eseproced
uresand
und
erstan
dtheirc
linicalre
levance.
2.Ph
ysiologicaltrackand
triggersystemss
houldbe
usedtom
onito
rallad
ultp
atien
tsin
acutehospitalsetti
ngs.
a.Ph
ysiologicalo
bservatio
nssh
ouldbemon
itoredatleaste
very12ho
urs,unlessa
decision
hasbee
nmad
eatase
niorleveltoincrea
seord
ecreasethisfreq
uencyfora
n
individu
alpati
ent.
b.Th
efreq
uencyofm
onito
ringshou
ldin
crea
seifabn
ormalphysio
logyisdetected,aso
utlin
edin
therecommen
datio
non
grade
drespon
sestrategy
3.Staff
caringforp
atien
tsin
acutehospitalsetti
ngss
houldha
vecom
petenciesinmon
itorin
g,m
easuremen
t,interpretatio
nan
dprom
ptre
spon
seto
theacutelyillpati
ent
approp
riateto
thelevelo
fcaretheyareproviding
.Edu
catio
nan
dtraining
shou
ldbeprovided
toensurestaff
havethesecompe
tencies,and
theysh
ouldbeassessed
toensure
they
can
dem
onst
rate
them
.

344.Agrad
edre
spon
sestrategyfo
rpati
entsid
entifi
edasb
eing
atrisk
ofclin
icaldeterioratio
nshou
ldbeagreed
and
delivered
locally.Itsho
uldconsistofthe
follo
wingthree
leve
ls.
a.Low-scoregroup
:
-Increased
freq
uencyofobservatio
nsand
thenu
rseincha
rgealerted.
b.Med
ium-scoregroup
:
-U
rgen
tcalltoteam
with
prim
arymed
icalre
spon
sibilityfo
rthe
pati
ent.
-Sim
ultane
ousc
alltope
rson
nelw
ithcorecompe
tenciesforacuteillness.The
secom
petenciesc
anbede
livered
byavarie
tyofm
odelsa
talo
callevel,suchasacriti
cal
careoutreachteam
,ahospital-a
t-nightte
amora
specialisttrainee
inanacutemed
icalorsurgicalspe
cialty.
c.High
-scoregroup
:
-E
mergencycalltote
amwith
criti
calcarecompe
tenciesa
nddiagn
ostic
skills.The
team
shou
ldin
clud
eamed
icalpracti
tione
rskilledinth
eassessmen
tofthe
criti
callyill
patie
nt,w
hopossessesadvan
cedairw
aym
anagem
enta
ndre
suscita
tionskills.The
resh
ouldbean
immed
iatere
spon
se.
5.Iftheteam
caringforthe
pati
entcon
siderstha
tadm
issiontoacriti
calcarearea
isclin
icallyin
dicated,th
enth
ede
cisio
ntoadm
itshou
ldinvolvebo
thth
econsultantcaringfor
thepa
tientonthewardan
dtheconsultantin
criti
calcare.
6.Aft
erth
ede
cisio
ntotran
sferapati
entfromacriti
calcarearea
toth
egene
ralw
ardha
sbee
nmad
e,heorsh
eshou
ldbetran
sferredasearlyasp
ossib
leduringtheda
y.
Tran
sferfrom
criti
calcarearea
stothegene
ralw
ardbe
twee
n22
.00an
d07
.00shou
ldbeavoide
dwhe
neverp
ossib
le,and
shou
ldbedo
cumen
tedasanad
verseincide
ntifit
occu
rs.
7.Th
ecriticalcarearea
tran
sferrin
gteam
and
thereceivingwardteam
shou
ldta
kesh
ared
respon
sibilityfo
rthe
careofth
epa
tientbeing
tran
sferred.The
yshou
ldjo
intly
ensure:
a.thereisconti
nuity
ofcarethroug
haform
alstructured
han
dovero
fcarefrom
criti
calcarearea
staff
towardstaff
(including
bothmed
icaland
nursin
gstaff
),supp
ortedby
awritt
enplan
b.thatth
ereceivingward,with
supp
ortfromcriti
calcareifrequ
ired,can
deliverth
eagreed
plan.
Theform
alstructured
han
dovero
fcareshou
ldin
clud
e:
c.asummaryofcriti
calcarestay,including
diagn
osisan
dtreatm
ent
d.amon
itorin
gan
dinvestigatio
nplan
e.aplan
foro
n-go
ingtreatm
ent,includ
ingdrug
sand
therap
ies,nutriti
onplan,in
fecti
onstatusand
anyagree
dlim
itatio
nsoftreatmen
t
f.ph
ysicaland
reha
bilitati
onnee
ds
g.psycho
logicaland
emoti
onalnee
ds
h.specificcommun
icati
onorlan
guagene
eds.

35
4.3.4 Effectiveness studiesOnlyonestudyexaminedtheeffectivenessofearlywarningsystemsandTTS(seeTable7Evidencetablebelow).Anon-randomisedcontrolleddesigncomparedtheeffectoftheModifiedEarlyWarningScore(MEWS)withclinicaljudgmentonchangesinthemanagementandadverseeventsofpatientswhoarewaiting for in-patientbeds in EDof a largehospital inHongKong.42 The authors concluded that theMEWSmightimprovetherateofactivatingacriticalpathwaybutmightmakelittleornodifferencetothedetectionofdeteriorationoradverseevents;however,weareveryuncertain since theevidencewasofverylowquality(GRADE)duetoseriousimprecisionandhighriskofbias(Appendix3).
Insummary,thereislimitedevidenceregardingtheeffectivenessofusingearlywarningsystemsintheEDandavailableevidencefromonestudyisofverylowquality,makingconclusionsuncertain.

36Ta
ble
7.Evide
nceTable:Effe
ctivene
ssstud
ies
(Risk
ofbiasand
qua
lityofevide
ncewereratedusingtheEP
OCqu
ality
assessm
entforqu
antitati
vestudies
27and
GRA
DE.26Fulld
etails
ofthe
assessmen
tareavailableinApp
endix3.)
Auth
ors (
year
), co
untr
ySt
udy
aim
Parti
cipa
nts
Inte
rven
tion
Cont
rol
Out
com
esRe
sults
Shuk-Ngo
reta
l(201
5),42
Hon
g Ko
ng
Desi
gn:n
on-
rand
omise
d co
ntro
lled
tria
l
Risk
of b
ias:
Hi
gh
GRA
DE le
vel:
Very
low
Tocom
pareth
epe
rforman
ceso
fde
tecti
ngpati
ent
deterio
ratio
nwith
an
d w
ithou
t usin
g theMod
ified
Early
War
ning
Sco
re
(MEW
S)fo
ragroup
ofpati
entswho
arewaitin
gforin-
patie
ntbed
sinan
ED
.
Emergencypa
tients
beinghe
ldin
the
EDobservatio
narea
becau
seof
accessblockto
the
spec
ialty
war
ds
wer
e in
clud
ed
in th
e st
udy.
544
pa
tientsrecruite
d:
•Interven
tion
grou
p(M
EWS):
269pa
tients
•Co
ntrol(Usual
Observatio
n):2
75
patie
nts
Emergencynu
rses
recorded
theMEW
Sof
accessblockpati
ents
4-ho
urly,and
follo
wed
MEW
Sactio
npa
thway
ford
ecision
makingto
triggera
ction
s:M
EWS
=0—
3 Re
gularo
bservatio
n
MEW
S=4
Seni
or e
mer
genc
y nu
rsereview
spati
ent’s
cond
ition
MEW
S>4
Triggeredthecritical
path
way
.
Anytim
eanu
rsefoun
dthatapati
entw
as
unwell,he
/she
cou
ld
overrid
eane
gativ
eMEW
Sde
cisio
n(i.e.
MEW
S<5)to
trigger
thecriticalp
athw
ay.
‘‘Clin
icalju
dgmen
t’’
=practic
ebynurses
usingindividu
al’s
know
ledg
e, c
linic
al
expe
rienc
e an
d gu
t feeling—ju
dging
basedon
strong
feelingsra
ther
than
facts,plusthe
mea
suremen
tof3
vitalsigns—
blood
pr
essu
re, p
ulse
and
bo
dyte
mpe
rature.
Prim
ary
outc
ome:
A
chan
ge in
pa
tient’sED
m
anag
emen
t pla
n byEDdo
ctorin
re
spon
se to
the
MEW
Scritical
pathwayacti
vatio
n.
Seco
ndar
y ou
tcom
e:
An a
dver
se e
vent
oc
curr
ed d
urin
g thefirst24hof
adm
issio
n to
the
war
d. A
dver
se
even
ts w
ere
defin
edasa
ctive
resuscita
tion,IC
U
adm
issio
n, c
ardi
ac
arre
st a
nd d
eath
.
Chan
ge in
man
agem
ent: Apo
sitivedoctor
respon
se=fo
llowingthecriticalp
athw
ay
activ
ation
,ase
niordoctorreviewed
apati
ent
andchan
gedtheman
agem
entp
lanofth
at
patie
nt.
Ane
gativ
edo
ctorre
spon
se=nochan
ge
inEDman
agem
entp
lanfollo
wingcritical
pathwayacti
vatio
n.
Inth
eMEW
Sgrou
p,th
erewasapp
roximately
1ep
isode
ofa
ctivatio
ninevery10pa
tients
butitw
as1in
20pa
tientsintheUsual
Observatio
ngrou
p.
Thepo
sitivedoctorrespo
nseratewashigh
inbothpa
tientgroup
s(87
.1%in
theMEW
Sgrou
p;92.9%
inth
eUsualObservatio
ngrou
p).
Adve
rse
even
ts:
0.4%
(n=1
)intheMEW
Sgrou
pan
d0.4%
(n=1
)intheUsualObservatio
ngrou
p,had
an
adverseeventwith
in24hofadm
issionto
the
war
d.
Obs
erva
tion
perf
orm
ance
(Det
ectio
n pa
tient
det
erio
ratio
n):
MEW
S:
Sensitivity:1
00.0%
Sp
ecificity:9
8.3%
Usualobservatio
n:
Sensitivity:1
00.0%
Sp
ecificity:9
7.8%

37
4.3.5 Development and validation studiesChallen and Goodacre 46reportedtheresultsofascopingreview(SeeTable9evidencetablebelow),whichidentified119toolsrelatedtooutcomepredictioninED;however,themajoritywerecondition-specific tools (n=94). They found the APACHE II score to have the highest reported area under thereceiveroperatingcharacteristic(AUROC)curveb(0.984)inpatientswithperitonitis.
Inaddition,35developmentand/orvalidationprimarystudyreportswereidentified(seeTable10, Table11 and Table12Evidence tablesbelow). Studieswereconductedbetween2003and2016 in theUK(n=5),43,49-52theUSA(n=5),53-57Turkey(n=4),58-60HongKong(n=3),61-63Singapore(n=3),64-66SouthAfrica(n=2),44, 45Sweden(n=2),67,68Denmark (n=1),69Germany(n=2),70,71China (n=1),32SouthKorea (n=2),72,73Thailand(n=1),74Taiwan(n=1),75theNetherlands(n=1)76andAustralia(n=2).77,78Twelvestudieswereretrospective,22wereprospectivecohortstudiesandonewasasecondaryanalysisofaRCT.56Eightstudiesdevelopedandvalidated(inthesamesample)anearlywarningsystem,while27validatedanexistingsysteminadifferentsample.All35studiesexaminedtheuseofearlywarningsystemsinanEDpopulation. Three studies includeda randomsample54,69,78 andparticipants in the remaining studieswererecruitedconsecutivelyorthesamplingstrategywasnotstatedclearly.
A total of 27 early warning systems were developed and/or validated. Condition-specific systems;forexample, theMortality inEmergencyDepartmentSepsis (MEDS) score,Sepsis inObstetricsScore(SOS), CURB-65, andTraumaand Injury Severity Score (TRISS)wereexcluded from this review. Toolsincludedwere:theModifiedEarlyWarningScore(MEWS),32,45,51-54,58-66,70,71,74,75,79theRapidEmergencyMedicineScore(REMS),53,59,61,62,67,68thePrinceofWalesEDScore(PEDS),61,62theRevisedTraumaScore(RTS),61theAcutePhysiologyandChronicHealthEvaluationscore(APACHEII),57,61,67,77TheResuscitationManagement score (THERM),62 the Simple Clinical Score (SCS),62 the Mainz Emergency EvaluationScore (MEES),62 National Early Warning Score (NEWS),49, 50, 62, 72, 76 the Bispebjerg EWS (BEWS),69 the Charlson comorbidity index (CCI),60, 71, 75 the Emergency severity index (ESI),71MEWSplus,54modifiedREMS(mREMS),55NationalEarlyWarningScoreincludingLactate(NEWS-L),72theNewSimplifiedAcutePhysiologyScore (SAPS) II,56,77 theMorbidityProbabilityModelatadmission (MPM0II),56 theLogisticOrganDysfunctionSystem(LODS),56theTriageEarlyWarningScore(TEWS),44thePredisposition,Insult/Infection,Response,andOrgandysfunction(PIRO)model,57theRapidAcutePhysiologyScore(RAPS),67,68 theAssessmentScoreforSickpatientIdentificationandStep-upinTreatment(ASSIST),51theSequentialOrganFailureAssessment (SOFA),77 thePatientStatus Index (PSI),43 theVitalPACEarlyWarningScore(VIEWS),79 theVitalPACEarlyWarningScore-Lactate (VIEWS-L)73and theEDCritical InstabilityCriteria(EDCIC).78
Churpek et al 80 classified early warning systems into single-parameter systems, multiple-parametersystems and aggregate weighted scores. A single-parameter system consists of a list of individualphysiologic criteria that, if reached by a patient, triggers a response. Multi-parameter systems usecombinations of physiologic criteria without calculation of a score to activate a response, whileaggregate systems categorise vital signs and sometimes other variables into different degrees ofphysiologic abnormality and then assign point values for each category. The early warning systemsexamined in the studies included in this review primarily developed/validated aggregate weightedscores(Table8).
b TheReceiverOperatingCurve(ROC)plotsthetruepositiverateagainstthefalsepositiverateatcertainthresholds.TheAUROCofaclassifierisequivalenttotheprobabilitythattheclassifierwillrankarandomlychosenpositiveinstancehigherthan a randomly chosennegative instance.48. FawcettT.An introduction toROCanalysis. PatternRecognition Letters.2006;27:861–74.

38
Table 8.Earlywarningsystemsincludedinthereviewbytypeofsystem
Types of systems80
Single-parametersystems Multiple-parametersystems Aggregate weighted scores
ESIEDCIC
Noneidentified MEWSREMSmREMSPEDSRTSAPACHEIITHERMSCSMEESNEWSBEWSCCIMEWSplusNEWS-LSAPSIILODSMPMOIITEWSPIRORAPSASSISTVIEWSVIEWS-LPSISOFA
Themostcommonoutcomesexaminedwerein-hospitalmortality(n=21),admissiontoIntensiveCareUnit (ICU) (n=12),mortality (not specifiedwhere or during a specific follow up time frame possiblybeyondhospitaldischarge)(n=10),hospitaladmission(n=7),andlengthofhospitalstay(n=4).
Overall,theAPACHEIIscore,PEDS,VIEWS-L,andTHERMscoresappearedrelativelybetteratpredictingmortalityandICUadmissioncomparedtoothertoolsassessedintheincludedstudies.TheMEWSwasthemostcommonlyassessedtoolandthecut-offvalueusedwas4or5,withtheexceptionofDundaret al 79whofoundanoptimalcut-offof4forin-hospitalmortalitybut3forpredictinghospitalisation.Forpredicting ICUadmissions, theAUROCofMEWSvaried from0.49 to0.73across studies. For theoutcome in-hospitalmortality, theAUROC ranged from0.61 to 0.89. The BEWS contained the sameparameters as theMEWS (respiratory rate,HR, SBP, temperature, LOC)and reporteda20% increaseinriskofdeathwithin48hoursanda4%increaseinriskforICUadmissionwithaBEWSscoreoffiveor more compared to a lower score.69 TheNEWS had a similar AUROC (0.70), predicting in-hospitalmortality,72 which is not surprising considering NEWS includesmost of the same parameters as theMEWS.TheMEWSplusscore,whichaddedtheparametersage,race,gender,EDlengthofstay,methodof arrival, and antibiotics given prior to or during ED visit, had a slightly greater AUROC (0.76) thanMEWS.54TheAUROCfortheREMSrangedfrom0.59to0.70forICUadmissionand0.71to0.91forin-hospital mortality.59,61,67,68ThemodifiedREMscorehadanAUROCof0.8055andVIEWShadanAUROCof 0.9079whenpredicting in-hospitalmortality. TheAUROC for predictingmortalitywas 0.64 for theCCI,600.71forthePIROscore,570.71-0.90fortheAPACHEIIscore,57,670.65-0.87fortheRAPS,67,680.69

39
for theMPMO II score,0.72 for theSAPS II score,0.60 for theLODSscore,56and0.83 forVIEWS-L.73 ThePEDSscorehadahigherAUROCforthepredictionofdeathoradmissionto ICU(0.75-0.90)thantheMEWS (0.73-0.76), theREMS (0.70), theAPACHE II score (0.73), theRTS (0.75), theMEES (0.75),theNEWS(0.71)andtheSCS(0.70).61,62Cattermoleetal62refinedthePEDSscoreanddevelopedtheTHERMscore,whichhadanevenhigherAUROC(0.84)forpredictiondeathorICUadmission.
Studies were subsequently categorised into three evidence tables according to the degree ofdifferentiationoftheEDpatientgroup:apatientgroupwithacertain(suspected)condition(Table10),apatientgroupinaspecifictriagecategory(ies)(Table11),oranundifferentiatedpatientgroup(Table12).
Twelve of the 35 validation studies only included participants in (a) specific triage category(ies) (seeTable10Evidencetablebelow).Triagesystemsusedvariedacrossthesestudies,butincludedcategoriesof patients that were critically ill and had to be seen with relative urgency (e.g.Manchester triagesystemI-III,Patientacuitycategoryscale1or2)orwereadmittedtotheresuscitationroom.Lookingatthefindingsofthissubgroupofstudiesinpredictingmortality,theAUROCfortheMEWSrangedfrom0.63to0.75,59,64-66itwas0.70-0.77forREMS,59,610.77-0.87forNEWS,760.90forPEDS,0.83forAPACHEII,and0.77forRTS.61PredictingICUadmission,theAUROCwere0.5459and0.4964forMEWSand0.59forREMS59,whiletopredicthospitaladmissiontheAUROCofNEWSwas0.66-0.70.76Cattermoleetal61andCattermoleetal62usedacombinedoutcomeofdeathandICUadmissionandfoundanAUROCof0.76and0.73 forMEWS,0.90and0.75 forPEDS,0.73 forAPACHE II, 0.75 forRTS,0.70and0.70forREMS,0.75 forMEES,0.71 forNEWS,0.70 forSCS,and0.84 forTHERM.Onestudyassessed thepredictionofsepticshockbyNEWS(AUROC0.89).50
Eleven other studies (12 records) included a differentiated patient groupwith a specific (suspected)condition (see Table 11 Evidence table below). Five studies only included patients with (suspected)sepsis.49, 52, 53, 57, 60, 71 Other study populations were restricted to patients with trauma,73 suspected infection,55,77 pneumonia72orwhohadsignsof shock.56Assessing thepredictiveabilityof systems topredictmortality,MEWShadanAUROCof0.6160and0.7252,CCIof0.65,60mREMSof0.80,55NEWSof0.70,72NEWS-Lof 0.73,72VIEWS-Lof 0.83,73 SAPS II of 0.7256 and0.90,77MPMO II of 0.69,56 LODSof0.60,56PIROof0.71,57APACHEIIof0.7157and0.90,77andSOFAof0.86.77
The remaining 12 studies assessed earlywarning systems in an undifferentiated ED population (seeTable12Evidencetablebelow).TheAUROCtopredictmortalitywas0.71,700.73,54and0.8979forMEWS,0.76forMEWSplus,540.9167and0.8568forREMS,0.8767and0.6568forRAPS,and0.90forAPACHEII.67 Insummary,manydifferentsystemshavebeendevelopedandevaluatedtopredictadverseoutcomesineitherdifferentiatedorundifferentiatedEDpopulations.Theparametersmost commonly includedwereHR,respiratoryrate,bloodpressure,temperature,oxygensaturationsandlevelofconsciousness.The MEWS was the most commonly assessed system and was better at predicting mortality thanICUadmission, but theAPACHE II score, PEDS,VIEWS-L, and THERMscoreswere relatively better atpredictingmortality and ICUadmission, althoughdifferences in study characteristics, theparametersmeasured and the weight given to individual parameters, may account for part of the observeddifferencesinpredictiveability.

40Ta
ble
9.Evide
ncetable:Develop
men
tand
validati
onstud
ies–
Scoping
Review
(Metho
dologicalqu
ality
wasrated
usin
gan
ada
pted
Nati
onalInstituteofH
ealth
che
cklist.23
Fullde
tailsofthemetho
dologicalassessmen
tare
availableinApp
endix3.)
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gnSe
tting
& P
artic
ipan
tsCo
nten
t of s
yste
m/
tool
Resu
lts
Chal
len
&
Good
acre
(201
1),46UK
Qua
lity
Ratin
g:Goo
d
Tocarryoutasc
oping
review
ofthe
literature
relatin
gtooutcome
pred
ictio
ninadu
ltno
n-tr
aum
a em
erge
ncy
patie
nts,in
orderto
iden
tifythenu
mbe
ran
drang
eofrisksc
ores
develope
dfora
cutelyill
adultsand
toid
entifythe
outc
omes
thes
e sc
ores
pr
edic
t.
Scop
ing
revi
ewPa
pers
that
det
aile
d a
clin
ical
ass
essm
ent
tool
that
was
app
lied
atth
epo
into
fpati
ent
presen
tatio
nto
unsc
hedu
led
heal
thca
re
serv
ices
with
out
com
e mea
sures3
0da
ysafte
rpresen
tatio
n.
Selecti
oncriteria:
Who
lly o
r pr
edom
inat
ely
clin
ical
as
sess
men
t too
l, ad
ultp
opulati
on,an
outc
ome
mea
sure
up
to30da
ysafte
rpresen
tatio
n.
Tools:
Scoringsystem
savailablefor1
7broa
dcond
ition
s(w
ith80diffe
rentin
clusioncrite
ria)
119toolsa
ssessed(ofw
hich25gene
ric)
Outcomes:
51differen
toutcomemea
suresu
sed(ofw
hich30
diseasespecific)
An
alysesth
atused‘death’aso
utcome(247
):19
0repo
rted
AURO
Cofwhich69AU
ROC>0.8.
An
alysesth
atdidnotuse‘death’aso
utcome(251
):15
1repo
rted
AURO
Cofwhich30AU
ROC>0
.8
LowestA
URO
C=0.44
(predicti
nghospitald
eathsin
patie
ntsw
ithacuteM
I)
High
estA
URO
C=0.98
(APA
CHEIIforp
redicti
ng
hospita
ldeathsinpa
tientsw
ithperito
nitis)

41Ta
ble
10.Evide
ncetable:Develop
men
tand
validati
onstud
ies–
Pati
entg
roup
sdifferen
tiatedbytriagecategory
(Risk
ofb
iasw
asra
tedusingatoolada
pted
from
Kan
sagaraeta
l(20
11).3
0 Fulld
etailsofth
eriskofbiasa
ssessm
enta
reavailableinApp
endix3.)
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Alam
et a
l (201
5),76
the
Net
herla
nds
Ris
k of
bia
s:
Unclear
Toexploreth
epe
rforman
ceof
NEW
Swith
regardto
pred
ictin
gad
verse
outc
omes
in a
dult
patie
ntsa
ndth
eab
ilityofN
EWSto
pred
ictthe
nee
dfor
hosp
ital a
dmiss
ion
inanED
pop
ulati
on.
Prospe
ctive
coho
rt
(Validati
on)
274pa
tients
(≥18
yea
rs)
presen
ting
(T0)to
theED
of
anurban
ac
adem
ic
tertiary
care
cen
tre
betw
een7
Jan-15
Feb
20
13with
an
Emergency
Seve
rity
Inde
xscore
of2and
3
not t
riage
d to
the
resuscita
tion
room
. For
24
7of
these27
4pa
tients,th
eNEW
Swas
calc
ulat
ed
an h
our l
ater
(T1).O
nly
133ofth
e24
7pa
tients
couldbe
follo
wed
up
at d
ischa
rge
from
theED
(T2).
NEW
S:Param
eters:
Resp
irato
ry ra
te, S
BP,
HR, t
empe
ratu
re,
oxygen
saturatio
n
Hosp
ital
adm
issio
n,
leng
thof
stay,ICU
ad
miss
ion,
m
orta
lity
Hosp
ital a
dmis
sion
(n=1
30)
NEW
Ssig
nifican
tlyassociatedwith
adm
issionatall3
timepo
ints(p
<0.001
).•T0
:AURO
C0.66
(95%
CI0
.60–
0.73
)•T1
:AURO
C0.69
(95%
CI0
.62–
0.75
)•T2
:AURO
C0.70
(95%
CI0
.61–
0.79
)
Leng
th o
f sta
yNEW
Ssig
nifican
tlyassociatedwith
leng
thofstayat
all3timepo
ints(p
<0.001
).Med
ianleng
thofstaymorethan
dou
bled
fora
score>7
com
paredwith
asc
oreof0–4
.(AU
ROCno
tprovided
)
ICU
adm
issi
on(n
=10)
NEW
Ssig
nifican
tlyassociatedwith
ICUadm
ission
atall3tim
epo
ints(T
0:p=0
.003
;T1:p=0
.001
;T2:
p=0.04
6).(AU
ROCno
tprovide
d)
30-d
ay M
orta
lity(n=1
1)NEW
Ssig
nifican
tlyassociatedwith
mortalityatall3
timepo
ints(p
<0.001
).30
-daym
ortalitywasnotsign
ificantlyre
latedtoESI(p
=0.81
6).
•T0
:AURO
C0.77
(95%
CI0
.62–
0.92
)•T1
:AURO
C0.87
(95%
CI0
.77–
0.96
)•T2
:AURO
C0.77
(95%
CI0
.57–
0.97
).
Ofthe
individu
alphysio
logicalm
easureso
fNEW
S:•
Resp
irato
ry ra
te w
as a
ssoc
iate
d w
ith m
orta
lity
at a
ll mea
suredtim
epo
ints(T
0:p=0
.017
;T1:p<0
.001
;T2
:p=0
.014
).•Pu
lsera
tehad
astrong
correlatio
nwith
mortalityat
T1(p
=0.037
)Nocorrelati
onsc
ouldbefoun
dfora
llothe
rph
ysio
logi
cal p
aram
eter
s.

42Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/too
lRe
fere
nce
crite
riaRe
sults
Arm
agan
et
al(2
008),58
Turkey
Risk
of b
ias:
Unclear
Todeterminethe
pred
ictiv
evalid
ity
ofth
eMod
ified
Early
Warning
Score
(MEW
S)in
aTurkish
EDse
tting
.
Prospe
ctive
coho
rt
(Validati
on)
309pa
tients
(Tria
geI,II,
II)in
EDof
one
hosp
ital
betw
een
April-Aug
20
07.
MEW
S: P
aram
eter
s:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e
Hosp
ital
adm
issio
n,
ICU
adm
issio
n,
in-hospital
death,ED
deat
h
Lowrisk(M
EWS≤4)(n
=106
);high
risk(M
EWS>4
)(n=2
03)
MEW
S(cut-off>4
)•Ad
miss
iontohospital:ad
justed
OR1.56
(95%
CI
0.93
-2.98)
•Ad
miss
iontoIC
U:adjustedOR1.95
(95%
CI1
.04-
366.00
)(p=
0.04
)•De
athinED:adjustedOR35
.13(95%
CI4
.58-
269.40
)(p<
0.00
1)•De
athinhospital:ad
justed
OR14
.80(95%
CI5
.52-
39.70)(p
<0.001
)Bu
lut e
t al
(201
4),59
Turkey
Risk
of b
ias:
Low
Com
pare
the
efficacyofM
odified
Early
Warning
Score(M
EWS)and
Ra
pidEm
ergency
Med
icin
e Sc
ore
(REM
S)onin-
hosp
ital m
orta
lity,
an
d as
a p
redi
ctor
ofhospitalisati
on
in g
ener
al m
edic
al
andsurgicalpati
ents
admitted
toED.
Prospe
ctive,
multic
entre
coho
rt
(Validati
on)
2000
gen
eral
med
ical
&
surg
ical
pa
tients
(red
&
yello
w tr
iage
catego
ry)
presen
ting
toEDs
of
3 ho
spita
ls be
twee
nOct
2011
-April
2012
.
REM
S:
Parameters:
Age
, HR,
Temp,RespiratoryRate,
Mea
n ar
teria
l pre
ssur
e,
GCS,oxygensaturatio
ns
MEW
S:
Parameters:
SBP
, HR,
Re
spira
toryra
te,Tem
p,
AVPU
Adm
issio
n to
war
d or
ICU/H
DU,
in-hospital
mor
talit
y
Med
ian(ran
ge):
•MEW
S:1(0
-9);RE
MS:5(0
-16)
40.8%hospitalised
ward,29.8%
-ICU/H
DU,2
9.2%
di
scha
rged
. Totalin-ho
spita
lmortalitywas7.7%(n
=153
).
Pred
ictin
g in
-hos
pita
l mor
talit
y•RE
MS(6–1
3)vsR
EMS<6
:RR2.92
(95%
CI0
.03to
4.22
);p<
0.00
1•RE
MS(>13
)vsR
EMS<6
:RR14
.56(95%
CI4
.57to
46.57);p
<0.001
•MEW
S≥5vsM
EWS<5
:RR3.84
(95%
CI2
.36to
6.24
);p<
0.00
1•MEW
SAU
ROC:0.63(95%
CI0
.61-0.65
)•RE
MSAU
ROC:0.71(95%
CI0
.67-0.72
)•Pe
rforman
ceofR
EMSwashighe
r(p<
0.00
1)
Pred
ictin
g di
scha
rge
vs h
ospi
talis
ation
:•MEW
SAU
ROC:0.57(95%
CI0
.55-0.59
)•RE
MSAU
ROC:0.64(95%
CI0
.62-0.66
)•Pe
rforman
ceofR
EMSwashighe
r(p<
0.00
1)
Pred
ictin
g ad
mis
sion
to IC
U/H
DU:
•MEW
SAU
ROC:0.54(95%
CI0
.52-0.56
)•RE
MSAU
ROC:0.59(95%
CI0
.57to0.61)
•Pe
rforman
ceofR
EMSwashighe
r(p<
0.00
1)

43
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Catte
rmole
etal(20
09),6
1 Ho
ngKon
g
Risk
of b
ias:
Low
(1)D
eterminea
newprogn
ostic
scoremakinguseof
rapidlyavailablean
dea
silymea
surable
phys
iolo
gica
l pa
ram
eter
s and
initiallabo
ratory
testsinresuscita
tion
room
pati
ents,in
orde
rtoiden
tify
patie
ntsm
osta
trisk
ofdeathorinne
ed
ofIC
Ucare.(2
)To
com
pare
the
new
scorewith
APA
CHE
II,RTS,R
EMSan
dMEW
Sscores
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
330ED
pa
tients≥
18
yearso
fage
tria
ged
to
resuscita
tion
room
in 1
ho
spita
l be
twee
n9th
April&6th
May200
6.
Prin
ce o
f Wal
es E
D Sc
ore
(PED
S) (n
ew
score)
Parameters:
SBP
, GCS
, Glucose,HCO
3, whi
te
bloo
dcells,m
etastatic
ca
ncer
hist
ory
Revi
sed
Trau
ma
Scor
e (RTS)
Rapi
d Em
erge
ncy
Med
icin
e Sc
ore (REM
S)
MEW
S
Acut
e Ph
ysio
logy
an
d Ch
roni
c He
alth
Ev
alua
tion
scor
e (APA
CHEII)
Para
met
ers n
ot st
ated
in
this
repo
rt
Prim
ary
outc
ome:
deat
h ad
miss
ion
to
ICUwith
in
7da
ysofE
Datt
enda
nce
(vss
urvival
at7days
with
outICU
ad
miss
ion)
Seco
ndar
y ou
tcom
e m
easu
res:
30
day
mor
talit
y an
d ho
spita
l leng
thof
stay
.
Pooroutcome:23.0%
(77/33
0)(4
0(12.1%
)adm
itted
toIC
Uor4
1(12.4%
)diedwith
in7days).
PEDS
scorerang
edfrom
-2to
58.
Com
paris
on o
f PED
S, A
PACH
E II,
RTS
, REM
S an
d M
EWS
(n=2
34) f
or th
e pr
imar
y ou
tcom
e:
PEDS
: AU
ROC0.90
(0.87–
0.94
),Sensitivity0.87,Spe
cificity
0.80
,PPV
0.57,NPV
0.95,Accuracy0.82
AP
ACHE
II:
AURO
C0.73
(0.68–
0.78
),Sensitivity0.61,Spe
cificity
0.70
,PPV
0.44,NPV
0.86Ac
curacy0.73
RTS:
AU
ROC0.75
(0.70–
0.79
),Sensitivity0.58,Spe
cificity
0.83
,PPV
0.51,NPV
0.87Ac
curacy0.82
REMS:
AURO
C0.70
(0.64–
0.75
),Sensitivity0.51,Spe
cificity
0.79
,PPV
0.42,NPV
0.84Ac
curacy0.73
MEW
S:
AURO
C0.76
(0.71–
0.81
),Sensitivity0.69,Spe
cificity
0.74
,PPV
0.45,NPV
0.89Ac
curacy0.73
Com
paris
on o
f PED
S, A
PACH
E II,
RTS
, REM
S an
d M
EWS
(n=2
34) f
or th
e se
cond
ary
outc
ome
(30
day
mor
talit
y):
PEDS
: AU
ROC0.90
(0.86–
0.93
)AP
ACHE
II:
AURO
C0.84
(0.79–
0.88
) RT
S:
AURO
C0.77
(0.72–
0.81
) RE
MS:
AURO
C0.77
(0.72–
0.82
) MEW
S:
AURO
C0.75
(0.70–
0.80
)

44Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/too
lRe
fere
nce
crite
riaRe
sults
Catte
rmole
etal(20
13),6
2 Ho
ngKon
g
Risk
of b
ias:
Unclear
(1)Tovalid
ate
PrinceofW
ales
EDScore(P
EDS)in
co
mpa
rison
with
othe
rprogn
ostic
scores(M
EWS,
SCS,REM
S,M
EES,
MED
S,W
orthing
&NEW
S);(2)to
sim
plify
and
refin
eth
e sc
ore,
usin
g on
lyvariablesth
at
are
imm
edia
tely
availableinth
eresuscita
tionroom
;(3)tovalid
atethe
new
scor
e to
dev
ise
originalPED
S
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
234
consecuti
ve,
≥18yearso
fage,pati
ents
man
aged
in
resuscita
tion
room
dur
ing
wee
kday
s ov
er a
3
mon
th
perio
d.
The
Resu
scita
tion
Man
agem
ent s
core
(THE
RM)(refin
edPED
Sscore):
Parameters:GCS
,HCO
3− an
d SB
P PE
DS
Parameters:
SBP
, GCS
, Glucose,HCO
3, whi
te
bloo
dcells,m
etastatic
ca
ncer
hist
ory
MEW
S Si
mpl
e Cl
inic
al S
core
(SCS
) RE
MS
M
ainz
Em
erge
ncy
Eval
uatio
n Sc
ore
(MEES)
Nati
onal
Ear
ly W
arni
ng
Scor
e(NEW
S)
Wor
thin
g(exclude
dbe
causeitisacond
ition
specificscore)
M
orta
lity
in th
e ED
Sep
sis(MED
S)
(exclude
dbe
causeit
isacond
ition
specific
score)
Pa
ram
eter
s not
stat
ed
in re
port
.
Prim
ary
outc
ome:
deat
h or
ad
miss
ion
to
ICU.
Seco
ndar
y ou
tcom
es:
30day
mor
talit
y &
hos
pita
l leng
thof
stay
.
37/234
adm
itted
toIC
Uord
iedwith
in7days.
PE
DS:A
URO
C0.75
(95%
CI0
.69to0.80)
MEES:AURO
C0.75
(95%
CI0
.69to0.80)
MEW
S:AURO
C0.73
(95%
CI0
.67to0.79)
NEW
S:AURO
C0.71
(95%
CI0
.64to0.76)
RE
MS:AURO
C0.70
(95%
CI0
.64to0.76)
SC
S:AURO
C0.70
(95%
CI0
.64to0.76)
TH
ERMsc
ores:m
axsc
ore=
37,H
ighrisk<3
0,m
edium
risk(30.1-35
),lowrisk(3
5.1-37
). Co
mpa
rison
of T
HERM
and
NEW
S (n
=234
) TH
ERM:
AURO
C:0.84(0.79to0.88)
High
riskcut-off:Sen
sitivity0.57(0.40to0.73),
Specificity0.89(0.84to0.93),P
PV0.50(0.34to0.66),
NPV
0.92(0.87to0.95)
Med
iumriskcut-off:Sen
sitivity0.89(0.75to0.97),
Specificity0.65(0.58to0.72),P
PV0.32(0.23to0.42),
NPV
0.97(0.92to0.99)
NEW
S:
AURO
C:0.71(0.64to0.76)
High
riskcut-off:Sen
sitivity0.65(0.48to0.80),
Specificity0.71(0.64to0.77),P
PV0.29(0.20to0.40),
NPV
0.91(0.86to0.95)
Med
iumriskcut-off:Sen
sitivity0.92(0.78to0.98),
Specificity0.44(0.37to0.51),P
PV0.24(0.17to0.31),
NPV
0.97(0.91to0.99)
TH
ERMhad
supe
riorspe
cificity
;the
rewasno
significan
tdifferen
cein
AURO
C,se
nsitivityor
pred
ictiv
evalues.

45
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Chris
tens
en
etal(20
11),6
9 De
nmar
k
Risk
of b
ias:
Low
Toevaluateab
ility
ofth
eBispeb
jerg
EWS(BEW
S)to
iden
tifycriticallyill
patie
ntsinED
and
to
exam
inefeasibility
ofusin
gBE
WSto
activ
ateMed
ical
Team
respon
se
Retro
spective
coho
rt
(Develop
ment
&Validati
on)
Rand
om
sampleof
300‘re
d’
cate
gory
pa
tients
visiti
ngED
of1hospital
betw
een
April-Sep
t20
09.
BEW
S Parameters:
Re
spira
tory
Rat
e, H
R,
SBP,Te
mp,LO
C
Adm
issio
n to
ICUwith
in
48hrsof
arriv
al a
t ED
ord
eath
with
in 4
8hrs
ofarrivalat
ED.
138pa
tientso
utof3
00wereexclud
edfo
rinsuffi
cien
tda
ta;1
62in
clud
ed.
Activ
ated
EmergencyCa
ll(EC):2
4
Admitted
toIC
Uwith
in48hrso
fED:4(2
died)
Deathswith
in48h
rsED:6
BEWS≥5(vs<
5):
Deat
h w
ithin
48
hour
s of a
rriv
al:
•RR
20.3(95%
CI6
.9-60.1)
•Sensitivity83.0%
,Spe
cificity
83.0%
,PPV
16.0,NPV
99
.0
ICUadm
issionwith
in48ho
urso
farrival:
•RR
4.1(9
5%CI1
.5-1
0.9)
•Sensitivity50.0%
,Spe
cificity
81.0%
,PPV
6.0,N
PV
98.0
Criti
cally
ill:
•RR
6.8(9
5%CI3
.3-13.8)
•Sensitivity63.0%
,Spe
cificity
82.0%
,PPV
16.0,NPV
98
.0

46Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/too
lRe
fere
nce
crite
riaRe
sults
Gu e
t al
(201
5),32
Ch
ina
Risk
of b
ias:
Unclear(O
nly
abstractin
En
glish
)
Toevaluatethe
valueofM
odified
Early
Warning
Score(M
EWS)in
pred
ictin
gmortality
ofcriti
callyill
patie
ntsa
dmitted
to
em
erge
ncy
depa
rtm
ent.
Prospe
ctive
coho
rt
(Validati
on)
176
emer
genc
y pa
tients
admitted
to
resuscita
tion
room
of
one
hosp
ital
betw
een13
Feb-20
April
2014
.
MEW
S(param
etersn
ot
listedinabstract)
3-day
mor
talit
y, al
l de
aths
, and
co
mpo
site
outc
ome
ofintensive
ca
re u
nit
(ICU)transfe
r,cardio-
pulm
onar
y resuscitatio
n,
and
deat
h.
Mea
nMEW
S4.30
±2.74;74casesM
EWS≥5an
d10
2inM
EWS0-4.
3-da
ys m
orta
lity
(n=4
1)
MEW
S0-1(12.7%
(13/10
2);ref)
MEW
S≥5(37.8(28/74
);OR4.2(95%
CI2.0-8.8,P<
0.00
1))
Multi-regressio
nlogisticshow
edabn
ormalm
ental
status(O
R3.6,95%
CI=1.5-8.4,P
=0.003
)butnot
MEW
S≥5(OR=1.7,95%
CI=0.6-4.5,P
=0.3)w
asth
epred
ictoro
f3-daym
ortality.
Al
l dea
th (n
=58)
MEW
S0-1(17.7%
(18/10
2);ref)
MEW
S≥5(54.1(40/74
);OR5.5(95%
CI2.8-1
0.9,P<
0.00
1))
ICU
tran
sfer
, car
dio-
pulm
onar
y re
susc
itatio
n an
d de
ath
(n=7
4)
MEW
S0-1(25.5%
(26/10
2);ref)
MEW
S≥5(64.9(48/74
);OR5.4(95%
CI2.8-1
0.4,P<
0.00
1))

47
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Ho e
t al
(201
3),64
Si
ngap
ore
Risk
of b
ias:
Low
Tovalidatetheuse
ofth
eMod
ified
Early
Warning
Score(M
EWS)
asapredictorof
patie
ntm
ortality
and
inte
nsiv
e ca
re
unit(IC
U)/high
depe
nden
cy u
nit
(HDU
)adm
issionin
anAsia
npo
pulatio
n.
Retrospe
ctive
coho
rt
(Validati
on)
1024
criticallyill
patie
nts,≥18
yearso
fage,
presen
tingto
a la
rge
Asia
n tertiaryED
be
twee
nNov
2006
and
De
c20
07,
andrequ
iring
conti
nuou
sEC
Gm
onito
ring
andPatie
nt
Acui
ty
cate
gory
Scale(PAC
S)
of1or2
.
MEW
S: P
aram
eter
s:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e
Mor
talit
y du
ring
the
inpa
tient
perio
d follo
wing
adm
issio
n from
the
EDupto
30days,
and
dire
ct
adm
issio
n from
theED
to
the
high
de
pend
ency
un
it,
inte
rmed
iary
ca
re a
rea
or
the
inte
nsiv
e ca
re u
nit.
713pa
tientsM
EWSscore<4
;311
pati
entsM
EWS≥4
. M
orta
lity
47deaths(6.6%
)inMEW
S<4
;53(17.0%
)deathsin
MEW
S≥4
(p<0
.001
) Forc
ut-offvalue≥4
: Sensitivity:4
7.0
Specificity:2
7.9
PPV:6.7
NPV
:83.0
AURO
C:0.68
Adm
issi
on
267(37.4%
)weread
mitted
toHDU
/ICA
inM
EWS
<4;8
6(27.7%
)adm
itted
toHDU
/ICA
inM
EWS≥4
(p=0
.00).
Forc
ut-offvalueof4:
Sensitivity:7
4.2
Specificity:3
3.9
PPV:46.7
NPV
:62.7
AURO
C:0.5

48Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/too
lRe
fere
nce
crite
riaRe
sults
HockOng
et
al(2
012),65
Si
ngap
ore
Risk
of b
ias:
Unclear
Tovalidatea
nove
l Mac
hine
Learning
(ML)sc
ore
incorporati
ngHea
rt
RateVariability
(HRV
)forrisk
stratifi
catio
nof
criticallyillp
atien
ts
presen
tingtoth
eED
bycompa
ring
the
area
und
er th
e curve,se
nsitivity
andspecificity
forp
redicti
onof
card
iac
arre
st w
ith
theMod
ified
Early
War
ning
Sco
re
(MEW
S).
Prospe
ctive
coho
rt
(Validati
on)
925pa
tients,
≥18years
ofage,
requ
iring
conti
nuou
sEC
Gm
onito
ring
tria
ged
asPati
ent
Acui
ty
Cate
gory
Scale(PAC
S)
1 or
PAC
S 2
wereeligible.
MEW
S: P
aram
eters:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e M
L-ba
sed
scor
e:
(exclude
dbe
cause
HRVisno
taro
utine
mea
sure)
Card
iac
arre
st w
ithin
72
ho
urso
fpresen
tatio
ntoth
eED
,de
athaft
er
adm
issio
n (in
-hospital
deat
h du
ring
curr
ent
adm
issio
n,
incl
udin
g with
in72
hours).
4.6%
(43)develop
edcardiacarrestw
ithin72ho
urs;
9.3%
(86)diedaft
eradm
ission.
Ca
rdia
c ar
rest
M
EWS
Sensitivity:7
4.4
Specificity:5
4.2
PPV:7.4(5
.3-10.3)
NPV
:97.8(95.9-98
.8)
+LR:1.6(1
.3-2.0)
AURO
C:0.7
De
ath
after
adm
issi
on
MEW
S Sensitivity:7
4.4
Specificity:5
5.7
PPV:14.7(11.5-18
.4)
NPV
:95.5(93.2-97
.1)
+LR:1.7(1
.5-1.9)
AURO
C:0.7
Keep
eta
l(201
5),50UK
Risk
of b
ias:
Low
Explorerelatio
nship
betw
eeninitial
Nati
onalEarly
War
ning
Sco
re
(NEW
SUK)in
ED
anddiagno
sisof
SevereSep
sis(S
S)
Retrospe
ctive
coho
rt
(Validati
on)
500pa
tients,
>16years
ofage,
presen
ting
atEDof
anurban
ho
spita
l in
a 5-da
ype
riod,
with
tria
ge
catego
ry1-3
(Man
chester
Triage
Score).
NEW
S: P
aram
eter
s:
Respira
toryRate,HR,O
2 saturatio
ns,SBP,Tem
p,
LOC.
Septi
cshock
(SS)
Sepsis:9.9%(n
=50);Sep
ticsh
ock(SS):5
.4%(n
=27)
Pred
ictio
n of
SS:
NEW
Sop
timalcut-off≥3
: AU
C0.90
(95%
CI0
.84-0.94
). Sensitivity92.6%
(95%
CI,74
.2%-98.7%
),specificity
of77%
(95%
CI7
2.8%
to80.6%
),PP
V18
.7%(9
5%CI
12.7%to
26.5%
),NPV
99.5%
(95%
CI97.8%
-99.9%
)

49
Auth
ors
(yea
r), co
untry
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Luieta
l(201
4),66
Si
ngap
ore
Risk
of b
ias:
Unclear
Topropo
sean
inte
llige
nt
scor
ing
syst
em a
nd
exploretheuti
lity
ofcom
bining
Hea
rt
RateVariability
(HRV
)and
12-lead
EC
Gpa
rameters,
and
vita
l sig
ns to
pr
edic
t acu
te ca
rdia
c complicati
onsw
ithin
72h.
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
564(of
eligible702
)ch
est p
ain
patie
nts
aged
≥30
,tr
iage
d as
PA
CS 1
or
2, re
crui
ted
betw
een
Mar
ch
2010
-April
2012
at
theED
of1
ho
spita
l.
ESS (Propo
sed
Ensemble-Ba
sed
ScoringSystem
:combine
sHRV
and
12-
lead
ECG
param
eters,
andvitalsigns).
(Exclude
dbe
causeno
trouti
nem
easuremen
t)
DIST
(anEu
clidea
ndistan
ce-based
scoringsystem
):uses
HRVcombine
dwith
vitalsigns(E
xclude
dbe
causeno
trou
tine
mea
suremen
t)
MEW
S (m
odified
ea
rlywarning
score:
referencetoSub
beeta
l20
03)
TIM
I (thrombo
lysis
in
myocardialinfarcti
on:
referencetoAntman
et
al200
0)
(Exclude
dbe
cause
cond
ition
(MI)specific
score)
Compo
siteof
fourse
vere
complica
tions
with
in72hof
arriv
al a
t the
ED
:mortality,
card
iac
arre
st,
sust
aine
d ve
ntric
ular
ta
chyc
ardi
a,
and
hypo
tens
ion
requ
iring
inot
rope
s or
intra
aortic
balloon
pum
pinsertion
.
19(3
.4%)o
utofthe
remaining
564
pati
entsm
etth
eco
mpo
site
outc
ome.
M
EWS
Cut-o
ff:1.0
AU
ROC:0.67(0.54-0.81
) Sensitivity:4
2.1%
(19.9%
-64.3%
) Sp
ecificity:7
8.5%
(75.1%
-82.0%
) PP
V:6.4%(2
.1%-10.7%
) NPV
:97.5%
(96.0%
-99.9%
)

50Au
thor
s (y
ear),
coun
trySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/too
lRe
fere
nce
crite
riaRe
sults
Wils
on e
t al
(201
6),43UK
Ris
k of
bia
s:
High
Toevaluatethe
abilityofa
data-
fusio
nPatie
nt
StatusIn
dex(PSI)
todetectp
atien
tde
terio
ratio
ninth
eED
in
com
paris
on w
ith
documen
tedTT
San
dretrospe
ctively
calculated
TTS.
Prospe
ctive
coho
rt
(Validati
on)
472ad
ults
(≥18
)en
terin
g on
eofth
ree
clini
cal a
reas
ofth
eED
(re
suscita
tion
room
, ‘m
ajors’,
observati
on
ward);d
uring
timesth
ere
sear
ch
team
was
available
(daytim
e).
Vita
l sig
n an
d TT
S da
ta:h
eartra
te(H
R),
syst
olic
and
dia
stol
ic
bloo
dpressure(B
P),
resp
irato
ry ra
te,
perip
hera
l oxy
gen
saturatio
n(SpO
2),
tem
pera
ture
and
Gl
asgo
w C
oma
Scal
e (GCS
)score.P
aper
TT
S:clin
icianassig
ns
scor
e eT
TS:Foreach
seto
fman
ually
reco
rded
vita
l sig
ns,
TTSwasre
trospe
ctively
calc
ulat
ed P
SI:
referenceto
Tarassen
koeta
l(20
06);
para
met
ers:HR,
resp
irato
ry ra
te, B
P,
tem
pera
ture
, oxy
gen
saturatio
n
Escalatio
nof
care
PSI t
rue
aler
ts
Escalatio
naft
erEDarriv
al:3
5,ofw
hich20ha
dPSI
data,o
fwhich:
1. De
tected
byTT
S:4
2. De
tected
byeT
TS:1
7
3. De
tected
byPSI:15
4. De
tected
byeT
TS,n
otPSI:5
5. De
tected
byPSI,no
teTT
S:3
PSI f
alse
ale
rts
False
alertra
te:1
.13alerts/bed
-day(4
9false
alerts
from
39pa
tients).

51Ta
ble
11.Evide
ncetable:Develop
men
tand
validati
onstud
ies–
Pati
entg
roup
sdifferen
tiatedby(suspe
cted
)con
ditio
n(Risk
ofb
iasw
asra
tedusingatoolada
pted
from
Kan
sagaraeta
l(20
11).3
0 Fulld
etailsofth
eriskofbiasa
ssessm
enta
reavailableinApp
endix3.)
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Albrightet
al.(20
14),53
USA
Risk
of
bias:Low
Todesignan
em
erge
ncy
depa
rtm
ent s
epsis
sc
orin
g sy
stem
toid
entifyrisk
ofIC
Uadm
ission
in p
regn
ant &
po
stpa
rtum
w
omen
.
Retro
spective
coho
rt
(Develop
ment
&va
lidati
on)
850pregna
nt
&post-p
artum
wom
en w
ith
suspectedSIRS
or
seps
is ev
alua
ted
inEDofalarge
tertiarycare
hospita
lbetwee
nFeb20
09-M
ay
2011
.
Seps
is in
Obs
tetr
ics S
core
(S
OS):(Exclud
edbecau
se
itisacond
ition
(sep
sis)
specifictool)
MEW
S(Param
etersn
otstated
in
repo
rt.)
REM
S(Param
etersn
otstated
in
repo
rt.)
Prim
ary
outc
ome:ICU
adm
issio
n w
ithin
48
hrso
fED
presentatio
n.
Seco
ndar
y ou
tcom
es:
• te
lem
etry
un
it ad
miss
ion
•lengthof
hosp
ital s
tay
• m
orta
lity
•po
sitive
bloo
dcu
lture
s•po
sitive
influ
enza
swab
•antib
ioticuse
• ad
vers
e pe
rinat
al
outc
ome
9(1.1%)a
dmitted
toIC
U,32(3.8%)to
telemetryunit,mortality(0.0%).
Pr
imar
y ou
tcom
e: IC
U A
dmis
sion
pre
dicti
on
MEW
S(cut-off≥5
): Sensitivity:1
00.0%,Spe
cificity
:77.6%
,PPV
:4.6%
,NPV
:100
.0%
REMS(cut-off≥6
): Sensitivity:7
7.8%
,Spe
cificity
:93.3%
,PPV
:11
.1%,N
PV:9
9.7%
Se
cond
ary
outc
omes
Notre
ported
forM
EWSan
dRE
MS

52Au
thor
s (y
ear)
, co
untr
y
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Cild
ir et
al
(201
3),60
Turkey
Risk
of
bias
:Low
Toevaluatethe
mod
ified
Mortality
inEmergency
Depa
rtm
ent S
epsis
(M
EDS)sc
ore,
MEW
Sscorean
dCC
Itopred
ict
prog
nosis
in
patie
ntsp
resenti
ng
toEDdiagno
sed
with
seps
is.
Prospe
ctive
coho
rt
(Validati
on)
230pa
tients≥
18
who
pre
sent
ed to
ED
of1
hospital
betw
een7Au
g20
09-15Feb
2011
,diagn
osed
w
ith c
omm
unity
acqu
iredsepsis.
Char
lson
Com
orbi
dity
In
dex
(CCI
):pa
rameters
not s
tate
d in
repo
rt
MEW
S: p
aram
eter
s not
st
ated
in re
port
M
orta
lity
in e
mer
genc
y de
part
men
t sep
sis
(MED
S):exclude
dfrom
review
becau
seitis
cond
ition
(sep
sis)spe
cific
Mor
talit
yPr
edic
tion
of th
e m
orta
lity
in th
e gr
oup
with
se
psis
acc
ordi
ng to
28-
day
mor
talit
y (n
= 6
4)
(8 p
atien
ts d
ied)
CC
I(cut-o
ff>5
) Sensitivity50%
,Spe
cificity
85.4%
,PPV
33.3,
NPV
92.2,AUC0.65
(p=0
.18)
MEW
S(cut-off≤5
) Sensitivity87.5%
,Spe
cificity
30.4%
,PPV
15.2,
NPV
94.4,AUC0.57
(p=0
.48)
Pr
edic
tion
of th
e m
orta
lity
in th
e gr
oup
with
se
vere
seps
is a
ccor
ding
to 2
8-da
y m
orta
lity
(n=1
66) (
66 p
atien
ts d
ied)
CC
I(cut-o
ff>5
) Sensitivity78.8%
,Spe
cificity
38%
,PPV
45.6,
NPV
73.1,AUC0.62
(p=0
.006
) MEW
S(cut-off≤5
) Sensitivity48.5%
,Spe
cificity
67.0%
,PPV
49.2,
NPV
66.3,AURO
C0.60
(p=0
.04)
Pr
edic
tive
valu
e of
the
scor
es fo
r 28-
day
mor
talit
y
CCI(cut-o
ff>5
) Sensitivity27.0%
,Spe
cificity
93.0%
,PPV
64.5,
NPV
72.9,AURO
C0.65
(p=0
.001
) MEW
S(cut-off≤5
) Sensitivity43.2%
,Spe
cificity
75.0%
,PPV
45.1,
NPV
73.6,AURO
C0.61
(p=0
.008
)

53
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Cons
idin
e et
al
(201
5),78
Au
stra
lia
Toevaluatethe
effecto
fthe
staged
im
plem
entatio
nof
a Ra
pid
Resp
onse
Sy
stem
on
repo
rting
ofclin
ical
deterio
ratio
nin
EDpati
ents.A
se
cond
ary
aim
w
as to
det
erm
ine
iftherewere
diffe
rences
betw
een
patie
ntsw
ho
did,
and
did
not
, ex
perie
nce
clin
ical
de
terio
ratio
ndo
cum
ente
d du
ring
EDcare.
Retrospe
ctive
cross-
secti
onal
desig
n (Validati
on)
Stratifi
edra
ndom
sampleof600
ad
ultE
Dpa
tients
(≥18
yea
rs)
with
presenti
ng
complaintso
fshortnesso
fbreath,
ches
t pai
n or
ab
dominalpainin
a30
0-be
durba
ndistric
thospital.15
0pa
tientin
eachof4
grou
ps. F
our g
roup
s ac
cord
ing
to st
age
ofim
plem
entatio
n:
(T0)Clin
ical
decisio
nmaking/
discretio
n,noTT
Schart(year200
9);
(T1)Escalati
on
ofcareprotocol
(ifanycriti
cal
instab
ilitycriteria
met
, an
emer
genc
y ph
ysic
ian
shou
ld
revi
ew w
ithin
5m
in),no
TTScha
rt
(yea
r201
0);(T2
)Escalatio
nofcare
prot
ocol
, sin
gle
parameterTTS
chart(year201
1);
(T3)Escalati
onof
care
pro
toco
l, sin
gle
parameterTTS
chart(year201
2).
Criti
cal i
nsta
bilit
y cr
iteria
(E
D CI
C):
•Airw
ay/b
reathing
:St
ridor
, upp
er a
irway
ob
structi
on,o
rth
reat
ened
airw
ay,
SpO2<90
%(o
noxygen
10
L/m
inviam
ask),
Arteria
lblood
gasespH
<7.20
,Respiratoryra
te
<10
breaths/m
inor>
30
breaths/m
in
•Circulati
on:H
eartra
te
<50
beats/m
inor>
120
be
ats/min,Systolicblood
pressure<90mmHg
or>200
mmHg
,Urin
eou
tput<20mL/hor<
100mL/6h
•Disability:Sud
den
decr
ease
in
consciou
sness(fallin
Glas
gow
Com
a Sc
ale
score>2),R
epeatedor
prol
onge
d se
izure
s •Worrie
d?:P
atien
tswho
maynotm
eetthe
abo
ve
crite
riabuthavea
sudd
endeterioratio
nin
theirm
edicalcon
ditio
n,
requ
iring
urgen
tmed
ical
revi
ew.
Prim
ary
outc
ome:
Unreporte
dcli
nica
l deterio
ratio
n(=presenceof
docu
men
ted
phys
iolo
gical
abnorm
alities
thatfulfilled
theED
Clinica
lInsta
bility
Crite
ria in
ED
nursin
gno
tes a
nd n
o documentatio
nth
at th
ese
wer
e re
porte
d to
a
medica
lofficer.)
AtT0,86.7%
ofe
pisode
sofclin
ical
deterio
ratio
nwereun
repo
rted
.Acrossthe
fouryea
rsstud
ied,episode
sofu
nrep
orted
clinicaldeterioratio
nde
crea
sedby17.9%
from
T0
toT1(68.8%
),13
.5%from
T1toT2(55.3%
)bu
tonly1.3%
from
T2toT3(54.0%
);no
neof
thesediffe
renceswerestati
sticallysign
ificant
(p=0.14).
Patie
ntsw
hoexperienced
clin
ical
deterio
ratio
ninth
eED
weremorelikelyto
arriv
ebyambu
lance(p<0.001
),be
triagedto
AustralianTriageScalecategories1
or2
,(p<
0.00
1),and
had
a2.8hou
rlon
germ
edianED
leng
thofstay,an
dwere31
.9%m
orelikelyto
beadm
itted
tohospital(p<0.00
1).

54Au
thor
s (y
ear)
, co
untr
y
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Corfieldet
al(2
014)
81
(and
re
late
d conferen
ce
abstract
Corfieldet
al(2
012),49
Sc
otla
nd
Risk
of
bias:Low
Todetermine
whe
ther
a si
ngle
Nati
onalEarly
War
ning
Sco
re
(NEW
S)onED
ar
rival
is a
pre
dict
or
ofoutcomein
patie
ntsw
ith
seps
is, e
ither
in-hospitald
eath
in30da
ysorICU
ad
miss
ion
with
in 2
da
ys
Retrospe
ctive
coho
rt
(Validati
on)
3890
(74%
of5
285
eligiblepati
ents)
adultp
atien
ts,
>16yearso
fage,
atten
ding
EDwith
sepsis(suspe
cted
or
confi
rmed
with
in2
daysofa
ttend
ance
and2orm
oreof
sepsiscrite
ria).
20/25Scotti
sh
mainlan
dED
spa
rticipa
ted.
NEW
S(0-20score)
Parameters:
resp
irato
ry
rate,o
xygensaturatio
ns,
tem
pera
ture
, SBP
, pu
lse, c
onsc
ious
leve
l, supp
lemen
talO
2
ICUadm
ission
with
in 2
day
s ofatte
ndan
ce
atEDan
d30
-da
y m
orta
lity
(in-hospital).
Acombine
den
dpoi
nt
ofIC
U
admiss
ion/
and
or
mor
talit
y w
as
also
ass
esse
d.
Includ
edin
ana
lysis
:n=200
3
ICU(w
ithin2days):n
=113
(6.0%)
30-daym
ortality:n=297
(15.0%
) Co
mbine
d(IC
Uand
/orm
ortality):n
=376
(19.0%
) IC
U (w
ithin
2 d
ays)(C
ompa
redtoNEW
S0-4;
Adjusted
fora
ge)
NEW
SScore
5-6:OR1.22
(95%
CI0
.59-2.54
;p=0
.59)
7-8:OR2.01
(95%
CI1
.02-3.97
;p=0
.04)
9-20
:OR5.76
(95%
CI3
.22-10
.31;p=0
.00)
M
orta
lity
(30
days
) (Co
mpa
redtoNEW
S0-4;
Adjusted
fora
ge)
NEW
SScore
5-6:OR1.95
(95%
CI1
.21-3.14
;p=0
.01)
7-8:OR2.26
(95%
CI1
.42-3.61
;p=0
.004
) 9-20
:OR5.64
(95%
CI3
.70-8.60
;p=0
.00)
Co
mbi
ned
(ICU
and
/or m
orta
lity)(C
ompa
red
toNEW
S0-4;Adjustedfora
ge)
NEW
SScore
5-6:OR1.72
(95%
CI1
.14-2.60
;p=0
.01)
7-8:OR2.17
(95%
CI1
.45-3.25
;p=0
.00)
9-20
:OR5.78
(95%
CI4
.02-8.31
;p=0
.00)
Cu
t-offpo
intw
ithhighe
stYou
den’sInd
ex1 :
NEW
S9:
Sensitivity0.52,sp
ecificity0.77,PPV
0.35,NPV
0.88
,You
den’sind
ex0.30

55
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Geie
r et a
l (201
3),71
Ge
rman
y
Risk
of
bias:Low
(1)Toevalua
te
Emergency
SeverityInde
x(ESI),Mod
ified
Early
warning
Score
(MEW
S),M
ortality
inEmergency
Depa
rtm
ent S
epsis
(M
EDS)sc
ore
conc
erni
ng th
eir
diagno
sticaccuracy
todetectp
atien
ts
with
Sev
ere
Seps
is an
dSepti
cSh
ock
score(SSSS).
(2)Tode
term
ine
theprog
nostic
accuracyofind
ices
inpredicti
ngth
ein-
hosp
ital m
orta
lity
ofpati
entswith
su
spec
ted
seps
is in
ED
.(3)Tocalculatethe
prog
nosticvalue
ofth
eCh
arlso
nCo
morbidityIn
dex
(CCI).
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
151consecuti
ve
adultp
atien
tswith
su
spec
ted
seps
is ad
mitted
toEDof1
hospita
lbetwee
n1
Aug-30
Sep
t201
2.
Emer
genc
y Se
verit
y In
dex
(ESI
) (5levels;th
ehi
gher
the
leve
l the
low
er
themed
icalurgen
cy)
Level1=acutelife
threaten
edillp
atien
ts
-req
uireim
med
iate
initiati
onofd
iagn
ostic
san
d th
erap
y.
Level2=pati
entsin
high-
risksitua
tion-initia
tionof
diagno
sticsand
therap
yha
stostartw
ithin10m
in
follo
wingtheinitialtriage
asse
ssm
ent.
Hi
gher
leve
ls no
t specified
inre
port.
MEW
S(0-14)
Parameters:SBP,H
R,
Tempe
rature,respiratory
rate,LOC
CC
I Sco
re (0
-37)
Parametersn
otsp
ecified
in
repo
rt.
MED
S sc
ore
(Exclude
dbe
causeitisa
cond
ition
(sep
sis)spe
cific
score).
In-hospital
mor
talit
y45
.0%(n
=72)diagn
osed
with
SSSS;33.1%
(n=5
3)uncom
plicated
sepsis(w
ithou
torgan
dysfun
ction
).21
.9%(n
=26)nosepsis,butSIRS
orlo
callycon
fined
infecti
on.
In-h
ospi
tal m
orta
lity(14.6%
ofa
llpa
tients;
27.8%ofp
atien
tswith
SSSS)
ESI
Sensitivity0.73,Spe
cificity
0.0,P
PV0.17,NPV
0.90
MEW
S
Sensitivity0.43,Spe
cificity
0.74,PPV
0.21,
NPV
0.89
CCI
Sensitivity0.82,Spe
cificity
0.64,PPV
0.21,
NPV
0.94

56Au
thor
s (y
ear)
, co
untr
y
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
How
ell e
t al(2
007),55
USA
Risk
of
bias:Low
Tovalidate
the
Mor
talit
y inEmergency
Depa
rtm
ent S
epsis
(M
EDS)sc
ore,
theCo
nfusion,
Ureanitrog
en,
Resp
irato
ry ra
te,
Bloo
d pr
essu
re,
65yea
rsofa
ge
andolde
r(CU
RB-
65)score,and
a
mod
ified
Rap
id
Emergency
Med
icin
e Sc
ore
(mRE
MS)in
pa
tientsw
ith
suspectedinfecti
on.
Prospe
ctive
coho
rt
(Validati
on)
2132
adu
ltpa
tients
with
clin
ical
ly
suspectedinfecti
on
admitted
toan
urba
nED
betwee
n10
Dec200
3-3
0Sept200
4.
mRE
MS
poin
ts d
epen
d on
se
verit
y M
ean
arte
rial p
ress
ure
(mmHg)
Pu
lse ra
te
Resp
irato
ry ra
te
Perip
hera
l oxy
gen
saturatio
n Gl
asgo
w C
oma
Scor
e
Age
M
EDS
scor
e (Exclude
dbe
causeitisa
cond
ition
(sep
sis)spe
cific
score.)
CURB
-65
scor
e (Exclude
dbe
causeitisacond
ition
(com
mun
ity-acquired
pneu
mon
ia)spe
cific
score.)
28-day
in-hospital
surv
ival
(pati
ents
disc
harg
ed
alivefrom
th
e ho
spita
l be
fore28
days
wer
e co
nsid
ered
alivefor
the28
-day
in-hospital
mor
talit
y en
d po
int).
Of2
,132
pati
entswith
uniqu
efirstvisits,8
3(3.9%;9
5%CI3
.1%to
4.7%)d
ied.
m
REM
S
Odd
sofd
eathin
crea
sedby1.40(95%
CI=
1.28
to1.45)with
eachpo
intincrease.
AU
ROC0.80
(0.75-0.85
)
Joeta
l(201
3),73
Ko
rea
Risk
of
bias:Low
Tocom
pareth
epred
ictiv
evalueof
theVitalPAC
Early
Warning
Score-
Lactate(VIEWS-L)
scorewith
thatof
theTrau
maInjury
Seve
rity
Scor
e (TRISS).
Retrospe
ctive
coho
rt
(Validati
on)
299pa
tients,≥15
yearso
fage,w
ith
blun
ttraum
a,In
jury
severityscore≥9
in
a10
00-bed
urban
ho
spita
lbetwee
n1
Apr2
010-31
March
2011
.
VIEW
S-L
Para
met
ers:SBP,
HR, r
espi
rato
ry ra
te,
tem
pera
ture
, oxy
gen
saturatio
ns,inspired
oxyg
en, c
entr
al n
ervo
us
syst
em a
lert
ness
TRIS
S(Exclude
dbe
causeitisa
trau
ma-specifictool)
In-hospital
mor
talit
yVI
EWS-
L
High
ersc
oreinnon
-survivors(m
edian7.9,IQ
R6.2-12
.9)tha
nno
n-survivors(med
ian3.7,IQ
R1.7-5.5).
AURO
C:0.83(95%
CI0
.77-0.91
)

57
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Joeta
l.(201
6),72
Ko
rea
Risk
of
bias:Low
Toinvestigate
theprog
nostic
pred
ictio
npo
werof
new
ly in
trod
uced
ea
rly w
arni
ng
scoremod
ified
by
seru
m la
ctat
e le
vel,
theNati
onalEarly
War
ning
Sco
re
(UK)in
clud
ing
Lactate(NEW
S-L),
amon
gcommun
ity-
acqu
ired
pneu
mon
ia
patie
nts,and
co
mpa
red
with
pr
evio
usly
use
d to
ols s
uch
as
Pneu
mon
ia S
ever
ity
Inde
xan
dCU
RB-65.
Retrospe
ctive
coho
rt
(Validati
on)
553pa
tients,≥18
yearso
fage,w
ith
an a
dmiss
ion
diagno
sisofa
ny
type
ofp
neum
onia
betw
een1Oct
2013
-30Sept201
4in
1 h
ospi
tal.
NEW
S-L
scor
e Parameters:SBP,
HR, r
espi
rato
ry ra
te,
tempe
rature,SpO
2,LO
C,
supp
lem
enta
l oxy
gen,
la
ctat
e le
vel
CURB
-65
(Exclude
dbe
causeitisa
cond
ition
(com
mun
ity-
acqu
iredpn
eumon
ia)
specifictool)
Pneu
mon
ia S
ever
ity
Inde
x
(Exclude
dbe
causeitisa
cond
ition
(pne
umon
ia)
specifictool)
Inpa
tient
mor
talit
yMortalitybyNEW
S-Lscore:
≤3.0:2.2%
3.1≤an
d≤5.2:7.9%
5.3≤an
d≤8.0:9.6%
≥8
.1:2
3.9%
N
EWS-
L
AURO
C;0.73(0.66-0.80
);reference
Cu
t-off≥3
.1:Sen
sitivity95.0(86.1-99
.0)
Specificity27.6(23.7-31
.8)P
PV(%
)13.8(10.6-
17.5)N
PV(%
)97.8(93.8-99
.6)P
LR1.3(1
.2-
1.4)NLR:0
.2(0
.06-0.6)
Cu
t-off≥5
.3:Sen
sitivity76.7(64.0-86
.6)
Specificity53.8(49.2-58
.2)P
PV16.8(12.6-
21.8)N
PV95.0(91.7-97
.2)P
LR1.7(1
.4-2.0)
NLR0.4(0
.3-0.7)
Cut-o
ff≥8
.1:Sen
sitivity55.0(41.6-64
.9),
Specificity78.7(74.8-82
.2),PP
V23
.9(1
7.1-
31.9),NPV
93.5(90.7-95
.7),PLR2.6(1.9-3.4),
NLR0.6(0
.4-0.8)
Cut-o
ff≥7
.3:Sen
sitivity63.3(49.9-75
.4),
Specificity73.2(69.1-77
.1),PP
V22
.4(1
6.3-
29.4),NPV
94.3(91.4-96
.4),PLR2.4(1.9-3.0),
NLR0.5(0
.4-0.7)
NEW
S
AURO
C0.70
(0.63-0.77
);p=
0.03
Cu
t-off≥5
includ
ingredscore:Sen
sitivity68.3
(54.9-79
.4),Sp
ecificity57.2(52.7-61
.6),PP
V16
.3(1
2.1-21
.5),NPV
93.7(90.2-96
.1),PLR
1.60
(1.3-2.0),NLR0.55(0.4-0.8)

58Au
thor
s (y
ear)
, co
untr
y
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Jone
seta
l(200
5),56
USA
Risk
of
bias:Low
Thehypo
thesisof
this
stud
y st
ates
th
at
the
phys
iolo
gic
scor
ing
syst
ems
New
Sim
plified
Ac
ute
Phys
iolo
gy
ScoreII(SAP
SII),M
orbidity
Prob
abilityM
odel
(MPM
0II),and
LogisticOrgan
Dy
sfun
ction
System
(LODS
),whe
ncalculated
from
varia
blesavailable
durin
g th
e ca
re
ofcriti
callyillED
patie
nts,willnot
performwith
high
diagno
sticaccuracy
forp
redicti
ng
hosp
ital m
orta
lity,
de
fined
asa
nar
ea u
nder
the
receiverope
ratin
gcharacteristic
(ROC)
curve<0
.80.
Seco
ndar
y an
alysisofa
rand
omize
d co
ntro
lled
tria
l (Validati
on)
91(4
5%ofe
ligible
patie
nts)non
-trau
maED
pati
ents
admitted
toan
inte
nsiv
e ca
re u
nit,
>17yearso
fage,
with
initialEDvital
signs
con
siste
nt
with
shock(systolic
bloo
dpressure
<100
mmHgor
shockinde
x>1
.0),
and
with
agr
eem
ent
oftw
oinde
pend
ent
observersforat
leas
t one
sign
an
dsymptom
of
inad
equa
tetissue
pe
rfusion.
SAPS
II
MPM
0 II
LODS
N
o da
ta p
rovi
ded
on
incl
uded
par
amet
ers.
In-hospital
mor
talit
yTh
ein-hospitalm
ortalityratewas21%
(19/91
). SA
PS II
Mea
n40
(SD14
) Pred
ictedmortality28
%
AURO
C0.72
(0.57-0.87
) M
PM0
II Mea
n-1.06(SD1.24
) Pred
ictedmortality28
%
AURO
C0.69
(0.54-0.84
) LO
DS
Mea
n5(SD3)
Pred
ictedmortality30
%
AURO
C0.60
(0.45-0.76
) Usin
gon
lyEDvaria
blesto
calculateth
esc
ores
resu
lted
in a
ll th
ree
scor
ing
syst
ems
overestim
ating
in-hospitalm
ortalitybya
mea
nof8%(ran
ge,7
–10%
). Th
escoringsystem
sapp
eartofunctio
nmosta
ccuratelyinth
elowerriskgroup
for
eachsc
oringsystem
(SAP
SII≤5
0,LO
D≤7
,an
dMPM
0II≤0
)with
anaveragediffe
rence
betw
eenactualand
predicted
mortalityof
only3%.A
llthreeofth
escoringsystem
sgreatly
overestimated
mortalityinth
ehigh
erriskgroup
,with
anaveragediffe
rence
betw
eenactualand
predicted
mortalityof
31%.

59
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Ngu
yen
et
al(2
012),57
USA
Risk
of
bias
: Unclear
Toexaminethe
performan
ceof
thePred
isposition
,Insult/Infecti
on,
Resp
onse
, and
Organ
dysfunctio
n(PIRO)m
odel
com
pare
d w
ith th
e Ac
ute
Phys
iolo
gy
and
Chro
nic
HealthEvaluati
on
(APA
CHE)II
and
Mor
talit
y inEmergency
Depa
rtm
ent
Sepsis(M
EDS)
scor
ing
syst
ems
inpredicti
ngin
-ho
spita
l mor
talit
y forp
atien
ts
presen
tingto
the
emer
genc
y de
partmen
t(ED
)w
ith se
vere
seps
is orse
pticshock.
Prospe
ctive
coho
rt
(Validati
on)
541pa
tients,>17
yearso
fage,w
ho
met
the
crite
ria
forh
igh-Rsevere
sepsis(sep
siswith
lactate≥4
mmol/L)
orse
pticshockin
theED
.
PIRO
Parameters:
Ag
e, c
hron
ic li
ver d
iseas
e,
and/orcon
gestive
card
iom
yopa
thy
Infecti
on
Tachycardia/tachyopn
ea
Organ
dysfunctio
n AP
ACHE
IIre
ference
Knau
seta
l(19
85)
MED
S(M
ortalityin
EmergencyDe
partmen
tSepsis;re
ferenceSapiro
etal200
3)(E
xclude
dbe
causeitisacond
ition
(sep
sis)spe
cificto
ol)
In-hospital
mor
talit
y62
%(6
1.9)ofp
atien
tswerediagno
sedwith
septi
cshock;63.4%
,with
positiveculture;and
46
.9%,w
ithpositiveblood
culture.D
uring
thecourseofcare,31.8%
pati
entsdiedinth
eho
spita
l. PI
RO
Pred
ictedmortality:48.5%
(40.1an
d63
.9)
AURO
C:0.71(0.66-0.75
) AP
ACHE
II
Pred
ictedmortality:66%
(42an
d83
) AU
ROC:0.71(0.66-0.76
) Ac
tualm
ortalitysig
nifican
tlyin
crea
sedwith
increa
singPIRO
scoreinpati
entswith
eith
er
APAC
HEIIlessth
an25(P=0
.01)orA
PACH
EII
25orm
ore(P<0
.01).The
PIROcon
sistently
overestim
ated
actua
lmortalitywhe
nstratifi
ed
bylevelsofpredicted
mortality.

60Au
thor
s (y
ear)
, co
untr
y
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Vorw
erk
et
al(2
009),52
UK
Risk
of
bias
:Low
Todetermine
theeffi
cacyof
theab
breviated
Mor
talit
y in
Em
ergency
Depa
rtm
ent S
epsis
(M
EDS)sc
ore
(with
outn
eutrop
hil
band
s),the
MEW
Sscorean
dNPT
lactateinpredicti
ng
28-daym
ortalityin
adultE
Dpa
tients
with
seps
is.
Retrospe
ctive
coho
rt
(Validati
on)
307ad
ultE
Dpa
tients(>1
6years)
w
ith se
psis
admitted
to2
hospita
ls.Pati
ents
wer
e ex
clud
ed
ifpa
rametersto
calculatetheMEW
orM
EDSscorewere
miss
ing.
Mea
n ag
e 69
.7yea
rs
(95%
CI6
7.5to
71.8);51
%m
en.
MEW
S:5Param
eters:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e Ab
brev
iate
d M
EDS
(Exclude
dbe
causeitisa
cond
ition
(sep
sis)spe
cific
score)B
lood
lact
ate
Wasonlyrouti
nely
mea
suredinth
eED
of1
ofth
eho
spita
ls(n=158
)
28-day
mor
talit
yM
EWS
MEW
S≥5
Sensitivity:7
2.2%
(95%
CI6
0.4%
to82.1%
) Sp
ecificity:5
9.2%
(95%
CI5
2.6%
to65.5%
) Sign
ificantpredictorfo
rnon
-survival(OR3.76
;95
%CI2
.11to6.71).
AURO
C:0.72(0.67to0.77)
La
ctat
e Lactatelevelo
f≥4mmol/l
Sensitivity:4
9.1%
(95%
CI3
5.1%
to63.2%
) Sp
ecificity:7
4.3%
(95%
CI6
4.8%
to82.3%
) Sign
ificantpredictorfo
rnon
-survival(OR2.80
;95
%CI1
.39to5.57).
AURO
C:0.62(0.54to0.70)

61
Auth
ors
(yea
r),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/t
ool
Refe
renc
e cr
iteria
Resu
lts
Will
iam
s et
al.(20
16),7
7 Au
stra
lia
Risk
of
bias
:Low
(1)Tovalid
atea
numbe
rofseverity
ofillnesss
coresin
patie
ntsa
dmitted
w
ith p
resu
med
infecti
on;
(2)Tocompa
re
thepe
rforman
ce
ofsc
oresin
pa
tientsu
bgroup
sw
ith in
crea
sing
mortality:infecti
on
with
out s
yste
mic
infla
mmatory
resp
onse
sy
ndro
me,
seps
is,
seve
re se
psis
and
septi
cshock
Prospe
ctive
coho
rt
(Validati
on)
8,87
1pa
tients
admitted
with
presum
edinfecti
on,
>17yearso
fage,to
EDof1
met
ropo
litan
ho
spita
lin16
0wee
ksin
2periods:
Oct200
7-De
c20
08
(pilo
t)and
June
20
09-M
ay201
1(fu
nded
).
Sim
plifi
ed A
cute
Ph
ysio
logy
Sco
re II
(SAP
S II)
Parameters:
Age
, chronicdisease,ty
peof
adm
issio
n, G
CS, t
emp,
BP,H
R,FiO
2/PaO
2/Aa
grad
ient,b
icarbo
nate,
sodi
um, p
otas
sium
, WBC
, bilirub
in,u
rea,urin
eou
tput
. Se
quen
tial O
rgan
Fai
lure
As
sess
men
t (SO
FA)
Parameters:
GCS
, BP,
vasopressoru
se,FiO
2/PaO
2/Aa
gradien
t,platelets,bilirubin,
creatin
e,urin
eou
tput.
Acut
e Ph
ysio
logy
an
d Ch
roni
c He
alth
Ev
alua
tion
II (A
PACH
E II)
sc
ore
Parameters:
Age
, chronicdisease,ty
peof
adm
issio
n, G
CS, t
emp,
BP,H
R,FiO2/PaO2/Aa
gr
adie
nt, p
H, re
spira
tory
ra
te, s
odiu
m, p
otas
sium
, W
BC, h
aem
atoc
rit,
creatin
ine,re
nalfailure.
Seve
re S
epsi
s Sco
re (S
SS)
(Exclude
dbe
causeitisa
cond
ition
(sep
sis)spe
cific
score)
M
orta
lity
in E
D Se
psis
Sc
ore
(MED
S)(E
xclude
dbe
causeitisacond
ition
(sep
sis)spe
cificsc
ore)
30-day
mor
talit
y30
-daym
ortality:3.7%.
Allscoreso
verestimated
mortality.
Scoresin
ICUse
tting
soverestimated
mortality
inED.
AU
ROC
(95%
CIs
) for
Sco
res,
by
Seps
is
Subg
roup
s AP
ACHE
II
EntireCo
hort=0.90(0.88–
0.91
) Sepsis:0.86(0.84–
0.88
) SevereSep
sis:0
.79(0.76–
0.83
) Septi
cSh
ock:0.79(0.74–
0.84
) ICU:0
.77(0.67–
0.87
) SA
PSII
En
tireCo
hort:0
.90(0.89–
0.92
) Sepsis:0.88(0.86–
0.90
) SevereSep
sis:0
.82(0.78–
0.85
) Septi
cSh
ock:0.82(0.78–
0.87
) ICU:0
.80(0.71–
0.88
) SO
FA
EntireCo
hort:0
.86(0.84–
0.88
) Sepsis:0.83(0.80–
0.86
) SevereSep
sis:0
.78(0.75–
0.82
) Septi
cSh
ock:0.74(0.68–
0.79
) ICU:0
.74(0.65–
0.84
)

62Ta
ble
12.Evide
ncetable:Develop
men
tand
validati
onstud
ies–
Und
ifferen
tiatedpa
tientgroup
s(Risk
ofb
iasw
asra
tedusingatoolada
pted
from
Kan
sagaraeta
l(20
11).3
0 Fulld
etailsofth
eriskofbiasa
ssessm
enta
reavailableinApp
endix3.)
Auth
ors (
year
), co
untr
ySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/to
olRe
fere
nce
crite
riaRe
sults
Burc
h et
al
(200
8),45
Sou
th
Afric
a
Risk
of b
ias:
High
Toevaluatetheuse
ofth
eMod
ified
Early
Warning
Score(M
EWS)as
a tr
iage
tool
to
iden
tifymed
ical
patie
ntsp
resenti
ng
to th
e em
erge
ncy
depa
rtm
ent w
ho
requ
ireadm
ission
to h
ospi
tal a
nd a
re
atin
crea
sedriskof
in-hospitald
eath.
Prospe
ctive
coho
rt
(Validati
on)
790(70.2%
of
thepo
tenti
al
stud
ycoho
rt)
med
ical
patie
nts(no
tsu
rgica
l, or
thop
aedi
c,
gyna
ecol
ogica
l or
trau
ma
related)
presen
ting
toEDofan
urba
npu
blic
hosp
ital.
MEW
S: P
aram
eter
s:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e
Adm
issio
n to
hos
pita
l, in-hospital
mor
talit
y
MEW
Sscoremed
ian3(ra
nge0-11
);26
.0%had
MEW
Sscore≥5.
Hosp
ital a
dmis
sion
Increa
sedad
miss
ionwith
increa
singMEW
S(trend
P-value<0
.001
). MEW
S0–
2(45%
;ref)
MEW
S3–
4(59%
;RR1.3;95%
CI1
.1to
1.6)
MEW
S≥5
(79%
;RR1.7;95%
CI1
.5to
2.0)
In-h
ospi
tal m
orta
lity
Increa
sedmortalitywith
increa
singMEW
S(trend
P-value<0
.001
). MEW
S0–
2(5%;ref)
MEW
S3–
4(16%
;RR2.8;95%
CI1
.7to
4.8)
MEW
S≥5
(26%
;RR4.6;95%
CI2
.7to
7.8)

63
Auth
ors (
year
), co
untr
ySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/to
olRe
fere
nce
crite
riaRe
sults
Dund
ar e
t al
(201
5),79
Turkey
Risk
of b
ias:
Low
Theaimofthis
stud
y w
as to
ev
alua
te th
e va
lue
ofth
eMod
ified
Early
Warning
Score(M
EWS)
and
the
Vita
lPac
Early
Warning
Score(VIEWS)
inpredicti
ng
hospita
lizati
on
andin-hospital
mor
talit
y in
ge
riatr
ic e
mer
genc
y de
partmen
t(ED
)pa
tients.
Prospe
ctive
coho
rt
(Validati
on)
671(all)
patie
nts(aged
≥6
5years)
presen
ting
toth
eED
of
1260
-bed
ho
spita
l be
twee
n15
Janu
ary
2014
and
15
Feb
ruary
2014
.
MEW
S Pa
ram
eter
s:
resp
irato
ry ra
te, S
BP,
HR,Tem
p,AVP
U
VIEW
SPa
ram
eter
s:
resp
irato
ry ra
te, S
BP,
HR,Tem
p,oxygen
saturatio
n,in
haled
oxygen
,AVP
U
Hospitalizati
on
&in-hospital
mor
talit
y
187(27.9%
)adm
itted
toaward
153(22.8%
)weread
mitted
toIC
U4(0.6%)p
atien
tsdieddu
ringthefollo
w-upatth
eED 8.5%
in-hospitalm
ortalityrate
Hosp
italis
ation
MEW
S(opti
malcut-off:3)
AURO
C:0.73(95%
CI0
.69–
0.77
)Sensitivity:4
2%,Spe
cificity
:89%
LR+:3.7,LR−
:0.7
VIEW
S(opti
malcut-off:6)
AURO
C:0.76(95%
CI0
.72–
0.79
)Sensitivity:5
6%,Spe
cificity
:85%
LR+:3.8,LR−
:0.5.
In-h
ospi
tal m
orta
lity
MEW
S(opti
malcut-off≥4
)AU
ROC:0.89(95%
CI0
.84–
0.94
)Sensitivity:7
4%,Spe
cificity
:89%
LR+:6.7,LR−
:0.3
VIEW
S(opti
malcut-off:≥8)
AURO
C:0.90(95%
CI0
.86–
0.94
)Sensitivity:8
4%,Spe
cificity
:83%
LR+:4.9,LR−
:0.2.
Therewasnostati
sticald
ifferen
cebetwee
nAU
ROC
ofM
EWS&VIEWSinpredicti
nghospitalizati
onand
in-hospitalm
ortality(P=0
.28an
d0.82
).

64Au
thor
s (ye
ar),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/
tool
Refe
renc
e cr
iteria
Resu
lts
Eicketa
l(201
5),70
Ge
rman
y
Risk
of b
ias:
Low
Toevaluatehe
art
ratedecelerati
on
capa
city
, an
electrocardiog
ram-
basedmarkero
fau
tono
mic
ner
vous
system
acti
vity,as
risk
pred
icto
r in
a m
edic
al e
mer
genc
y de
part
men
t and
to
test
its i
ncre
men
tal
pred
ictiv
evalueto
theMod
ified
Early
War
ning
Sco
re
(MEW
S).
Prospe
ctive
coho
rt
(Validati
on)
5730
consecuti
ve
patie
nts
≥18years
admitted
toEDof1
hosp
ital o
ver
a 22
mon
th
perio
d an
d in
sin
us rh
ythm
.
MEW
S
Parameters:
re
spira
tory
rate
, SBP
, HR
,Tem
p,LO
CatED
adm
issio
n
Hear
t rat
e va
riabi
lity
(dec
eler
ation
ca
paci
ty) (exclud
ed
becauseno
trou
tine
assessmen
t)
Prim
ary
outc
ome:
intra-ho
spita
lm
orta
lity
Seco
ndar
y ou
tcom
e:
tota
l m
orta
lity
at
30and
180
da
ys,transfer
toIC
Uduring
hosp
ital s
tay
Admiss
iontoIC
U(%
)n=3
66(6
.4%)
In-hospitald
eaths:n=1
42(2
.5%)
Deathsat3
0da
ys:n
=196
(3.4%)
Deathsat1
80days:n=4
36(7
.6%)
Mea
n(SD)M
EWSSu
rvivors2
.3±1
.4vsN
on-
survivorsM
EWS=5.0±1
.7(p
<0.00
1)
In-h
ospi
tal m
orta
lity:
MEW
S:
AURO
C:0.71(0.67–
0.75
;p<0.00
1)
Adjusted
OR1.14
(95%
CI1
.09–
1.19
) Se
cond
ary
outc
omesnotre
ported
forM
EWS.
Grah
am e
t al
(200
7),63
Hon
g Ko
ng
Risk
of b
ias:
Unclear
(Con
ference
abstractonly)
Tovalidatetheuse
ofaM
odified
Early
War
ning
Sco
re
(MEW
S)in
EDto
iden
tifypa
tients
atriskofserious
illne
ssre
quiring
ho
spita
l adm
issio
n.
Prospe
ctive
coho
rt
(Validati
on)
413pa
tients
(96.5%
of
eligible
patie
nts)
admitted
to
a16
-bed
ED
observati
on
wardof1
hosp
ital.
MEW
S
Parameters:
re
spira
tory
rate
, SBP
, HR
,Tem
p,LO
C
Inpa
tient
hosp
ital
adm
issio
n,
reatt
enda
nce
atEDwith
in
48 h
rs re
late
d toin
dexof
diag
nosis
aft
er
discha
rge,30
day
mor
talit
y.
Admitted
:46
Reatt
ende
dwith
in48hrso
fdisc
harge(4re
quire
dad
miss
ion):1
0
Deceased
30da
ys:2
MEW
Sscore>4
: •Increa
sedne
edfo
rhospitaladm
issionOR8.3:
95%CI=1.1-60.4,p=0
.013
) •Increa
sedED
reatt
enda
ncewith
in48hrs(OR
45.2:9
5%CI=3.4to568
.9,p
<0.00
01)(Limite
dinform
ation
;abstracto
nly)

65
Auth
ors (
year
), co
untr
ySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/to
olRe
fere
nce
crite
riaRe
sults
Heitz
et a
l (201
0),54USA
Risk
of b
ias:
Low
Exam
inethe
performan
ce
characteristic
sand
di
scrim
inat
ory
abilityofthe
most
abno
rmalM
odified
Early
Warning
Score
(MEW
S)(M
EWS
Max)scoreduring
theen
tireED
stayin
pred
ictin
gthene
ed
forh
ighe
rlevels
ofcaream
ongED
pa
tientsp
resenti
ng
toate
rtiarycare
facility.
Retrospe
ctive
coho
rt
(Validati
on)
280of500
ra
ndom
ly
sele
cted
chartsof
allp
atien
ts
presen
ting
toth
eED
of
one
Med
ical
Ce
nter
in
2005
.
Adap
ted
MEW
S (M
EWS
Max
):Pa
ram
eters:SBP,
pulse
rate
, res
pira
tory
ra
te, t
empe
ratu
re,
Glas
gow
Com
a Sc
ale
(GSC
).M
EWS
plus:
Parameters:M
EWS
max,age60,ra
ce,
gend
er,EDleng
thof
stay,m
etho
dofarrival,
andan
tibiotic
sgiven
priortoorduringED
vi
sit.
Com
posit
e of:N
eedfor
high
erlevelo
fcare(d
efine
dasin
itial
adm
issio
n from
theED
ortran
sfer
with
in 2
4 ho
urs t
o a
non-flo
orbed
(acutecare,
inte
rmed
iate
ca
re u
nit,
orcriti
cal
careunit)
or m
orta
lity
with
in 2
4 ho
urso
fED
presen
tatio
n.
27%(7
6/28
0)m
etcom
positeou
tcom
eofdeath
(n=1
)orn
eedforh
ighe
rcare(n=7
5).
MEW
S M
ax
TheMEW
SMaxwassign
ificantlyassociated
with
theprim
arycompo
siteou
tcom
e(P<0.001
,Co
chran-Armita
getren
dtest).
Opti
mum
thresholdMEW
SMax:≥
4
Sensitivity:6
2%(9
5%CI5
0-73
) Sp
ecificity:7
9%(9
5%CI7
3-84
) PP
V:52
NPV
:85
AURO
C0.73
(95%
CI,0.66
-0.79)
Each1-pointin
crea
sein
theMEW
SMaxsc
ore
associated
with
a60%
increa
sein
theod
dsof
mee
tingthecompo
siteen
dpoint(O
R1.6;95%
CI,
1.3-1.8).
MEW
S Pl
us
AURO
C0.76
(95%
CI,0.69
-0.82)
In58cases(21
.7%),usingMEW
SPluswou
ldhave
placed
pati
entsin
am
oreap
prop
riateriskcategory
than
MEW
SMax,w
hile5.6%ofcaseswou
ldhave
resulte
dinin
approp
riatere
classifi
catio
n.

66Au
thor
s (ye
ar),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/
tool
Refe
renc
e cr
iteria
Resu
lts
Junh
asavasdiku
etal(20
12),7
4 Th
ailand
Risk
of b
ias:
Unclear
Todetermine
whe
ther
adm
issio
n de
lay(le
ad-time)
andothe
rfactors
are
asso
ciat
ed w
ith
hosp
ital m
orta
lity
rateso
femergency
med
icalpati
ents.
(Mod
ified
Early
War
ning
Sco
re
(MEW
S)dataused
inth
issynthe
sis).
Prospe
ctive
coho
rt
(Validati
on)
381pa
tients,
>15years
ofage,
presen
tingto
EDbetwee
nAu
g-Nov
2009
,and
ad
mitted
to
med
ical
wardsofa
tertiaryurba
nca
re c
entr
e,
incl
udin
g in
tens
ive
care
un
its.
MEW
S: P
aram
eter
s:
SBP,
pul
se ra
te,
resp
irato
ry ra
te,
tempe
rature,A
VPU
scor
e
Mor
talit
y Overallmortalityratewas8.9%.
MEW
SatEDwasassociatedwith
mortality
(p<0
.001
):Non
-survivorsm
edian4(ran
ge1-10),
survivorsm
edian2(ran
ge0-11)
Nai
doo
et a
l (201
4),44
Sou
th
Afric
a
Risk
of b
ias:
Hi
gh
Toevaluatethe
useofth
eTriage
Early
Warning
Score(TEW
S)by
heal
thca
re w
orke
rs
inanED
inalarge
urba
nho
spita
lin
KwaZulu-Natal,and
itsabilitytoid
entify
patie
ntsw
ho
requ
ireadm
ission
and
at in
crea
sed
riskforin-ho
spita
lm
orta
lity.
Retrospe
ctive
coho
rt
(Validati
on)
265pa
tient
reco
rds i
n an
ED
of1
urban
ho
spita
l.
TEW
S :
Parameters:
Mob
ility,R
estin
grate,
HR,SBP,A
VPU,Traum
a
Disc
harg
e w
ithin
24
hourso
fad
miss
ion,
ad
miss
ion
to a
war
d,
adm
issio
n to
an
inte
nsiv
e ca
re u
nit
(ICU),an
dde
ath
in
hosp
ital.
47.6%weread
mitted
towardsand
3(1
.1%)
admitted
toIC
U;4
pati
ents(1
.5%)d
iedwith
in24
hourso
fadm
ission.
23
3(87.9%
)had
aTEW
S<7,while32(12.1%
)had
aTEWS≥7.
Asig
nifican
tassociatio
nbe
twee
ntheTEWS
catego
ryand
outcomewasestab
lishe
d(node
tails
ofsign
ificancetestsp
rovide
d):
53.7%ofp
atien
tswith
aTEW
Sof<7were
discha
rged
,com
paredto18.7%with
asc
ore≥7
who
weredischa
rged
.Nopa
tientsinthelow-score
catego
ryweread
mitted
toIC
U.Nopa
tientsd
ied.
Threepa
tientsw
eread
mitted
toIC
U,and
fourdied
inth
ehigh
-scorecategory.

67
Auth
ors (
year
), co
untr
ySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/to
olRe
fere
nce
crite
riaRe
sults
Olss
onet
al(2
003),67
Sw
eden
Risk
of b
ias:
Low
(1)C
ouldth
eabbreviated
severityofdise
ase
classificatio
nsy
stem
Rap
id A
cute
Ph
ysio
logy
Sco
re
(RAP
S),created
for
useinth
eou
t-of-
hospitalsetti
ng,
beusefulin
the
EDfo
rpredicting
in-hospitalm
ortality
andthelengthof
hospitalstay(LOS)
in n
onsu
rgica
l patie
nts?(2)Isit
possibleto
mod
ify
RAPS
to p
rovi
de
a m
ore
pote
nt
scoringsystem
(the
Ra
pidEm
ergency
Med
icine
Sco
re
[REM
S])b
yinclu
ding
ag
e an
d on
e or
tw
o pa
ram
eter
s easilyob
tained
by
mod
ern
tech
nolo
gy
(oxygenatio
nand
bodyte
mpe
rature)
forthe
purpo
seof
pred
ictingin-hospital
mortality?(3)C
ould
REMS,with
its
simplicityand
fewer
varia
bles,perform
as
wellasA
PACH
EIIin
theno
nsurgicalED?
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
1027
adu
ltno
nsur
gica
l pa
tientsw
ere
recr
uite
d from
two
sources:185
no
nsur
gica
l, critically
illpati
ents
referred
to
theICUfrom
1Nov199
5-1
Nov199
6,and
88
5pa
tients
at th
e no
nsur
gica
l ED
who
were
admitted
ei
ther
to
an o
rdin
ary
med
ical
de
part
men
t (n=758
),to
a g
ener
al
ICU(n
=9),
to a
cor
onar
y careunit(n
=84
),orto
a
neuro-ICU(n
=15
)betwee
n1Jan19
96-1
March199
6.
Mod
el V
alid
ation
AP
ACHE
II
Parameters:
te
mpe
ratu
re, m
ean
arte
rial p
ress
ure,
HR,
oxygen
ation
ofarterial
bloo
d(PaO
2),arterial
pH, s
erum
sodi
um,
seru
m p
otas
sium
, serumcreatin
ine,
haem
atoc
rit, w
hite
bloo
dcellc
ount,and
GC
Sscore.(A
rterialpH
was
not
use
d in
the
scoringsystem
because
thisvaria
bleis
notm
easuredrouti
nely
inth
eED
.) RA
PS
Parameters:
HR, B
P, re
spira
tory
rate
, and
GC
S sc
ore.
+pe
riphe
raloxygen
saturatio
n(0–4points),
bodytempe
rature(0–4)
and
age
wer
e ad
ded
to
thefourRAP
Svaria
bles.
Mod
el d
evel
opm
ent
REM
S(based
onbe
st
pred
ictorso
fRAP
S)
Parameters:
com
a,
respiratoryfreq
uency,
oxygen
saturatio
n,BP,
andHR
(maxim
alscore
being4fora
ll)and
age
(maxim
alscorebe
ing
6).
In-hospital
mor
talit
yMortalityof116
(11%
). RE
MS
Likelih
oodratio
chi-squ
arevalueof318
.7(p
<
0.00
01)
OR1.58
(95%
CI1
.48to1.70).
AURO
C:0.91+/-0
.02(had
asu
perio
rdisc
riminati
ng
powercom
paredtoRAP
S(p<0
.001
)) RA
PS
Likelih
oodratio
chi-squ
arevalueof273
(p<0
.000
1)
OR1.77
(95%
CI1
.62to1.93).
AURO
C:0.87+/-0
.02
APAC
HE II
Likelih
oodratio
chi-squ
arevalueof278
.5(p
<0
.000
1)
OR1.25
(95%
CI1
.21to1.29).
AURO
C:0.90+/-0
.02(nosig
nifican
tdifferen
cewith
RE
MS)

68Au
thor
s (ye
ar),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/
tool
Refe
renc
e cr
iteria
Resu
lts
Olss
onet
al(2
004),68
Sw
eden
Risk
of b
ias:
Low
(1)C
ouldth
eab
breviated
severityofdise
ase
classifi
catio
nsy
stem
Rap
id A
cute
Ph
ysio
logy
Sco
re
(RAP
S),created
tobeused
inth
epre-ho
spita
lsetti
ng,
beusefulinthe
EDto
predictin
-ho
spita
l mor
talit
y an
d ho
spita
l len
gth
ofstay(LOS)
in n
onsu
rgic
al
patie
nts?;(2)Isit
possibleto
mod
ify
RAPS
to p
rovi
de
amorepo
werful
scoringsystem
for
med
icalpati
ents
(Rap
idEmergency
Med
icin
e Sc
ore,
RE
MS)to
predictin
-ho
spita
l mor
talit
y?
Prospe
ctive
coho
rt
(Develop
ment
&Validati
on)
1175
1no
nsur
gica
l pa
tients
presen
ting
toth
eED
du
ring
12
consecuti
ve
mon
ths.
RAPS
Parameters:blood
pr
essu
re, r
espi
rato
ry
rate
, pul
se ra
te a
nd
Glas
gow
com
a sc
ale
Mod
el D
evel
oped
RE
MS(based
on
significan
tpredictors
ofRAP
S)
Parameters:
com
a,
respira
toryfreq
uency,
oxygen
saturatio
n,
bloo
dpressureand
pu
lsera
te(m
axim
al
scorebe
ing4fora
ll)
andage(m
axim
al
scorebe
ing6)
In-hospital
mor
talit
y Mortality:n=2
85
RAPS
Likelih
oodratio
chi-squ
arevalueof261
.2(P
<
0.00
01)
OR1.47
(95%
CI:1.41
–1.54).
AURO
C:0.65±0.02
RE
MS
Likelih
oodratio
chi-squ
arevalueof487
.3(P
<
0.00
01)
OR1.40
(95%
CI:1.36
–1.45)
AU
ROC:0.85±0.01
;sup
eriord
iscrim
inati
ngpow
er
compa
redwith
RAP
S(P<0.001
)

69
Auth
ors (
year
), co
untr
ySt
udy
aim
Stud
y de
sign
(t
ype)
Parti
cipa
nts
Cont
ent o
f sys
tem
/to
olRe
fere
nce
crite
riaRe
sults
Subb
eetal
(200
6),51UK
Risk
of b
ias:
Low
Toestab
lish
afreq
uency
distrib
ution
for
typi
cal p
hysio
logi
cal
scor
ing
syst
ems
andtoestab
lishthe
potenti
alben
efit
ofadd
ingtheseto
anexisting
triage
syst
em in
acc
iden
t an
d em
erge
ncy
depa
rtm
ents
.
Retrospe
ctive
coho
rt
(Validati
on)
Grou
p1:53
unse
lect
ed
patie
nts
presen
ting
atEDintw
osamplesof
consecuti
ve
patie
ntso
n30
and
31Oct
2003
. Grou
p2:
49dire
ct
adm
issio
ns
from
ED
toth
eICU
admitted
be
twee
n1
April-31Oct
2003
. Grou
p3:
49pati
ents
admitted
to
ED,w
howere
tran
sferred
to a
gen
eral
m
edic
al o
r su
rgic
al w
ard
and
then
ad
mitted
to
ICUbetwee
n1Ap
ril-31Oct
2003
. Totalo
f151
pa
tients.
MEW
S (M
odified
Early
Warning
Score):
Parameters:
SBP
, pu
lse ra
te, r
espi
rato
ry
rate
, tem
pera
ture
, AV
PUsc
ore
ASSI
ST
(Assessm
entS
core
forS
ickpa
tient
Iden
tificatio
nan
dStep
-upinTreatmen
t)
Parameters:
SBP
, pul
se
rate
, res
pira
tory
rate
, levelo
fcon
sciousne
ss
(ACD
Nsc
ore),age.
MET
(Med
ical
EmergencyTeam
) Crite
riafo
rthe
call-
outo
faM
ETbased
on
Airw
ay, B
reat
hing
, Circulati
on,D
isability
asse
ssm
ent.
Nur
sing
staff
areasked
to
callou
tsen
iorstaffif
bedsideob
servati
ons
arebe
lowora
bove
defin
edth
resholdsfo
rbloo
dpressure,h
eart
rate
, res
pira
tory
rate
&
levelo
fcon
sciousne
ss,
orifworrie
dab
outa
pa
tient.
Existi
ngtriagesy
stem
: M
TS(M
anchester
TriageSystem)
Usesp
rotocolsba
sed
onth
epresen
ting
com
plai
nt a
nd
questio
nsabo
ut
aggravati
ngfa
ctors.
Criticallyill
(defi
nedas
MEW
S>2
,AS
SIST>3an
dMETcriteria
applicab
le,
with
MTS
cate
gorie
s or
ange
or
red).
Patie
ntside
ntifie
dascriti
callyill(atriskof
deterio
ratio
n):
MTS(o
rang
eorre
d)
Grou
p1:Sen
sitivity15%
Grou
p2:Sen
sitivity96%
Grou
p3:Sen
sitivity65%
M
EWS(>2)
Grou
p1:Sen
sitivity8%
Grou
p2:Sen
sitivity77%
Grou
p3:Sen
sitivity55%
AS
SIST(>
3)
Grou
p1:Sen
sitivity0%
Grou
p2:Sen
sitivity22%
Grou
p3:Sen
sitivity16%
M
ET(=
1)
Grou
p1:0
Grou
p2:Sen
sitivity2%
Grou
p3:Sen
sitivity7%

70Au
thor
s (ye
ar),
coun
try
Stud
y ai
mSt
udy
desi
gn
(typ
e)Pa
rtici
pant
sCo
nten
t of s
yste
m/
tool
Refe
renc
e cr
iteria
Resu
lts
Wan
g et
al
(201
6),75
Taiwan
Risk
of b
ias:
Unclear
Toevaluatewhe
ther
peri-arrestM
odified
ea
rly W
arni
ng S
core
(M
EWS)cou
ldbea
prog
nosticfactorin
in-hospitalcardiac
arrest(IHC
A).
Tocom
bine
pre-
arrestcom
orbidity
factors(Ch
arleson
ComorbidityIn
dex,
CCI),peri-a
rrest
physiologicalfactors
(MEW
S)and
arrest
factorstoevalua
te
theou
tcom
eof
IHCA
inED.
Retrospe
ctive
coho
rt
(Validati
on)
99non
-trau
mati
c,>20
yearso
fage,
patie
ntsE
Drecordso
fone
ho
spita
l ove
r 30
mon
ths
perio
d.
Char
lson
Com
orbi
dity
In
dex
1-6po
intsallo
catedby
morbidity.
Peri-
arre
st M
EWS
Temp,BP,HR,
Respira
toryRate,LoC
(AVP
U)fromtriageto
0.5h
rsprio
rtoarrest
(peri-a
rrestM
EWS)
In-hospital
card
iac
arre
st,
Surv
ival
to
disc
harg
e (STD
G)
LowerCCIin
STD
Ggrou
p(n=2
2)th
anm
ortality
grou
p(n=7
7)(2
.27±
1.87
vs3
.87±
2.83
;p=0
.001
) Nosig
nifican
tdifferen
cein
MEW
Sattriage
betw
eenSTDG
vsm
ortalitygrou
p(3.42±
2.2vs4
.02
±2.65
;p=0
.81)
LowerperiarrestM
EWSinSTD
Gvsm
ortalitygrou
p(4.41±
2.28vs5.82±2.84
;p=0
.05)
Su
rviv
al to
dis
char
ge
CCI
Adjusted
OR0.57
(95%
CI0
.38-0.84
);p=
0.00
5
Peri-arrestM
EWS
Ad
justed
OR0.77
(95%
CI0
.60-0.97
);p=
0.02
8

71
4.3.6 Health economics WedidnotidentifyanyformalevaluationsthatexaminethecosteffectivenessofearlywarningsystemsorTTSorotherscoringsystemsinhospitalEmergencyDepartments.Whileitisclearthatimplementingearlywarning systems requires ahealthcare resource investment, thedegree towhich such systemsmay or may not result in cost savings elsewhere in the healthcare system, or in improved patientoutcomes,remainsunclear.Asdescribedearlierinthisreport,thelimitedevidencebasesuggeststhatearlywarningsystemsareeffectivein,forexample,identifyingdeterioratingpatients,reducingcardiacarrestsandreducingintensivecareunitadmissions.Shouldtheseeffectsexist,thepotentialhealthcarecostsavingscouldgotofund,atleasttosomedegree,theimplementationofearlywarningsystemsinEDclinicalpractice.Whilethistheoryisopentoquestion,itdoesgotohighlighttheneedforprimaryresearchstudiestobeconductedtodirectlyevaluatethecosteffectivenessofearlywarningsystems.Suchstudiesshouldfocusonthemonitoringofresourceuse,costsandpatientoutcomes inordertodeterminewhetherearlywarningsystemsarelikelytodelivergoodvalueformoney.

72
Conclusion
Implications for practiceFive objectives were addressed in this review. The first objective was to describe the use of earlywarningsystemsintheED.MultipleearlywarningsystemswereidentifiedbuttheextenttowhichtheyareusedintheEDseemstovaryindifferentcountriesfromwhichdatawasavailable(UKandAustralia).Ten descriptive studies included in this review demonstrated that the use of early warning systemsinEDwas linkedwithan increase inescalationprotocolactivation,but incorrectcalculationofscoreswas common. Compliance with recording early warning system scores was relatively low, althoughthevital signsHRandBPwereusually recorded.Thisfindingemphasises the importanceofeffectiveimplementationstrategies.However,wedidnotidentifyanystudiesexaminingeducationalprogrammesforearlywarningsystems(objective5).Existingguidelinesregardingtheuseofearlywarningsystemstomonitoracutepatientsinhospitaldidincludeeducationaltools,butwerenotspecifictotheED.Thethreeguidelinesweidentifiedallrecommendinclusionofthefollowingsixparameters:respiratoryrate,heartrate,systolicbloodpressure,temperature,oxygensaturations,andlevelofconsciousness.
Evidence from35 validation and development studies, assessing 27 different systems, demonstratedthatearlywarningsystemsusedinEDsettingsseemtobeabletopredictadverseoutcomesincludingmortality, admission to hospital or ICU, and length of hospital stay, but there is variability betweenstudies(objective3).Allbuttwoearlywarningsystemswereaggregatedscores.Thislimitedtheabilitytocomparecomprehensivelybetweensingle,multipleparameterandaggregatedscores.TheAPACHEIIscore,PEDS,VIEWS-L,andTHERMscoreswererelativelybestatpredictingmortalityandICUadmission,providing excellent discrimination ability (AUROC > 0.8),83 but differences between studies may, inpart, account for this. TheMEWSwas themost commonly used and assessed system, but findingsof this reviewsuggesta relatively lowerability topredictmortalityand ICUadmissions compared tothe four scoresmentionedabove,withonly somestudies indicatingacceptablediscriminatoryabilityof theMEWS (AUROC > 0.7) and other studies indicating a lack of discriminatory ability (AUROC <0.7),83 especially for the outcome ICU admission. The exceptionwas one study that found excellentdiscriminatory ability of MEWS for the outcome in-hospital mortality (AUROC 0.89).79 However, the ability of earlywarning systems to predict adverse outcomes does notmean that earlywarningsystemsareeffectiveatpreventingadverseoutcomes.Onlyonestudywasidentifiedthataddressedthisquestionanditfoundthattheintroductionofanearlywarningsystemmayhavelittleornodifferencein detecting deterioration or adverse events however the evidence was of very low quality makingit impossible to draw any strong conclusions (objective 2). In addition, we did not find any studiesexaminingthecost-effectivenessofearlywarningsystemsandTTS(objective4).
Implications for researchThere is a clearneed forhighquality effectiveness studies to test the impactof usingearlywarningsystems or TTS in the ED on patient outcomes. The cost-effectiveness of such interventions, theeffectivenessofrelatededucationalprogrammes,andbarriersandfacilitatorsto implementationalsoneedtobeexamined,asthereisaclearlackofsuchevidence.
LimitationsThiswas a rapid review; however, current literature suggests that putting some restrictions in placein the reviewprocessdoesnot significantly impacton thequalityandconclusionsofa review.84 Therestrictionsforthisreviewincludednotranslationofreports,althoughonlyonenon-Englishstudywasidentified.Dataextractionwasinitiallydonebyonlyonereviewer,but50%ofrecordswherecheckedforaccuracybyasecondreviewer.Strengthsofthereviewlieinitsthoroughsearchstrategy,itsscopeand inclusion of different studies and reports to address the research objectives, and in its rigorousmethodologywithdualindependentscreeningandqualityassessment.

73
References
1. GoldhillDR,McNarryAF.Physiologicalabnormalitiesinearlywarningscoresarerelatedtomortalityinadultinpatients.Britishjournalofanaesthesia.2004;92(6):882-4.
2. Buist M, Bernard S, Nguyen TV, Moore G, Anderson J. Association between clinically abnormalobservationsandsubsequentin-hospitalmortality:aprospectivestudy.Resuscitation.2004;62(2):137-41.
3. Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospitalcardiopulmonaryarrest.Chest.1990;98(6):1388-92.
4. Smith AF, Wood J. Can some in-hospital cardio-respiratory arrests be prevented? A prospectivesurvey.Resuscitation.1998;37(3):133-7.
5. FranklinC,MathewJ.Developingstrategiestopreventinhospitalcardiacarrest:analyzingresponsesofphysiciansandnursesinthehoursbeforetheevent.Criticalcaremedicine.1994;22(2):244-7.
6. Rivers EP, Coba V, Whitmill M. Early goal-directed therapy in severe sepsis and septic shock: acontemporaryreviewoftheliterature.Currentopinioninanaesthesiology.2008;21(2):128-40.
7. Department of Health. National Early Warning Score: National Clinical Guideline No.1. Dublin:DepartmentofHealth,2013.
8. RoyalCollegeofPhysicians.NationalEarlyWarningScore(NEWS):Standardisingtheassessmentofacute-illness severity in theNHS.Reportofaworkingparty. London:RoyalCollegeofPhysicians,2012.
9. NationalInstituteforHealthandCareExcellence.AcutelyIllPatientsinHospital.RecognitionofandResponsetoAcuteIllnessinAdultsinHospital(CG50).London:NICE,2007.
10. MitchellIA,McKayH,VanLeuvanC,BerryR,McCutcheonC,AvardB,etal.Aprospectivecontrolledtrialoftheeffectofamulti-facetedinterventiononearlyrecognitionandinterventionindeterioratinghospitalpatients.Resuscitation.2010;81(6):658-66.
11. AgencyforHealthcareResearchandQuality.RapidResponseSystemsUSA:AHRQ,U.S.DepartmentofHealthandHumanServices,USA;2014[Availablefrom: https://psnet.ahrq.gov/primers/primer/4/rapid-response-systems.
12. DepartmentofHealth.TheIrishMaternityEarlyWarningSystem(IMEWS):NationalClinicalGuidelineNo.4.Dublin:DepartmentofHealth,2014.
13. Singh S, McGlennan A, England A, Simons R. A validation study of the CEMACH recommendedmodifiedearlyobstetricwarningsystem(MEOWS)*.Anaesthesia.2012;67(1):12-8.
14. MaguireP,O’HigginsA,PowerK,TurnerM.TheIrishMaternityEarlyWarningSystem(IMEWS).IrishMedicalJournal.2014;107(10):309.
15. DepartmentofHealth.TheIrishPaediatricNationalEarlyWarningSystem(PEWS):NationalClinicalGuidelineNo.12.Dublin:DepartmentofHealth,2015.
16. SmithM,FeiedC.TheEmergencyDepartmentasaComplexSystem1999[Availablefrom:http://www.necsi.edu/projects/yaneer/emergencydeptcx.pdf.
17. CourtneyDM,NeumarRW,VenkateshAK,KajiAH,CairnsCB,LavonasE,etal.Uniquecharacteristicsofemergencycareresearch:scope,populations,andinfrastructure.Academicemergencymedicine:officialjournaloftheSocietyforAcademicEmergencyMedicine.2009;16(10):990-4.
18. RolandD, Coats TJ. An earlywarning?Universal risk scoring in emergencymedicine. EmergencyMedicineJournal.2011;28(4):263.
19. GriffithsJR,KidneyEM.CurrentuseofearlywarningscoresinUKemergencydepartments.EmergencyMedicineJournal.2012;29(1):65-62p.
20. SubbeCP,KrugerM,RutherfordP,GemmelL.Validationofamodifiedearlywarningscoreinmedicaladmissions.QJM-MonthlyJournaloftheAssociationofPhysicians.2001;94(10):521-6.
21. MoherD,LiberatiA,TetzlaffJ,AltmanDG.Preferredreportingitemsforsystematicreviewsandmeta-analyses:thePRISMAstatement.BMJ(Clinicalresearched).2009;339.
22. TheNordicCochraneCentre;TheCochraneCollaboration.ReviewManager (RevMan) [Computerprogram]Version5.3.Copenhagen2014.

74
23. NationalHeartLungandBloodInstitute.StudyQualityAssessmentTools.SecondaryStudyQualityAssessmentTools2014[Availablefrom: http://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools.
24. TheAGREE collaborationGW,Cluzeau FA, et al,. Development and validationof an internationalappraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project.QualityandSafetyinHealthCare.2003;12(1):18-23.
25. HigginsJ,GreenS.CochraneHandbookforsystematicReviewsofInterventionsVersion5.1.0[updatedMarch2011]:TheCochraneCollaboration;2011.Availablefrom:www.cochrane-handbook.org.
26. AtkinsD,BestD,BrissPA,EcclesM,Falck-YtterY,FlottorpS,etal.Gradingqualityofevidenceandstrengthofrecommendations.BMJ(Clinicalresearched).2004;328(7454):1490.
27. EffectivePracticeandOrganisationofCare(EPOC).SuggestedriskofbiascriteriaforEPOCreviews.EPOCResourcesforreviewauthorsOslo:NorwegianKnowledgeCentrefortheHealthServices;2015[Availablefrom:http://epoc.cochrane.org/epoc-specific-resources-review-authors]
28. DrummondMF,JeffersonTO.GuidelinesforauthorsandpeerreviewersofeconomicsubmissionstotheBMJ.TheBMJEconomicEvaluationWorkingParty.BMJ:BritishMedicalJournal.1996;313(7052):275-83.
29. PhilipsZ,Ginnelly L, SculpherM,ClaxtonK,GolderS,RiemsmaR,etal.Reviewofguidelines forgoodpracticeindecision-analyticmodellinginhealthtechnologyassessment.HealthTechnolAssess.2004;8(36):iii-iv,ix-xi,1-158.
30. Kansagara D, Englander H, Salanitro A, et al. Risk predictionmodels for hospital readmission: Asystematicreview.JAMA.2011;306(15):1688-98.
31. AbramiP,BorokhovskiE,BernardR,WadeA,TamimR,PerssonT,etal. Issues inconductinganddisseminatingbriefreviewsofevidence.Evidence&Policy.2010;6(3):371-89
32. GuM,FuY,LiC,ChenM,ZhangX,XuJ,etal.Thevalueofmodifiedearlywarningscoreinpredictingearlymortality of critically ill patients admitted to emergency department. Chinese Critical CareMedicine.2015;27(8):687-90.
33. CoughlanE,DeasyC,McDaidF,GearyU,WardM,O’SullivanR,etal.AnintroductiontotheEmergencyDepartmentAdultClinicalEscalationProtocol:ED-ACE.Resuscitation.2015;96:33-1p.
34. ConsidineJ,LucasE,WunderlichB.TheuptakeofanearlywarningsysteminanAustralianemergencydepartment:Apilotstudy.CriticalCareandResuscitation.2012;14(2):135-41.
35. CorreiaN,RodriguesRP,SáMC,DiasP,LopesL,PaivaA.ImprovingrecognitionofpatientsatriskinaPortuguesegeneralhospital:resultsfromapreliminarystudyontheearlywarningscore.InternationalJournalofEmergencyMedicine.2014;7(1):Articlenumber22.
36. GriffithsJR,KidneyEM.CurrentuseofearlywarningscoresinUKemergencydepartments.Emergencymedicinejournal:EMJ.2012;29(1):65-6.
37.WilsonSJ,WongD,CliftonD,FlemingS,WayR,PullingerR,etal.Trackandtriggerinanemergencydepartment:anobservationalevaluationstudy.EmergencyMedicineJournal.2013;30(3):186-916p.
38. Christensen D, Jensen NM,Maaloe R, Rudolph SS, Belhage B, Perrild H. Low compliancewith avalidatedsystemforemergencydepartmenttriage.DanishMedicalBulletin.2011;58(6):A4294.
39. JohnsonKD,WinkelmanC,BurantCJ,DolanskyM,TottenV.TheFactorsthatAffecttheFrequencyof Vital Sign Monitoring in the Emergency Department. JEN: Journal of Emergency Nursing.2014;40(1):27-359p.
40. AustenC,PattersonC,PootsA,GreenS,WeldringT,BellD.Usingalocalearlywarningscoringsystemasamodelfortheintroductionofanationalsystem.AcuteMedicine.2012;11(2):66-73.
41. HudsonP,EkholmJ, JohnsonM,LangdonR.Early identificationandmanagementoftheunstableadultpatientintheemergencydepartment.JournalofClinicalNursing.2015;24(21-22):3138-46.
42. Shuk-NgorS,Chi-WaiO,Lai-YeeW,ChungJYM,GrahamCA.IstheModifiedEarlyWarningScoreabletoenhanceclinicalobservationtodetectdeterioratingpatientsearlierinanAccident&EmergencyDepartment?AustralasianEmergencyNursingJournal.2015;18(1):24-329p.

75
43.WilsonSJ,WongD,PullingerRM,WayR,CliftonDA,TarassenkoL.Analysisofadata-fusionsystemforcontinuousvitalsignmonitoringinanemergencydepartment.EuropeanJournalofEmergencyMedicine.2016;23(1):28-32.
44. NaidooDK,RangiahS,NaidooSS.AnevaluationoftheTriageEarlyWarningScoreinanurbanaccidentandemergencydepartmentinKwaZulu-Natal.SouthAfricanFamilyPractice.2014;56(1):69-735p.
45. BurchVC,TarrG,MorroniC.Modifiedearlywarningscorepredictstheneedforhospitaladmissionandinhospitalmortality.EmergencyMedicineJournal.2008;25(10):674-85p.
46. ChallenK,GoodacreSW.Predictive scoring innon-traumaemergencypatients: a scoping review.EmergencyMedicineJournal.2011;28(10):827-3711p.
47. Australian Commission on Safety andQuality in Health Care (the Commission). Recognising andrespondingtoclinicaldeterioration,Surveyofrecognitionandresponsesystemsinaustralia.2011.
48. FawcettT.AnintroductiontoROCanalysis.PatternRecognitionLetters.2006;27:861–74.49. CorfieldAR,LeesF,HoustonG,ZealleyI,DickieS,WardK,etal.Earlywarningscoresinsepsis:Utilityofa
singleearlywarningscoreintheemergencydepartment?IntensiveCareMedicine.2012;38:S296-S7.50. KeepJW,MessmerAS,SladdenR,BurrellN,PinateR,TunnicliffM,etal.Nationalearlywarningscore
atEmergencyDepartmenttriagemayallowearlieridentificationofpatientswithseveresepsisandsepticshock:Aretrospectiveobservationalstudy.EmergencyMedicineJournal.2016;33(1):37-41.
51. SubbeCP,SlaterA,MenonD,GemmellL.Validationofphysiologicalscoringsystemsintheaccidentandemergencydepartment.EmergencyMedicineJournal.2006:841-55p.
52. VorwerkC,LorymanB,CoatsTJ,StephensonJA,GrayLD,ReddyG,etal.Predictionofmortalityinadultemergencydepartmentpatientswithsepsis.EmergencyMedicineJournal.2009;26(4):254-85p.
53. AlbrightCM,Ali TN, LopesV, RouseDJ,AndersonBL. The Sepsis inObstetrics Score: amodel toidentifyriskofmorbidity fromsepsis inpregnancy.AmericanJournalofObstetrics&Gynecology.2014;211(1):39.e1-81p.
54. HeitzCR,GaillardJP,BlumsteinH,CaseD,MessickC,MillerCD.Performanceofthemaximummodifiedearly warning score to predict the need for higher care utilization among admitted emergencydepartmentpatients.JournalofHospitalMedicine.2010;5(1):E46-521p.
55. HowellMD,DonninoMW,TalmorD,ClardyP,NgoL,ShapiroNI.Performanceofseverityofillnessscoringsystemsinemergencydepartmentpatientswithinfection.AcademicEmergencyMedicine.2007;14(8):709-146p.
56. JonesAE,FitchMT,KlineJA.Operationalperformanceofvalidatedphysiologicscoringsystemsforpredicting in-hospital mortality among critically ill emergency department patients. Critical caremedicine.2005;33(5):974-85p.
57. Nguyen HB, Van Ginkel C, BatechM, Banta J, Corbett SW. Comparison of Predisposition, Insult/Infection, Response, and Organ dysfunction, Acute Physiology And Chronic Health Evaluation II,andMortalityinEmergencyDepartmentSepsisinpatientsmeetingcriteriaforearlygoal-directedtherapyandthe.JournalofCriticalCare.2012;27(4):362-98p.
58. ArmaganE,YilmazY,OlmezOF,SimsekG,GulCB.Predictivevalueofthemodifiedearlywarningscoreinaturkishemergencydepartment.EuropeanJournalofEmergencyMedicine.2008;15(6):338-40.
59. BulutM,CebicciH,SigirliD,SakA,DurmusO,TopAA,etal.Thecomparisonofmodifiedearlywarningscorewithrapidemergencymedicinescore:Aprospectivemulticentreobservationalcohortstudyonmedicalandsurgicalpatientspresentingtoemergencydepartment.Emergencymedicinejournal[Internet].2014;31(6):[476-81pp.].Availablefrom:http://emj.bmj.com/content/31/6/476.full.pdf.
60. ÇildirE,BulutM,AkalinH,KocabaşE,OcakoǧluG,AydinŞA.EvaluationofthemodifiedMEDS,MEWSscoreandCharlsoncomorbidityindexinpatientswithcommunityacquiredsepsisintheemergencydepartment.InternalandEmergencyMedicine.2013;8(3):255-60.
61. CattermoleGN,MakSKP,LiowCHE,HoMF,HungKYG,KeungKM,etal.Derivationofaprognosticscoreforidentifyingcriticallyillpatientsinanemergencydepartmentresuscitationroom.Resuscitation.2009;80(9):1000-5.

76
62. CattermoleGN,LiowECH,GrahamCA,RainerTH.THERM:theResuscitationManagementscore.Aprognostictooltoidentifycriticallyillpatientsintheemergencydepartment.EmergencyMedicineJournal.2014;31(10):803-75p.
63. GrahamCA,ChoiKM,KiCW,LeungYK,LeungPH,MakP,etal.EvaluationandvalidationoftheuseofModifiedEarlyWarningScore(MEWS)inemergencydepartmentobservationward...2007SocietyforAcademicEmergencyMedicineAnnualMeeting.AcademicEmergencyMedicine.2007;14:S199-2001p.
64. HoLO,LiH,ShahidahN,KohZX,SultanaP,OngMEH.Poorperformanceofthemodifiedearlywarningscoreforpredictingmortalityincriticallyillpatientspresentingtoanemergencydepartment.WorldJournalofEmergencyMedicine.2013;4(4):273-7.
65. HockOngME,LeeNgCH,GohK,LiuN,KohZX,ShahidahN,etal.Predictionofcardiacarrestincriticallyillpatientspresentingtotheemergencydepartmentusingamachinelearningscoreincorporatingheartratevariabilitycomparedwiththemodifiedearlywarningscore.CriticalCare.2012;16(3).
66. LiuFY,QinJ,WangRX,FanXL,WangJ,SunCY,etal.AprospectivevalidationofnationalearlywarningscoreinemergencyintensivecareunitpatientsatBeijing.HongKongJournalofEmergencyMedicine.2015;22(3):137-44.
67. OlssonT,LindL.ComparisonoftheRapidEmergencyMedicineScoreandAPACHEIIinnonsurgicalemergencydepartmentpatients.AcademicEmergencyMedicine.2003;10(10):1040-89p.
68. Olsson T, Terent A, Lind L. Rapid Emergency Medicine score: a new prognostic tool for in-hospital mortality in nonsurgical emergency department patients. Journal of Internal Medicine.2004;255(5):579-879p.
69. ChristensenD, JensenNM,MaaløeR,RudolphSS,BelhageB,PerrildH.Nurse-administeredearlywarning score system can be used for emergency department triage. Danish Medical Bulletin.2011;58(6).
70. EickC,RizasKD,Meyer-ZürnCS,Groga-BadaP,HammW,KrethF,etal.Autonomicnervoussystemactivityasriskpredictorinthemedicalemergencydepartment:aprospectivecohortstudy.Criticalcaremedicine.2015;43(5):1079-868p.
71. GeierF,PoppS,GreveY,AchterbergA,GlocknerE,ZieglerR,etal.Severityillnessscoringsystemsfor early identification and prediction of in-hospital mortality in patients with suspected sepsispresentingtotheemergencydepartment.WienerklinischeWochenschrift.2013;125(17-18):508-15.
72. JoS,JeongT,LeeJB,JinY,YoonJ,ParkB.Validationofmodifiedearlywarningscoreusingserumlactatelevelincommunity-acquiredpneumoniapatients.TheNationalEarlyWarningScore-Lactatescore.AmericanJournalofEmergencyMedicine.2016.
73. JoS,LeeJB,JinYH,JeongTO,YoonJC,JunYK,etal.Modifiedearlywarningscorewithrapidlactatelevelincriticallyillmedicalpatients:theViEWS-Lscore.EmergencyMedicineJournal.2013;30(2):123-97p.
74. JunhasavasdikulD, Theerawit P, Kiatboonsri S.Associationbetweenadmissiondelay andadverseoutcomeofemergencymedicalpatients.EmergencyMedicineJournal.2013;30(4):320-34p.
75.Wang AY, Fang CC, Chen SC, Tsai SH, KaoWF. PeriarrestModified EarlyWarning Score (MEWS)predicts theoutcomeof in-hospital cardiac arrest. Journal of the FormosanMedicalAssociation.2016;115(2):76-827p.
76. AlamN,VegtingIL,HoubenE,vanBerkelB,VaughanL,KramerMH,etal.ExploringtheperformanceoftheNationalEarlyWarningScore(NEWS)inaEuropeanemergencydepartment.Resuscitation.2015;90:111-5.
77.WilliamsJ,GreensladeJ,ChuK,BrownA,LipmanJ.SeverityScoresinEmergencyDepartmentPatientsWithPresumedInfection:AProspectiveValidationStudy.Criticalcaremedicine.2016;44(3):539-479p.
78. ConsidineJ,RawetJ,CurreyJ.Theeffectofastaged,emergencydepartmentspecificrapidresponsesystemonreportingofclinicaldeterioration.AustralasianEmergencyNursingJournal.2015;18(4):218-26.

77
79. DundarZD,ErginM,KaramercanMA,AyranciK,ColakT,TuncarA,etal.ModifiedEarlyWarningScoreandVitalPacEarlyWarning Score in geriatricpatients admitted toemergencydepartment.Europeanjournalofemergencymedicine:official journaloftheEuropeanSocietyforEmergencyMedicine.2015.
80. ChurpekMM,YuenTC,EdelsonDP.Riskstratificationofhospitalizedpatientsonthewards.Chest.2013;143(6):1758-65.
81. CorfieldAR, LeesF,Zealley I,HoustonG,DickieS,WardK,etal.Utilityofa singleearlywarningscore in patientswith sepsis in the emergency department. Emergencymedicine journal : EMJ.2014;31(6):482-7.
82. RuoppMD,PerkinsNJ,WhitcombBW,SchistermanEF.YoudenIndexandOptimalCut-PointEstimatedfrom Observations Affected by a Lower Limit of Detection. Biometrical journal BiometrischeZeitschrift.2008;50(3):419-30.
83. HosmerD,LemeshowS.AppliedLogisticRegression.2ed.NewYork:JohnWiley&Sons,Inc.;2000.84.WattA,CameronA,SturmL,LathleanT,BabidgeW,BlameyS,etal.Rapidversus full systematic
reviews:validityinclinicalpractice?ANZJSurg.2008;78(11):1037-40.

78
Appendix 1: Search strategies
Cochrane Library Search Strategy
Platform: John Wiley and Sons
Date of search: 04/03/2016
ID Search Hits
#1 MeSHdescriptor:[EmergencyService,Hospital]explodealltrees 2078
#2
Emergencynear/1(careorwardorwardsordepartmentordepartmentsorunit or units or roomor roomormedic*orhealthorhealthcareorhospital or service or services or centre or centres or center or centers or treatmentortreatmentsoroutpatientoroutpatients)
12379
#3Casualtynear/2(careorwardorwardsordepartmentordepartmentsorunit or units or room or room or service or services or centre or centres orcenterorcentersoroutpatientoroutpatients)
68
#4Traumanear/2(careorwardorwardsordepartmentordepartmentsorunitorunitsorroomorroomormedic*orhospitalorserviceorservicesorcentreorcentresorcenterorcentersoroutpatientoroutpatients)
1505
#5Triagenear/2 (careorwardorwardsordepartmentordepartmentsorunitorunitsorroomorroomormedic*orhospitalorserviceorservicesorcentreorcentresorcenterorcentersoroutpatientoroutpatients)
98
#6 “accidentandemergency”or“accident&emergency”orA&Eor“A&E”or“AandE” 1431
#7 {or#1-#6} 14493
#8 Warningnear/2(earlyorsystemorsystemsorscoreorscores) 168
#9 Triggernear/2track 6
#10 Triggernear/4(scoreorscoresorscoring) 20
#11 Escalationnear/2(protocolorprotocolsorpolicyorpoliciesorprocedureorproceduresorguidelineorguidelinesorguidance) 25
#12 EWSorMEWS 75
#13 POTTS 177
#14 {or#8-#13} 443
#15 adult or adults or adulthood 402614
#16 #7and#14and#15 38

79
Medline Search Strategy
Platform: Ovid MEDLINE In-Process & Other Non-Indexed Citations and Ovid MEDLINE 1946 to Present
Date of Search: 04/03/2016
ID Search Hits
#1 emergency service, hospital.sh. 48807
#2
(Emergencyadj(careorwardorwardsordepartmentordepartmentsorunitorunitsorroomorroomormedic*orhealthorhealthcareorhospital or service or services or centre or centres or center or centers ortreatmentortreatmentsoroutpatientoroutpatients)).af.
197858
#3(Casualtyadj2(careorwardorwardsordepartmentordepartmentsorunit or units or room or room or service or services or centre or centres orcenterorcentersoroutpatientoroutpatients)).af.
1309
#4
(Trauma adj2 (care or ward or wards or department or departmentsor unit or units or room or room or medic* or hospital or serviceor services or centre or centres or center or centers or outpatient oroutpatients)).af.
47447
#5
(Triage adj2 (care or ward or wards or department or departmentsor unit or units or room or room or medic* or hospital or serviceor services or centre or centres or center or centers or outpatient oroutpatients)).af.
1679
#6 (“accidentandemergency”or“accident&emergency”orA&Eor“A&E”or“AandE”).af. 1886693
#7 1or2or3or4or5or6 2093553
#8 (Warningadj2(earlyorsystemorsystemsorscoreorscores)).af. 4296
#9 (Triggeradj2track).af. 67
#10 (Triggeradj4(scoreorscoresorscoring)).af. 56
#11 (Escalationadj2(protocolorprotocolsorpolicyorpoliciesorprocedureorproceduresorguidelineorguidelinesorguidance)).af. 168
#12 (EWSorMEWS).af. 2180
#13 POTTS.af. 5046
#14 8or9or10or11or12or13 11541
#15 (adultoradultsoradulthood).af. 4789831
#16 7and14and15 362

80
Embase Search Strategy
Platform: Elsevier
Date of Search: 22/02/2016
ID Search Hits
#1 ‘emergencyward’/exp 82019
#2
emergency NEAR/1 (care OR ward OR wards OR department ORdepartmentsORunitORunitsORroomORroomsORmedic*ORhealthORhealthcareORhospitalORserviceORservicesORcenterORcentersOR centre OR centres OR treatment OR treatments OR outpatient ORoutpatients)
317266
#3casualtyNEAR/2(careORwardORwardsORdepartmentORdepartmentsORunitORunitsORroomORroomORserviceORservicesORcentreORcentresORcenterORcentersORoutpatientORoutpatients)
1741
#4
traumaNEAR/2(careORwardORwardsORdepartmentORdepartmentsORunitORunitsORroomORroomORmedic*ORhospitalORserviceORservicesORcentreORcentresORcenterORcentersORoutpatientORoutpatients)
51937
#5
triageNEAR/2(careORwardORwardsORdepartmentORdepartmentsORunitORunitsORroomORroomORmedic*ORhospitalORserviceORservicesORcentreORcentresORcenterORcentersORoutpatientORoutpatients)
1827
#6 accidentandemergency’OR‘accident&emergency’ORa&eOR‘a&e’OR‘aande’ 168515
#7 #1OR#2OR#3OR#4OR#5OR#6 512537
#8 warningNEAR/2(earlyORsystemORsystemsORscoreORscores) 5852
#9 triggerNEAR/2track 110
#10 triggerNEAR/4(scoreORscoresORscoring) 116
#11 escalation NEAR/2 (protocol OR protocols OR policy OR policies ORprocedureORproceduresORguidelineORguidelinesORguidance) 341
#12 ewsORmews 4360
#13 potts 4486
#14 #8OR#9OR#10OR#11OR#12OR#13 14723
#15 adultORadultsOR‘adulthood’ 5624653
#16 #7AND#14AND#15 254

81
CINAHL Complete Search Strategy
Platform: EBSCOhost
Date of Search: 04/03/2016
ID Search Hits
S1 (MH“EmergencyService”) 34352
S2
EmergencyN1(careORwardorwardsORdepartmentordepartmentsORunitorunitsORroomorroomsORmedic*ORhealthORhealthcareOR hospital OR service or services OR center or centers OR centre orcentresORtreatmentortreatmentsORoutpatientoroutpatients)
99485
S3Casualty N2 (care OR ward or wards OR department or departmentsORunitorunitsORroomorroomsORserviceorservicesORcenterorcentersORcentreorcentresORoutpatientoroutpatients)
402
S4TraumaN2(careorwardorwardsordepartmentordepartmentsorunitorunitsorroomorroomormedic*orhospitalorserviceorservicesorcentreorcentresorcenterorcentersoroutpatientoroutpatients)
9842
S5TriageN2(careorwardorwardsordepartmentordepartmentsorunitorunitsorroomorroomormedic*orhospitalorserviceorservicesorcentreorcentresorcenterorcentersoroutpatientoroutpatients)
978
S6 “accidentandemergency”or“accident&emergency”orA&Eor“A&E”or“AandE” 52174
S7 S1ORS2ORS3ORS5ORS6 149039
S8 WarningN2(earlyorsystemorsystemsorscoreorscores) 1131
S9 TriggerN2track 44
S10 TriggerN4(scoreorscoresorscoring) 26006
S11 EscalationN2(protocolorprotocolsorpolicyorpoliciesorprocedureorproceduresorguidelineorguidelinesorguidance) 37
S12 ewsORmews 196
S13 potts 184
S14 S8ORS9ORS10ORS11ORS12ORS13 27422
S15 adultORadultsORadulthood 892275
S16 S7ANDS14ANDS15 653

82
Cost Effectiveness Resources
Date of Search: 11/03/2016 (except * searched 04/03/2016)
Website/Database URL Search Terms Hits
Health Technology Assessment Database, NHS Economic Evaluation Database (NHSEED) & Health Economic Evaluation Database (HEED) via The Cochrane Library*
www.cochranelibrary.com
SeeCochraneLibrarytab
n/a
NHS Service Delivery and Organisation (SDO) Research and Development Programme
www.nets.nihr.ac.uk/programmes/hsdr
patientdeteriorationemergency department
0
patientdeteriorationemergency
4.Aftersifting=0
patientdeterioration 46.Aftersifting=0
early warning 13.Aftersifting=1
track and trigger 5.Aftersifting=0
National Coordinating Centre for Health Technology Assessment (NCCHTA)
www.nets.nihr.ac.uk/programmes/hta
patientdeteriorationemergency department
0
patientdeteriorationemergency
4.Aftersifting=0
patientdeterioration 46.Aftersifting=0
early warning 13.Aftersifting=1.Sameasresultforwebsiteabove,hencediscarded
track and trigger 5.Aftersifting=0
NIHR-HTA Database http://www.crd.york.ac.uk/CRDWeb/
patientdeterioration.Filters:HTApublishedandHTAinprogress
2

83
Guidance Resources
Date of Search: 13/03/2016 (except * searched 11/03/2016)
Website/ Database URL Search Terms Hits
Department of Health (including National Clinical Guidelines)*
via Google Advanced Search https://www.google.com/advanced_search
emergencyadult*warningORORORtriageORORORcareORORORtraumaORORORtriggerOROROResclat*OROROREWSORORORMEWSORORORPOTTS.Sitefilter:health.gov.ieRegionfilter:Ireland
495.Aftersiftingfirst200hits=4.Plus2addedfrombriefmanualsearch.
Health Service Executive (HSE)*
via Google Advanced Search https://www.google.com/advanced_search
emergencyadult*warningORORORtriageORORORcareORORORtraumaORORORtriggerOROROResclat*OROROREWSORORORMEWSORORORPOTTS.Sitefilter:hse.ieRegionfilter:Ireland
1880.Aftersiftingfirst200hits=4.
Health Information and Quality Authority (HIQA)
www.hiqa.ie “emergency department patientdeterioration”inkeywordbox
92.Aftersifting=0
National Institute for Health and Care Excellence (NICE)
https://www.nice.org.uk/guidance
patientdeteriorationemergency department
55.Aftersifting=4
“earlywarning”or“trackandtrigger”orewsormewsorpotts
38.Aftersifting=5
NHS Evidence (incorporating Scottish Intercollegiate Guidelines Network (SIGN) & Guidelines International Network (GIN))
https://www.evidence.nhs.uk
"patientdeterioration"and"emergency department" and("earlywarning"or"track and trigger" or ews or mewsorpotts)
17.Aftersifting=1
emergency department and ("earlywarning"or"trackand trigger" or ews or mews orpotts)
419.Aftersifting=3
Agency for Healthcare Research and Quality (AHRQ) National Guideline Clearinghouse
http://www.guideline.gov
(triageorcasualtyortrauma or "emergency department")'and'("earlywarning" or trigger or ews or mewsorpotts)'Filters:Adult(19to44years)Aged(65to79years)Aged,80andover
76.aftersifting=0
Patientdeterioration 187.Aftersifting=0

84
Professional Bodies
Date of Search: 09-11/03/2016
Website/ Database URL Search Terms Hits
Irish Association for Emergency Medicine (IAEM)
www.iaem.ie Singlesearchbox,noinstructions.Booleanoperatorsareacceptedbutonly with certain search terms themoreoptionsadded,the less it seems to work. Therefore,amanualsearchwasperformed.
0
Royal College for Emergency Medicine (UK)
www.rcem.ac.uk Singlesearchbox,noinstructions.Booleanoperatorsareacceptedbutonly with certain search terms themoreoptionsadded,the less it seems to work. Therefore,amanualsearchwasperformed.
3
European Society for Emergency Medicine (EuSEM)
www.eusem.org Noresultsforsimplesearchessuchas:“patientdeterioration”,“trackandtrigger”or“earlywarning”.
0
American Academy of Emergency Medicine (AAEM)
www.aaem.org (emergencyORtraumaORcasualtyORtriage)AND(careORwardORwardsORdepartmentORdepartmentsORunitORunitsORroomORroomsORhealthORhealthcareORhospitalORservice)AND(warningORtriggerOREWSORMEWSORPOTTS)AND(deteriorateORdeteriorationORdeterioratedORdeterioratesORworseORworsenORworseningORadverseORweakenORweakenedORweakensORweakerOR“acuteillness”)AND(Monitorormonitorsor monitored or monitoring ORescalateORescalatesORescalatedORescalationORescalatingORreassessORreassesses or reassessed or reassessmentORreassessing)AND(adultORadultsORadulthood)
67Hits.Aftersifting=0

85
American College of Emergency Physicians (ACEP)
www.acep.org Singlesearchbox,noinstructions.Booleanoperators not accepted.
1
Society for Academic Emergency Medicine (SAEM)
www.saem.org (emergencyORtraumaORcasualtyORtriage)AND(careORward*ORdepartment*ORunit*ORroom*ORhealth*ORhospitalORservice)AND(warningORtriggerOREWSORMEWSORPOTTS)AND(deteriorat*ORworse*ORadverseORweaken*ORweakerOR“acuteillness”)(Monitor*ORescalate*ORreassess*)AND(adult*)
4.Aftersifting=0
Canadian Association of Emergency Physicians
www.caep.ca (emergencyORtraumaORcasualtyORtriage)AND(escalate*ORtriggerORwarningORewsORpotts)
110.Aftersifting=0
Australasian Society for Emergency Medicine (ASEM)
www.asem.org.au Manual1 0
Australasian College of Emergency Medicine (ACEM)
www.acem.org.au Manual 1
International Federation for Emergency Medicine (IFEM)
http://www.ifem.cc Manual 2
Faculty of Emergency Nursing
www.fen.uk.com Manual 0
RCN Emergency Care Association
www.rcn.org.uk Manual 0
Emergency Nurses Association
www.ena.org Manual 0
Canadian Emergency Nurses
www.nena.ca Access to this site not allowed forsecurityreasons
European Society for Emergency Nursing
www.eusen.org Manual 0
Emergency Nursing weblinks
www.enw.org (emergencyORtraumaORcasualtyORtriage)AND(escalateORtriggerORwarningORewsORpotts)
5.Aftersifting=0

86
Philippine Society of Emergency Care Nurses
www.philippine nursingdirectory.com/associations/philippine-society-of-emergency-care-nurses-psecn/
Manual 3.Aftersifting=0
Emergency Nursing Society of South Africa
http://emssa.org.za/enssa/
Manual 0
Australian College of Emergency Nursing
www.acen.com.au Manual 0
College of Emergency Nursing Australia
www.cena.org.au Manual 0
College of Emergency Nurses (New Zealand) CENNZ - NZNO
www.nzno.org.nz/colleges/college_of_emergency_nurses
Manual 0
Hong Kong Emergency Nursing
www.hkena.org Manual 0
1Manualsearcheswereperformedonwebsiteswhereregularelectronicsearchingattemptswerenotuseful.Thisiscausedbyreducedsearchingfunctionalitysuchassearchboxesthatcanonlysearchoneword,oralackofsearchbox.Manualsearchinginvolvesexploringclickablewebpagecontente.g.,tabs,buttons,hyperlinksetc.inaniterativewaytoidentifyrelevantresources.

87
Grey LiteratureDate of Search: 12-13/03/2016
Website/Database URL Search Terms HitsRIAN http://rian.ie/en/
static/User#searchAllof‘patient’,‘deterioration’,‘emergency’and‘department’inallfields;withanyof‘”trackandtrigger”’,‘”earlywarning”’,‘’,‘OR’,‘EWS’,‘OR’,‘MEWS’,‘OR’or‘POTTS’inallfields
0
Allof‘patient’,‘deterioration’,‘emergency’and‘department’inallfields
1
Allof‘early’,‘warning’,‘emergency’and‘department’inallfields
0
Allof‘early’and‘warning’inallfields
37.Aftersifting=4
Allof‘track’,‘and’and‘trigger’inallfields
2.Aftersifting=1
Proquest Dissertations and Theses UK & Ireland
www.library.nuigalway.ie
ab(emergencyORtraumaORcasualtyORtriage)AND(careORward*ORdepartment*ORunit*ORroom*ORhealth*ORhospitalORservice)AND(warningORtriggerOREWSORMEWSORPOTTS)AND(deteriorate*ORworse*ORadverseORweaken*ORweakerOR“acuteillness”ORMonitor*ORescalate*ORreassess*)ANDadult*
24aftersifting=0
Proquest Dissertations and Theses A & I
www.library.nuigalway.ie
ab(warningORtriggerOREWSORMEWSORPOTTS)ANDab(deteriorate*ORworse*ORadverseORweaken*ORweakerOR“acuteillness”ORMonitor*ORescalate*ORreassess*)ANDadult*
23.Aftersifting=0
ab(emergencyORtraumaORcasualtyORtriage)ANDab(careORward*ORdepartment*ORunit*ORroom*ORhealth*ORhospitalORservice)ANDab(warningORtriggerOREWSORMEWSORPOTTS)AND(deteriorate*ORworse*ORadverseORweaken*ORweakerOR“acuteillness”ORMonitor*ORescalate*ORreassess*)ANDadult*
88.Aftersifting=0

88
Clinical Trials RegistriesDate of Search: 12-13/03/2016Website/ Database URL Search Terms HitsCENTRAL www.cochranelibrary.
comSeeCochraneLibrarytab n/a
Prospero www.crd.york.ac.uk/PROSPERO
Trackandtrigger 3.Aftersifting=0Earlywarning 12.Aftersifting=2Patientdeteriorationemergency department
0
Patientdeteriorationemergency
0
Patientdeterioration 5.Aftersifting=0EWS 3.1relevantbut
already picked up in early warning search.0
MEWS 6.1relevantbutalready picked up in early warning search.0
POTTS 4.Aftersifting0ClinicalTrials.gov https://clinicaltrials.
gov/ct2/search/advanced
“patientdeterioration”AND(emergencyORtraumaORcasualtyORtriage)AND(warningORtriggerORescalationOREWSORMEWSORPOTTS)Filtersused:Adult(18–65)&Senior(66+)
0
patientdeteriorationAND(emergencyORtraumaORcasualtyORtriage)AND(warningORtriggerORescalationOREWSORMEWSORPOTTS)Filtersused:Adult(18–65)&Senior(66+)
9.Aftersifting=1
(emergencydepartmentORtraumaORcasualtyORtriage)AND(earlywarningORtrackandtriggerORescalationOREWSORMEWSORPOTTS)Filtersused:Adult(18–65)&Senior(66+)
107.Aftersifting=2

89
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP)
http://apps.who.int/trialsearch/AdvSearch.aspx
Advancedsearchstrategy.Onlyoptionstolimitto1)title2)conditionor3)intervention.Triedusingfollowingininterventionfield:earlywarningor track and trigger or ews or mewsorpotts.
1138 results. Skim through shows low specificitythereforestrategyabandoned.
Advancedsearchoptionnotuseful.Basicsearch:(emergencyORtraumaORcasualtyORtriage)AND(careORward*ORdepartment*ORunit*ORroom*ORhealth*ORhospitalORservice)AND(warningORtriggerORescalate*OREWSORMEWSORPOTTS)AND(deteriorate*ORworse*ORadverseORweaken*ORweakerOR“acuteillness”)(Monitor*ORescalate*ORreassess*)AND(adult*)
Siteunabletohandle this strategy and kept crashing
Basicoptionusedagain:patientdeteriorationANDemergencydepartmentORTriageANDearlywarningORtrackandtriggerOREWSORMEWSORPOTTS
29.Aftersifting9wereusefulbutoverlapwithClinicaltrials.gov results.6kept

90Ap
pend
ix 2
: Che
cklis
ts fo
r rap
id re
view
s (Ab
ram
i et a
l 201
0)31
Key
aspe
cts
Cons
ider
ation
s/re
com
men
datio
nsSe
ction
whe
re it
has
bee
n ad
dres
sed
Researchque
stion
The
researchq
uestion
sho
uld
beclearlystated
and
any
decisio
ntolim
itthe
treatm
entcon
ditio
nsand
outcomesm
easuress
houldbe
explained
.2
Inclusioncrite
riaAn
explan
ation
ofthe
inclusion
and
exclusion
crite
riashou
ldbe
provided
,no
tingwhe
therthe
revieww
illbelim
itedbyti
me,sou
rce,locati
on,contextor
metho
dologicalq
uality.
3.1
Sear
ch st
rate
gies
Theelectron
icand
othersea
rchstrategiessho
uldbe
explicitlystated
sothatitis
clea
rhow
thereview
iscom
preh
ensiv
ean
dfree
ofb
ias.
3.2
Inter-rateragree
men
tTh
ereview
sho
uldde
scrib
ethestep
stakentoensureinter-rateragree
men
tduring
theph
asesofstudy
iden
tificatio
n,calculatio
nofeffe
ctsa
ndcod
ingofstud
yfeatures
(ifapp
licab
le).
3.3-3.5
(inde
pend
entscree
ning
and
qu
ality
assessm
ent)
Effecte
xtracti
onTh
emetho
dused
toaggregatere
sultssh
ouldbeexplaine
dan
dde
fend
ed.
3.5
Stud
yfeatures
Thereview
shou
lddescribewhe
therorh
owvariabilityam
ongstud
iesw
asexplored,
andifno
t,whynot.
4
Anal
ysis
Mea
suresofcen
tralte
nden
cyand
variabilityshou
ldberepo
rted
.The
heterog
eneity
ofeffe
ctss
houldbe
noted
.N/A
Interpretatio
nan
dim
plicati
ons
Thereview
shou
ldcon
tainaclearse
tofcon
clusionsand
implicati
ons.
5
Cauti
onsa
nd
limita
tions
Theconclusio
nshou
ldoutlin
einthe
waysinw
hichthe
brie
freviewdiffersfrom
a
compreh
ensiv
ereview
,especiallythe
limita
tionsofbriefreview
metho
dologyand
theriskassociated
with
thetruthfulne
ssofthe
find
ings.
5
Other
Sourcesofe
vide
nce
(i.e.p
ublicati
oninformati
on)shou
ldb
eavailable
butno
tne
cess
arily
incl
uded
in th
e re
port
.Re
ferences

91
Appe
ndix
3: R
isk
of b
ias a
nd m
etho
dolo
gica
l qua
lity
asse
ssm
ent
Desc
riptiv
e st
udie
s: E
xten
t of u
seAs
sess
ed u
sing
the
Qua
lity
Asse
ssm
ent T
ool a
dapt
ed fr
om N
IH (2
014)
23
Note:th
estud
iess
hownhe
rere
lateto
table4ofth
eeviden
ceta
bles.
Crite
riaAu
stra
lian
Com
mis
sion
(2
011)
47
Cons
idin
e et
al
(201
2)34
Corr
eia
et a
l (2
014)
35Co
ughl
an e
t al
(201
5)33
Co
nferen
ce
abstract
Griffi
ths e
t al
(201
2)36
Wils
on e
t al
(201
3)37
1.Wasthe
researchqu
estio
nor
objecti
vein
thispa
perc
learlystated
?Yes
Yes
Yes
Yes
Yes
Yes
2.W
asthe
study
pop
ulati
onclearly
specified
and
defi
ned?
Yes
Yes
Yes
No
Yes
Yes
3.W
asth
epa
rticipa
tionrateatlea
st
50%?
Yes
No
(Totalsa
mple
repr
esen
ted
9.8%
ofE
DEW
Sactiv
ation
s)
Yes
NR
Yes
(57%
re
spon
se
rate)
Yes
4.W
ereallthe
sub
jectsselected
or
recruited
from
the
sam
eorsim
ilar
popu
latio
ns(in
clud
ing
the
same
time
perio
d)?
Were
inclusion
and
exclusion
crite
riaforb
eing
in
the
stud
ypre-specified
an
dap
plied
unifo
rmlyto
allpa
rticipa
nts?
Yes
Yes
Yes
NR
NR
No
(Restrictedto
timeswhe
namem
ber
ofre
search
team
was
on
duty)
5.W
asasa
mplesiz
ejustifie
d?N
oN
oN
oN
RN
oN
o
6.Were
the
outcom
emea
sures
clea
rlyd
efine
d,v
alid,reliable,a
nd
impl
emen
ted
cons
isten
tly a
cros
s al
l stud
ypa
rticipa
nts?
NR
Yes
Yes
NR
Yes
Yes
Qua
lity
Ratin
g (G
ood,
Fai
r, or
Poo
r)Fa
irFa
irFa
ir Po
orFa
irFa
ir
*CD,can
notd
etermine;NA,notapp
licab
le;N
R,notre
ported

92De
scrip
tive
stud
ies:
Com
plia
nce
Asse
ssed
usi
ng th
e Q
ualit
y As
sess
men
t Too
l for
Bef
ore-
After
(Pre
-Pos
t) S
tudi
es w
ith N
o Co
ntro
l Gro
up (N
IH 2
014)
23
Note:th
estud
iess
hownhe
rere
lateto
table5ofth
eeviden
ceta
bles.
Crite
riaAu
sten
et
al
(201
2)40
Chris
tens
en
et al
(2
011)
38
Huds
on
et a
l (2
015)
41
John
son
et a
l (2
014)
39
1.W
asth
estud
yqu
estio
norobjectiv
eclea
rlystated
?Yes
Yes
Yes
Yes
2.W
ereeligibility/selectio
ncrite
riaforthe
study
pop
ulati
onpre-spe
cifie
dan
dclea
rly
describ
ed?
Yes
Yes
No
Yes
3.W
erethepa
rticipa
ntsinth
estud
yrepresen
tativ
eofth
osewho
wou
ldbeeligiblefo
rthetest/service/in
terven
tioninth
egene
ralo
rclin
icalpop
ulati
onofinterest?
Yes
Yes
Yes
Yes
4.W
erealleligiblepartic
ipan
tsth
atm
etth
epre-specified
entrycriteriaenrolled?
Yes
Yes
CDYes
5.W
asth
esamplesiz
esufficien
tlylargetoprovide
con
fiden
cein
thefin
ding
s?CD
Yes
CDYes
6.W
asth
etest/service/in
terven
tionclea
rlydescribed
and
delivered
con
sistentlyacross
thestud
ypo
pulatio
n?Yes
Yes
Yes
(post)
N/A
7.W
ere
the
outcom
emea
surespre-specified
,clea
rlyd
efine
d,valid,reliable,a
nd
assessed
con
sistentlyacrossa
llstud
ypa
rticipa
nts?
Yes
Yes
No
(notpre-
specified
)
Yes
8.W
erethepe
opleassessin
gtheou
tcom
esblin
dedtothe
partic
ipan
ts’expo
sures/
interven
tions?
N/A
N/A
NR
N/A
9.W
asthe
losstofollo
w-upaft
erbaseline20
%orless?Werethoselosttofollo
w-up
accoun
tedforinthean
alysis?
Yes
Yes
Yes
Yes
10.D
idthe
statisticalm
etho
dsexaminechan
gesinoutcomemea
suresfrom
beforeto
afterth
einterven
tion?
Werestati
sticaltestsdon
ethatprovide
dpvaluesfo
rthe
pre-to
-po
st c
hang
es?
N/A
N/A
Yes
N/A
11.W
ereou
tcom
emea
suresofin
teresttaken
multip
letimesbeforetheinterven
tion
andmultip
letimesafte
rtheinterven
tion(i.e.,d
idthe
yusean
interrup
tedtim
e-serie
sde
sign)?
N/A
N/A
N/A
N/A
12.If
the
interven
tion
wascon
ducted
ata
grou
plevel(e.g.,
awho
leh
ospital,
acommun
ity,e
tc.)didthestati
sticalana
lysis
takein
toaccou
ntth
euseofin
dividu
al-le
vel
datato
determineeff
ectsatthe
group
level?
N/A
N/A
N/A
N/A
Qua
lity
Ratin
g (G
ood,
Fai
r, or
Poo
r)G
ood
Goo
dFa
irG
ood
*CD,can
notd
etermine;NA,notapp
licab
le;N
R,notre
ported

93G
uide
lines
:As
sess
ed u
sing
the
AGRE
E II
qual
ity a
sses
smen
t too
l24
Note:th
estud
iess
hownhe
rere
lateto
table6ofth
eeviden
ceta
bles.
AGRE
E II
TOO
L (2
revi
ewer
s)
NCG
No.
1 N
EWS7
NIC
E CG
509
RoCP
NEW
S8
DOM
AIN
1: S
cope
and
pur
pose
(3 it
ems)
97.2%
91.7%
91.7%
DOM
AIN
2: S
take
hold
er in
volv
emen
t (3
item
s)91
.7%
91.7%
91.7%
DOM
AIN
3: R
igou
r of d
evel
opm
ent (
8 ite
ms)
93.8%
92.7%
69.8%
DOM
AIN
4: C
larit
y of
pre
sent
ation
(3 it
ems)
91.7%
100.0%
100.0%
DOM
AIN
5: A
pplic
abili
ty (4
item
s)91
.7%
89.6%
64.6%
DOM
AIN
6: E
dito
rial i
ndep
ende
nce
(2 it
ems)
95.8%
87.5%
62.5%
OVE
RALL
GU
IDEL
INE
ASSE
SSM
ENT
(1 it
ems)
91.7%
91.7%
66.7%
I wou
ld re
com
men
d th
is g
uide
line
for u
se.
Yes
Yes
Yesw
ithm
odificatio
n

94Eff
ectiv
enes
s stu
dies
:As
sess
ed u
sing
the
EPO
C Ri
sk o
f Bia
s Too
l27
Note:th
estud
iess
hownhe
rere
lateto
table7ofth
eeviden
ceta
bles.
EPO
C cr
iteria
Shuk
-Ngo
r et a
l (20
15)42
Two
grou
p no
n-ra
ndom
ised
com
paris
on
(MEW
S gr
oup
vers
us u
sual
obs
erva
tion
grou
p)
Wasth
eallocatio
nsequ
enceade
quatelygene
rated?
High
riskofb
ias
Wasth
eallocatio
nad
equa
telycon
cealed
?High
riskofb
ias
Wereba
selin
eou
tcom
emea
suremen
tssimilar?
Unclearriskofb
ias
Wereba
selin
echaracteristic
ssim
ilar?
Lowriskofb
ias
Wereincompleteou
tcom
eda
taade
quatelyad
dressed?
Lowriskofb
ias
Waskno
wledg
eofth
eallocatedinterven
tionsade
quatelypreven
teddu
ringthestud
y?Unclearriskofb
ias
Wasth
estud
yad
equa
telyprotected
againstcon
taminati
on?
Unclearriskofb
ias
Wasth
estud
yfree
from
selecti
veoutcomerepo
rting
?Lowriskofb
ias
Wasth
estud
yfree
from
otherriskso
fbias?
Unclearriskofb
ias
Ove
rall
Risk
of B
ias J
udge
men
t Hi
gh ri
sk o
f bia
s

95Eff
ectiv
enes
s stu
dies
: As
sess
ed u
sing
the
GRA
DE a
sses
smen
t of q
ualit
y of
evi
denc
e26
Note:th
estud
iess
hownhe
rere
lateto
table7ofth
eeviden
ceta
bles.
Stud
y: S
huk-
Ngo
r et a
l (20
15)42
Outcome
No. of studies
Design
ROB
Inconsistency
Indirectness
Imprecision
Publication bias
Large magnitude effect
Dose-response gradient
Effect of plausible residual confounding
MEWS
Usual observation
Relative risk
Quality
Chan
ge in
m
anag
emen
t (noof
activ
ation
s)
1Non
-RC
TSe
rious
RO
BaN
o se
rious
in
cons
isten
cyN
o se
rious
in
dire
ctne
ssSe
rious
im
prec
ision
bN
o se
rious
pu
blicati
on
bias
No
larg
e eff
ect
N/A
N/A
1/10
of
269
1/20
of
275
2.0
(95%
CI1.1;
3.8)
Very
lo
w
Adve
rse
even
ts1
Non
-RC
TSe
rious
RO
BaN
o se
rious
in
cons
isten
cyN
o se
rious
in
dire
ctne
ssSe
rious
im
prec
ision
bN
o se
rious
pu
blicati
on
bias
No
larg
e eff
ect
N/A
N/A
1/26
91/27
51.02
(95%
CI
0.06
;16
.3)
Very
lo
w
a Do
wng
rade
don
elevelb
ecau
seth
eRO
Bforthiss
tudy
wasra
tedashigh.
bDo
wng
rade
don
elevelb
ecau
seofsmalln
umbe
rofe
ventsinthestud
y.

96De
velo
pmen
t and
val
idati
on st
udie
s – S
copi
ng R
evie
w:
Asse
ssed
usi
ng th
e Q
ualit
y As
sess
men
t Too
l ada
pted
from
NIH
(201
4)23
Note:th
estud
iess
hownhe
rere
lateto
table9ofth
eeviden
ceta
bles.
Crite
ria (Q
ualit
y As
sess
men
t Too
l ada
pted
from
NIH
(201
4))
Chal
len
et a
l (20
11)46
A Sc
opin
g re
view
1.W
asth
eresearchque
stion
oro
bjectiv
einth
ispa
perc
learlystated
?Yes
2.W
asth
estud
ypo
pulatio
nclea
rlysp
ecified
and
defi
ned?
N/A
3.W
asth
epa
rticipa
tionrateatlea
st50%
?N/A
4.W
ereallthe
sub
jectsselected
orrecruite
dfrom
thesameorsim
ilarp
opulati
ons(in
clud
ingthe
sametim
epe
riod)?Wereinclusionan
dexclusioncrite
riafo
rbeing
inth
estud
ypre-specified
and
ap
pliedun
iform
lyto
allpa
rticipa
nts?
Yes
5.W
asasa
mplesiz
ejustifie
d?N/A
6.W
ere
the
outcom
emea
sures(dep
ende
ntv
ariables)clea
rlyd
efine
d,v
alid,reliable,a
nd
implem
entedconsisten
tlyacrossa
llstud
ypa
rticipa
nts?
Yes
Qua
lity
Ratin
g (G
ood,
Fai
r, or
Poo
r)G
ood

97De
velo
pmen
t and
val
idati
on st
udie
s:
Asse
ssed
usi
ng th
e Q
ualit
y As
sess
men
t Too
l (ad
apte
d fr
om K
ansa
gara
et a
l 201
1)Note:th
estud
iess
hownhe
rere
lateto
tables10,11an
d12
ofthe
evide
ncetablesand
arepresented
alpha
beticallybyau
thor.
Stud
y (y
ear)
Adeq
uate
de
scrip
tion
of
popu
latio
na
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Albrightet
al(2
014)53
(Develop
men
t&
Valid
ation
)
Yes
No
(Onlythosewho
had
bloo
dcultu
reso
rinflu
enzasw
abwere
includ
ed)
Yes
(SOS(fo
rhighrisk
ofoutcome)≥6)
Yes
Yes
(New
instrumen
tagainsto
therED
system
;AURO
Can
dSO
S≥6versus<6)
Lowriskofb
ias
Alam
eta
l(20
15)76
(Validati
on)
Yes
No
(Recruitm
entb
etwee
n12
-8pm
only)
Yes
(NEW
S0-4,5-6,
≥7)
Yes
Unclear
(AURO
Crepo
rted
for
only2of4
outcomes)
Unclearriskof
bias
Arm
agan
et a
l (200
8)58
(Validati
on)
Yes
Unclear
(Noclea
rstatemen
t)Yes
(mEW
S>4)
Yes
Unclear
(Multi-varia
te
regressio
non
ly)
Unclearriskof
bias
Bulute
tal(20
14)59
(Validati
on)
Yes
Unclear
(Noclea
rstatemen
t)Yes
(MEW
S≥5
REMS>13
)
Yes
Yes
(Againstothersy
stem
;AU
ROC)
Lowriskofb
ias
Burchetal(20
08)45
(Validati
on)
Yes
No
(Every6thdayonly
and79
0pa
tients
includ
ed=70.2%
of
potenti
alstud
ycoho
rt)
Unclear
(IndicatesM
EWS
≥5bu
tnoclea
rstatem
ento
fcut-
offfo
rhighriskof
outcom
e)
Yes
Unclear
(Univaria
tere
gressio
non
ly)
High
riskof
bias
Catte
rmoleet
al(2
009)61
(Develop
men
t&
Valid
ation
)
Yes
Yes
Unclear
(Noclea
rstatem
ento
fcut-o
ffscoresfo
rsystem
s)
Yes
Yes
Agai
nst o
ther
system
s;m
ultiv
ariate
regressio
nan
dAU
ROC
Lowriskofb
ias

98St
udy
(yea
r)Ad
equa
te
desc
riptio
n of
po
pula
tiona
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Catte
rmoleet
al(2
014)62
(Develop
men
t&
Valid
ation
)
Yes
No
(Wee
kda
ysonly)
Unclear
(Noclea
rstatem
ento
fcut-o
ffscoresfo
rsystem
s)
Yes
Yes
(Againstother
system
s;m
ultiv
ariate
regr
essio
n an
d AU
ROC)
Unclearriskof
bias
Chris
tens
en
etal(20
11)69
(Develop
men
t&
Valid
ation
)
Yes
Yes
Yes
BEWS≥5
Yes
Yes
(BEW
S≥5versus
BEWS<5;se
nsitivity,
specificity)
Lowriskofb
ias
Cıldıretal(20
10)60
(Validati
on)
Yes
Unclear
(Noclea
rstatemen
t)
Yes
(Sep
sisdefi
ned
MEW
S>4
CCI>4)
Yes
Yes
(Againstother
system
s;su
rvivor
versusnon
-survivor
andAU
ROC)
Lowriskofb
ias
Cons
idin
e et
al
(201
5)78
(Validati
on)
Yes
Yes
(strati
fiedrand
om
sample)
Yes
(Singlepa
rameter
system
)
Yes
No
(OnlyMan
n-Whitney
Uand
KruskalW
allis
tests)
Lowriskofb
ias
Corfieldetal
(201
4)81
(Validati
on)
Yes
Yes
Yes
(N/Afo
rhigh
riskpred
ictio
ncut-o
ffscores
as d
evel
opm
ent
stud
y)
Yes
Yes
(Regression;su
rvivor
versusnon
-survivor
andAU
ROC)
Lowriskofb
ias
Dund
ar e
t al
(201
5)79
(Validati
on)
Yes
Yes
Yes
(opti
malcut-off
determ
ined
by
Youd
en’sinde
x)
Yes
Yes
(Twosystem
sco
mpa
red
and
AURO
C)
Lowriskofb
ias

99
Stud
y (y
ear)
Adeq
uate
de
scrip
tion
of
popu
latio
na
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Eicketa
l(20
15)70
(Validati
on)
Yes
Yes
Unclear
Cut-o
ffsfo
rDC
andMEW
S(high-
risk)notclearly
prov
ided
Yes
Yes
(Againstother
system
s;m
ultiv
ariate
regressio
n;
bootstrapp
ingan
dAU
ROC)
Lowriskofb
ias
Geiere
tal(20
13)71
(Develop
men
t&
Valid
ation
)
Yes
Yes
Yes
(ESI≤2;M
EWS
≥5
MED
S≥8;CCI≥
2)
Yes
Yes
(Againstothersy
stem
san
dAU
ROC)
Lowriskofb
ias
Grah
am e
t al(2
007)63
(Con
ferenceab
stract
only)(Va
lidati
on)
Yes
Yes
Unclear
(Insufficien
tde
tail)
Yes
Unclear
(Men
tionsAURO
Cbu
tinsufficien
tdetailto
fullyassess)
Unclearriskof
bias
Gueta
l(20
15)32
(Onlyab
stractin
En
glish
)(Va
lidati
on)
Unclear
Partialdetails
give
n in
resultsbut
no c
lear
st
atem
ent
onse
lecti
on
crite
ria
Unclear
No
clea
r sta
tem
ent
Yes
(MEW
S≥5)
Yes
Yes
(Multiv
ariate
regressio
nan
dMEW
Spo
sitive(≥
5)versus
MEW
Sne
gativ
e(0-4))
Unclearriskof
bias
Heitzeta
l(20
10)54
(Validati
on)
Yes
Yes
Yes
(N/Afo
rhigh
riskpred
ictio
ncut-o
ffscores
as d
evel
opm
ent
stud
y)
Yes
Yes
(Multiv
ariate
regressio
n;AURO
Can
dMEW
SMaxcut-of
scores(≥
1th
roug
hto
≥9))
Lowriskofb
ias

100St
udy
(yea
r)Ad
equa
te
desc
riptio
n of
po
pula
tiona
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Hoeta
l(20
13)64
(Validati
on)
Yes
No
(Noclea
rstatemen
tan
d8a
mto
6pm
recruitm
ento
nly)
Yes
(MEW
S≥4)
Yes
Yes
(Regression;AURO
Can
dMEW
S<4versus
MEW
S≥4)
Lowriskofb
ias
HockOng
eta
l(201
2)65
(Validati
on)
Yes
No
(Noclea
rstatemen
tan
d‘officehou
rs’
recruitm
ento
nly)
Unclear
(Cut-offsfo
rDC
andMEW
S(high-
risk)notclearly
provided
)
Yes
Yes
(MEW
SversusM
Lsystem
and
AURO
C)
Unclearriskof
bias
Howelleta
l(20
07)55
(Validati
on)
Yes
Yes
Unclear
(Referstoothe
rpu
blicati
onfo
rcalculati
ons)
Yes
Yes
(Againstother
system
s;re
gressio
nan
dAU
ROC)
Lowriskofb
ias
Joeta
l(20
13)73
(Validati
on)
Yes
Yes
Unclear
(Cut-offfor
VIEW
S-Lno
tclea
rlyprovide
d)
Yes
Yes(Ag
ainsto
ther
system
;AURO
C)Lowriskofb
ias
Joeta
l(20
16)72
(Validati
on)
Yes
Unclear
Yes(Opti
malcut-
offdetermined
by
Youd
enIn
dex)
Yes
Yes
(Againstother
system
s;AURO
C)
Lowriskofb
ias
Jone
seta
l(20
05)56
(Validati
on)
Yes
Unclear
(Noclea
rstatemen
t)Yes
(Predicted
mortality>50
%)
Yes
Yes
(Againstother
system
s;AURO
C)
Lowriskofb
ias
Junh
asavasdikuleta
l(201
3)74
(Validati
on)
Yes
Unclear
(Statesa
llbu
tno
clea
rstatemen
tif
consecuti
veenrolmen
toccurred
)
Unclear
(Vita
lsigncut-o
ffvaluesfo
rhigh-
riskno
tprovide
d)
Yes
Yes
(Multiv
ariate
regressio
nan
dR2
)
Unclearriskof
bias

101
Stud
y (y
ear)
Adeq
uate
de
scrip
tion
of
popu
latio
na
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Keep
eta
l(20
16)50
(Validati
on)
Yes
Yes
Unclear
(Cut-offvalues
forh
igh-riskno
tprovided
)
Yes
Yes
(NEW
Scut-o
ff≥1
throug
hto≥11;
AURO
C)
Lowriskofb
ias
Liuetal(20
14)66
(Develop
men
t&
Valid
ation
)
Yes
Unclear
(Noclea
rstatemen
t)Unclear
(Node
tailon
scores)
Yes
Yes
(Againstothersy
stem
san
dAU
ROC)
Unclearriskof
bias
Nai
doo
et a
l (201
4)44
(Validati
on)
No
(Selectio
ncr
iteria
un
clea
r)
No
(Every5thre
cord)
Yes
(TEW
S≥7)
Yes
Unclear
(TEW
S<7versus
TEWS≥7on
ly)
High
riskof
bias
Ngu
yen
et a
l (201
2)57
(Validati
on)
Yes
Unclear
(Onlypa
tientse
nrolled
inth
eregistryfo
rw
hom
all
3 ph
ysio
logi
c scoreswereavailable)
Yes
No
(Rep
orts
mortalitybu
titisno
tpre-
specified
or
defin
ed)
Yes
(Againstother
system
s;AURO
C)
Unclearriskof
bias
Olss
on&Lind
(200
3)67
(Develop
men
t&
Valid
ation
)
Yes
Yes
Unclear
(Noclea
rstatem
ento
ncut-
offsc
oresfo
rhigh
risk)
Yes
Yes
(Splitsample
techniqu
e;
multiv
ariate
regressio
n;AURO
C)
Lowriskofb
ias
Olss
oneta
l(20
04)68
(Develop
men
t&
Valid
ation
)
Yes
Yes
Unclear
(Noclea
rstatem
ento
ncut-
offsc
oresfo
rhigh
risk)
Yes
Yes
(Splitsample
techniqu
e;
multiv
ariate
regr
essio
n an
d AU
ROC)
Lowriskofb
ias

102St
udy
(yea
r)Ad
equa
te
desc
riptio
n of
po
pula
tiona
Non
-bia
sed
sele
ction
bAd
equa
te
prog
nosti
c fa
ctor
m
easu
rem
entc
Adeq
uate
ou
tcom
e m
easu
rem
entd
Met
hod
of
valid
ation
eO
vera
ll ris
k of
bi
as
Subb
eetal(20
06)51
(Validati
on)
Yes
Yes
Yes
(Cut-offscores
forrisk
predicti
on
provided
fore
ach
system
)
Unclear
(ICUadm
issions
repo
rted
but
outc
ome
not
pre-specified
or
defin
ed)
Yes
(Againstothersy
stem
s(correlatio
ns))
Lowriskofb
ias
Vorw
erk
et a
l (200
9)52
(Validati
on)
Yes
Yes
Yes
(Cut-offscores
forrisk
predicti
on
provided
fore
ach
system
)
Yes
Yes
(Byou
tcom
egrou
ps
andAU
ROC)
Lowriskofb
ias
Wan
getal(20
16)75
(Validati
on)
Yes
Unclear
(Only99
of2
34
initiallyeligiblehad
a
peri-arrestM
EWS)
Unclear
(Noclea
rstatem
ento
ncut-
offsc
oresfo
rhigh
risk)
Yes
Unclear
(Multiv
ariate
regressio
non
ly)
Unclearriskof
bias
Will
iam
s et a
l (201
6)77
(Validati
on)
Yes
Yes
Yes
(Tab
le1;score
>15
=50%
pr
edic
ted
mortality)
Yes
Yes
(Againstothersy
stem
san
dAU
ROC)
Lowriskofb
ias
Wilson
eta
l(20
16)43
(Validati
on)
Unclear
(Selectio
ncr
iteria
un
clea
r)
No
(Recruitm
ent
restric
tedtotimes
whe
n re
sear
ch te
am
available)
Unclear
(Cut-offvalues
notp
rovide
d)
Yes
Unclear
High
riskof
bias
a Stud
yde
scrib
esin
clusioncrite
riafo
rselectin
gpa
tients,and
fore
nrolledpa
tientsd
escribesdurati
onand
severityofsy
mptom
s,dem
ograph
ics(atleasta
ge),an
dsetting
(prim
ary
carevs.occup
ation
alvs.other).
bStud
yeitherre
portse
nrollin
g(ora
ttempti
ngto
enrol)a
con
secutiv
eserie
sofp
atien
tsm
eetin
ginclusioncrite
ria,o
rara
ndom
sample.
c Stud
yde
scrib
esre
prod
ucibleand
app
ropriatem
etho
dsfo
rmea
surin
gprog
nosticfactors
d Stud
yde
scrib
esre
prod
ucibleand
app
ropriatem
etho
dsto
defi
neand
iden
tifyou
tcom
ee Metho
dofvalidati
onisclearand
app
earsto
beap
prop
riate


Department of Health, Hawkins House, Hawkins Street, Dublin 2, D02 VW90, IrelandTel: +353 1 6354000 • Fax: +353 1 6354001 • www.health.gov.ie